Monday 27 June 0900-1000 Room 3B Best Academic Paper Session Chair: Professor Howard Kynaston
1 Results of the British Association of Urological Surgeons female stress urinary incontinence procedures outcomes audit
S Cashman, N Thiruchelvam, R Morley
Bedford Hospital NHS Trust
Introduction: Following the government’s plans to publish individual surgeon’s outcome data in 2012, the British Association of Urological Surgeons (BAUS) initiated a number of nationwide audits in order to capture current UK practice and outcomes. We present the results of the first two years of the BAUS female stress urinary incontinence procedures outcomes audit.
Materials/Methods: Data from relevant procedures performed in 2013-2014 was prospectively entered into the online database. Metrics included both surgeon-specific and patient-specific data. The results were collated centrally by the BAUS audit office and subsequently analysed.
Results: 1381 procedures were reported, with 91 consultants submitting data from 72 centres, with increasing data submission from 2013 to 2014. A median of 11 procedures were performed by each consultant, with variability in the range of procedures performed by each individual. 93.5% of patients had pre-operative urodynamic assessment, with urodynamic stress urinary incontinence identified in 73.9% cases. No complications were recorded in 91% of procedures. In those patients with follow up data entered, patient reported outcome measurements demonstrated reduced pad usage in 86.6%, and ICIQ sum score improvement in 92.2%.
Conclusion: Initial results demonstrated good clinician engagement, with increasing year on year uptake. Some initial areas for improvement within the database have been identified. Variation in the number and range of procedures offered by individual clinicians has been identified. Perioperative complication rates were comparable to those reported in other series, with good patient outcomes measures reported. We hope data entry will continue to improve in the coming years.
2 Randomised controlled trial of ultra mini percutaneous nephrolithotomy versus retrograde intrarenal surgery in the treatment of 10-30mm calculi
SN Datta, K-W Ng, R Solanki, Janak Desai
Colchester Hospital University Foundation Trust
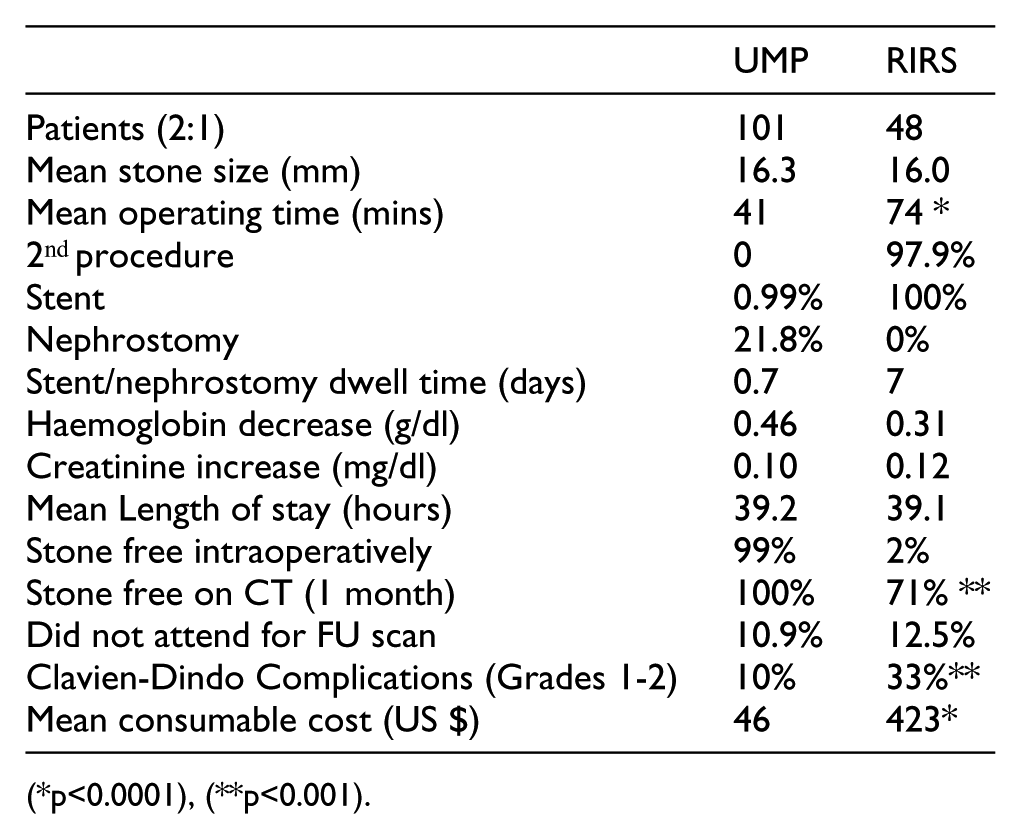
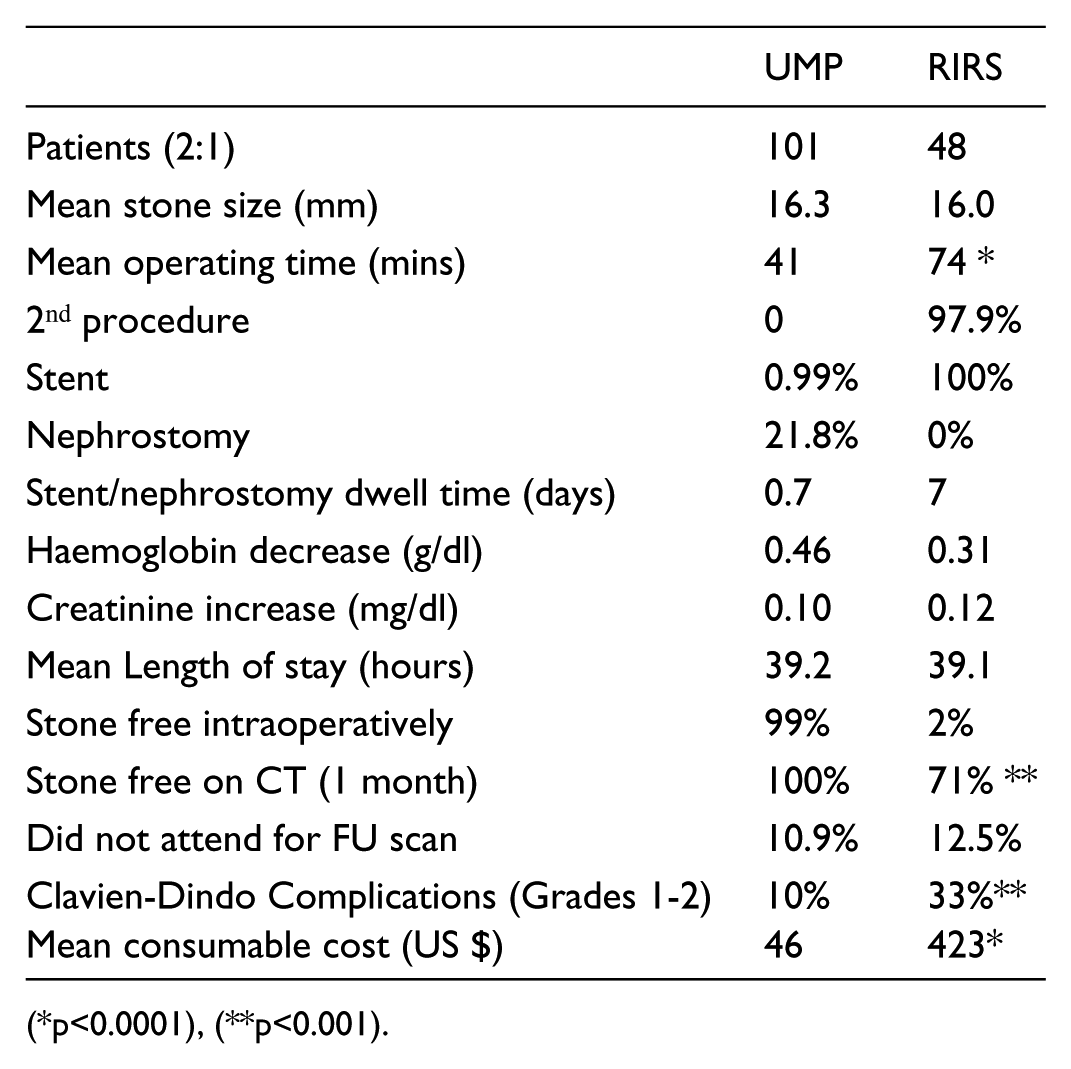
Introduction: Recently it has been shown prospectively, that Ultra Mini PCNL (UMP) is safe and effective in treating renal 1-3 cm calculi. The objective of this study was to compare UMP and RIRS in a Randomised Controlled Trial (RCT).
Methods: Prospective RCT of UMP and RIRS with an allocation ratio of 2:1 in favour of UMP by a single surgeon. Ethical committee approval was obtained and all patients provided informed consent. Effectiveness was assessed by stone-free rates, operative time, complication rate, length of stay and consumable cost. Inclusion criteria were 1-3cm stones with no history of bleeding diathesis and screened for infection.
Conclusions: UMP has a superior stone free rate and fewer complications compared to RIRS in this prospective randomised study in the treatment of 1-3cm stones. There is no routine need for stenting and the cost of consumables is almost one tenth of RIRS. Further multi-centre studies are required but UMP should be considered strongly as a first line treatment.
3 A urinary peptide biomarker panel to identify significant prostate cancer
MJS Salji, A Latosinska, A McKay, J Clark, H Mischak, HY Leung
CRUK Beatson Institute
Background: Urinary biomarkers which can identify patients with significant prostate cancer (PC) used as an adjunct to PSA testing is an attractive clinical prospect. Capillary electrophoresis coupled to mass spectrometry (CE-MS) is a tool for the discovery of such potential urinary peptide biomarkers.
Methodology: CE-MS was performed on 313 samples of urine obtained from patients with significant PC with Gleason 8-10 or T3/4 disease (n=66) and controls with High Grade -PIN, low volume low grade Gleason 6 disease, Prostatitis, BPH or normal histology (n=247). An initial training set of 236 patients was used to identify a biomarker panel separating controls (n=188) from significant PC (n=48). Performance was then compared to PSA by ROC analysis in a clinical test set (n=77, 18 cases and 59 controls) classified by PSA.
Results: A panel of 94 peptides were identified in the training cohort separating significant PC and controls (p<0.05, using Benjamini and Hochberg adjustment and bootstrapping cross validation). ROC analysis showed an AUC=0.82 for our biomarker panel in the training cohort. As expected the AUC for PSA in the test cohort was almost perfect (0.968) as it was classified by PSA. Our biomarker panel showed AUC of 0.69 in the test cohort which significantly differed from PSA (p<0.001).
Conclusions: Using CE-MS we have generated a 94 peptide urine biomarker panel specifically to identify significant PC from insignificant disease. Our biomarker panel shows differing ROC to PSA in an independent PSA classified test cohort and may provide a useful adjunct to PSA testing.
4 The significance of close surgical margins in organ sparing surgery for penile squamous cell cancer
D Sri, A Sujenthiran, W Lam, C Corbishley, BE Ayres, N Watkin
St Georges Hospital
Introduction: Organ sparing surgery (OSS) for penile squamous cell cancer (pSCC) is established. A 5mm margin has previously been considered oncologically safe. This study evaluates the significance of close surgical margins in OSS and clinico-pathological factors that may influence local recurrence.
Patients: Analysis was carried out on an on-going prospective database, which includes accurate recording of surgical margins. Between March 2001 and September 2012, 332 patients treated with OSS for pSCC had clear surgical margins. Local recurrence was defined as residual invasive disease not identified at first surgery. Fisher’s exact test was used to analyse the impact of close surgical margins on local recurrence.
Results: Of 332 patients 64% had < 5mm clear deep surgical margin with 16% clear by <1mm. Overall, 15 patients (4%) had local recurrence, with a median time to recurrence of 6 months. Eight were embolic spread and 7 residual contiguous disease. Lymphovascular invasion (LVI) was present in 67% and cavernosal involvement in 27%.
There was a statistically significant relationship between cavernosal involvement (p = 0.04), LVI (p = 0.0001) and local recurrence. There was no significant relationship (p= 1.00) with close surgical margins (<5mm vs. >5mm). However a margin of <1mm did show increased risk of local recurrence (p=0.0003).
Conclusions: Recurrence due to contiguous residual disease in margin clear OSS in our experience is very low (2%). Tumour embolism is as likely to occur. We conclude that a deep clear margin of 1mm or more is sufficient in the absence of LVI and/or cavernosal involvement.
5 Significance of negative margin in nephron sparing nephrectomy and its implications on disease free survival
A Shafik, A Kodera, T King, N Hicks, T Chen, A Makar
Worcester Royal Hospital
Introduction & Objectives: We present long term oncological outcomes of nephron sparing surgery over a period of 11 years and 10 months. Our study focuses on the impact of surgical margin on disease recurrence with a mean follow up of 8.5 years.
Method: A total of 162 patients underwent either open (146) or laparoscopic (16) partial nephrectomy in the period from November 2003 till September 2015 at a UK District General Hospital. Data was retrieved from a prospectively maintained data base.
Results: A total of 162 patients were identified, of these 146 had an open partial nephrectomy and 16 had laparoscopic surgery. Post-operative histology revealed renal cell carcinoma in 119 cases (73.4%), with the remaining cases having benign histopathology. Of the malignant cases, pathological staging was PT1a in 75 cases (46.2%), PT1b in 32 cases (19.7%), PT2 in 2 cases (1.2%), PT3a in 9 cases (5.4%) and PT3b in one case (0.6%).
In 10 cases (6%) there were positive surgical margins. This subgroup had a mean follow-up of 7 years, 8 months over which there were no cases of recurrence. Recurrence did occur in 3 cases (1.8%), 2 of which were local recurrences requiring radical nephrectomy and one of which developed metastatic disease that required systemic therapy. Median post-operative follow-up was 8.5 years.
Conclusions: Our study demonstrates no correlation between positive surgical margin and local recurrence. A negative margin did not preclude future local recurrences. 8.5 years follow up demonstrates a low rate of recurrence following partial nephrectomy for localized renal tumours.
6 Open radical cystectomy in the UK – the current standard of care? Analysis of the BAUS cystectomy audit
ER Jefferies, J Cresswell, JS McGrath, C Miller, L Hounsome, S Fowler, EW Rowe
Cheltenham General Hospital
Introduction: The enhanced data entry into the BAUS database since becoming mandatory for 2014-15 has enabled greater assessment of surgical outcomes following radical cystectomy. The aim of this paper is to establish comprehensive UK standard outcomes (using the available metrics) for open radical cystectomy over a two-year period.
Materials and Methods: All open radical cystectomies performed in the last two years and recorded in the BAUS database were analysed.
Results: Data entry into the BAUS cystectomy audit has increased from 37% to ~80% following its mandate and we would expect this to increase following the March 2016 deadline for 14/15 data, ready for June presentation. Early analysis of 1751 open radical cystectomies shows 73.3% were performed on men with a median age of 69. The median number performed per consultant was 11 (range 1-75) and 19 per centre (range 1-92). 58.1% was for preoperatively staged T2+ disease. Neobladder diversion rate was 6.3%. Lymph node dissection was performed to level 1, 2, 3 in 20.5%, 49.8% and 11% respectively. The transfusion rate was 30.4%. The intraoperative rectal injury rate was 1.1%. We expect complications will be under-reported due to the nature of the audit but are reported as 10.5% (Clavien Dindo 3-5).The positive margin rate was 10%. The median length of stay was 12 days. The reported 30 & 90-day mortality were 0.8% and 1.6% respectively.
Conclusions: We now have a UK benchmark of care to compare any future techniques or modifications (such as enhanced recovery or minimally invasive techniques).
Tuesday 28 June 1045-1215 Room 4 ePoster Session 1 - Endourology Chairs: Jake Patterson & Marius Conradie
P1-1 Recurrence of kidney stones: A UK cohort study
J Tanner, K Subramonian
Queen Elizabeth Hospital, Birmingham
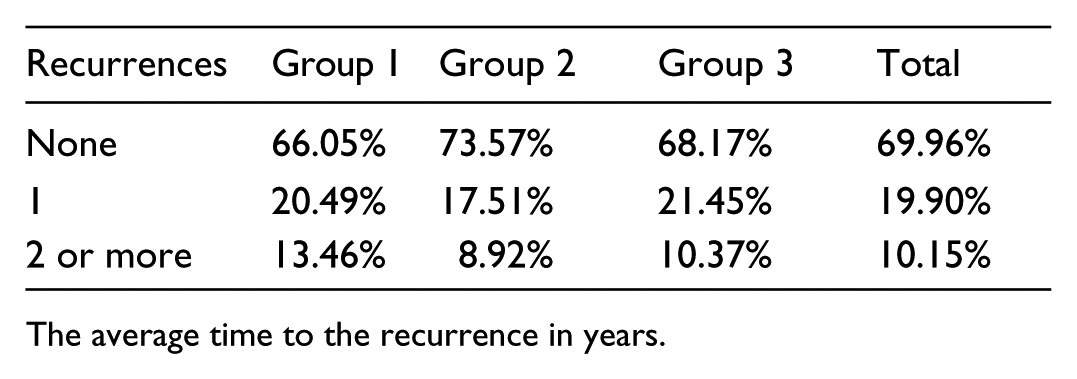
Aims: Kidney stone recurrence rate varies in different populations. There are no long term studies in the UK looking at the recurrence rate. We aim to study a large cohort of stone patients presenting in 2005 for recurrence over 10 years.
Methods: HES data was searched for stone-related episodes in 2005/06, yielding 13,880 patients. Patients with previous history of stones were excluded resulting in 8062 patients. Patients were classified based on the intervention into: Group 1 undergoing PCNL, Group 2 undergoing Ureteroscopy and Group 3 undergoing Lithotripsy.
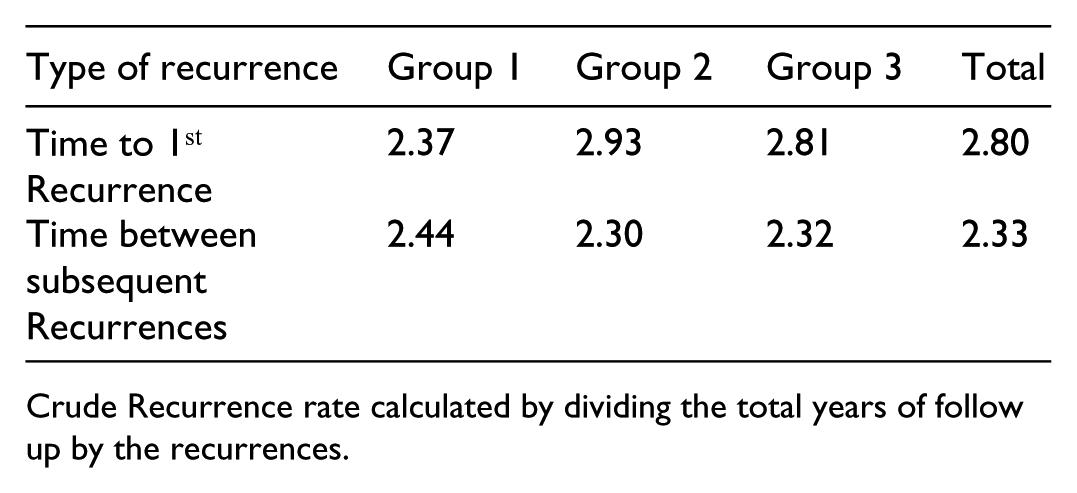
Recurrent episodes of stone-related admission for this cohort was recorded for next 10 years and data analysed for rate and time to recurrences and the crude recurrence rate per person years.
Results: (P1-1)
Recurrences
Group 1
Group 2
Group 3
Total
None
66.05%
73.57%
68.17%
69.96%
1
20.49%
17.51%
21.45%
19.90%
2 or more
13.46%
8.92%
10.37%
10.15%
The average time to the recurrence in years.
Type of recurrence
Group 1
Group 2
Group 3
Total
Time to 1st Recurrence
2.37
2.93
2.81
2.80
Time between subsequent Recurrences
2.44
2.30
2.32
2.33
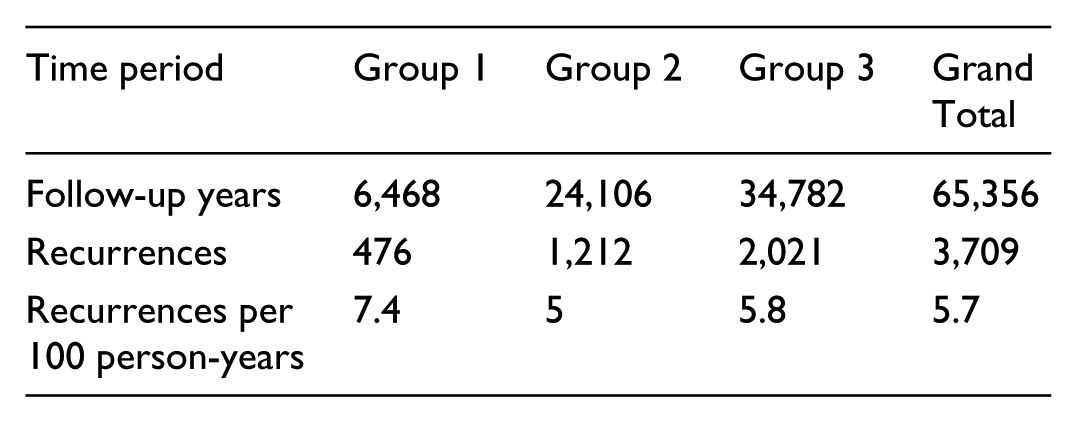
Crude Recurrence rate calculated by dividing the total years of follow up by the recurrences.
Time period
Group 1
Group 2
Group 3
Grand Total
Follow-up years
6,468
24,106
34,782
65,356
Recurrences
476
1,212
2,021
3,709
Recurrences per 100 person-years
7.4
5
5.8
5.7
Conclusion: This large cohort study shows that overall 30% patients get recurrent stone disease over a 10 year period and mean time to first recurrence of 2.8 years. These results provide guidance in counselling patients and help in planning follow up.
P1-2 Urolithiasis represents a significant and growing burden for the NHS: a contemporary assessment of urinary stone related clinical activity within the NHS in England
SJ Srirangam, P Cleaveland, L Olson
Royal Blackburn Hospital
Introduction: Current evidence suggests that kidney stone related hospital activity is increasing. We seek to understand the contemporary burden of kidney stone disease on the NHS in England.
Materials and Methods: We interrogated Dr Foster Intelligence (http://www.drfoster.com), a publically available provider of hospital information to identify urolithiasis related elective and non-elective activity in acute hospitals in England for 5 years up to September 2015.
Results: Data was available on 137 English acute hospitals trusts. Across most measurable parameters over a 5-year period, all urolithiasis related activity in England has increased. Total (elective/emergency) activity increased by 9.3% from 68,604 to 74,975 per year over a 5-year period. Non-elective, emergency urolithiasis related activity increased by 11.1% from 34,647 to 38,506 per year resulting in a total LOS of 5891 days. With regards to elective activity, ureteroscopy procedures for stone extraction increased substantially (61.6%) from 8578 to 13,862 procedures/year. The trend for PCNL procedures (from 3149 to 3308 (5% increase)) and ESWL (from 21,758 down to 21,375 (1.8% decrease)) remained relatively stable. Urolithiasis remains a contributor to 28-day non-elective mortality with 46 deaths/year (0.15% mortality) compared to 46 deaths/year five years ago (0.20% mortality).
Conclusions: Kidney stone disease places enormous demands on the English NHS but is often side-lined in favour of cancer-related policies. Its prevalence appears to be rising and requires a multi-pronged approach including appropriate workforce planning, improved understanding of treatment cost-effectiveness, development of national strategies to reduce stone recurrence and co-ordinated epidemiological research to manage the challenge for the future.
P1-3 Audit of emergency re-attendance post-ureteroscopy at a district general hospital
CE Lovegrove, N Shrotri
Guy’s Hospital, London
Introduction: The British Association of Urological Surgeons (BAUS) and European Association of Urology (EAU) published guidelines regarding the use of forceps, stone baskets and post-operative stenting when extracting renal or ureteral stones. Surgical practice is variable and this audit sought to examine:
Trends in initial ureteroscopy procedures
The timing of re-attendance
Common causes of re-attendance
Instrumentation used in the initial ureteroscopy procedure; is there a relationship with re-attendance?
Subsequent management
Patients and Methods: Retrospective audit was conducted of all patients who underwent ureteroscopy at Kent and Canterbury Hospital and had a subsequent emergency re-attendance from November 2013 to October 2014. Data regarding timing, symptoms, investigation and management was systematically extracted from patient records.
Results: In one year 237 ureteroscopies were undertaken with an emergency re-attendance rate of 11.81%. Patients were most likely to re-attend the emergency department within one week of their initial presentation due to stent symptoms, most frequently flank pain. 72.22% patients had stone extraction via instrumentation of the urinary tract though no causality with emergency re-attendance could be ascertained. Of those who re-attended, 28.57% underwent a subsequent procedure.
Conclusions: Ureteroscopy was largely undertaken to address the presence of stones within the urinary tract. Emergency re-attendance was most frequently attributable to stent symptoms, though causality with instrument use for stone retraction could not be confirmed. Future work should focus on prospective assessment of overall use of stone baskets and forceps in ureteroscopy and promoting thorough annotation in surgical records.
