
Abstract
Objective:
The objective of this study was to review the effectiveness and safety of a one stop urology clinic led by a consultant diagnostic urologist.
Methods:
Data were collected prospectively on all patients seen by a single consultant diagnostic urologist from February 2007 to February 2008. In 2013, patient records were reviewed and cross-referenced to identify if any patients had been re-referred to the urology service and why.
Results:
From 889 referrals, 799 patients attended, of these 689 (86%) were discharged after a single visit with 110 (14%) booked follow-up appointments. Ninety patients were re-referred, only two of these had a significant diagnosis. Thirty-four (38%) had a new referral reason.
Conclusion:
The one stop method of consultation is effective and efficient across a range of presenting complaints in urology. It is safe for patients and leads to a high discharge rate with a low re-referral rate without missing clinically significant diagnoses.
Introduction
Targets and performance objectives are an important part of the delivery of quality care to patients in the NHS. For example, the handbook to the NHS constitution states that patients have the ‘right to start consultant-led treatment within a maximum of 18 weeks from the referral for non-urgent conditions; and to be seen by a cancer specialist within a maximum of 2 weeks from GP referral, for urgent referrals where cancer is suspected’. 1 Outside of these imposed standards, clinicians have recognised that reducing the number of attendances in outpatient clinics improves the service for patients and is a more cost effective use of resources. 2
It is known that a single clinic visit thath combines consultation, imaging, diagnosis and discharge is proved to be of higher quality and efficiency. 3 Such models have been used for a range of pathologies and specialities as in breast surgery (breast lump clinic), 4 orthopaedic surgery (one stop hip assessment 5 and carpal tunnel clinic) 6 and gynaecology (infertility clinic). 7
One stop clinics have been advocated as the new standard in outpatient urological care. 2 The long term outcome, however, has not previously been investigated with regard to missed or delayed diagnoses. We aimed to determine the re-referral rate of patients seen and discharged after a single clinic visit in our one stop urology clinic and whether significant diagnoses had been missed.
Patients and methods
All patients referred from primary care, from February 2007 to February 2008, to a single diagnostic urologist at our centre were included. Data were collected prospectively. In 2013, patient records were revisited via an electronic clinical portal available at our trust. This is an electronic gateway through which we can review all clinic letters, investigations and referrals. A five year timescale was chosen as any significant diagnoses would have become apparent in this period.
The referrals were made using a standard proforma stating the reason and urgency of the referral. Two week wait and one stop haematuria clinics were included. All referrals were vetted by the diagnostic urologist and assigned to the appropriate clinic type.
The patients were seen in the urology centre by a dedicated team consisting of a diagnostic urologist, specialist nurse, staff nurse and healthcare assistant. Laboratory investigations, such as prostate-specific antigen (PSA), were requested in advance if appropriate. Investigations available on the day included urine dipstick analysis, diagnostic ultrasound, plain x-ray, transrectal ultrasound, uroflowmetry and flexible cystoscopy.
Outcome data were calculated using Microsoft Excel 2010.
Results
A total of 889 new referrals were made to the service; 799 (90%) attended their first outpatient appointment and 90 (10%) did not attend. Of the 799 that attended, 689 (86%) were discharged from the service as a result of the single clinic visit, and 110 (14%) patients were given follow-up appointments (Table 1). The most common reasons for referral in those patients that attended their initial referral were penoscrotal pathology (26%), haematuria (20%) and lower urinary tract symptoms (18%) (Table 2).
Summary of the follow-up outcome of patients who attended one stop urology clinic at the time of initial referral and re-referral.