P1-4 Predictors for spontaneous stone passage at acute presentation
HK Sra, C Cumby, T Bracewell, R Kucheria, A Goyal
Royal Free Hospital NHS Trust
There remains significant variation in the likelihood of spontaneous stone passage among patients presenting acutely with ureteric colic. We evaluated the relationships between commonly assessed radiological and laboratory and stone passage.
All patients presenting with unilateral acute ureteric colic from Jan 2015 to Jun 2015 that did not undergo acute surgical intervention were retrospectively analysed. Univariate and multivariate analysis was conducted to identify factors which significantly contributed to stone passage.
Of 132 patients presenting with acute ureteric colic who did not undergo acute intervention, 90 patients were included. Determination of stone passage was made by further imaging after 4 weeks from initial presentation – 93% underwent NCCT. Spontaneous stone passage was observed in 71 (78.9%). Univariate analysis revealed that increasing stone size (p=0.029), and prolate ellipsoid model stone volume (p=0.0004) were significantly predictive of failure to expel the stone with a stone volume mean of 45.5 in the successful group compared to 125.7 in those that failed to expel their stones. Further, white cell count (p=0.026) and stone density (HU) (p=0.0030) were significant predictors of stone passage in our study. CRP, creatinine or degree of hydronephrosis at time of presentation did not demonstrate a significant relationship.
Increasing stone size and especially stone volume was found to be associated with a decreased likelihood of stone passage, as was stone density and white cell count. These factors are easily assessed with NCCT at initial presentation and should be considered when deciding on whether to pursue expectant management.
P1-5 Do stones still kill? An analysis of death from stone disease 1999 to 2013 in England and Wales
FEC Kum, W Mahmalji, J Hale, K Thomas, M Bultitude, J Glass
Guy’s and St. Thomas’ Hospitals, London
Introduction: Urolithiasis has an estimated lifetime risk of 12% in males and 6% in females. It is not perceived as a life-threatening pathology. Admissions with urinary calculi contribute to 0.5% of all inpatient hospital stays. The number of deaths attributable to urolithiasis has yet to be identified.
Materials & Methods: Office of National Statistics Data relating to causes of death from urolithiasis, coded as ICD-10 N20-23, was collated and analysed for the 15 year period from 1999-2013 in England and Wales. This data is sub-categorised into anatomical location of calculi, age and gender.
Results: 1954 deaths were attributed to urolithiasis from 1999-2013 (mean 130.3 deaths/year). Of which, 141 were attributed to ureteric stones (mean 9.4 deaths/year). Calculi of the kidney and ureter accounted for 91% of all deaths secondary to urolithiasis; lower urinary tract (bladder or urethra) calculi contributed to only 7.9% of deaths.
Data revealed an overall increasing trend in mortality from urolithiasis over this 15 year period with an increase of 3.8 deaths/year based on a linear trend (R2 0.65).
Overall, the number of deaths in females was significantly higher than in males, (ratio 1.5:1, P<0.001); kidney and ureteric calculi causing death had a female preponderance (1.7:1, F:M); whereas calculi of the lower urinary tract in males was more common (1:2.2, F:M).
Conclusions: Stone disease still causes death in the 21st century in England and Wales. The trend to increased deaths must be placed in the context of an increasing incidence of stone disease in the UK.
P1-6 PCNL access by Urologist or Radiologist: An analysis of the BAUS PCNL Registry
JN Armitage, S Fowler, WJ Finch, NA Burgess, SO Irving, J Withington, J Glass, OJ Wiseman
Addenbrooke’s Hospital
Introduction and Objective: Obtaining percutaneous access to the renal collecting system is fundamental to safe and effective PCNL. Practice varies between countries, hospitals and individual surgeons as to whether access is obtained by a urologist or an interventional radiologist (IR). We compared outcomes of urologist versus IR tracts.
Methods: Data submitted to the BAUS PCNL data registry between 2009 and 2015 were analysed according to whether access was obtained by a urologist or an IR. We evaluated access success, number and type of tracts, perceived and actual access difficulty, as well as outcomes including stone free rate, length of stay and complications including transfusion rates.
Results: Overall, percutaneous renal access was undertaken by an IR in 3,453 of 5,211 procedures (66.3%); this rate appeared stable over the entire study period, for all categories of stone complexity and in cases where there was predicted or actual difficulty with access. Only 1% of procedures were abandoned because of failed access and this rate was identical in each group.
IRs did more multiple tracts than urologists (6.8% vs 5.1%, p=0.02) but did similar rates of supracostal punctures (8.2% vs 9.2%, p=0.23). Ultrasound was used more commonly by IRs than urologists to guide access (56.6% vs 21.7%, p=0.0001). There were no significant differences in complication rates, lengths of stay or stone free rates.
Conclusions: Our findings suggest that favourable PCNL outcomes may be expected where access is obtained by individuals who have been appropriately trained and who are skilled and proficient in the procedure.
P1-7 Assessing the Volume-Outcome Relationship for PCNL in 2014 - Analysis using BAUS Registry Data of over 2000 cases
JM Withington, WJG Finch, S Fowler, JN Armitage, JM Glass, SO Irving, NA Burgess, K Thomas, OJ Wiseman
Whittington Hospital
Introduction: This study investigates the relationship between PCNL stone clearance and hospital volume, adjusted for stone complexity, using the British Association of Urological Surgeons registry.
Patients and Methods: Prospective registry data from 2014 were analysed.
Dividing cases at an annual volume threshold of 20 generated two approximately equal-sized groups. Comparisons were made between these groups, including stone complexity, stone clearance at day one, transfusion, sepsis and median length of stay (LOS) and for subgroups of complex (Guy’s Stone Score III-IV) and non-complex (GSS I-II) stones.
Results: 2042 procedures were recorded in 2014, from 129 hospitals. There was no significant difference between stone complexity of cases undertaken at high and low volume centres (p=0.056).
Transfusion rates did not differ significantly between high and low volume groups (2.5% vs 2.6%, p=0.92), including when subdivided by stone complexity (GSS III-IV: 3.0% vs 4.9%, p=0.22; GSS I-II, 0.9% vs 2.2%, p=0.09).
Post-operative sepsis occurred after 3.1% procedures. Volume made no significant difference overall (p=0.1), in complex (p=0.09) or non-complex stones (p=0.97).
Stone clearance was higher in the high volume group (73% vs 63%, p<0.05). This was true for both complex and non-complex stones (55% vs 45%, p<0.05; 85% vs 77%, p<0.05). LOS was shorter at high volume centres (2d vs 3d).
Conclusion: Volume was not significantly associated with transfusion or sepsis rates; stone complexity appears more relevant to complications. Stone clearance, however was associated with volume, for both complex and non-complex stones. Length of stay appears shorter in high volume centres. These findings inform the debate around centralisation of complex PCNL.
P1-8 5000 cases from the BAUS PCNL Registry - a changing population and practices?
WJG Finch, L Derbyshire, RC Calvert, S Fowler, JN Armitage, J Glass, J Withington, OJ Wiseman, SO Irving, NA Burgess
Norfolk and Norwich University Hospital
Introduction: PCNL continues to be used to treat large renal stones. This study evaluates changes in UK PCNL practice, patients and outcomes 2010-2015 using a national registry and defines the comorbidities of this population in the UK in 2014.
Materials and Methods: The BAUS PCNL registry was analysed with 5285 cases to evaluate trends in patient demographics, operative technique, outcomes and complications and compared with previous analysis of 1028 cases in 2011. 2042 cases from 2014 with detailed co-morbidity data were analysed to assess health of patients undergoing PCNL.
Results: Gender and age of patients undergoing PCNL remains unchanged. Most PCNL is prone, but supine has significantly increased (16.2% vs. 6%, p=0.0001). Access by interventional radiologist has increased slightly (66.2% vs. 62%, p<0.006). Balloon tract dilatation has increased in popularity (63.4% vs. 48%, p=0.0001). More Consultants perform PCNL themselves compared with 2011 (84.4%vs.79%, p=0.0001). Ultrasound fragmentation devices are more widely used (48.8% vs 42.2%, p=0.0002) with lift-out PCNL less commonly reported (-5.6%, p=0.0001). Comparison with 2011, stone free rates are unchanged and complications similar (visceral injury 0.3%, transfusion 2.4%). 2014 co-morbidity data revealed 41% of patients were obese/very obese. Few patients have significant comorbidities measured by the Charlson comorbidity index with age-adjustment (14% with score ⩾5)
Conclusions: The BAUS PCNL registry is a unique resource for UK surgeons, providing vital information on current practice, and a useful baseline to measure changes in future PCNL practice. Using the registry allows audit of individual practice against national outcome data and helps surgeons counsel patients as to possible outcomes for this complex endourological procedure.
P1-9 Do patients with urinary diversions have worse peri-operative outcomes after percutaneous nephrolithotomy?
M Bolgeri, G Mazzon, V Arumuham, R Dale, C Allen, S Allen, D Smith, S Choong
University College Hospitals
Introduction: Percutaneous nephrolithotomy is challenging in patients with urinary diversions due to difficult retrograde access, stone- and patient-related complexity.
Internationally adopted stone complexity scores place them in the highest-risk categories.
We reviewed the peri-operative outcomes of PCNLs in these patients at our tertiary referral centre.
Material and methods: PCNLs performed between 2008 and 2014 in patients with urinary diversions were included.
Stone parameters, success rate and peri-operative outcomes were compared to 50 controls with normal lower urinary tract.
Subgroup analyses were performed comparing different types of diversion.
Results: 42 patients were included (5.2% of all PCNLs).
Stone complexity was higher in the diversion group (Guy’s score 3-4 in 83.3% vs 48%, p=0.001), with higher prevalence of struvite composition and positive stone culture (p<0.001).
Ultrasound-guided access was successful in 100% of cases.
Complication rates were similar, but length of hospital stay was longer in diversion patients (6 vs 4 days, p=0.03).
Stone-free rate was comparable (52.4 vs 65.3%, p=0.3).
Patients with ileal conduits had longer hospital stays, while colonic continent diversions showed more infected stones (80% vs 47.1%, p<0.001).
Conclusions: Within a specialized tertiary centre, the outcomes of PCNLs in patients with urinary diversions appear to be non-inferior.
Proficiency in ultrasound-guided access is necessary to achieve technical success.
The knowledge of biochemical and microbiological profiles associated with specific types of diversion could contribute to a more insightful pre and perioperative management.
P1-10 Randomised controlled trial of ultra mini percutaneous nephrolithotomy versus retrograde intrarenal surgery in the treatment of 10-30mm calculi
SN Datta, K-W Ng, R Solanki, Janak Desai
Colchester Hospital University Foundation Trust
Introduction: Recently it has been shown prospectively, that Ultra Mini PCNL (UMP) is safe and effective in treating renal 1-3 cm calculi. The objective of this study was to compare UMP and RIRS in a Randomised Controlled Trial (RCT).
Methods: Prospective RCT of UMP and RIRS with an allocation ratio of 2:1 in favour of UMP by a single surgeon. Ethical committee approval was obtained and all patients provided informed consent. Effectiveness was assessed by stone-free rates, operative time, complication rate, length of stay and consumable cost. Inclusion criteria were 1-3cm stones with no history of bleeding diathesis and screened for infection.
Conclusions: UMP has a superior stone free rate and fewer complications compared to RIRS in this prospective randomised study in the treatment of 1-3cm stones. There is no routine need for stenting and the cost of consumables is almost one tenth of RIRS. Further multi-centre studies are required but UMP should be considered strongly as a first line treatment.
P1-11 Normocalcemic Hyperparathyroidism - an unexplored factor in recurrent stone disease?
HE Smith, RA Chapman, SG Kata
Ninewells Hospital
Introduction: Urolithasis is a common urological condition which often recurs and results in hospital admissions and outpatient appointments. Urolithiasis is often a symptom of underlying endocrine conditions including hyperparathyroidism. Current EAU guidelines (2014) recommend metabolic screening in all patients with stones. This includes creatinine, uric acid, ionised calcium, sodium and potassium for all patients and 24h urine collection for high risk patients. It does not recommend routine testing of parathyroid hormone.
Patients and Methods: This is a retrospective study of new (n=157) and recurrent (n=193) stone formers over a 33 month period. All stone formers routinely had PTH and vitamin D tested in addition to the standard screening.
Results: We found that 67/350 (19.1%) of all patients had raised PTH. This was more prevalent in the recurrent group, 44/193 (22.8%) than the new stone formers 23/157 (14.6%). Of the patients with raised PTH 58/67 (86.6%) had normal calcium levels. Of the patients with normocalcemic hyperparathyroidism, 88.7% had low vitamin D levels with an average level of 27 nmol/L.
Conclusions: Our study has shown a surprising number of patients with recurrent stones have normocalcaemic hyperparathyroidism, most of these are also insufficient in vitamin D. We would suggest including PTH testing in all recurrent stone formers and if raised, vitamin D and 24h urinary calcium should be measured. Treatment of normocalcemic hyperparathyroidism could be an important strategy in reducing stone recurrence. Further study of recurrent stone formers and the assessment of urinary calcium loss and the role of vitamin D in normocalcaemic hyperparathyroidism is required.
P1-12 Prevalence of hypertension and renal impairment in patients with cystinuria
FEC Kum, K Wong, D Game, J Glass, M Bultitude, K Thomas
Guy’s and St. Thomas’ Hospitals, London
Introduction: In the healthy adult population, prevalence of hypertension (BP⩾140/90mmHg) is 31% in men and 27% in women, and increases with age. Patients with calcium urolithiasis have significantly higher blood pressures compared to matched individuals, with a mean systolic difference of 16.8mmHg.
We present the frequency of hypertension and renal impairment in a large cohort of cystinuric patients.
Materials & Methods: A database was created to include all patients who attend a specialist cystinuria service. Data included basic demographics, diagnosis of hypertension, and factors indicating renal function. CKD (chronic kidney disease) stage was recorded as per Kidney Disease Outcomes Quality Initiative guidelines.
Results: 131 patients attend the service, 6 patients were excluded due to incomplete data, leaving 125 patients included. Mean age was 40.3 years (range 3.5-76 years). Prevalence of hypertension was 48.8% (n=61), with a strong male preponderance (67.2% vs. 32.8%). Of these, 50 were taking regular antihypertensive medication.
Mean creatinine was 87.4µmol/l and eGFR was 77.6 (range 32-127). All patients with previous nephrectomy (n=10) or a poorly functioning kidney (n=18) have renal impairment (CKD stage 2 or 3). When categorized by CKD stage, only 25% (27% vs. 21%, M vs. F) patients have normal renal function.
Conclusions: Presence of hypertension in patients with cystinuria is significantly greater than that of the normal population, with a strong male preponderance. A large proportion of cystinuric patients have evidence of renal impairment. This preliminary data highlights long-term renal and cardiovascular risks in the cystinuric population, in addition to challenges of managing recurrent urolithiasis.
P1-13 Ureteric extra-anatomic stents: Long term experience and the suitability in palliative cases with a short term prognosis
CJ Johnstone, A Gkentzis, P Hughes, M Kimuli, J Cartledge, S Biyani, G Mori, M Kimuli
St James Hospital
Introduction: The purpose of this study is to review extra-anatomic stent (EAS) insertion in palliative cases with short term prognosis (<1 year) and the long term outcomes in those who survive beyond the 1st exchange date. This is to our knowledge is the largest analysis of cases to date within the UK.
Methods: Retrospective analysis via the radiology department database. Data has been analysed over a 7 year period. Respective data was collated for demographics, diagnoses and intervention factor.
Results: 70 patients have had EAS over 7 years with FU data available in 44. Mean age at EAS insertion was 61 (range 24-85 years). 32 patient’s female (73%). Commonest indication for EAS was invasion/compression from a non-ureteric malignancy in 21/44 (48%). 17/44 (39%) were idiopathic (radiotherapy/surgical complications).
35 patients (50% bilateral) were initially managed with stents, 95% of which experienced recurrent complications prior to EAS. 41/44 patients had Forrester-Patterson stents. Initial nephrostomy to 1st EAS averaged 41 days. 1st exchange date averaged 9 months (range 2-16 months). Average number of exchanges to date is 4. 16/44 (36%) patients died prior to 1st exchange (3 converted to nephrostomy). 28 survived >1st exchange with nine requiring conversion back to nephrostomy. 7/44 required re-admission during follow up secondary to infection. One patient died peri-operatively.
Conclusion: EAS is a viable long term solution for urinary diversion. Within the setting of palliative care EAS offers a short term solution to the comorbidity associated with nephrostomy/retrograde stenting.
P1-14 Effects of silicone hydrocoated double loop ureteral stent on symptoms and quality of life in patients undergoing FURS for kidney stone: A comparative randomized multicentre clinical study intermediate results
EWY Lee, OB Pullar, M Daudon, F Kleinclauss, G Guichard, J Letendre, P Holliday, I Desriac, O Traxer, OJ Wiseman
Cambridge University Teaching Hospitals NHS Trust
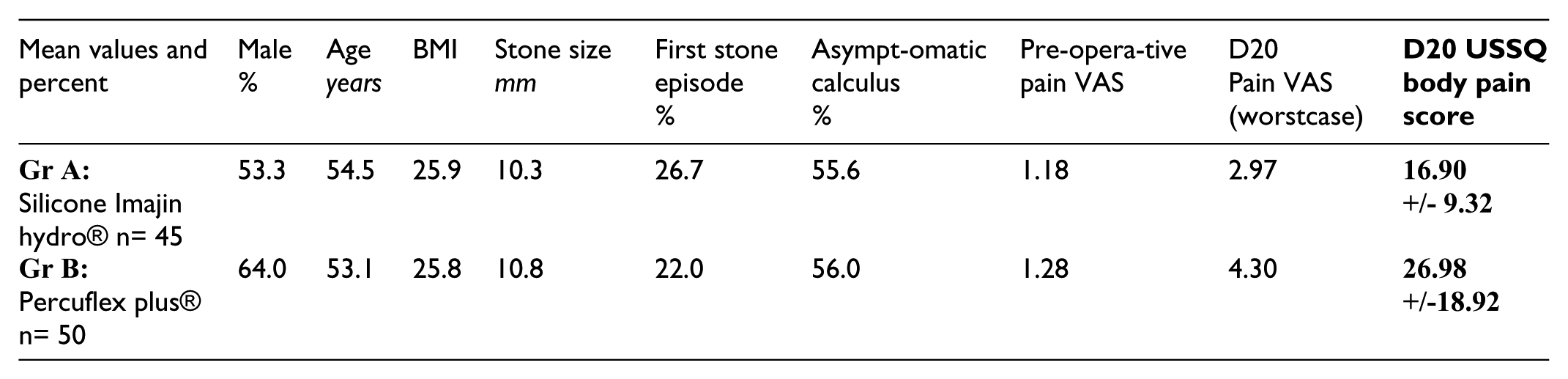
Introduction and Objectives: Double J ureteral stents are often implanted after flexible ureteroscopy (FURS), and silicone stents are made of soft material which is presumed to be associated with less patient discomfort. We compared patient comfort after FURS between a Coloplast-Porgès Imajin® hydrocoated silicone stent (group A) and a Percuflex Plus® stent, Boston Scientific Corp (group B).
Materials and Methods: 4 centres, comparative, randomized, single blind, parallel groups study over a population of 140 patients treated for unilateral renal stones (5-25 mm) by FURS. The primary endpoint was USSQ BODY pain score at D20. Secondary endpoints included pain VAS.
Results: The present results are descriptive data obtained over the first 95 randomized patients. (P1-14)
Mean values and percent
Male %
Age years
BMI
Stone size mm
First stone episode %
Asympt-omatic calculus %
Pre-opera-tive pain VAS
D20 Pain VAS (worstcase)
D20 USSQ body pain score
Gr A: Silicone Imajin hydro® n= 45
53.3
54.5
25.9
10.3
26.7
55.6
1.18
2.97
16.90 +/- 9.32
Gr B: Percuflex plus® n= 50
64.0
53.1
25.8
10.8
22.0
56.0
1.28
4.30
26.98 +/-18.92
The USSQ score at D20 appears to be lower for group A. This difference persists after correction of the USSQ Scores to take into account the relative imbalance in gender between the groups.
Conclusion: The descriptive data of the first 95 patients indicate that the silicone Imajin® hydrocoated stent is better tolerated by patients when evaluated after 3-week indwell time.
This study was supported by funding from Porges Coloplast.
P1-15 Should we save them? Analysis of the management of relatively poorly functioning (<25%) obstructed kidneys
CJ Johnstone, A Gkentzis, S Biyani, M Kimuli, J Cartledge, C Patel, S Biyani
St James Hospital
Introduction: The management of obstructed kidneys with poor relative function remains controversial. Guidance is minimal regarding split function on renogram of <25%. We reviewed the local experience in such cases and explored how interventions affected the final outcome. To our knowledge this is the largest analysis of its kind.
Patients and Methods: We identified patients with <25% split renal function in either kidney post diuretic renography (MAG-3) through the Radiology department database and reviewed their management and outcome. We subclassified the relative renal function into subgroups as follows: (0-15%, 16-20%, 21-25%). Respective data was collated for demographics, diagnoses and intervention factor.
Results: 87 patients identified. Median age: 44 years (2-90). Females: 57%. Left kidney (63%). Most presented with loin pain (46%). Majority (70%) diagnosed with pelvi-ureteric junction obstruction (PUJO) followed by ureteric strictures (21%). Complete follow-up (FU) data was available in 55 (63%). Median FU: 18 months.
In group ‘0-15%’ (7 patients), four had pyeloplasty or stent but nobody gained significant functional benefit. In group ‘16-20%’ (10 patients), five had intervention in an attempt to preserve function; in only one case this was transiently achieved with a stent (23% from 17%) but required subsequent procedures and eventually a nephrectomy. In group ‘21-25%’ (38 patients), early intervention resulted in 8% mean relative renal function improvement.
Conclusion: Our data indicates that in obstructed kidneys, 21-25% split function shows favourable outcomes following intervention. However, attempts to improve relative renal function in patients with <20% is rarely successful and perhaps an alternative approach should be considered.
Tuesday 28 June 1045-1215 Room 12 ePoster Session 2 - Bladder Cancer Management Shifting Sands Chairs: Jon Aning & John McGrath
P2-1 Evaluation of the new NICE two week wait referral guidelines for non-visible haematuria
SS Rai, AM Davies, R Morrison, P Singh, J Gill
Harrogate and District NHS Foundation Trust
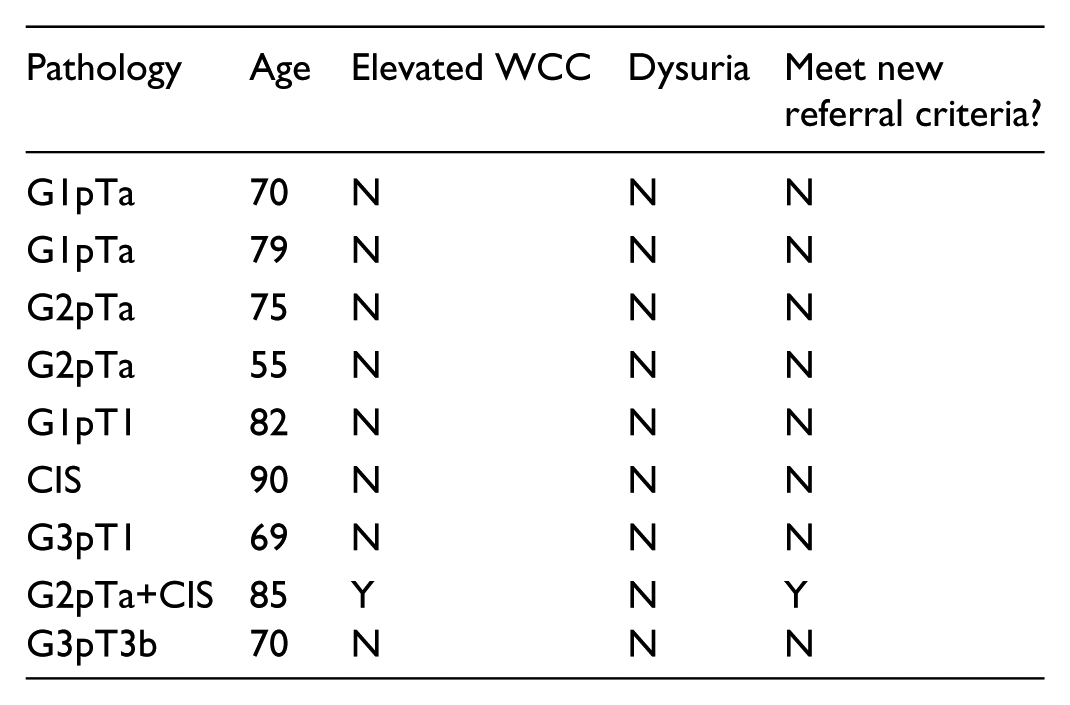
Introduction: New NICE guidelines have changed the referral criteria for urgent investigation of suspected bladder cancer; in particular for NVH: ‘aged 60 and over and have unexplained non-visible haematuriaandeither dysuria or a raised white cell count.’ We assess the potential impact on cancer detection rates at our institution.
Materials and Methods: A retrospective analysis of all two-week wait referrals for NVH between July 2014-June 2015 was undertaken. Referral criteria were evaluated against the latest guidelines.
Result: 414 patients were referred over the 12-month period. Cancer was detected in 14 (3.1%) patients; 9 bladder cancer, 2 renal cell carcinoma, 1 lymphoma, 2 prostate cancer. 8 of the 9 (88.9%) bladder cancer patients failed to meet latest NICE referral criteria (see table). (P2-1)
Pathology
Age
Elevated WCC
Dysuria
Meet new referral criteria?