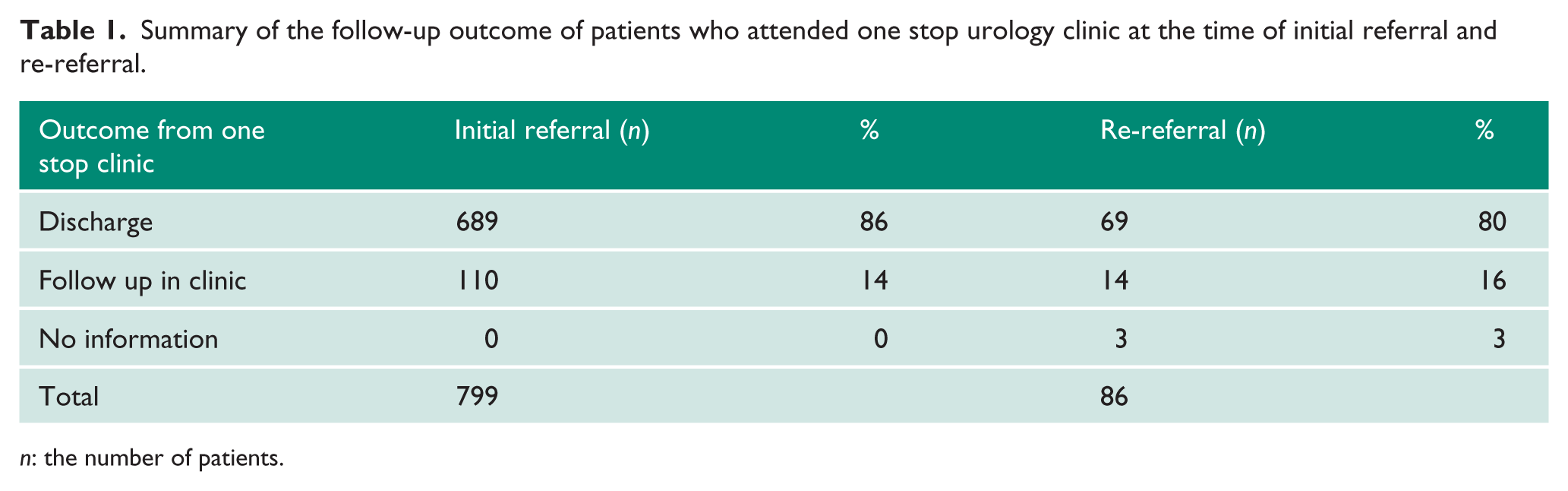
n: the number of patients.
Referral diagnosis at initial referral and re-referral appointments for patients who attended one stop diagnostic clinic.
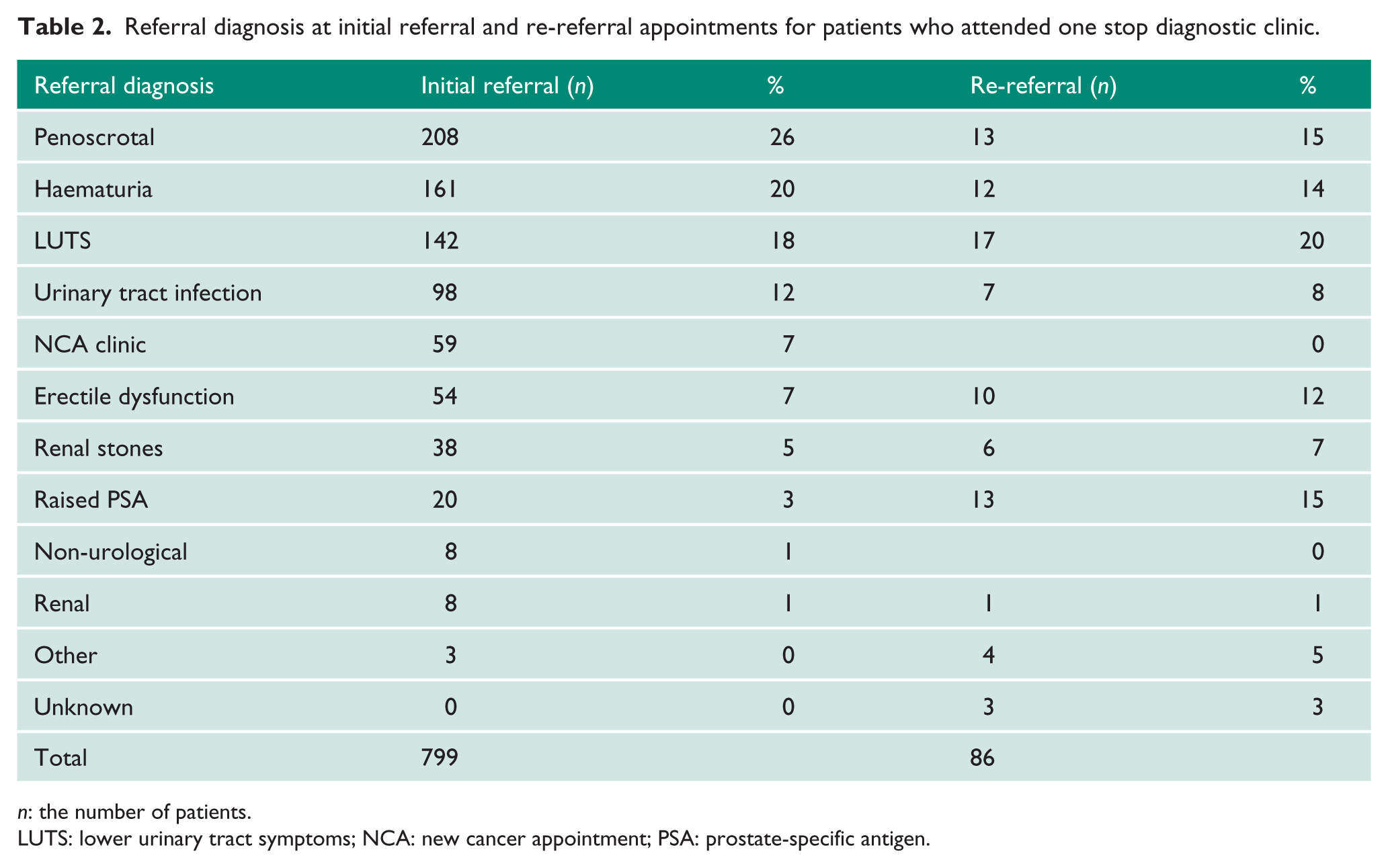
n: the number of patients.
LUTS: lower urinary tract symptoms; NCA: new cancer appointment; PSA: prostate-specific antigen.
Following the initial clinic visit 416 were discharged completely, with 273 patients dealt with in varying ways. The majority of these (156 patients; 23%) were given a date for day case surgery that did not require follow-up after the procedure. Ninety-five patients (14%) were referred to other subspecialist urologists or oncologists (Table 3).
Detailed outcomes of patients who attended one stop clinic and were discharged at initial and re-referral appointments.
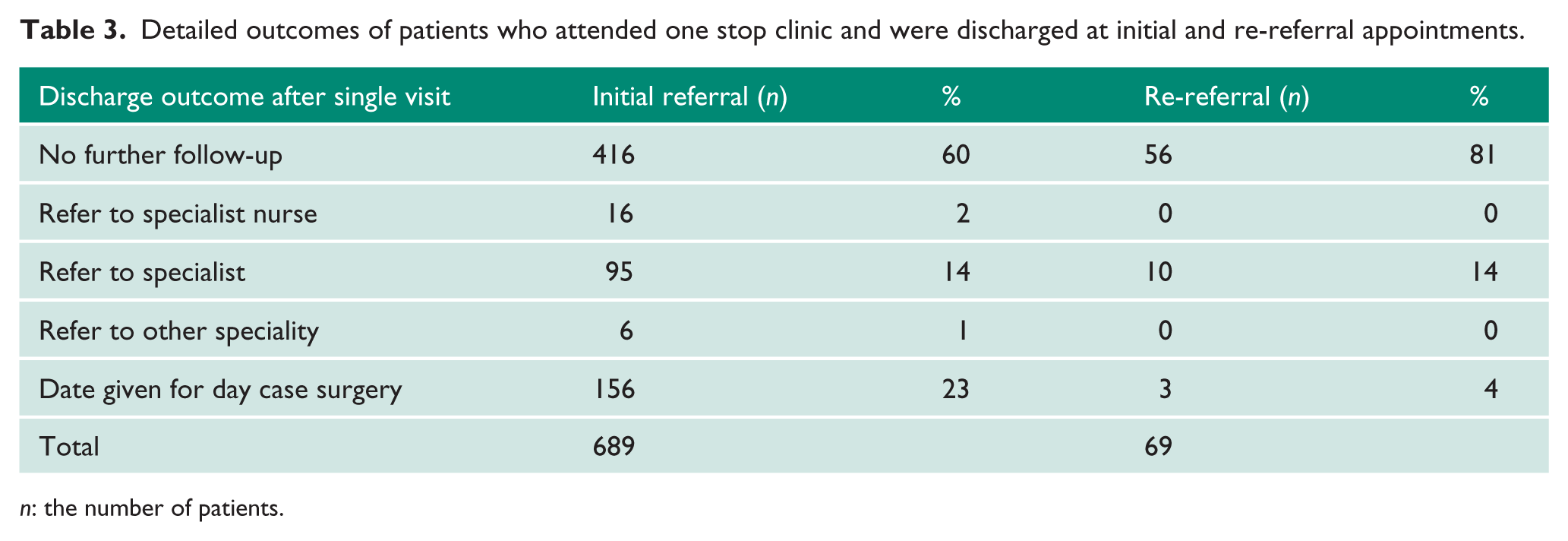
n: the number of patients.