G1pTa
70
N
N
N
G1pTa
79
N
N
N
G2pTa
75
N
N
N
G2pTa
55
N
N
N
G1pT1
82
N
N
N
CIS
90
N
N
N
G3pT1
69
N
N
N
G2pTa+CIS
85
Y
N
Y
G3pT3b
70
N
N
N
Conclusion: Significant bladder cancers would have been missed using the updated NICE guidelines. Excluding dysuria and elevated WCC would simplify the referral criteria and capture most cancers.
P2-2 Rejecting referrals for asymptomatic non-visible haematuria: Implications of a change in practice
AC Cox, M Kamarizan, M Hunter, JRM Wilson, DJ Painter, AC Carter
Royal Gwent Hospital
Introduction: The NICE NG12 guidance for urgent suspected cancers (USC) suggests that asymptomatic non-visible haematuria (aNVH) need not be seen as USC. Whilst implementing NG12, we also present the early outcome of rejecting referrals for aNVH entirely.
Patients and Methods: USC haematuria referrals to a large district general hospital from April to November 2015 were strictly vetted prospectively against NG12 recommendations, and compared to data from a similar time period prior to implementation. Simultaneously aNVH referrals were rejected in writing.
Results: In 8 months, 676 patients were seen in a one stop haematuria clinic (OSHC); 352 prior to implementing NG12 (cohort 1), and 324 afterwards (cohort 2). In cohort 1, 212 had visible haematuria (VH), and 140 had non-visible haematuria (NVH) with 34 cancers being diagnosed. Thirteen of these were either high risk non-muscle invasive (HRNMIBC) or muscle invasive (MIBC) bladder cancer. Of those with NVH, only 1 low risk non-muscle invasive bladder cancer (LRNMIBC) was diagnosed. In cohort 2, 39 cancers were diagnosed; 11 HRNMIBC and 4 MIBC. Seventy-six aNVH referrals were rejected. At NG12 implementation the average referral to treatment time (RTT) was 39 days, with 136 OSHC appointments being required in the previous month. After NG12 implementation RTT fell to 18 days (50% reduction), requiring only 90 appointments (34% reduction) during a similar period.
Conclusion: Prior to NICE NG12 implementation no significant tumour was found in patients referred with aNVH. After implementation, and rejecting patients with aNVH, patients with bladder cancer were seen and treated earlier and required fewer OSHC appointments.
P2-3 How safe is it to discharge low-risk non-muscle invasive bladder cancer at 12 months?
DR Thurtle, HJ Cho, EM Gordon, M Johnson, G Wilson
West Suffolk Hospital NHS Trust
Introduction: 2015 NICE guidelines advise that patients with low-risk non muscle-invasive bladder cancer (NMIBC) should be discharged from cystoscopic follow-up, if recurrence-free, at 12 months. This change has been met with some trepidation. We retrospectively applied these guidelines to assess potential change in our clinical practice.
Patients and Methods: Patients with a new histologically-proven bladder cancer diagnosis between January 2010 and December 2014 were included. Risk categories were established and subsequent cystoscopic follow-up and pathological outcomes retrospectively recorded for all low-risk cases with a minimum 1 year follow-up.
Results: Of 474 new diagnoses, 60 (12.7%) were low-risk NMIBC. 9 (14.8%) had recurrence within 12 months and 7 patients had not yet reached beyond 12 months. Of the remaining 44 patients, 7 (15.9%) had recurrent disease; 5 unifocal small G1pTa, and 2 intermediate-risk G2pTa over a mean follow-up of 35.6 months. This equates to a 7.9% recurrence-risk per-year after year one. 103 cystoscopies were performed after the initial 12-months, to yield these 7 recurrent cases.
Recurrence rates, of 14.8% and 7.9%, are similar to those used in NICE cost-analysis calculations of 15.9% for first-year and 7.4% for subsequent annual recurrence-risk respectively. Our overall progression risk of 6.6% with the G2pTa exceeds used progression probabilities, which are based on a longer 5-year follow-up.
Conclusions: Although low-risk NMIBC represents a minority of cases, updated NICE guidelines will change practice significantly. Our recurrence rates are similar to those used in cost analyses, however, a small but significant risk of developing intermediate-risk NMIBC, still needs to be considered.
P2-4 Shortages of intravesical Bacillus Calmette-Guérin (BCG): Are patients being harmed?
KR MacKenzie, L Mudd, J Cresswell
James Cook University Hospital
Introduction: Intravesical BCG treatment for high risk (HR) non-muscle-invasive bladder cancer (NMIBC) has become challenging due to unreliable BCG supplies since 2012. Treatment is recommended for up to 3 years. In response to shortages, BAUS recommends a minimum of one year of treatment. The aim was to assess compliance with this recommendation and effect on oncological outcome.
Patients and Methods: All newly diagnosed cases of HR NMIBC, treated at a UK cancer centre between August 2012 and August 2014, were analysed. Dose and number of treatments of BCG received during the first year were recorded. Compliance was defined as 6 doses at induction, followed by 3 doses at 6 and 9 months.
Result: 114 patients completed an induction course of BCG. The overall recurrence rate (RR) at 12 months was 40%, and the progression rate (PR) 13%. Those clear at first check cystoscopy were scheduled to complete 12 months treatment. 28% (32/114) did not receive planned maintenance treatment due to shortage of BCG. The RR and PR at 12 months for this group were 13% and 3% respectively. For those able to adhere to BAUS recommendation, the RR was 5%, and there was no progression.
Conclusion: A high proportion of patients have been inadequately treated due to the shortage of available BCG, with a trend towards increased recurrence and progression. The psychological harm is difficult to assess but must be considered. The use of other treatments, as per the BAUS consensus document, should be utilised to reduce harm.
P2-5 Hyperthermic intra-vesical chemotherapy (HIVEC) neoadjuvant and adjuvant treatment of intermediate or high risk non-muscle invasive bladder cancer
ASE Sousa, I Piñeiro, S Rodriguez, J Flores-Carvajal, C Uribarri
Comarcal Hospital of Monforte
Introduction & Objectives: We review the safety and efficacy of Hyperthermic Intra-VEsical Chemotherapy (HIVEC™), delivered with the COMBAT system in a group of 40 patients with intermediate or high risk NMIBC. 24 patients were treated with neoadjuvant chemo-hyperthermia prior to TURB and 16 patients adjuvant chemo-hyperthermia treatment after complete removal of tumour post TURB. This was undertaken between December 2010-April 2015 in the Monforte Comarcal Hospital (Spain).
Material & Methods: Protocol for neoadjuvant chemo-hyperthermia treatment 8 weekly instillations of mitomycin C (MMC) 80mg diluted in 50ml of distilled water, recirculated in the bladder at a 43°C(±0.5°C)60’. Post TURB adjuvant chemo-hyperthermia treatment schedule 4 weekly instillations of MMC followed by 6 monthly instillations MMC 40mg diluted in 50ml of distilled water, recirculated at 43°C(±0.5°C)60’. Tolerance data were recorded and quality of life FACT-BI and IPSS questionnaires completed.
Results: Neoadjuvant patient group: 95.8% (n=184) of the scheduled HIVEC™ treatments were accomplished. The most frequent adverse events were mild (Grade1). Patient outcome: complete response (confirmed pathology) rate 62.5% (n=15). Partial response (reduction of tumour load >50%) 33.3% (n=8). Non-responder 4.2% (n=1). The cumulative incidence of recurrence at 4 years was 20.8% (95% CI: 4.1 to 45.3%). Adjuvant patient group: 98.7% (n=158) of the scheduled HIVEC™ treatments were accomplished. The most frequent adverse events were mild (Grade1). Patient outcome: The cumulative incidence of recurrence at 2 years was 12.5% (95%CI:7.8 to 19.3%).
Conclusions: Combat-BRS has a favourable side effect profile. HIVEC™ treatment demonstrates preliminary evidence to suggest is effective against NMIBC and possible alternative to cold MMC and BCG. More randomised trials are needed.
P2-6 Survival of patients undergoing early radical cystectomy (ERC) versus cystectomy following intra-vesical BCG immunotherapy (RC) for T1G3 bladder cancer
PL Caygill, M Hadjipavlou, D Wilby
Queen Alexandra Hospital
The treatment of T1G3 bladder tumours is currently inconsistent. The aim of this study was to determine whether early radical cystectomy (ERC) has improved outcomes or offers a survival benefit compared to post BCG radical cystectomy (RC).
A retrospective analysis was performed for patients diagnosed with T1G3 bladder cancer who underwent radical cystectomy in our institution between 2003 and 2013.
A total of 359 patients underwent radical cystectomy, 58 (16%) of which were for T1G3 disease. Of the 58 patients, 28 underwent ERC while 23 received intravesical BCG treatment prior to RC. 11 (48%) patients in the BCG group had progressed to muscle invasive disease at first check cystoscopy. Mean time from diagnosis to cystectomy was 5.1 months and 13.3 months respectively (p=0.01). Mean follow-up was 44.3 months (range: 1-145 months). Ten patients (35.7%) from the early cystectomy group developed tumour recurrence at a mean interval of 41 months following cystectomy while 7 patients (30%) developed recurrence at 38 months. The 1, 3 and 5 year overall survival for the EC group was 77%, 57% and 47% respectively while for the post BCG RC group this was 81%, 55% and 55% respectively. The difference in disease recurrence timing and overall survival was not significant between the two groups (p=0.76 and p=0.58 respectively).
In our hands EC and Post BCG RC appear have similar outcomes. This study demostrates the importance of accurate initial diagnosis of T1G3 disease at presentation and that EC should be considered in high-risk patients.
P2-7 Is cardiopulmonary exercise testing in patients undergoing radical cystectomy a useful preoperative tool?
R Khan, O Elhage, C Amadi, F Ismail, C Gan, K Thomas, T O’Brien, R Thurairaja, P Dasgupta, MS Khan
Guy’s Hospital, London
Introduction: Preoperative cardiopulmonary exercise testing (CPET) has been suggested as a predictor of perioperative morbidity and mortality after radical cystectomy. This study aimed to evaluate whether CPET and serum lactate testing correlate with post-operative course.
Methods: All patients planned for radical cystectomy underwent CPET testing between 2009-15. Peri-operative parameters including complications (Clavien-Dindo) and hospital stay were recorded prospectively. Serum lactate was measured intra-operatively, immediate and 24-hour post-operatively. Logistic regression analysis was performed to assess whether CPET and lactate could independently predict post-operative complications.
Results: 148 patients (33F, 115M), mean age 68.7 years (40-90) underwent robot assisted (n=84), open (n=63) or laparoscopic (n=1) radical cystectomy. The mean anaerobic threshold (AT) was 11.4 ml/kg/min (range 6.5-24.4) and mean peak V02 16.23 ml/kg/min (range 7-36.1). 23 patients did not achieve AT. There was no correlation between low AT and risk of post-operative complications up to 30-days. This subgroup however, had a significantly longer LOS compared to those with AT ⩾11 mL/kg/min (14 Vs 11), P = 0.04. Multivariate binary logistic regression analysis demonstrated that 24-hour post-operative serum lactate concentration was the only significant predictor of post-operative major complications, Clavien ⩾3 (OR 4.8, 95% CI 1.71-13.48; P = 0.003).
Conclusion: This study shows that CPET does not predict the risk of post-operative complications or short-term surgical outcomes up to 30 days post-operation. This test besides being labour intensive is expensive, hence may only be used in selective patients undergoing cystectomy. On the contrary, lactate at 24h post-operative is a better predictor of post-operative complications.
P2-8 Can pre-operative gait velocity (GV) replace cardiopulmonary exercise testing (CPET) as an independent predictor of survival and complications following radical cystectomy (RC)?
C Down, R Nair, T Fynmore, K Omar, S Itam, MS Khan, R Thurairaja
Guy’s and St. Thomas’ NHS Foundation Trust
Introduction: CPET is increasingly employed to risk-stratify patients prior to RC. It remains however a costly, labour intensive and poorly tolerated test in some. We evaluate pre-operative GV as an alternative to CPET and establish criteria predictive of survival and complications following RC.
Patients: A prospective single-centre review of 97 (80 male, 20 female, mean age 67 years, range: 56-83) patients undergoing RC between March-2014 and December-2015 was performed. Pre-operative GV was correlated with outcome parameters of CPET-anaerobic threshold (AT), 90-day mortality and Clavian-Dindo complications (CDC).
Results: The mean Charlson co-morbidity index scores for patients undergoing RC was 4.8. 81 and 19 patients underwent robotic and open procedures respectively. The median pre-operative GV was 1.07m/s (0.28-2.77) versus 0.52 m/s (0.01-1.27) on discharge. The median AT was 11.9 ml/min/kg (0–24). All patients performed a GV assessment, however, 20% of these could not complete CPET.
There is a direct relationship between pre-operative GV and AT (p<0.001). Pre-operative GV of <1m/s, 1-2m/s and >2m/s, corresponded to a median AT of 9.7, 12.1 and 13.9ml/min/kg respectively. There is an association between AT and median length of stay of 10.5-days (6–98, p<0.01). A GV <1m/s was associated with a higher morbidity (CDC 2-5, 62% versus 51%) and increased 90-day mortality (3% versus 1%) compared to GV >1m/s.
Conclusions: Patients with a pre-operative GV of <1m/s experience poorer clinical outcomes following RC. Since there is direct correlation between GV and outcome parameters from CPET, GV assessment is a simpler alternative saving on cost, resource and time.
P2-9 ‘Prehabilitation’ of patients undergoing radical cystectomy to assist recovery: results of a feasibility study
S Banerjee, K Manley, B Shaw, J Saxton, M Rochester, R Mills
Norfolk and Norwich University Hospial
Introduction: The role of exercise training or ‘prehabilitation’ for optimising preoperative physiological function has received little attention in patients undergoing radical cystectomy (RC). This randomised controlled feasibility study examines whether a short preoperative course of supervised exercise sessions is tolerated and whether it can lead to an improvement in cardiopulmonary fitness in patients undergoing RC.
Method: Over a 2-year period patients awaiting RC were randomised to either control or intervention arm. Patients in the intervention arm were offered twice weekly supervised exercise sessions preoperatively for 4 weeks, whilst the control arm had standard care. Both groups had CPET at the beginning and end.
Results: 60 patients were recruited into the study, with a recruitment rate of 53.5%. Mean age was 72 years (range 52-85). No adverse events were recorded during CPET testing or exercise sessions. Compliance to exercise sessions was satisfactory with patients attending for a median of 8 sessions. A multivariate analysis (ANOVA) showed a statistically significant increase in mean VO2 max in the intervention group when compared to the control group by +1.9ml/kg/min (0.87-3, 95%CI), p=0.001). Anaerobic Threshold was also similarly increased by +0.33ml/kg/min (-0.68-1.3, 95%CI) (p=0.5).
Mean preoperative VO2 max was found to be significantly higher (p<0.001) in patients who had an uncomplicated recovery (22.04ml/ks/min) when compared to those with complications (Clavien grade I or above) (16.32ml/kg/min).
Conclusion: CPET assessment and exercise training is safe and well tolerated. Patients comply with a supervised exercise regime and there is a measurable improvement in their cardiorespiratory fitness after 4 weeks.
P2-10 Patients with low cardiorespiratory fitness benefit from robotic cystectomy with intracorporeal diversion for: a prospective cohort study
BW Lamb, WS Tan, A Sridhar, I Ahmad, P Eneje, S Nathan, J Hines, TP Briggs, R Stephens, JD Kelly
University College London Hospital
Background: Patients undergoing radical cystectomy have comorbidities resulting in reduced cardiorespiratory fitness. Preoperative cardiopulmonary exercise testing (CPET) measures can predict major adverse events (MAE) and length of stay (LOS) for patients undergoing open and robotic cystectomy with extracorporeal diversion. We aimed to determine the relationship between CPET and outcome in patients undergoing robotic radical cystectomy and intracorporeal diversion (iRARC).
Methods: A single institution prospective cohort study in patients undergoing iRARC for muscle invasive and high grade bladder cancer. Inclusion: patients undergoing standardised CPET prior to iRARC. Exclusions: patients not consenting to data collection. Data on CPET measures (AT, ventilatory equivalent for carbon dioxide (VE/VCO2) at AT, peak oxygen uptake (VO2)), and demographics prospectively collected. Outcome Measurements included LOS; 30-day MAE and 90-day mortality were prospectively recorded. Descriptive and regression analyses were used to assess whether CPET measures were associated with or predicted outcomes.
Results: From March 2011 to March 2015 135 patients underwent radical cystectomy (ORC n=25, iRARC n=111). 82 patients who underwent iRARC and CPET and consented to participation were included. Median (IQR): Age=65 (58−73); BMI=27 (23−30); AT=10.0 (9−11), Peak VO2=15.0 (13−18.5), VE/VC02 (AT)=33.0 (30−38). 30-day MAE=14/111 (12.6%): Death=2, Multi organ failure=2, abscess=2, Gastrointestinal=2, Renal=6; 90-day mortality=3/111 (2.7%). AT, Peak VO2, VE/VC02 (at AT) were not significant predictors of 30-day MAE or LOS. The results are limited by the absence of control group undergoing open surgery.
Conclusions: Poor cardiorespiratory fitness does not predict increased LOS or MAEs in patients undergoing iRARC. Overall, MAE and LOS comparable with other series.
P2-11 Complications following robotic assisted radical cystectomy (RARC) with intracorporeal urinary diversion: An analysis of 90 day outcomes stratified according to type of urinary diversion
WS Tan, BW Lamb, MY Tan, I Ahmad, A Sridhar, S Nathan, J Hines, G Shaw, TP Briggs, JD Kelly
University College London
Introduction: Intracorporeal robotic assisted radical cystectomy (iRARC) is the standard of care for muscle invasive bladder cancer at our center. We evaluate early postoperative morbidity and mortality for patients undergoing iRARC stratified according to urinary diversion type using a standardised reporting criteria.
Patient & Methods: 134 patients underwent iRARC with extended pelvic lymph node dissection between June 2011 and July 2015. Patient demographics, pathological data and perioperative mortality were recorded. 90 day complication data were reporting according to Clavien-Dindo (CD) classification and stratified according to urinary diversion type.
Results: Patients receiving continent diversion were significantly younger, more likely to have an ASA⩽2, a higher anaerobic threshold, peak oxygen consumption and minute ventilation-carbon dioxide production and less likely to have advanced disease or lymph node positive disease. 90 day complication rate for ileal conduit and continent diversion patients were 68% and 82.4% while CD⩾3 complications were 21.0% and 20.6% respectively.90 day mortality was 3% and 2.9% respectively. Five cases required an open conversion. Urinary leak was significantly more common in the continent diversion group (p=0.001) although 75% of cases were managed conservatively. The requirement for blood transfusion (p=0.024) and male patients (p=0.016) were independent predictors for major complications at 90 days. Cardiopulmonary exercise tolerance test parameters and ASA score were not associated with 90 day CD⩾3 complications.
Conclusion: Complications following iRARC are common but most complications are low grade. It is feasible to perform most RARC cases intracorporeally and iRARC may reduce the risk of complications especially in comorbid patients.
P2-12 The role of lymphadenectomy in radical cystectomy
KAS Sharif, OE El-Hage, FI Ismail, CG Gan, KA Ahmed, RT Thurairaja, PD Dasgupta, SK Khan
King’s College London
Introduction: Pelvic lymph node dissection (PLND) is a standard component of radical cystectomy (RC). There is evidence suggesting a survival advantage with extended lymphadenectomy with complication rates of both extended and standard techniques reported to be similar. In this study we aim to compare extended lymph node dissection (eLND) with standard lymph node dissection (sLND).
Materials & Methods: Between 2009 and 2015, prospectively collected data on 296 patients undergoing RC with either sLND (n=160) or eLND (n=136) was evaluated. sLND included removal of the lymph nodes up to the common iliac bifurcation, whereas eLND included removal up to the aortic birfucation.
Results: The mean nodal count was 19 in eLND and 15 in sLND (p<0.001). Operative time was 400 vs 331 minutes (p<0.001). There were a total of 131 complications (52.9% vs 36.9%, p>0.05), of which 84.7% and 78% (p>0.05) were Clavien 2 and above, in the eLND and sLND groups respectively. Specifically, complication rates of ileus and pelvic collection combined were significantly greater in eLND group (31% vs 19.3%, p=0.022). There was no difference in length of stay, blood loss and transfusion rates. Overall and cancer-specific survival after five years were greater in the eLND group (86% vs 69.4%) and (89.7% vs 73.8%), as well as recurrence-free survival (82.4% vs 66.3%).
Conclusions: Extended lymphadenectomy is associated with better survival rates, however this is at the expense of higher complications. The extent of lymph node dissection should be considered carefully, especially in patients with increased comorbidities.
P2-13 Open radical cystectomy in the UK – the current standard of care? Analysis of the BAUS cystectomy audit
ER Jefferies, J Cresswell, JS McGrath, C Miller, L Hounsome, S Fowler, EW Rowe
Cheltenham General Hospital
Introduction: The enhanced data entry into the BAUS database since becoming mandatory for 2014-15 has enabled greater assessment of surgical outcomes following radical cystectomy. The aim of this paper is to establish comprehensive UK standard outcomes (using the available metrics) for open radical cystectomy over a two-year period.
Materials and Methods: All open radical cystectomies performed in the last two years and recorded in the BAUS database were analysed.
Results: Data entry into the BAUS cystectomy audit has increased from 37% to ~80% following its mandate and we would expect this to increase following the March 2016 deadline for 14/15 data, ready for June presentation. Early analysis of 1751 open radical cystectomies shows 73.3% were performed on men with a median age of 69. The median number performed per consultant was 11 (range 1-75) and 19 per centre (range 1-92). 58.1% was for preoperatively staged T2+ disease. Neobladder diversion rate was 6.3%. Lymph node dissection was performed to level 1,2,3 in 20.5%, 49.8% and 11% respectively. The transfusion rate was 30.4%. The intraoperative rectal injury rate was 1.1%. We expect complications will be under-reported due to the nature of the audit but are reported as 10.5% (Clavien Dindo 3-5). The positive margin rate was 10%. The median length of stay was 12 days. The reported 30 & 90-day mortality were 0.8% and 1.6% respectively.
Conclusions: We now have a UK benchmark of care to compare any future techniques or modifications (such as enhanced recovery or minimally invasive techniques).
P2-14 The BAUS radical cystectomy audit –an update on current practice (2014), and an analysis of differences in practice between centres and surgeons performing differing volumes of surgery
C Miller, J Cresswell, E Rowe, E Jefferies, L Hounsome, S Fowler, JS McGrath
BAUS Section of Oncology
Introduction: The BAUS Data and Audit platform allows surgeons to upload their surgical activity to a national registry. NICE IOG guidance recommended centralisation of major urological cancer surgery alongside minimum criteria for volumes of cases performed with the aim of improving outcomes. Mean cases per surgeon and per centre have increased in recent years but there are significant differences in volume between surgeons/centres. The current analysis describes an overview of the data on radical cystectomy (RC) practice during 2014, including differences in RC practice between low, medium and high volume practices.
Methods: Individual surgeons / units uploaded their data on RC to the BAUS Registry. Once extracted, data were transferred to an Access™ database for validation prior to analysis using Tableau™ software. Surgeons were given two opportunities to validate their data. Centres were defined as low (<15), medium (15-30) and high (>30) volume according to annual caseload. Surgeons were similarly grouped into low (<5), medium (5-15) and high (>15) volume. Adequacy of lymph node dissection was used as surrogacy for surgical quality.
Results: Details on 1,601 RC were uploaded from 135 consultants at 64 sites, representing 78% of cases undertaken in England (compared with 60% in 2013). Median number of cases per surgeon was 9 (1-86) with a median of 19.5 cases per centre (a 50% increase compared to data reported in 2013). Over 70% of patients still underwent open RC with 14.5% having robotically-assisted RC. Less than half of RC (46%) were performed for muscle-invasive BC. Orthotopic bladder substitution was only performed in 6% of cases. Length of stay (LOS) varied widely by surgical approach – Open(12d), lap(8d) and robotically-assisted(8d). Transfusion rates were lower with lap/robotic (10.4/11.1%) than open (28.5%). 30-day mortality was <1% in all approaches. 1 in 4 RCs were performed as joint consultant cases. (P2-14)
Surgeon
Centre
Volume
>11nodes
Robotic
Volume
>11 nodes
Robotic
LOW
5.3%
35%
2.6%
14.8%
61%
4.7%
MEDIUM
35.6%
62%
28.4%
25.2%
51%
20.7%
HIGH
59.1%
70%
69%
60%
70%
74.6%
Conclusions: Compliance with national registration of data on RC is improving. Median case volume per surgeon and per centre at a national level is improving and compares favourably with European and US practice. Minimally invasive surgical rates are improving with advantages seen in LOS and transfusion rates. However, rates of bladder reconstruction are low.
A majority of surgery was performed by high volume surgeons in high volume centres. Lymph node dissection was more likely to be adequate when performed by high volume surgeons, though effect of centre volume was less marked. Robotically-assisted surgery is predominantly delivered in high volume centres.
P2-15 Oncological and non-oncological outcomes following open cystectomy with Enhanced Recovery After Surgery (ERAS): results from a 10-year contemporary high-volume, prospectively maintained UK series
HM Simpson, K Mistry, SK Stewart, LA McAughtrie, LB Loureiro, ALJ Carroll, S Middleton, JJC Morton, P Mariappan
Edinburgh Urological Cancer Group, Western General Hospital
Introduction: Outcomes following cystectomy for bladder cancer are expected to improve with surgeon experience and implementation of quality control and ERAS protocols. However, there is sparse data from high-volume surgeons’ prospective open cystectomy experience which could be valuable in comparing with minimally invasive techniques. We evaluated the early and long term complications as well as survival in a prospectively maintained cohort of patients undergoing cystectomy in one surgeon’s high volume practice.
Patients and Methods: All patients undergoing cystectomy from one surgeon’s series between 2006 and 2015 had detailed proformas completed prospectively, documenting peri-operative and follow up variables. ERAS was introduced in May 2007. Follow up included timed, protocol-driven, cross–sectional and upper-tract imaging. Kaplan-Meier graphs and log-rank tests assessed overall and stage stratified cancer specific survival.
Results: In all, 451 operations were performed. Analysis of the urothelial cancer patients in the first 5 years of the series revealed the incidence of Clavien-Dindo 3 or more complications was 6.2%, with none experiencing rectal injury or bowel anastomotic leaks. ERAS resulted in a significantly earlier return of bowel function and reduced infection rates. The 30-day mortality was 0.4%. The 5-year overall and cancer specific survival were 55.2% and 65.7%, respectively and was noted to be improved in those who received neo-adjuvant chemotherapy. At 5 years, 3.0% patients with ileal conduits developed uretero-ileal anastomotic stricture.
Conclusions: This contemporary UK series of open cystectomies reveals that low mortality with acceptable morbidity and cancer specific survival can be achieved with high surgical throughput and ERAS.
Tuesday 28 June 1400-1530 Room 4 ePoster Session 3 – Prostate Cancer Diagnosis: An Evolving Journey Chairs: Miles Walkden and Prasanna Sooriakumaran
P3-1 Has perception of abnormal PSA values amongst GPs changed over the last 10 years?
EM Gordon, D Thurtle, R Brierly, J McLoughlin
Ipswich General Hospital
Introduction: In 2006 a survey of family practitioners across Suffolk showed a reluctance to refer younger men with abnormal PSA levels. Increasing evidence supports curative therapy for prostate cancer (PCa) in men aged under-55 and early-detection remains a government priority. This survey was repeated in 2015 to assess change in perception of abnormal PSA-values.
Patients and Methods: 500 self-administered paper questionnaires were distributed. 142 GPs responded (28.4%), representing a patient population of approximately 600,000. A series of visual analogue questions assessed referral thresholds and understanding of high-risk PCa groups.
Results: GPs with a median of 23-years experience responded. The perceived number of new PCa diagnoses, per GP per year, increased significantly from 2, in 2006, to 8 this year. The median (range) thresholds that GPs reported for referral at ages 45, 55, 65 and 75 were 4.5ng/mL (2.5-10.5), 5.5ng/mL (2.5-10.5), 5.5ng/mL (3.5-10.5) and 6.5ng/mL (4.5-25.5) respectively. These values are unchanged from data a decade earlier and, especially for younger men, are considerably higher than recognised maximum PSA-levels. 95.1% recognised a family history of PCa to be a potential risk factor. Using case-based scenarios, practitioners were more likely to refer older men with abnormal PSA values compared to 2006; however, only 56.2% of GPs would refer an asymptomatic 55-year-old with PSA of 4.6ng/mL.
Conclusions: Awareness of abnormal PSA values in primary care, particularly in younger patients, is lagging behind the evidence, with no change in referral thresholds over the last decade. Strategies to disseminate knowledge of maximum PSA-values to GPs should focus on those for younger patients.
P3-2 Comparison of age specific PSA cutoffs in a UK cohort with prostate cancer: Are BAUS Guidelines the best?
LJ Tay, LJE Spurling, JEW Hines, JSA Green
Whipps Cross University Hospital
Introduction: NICE recommend age-specific PSA values developed from the National Prostate Cancer Risk
Management Program. BAUS has also introduced alternative ranges, with higher cut-off values. We aimed to identify the most appropriate age-specific PSA ranges to include younger men with prostate cancer while reducing investigation in older men. We compared the age-specific ranges from Oesterling, BAUS, London Cancer Alliance’s (LCA) and the Gwent Prostate Cancer Screening Study values.
Methods: Based on a prospective database since 1990, we analysed consecutive patients diagnosed with prostate cancer within six years. We included all patients above 80 years and below 50 years to increase numbers in these groups. We compared the sensitivity of Oesterling, BAUS, LCA and Gwent criteria.
Clinically significant cancers were defined as Gleason ⩾7. Statistical analysis was performed using R.
Results: 1330 patients were included. The percentage for each group 40-49, 50-59, 60-69, 70-79, 80-84 and >85 were 3.5%,11.4%, 27.7%, 30.5%, 18.3%, 8.4% respectively. 71.2% had Gleason ⩾7. Across all groups, Oesterling and LCA are the most sensitive in detecting Gleason ⩾7; 92.6% (CI 90.5-94.3) and 90.4% (CI 88.5-92.2) respectively. In the 60-69 group, Oesterling and LCA have the highest sensitivity. However sensitivity is comparable between all criteria in the 50-59 and 70-79 group. In the over 80s, the sensitivity for BAUS was 87.4 (CI 84.4-90.8). No meaningful conclusion could be drawn from the under-50s.
Conclusion: The difference in performance between each criteria is minimal. There doesn’t appear to be a clinically significance difference by using the BAUS criteria, and seems safe to do so in our population.
P3-3 Improving multivariable prostate cancer risk assessment
R.W. Foley, RM Maweni, K Murphy, G Durkan, R Power, F O’Brien, K O’Malley, D Galvin, TB Murphy, RW Watson
University College Dublin
Introduction: In order to diagnose prostate cancer (PCa) effectively, the best possible risk factors should be utilised. We analysed the performance of the PCPT risk calculator and two iterations of the ERSPC risk calculator, one of which incorporates prostate volume and another, which also incorporates the Prostate Health Index (ERSPC-PHI).
Patients & Methods: The risk of PCa and significant PCa (Gleason ⩾7) in 2,001 patients from 6 tertiary referral centres was calculated according to the PCPT and ERSPC formulae. Predictions were analysed using ROC analysis, calibration analysis and decision curve analysis. In a subset of 222 patients, risk predictions were calculated as per the ERSPC and ERSPC-PHI.
Results: The ERSPC outperformed the PCPT in the prediction of PCa and significant PCa on ROC analysis (p<0.001). The performance of the ERSPC was further improved through the addition of the PHI score. The AUC of the ERSPC-PHI was 0.76 and 0.78 for PCa and significant PCa prediction respectively, in comparison to AUC values of 0.72 for the ERSPC (p=0.12 and p=0.04). The ERSPC-PHI demonstrated good calibration in this cohort and superior net benefit over that of the ERSPC.
Conclusion: The performance of the ERSPC demonstrates that prostate volume has the potential to improve PCa diagnosis. The incorporation of the PHI score allowed each patient’s risk to be more accurately quantified. Individual patient risk calculation using the ERSPC-PHI can be undertaken in order to allow for a systematic approach to patient risk stratification and to aid in the diagnosis of PCa.
P3-4 Transperineal targeted biopsy - results from a local anaesthetic service
EJ Bass, IA Donaldson, A Freeman, C Jameson, N Ramachandran, S Punwani, M Emberton, M Arya, HU Ahmed
University College London Hospital
Introduction: The random nature of TRUS biopsy and its associated risks of sepsis and disease misclassification are well described.
An alternative approach is the transperineal template biopsy. This reduces miss-classification but is associated with higher patient burden.
Evidence suggests that targeted transperineal prostate biopsies visually directed to an MRI have high rates of detection for clinically significant disease.
We set up a local anaesthetic (LA), transperineal targeted prostate biopsy service to evaluate service delivery and cancer detection.
Patients & Methods: Men with mpMRI visible targets and clinical indication for prostate biopsy underwent LA visually-guided transperineal biopsies. Pathology and mpMRI data were collected for each patient.
Results: Between September 2013 and October 2014 125 men underwent LA targeted biopsy. Biopsies were either primary, post treatment or post failed TRUS biopsy.
Median PSA was 9.29ng/ml. All mpMRI scans had a visible target. 35 scored PIRADS 3/5 for radiological likelihood of disease, 50 4/5 and 49 5/5. Median target size was 0.80ml.
Mean number of cores taken was 6. Cancer was detected in 91/130 men (70.0%), 75/130 (57.6%) with Gleason 3+4 or higher.
5/35 scans (14.3%) scoring PIRADS-3 were found to have significant cancer and those scoring 4 or 5, 31/50 (60.7%) and 43/49 (87.7%) respectively.
Conclusion: Local anaesthetic, targeted transperineal biopsy is a feasible diagnostic procedure with high rates of detection for clinically significant cancer.
The incorporation of MRI allows the selection of men who have a clearly visible lesion to undergo a less invasive test to establish the presence of disease.
P3-5 Early experience and Patient Reported Outcomes using a novel device (CAMPROBE) to undertake local anaesthetic out-patient transperineal prostate biopsies
VJ Gnanapragasam, S Stearn, L Starling, C Kastner, A Doble, T Stone
Academic Urology Group, University of Cambridge
Introduction: Transperineal biopsies (TP-Bx) are a potentially safer alternative to transrectal biopsies (TRUS-Bx) in acquiring prostate tissue. It is however challenging under local anaethesia (LA) as multiple perineal punctures are needed. Here we report a novel device to facilitate TP-Bx as a LA out-patient procedure.
Methods: Men undergoing re-biopsy as part of surveillance were recruited. The CAMPROBE (pat:1412726.0) is placed under ultrasound guidance and synchronous LA infiltration at 2 points either side of the midline with the patient in lithotomy (ciprofloxacin cover). Sectoral biopsies were taken through the CAMPROBE. Patient reported outcomes (PROM) (post-biopsy and at 1 week) were assessed using the PROBE study questionnaire.
Results: To date 20 men have undergone a CAMPROBE biopsy (procedure time 15-30 minutes). There were no immediate complications and all men were discharged within an hour. All 20 scored the procedure as minor/ moderate under LA with a median pain score of 1.5 (range 1-5). In comparison to TRUS-Bx (PROBE study), PROM outcomes at 1 week were; Fever 0% vs 12%, Shivers 0% vs 12%, Haematuria 68% vs 64%, Haematochezia 10% vs 33%, biopsy related GP visits 0% vs 10.4%. There were no retention episodes and no readmissions. 17/19 (89%) men rated the CAMPROBE experience equivalent (n=3) or superior (n=14) to a TRUS-Bx. 14/19 (74%) men would prefer a CAMPROBE over TRUS-Bx for a next biopsy with another 4 willing to have either.
Conclusions: The CAMPROBE LA TP-Bx procedure appears well tolerated with improved PROMs compared to TRUS-Bx and an apparent reduced infective risk.
P3-6 An audit to assess the role of pre-biopsy rectal swab culture and targeted antibiotic prophylaxis on the incidence of urosepsis post transrectal ultrasoundguided (TRUS-guided) biopsy of the prostate
P Rouse, S Saad, M Abdulnabi, A Deb, I Bourghi, P Verma, S Rai, S Kommu, J Urry, I Rudd
Eastbourne District General Hospital
Introduction: Urosepsis post TRUS-guided biopsy of the prostate is a common and potential fatal complication. It is preventable with antibiotic prophylaxis: Ciprofloxacin and Gentamicin are commonly used. However, antibiotic resistance is increasing. At our institution, we have implimented a policy of pre-biopsy rectal swab culture and targeted antibiotic prophylaxis to reduce the incidence of urosepsis post procedure. We performed an audit to assess the impact of this policy.
Patients and Methods: A restrospective review of the electronic medical notes of patients from May 2015 to August 2015 was performed to determine our incidence of urosepsis post-TRUS guided biopsy of the prostate. A policy of prebiopsy rectal swab culture for all patients booked for prostate biopsy was implemented. A re-audit was performed between September 2015 and Dec 2015.
Results: Ninty-nine patients had TRUS-guided biopsy of the prostate between May 2015 and August 2015. Seven (7.1%) patients were admitted to hospital with urosepsis post procedure (two patients had severe sepsis). This policy was implemented and a re-audit was performed. 139 patients had TRUS-guided prostate biopsy between Sep 2015 and December 2015. 112 patients (80.6%) had pre-biopsy rectal swabs done. Eight patients had positive pre-biopsy rectal swabs cultures which grew extended spectrum beta-lactamase organisms and targeted antibiotic prophylaxis was given. 6/8 organisms (75%) were resistant to Ciprofloxacin and/or Gentamicin. Only two patients (1.4%) were admitted to hospital with urosepsis post procedure.
Conclusion: Pre-biopsy rectal swab culture and targeted antibiotic prophylaxis post TRUS-guided biopsy of the prostate is recommended. A cost-effectiveness analysis is needed.
P3-7 Is a routine bone scan staging really necessary for staging in intermediate risk (PSA 10-20), Gleason score 7 prostate cancer?
SJ Srirangam, GD Wemyss-Holden
Royal Blackburn Hospital
Introduction: Bone scan (BS) is an important tool in prostate cancer (CaP) staging, and is mandatory in high-grade disease (Gleason score >7) and high PSA (>20ng/ml). The NICE guidelines categorise patients with Gleason score 7 CaP and PSA of between 10 and 20ng/ml as intermediate risk, and though optional in this group, most centres undertake routine BS staging. We evaluated the incidence of positive BS in this intermediate risk group.
Patients & Methods: All patients diagnosed with histologically-proven Gleason 7 CaP (both 3+4 and 4+3) over a 5-year period (2010-2015) were included.
Results: Of 514 patients with Gleason score 7 disease, 140 (27.2%) had a PSA of 10-20ng/ml. Of these, 136 underwent initial BS staging. The BS was positive in only two cases – one with metastatic CaP and another with skeletal metastases secondary to lymphoma. Therefore a positive BS due to metastatic CaP was encountered in only one out of 136 (0.7%) patients. This patient had a PSA of 19.ng/ml, Gleason 3+4 CaP and complained of recent-onset bone pain. This patient also had an elevated alkaline phosphatase (ALP) and demonstrable locally advanced disease on MR scanning, potentially alerting to the possibility of bone metastases.
Conclusion: Our single-centre data shows that demonstrable bony metastasis is uncommon in the NICE intermediate risk group (Gleason score 7 and PSA 10-20ng/ml). In this group, restricting BS imaging to patients with bone pain, elevated ALP levels and radiologically-proven locally advanced disease will avoid unnecessary scans, potentially reduce overall costs and minimise false negative cases.
P3-8 Prostate Imaging Compared to Transperineal Ultrasound-guided biopsy for significant prostate cancer Risk Evaluation (PICTURE): a prospective cohort validating study assessing multi-parametric MRI
LA Simmons, A Kanthabalan, J Gelister, T Briggs, A Freeman, SC Charman, C Jameson, CM Moore, M Emberton, HU Ahmed, J Neves
University College London
Introduction: Risk stratification with TRUS biopsy for prostate cancer can be inaccurate. As a result, men with negative biopsies or those with low risk prostate cancers often require a second biopsy prior to treatment decision. Multi-parametric Magnetic Resonance Imaging (mpMRI) of the prostate might allow men to avoid further biopsies. PICTURE was a prospective, paired cohort validating trial, assessing the diagnostic accuracy of mpMRI in men who required a further biopsy.
Patients and Methods: Men who had undergone prior TRUS biopsy but where diagnostic uncertainty remained were eligible. Participants underwent mpMRI and transperineal template prostate mapping (TTPM) biopsy. The ability of mpMRI to rule-out clinically significant prostate cancer (Gleason >/=4+3 AND/OR a Maximum Cancer Core Length (MCCL) ⩾6mm ) as demonstrated by the NPV and sensitivity was assessed.
Result: Between 11th January 2012 and 29th January 2014, 330 men were enrolled of which 249 underwent both index and reference tests. Mean (SD) age was 62 (7) years, median (IQR) PSA 6.8 (4.98-9.50) ng/ml, median (IQR) number of previous biopsies 1 (1-2) and mean (SD) gland size 37 (15.5) ml. 146 men (59%) were free from clinically significant cancer. In ruling-out clinically significant prostate, mpMRI of the prostate had a NPV of 91.4% (95% CI 76.9-98.1) and sensitivity of 97.1% (95% CI 92-99). Specificity was 21.9% (95% CI 15.5-29.5) and PPV 46.7% (95% CI 35.2-47.8).
Conclusion: PICTURE trial results suggest that mpMRI of the prostate could reduce unnecessary repeat biopsies without compromising the detection of clinically significant prostate cancer.
P3-9 MRI based surgical planning is accurate at excluding extra-capsular disease extension prior to robotic prostatectomy: a prospective cohort study of 683 cases
AN Sridhar, BW Lamb, N Ramachandran, M Dawari, K Zaccai, I Ahmad, G Shaw, TP Briggs, S Nathan, JD Kelly
University College London NHS Trust
Introduction and Objectives: Accurate identification of extra-capsular extension (ECE) in men undergoing RARP can improve rates of nerve sparing (NS) without an increase in positive surgical margin (PSM) rates. The objective of this study was to assess the accuracy of MRI to identify ECE.
Methods: All cases undergoing RARP at a single institution between 07/13 and 11/15 were reviewed at a pre-operative surgical planning meeting involving urologists and radiologists. MRI was used to annotate tumour location and ECE. A surgical planning decision to proceed to unilateral (UNS), bilateral (BNS) or non-nerve spare (NNS) based on MRI, biopsy, DRE findings and pre-operative IIEF was recorded. MRI reported stage was compared to the post-op pathological stage. Descriptive and multi receiver-operator-characteristic (ROC) analyses were performed using R.
Results: 687 consecutive patients underwent RALP; complete data was missing in 4 cases. Postoperative histology showed T2in 311/683 (45.6%); T3 in 372/683 (54.4%). The PPV and NPV of MRI to identify ECE was 0.57 (0.12-0.78) and 0.93 (0.89-0.99) respectively (sensitivity 0.616 (0.18-0.83) and specificity (0.84 (0.79-0.96)). Using a multi ROC analysis the area under the curve was highest for postero- lateral ECE and lowest for the apical ECE (0.92 vs 0.24). NS rates were UNS (41.6%), BNS (15.5%) and NNS in 43%.
Conclusions: MRI can exclude ECE with a high degree of certainty but cannot reliably identify ECE. It is of greatest value when assessing posterolateral margins. There remains a need to develop tools to reliably identify ECE.
P3-10 Transperineal MRI visually-targeted prostate biopsies compared to template mapping biopsy in 534 men requiring further risk stratification
ADR Grey, TR Hartington, V Kasivisvanathan, M Arya, M Emberton, A Freeman, CM Moore, S Punwani, N Ramachandran, HU Ahmed
UCL Division of Surgery and Interventionl Science
Introduction: Transperineal template prostate mapping (TTPM) biopsies are highly accurate and benefit from a low infection rate. However, over-detection of clinically insignificant disease and resource use are problematic. Targeted transperineal biopsy may overcome these problems.
Methods: 535 men underwent MRI-targeted and TTPM-biopsies at the same sitting at a single centre (2007-2015). All had multi-parametric MRI (T2W/Diffusion/Dynamic-contrast) with lesions scored 1-5. Primary outcome was detection of clinically significant disease (primary Gleason pattern 4 and/or maximum cancer core length >6mm) and detection of clinically insignificant cancer.
Results: Mean age was 65 years (SD+/-22), mean PSA 9.6 (SD+/-15), mean number of cores at MRI-targeted biopsy 3.7 (SD+/-1.93) and TTPM-biopsy 42.7 (SD+/-16.8). Cancer was detected in 355 (66%) using MRI-targeted biopsy and 461 (86%) using TTPM-biopsies. Clinically significant prostate cancer was detected in 212 (40%) and 250 (47%), respectively. MRI-targeted biopsy detected 51 (9.5%) clinically significant prostate cancers missed by TTPM-biopsy; TTPM-biopsy detected 89 (17%) cases missed by MRI-targeting.
TTPM-biopsies detected 85 (16%) cases of clinically insignificant prostate cancer that were not detected by MRI-targeting. (P3-10)
MRI-targeted biopsies
TOTALS
All significance is UCL definition 1
Clinically significant prostate cancer
Clinically insignificant prostate cancer
No cancer
Mapping Biopsies
Clinically significant prostate cancer
161
61
28
250
Clinically insignificant prostate cancer
47
79
85
211
No cancer
4
3
66
73
TOTALS
212
143
179
534
Conclusion: A transperineal MRI-targeted biopsy strategy has a high detection rate for clinically significant disease and requires fewer biopsies. It also reduces the detection of clinically insignificant prostate cancer.
P3-11 Understaging of prostate cancer on multi-parametric MRI – single institution prospective experience
AA Deshpande, A Mevcha, N Hedley, V Sherwood, D MacDonald, K Jefferson
University Hospital Coventry & Warwickshire
Introduction: NICE guidelines suggest that multi-parametric MRI scan (mpMRI) should be performed if initial TRUS-guided prostate biopsies are negative. No further biopsy is required if mpMRI is negative. We evaluated results of transperineal template biopsies (TTb) to assess diagnostic accuracy of mpMRIin prostate cancer (PCa).
Patients & Methods: We prospectively collected data on all TTb at our institution from December 2014 to October 2015. TTb was performed using 5mm-intervals with apical and basal cores as required. 1.5T mpMRI T2, DWI/ADC and post-contrast images were obtained and reported blind according to PIRADS v2 by an experienced uroradiologist. We present histological results of TTb with negative mpMRI.
Results: 151 patients underwent TTb, either as a part of PSA follow-up or as part of active surveillance. Median age was 66 years (range 49 – 80) with a median PSA of 9.2ng/mL (range 0.6 – 110). The median number of previous negative biopsies was 1 (range 1 – 5). 59 (39%) of 151 patients had a negative mpMRI. Out of these, 30 (51%) had PCa on TTb, thereby being understaged on mpMRI. 16 (53%) of these had Gleason 3 + 3 PCa with the remainder 14 (47%) having Gleason>/= 3 + 4.
Conclusion: This early dataset suggests that NICE recommendation would have missed significant prostate cancer in 24% of men with negative mpMRI. Thus, patients with negative mpMRI cannot be reassured and we recommend that it should be complemented with TTb. Further research is recommended and is currently ongoing at our institution.
P3-12 Targeted only biopsies of the prostate based on mpMRI: performance and accuracy of the transperineal route under conscious sedation
CG Orczyk, H Sidhu, P Punwani, A Freeman, C Moore, M Arya, M Emberton, HU Ahmed
University College London
Introduction: MRI-Targeted biopsies are increasingly common in the prostate cancer detection and risk stratification. Whilst commonly transrectal, the risk of sepsis secondary to faecal contamination and multi-resistant bacteria is rising. Transperineal biopsies rarely cause sepsis. Hitherto, transperineal biopsies have been conducted under general anaesthesia making widespread use unfeasible. We report on the performance of transperineal MR-targeted biopsies alone using local anaesthetic and conscious sedation.
Materials and Methods: We retrospectively reviewed consecutive treatment-naïve patients undergoing transperineal MR-targeted only biopsies under conscious sedation using visual/cognitive estimation (2014-2015). Local anaesthetic combined with intravenous propofol or intravenous midazolam was used. MRI sequences included T2W, DWI with ADC map and long b-value and dynamic-contrast.
Results: 89 patients with 166 mpMRI suspicious lesions were targeted (Table 1). All men were discharged the same day 1-2 hours after biopsy. There was no reported urinary infections or sepsis within 30 days of the procedure. The overall cancer detection rate was 72/89 (81%). 60/72 (83.3%) harboured significant cancer (UCL definition 2: Gleason ³3+4=7 and/or maximal cancer core length>3mm). Cancer detection rate for clinically significant disease was 34/34 (100%) for PIRADS score 5, 35/43 (81.3%) for score 4 and 25/89 (28%) for score 3 (Table 2).
(P3-12 Table 1)
Population
PSA (ng/ml, median)
7.2
Age (years, median)
66
Number of targeted suspicious lesion (median)
2
Targeted biopsy maximum Gleason Score (n=72)
3+3
15
3+4
45
4+3
10
4+5
2
(P3-12 Table 2)
mpMRI lesion score (n=166)
No. suspicious lesions (%)
No. lesions with any cancer (%)
No. lesions with significant cancer (UCL definition 2) (%)
Score 5
34 (20)
34 (100)
34 (100)
Score 4
43 (25.9)
35 (81.3)
29 (67.1)
Score 3
89 (54)
41 (46)
25 (28)
166
110 (66)
88 (53)
Conclusion: Patients and their physicians wishing to virtually eliminate risk of sepsis from a transrectal MR-targeted biopsy should be aware that transperineal MR-targeted prostate biopsy under local anaesthetic and conscious sedation is feasible, safe, tolerable and has high diagnostic performance.
P3-13 What are the radiological, surgical and patient factors influencing detection of cancer by MRI-targeted prostate biopsy?
V Kasivisvanathan, S Renshaw, A Grey, H Mair, O Nehikhare, E van der Saar, R Warner, M Emberton, H Ahmed, C Moore
University College London / UCLH
Introduction: Although the early detection rates of MRI-targeted prostate biopsy (MRI-TB) are encouraging, there is little evidence on what radiological, surgical and patient factors influence detection of cancer by MRI-TB.
Methods: Men with suspected prostate cancer undergoing multiparametric MRI (scored on a 1-5 Likert scale) followed by cognitively registered transperineal MRI-TB at a single centre in a 30-month period, were included. MRI included T2-weighted, diffusion-weighted and dynamic-contrast enhanced sequences. Factors influencing detection of cancer by MRI-TB were investigated with a multivariate logistic regression using STATA software.