Of the 90 who did not attend 85 were discharged directly back to their GP but five were booked a further appointment because they were suspected cancer referrals.
During the study period, 90 patients (10% of 889) were re-referred to the service. Four patients did not attend their re-referral appointment and 69 (80%) of those that did attend were discharged after a single clinic visit (Tables 1 and 3). A re-referral diagnosis was available for 87 of the re-referred patients, one of whom did not attend. The mean interval to re-referral was 29.2 months (median 25 months). Thirty-four of these (38%) were re-referred with a completely new problem and 12 (13%) had not attended their first appointment.
Only two patients (0.2%) were referred back with significant diagnoses. The first with a presentation of haematuria, who had declined further investigation at the first visit, was found to have transitional cell carcinoma of the ureter at 16 months. The second was re-referred with a raised PSA and had prostate biopsies confirming prostate cancer at 35 months. The most common reasons for repeat referral due to the same problem were deteriorating lower urinary tract symptoms (20%) and rising PSA above previously agreed levels (15%) (Table 2).
Discussion
We have demonstrated that the one stop method of consultation is effective and efficient across a range of presenting complaints, from open access haematuria clinic to urgent cancer referrals.
Accurate diagnoses can be provided within a single consultation in a safe manner. We have a high discharge rate at 86% and a low re-referral rate at 10%.
During a 62 month follow-up period only two patients (0.2%) were re-referred to the urology service where a significant diagnosis was found at 16 and 35 months, respectively. Upon review of the cases, the first patient had originally declined any further investigations. The second patient had been discharged with GP follow-up and re-referral instructions, which were accurately followed and with the patient receiving the appropriate care.
This study is the first to review re-referral rates in one stop urology clinics. It is widely established that one stop clinics are effective across a range of specialities regarding the accuracy of diagnosis.4–7 The re-referral rate has, however, not been examined. We can confidently state that one stop clinics accurately assess and treat patients with a re-referral rate of 10% across a five year survey.
The Institute of Medicine, in its landmark publication Crossing the Quality Chasm, 8 stated that, for care to be high quality, it must be effective, efficient, safe, patient centred, timely and equitable. All these criteria are met in a one stop approach.
One stop consultation is a complex clinical interaction; accurate communication is vital, especially as there is no second visit. All patients received a detailed letter prior to attending. This outlined what to expect on their visit and warned patients that their visit may be prolonged. All patients who were discharged received information on their diagnosis as well as a detailed management plan. Letters were sent to patients and GP practices detailing the visit, management plan, re-referral criteria and how to re-refer if necessary.
A one stop clinic requires not only dedicated and specific infrastructure but a change in mentality, way of working and the support of managers. It necessitates confidence from the clinician to provide a diagnosis in a single visit, as well as effective communication skills to counsel and reassure patients.
Cost benefit analysis was not undertaken in this study but the estimated number of appointments saved from the one stop haematuria clinic alone was 573.
Although we cannot compare our service to an alternative pathway, a patient satisfaction survey was undertaken in 2009 reviewing the one stop clinic model. This revealed that 85% of patients prefer the one stop approach to multiple appointments, and 90% of patients felt they were involved as much as they wanted to be in decisions about care and treatment. Similar results have been seen in the Norfolk model. 9
A potential weakness in our study is the possibility of patients being referred to another trust and another urology service.
Conclusion
The one stop method of consultation is effective and efficient across a range of presenting complaints in urology. It is safe for patients and leads to a high discharge rate with a low re-referral rate without missing clinically significant diagnoses.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
KE.
Contributorship
RH conceived the study. ST collected data. KE researched the literature and provided the data analysis. KE wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.