Results: The analysis included 744 men undergoing MRI-TB, with mean age 66 and median PSA 7.4. Cancer was detected in 543 men (73%). After adjusting for age, MRI-reporter and surgeon, factors associated with the detection of cancer included the MRI-Likert score (p<0.0001), prior biopsy status (biopsy naive, previous negative biopsy, previous positive biopsy, p=0.0013), the number of targeted cores taken (p=0.0032) and MRI-coil strength (1.5T vs 3T, p=0.018). Factors not associated with detection of cancer included anaesthetic (general versus local, p=0.316), abnormal digital rectal examination (p=0.538) and location of tumour (anterior vs posterior, p=0.5952; basal vs apical, p=0.4324).
Conclusion: MRI-TB is a complex intervention with high detection rates of cancer. Several key factors that influence the odds of detection of cancer have been identified in this study and their relative importance established. This study validates the MRI-Likert score as one of the strongest predictors of cancer detection. It supports taking more than 3 targeted biopsies per patient. Notably, this data also supports the feasibility of a local anaesthetic-only approach.
P3-14 Multiparametric MRI and targeted biopsy: Use in active surveillance protocols
J Eldred-Evans, K Wong, A Polson, G Rottenberg, B Challacombe, S Van Riji, R Popert
Guy’s and St Thomas’ NHS Trust
Introduction: Multiparametric MRI (mpMRI) andtargeted biopsy have a growing importance in active surveillance protocols. Multiparametric MRI (mpMRI) is required in some active surveillance protocol prior to enrolment and for surveillance. This study assessed the ability of Multiparametric MRI and MRI-US fusion targeted biopsy to detect clinically significant prostate in active surveillance patients.
Methods: A prospective paired cohort of 53 active surveillance patients with suspicious lesions on mpMRI. Lesions were scored from 1 to 5 by an expert uro-radiologist according to the European Consensus guidelines (PI-RADS). MRI-US fusion targeted biopsy of the lesion was performed using Varian brachytherapy software. After targeting the lesion, the remaining prostate was systematically sampled with transperineal sector biopsy.
Results: The overall detection rate was 98% (52/53) and 79% was clinically significant (42/52). Targeted biopsy alone identified 83% of cancers (44/53). As the PI-RADS score increased, the detection rate of clinically significant cancer increased (AUC 0.82 CI 0.74-0.88). Gleason score was upgraded in 30% (16/53) and 49% (26/53) opted for active treatment.
Conclusions: Patients with a lesion identified on mpMRI have a greater risk of Gleason Score upgrading at targeted biopsy. Targeted biopsy has a high overall detection rate particularly with PI-RADS 4 and PIRADS 5 lesions. However, clinically significant cancer will be missed if biopsies are limited to the lesion only. mpMRI should not be used to exclude clinically significant prostate cancer in active surveillance protocols.
P3-15 Combining mpMRI sequences for the diagnosis of prostate cancer – the value of adding diffusion and contrast enhancement to T2: outcomes from the PICTURE trial
JB Neves, L Simmons, A Kanthabalan, A Freeman, S Punwani, Emberton, C Moore, M Arya, S Charman, HU Ahmed
Division of Surgery and Interventional Science, University College London
Introduction: Consensus is still lacking on which multi-parametric MRI (mpMRI) sequences provide better diagnostic accuracy in prostate cancer.
Patients and Methods: Analysis of prospectively collected data from a single-centre trial cohort (PICTURE). All patients had prostate 3T-mpMRI and template transperineal prostate mapping biopsies (reference). All had undergone previous TRUS-biopsies. mpMRI was scored sequentially [T2-weighted (T2W) alone vs. T2W+ diffusion weighted imaging incorporating ADC-map and b2000 (DWI) vs. T2W+DWI+ dynamic contrast enhancement (DCE)]. A score⩾3 was considered positive for cancer. Clinically significant cancer was defined using UCH1 (Gleason⩾4+3 and/or maximum cancer core length (MCCL)⩾6mm) and UCH2 (Gleason⩾3+4 and/or MCCL⩾4mm) definitions. Sensitivity, specificity, positive predictive value and negative predictive value (NPV) of combining mpMRI sequences were calculated. Area Under Receiver operating characteristic (AUROC) were compared.
Results: 249 men had median age 62±7.1years, median PSA 6.8±4.3, mean number of previous biopsies 1.41±0.69. Using UCH1 definition, for T2W vs. T2W+DWI vs. T2W+DWI+DCE the AUROC were 0.742, 0.764, and 0.766, respectively (p=0.55). Sensitivity was 96%(95%CI 90-99), 96%(95%CI 90-99), and 97%(95%CI 92-99), respectively. Using UCH2 definition, for T2W vs. T2W+DWI vs. T2W+DWI+DCE the AUROC were 0.772, 0.783, and 0.790, respectively(p=0.79). Sensitivity was 92%(95%CI 87-96), 95%(95%CI 90-98), and 96%(95%CI 92-99), respectively. NPV showed no significant change (range 86-91% for UCH1, 71-73% for UCH2).
Conclusion: Using 3T-mpMRI in men with prior TRUS-biopsies requiring risk stratification leads to high sensitivity and NPV. The added-value of functional sequences was marginal with only a trend towards better sensitivity for T2W+DWI versus T2W alone. The added-value of DCE remains questionable in this scenario.
Tuesday 28 June 1430-1545 Room 12 ePoster Session 4 – Education and Managing Urological Practice Chairs: Kieran O’Flynn and Richard Robinson
P4-1 Initial experience of an algorithm-based protocol for the community follow-up of men with stable prostate cancer
PP Goodall, J Little, E Robinson, I Trimble, OJ Cole, TJ Walton
Nottingham City Hospital
Introduction: We evaluated the implementation of a novel algorithm-based discharge programme for the community follow-up of men with stable prostate cancer.
Patients and Methods: Patients with stable prostate cancer considered suitable for discharge were identified. Men were discharged on to one of four discharge pathways: watchful waiting, androgen deprivation therapy (ADT), post-prostatectomy and post-radiotherapy. Primary care providers were asked to adhere to specific surveillance measures and refer patients back to secondary care following breach of pre-defined PSA threshold criteria. Reasons for non-compliance, re-referral and cause of death were determined for all discharged men.
Results: 573 men were discharged across all four pathways. All patients had a minimum 12 months follow-up. 48 of 54 (88.9%) of men were re-referred to promptly following PSA-threshold breach. Of the remaining six patients there were three refusals, one unrelated death prior to referral and two late referrals at four months. Three patients were lost to follow-up due to database non-registration and were subsequently recalled, none of whom had a PSA-threshold breach. There were three unexpected deaths attributed to prostate cancer: two were community deaths with no biochemical or clinical evidence of prostate cancer progression; one was due to a likely progressive PSA non-secreting tumour five months after discharge to primary care.
Conclusion: Initial results suggest the algorithm-based protocol is a viable, effective and oncologically safe method for the controlled discharge of men from secondary to primary care. Longer-term follow-up, patient satisfaction and cost-effectiveness data are required to assess the true impact of the initiative.
P4-2 Who manages metastatic prostate cancer? Results from the National Prostate Cancer Audit
MG Parry, A Sujenthiran, A Aggarwal, P Cathcart, S Charman, J Nossiter, H Payne, J van der Meulen, N Clarke
Clinical Effectiveness Unit, The Royal College of Surgeons of England
Introduction: The management of men with metastatic prostate cancer has traditionally been shared between urologists and oncologists. However, the paradigm of shared care continues to evolve with the advent of new drugs. Many of these drugs are only available through the Cancer Drugs Fund which urologists cannotaccess. This has led to a debate regarding who should manage men with metastatic disease. This study aims to identify current specialist care pathways in the NHS.
Patients and Methods: A survey was sent out to 154 local multi-disciplinary teams (MDTs) managing prostate cancer at 144 NHS providers in England and 10 in Wales. MDT lead clinicians were asked about the availability of urologists and/or oncologists at clinic appointments, and the presence of a dedicated metastatic clinic.
Results: There was a 100% response rate from the MDTs. 33% had a dedicated clinic for patients with metastatic prostate cancer. 73% of MDTs had access to both a urologist and a clinical/medical oncologist with 35% having a joint specialist clinic. Only 9% had a clinic with solely urological input and only 18% with solely oncological input.
Conclusion: The majority of MDTs in England and Wales had urological and oncological input into the management of patients with metastatic prostate cancer. MDTs which do not provide input from oncology should aim to do so in order to improve access to newer therapies. A dedicated joint specialty clinic was only available in about one in three MDTs and remains the best resource available for patients with metastases.
P4-3 Can we delegate TRUS biopsies to nurse urologists or middle grades and how much training do they require?
JFD Donaldson, WG Gietzmann, ML Lardas, KW Wardlaw, AR Rawlinson, JS Royle
Aberdeen Royal Infirmary
Introduction: TRUS prostate biopsy is increasingly performed by nurse urologists or middle grades. This study aims to compare the outcomes of experienced urologists with nurse urologists and speciality trainees (ST3) with no prior experience of TRUS biopsy. Guidelines require 50 biopsies for the award of a certificate of completion of training.
Patients & Methods: A prospective cohort analysis of all patients with PSA ⩽20ng/ml undergoing first TRUS biopsy was performed. Technique was standardised. A visual analogue pain score was completed (0:none to 10:agonising). Learners were first taught to scan, then to infiltrate local before undertaking biopsies.
Results: 252 men aged 65.8 years (48-80) underwent biopsy. There were no significant differences in cancer detection, core length, pain score, age or PSA (see Table 1). Initial direct supervision was withdrawn when appropriate, which varied between learners (6-14 biopsies). A learning curve was not demonstrated (likely due to appropriate supervision).
(P4-3 Table 1)
Number of patients
Average PSA (ng/ml)
Cancer Detection rate
Core length (mm)
Pain Score (0-10)
Experienced Urologists (n=2)
87
8.1
40.2%
14.5
2.3
Novice operators (3 trainees, 1 nurse)
165
8.5
40.6%
14.2
2.5
p value
0.477
0.954
0.580
0.418
Conclusion: There are no significant differences between a nurse urologist, ST3 or experienced urologists in TRUS biopsy cancer detection, core length and pain outcomes. This supports the continued training of, and service delegation to nurse urologists and middle grades. This study also demonstrates that competency in terms of cancer detection and patient acceptability can be achieved with a small numbers of biopsies.
P4-4 Do specialist renal MDT meetings provide good value?
JB Neves, S Shepherd, J Morales, D Cullen, M Aitchison, M Tran
Division of Surgery and Interventional Science, University College London
Introduction: The National Peer Review Programme mandates that all cancer patients are reviewed at multidisciplinary team (MDT) meetings. At a time when the NHS budget is under unprecedented pressure, we report on the cost of the specialist Renal MDT (sMDT) meeting at our high volume specialist centre.
Materials and Methods: Cases discussed and member attendance records from 10 three-hour sMDT meetings (14/10/2015 to 16/12/2015) involving 13 referring hospitals were reviewed. The cost of the meeting was calculated as the number of hours required to prepare and attend the meeting, using the mid-point of pay band attributable to the attendees. The cost per meeting, per case, and per patient was calculated. Annual cost was extrapolated.
Results: The renal sMDT involves 15 core and 18 extended members. Over 10 weeks, 518 cases (478 of suspected cancer – 222 first-time discussions, 256 re-discussions – and 40 of benign lesions) were discussed. In total, 393 patients were discussed (366 with suspected cancer and 27 with benign lesions). A quarter of cases were discussed to review histology. On average, each case discussion took 3.5 minutes. The estimated average cost was: £146,852.7 per year, £2820.2 per meeting, £53.5 per case discussed, and £70.5 per patient.
Conclusions: The headline annual cost for our sMDT surpasses the highest pay-point of a Consultant salary and reflects the clinical time involved in the process. In a high volume centre, the cost per case is modest and represents good value in providing a focused decision making structure for renal cancer patients.
P4-5 Trends and outcomes in a ward-based urology assessment unit – implications for ambulatory care provision
RD Sandler, SK Conroy, S Miah, S Venugopal, DJ Rosario
Sheffield Teaching Hospitals NHS Foundation Trust
Introduction: Relocation of the emergency department and changes in cross-city on-call arrangements led to the development of a ward-based urology assessment unit (UAU) for assessment and management of acute urological episodes. With an improving clinical armamentarium alongside financial and political pressure towards developing ambulatory emergency care; the aim of this evaluation was to identify a cohort of acute urological patients who could be safely relocated to an ambulatory assessment setting.
Patients and Methods: Review of all patients managed through UAU over 3 months (December 2014 to March 2015).
Result: Of 824 total referrals, 21% (n=170) were semi-elective post-intervention reviews. The remainder were unplanned referrals (n=654), with 10% (n=66) requiring emergency intervention (53% radiological, 47% surgical). UTI (n=108), loin pain (n=94) and catheter-related issues (n=80), were the commonest indications for referral. Of those attending with loin pain 40% (n=38) were referred prior to diagnostic imaging. Of these, 40% (n=15) subsequently received no urological diagnosis. 73% (n=58) of patients presenting with catheter-related issues (n=80), underwent same-day discharges, which increased to 86% when these patients presented “in-hours”.
Conclusion: Relocation of an acute urology unit to an ambulatory setting is a feasible and safe but will require close co-ordination with an inpatient setting, a policy of accepting ‘proven urological diagnosis’ and improved integration with community services. Piloting an ambulatory assessment unit and comparing outcomes with these benchmark data is planned, to aid the reform of existing care pathways.
P4-6 An audit of outpatient procedure income
S Muktar, C Brown, C Martyn-Hemphill
King’s College Hospital
Introduction: Coded clinical data uses rules and conventions that, when applied accurately, result in the provision of high quality statistically meaningful data. Financially, coded clinical data is grouped to meet the reporting structure of ‘Payment by Results’ to ensure trusts are paid accurately for activity.
Methods: A retrospective audit to review the number of outpatient procedures performed over a one week period within a busy urology department. Clinic letters were reviewed for evidence of procedures performed that were previously not specifically coded for. New outcome forms were implemented to include an ‘outpatient procedure income table’ to be completed by the clinician at the end of the consultation to aid accurate coding. Following new outcome forms, we re-audited a further week of clinic letters to assess the financial implication of the new forms.
Results: On average there were 368 patients reviewed in urology outpatients with 86 procedures performed per week. If all procedures were coded correctly this audit demonstrates an expected weekly income increase of £23,754 per week.
Conclusion: The business intelligence unit at our trust has seen an increase of average weekly income by £14,000 in urology outpatients following new outcome forms. The discrepancy in actual financial gain compared to expected gain likely highlights inaccurate completion of the outcome forms. Coding data should be a true reflection of hospital activity so establishing a clinical coding system for all procedures financially benefits the department significantly.
P4-7 A mathematical approach to theatre list planning reduces wasted time and has the potential to reduce cost
JE Dyer, T Brophy, M Nagarajan, J Husain, A Thompson, EA Green
Wrightington, Wigan and Leigh NHS Foundation Trust
Introduction: Poor theatre utilisation, either in the form of over or under-running lists represents a significant problem across the UK. It is costly and features in quality indicator reporting.
Method: 500 consecutive patient records were interrogated to ascertain the anaesthetic and operative time for common urological procedures. The mean and standard deviation for each procedure was used to create a calculator, using Microsoft excel, that could predict the likelihood of overrun or underrun.
ROC analysis was then used to test our calculator and generate threshold values for further use. The calculator was then applied in a validation exercise and to test its feasibility. Finally, a single consultant used our calculator to plan their lists. The effect on wasted time (minutes either over or under run), was calculated.
Results: There was a high degree of agreement between then predicated and actual outcome of overrun (AUC 0.817) and underrun (AUC 0.824). In the validation phase our calculator correctly predicted overrun 5/12 and under run 7/8 times, 4 lists finshed on time, giving a PPV of 85%.
Use of our calculator lead to a non-significant change in the occurrence of underrun or overrun (13/19 before and 6/12 after). However, and most crucially, the mean number of minutes wasted per list more than halved from 45.8 minutes before to 18.8 minutes after (P<0.05).
Conclusion: Poor theatre utilisation leads to potentially unnecessary expense. A simple mathematical approach can improve listing and has the potential to reduce wasted time due to over or under running lists.
P4-8 Post-operative blood tests in patients undergoing urological surgery
P Ravindra, G Lam, MAW Miller
Northampton General Hospital
Most surgical procedures within Urology have a low rate of complications. There is no guidance in the literature on which patients should have post-operative blood tests. Anecdotal evidence suggests that current practice is based on tradition. We aimed to quantify the incidence of post–operative blood tests and to establish if patient management was consequently changed.
All adult patients undergoing Grade 1, 2 or 3 urological procedures that spent at least one night in hospital over a three month period was identified. The incidence of Day 1 post-operative blood tests was recorded. The consequence of any abnormal results was investigated.
170 patients satisfied the inclusion criteria. Median length of stay was 1 day (range 1-27). 94/170 (55%) patients underwent post-operative blood tests. The majority underwent FBC & U&E (92/94). There was no significant difference between pre-operative and post-operative haemoglobin and creatinine (p>0.05). There was a significant difference between pre-operative and post-operative sodium (average drop 2.02mmol/L [p=0.0004]). No patients received an unplanned blood transfusion. One patient was diagnosed with new severe hyponatraemia after a prolonged TURBT. The total cost of performing these tests was £854.02 (annual cost £3416.08). >90% of results were reported after 11AM thus delaying patient discharge.
There are a considerable number of blood tests performed with no clinical indication. Based on these findings, surgeons should adopt a patient-specific approach based on intra-operative judgement and clinical assessment. This would result in significant savings to the Trust both in terms of laboratory requirements and patient flow whilst maintaining safe practice.
P4-9 Safer handover at weekends: Making it stick
CK Gunner, N Mayall, E Bryan, R Inman
Royal Hallamshire Hospital
Introduction: Observation of poor documentation of weekend handover in urology inpatient notes led to the implementation of this audit. The Royal College of Surgeons guidance document ‘Safe Handovers’ details key components of a written handover that are vital for the protection of patient safety. We sought to assess compliance of our practice with these guidelines, to intervene if necessary and to re-audit in order to assess effectiveness of intervention.
Method: An initial audit was carried out on the urology wards of a single hospital. A weekend summary sticker was designed, including 11 pieces of information required for a safe, note-based handover to be completed easily by junior doctors, as highlighted in ‘Safe Handovers’. A closed-loop audit was carried out 4 weeks after the introduction of the sticker and a further cycle 8 weeks later. A staff opinions survey was also circulated.
Results: 90 patient notes were analysed overall. Initial audit revealed documentation of a weekend summary in 25% of notes. 64% documented current issues and 71% contained clear plans. After sticker introduction, use of a summary improved to 89% (81% at 12 weeks). Documentation of all audited parts of the plan improved, with 94% of notes containing a clear plan (81% at 12 weeks). 100% of urology staff (n=15) liked the stickers and 93.3% felt they improved safety.
Conclusions: Introduction of a weekend summary sticker dramatically improves documentation of clinical handover at weekends in urology inpatients. The improvement is sustained with time and the intervention is well-liked by staff.
P4-10 Is there increased mortality in urology patients admitted to hospital at the weekend?
R Hilbert, A Pai, S Bott
Frimley Park Hospital
Introduction: Government policy is to have seven day working including senior level input at the weekend. Urology patients in our hospital are currently seen at the weekend by a SpR or consultant in the morning and then are cared for by the on-call general surgical team. The current publicity around 24/7 working based on mortality statistics has led us to look at whether there is any evidence of increased mortality in hospital in urology patients at the weekend.
Method: Mortality data from general medicine, general surgery and urology from 2012 to 2015 and been used to produce SHMI (summary hospital-level mortality indicator) and HSMR (hospital standardised mortality ratio). The weekend and weekday data has been separated and compared.
Results: Over the last 3 years there have been 51 urology deaths within 30 days of leaving hospital of patients admitted during the week and 8 at the weekend. This equates to a SHMI of 82 and 60 respectively showing there is no increase in mortality at the weekend, quite the contrary. For general surgery the SHMIs are 78 and 82 for weekday and weekend respectively and for medicine the figures are 100 for weekdays and 107 for the weekend. HSMR data also reflects this pattern.
Conclusion: The comparison of weekend mortality index for Urology at our hospital to the weekday data and that of other specialties does not support the argument for increasing the number of urology doctors in hospital at the weekend at a senior level or otherwise.
P4-11 Which is better? Live surgical broadcasts vs better than live surgery
YC Phan, O Wiseman, P James, R Clayman, A Smith, A Rane
East Surrey Hospital
Introduction: Recently, the use of “live surgical broadcasts” (LSB) as an educational tool to demonstrate surgical techniques at conferences has come under the spotlight with concerns surrounding the patient’s and surgeon’s wellbeing and safety. Additionally, there are notions that “better than live surgery” (BTLS), pre-recorded unedited videos showing either the whole procedure or key features, may be educationally superior. Our study was undertaken to determine which was deemed better by a diverse group of international urologists.
Methods: At the World Congress of Endourology held in London in October 2015, all participants were invited to complete an electronic survey using the conference app regarding LSB demonstrations compared to BTLS videos before and after the congress. Only BTLS were used in the congress.
Results: In the pre-conference survey, 212 participants replied. 76.9% thought more teaching could be achieved in less time with BTLS; while 52.8% replied that BTLS was more educational, and 52.8% rated BTLS as superior to LSB.
In the post-conference survey, 156 participants replied. 78.2% thought more teaching could be achieved in less time with BTLS; 54.5% thought that BTLS was more educational, and 60.3% rated BTLS as being better and more superior to LSB.
Conclusion: The pre-conference and post-conference survey revealed an increase percentage of respondents who thought BTLS is more educational and better than LSB after being exposed to BTLS during the congress. This suggests that BTLS is a better and more effective educational tool than LSB while ensuring the safety and well-being of both surgeons and patients.
P4-12 Impact of Urology Simulation Boot Camp in improving the endoscopic instrument knowledge
S Rajpal, VS Hanchanale, S Jain, K Rogawski, J Taylor, R Gowda, I Eardley, T Terry, A Myatt, CS Biyani
LIMIT, Leeds Teaching Hospitals
Objective: Education and training of surgeons has traditionally focused on the development of individual knowledge, technical skills, and decision-making. The knowledge about endoscopic instruments is one of the core elements of urological training. We assessed the pre-course knowledge of newly appointed urology trainee and the impact of boot camp in improving their knowledge.
Methods: Sixteen newly appointed specialty trainees in urology took part in a pilot 5-day urology simulation boot camp. One of the modules looked at the trainee’s knowledge about common endoscopic instruments in urology. Delegates were first asked to identify and assemble instruments followed by one-to-one teaching about instruments. An Objective Structured Assessment Tool (OSAT) was used to assess their knowledge and assembly of cystoscope, resectoscope and optical urethrotome; before and at the end of the course.
Results: The proportion of trainees with good pre-course knowledge about cystoscope, resectoscope and urethrotome was 93%, 64% and 19% respectively. Post-course, all participants were able to identify and assemble the cystoscope and resectoscope sets. Despite the complexity of urethrotome assembly nearly all trainees (90%) attained confidence post-course. This shows that the urology boot camp significantly improved the equipment knowledge of urology trainees.
(P4-12)
Trainee Competency
Pre-Course (%)
Post-Course (%)
Cystoscope
Identify
95
100
Assembly
90
100
Resectoscope
Identify
70
100
Assembly
58
100
Urethrotome
Identify
24
95
Assembly
15
90
Conclusion: This urology boot camp has addressed gaps in the trainee’s core equipment knowledge and guided them to improve their knowledge with respect to identification and assembly of cystoscope, resectoscope and urethrotome.
P4-13 A 5-year review of operative experience and indicative numbers in urological training in the UK and Ireland
R Robinson, JE Dyer, E Lee, KJ O’Flynn, T Terry
Central Manchester University Hospitals NHS Foundation Trust
Introduction: JCST guidelines for the award of a CCT in urology were updated in 2015, with 17 operative domains and reduced indicative numbers for TURBT, procedures for male LUTS (PML), cystectomy, female incontinence and paediatric urology. In 2015 we published operative logbook data from urology CCT applications in 2010-2012. The aim of this study was to review a contemporary cohort against the 2015 guidelines and the previous cohort.
Materials and Methods: 77 Urology CCT application logbooks, March 2014 to October 2015 (2015 cohort), were reviewed and compared to 154 logbooks from 2010-2012 (2012 cohort).
Results: Across 14 directly comparable domains, there was a significant improvement (p<0.01) in the percentage of trainees achieving indicative exposure. Percentage increase in 13 of the 14 domains included PML 68% to 88%, TURBT 64% to 90%, paediatric urology 2% to 23%, female incontinence 9.5% to 34% and andrology 9% to 43%. There were significant reductions (p<0.01) in mean operative numbers for TURBT and PML at 184 to 162 and 187 to 161 respectively. Significant increases were identified in all other domains (p<0.05), apart from inguinal orchidectomy, PCNL, radical prostatectomy and radical cystectomy. In the 2015 cohort one trainee achieved the requirement in all 17 domains and 55% failed to meet the requirement in ⩾5 domains.
Conclusion: While increasing number of trainees currently meet JCST expectations, some domains remain at low levels. Continued reductions in exposure to core procedures of TURBT and PML is of concern. Further innovation in the delivery of surgical training is required.
P4-14 Updated indicative numbers: Are they now achievable? A UK regional training perspective
AK Nambiar, A Wright, O Fuge, L McGuinness, H Morton, J Cresswell
Cumberland Infirmary
Introduction: Indicative numbers for core urology procedures are set out by the JCST and are mandatory for award of CCT. Despite revision for 2015, there is concern among trainees about their practicality. In this audit we focus on bladder outlet (BO) and female incontinence (FI) procedures, reported by trainees as being most difficult to achieve.
Materials and Methods: We collected the total number of BO and FI procedures performed at the 4 main teaching centres in the north-east between 1st September 2014 and 31st August 2015. Theoretical averages for each trainee were calculated to compare JCST figures. Trainees provided individual numbers for comparison, and commented on factors they felt impeded them.
Results: 1113 BO and 96 FI procedures were performed in the year. With an average of 20 trainees this equates to 56 BO and 5 FI procedures per trainee per year. JCST requirements as of 2015 are 24 BO and 4 FI procedures per year (on average). But figures from trainee logbooks show that trainees are actually performing only approximately 20 BO and 4 FI procedures per year. Moving benign core urology cases to weekend lists (105 BO cases/year) and the sub-speciality nature of FI procedures were considered hindrances.
Conclusions: Revised JCST indicative numbers are a more realistic target, but FI procedures are still difficult to achieve because of poor access to lists, and smaller numbers conducted by urologists outside tertiary centres. BO numbers are adequate but some factors prevent trainees achieving them, and these need to be highlighted.
P4-15 Publication rate of abstracts presented at the British Association of Urological Surgeons (BAUS) Annual Meeting – 10 years on
AD Moon, C Harding
Freeman Hospital
Introduction: The presentation of abstracts at BAUS is sought after by trainees and encouraged by trainers, however it is the publication of this research in a peer-reviewed journal that validates the significance of the work.
We wanted to reassess the rate and time to publication of abstracts presented at BAUS following a similar piece of work ten years earlier. In addition, whether there was a difference in the presentation and subsequent publication rates between UK deaneries.
Methods: Abstracts accepted for presentation at the BAUS 2012 and 2013 annual meetings were identified from published conference supplements. Abstracts were searched for using the Medline Plus (PubMed) database using authors’ names and title of the presented abstract to assess for successful conversion to peer-reviewed publication.
Results: 281 abstracts were presented - 144 in 2012 and 137 in 2013. Of these, 68 / 281 (24.2%) resulted in a successful conversion to a peer-reviewed publication. 10 years ago, the previous BAUS publication rate was 42%.
Mean time to publication was 11.59 months and mean impact factor of the publishing journal was 3.854. There was no correlation between the number of abstracts presented from a region and the subsequent successful conversion to publication.
Conclusions: There has been a decline in the number of BAUS abstracts being successfully converted into peer-reviewed publications. It has fallen from 42% to 24.2% over the past decade. This is an important finding as the quality of any scientific meeting can be quantified by the number of publications arising from its abstracts.
Wednesday 29 June 1030-1215 Room 4 ePoster Session 5 – Female Urology and Bladder Dysfunction Chairs: Claire Taylor & Marco Spilotros
P5-1 Results of the British Association of Urological Surgeons Female Stress Urinary Incontinence Procedures Outcomes Audit
S Cashman, N Thiruchelvam, R Morley
Bedford Hospital NHS Trust
Introduction: Following the government’s plans to publish individual surgeon’s outcome data in 2012, the British Association of Urological Surgeons (BAUS) initiated a number of nationwide audits in order to capture current UK practice and outcomes. We present the results of the first two years of the BAUS female stress urinary incontinence procedures outcomes audit.
Materials/Methods: Data from relevant procedures performed in 2013-2014 was prospectively entered into the online database. Metrics included both surgeon-specific and patient-specific data. The results were collated centrally by the BAUS audit office and subsequently analysed.
Results: 1381 procedures were reported, with 91 consultants submitting data from 72 centres, with increasing data submission from 2013 to 2014. A median of 11 procedures were performed by each consultant, with variability in the range of procedures performed by each individual. 93.5% of patients had pre-operative urodynamic assessment, with urodynamic stress urinary incontinence identified in 73.9% cases. No complications were recorded in 91% of procedures. In those patients with follow up data entered, patient reported outcome measurements demonstrated reduced pad usage in 86.6%, and ICIQ sum score improvement in 92.2%.
Conclusion: Initial results demonstrated good clinician engagement, with increasing year on year uptake. Some initial areas for improvement within the database have been identified. Variation in the number and range of procedures offered by individual clinicians has been identified. Perioperative complication rates were comparable to those reported in other series, with good patient outcomes measures reported. We hope data entry will continue to improve in the coming years.
P5-2 Female urethral diverticula: Presenting features and symptomatic outcomes
S Malde, N Sihra, S Naseeri, MH Pakzad, R Hamid, PJR Shah, JL Ockrim, TJ Greenwell
University College London Hospital
Introduction: Female urethral diverticula are rarely seen in general urological practice and their nonspecific presenting symptoms can result in misdiagnosis and delayed management. We aim to review the presenting features and symptomatic outcomes of all women who have undergone urethral diverticulectomy surgery in our specialist centre.
Patients and Methods: We reviewed our prospectively gathered database of all female patients having excision of a symptomatic urethral diverticulum between 2007 and 2015.
Results: A total of 70 women with a mean age of 46.5 years (range 24-77) had excision of a urethral diverticulum with Martius fat pad interposition over this 8 year period. Pre and post-operative symptoms at a median follow up of 14 months (range 1-72 months) are shown in table 1.
(P5-2)
Symptom
Before surgery
N (%)
After surgery
N (%)
Pain
43 (61)
8 (11)
Dysuria
40 (57)
2 (3)
Dyspareunia
37 (53)
2 (3)
UTIs
32 (46)
1 (1)
Dribble
29 (41)
1 (1)
Stress urinary incontinence
28 (40)
13 (19)
Frequency/Urgency
19 (27)
7 (10)
Poor flow
19 (27)
1 (1)
Urethral discharge
16 (23)
0 (0)
New onset USUI
0 (0)
4 (5)
Conclusion: The commonest presenting symptom of a female urethral diverticulum is urethral pain followed by dysuria and dyspareunia. Surgical excision results in complete resolution of symptoms in the majority of women. The incidence of de novo SUI is low at 5% and pre-existing SUI resolves post surgery in 57%.
P5-3 Can pre-operative MRI characteristics predict new onset urodynamically proven stress urinary incontinence post excision of female urethral diverticulum
S Malde, N Sihra, M Spilotros, S Naseeri, MH Pakzad, R Hamid, JL Ockrim, TJ Greenwell
University College London Hospital
Aims: To assess the ability of pre-operative MRI characteristics to predict new onset urodynamic stress urinary incontinence (USUI) following excision of urethral diverticulum in females.
Patients and Methods: Review of a prospectively gathered database of all female patients having excision of urethral diverticulum and comparison of their pre-operative MRI characteristics with the post-operative incidence of new onset USUI.
Results: 95 women mean age 46.5 years (range 24-77) had excision of urethral diverticulum between 2002 and 2015 – 71 of whom had both preoperative MRI and VCMG.
30 women had preoperative USUI and were excluded from further analysis. The remaining 41 women (mean age 44.6 years range 24-73) did not have pre-operative USUI (Table 1).
(P5-3)
MRI characteristic
No Post-Op USUI
Post-Op USUI 3m
Post-Op USUI 12m
Number
31 (76)
10 (24)
5 (12)
Simple N (%)
5 (17)
1 (10)
1 (20)
Horseshoe N (%)
16 (52)
5 (50)
1 (20)
Circumferential N (%)
10 (32)
4 (40)
3 (60)
Mean Transverse Diameter (mm)
28
27
28
Mean Coronal Diameter (mm)
25
24
31
Mean Sagittal Diameter (mm)
29
26
29
Loculated (%)
89
66
60
Degree of Urethra Surrounded by Diverticulum
256
268
298
Os N (%)
1 (100)
1 (100)
1 (100)
Mean Os Distance to Meatus (mm)
20
18
17
Mean Os Distance to Bladder Neck (mm)
18
17
21
Length of Urethra
37
35
38
Mean Age Years
43
46
49
Conclusion: In women having excision of urethral diverticulum new onset USUI persists at 12 months in 12%. These women tend to be older with a larger degree of their urethra surrounded by their diverticulum but this does not reach statistical significance.
P5-4 Total pelvic exenteration for locally advanced and recurrent rectal cancer: Urological outcomes and adverse events
O Khan, D Patsouras, R Thuairaja, MS Khan, A Schizas, M George, A Sahai
Guy’s Hospital
Introduction: The aim of this study was to assess the outcomes of urinary tract reconstruction following total pelvic exenteration (TPE) for advanced or recurrent rectal cancer with a specific focus on adverse events and complications.
Patients and Methods: All patients who underwent TPE for primary advanced or recurrent rectal cancer at our centre from 2004 to 2014 were included in this single centre retrospective study. A colorectal database, electronic patient records and notes were evaluated for data extraction. We used chi square tests to compare outcomes between patient groups with a threshold of significance of p<0.05.
Results: A total of sixty patients (21 females, 39 males, mean age 61 years) were identified. 70% received chemo-radiation prior to TPE. Fifty-seven patients (95%) received an incontinent diversion, including fifty-five ileal conduits and two colonic conduits. Three (5%) patients received a continent diversion (Penn pouch with mitrofanoff). The rate of urological complications in our series was 55%. The majority of patients had a Clavien-Dindo score of 2 (30%), while only two patients (3%) suffered life-threatening complications. The most common complications were urinary tract infection (37%) and renal insufficiency (13%). Ureteric strictures were seen in 5% and re-operation rates were 10% for the cohort. There was no significant difference in urological outcomes in patients with primary or recurrent rectal cancer (p=1) or chemo-radiation status (p=0.78).
Conclusions: Our urological outcomes and complication rates are acceptable following TPE with no significant difference between primary and recurrent rectal cancer or those receiving chemo-radiation in our cohort.
P5-5 Bladder cancer in the neuropathic bladder
A Mangera, K Dubey, D Drummond, SV Reid, PR Tophill
Princess Royal Spinal Injuries Unit
Introduction: A higher risk of developing bladder cancer has been suggested for patients with a neuropathic bladder. Risk factors are poorly understood. We aimed to look at the bladder management strategies employed in a cohort of patients with neuropathic bladder who developed bladder cancer.
Methods: Bladder cancer diagnoses were identified and recorded by one author from 2001 to 2014. Analysis of medical records of all identified urological cancer diagnoses from patients at our Spinal Injuries Unit was undertaken in March 2014.
Results: We identified 22 cases of bladder cancer. Mean age was 52 years, 73% were male, 21% smokers and mean time to cancer diagnosis after neuropathic insult was 36.5 years. Histologic type included SCC 36%, TCC 36%, adenocarcinoma 14% and others 14%. The majority (86%) were pT2 or above at diagnosis, half were diagnosed incidentally on routine imaging and mortality was 59%. Three patients (14%) have survived beyond 10 years after cancer diagnosis. Table 1 shows the bladder management strategies and risk factors found in patients with bladder cancer.
(P5-5 Table 1)
Bladder management strategy
Frequency/ 22 (%)
ISC> 1 year
4 (18)
LTC/SPC> 1 year
12 (55)
Cystoplasty
1 (5)
Diversion/ no cystectomy
5 (23)
Reflex voiding
9 (41)
Recurrent UTI
13 (60)
Bladder stones
2 (9)
Conclusions: Cancer was often of high grade and stage, with high mortality. Chronic indwelling catheter use, pyocystis, and recurrent UTI are linked to bladder cancer. Intermittent self-catheterisation, cystoplasty and bladder stones were less frequently associated with bladder cancer.
7 out of 8 (87.5%) women who completed the treatment reported no subsequent UTIs. 1 case was excluded as the patient was given empirical antibiotics for dysuria by the GP before sending culture for confirmation of infection.
P5-7 The MIC-KEY Button vesicostomy: A superior alternative for supra-pubic bladder drainage?
J Seth, E Hazell, W Nugent, C Taylor, A Sahai, J Olsburgh
Guy’s Hospital
Introduction: The complications of indwelling suprapubic-catheters (SPCs) result in multiple hospital attendances in up to 43%. An alternative form of bladder drainage offering fewer UTIs, more comfort, less blockages and spasms would be highly desirable. The aim of this study was to capture patient-reported outcome measures (PROMS) to assess the feasibility of the MIC-KEY vesicostomy button as a novel form of bladder drainage.
Patients and Methods: This prospective pilot study recruited patients with long-term indwelling SPCs who were seeking an alternative. At the next catheter change, SPC tubes were removed and replaced by MIC-KEY button tubes. Catheter-related quality of life (C-IQoL) questionnaires were completed at baseline and at three-months. The C-IQoL consists of three domains assessing management, psychosocial and interpersonal aspects.
Results: Seven female patients were recruited (mean age 34.9 years; range 25-46 years). The mean duration of SPC use was 3.5 years. Improvements were seen for all three C-IQoL domains at three-months follow-up, with improvement in mean total score from 52.2 at baseline to 80.1 at 3 months (p=0.006). This reached significance for the management and psychosocial domains, with patients reporting fewer blockages, superior comfort and less bladder spasm. All patients requested continuation with MIC-KEY and declined transferring back to traditional SPC use.
Conclusion: This pilot study suggests that use of the “MIC-KEY button” as an alternative to SPC is feasible, safe and satisfactory in this group of adult patients. Significant benefits were seen with the catheter management and psychosocial domains of C-IQoL. Further evaluation is required to assess long-term efficacy and cost-effectiveness.
P5-8 Evaluating pad weight gain in asymptomatic women
M Duffy, C Nicholls, A Gora, R Hamid, JL Ockrim, TJ Greenwell, MH Pakzad
University College London Hospital
Introduction: Pad weight gain (PWG) is widely used as a measure of the volume of urine leakage in women. The ICS assessment of incontinence committee suggests that a pad weight gain >1g/hr or 4g/24 hrs is a positive test for urinary incontinence. We hypothesise that the threshold for bothersome as well as normal levels of leakage are far lower than this threshold.
Materials & Methods: A pilot observational study was performed measuring the increase in weight of small sanitary pads worn by 21 healthy, female volunteers of mean age 41.9 (±10.8) years for a minimum of 5 hours. Pads were placed in an airtight medical grade plastic sample bags, and combined bag and dry pad weight measured using scales accurate to 0.001g.
Anonymous data was collected on age; weight; height; obstetric, gynaecological and urological history.
Results: The mean pad weight gain (±SD) was 0.166 (±0.158)g (range 0.024-0.621). The mean time of pad wear (±SD) was 5.71 (±0.94) hours. A histogram showing the distribution of recorded pad weight gains is included (Figure 1). (P5-8)
No correlation was observed between pad weight gain and BMI, parity, age, hours worn or years since last birth.
Conclusions: pPd weight gain in women who do not complain of urinary incontinence is typically in the range 0-0.48g (95% confidence interva). This suggests that symptomatic women ‘leaking’ more than 0.5ml in 5 hours may be considered to have urinary incontinence. Further volunteers will be sought to validate the results of this pilot.
P5-9 A single centre experience with Bulkamid® a urethral bulking agent for the treatment of stress urinary incontinence in females
FA Kamarizan, T Jabbar, M Saeed, J Filby, O Aboumarzouk, A Thomas
Royal Gwent Hospital
Introduction: Periurethral injections using bulking agents is a recognised and common management option for urinary stress incontinence in women. Bulkamid® is a homogenous hydrophilic gel consisting of 2.5% polyacrylamide and 97.5% water, allowing in-growth and proliferation of blood vessels originating from the periurethral tissue.
The primary aim of this study was to demonstrate the efficacy of Bulkamid® as a bulking agent for the treatment of stress urinary incontinence in adult females. The secondary aims were to investigate the effects of BMI, duration of urinary symptoms and age on the efficacy of this treatment.
Method: A retrospective study performed in a district hospital evaluated 143 patients who underwent periurethral Bulkamid® injection between April 2010 and March 2015. All patients included in this study had urodynamic stress urinary incontinence, and efficacy was assessed using a subjective self-assessment questionnaire after at least 1 injection.
Further sub-analysis was performed to investigate the effects of age, duration of symptoms and BMI on the effectiveness and complications of using Bulkamid®.
Results:
(P5-9 Table 1) Outcome of patients receiving Bulkamid® injections.
Complications
15/143 (10.2%)
UTI
9/143 (6%)
ISC
4/143 (2.8%)
Haematuria
2/143 (1.4%)
Failed procedure
36/143 (25.2%)
Primary procedure
134 (94%)
Secondary procedure
9 (6%)
Requiring repeated injections
61/142 (42.7%)
1 further injection
38 (26.2%)
2 further injection
18 (12.6%)
3 further injection
4 (2.8%)
>3 further injection
1 (0.7%)
Conclusion: Bulkamid® is an effective and safe bulking agent in women with stress or mixed incontinence, comparing favourably with other reported urethral bulking procedures with medium-term responders.
P5-10 Management of stress urinary incontinence in females after spinal cord injury with mid-urethral tapes – a tertiary centre experience
V Sakalis, M Floyd, C Price, B Hartwell, P Guy, M C Davies
Salisbury NHS Foundation Trust & The Duke of Cornwall Spinal Injuries Unit
Introduction: The incidence of stress urinary incontinence (SUI) in females after spinal cord injury (SCI) is not known. The negative impact of SUI in these patients is significant and results in dermatitis and pressure sores. We report the outcomes of mid-urethral tape (MUT) surgery in this group.
Patients & Methods: All SCI patients who had MUT insertion between 2007 and 2015 were reviewed. All patients had pre-operative video-urodynamic studies (VUDS) and proven SUI. The patient’s notes and the International Consultation on Urinary Incontinence Questionnaire (ICIQ-UI) were assessed.
Results: 22 SCI patients were identified who had undergone MUT surgery. Results were available for 17 patients, 5 were lost to follow up. There were 12 TVTs and 5 TOT procedures undertaken. The mean age at operation was 54.5 years (range 26-73 years). The mean follow-up was 54.5 months (range 6-92 months).
Pre-operatively 14/17 (82.3%) patients reported that SUI was a major problem. Post-operatively; 5 patients (30%) are completely dry, 9 patients (53%) leak once a week or less and 2 patients (12%) leak two or three times per week. Only 1 reported leaking several times per day. Mean ICIQ score pre-operatively was 16.1 (range 6-21) and post-operatively 3.75 (range 0-18), p<0.001. After surgery 16/17 (94%) reported their quality of life (QoL) was improved.
Conclusions: MUT surgery is effective in the management of SUI in SCI patients. There are improvements in both continence and QoL. The benefits are durable and comparable to outcomes seen in the general female population.
P5-11 The efficacy of sacral neuromodulation for treatment of male voiding dysfunction
M. Spilotros, S Malde, J Shah, M Pakzad, JL Ockrim, TJ Greenwell, R Hamid
University College London Hospitals
Introduction: Sacral neuromodulation (SNM) is an established treatment for controlling overactive bladder symptoms especially in females. Its role in males is not well defined. We reviewed our experience with this technique in this group.
Materials & Methods: We reviewed our prospectively collected database to identify male patients with voiding dysfunction undergoing trial of SNM over the last 18 months. All presented with voiding dysfunction with some in retention requiring self intermittent catheterization (SIC). All underwent video-urodynamic studies (VCMG). A neurological cause was excluded with clinical examination and cross sectional imaging.
Results: We identified 16 patients. The mean age was 44 years. Eight patients were performing SIC. One had a suprapubic catheter and 7 voiding with straining. VCMG revealed no detrusor overactivity in any with 10 demonstrating a contractile detrusor and 6 high pressure low flow system consistent with high tone non relaxing sphincter (HTNRS) on accompanying video clip. All underwent trial of tined lead for a minimum of 4 weeks. There was no significant benefit in 12/16 and the tined lead was removed. A successful outcome was demonstrated in 4/16 (25%) and a permanent pulse generator was implanted. It stopped working after few months in 1 patient. One needed to be explanted due to infection. Currently, 2/16 patients have a working implant.
Conclusion: It appears SNM is not an optimal therapy for treatment of non-neurogenic voiding dysfunction in male patients. We feel further work is required to identify specific-select patients with a larger cohort to evaluate its role in this particular condition.
P5-12 The outcomes in women with non-obstructive urinary retention and detrusor underactivity treated by sacral neuromodulation
V Phe, EM Solomon, J Jenks, N Sihra, J Panicker, R Hamid, JL Ockrim, TJ Greenwell, MH Pakzad
University College London Hospital
Introduction: We assessed the outcomes of SNM for treating non-obstructive urinary retention (NOUR) in female patients with detrusor underactivity (DU) and the factors predictive of successful or unsuccessful SNM outcome.
Patients and Methods: 45 female patients mean age 37.8 years (17-74) with NOUR and DU treated by SNM from January 2011 to July 2015 were retrospectively reviewed and data collected on: patient demographics, past medical history, mode of voiding, urodynamic parameters, urethral pressure profilometry (UPP) parameters including actual and expected maximal urethral closure pressures (aMUCP/eMUCP). Patients were assessed 4-6 weeks after tined lead insertion with a bladder diary. The SNM test was considered successful if: catheter usage was reduced by 50%+ ; spontaneous voiding was restored or there was a patient-reported improvement by 50%+.
Statistical analysis was by Mann-Whitney U, Chi-square and binary logistic regression analyses.
Results: The mean follow up was 15.5 months (2-62). All patients had higher than expected aMUCP.
Success rates after first and second stage were 68.9% and 77.4% respectively. After the second stage, the explantation rate was 2.2% due to pain. The revision rate was 12.9% due to pain or discomfort leading to resitting the battery.
None of the potentially prognostic factors investigated were found to significantly correlate with successful outcomes (all p>>0.05).
Conclusion: SNM is a safe and efficacious therapy for the treatment of NOUR and DU with a 77.4% success rate at a mean of 15.5 months. There were no significant positive or negative predictive factors for a successful outcome.
P5-13 Percutaneous nerve stimulation for overactive bladder: cost-effectiveness compared to mono and dual pharmacotherapy
J Jenks, E Solomon, S Malde, M Spilotros, R Hamid, M Pakzad, TJ Greenwell, JL Ockrim
Institute of Urology, University College London Hospitals NHS Trust
Introduction: Pharmacological treatments of overactive bladder (OAB) with anticholinergics and/or beta-3-adrenergic receptor agonists are standard treatment, but persistence with medical therapy is poor. Posterior tibial nerve stimulation (PTNS) is a minimally-invasive alternative but its cost-effectiveness is unknown. We compared cost-effectiveness of PTNS with mono (anticholinergic) pharmacotherapy and dual (anticholinergics and beta-3-adrenergic) therapy.
Methods: Pharmacotherapy consisted of monotherapy with solifenacin 10mgs, and dual therapy with the beta-3-adrenergic receptor agonist Mirabegron 50mgs. PTNS was based on twelve weekly sessions, then top-ups monthly. Treatment success was defined as >50% improvement in OAB symptoms. A Spanish Markov model was used based on published efficacy data and expert opinion. Persistence for treatment was taken to be 24% for both mono and dual pharmacotherapy (published data) and 60% for PTNS (hospital data). Health resource use included pre-/peri-/and post-procedure assessments; adverse events and procedure (PTNS) costs. Incremental-cost-effectiveness-ratios (ICER; costs per quality-adjusted-life-year) were calculated for PTNS monotherapy versus monotherapy and PTNS versus dual therapy at 5yrs; with univariate sensitivity analyses.
Results: At 5 years, the cumulative costs of monotherapy, dual therapy and PTNS therapy were £3,451, £5,222 and £8,011 respectively. The QALYs for monotherapy, dual therapy and PTNS therapy were 2.92, 3.11, and 3.45. ICERs for PTNS versus monotherapy were £10,604, and PTNS versus dual pharmacotherapy were £11,620 at 5 years.
Conclusions: PTNS for OAB patients provides quality of life improvement and ICERs that are below the threshold for UK cost-effectiveness. PTNS represents value for money but at incremental cost (more effective/more costly) compared to mono and dual pharmacotherapy.
P5-14 Sacral nerve stimulation versus botox for medically refractory overactive bladder: A contemporary review of UK clinician and patients’ perspectives
R Nobrega, S Malde, T Greenwell, R Pickard, JL Ockrim, C Harding
Institute of Urology, University College London Hospitals NHS Trust
Introduction: The prevalence of overactive bladder (OAB) in Europe is estimated to be 12.8-17.4%. In the UK, 97% (10,000/year) of medically refractory OAB patients receive Onobutulinum Toxin A (BTX) treatment and around 3% (300/year) receive sacral nerve stimulator (SNS) implants. Information culture and particularly the resistance to high initial capital costs have limited access to SNS. Current NICE guidelines propose using BTX before SNS whilst EUA/AUA offers both with equipoise, although these treatments have not been compared in any comparative study. The aim of this study was to explore both patients and clinician views regarding these two treatments.
Patients and Methods: Fifty consecutive OAB patients refractory to medical therapy were interviewed using structured questionnaires about their treatment preferences. We also asked 100 UK Consultant Urologists which treatment modalities they had available in their Trusts and were currently in use.
Results: 60% of patients preferred SNS over BTX, of these 80% would happily randomise into a trial between the two treatments. 97% of 100 Consultant Urologists in the UK have access to BTX in their hospitals, but only 39% have access to SNS. However, 71% of clinicians would use BTX as their first choice treatment.
Conclusions: There appears to be a significant disparity between current UK OAB guidance, NHS accessibility to BTX and SNS therapies, the views of clinicians, and patient preferences for treatment.
P5-15 The efficacy and safety of onabotulinumtoxinA and solifenacin compared to placebo in solifenacin-naïve patients with idiopathic overactive bladder: Results from a multicentre, randomised, double-blind trial
S Sriram, S Herschorn, A Kohan, P Aliotta, K McCammon, S Abrams, W Lam, K Everaert
University Hospital Coventry
Introduction: This randomised, double-dummy, double-blind study compared the efficacy/safety of onabotulinumtoxinA 100U or solifenacin with placebo in solifenacin-naïve patients with overactive bladder (OAB) who were inadequately managed by ⩾1 anticholinergic. A post-hoc analysis compared onabotulinumtoxinA and solifenacin.
Methods: Eligible patients were randomised 2:2:1 to onabotulinumtoxinA 100U/oral placebo (n=145), solifenacin 5-10 mg/placebo injection (n=151), or double placebo (n=60). Assessments (week 12) included LS mean change from baseline in urinary incontinence episodes (UIE)/day (co-primary), responder analysis of ⩾50% and 100% (‘dry’, co-primary) UIE reduction, and adverse events (AEs).
Results: 356 patients were randomised; discontinuations due to AEs (3.1%) and lack of efficacy (0.3%) were low. Mean baseline UIE/day was 4.94 and mean number of prior anticholinergics was 1.6. For onabotulinumtoxinA, solifenacin, and placebo patients, respectively, mean UI reductions/day were -3.2*, -2.6*, and -1.3; proportion of patients achieving 100% UI reduction were 33.8%*, 24.5%*, and 11.7%; and proportions of patients achieving ⩾50% UI reduction were 77.2%*, 64.9%*, and 33.3%. In the post-hoc analysis, onabotulinumtoxinA resulted in significantly greater mean UIE reductions/day (P=.022) versus solifenacin. Higher proportions of onabotulinumtoxinA-treated patients achieved 100% (P=.107) and ⩾50% (P=.025) UIE reduction versus solifenacin. Most common AEs were UTI, bacteriuria, dry mouth, and urinary retention. *P<.05 versus placebo.
Conclusion: OnabotulinumtoxinA resulted in greater reductions in daily UIE and higher proportions of patients with 100% and ⩾50% reduction in UIE than solifenacin or placebo, with 1/3 of patients becoming ‘dry’. There were no unexpected AEs.
P5-16 OnabotulinumtoxinA in refractory overactive bladder: Licensed vs traditional dose
J Eldred-Evans, J Seth, C Dowson, S Malde, C Taylor, J Watkins, MS Khan, P Dasgupta, A Sahai
Guy’s and St Thomas’ NHS Trust
Introduction: The licensed dose of OnabotulinumtoxinA in refractory idiopathic overactive bladder (OAB) is 100U based on phase II and phase III RCTs. Prior to regulatory approval our centre was administering 200U on an off-license basis. The effect of reducing the dosage in a ‘real life’ practice setting needs to be established and this study compares the outcomes of these two groups.
Patients and Methods: A prospective database was accessed to gather information on patients’ first OnabotulinumtoxinA injection with either 100U or 200U. Outcome measures included voiding diary parametres, quality of life scores and adverse events. Additional retrospective data was collected on discontinuation rates, time to request re-treatment and inter-injection interval.
Results: A total of 164 patients received 100U (78 patients) or 200U (86 patients). The efficacy outcomes and adverse events are compared in Table 1. 41.8% of patients who had 100U required dose escalation to improve efficacy. A longer duration of effect was demonstrated in 200U (13.2 months vs. 9.4 months). (P5-16)
100U
200U
p-value
Voiding Diary
Frequency/day
−3.51
−5.54
0.025
Urgency/day
−6.27
−6.95
0.579
Urgency Incontinence/day
−3.80
−3.16
0.609
Quality of life Scores
KHQ
17.17
26.77
0.160
UDI6
3.00
4.10
0.640
IIQ7
9.26
11.40
0.356
Side Effects
UTI
16.6%
17.4%
0.895
PVR
+96.77ml
+168.9ml
0.024
CISC
26.9%
38.3%
0.043
Conclusions: Efficacy outcomes in general were comparable. However longer duration of effect, higher CISC and higher discontinuation rate was observed in the 200U group. Overall this study supports the initial dose of 100U in patients with refractory idiopathic OAB, however, dose escalation maybe required.
P5-17 Urinary tract infections in the intradetrusor Botox® population
E White, S Ahmed, J Clark, R Walker, T Nitkunan
Epsom and St Helier University Hospitals NHS Trust
Introduction: A significant side effect following intradetrusor Botox® is urinary tract infections (UTI), affecting between 2 – 32% of patients. We investigated the incidence of UTI following intradetrusor Botox® procedures within our trust and reviewed our antibiotic policy of a three day course of Trimethoprim for local anaesthetic procedures.
Methods: Data was collected for Botox® procedures carried out at our trust from 2005 to August 2015. Information was taken from our Botox® database, clinic letters and microbiology results.
Results: There were a total of 290 Botox® procedures, on a population of 86 patients with 20% under local anaesthetic. Idiopathic and neurogenic populations were 70% and 30% respectively. The rate of proven UTI following a procedure was 33% (32% and 34% of idiopathic and neurogenic populations respectively). 42% of those performing self-catheterisation had UTIs compared to 18% of those who were not. 50% of patients never had a proven UTI following their Botox procedure.
Coliform species was the most common organism cultured accounting for 88% of infections. The percentage of all organisms sensitive to Trimethoprim was 43%. The antibiotic agents found to have the highest susceptibility against all isolates were Gentamicin, Nitrofurantoin and Co-amoxiclav, with sensitivities at 87%, 84% and 83% respectively.
Conclusion: Our audit showed a high rate of resistance to Trimethoprim in this intradetrusor Botox® population with an increased risk of UTI with self-catheterisation. Liaising with our microbiologists our policy has now changed to the use of prophylactic oral Co-amoxiclav for local anaesthetic cases.
P5-18 Consistent and durable improvements in quality of life with long-term onabotulinumtoxinA treatment in patients with overactive bladder
CR Chapple, M Drake, D Ginsberg, V Nitti, S Radomski, A Gousse, A Magyar, JP Nicandro, A Kaufmann
Bristol Urological Institute
Introduction: We evaluated the long-term effects of onabotulinumtoxinA 100U on quality of life (QOL) of patients with overactive bladder (OAB) who were inadequately managed by ⩾1 anticholinergic.
Methods: Eligible patients who completed either of two phase 3 trials could enter a 3-year extension study to receive onabotulinumtoxinA treatment ‘as needed’ for control of symptoms. Results are reported for up to 6 treatments. Assessments included change from baseline in Incontinence-QOL (I-QOL) total score and proportions of patients who achieved/exceeded the minimally important difference (MID) in I-QOL score (+10 points) after each treatment. Consistency of response over repeat treatments was evaluated by determining whether patients achieved ⩾MID after the first treatment, and then analysing the proportion who achieved ⩾MID for all subsequent treatments.
Results: Of the 829 patients enrolled, discontinuations due to lack of efficacy/AEs were 5.7%/5.1%. After onabotulinumtoxinA treatments 1-6, QOL improvements were consistently 2-3X MID, with most patients achieving ⩾MID (range: 65.2% to 76.1%). 72.9% of patients who achieved ⩾MID after treatment 1 maintained I-QOL improvements ⩾MID in all subsequent treatments. Over one-third (38.3%) of patients who did not achieve the MID after treatment 1 achieved improvements ⩾MID in all subsequent treatments. No new safety signals were observed.
Conclusion: The consistent improvements in OAB symptoms after long-term treatment with onabotulinumtoxinA corresponded with durable QOL improvements, with no new safety signals. Patients with clinically meaningful QOL improvements after treatment 1 had similar improvements in subsequent treatments, while lack of response to treatment 1 did not preclude positive response(s) in subsequent treatments.
P5-19 Overnight ambulatory urodynamics findings in patients with nocturia and/or nocturnal enuresis
E Solomon, M Duffy, S Malde, M Pakzad, R Hamid, TJ Greenwell, JL Ockrim
Institute of Urology, University College London Hospitals NHS Trust
Introduction: To determine the prevalence of detrusor overactivity in patients with nocturia and nocturnal enuresis during overnight ambulatory urodynamics.
Methods: We reviewed the overnight ambulatory urodynamic studies of 20 patients whose most bothersome symptoms are nocturia and/or nocturnal enuresis that were performed following undiagnostic standard filling cystometry. We documented if detrusor overactivity (DO) +/- leakage was demonstrated, maximum voided volume and nocturnal urine output.
Results: The mean (SD) age for the 14 female and 6 male patients reviewed was 45.1 (19.9) years. All patients had nocturia and 17 patients also had nocturnal enuresis. Only 5 patients reported bothersome daytime frequency. DO was demonstrated in 80% (n=16) of patients. 15 of 17 (88.3%) patients demonstrated DO and small volume SUI in 4 of 17 (23.5%) patients. The mean and median peak DO pressure was 68.3 (+/-50.9) and 50 cmH2O. No significant difference in maximum voided volume and nocturnal urine output between the two DO groups was noted (Nb: small sample DO–ve patients). Incontinence was observed in 15 of 16 (93%) patients with DO. (P5-19)
DO demonstrated
n
DO peak pressure (cmH20)
Max voided volume (ml)
Nocturnal urine output (ml)
No
4
−
157.1 + 50.7
603.4 + 53.5
Yes
16
68.3 + 50.9
363.4 + 236.3
575.8 + 397
Total = 20
Conclusion: 80.0% of patients presenting with nocturia and 88% with nocturnal enuresis demonstrate detrusor overactivity on overnight ambulatory urodynamics tests. The DO pressures demonstrated are typically large amplitude and result in incontinence by overcoming in most case an otherwise competent outlet.
P5-20 The correlation between retrograde leak point pressure and 24-hour pad weight for men with post prostatectomy incontinence
E Solomon, S Malde, M Spilotros, M Pakzad, R Hamid, PJR Shah, TJ Greenwell, JL Ockrim
Institute of Urology, University College London Hospitals NHS Trust
Introduction: To assess the correlation between retrograde leak point pressure (RLPP) and 24-hour pad weight (24PW) in men with post prostatectomy incontinence
Methods: We performed RLPP and 24PW measurements on 61 patients with post-prostatectomy stress urinary incontinence (SUI). We examined the relationship of RLPP and 24PW. We also reviewed the urodynamic and clinical data of these patients to explain our findings.
Results: The mean age was 69.5 years (SD + 7.4, range: 51-87). The mean RLPP was 36.8 cmH2O (SD +/- 15.3, range: 9-76), the mean 24h pad-weight was 499g (+ 677g, range: 16.5g-3177g). There was a strong and significant negative correlation between RLPP and 24h pad-weight (r=0.56, p<0.0001). RLPP was a strong predictor of cases of mild/moderate (<400g) and severe (>400g) incontinence (Figure 1). Patients with RLPP ⩽ 30 had significantly higher 24h pad weight (mean 825g, median 768g) when compared with patients with RLPP > 30 (mean 257.8g, median 100g), p < 0.0001.
Conclusions: There is a good correlation between RLPP and 24PW. RLPP can distinguish between mild/moderate and severe levels of incontinence. RLPP could be used as an objective and more reliable substitute to pad weight to objectify and stratify SUI in post-prostatectomy patients. (P5-20)
Boxplot showing that patients with severe incontinence had statistically significantly lower RLPP than patient with mild or moderate incontinence.
Wednesday 29 June 1030-1200 Room 12 ePoster Session 6 – Renal and Testis Cancer: Organ Sparing and Reducing Morbidity Chairs: Axel Bex and Maxine Tran
P6-1 Significance of negative margin in nephron sparing nephrectomy and its implications on disease free survival
A Shafik, A Kodera, T King, N Hicks, T Chen, A Makar
Worcester Royal Hospital
Introduction & Objectives: We present long term oncological outcomes of nephron sparing surgery over a period of 11 years and 10 months. Our study focuses on the impact of surgical margin on disease recurrence with a mean follow up of 8.5 years.
Method: A total of 162 patients underwent either open (146) or laparoscopic (16) partial nephrectomy in the period from November 2003 till September 2015 at a UK District General Hospital. Data was retrieved from a prospectively maintained data base.
Results: A total of 162 patients were identified, of these 146 had an open partial nephrectomy and 16 had laparoscopic surgery. Post-operative histology revealed renal cell carcinoma in 119 cases (73.4%), with the remaining cases having benign histopathology. Of the malignant cases, pathological staging was PT1a in 75 cases (46.2%), PT1b in 32 cases (19.7%), PT2 in 2 cases (1.2%), PT3a in 9 cases (5.4%) and PT3b in one case (0.6%).
In 10 cases (6%) there were positive surgical margins. This subgroup had a mean follow-up of 7 year, 8 months over which there were no cases of recurrence. Recurrence did occur in 3 cases (1.8%), 2 of which were local recurrences requiring radical nephrectomy and one of which developed metastatic disease that required systemic therapy. Median post-operative follow-up was 8.5 years.
Conclusions: Our study demonstrates no correlation between positive surgical margin and local recurrence. A negative margin did not preclude future local recurrences. 8.5 years follow up demonstrates a low rate of recurrence following partial nephrectomy for localized renal tumours.
P6-2 A century in laparoscopic zero-ischaemia partial nephrectomy in the UK
RH Gray, AS Fernando, P Grange, G Kooiman
Kings College Hospital
Introduction: Partial nephrectomy is now the gold-standard surgical intervention for the management of small renal masses. Minimally invasive surgery has been shown to improve length of stay and reduce post-operative pain but remains a complex procedure to perform laparoscopically.
Patients (or Materials) and Methods: 100 patients underwent laparoscopic partial nephrectomy between February 2009 and January 2016 at our institution by a single surgeon. We present our current technique in video format and the results from the first 100 patients. The attached video demonstrates port placement, dissection and zero ischaemia extraction utilising the Harmonic ACE scalpel.
Results: The median operative time for the first 50 cases was 270 mins, and 210 mins for the latter cases. The overall transfusion rate was 2% and median length of stay of 4 days (3 days for the last 50 cases), this is favourable with respect to published series. The renal resection was performed without ischaemia and a median fall in eGFR was 4mL/min pre and post-operatively and is consistent with an excellent functional outcome. The oncological outcomes were excellent with only 5% positive margins reported. Histology was malignant in 87% of cases.
Conclusions: We report the technique and results for 100 cases of zero-ischaemia laparoscopic partial nephrectomy; a safe technique with an excellent safety profile and oncological outcome.
P6-3 Extending indications in robotic partial nephrectomy: the development of the practice after 200 cases
F Al-khalidi, W Lam, J Dargan, G Blecher, R Catterwell, S Van Rij, B Challacombe
Guy’s Hospital
Introduction: Robotic partial nephrectomy (RPN) is becoming the gold standard technique in the surgical management of small renal masses. Here we assess development of RPN within one centre over 5 years to assess quality outcomes and changes in case complexity.
Patients and Methods: A prospective database of 200 elective cases from one institution was chronologically split into 4 groups of 50 patients: peri-, intra- and post-operative outcomes were compared. We compared length of stay, tumour size, warm ischaemic time (WIT), operative time and PADUA score.
Result: 181 cases were performed transperitoneally with 4 conversions to radical nephrectomy for tumour factors. There were no conversions to open surgery. Mean age was 55.8 years. Complications consisted of 1 transfusion, 5 positive margins and 3 Clavien IIIa/b complications.
In comparing groups 1 and 4, mean PADUA score increased from 7.11 to 7.63 (p=0.045), mean length of stay decreased from 3.76 to 2.6 days (p<0.001), mean WIT decreased from 18.3 to 16.4 minutes (p=0.0245), mean operative time decreased from 180 to 162 minutes (p=0.012). We also found a non-significant mean increase in tumour size of 2.8 to 3.32cm (p=0.06). More patients with single kidneys and poor renal function were undertaken in group 4.
Conclusion: We report the largest RPN series in the UK. We demonstrate that despite taking on more complex cases, we have reduced length of stay, WIT and operative times. Here we conclude that with increased experience it is possible to broaden the suitability of patients for RPN without compromising outcomes.
P6-4 Robotic versus laparoscopic nephrectomy from a single centre: are we comparing apples with oranges?
W Lam, M Chakravorty, T Malthouse, J Dargan, A Kadirvelarasan, N Doeuk, B Challacombe
Guy’s and St Thomas’ NHS Foundation Trust
Introduction: Laparoscopic nephrectomy (LN) is the standard approach for localised renal tumours or simple nephrectomy. The role of robotic-assisted nephrectomy (RN) is yet to be determined. We compared surgical outcomes of RN with LN.
Patients and Methods: Data was collected retrospectively in patients undergoing LN and RN (April 2011-June 2015). 179 patients underwent minimally-invasive nephrectomy. 79(44%) had RAN and 100(56%) LN. Patient’s ASA grade, tumour size, stage, BMI, length of stay (LOS), additional procedures and complications were compared. Comparative analyses were performed using Mann-Whitney-U test and Chi-squared test.
Results: 89% of RN and 62% of LN were performed for cancer. RN had a significantly higher ASA (p<0.05) with higher stage and tumour size (6.9 vs 5.9 cm). 46% of RN malignant tumours were stage ⩾T2b (1 requiring caval thrombus resection, 2 renal vein invasion, 2 IVC repairs, 2 splenectomies, 1 BMI >70, 5 retroperitoneal lymphadenectomies) compared with 32% in the LN cohort. There was an increased LOS, median 4 vs. 3 days (p<0.05) in the RN cohort, likely due to higher ASA. 1 LN required open-conversion, with none for RN. No significant differences in pre & post-op Hb, eGFR, operating time, EBL or Clavien-Dindo complications (2 vs 3 grade III/IV) were identified.
Conclusions: Surgical outcomes of RN and LN are comparable despite more challenging, larger tumours and co-morbid patients in the RN group. RN may provide the surgeon with greater ability to attempt more difficult and higher stage cases and manage intra-operative complications that may otherwise lead to open-conversion.
P6-5 Length of stay and supported discharge following laparoscopic nephrectomy: Experiences of a regional cancer centre
FG Ghumman, S Nazad, F Kum, MKM Sheriff
Medway NHS Trust
Introduction: Laparoscopic Nephrectomy (LN) is the gold standard treatment of renal tumours stage 2 and below. LN can be performed via a transperitoneal or retroperitoneal approach, depending on tumour characteristics and surgeon preference. Previous research indicates that the retroperitoneal approach is associated with shorter post-operative length of stay (LOS). Supported early discharge is found to decrease LOS following stroke and orthopaedic operations. Studies assessing supported discharge following LN are lacking.
Patients & Methods: 117 patients underwent LN for a T1, T2 or T3a tumour at a single centre between August 2013 and October 2014. Cases were grouped by surgical approach and LOS assessed. Cases in which there was conversion to laparotomy; procedure aborted; or operation sufficiently complicated which required a post-operative stay in intensive care, were excluded.
Results: 77 patients were included for analysis. Mean age was 64.7 (Range 37-88). There were no differences in demograpics or tumour stage between groups.
Mean LOS was significantly shorter after transperitoneal LN, 2.24 days (n=54; 95% CI 1.98-2.50), than after retroperitoneal LN, 3.00 days (n=23; 95% CI 2.45-3.55), P=0.0068. No patients in the retroperitoneal group received early supported discharge, while majority of the patients in the Transperitoneal group did.
Conclusions: In contrast to previously published research, LOS was significantly shorter following transperitoneal LN versus the retroperitoneal approach. We attribute this difference to use of specialist-nurse supported discharge. Prospective research will be needed to further determine the use of supported discharge following urological surgery and potential benefits of ERAS (enhanced recovery after surgery) programs.
P6-6 The training concept of whole procedure equivalent applied to laparoscopic renal surgery. A single surgeons experience
P Rouse, S Garnett, S Ahmed, P Grange
Eastbourne District General Hospital
Introduction: The concept of “whole procedure equivalent” addresses two main surgical training challenges: specialty training in laparoscopic surgery and service delivery. Renal laparoscopic surgery can be broken down into standardised steps: Patient Positioning, Port Placement, Colon Mobilization, Renal Hilium Dissection, Renal Dissection, Specimen Removal and Closure. We report on how this non-sequential concept of modular training can be applied to training in renal laparoscopic surgery.
Materials and Method: After feedback, the trainee surgeon recorded his performance of each step in every case, in a training spreadsheet. Patient demographics and other standard operative parameters were recorded. A colour code of performance was used:
Blue when the trainee was in an assistant role
Yellow when a step was completed under active or pro-active supervision
Green when a step was completed with passive supervision (NO INPUT needed by the supervising trainer)
A simple sum formula was used to assess how many times the trainee had completed the individual steps.
Results: The operative time (average 170 minutes), estimated blood loss (median <250mls), intra- and post-operative complication rate (No Clavien grade ⩾ 3 complications) and hospital stay (median four days) were within the ranges of the published literature. After 30 procedures, the trainee has performed a large number of steps and has competently performed twelve procedures with passive supervision, including 4 moderate-difficult cases (including radical resection of two tumours ⩾10 cms).
Conclusion: The advantage of this modular non-sequential method of teaching/learning is that competent training can be achieved within the constraints of NHS service provision.
P6-7 How does ureteroscopy prior to nephroureterectomy impact on the patient pathway and oncologic outcomes in a UK tertiary referral centre?
A Pai, R Hilbert, A Ali, N Barber
Frimley Park Hospital
Introduction: The aggressive nature of upper tract urothelial cancer (UTUC) means that prompt treatment is required to minimise the risk of cancer progression. The role of ureteroscopy prior to nephroureterectomy is controversial. The aim of our study is to assess the impact of ureteroscopy on the patient pathway and oncologic outcomes.
Methods: A single centre prospective study of 100 patients who underwent nephroureterectomy for UTUC over a 9 year period. Patients were divided into those who had nephroureterectomy based on imaging/cytology alone and those who had prior ureteroscopy. Patients who had attempts at endoscopic control of UTUC were excluded.
Results: 45 patients had ureteroscopy or attempted ureteroscopy prior to nephroureterectomy and 55 patients had nephroureterectomy based on imaging alone. Mean follow up was 40 months. In the ureteroscopy group, the mean time from ureteroscopy to nephroureterectomy was 49 days. 5 year cancer specific survival (CSS) was 64% for the ureteroscopy group and 79% for the non-ureteroscopy group. There was no significant difference in the intravesical recurrence rate between the two groups. On multi-variate analysis, pre-nephroureterectomy ureteroscopy was independantly associated with CSS.
Conclusions: Ureteroscopy prior to nephroureterectomy adversely affects oncologic outcomes and should be reserved for those cases with diagnostic uncertainty. In those cases where ureteroscopy is required prior to nephroureterectomy it is imperative that cancer pathways are designed to minimise delay.
P6-8 Robotic assisted nephroureterectomy for upper urinary tract urothelial carcinoma: A large single centre UK experience
A Pai, M Hussain, A Ali, R Hilbert, G Mueller, A Emara, N Barber
Frimley Park Hospital
Introduction: Published outcomes on robotic-assited nephroureterectomy (RANU) are currently limited. We describe our institutions experience of RANU employing a closed technique with full bladder cuff excision.
Methods: A 5 year prospective study of 69 patients undergoing RANU. All cases were performed with 2 docking positions, employing a transperitoneal technique, allowing a cuff of bladder mucosa to be excised with the ureter by placing 2 transfixion sutures distal to the line of division; thus keeping the urinary system closed throughout the procedure.
Results: Median age was 69. Median operative time was 210 minutes (Inter-Quartile Range 190 to 240) with median blood loss of 50ml. The median period ofurinary catheterisation was 1 day (IQR 1-3) with a median in-patient stay of 2 days (IQR 2-4). There was one open conversion. Two patients had Clavien Grade 3b complications (splenectomy and laparotomy for hernia).
61 patients had transitional cell carcinoma. 33 patients had high grade disease. There were four positive margins. Median follow-up was 21 months. Six intravesical recurrences occurred at a median of eleven months. 2 year overall survival was 74%. 2 year cancer specific survival was 100% for patients with pta (n=15) and pt1 (n=14) disease, 58% in pT2 (n=10) and 47% in pT3 (n=21) disease.
Conclusions: RANU using a 2 dock technique, which keeps the urinary system closed at all times, achieves acceptable early oncological outcomes with reasonable operative time, low morbidity and rapid, secure removal of the urinary catheter, allowing patients to be discharged home quickly and catheter free.
P6-9 Practice and outcomes in the endoscopic management of upper tract TCC – initial results from the BAUS Registry
JM Withington
Whittington Hospital
Introduction: The British Association of Urological Surgeons (BAUS) has undertaken to monitor UK endoscopic management of UTTCC in a perpetual prospective registry.
Patients and Methods: BAUS invited online data submission from March 2011, including previously collected local data. All patients undergoing endoscopic management of UTTCC at a UK centre were eligible. Data were cross-referenced with the BAUS nephrectomy audit to check nephroureterectomy (NU) rates.
Results: From March 2011 to February 2015, 374 procedures were recorded, for 106 patients Mean age at first procedure was 71.4 (35-90). Mean follow-up was 10.3 months (0-113m).
WHO performance status was 0 in 35 patients, 1 in 31, 2 in 30 and 3 in 9. 17 had moderate to severe CKD; 23 had a solitary kidney. 38 patients (36%) had an imperative indication for endoscopic management.
Conclusions: While no grade-dependent trend in recurrence is observable, failure of endoscopic management (NU, disease specific mortality) is proportionately higher in G3.
These initial results demonstrate the feasibility of using national registries to collate evidence in this challenging area. As follow-up duration matures, these data have the potential to inform best practice.
(P6-9 Table 1) Summary of outcomes by WHO(1973) Grade.
Grade
G1
G2
G3
Unknown
Combined
Total
27
35
13
31
106
Upper Tract Recurrence
9 (39%)
16 (52%)
3 (20%)
11 (35%)
39 (37%)
NU
4 (15%)
4 (11%)
4 (31%)
9 (29%)
21 (20%)
Time to NU (months)
53
2.1
1.8
−
17.8
Disease-specific survival
27 (100%)
35 (100%)
12 (93%)
31 (100%)
105 (99.1%)
Grade Progression
2 (7%)
0
0
N/A
2 (1.9%)
P6-10 Acute toxicity data from POUT: a phase III randomised trial of peri-operative chemotherapy versus surveillance in upper tract urothelial cancer
AJ Birtle, L Maynard, M Johnson, R Kockelbergh, R Jones, J Chester, J Catto, A Blacker, E Hall, On behalf of the POUT TMG
Rosemere Cancer Centre
Introduction: The POUT randomised trial compares immediate chemotherapy with surveillance following nephroureterectomy (CRUK/11/027). The primary endpoint is disease free survival. Secondary endpoints include acute toxicity.
Patients and Methods: Recruitment commenced 31/05/2015 and is ongoing. Patients are randomised (1:1) following nephroureterectomy to either 4 cycles of gemcitabine-cisplatin (or gemcitabine-carboplatin if GFR 30-49ml/min) or surveillance with subsequent chemotherapy if required. Acute safety assessments (CTCAEv4) are conducted pre-randomisation, pre-cycle 1,2,3,4, and after cycle 4 (equivalent timepoints for surveillance patients).
Results: Acute toxicity data are available for an initial cohort of 129 patients: median age: 68.9 (IQR 62.4, 75.0); stage: 28.7% pT2, 65.1% pT3, 6.2% pT4; baseline WHO performance status 57.4% 0, 34.9% 1, 0.8% 2, 7.0% missing; baseline median (IQR) GFR: 55 (44, 67). Gemcitabine-cisplatin was planned for 64.3% patients (median (IQR) GFR: 64 (55, 72)), gemcitabine-carboplatin for 35.7% (median (IQR) GFR: 43 (39, 46)).
To date, 46.8% (29/62) chemotherapy and 22.4% (15/67) surveillance patients had ⩾1 grade 3-4 acute toxicity (p=0.005). Grade 3-4 haematological toxicity occurred in 29.0% (18/62) chemotherapy patients and 0% (0/67) surveillance patients, with a peak at pre-cycle 2. The commonest haematological toxicities were neutropaenia (22.6% chemotherapy; 0% surveillance) and low platelet counts (9.7% chemotherapy, 0% surveillance); febrile neutropenia was reported by 3.2% chemotherapy and 0% surveillance patients. The commonest grade 3-4 non-haematological toxicity was hypertension (1.6% chemotherapy, 6.0% surveillance).
Conclusions: Whilst toxicity rates are higher with chemotherapy than surveillance, they are lower than anticipated in this population.
P6-11 The surgical management of complex bilateral renal cancer - are we getting it right?
N Lobo, E Anastasiadis, A Fernando, TS O’Brien
Guy’s Hospital
Introduction: Patients with localized bilateral renal masses present a unique treatment challenge. Optimal strategies for achieving oncological control with maximal renal functional preservation are debated. We report our experience of managing patients undergoing surgery for bilateral renal masses.
Patients and Methods: A retrospective review of patients with bilateral renal masses undergoing surgery between 2005-2015 at our institution. Oncological and renal functional outcomes are reported.
Result: Mean follow-up was 36 months (range 2-121 months).
50 operations were performed in 29 patients. 4/29 (14%) had Von Hippel-Lindau.
11/29 (40%) underwent bilateral partial nephrectomy (10 staged procedures, 1 simultaneous). 9/29 (31%) underwent radical nephrectomy and partial nephrectomy (5 staged, 4 simultaneous). The remainder underwent partial nephrectomy followed by surveillance (7/29; 24%) or radiofrequency ablation (2/29; 7%).
Mean of 2 tumours excised (range 1-10). Mean tumour size was 36mm (range 7- 185mm).
The most common histological finding was clear cell carcinoma in 27/50 (54%) cases, followed by papillary carcinoma in 12/50 (24%), and oncocytoma in 8/50 (16%).
10/29 (34%) had bilateral clear cell tumours; of these, none had recurrence.
Post-operatively, median loss of GFR was 18ml/min/1.73m2 (range -4 to-32). No patients required dialysis or transplantation.
Recurrence was seen in 1 patient. 1 patient developed metastases, constituting the only death from RCC in the cohort.
Conclusion: In our experience, patients with bilateral renal cancer undergoing either partial nephrectomy or radical with partial nephrectomy have excellent oncologic and functional outcomes. However, several patients underwent surgery for benign disease, thus emphasising the need for pre-operative biopsy.
P6-12 How we manage small intratesticular lesions - A single centre experience
EWY Lee, K Biddle, F Chaudhry, F Douglas, N Kardaman, BC Thomas
Cambridge University Hospitals NHS Foundation Trust
Introduction: Small testicular lesions can pose a diagnostic challenge and controversy over their management exists. We therefore evaluated the management of small testicular lesions over a 12 month period at our institute.
Patients and Methods: Retrospective analysis of all patients who underwent a scrotal ultrasound at a single institution was performed over a consecutive 12 month period. Patients found to have a testicular mass were identified and those with a solid intratesticular mass measuring 5-10mm had their case notes reviewed to determine the management and outcomes of these masses. Exclusion criteria included cystic masses, tubal ectasia, testicular calcifications and previous history of testicular cancer.
Results: 1453 scrotal ultrasound scans were performed over the 12 month period. 184 ultrasound scans revealed an intratesticular mass <10mm in size. 14 patients met the inclusion criteria. Radical orchidectomy was performed in 6 patients, surveillance performed in 6 patients with follow up ultrasounds and 2 patients were discharged with no follow up. The pathology in 4 out of 6 patients (67%) who underwent orchidectomy revealed tumour. None of the surveillance scans resulted in patients having an orchidectomy.
Conclusions: Small solid intratesticular masses <10mm in the majority of patients (71%) did not result in a diagnosis of testicular cancer. Interval ultrasound maybe a useful adjunct to determine further management of indeterminate lesions. Larger studies are required to support these findings.
Introduction: We undertook a preliminary evaluation of MI-RPLND (robotic/laparoscopic) as a potential alternative to current standard therapy for clinical stage 2a seminoma.
Patients and Methods: Patients were identified from weekly case discussion meetings of our supraregional testicular cancer network. Cases with clinically suspected low volume stage 2a seminoma were offered MI-RPLND (robotic or laparoscopic) based on isolated or equivocal nodal enlargement on imaging. A unilateral template dissection based on site of the involved nodes.
Results: From Jan 2013 - Dec 2015 11 patients underwent MI-RPLND for clinical stage 2a seminoma with equivocal or isolated nodal disease <3cm. These comprised 8 with lymph node enlargement at /<6 months from presentation and 3 with late relapse or persistent lymph node enlargement 18-66 months after diagnosis. In all cases blood loss was <50mls with an average 2 day hospital stay. An ileus, which was managed conservatively, was the only post-operative complication. Final pathology demonstrated pN0 in 2 cases with non-specific inflammatory changes in the enlarged nodes. The remaining 8 had pN1 or pN2 disease. In one case embryonal carcinoma was present in the involved node who opted for adjuvant BEPx2 rather than surveillance. The other 8 cases received single agent adjuvant carboplatin. Follow-up ranges 2-34 months (mean/median 18 months) with no recurrences or late surgical complications to date.
Conclusions: Our initial experience suggests that MI-RPLND may be a potential treatment option, as an alternative to radiotherapy or multiagent chemotherapy, in selected cases of clinical Stage 2a seminoma that warrants ongoing evaluation.
P6-14 Cryoablation outcomes for small renal masses: 2004-2015
P Brousil, W Lam, G Ibe, G Munneke, M Gonsalves, U Patel, S Sandhu, P Le Roux, C Anderson
St Georges’ Hospital
Introduction: Cryoablation is an established treatment for the management of small renal masses (SRM), particularly in the comorbid patient. We present long term follow up data from a single centre series.
Methods: A prospective cryoablation database from a single centre was conducted between 2004 to the present day. Demographics, tumour characteristics, treatment failures (tumour progression within an ablated lesion) and response to retreatment were evaluated. Exclusion criteria: patients without surveillance imaging.
Results: 96 cases were identified. 4 cases were excluded. The mean age was 69 years with a median Charleston score of 5. The mean tumour size was 2.8cm with a median PADUA score of 8. Mean follow-up time was 3 years. Cryoablation was performed laparoscopically in 48 cases (78% of which comprise the first 50 cases) vs 44 cases percutaneously. Clavien-Dindo classification grade 3 complications were 2% (none higher). Post-operative renal function was seen unchanged in 99%.
Overall treatment failure occurred in 12 patients (13%). 8 patients had just one failure (9%) whilst 4% had 1-2 treatment failures of the same lesion. 1 patient with intraoperative bleeding required conversion to partial nephrectomy. In the overall treatment failure group the mean tumour size was 3.0 cm and PADUA score was 8.0.
Conclusion: This large series demonstrates that cryoablation is an effective low risk treatment option for small renal masses and is feasible in co-morbid patients. Retreatment is feasible in patients with initial treatment failures. Our service has evolved to delivering this therapy percutaneously, with success.
P6-15 Is it safe to leave a renal biopsy proven oncocytoma alone? An observational cohort study
M Moghul, BP Rai, A Abroaf, M Hosny, S Agarwal, P Nathan, T Lane, D Hanbury, N Vasdev, J Adshead
Lister Hospital
Introduction: Oncocytomas and chromophobe renal cell carcinomas, particularly eosinophillic variants, share clinical, histological and radiological similarities.
Patients and Methods: We retrospectively reviewed our histological database for patients who had renal biopsies for suspected oncocytoma or chromophobe RCC between 2011 and 2015. We evaluated histological concordance rates between renal biopsy and partial nephrectomy specimens and also present the follow-up of renal biopsy proven oncoctyoma patients who did not proceed to surgical intervention.
Results: 16 renal biopsies were performed. The mean age was 71 years (range 53-87 years, SD +/- 8 years). The male to female ratio was 3:1. The mean tumour size on cross-sectional imaging was 28.6mm (range 13-60mm, SD +/- 12.5mm). The histological diagnoses were oncocytoma (10), chromophobe RCC (4), oncocytic papillary carcinoma (1), possible malignancy (1). Five patients were suitable for surgical treatment. Four of these patients had partial nephrectomies and one had cryoablation. One patient had metastatic disease and died before commencing treatment. The histological concordance between renal biopsies and nephrectomy specimens was 100%. Ten patients with biopsy proven oncocytomas were followed with surveillance imaging. The median follow up of these patients was 27 months (range 6-57 months). All of these patients continue to be asymptomatic. None of these patients have required re-biopsy or surgical intervention.
Conclusions: This study would suggest that active surveillance of renal biopsy proven oncocytoma in the short term may be safe. However larger studies with longer follow up are still required.
P6-16 The small renal mass – changing the treatment paradigm
X Cheng, I Ioannidis, M Tran, F Mumtaz, G Webster, M Al-Akraa, S El-Sheik, A Goode, M Aitchison,S Tadtayev
The Royal Free Hospital
Introduction: Incidentally discovered small renal masses (SRM<4cm) are the commonest mode of presentation of renal cancer. Pre-operative renal biopsy is not routinely utilised. Increasing accuracy and safety of biopsy led us to change our policy to offer renal biopsy to those considered for surgery with the objective of determining whether this changed the treatment decision.
Materials and methods: Between October 2014-September 2015. 113 patients with SRMs who were fit for surgery were offered initial biopsy. All cases were reviewed at our specialist MDT (sMDT). Ultrasound/CT guided biopsy was used depending on which modality offered optimal visualisation of the SRM. The biopsies were reported by a specialist uro-pathologist and discussed at sMDT prior to discussion with patients.
Results: The diagnostic biopsy rates by size of tumour, and the benign vs malignant histology by age group are shown in Tables 1&2. There was a 3.8% complication rate (all < Clavien IIIa).
(P6-16 Table 1)
Size (cm)
Initial diagnostic rate
Final diagnostic rate
0 - 1.5
62.50%
87.50%
1.6 - 2.0
83%
92%
2.0 - 3.0
76%
90%
3.0 - 4.0
75%
90%
(P6-16 Table 2)
Age (years)
Benign (%)
Malignant (%)
<45
30%
70%
46 - 55
13%
87%
56 - 65
17%
83%
66 - 75
21%
79%
76+
42%
58%
In terms of treatment decision 62 (55%) patients did not undergo RALPN. 23 patients (20%) with benign disease, 39 with low grade tumours of whom 25 opted for cryotherapy and 14 for surveillance.
Conclusions: Pre-operative biopsy of small renal masses informs patient treatment choice and with a high incidence of benign lesions in the younger and elderly groups allows surgical intervention to be avoided in a significant proportion of cases.
P6-17 The role of biopsy in the management of small renal masses
CR Jelley, H Bardgett, R Singh, SK Addla
Bradford Royal Infirmary
Introduction: Percutaneous renal biopsy is accurate at diagnosing renal cell cancer with a sensitivity of 86-100%. However, with improvements in imaging and the development of new minimally invasive surgical interventions, its role in the management of small renal masses (SRM) has been questioned. We had routinely biopsied SRM until 2014 when we changed our protocol to be in line with new EAU guidelines, offering biopsy only for indeterminate SRM and surveillance patients. We assessed the impact of this new protocol on patient’s outcomes following NSS.
Methods: From 2009 to 2015 151 patients had nephron sparing surgery (NSS). The change in protocol coincided with the introduction of robotic assisted NSS at our centre. Prior to 2014 78 NSS were done; the majority were performed open except for 2 which were robotic assisted. Since the beginning of 2014 73 patients have had NSS of which 68 were robotic assisted.
Results: 51% of patients before 2014 had a biopsy pre-operatively compared to 10% after 2014. Pathological benign histology was found following NSS in 14% of the pre-2014 group and 18% of the post-2014 group. However, further analysis of this cohort showed only 3% (2 patients) would have had a change in management if all patients were subjected to biopsy.
Conclusions: A change in the protocol of limiting the usage of renal biopsy has not lead to a significant increase in benign histology following NSS. This audit provides evidence that the new EAU guideline is effective in clinical practice.
P6-18 Radical nephrectomy and nephroureterectomy practice in the United Kingdom: BAUS Data (2012-2014) Analysis- trends in blood transfusion rate and complications
U Mufti, V Hanchanale, S Fowler, F Keeley, CS Biyani, S Jain
St James University Hospital
Background: Since 2012, all urologists in the UK have submitted data on nephrectomy to the national audit British Association of Urological Surgeons (BAUS) database. In the current practice, the majority of surgeons doing a radical nephrectomy (RN) also perform nephroureterectomy (NU).
Methods: The BAUS database was interrogated to gain an insight into RN and NU practice. Short-term outcomes (transfusion-rate, complications, hospital-stay) were assessed and statistical analysis (Chi-square test) was performed to compare the outcomes during these 3 years.
Results: Over 36 months, 2704 NU and 9668 RN were performed. There was a gradual increase in the number of RNs (10-20%) but the numbers of NUs were static in the last 2 years. Over three year period, transfusion rates were significantly reduced for RN (p=0.005), but similar trend was not seen for NU. There was no difference in the complication rate between RN and NU over the study period. The median number NUs performed by each surgeon was 3 cases compared to 9 cases for RN.
Conclusion: This study highlights that NU is a low-volume procedure as compared to RN. There was a trend towards reduced transfusion and low complications over time for RN during the study period, but a similar trend was not seen for NU. We could speculate this is due to a low-case volume for NU compared to RN, increased age and complexity of patients may also play a part. Further study to assess the volume-outcome relationship for NU is planned.
RN
NU
Year (n)
2012 (2711)
2013 (3400)
2014 (3557)
Chi-Square (p-Value)
2012 (775)
2013 (985)
2014 (944)
Chi-Square (p Value)
Transfusion, n (%)
301 (11.1%)
362 (10.65%)
314 (8.83)
x2=10.46 (p=0.005)
65 (8.38%)
66 (6.7%)
60 (6.36%)
x2=2.98 (p=0.22)
In-hospital complications, n (%)
498 (17.16%)
604 (16.51%)
618 (16.04%)
x2=1.52 (p<0.47)
164 (19.74%)
220 (20.50%)
199 (19.40)
x2=0.56 (p=0.75)
Complications (Grade 3+ Clavien-Dindo), n (%)
89 (3.07%)
112 (3.06%)
101 (2.62%)
x2=1.70 (p=0.42)
34 (4.09%)
50 (4.66%)
44 (4.29%)
x2=0.38 (p=0.82)
Median-Hospital-stay, days
4
4
4
NS
5
5
5
NS
Median-Age, years
65
66
65
NS
72
71
71
NS
Procedures/year/consultant, Median, n
8
9
10
NS
3
3
3
NS
Wednesday 29 June 1330-1445 Room 3A/B ePoster Session 7 – Surgical Andrology (Urethral and Penile) and Infertility Chairs: Tim Terry and Vaibhav Modgil
P7-1 Augmented non-transecting urethroplasty for bulbar urethral strictures
S Bugeja, S Ivaz, A Frost, DE Andrich, AR Mundy
University College London Hospital
Introduction: We describe the augmented non-transecting technique (ANTABU) using oral mucosal graft (OMG) for long non-traumatic bulbar strictures with a short obliterative segment.
Patients and Methods: 26 ANTABU for idiopathic bulbar strictures were performed in a single unit. Through a dorsal stricturotomy, spongiofibrosis in the obliterative segment was excised in a non-transecting fashion leaving the ventral spongiosum intact and anastomosing the mucosal edges to reconstitute the urethral plate. The entire stricturotomy was then augmented with OMG. Patients were followed up objectively (urethrogram; flow-rate) and subjectively (PROMS) for a mean of 19.2 months (range 6-37 months).
Results: Mean stricture length was 5.3cm (range 3–8cm); Mean length of obliterative spongiofibrosis excised in a non-transecting manner was 1.2cm (range 0.5–2cm). OMG was harvested from the cheek in 22 (84.6%) patients and sublingually in the remaining 4 (15.4%). None of the 26 patients had radiological evidence of stricture recurrence. Mean flow-rate of the cohort postoperatively was 26.6ml/s. 19 of 20 patients (95%) reported that they were satisfied or very satisfied with the surgical outcome. 7 patients (26.9%) reported post-micturition dribble which was not bothersome. Erectile dysfunction lasting longer than 6 months and requiring treatment was reported in 1 patient (3.8%).
Conclusion: ANTABU allows excision of the narrowest segment of a longer bulbar stricture, reconstituting the urethral plate to a wider calibre, avoiding an almost circumferential substitution (which is associated with suboptimal results) in this area. This also permits use of narrower and shorter oral grafts, reducing donor site morbidity. The technique is associated with excellent objective and subjective outcomes.
P7-2 Full-length urethral stricture disease secondary to Lichen Sclerosis: long-term outcomes of urethroplasty
NE Boxall, A Mangera, RD Inman, CR Chapple
Royal Hallamshire Hospital
Introduction: Urethral strictures secondary to Lichen Sclerosis (LS) are difficult to manage and cause significant obstructive symptoms. Surgical options include perineal urethrostomy and full-length urethroplasty.
This study aims to evaluate the long-term outcomes of urethroplasty as a surgical option for treating full-length urethral strictures.
Methods: All patients with full-length anterior urethral strictures due to LS who underwent urethroplasty prior to 2008 (ensuring at least six years follow-up) were retrospectively analysed. All patients underwent a one-stage dorsal onlay technique for the bulbar urethra and a two-stage technique for the penile urethra. Buccal mucosa grafts were used.
Results: 25 cases were identified, three of which were lost to long-term follow-up. At mean 110 months follow-up (range 72-213), 60% are voiding freely with no endoscopic recurrence. Complications (detailed in
Table 1
) occurred between 15-96 months post-operatively. Of these, 22% underwent dilatation and are now self-dilating and 18% underwent major revision surgery (re-do urethroplasty or perineal urethrostomy).
Conclusion: Full-length urethral strictures secondary to LS are difficult to manage. The overall long-term success rate of urethroplasty (defined as ‘no further intervention post-urethroplasty’) is 60% with 82% avoiding major revision surgery. As LS is potentially progressive, long-term careful endoscopic surveillance is required.
(P7-2 Table 1) Outcomes and complications of full-length urethroplasty for LS.
Complication 1st stage- n=25
Graft contracture
3
Meatal stricture
3
Graft hypertrophy
1
Complications 2nd stage- n=25
Urethral fistula
3
Re-Stricture
7
Diaphragm
2
Final outcomes (>6years follow-up)n=22
Voiding freely
13
ISD
5
Urethrostomy
1
Re-do Urethroplasty
3
P7-3 Management of sphincter weakness incontinence (SWI) in patients with concomitant bladder neck contractures (BNC) after the treatment of prostate cancer
S Bugeja, S Ivaz, A Frost, DE Andrich, AR Mundy
University College London Hospital
Introduction: This study evaluates outcome after artificial sphincter (AUS) insertion in patients with concomitant BNC managed either endoscopically or by open surgical reconstruction.
Patients and Methods: 157 bulbar AUS (AMS800TM) were implanted over a 6 year period after radical prostatectomy ± radiotherapy. Patients were followed up for a mean of 22.4 months (6-62.9 months) after AUS insertion. 69 of 157 (44%) had concomitant BNC.
Results: BNC were managed endoscopically (transurethral resection or dilatation) in 50 patients (72.5%): 21 had only resections (one attempt n=18; 2 attempts n=3); 22 had dilatations (one attempt n=10; two attempts n=10; 3 attempts n=2). 7 had combinations of resections and dilatations up to a maximum of 5 procedures. 14 of the 50 (28%) performed self-dilatation for a mean of 3 months in addition (only 3 continued self-dilatation after AUS implantation). Only 2 of 50 (4%) required further intervention for recurrent BNC after AUS insertion.
19 (27.5%) patients were managed by transperineal revision of the vesico-urethral anastomosis. These had undergone a median of 4 failed endoscopic procedures (range 0-8). None had recurrent strictures after reconstruction.
40 of 50 (80%) patients managed endoscopically and 17 of 19 (89%) undergoing surgical reconstruction were restored to functional normality (unobstructed and dry).
Conclusion: An AUS can be safely implanted in selected patients with BNC stabilised by endoscopic measures with a very small risk of contracture recurrence once the device is in place with a good functional outcome. Generally, however, contractures which recur after more than 2 endoscopic attempts are best managed (and cured) by open reconstruction prior to AUS insertion.
P7-4 Can filling phase urodynamic parameters predict the success of the bulbar artificial urinary sphincter in treating post-prostatectomy incontinence?
EM Solomon, R Veeterapillay, CK Harding, TJ Greenwell
University College London Hospital
Introduction: To evaluate whether filling phase urodynamic parameters can predict the success of the artificial urinary sphincter (AUS) in treating post-prostatectomy incontinence (PPI).
Patients and Methods: Review of pre-AUS urodynamics in 99 PPI-patients at two tertiary referral centres for detrusor overactivity (DO), peak DO pressure (PDO), capacity and compliance (C). Success was defined as patient reported complete continence or one safety pad. Statistical analysis wasby Mann-Whitney U, Chi-square and binary logistic regression analyses.
Results: 68% of patients had a successful outcome. The mean compliance for the “success” and “failure” group was 112.3ml/cmH2O (+ 119.7) and 34.1ml/cmH2O (+ 36.2) respectively. 55% of ‘failure’ patients demonstrated DO (PDO=36.2+18.2cmH20) whilst only 15% of ‘success’ patients had DO (PDO=15.6+6.3cmH2O). The differences between the two groups in terms of presence of DO, PDO and compliance were statistically significant (all p <0.01) whilst those for cystometric capacity were not.13/18 (72%) patients that had radiotherapy had a poor outcome. In contrast, only 9 (15%) patients in the “success” group had received radiotherapy. These results were used to develop a nomogram for the probability of AUS success.
A nomogram representing the probability of AUS success based on the compliance index C value and PDO.
Conclusion: Compliance and PDO are predictors of outcome following AUS implantation for PPI. We have developed a nomogram that may be used to determine an individualised likelihood of AUS success using the compliance index and PDO from the pre-AUS urodynamics.
P7-5 Validation of a Patient Reported Outcome Measure (PROM) for penile curvature surgery
AE Campbell, D Akiboye, S Mukhtar, M Jackson, N Watkin
Epsom and St Helier University Hospitals NHS Trust
Introduction: The subjective measures of successful penile curvature surgery are poorly defined. This study describes a PROM for baseline and post-operative assessment of patients with Peyronie’s disease (PD).
Methods:
PROM design: Questions were selected following semi-structured interviews with PD patients. A multidisciplinary RAND consensus group of UK andrologists defined the item-specific PROM.
The final construct domains were penile curvature (PC), erectile function (EF), sexual relationships and generic health related quality of life (HRQoL). The draft PROM was piloted until a final version was agreed for this validation study.
Patient group: Over a 3-year period, all consecutive patients being considered for PD surgery were offered the PROM in one specialist centre.
Statistical analysis: Internal consistency was assessed using Cronbach’s a to understand if construct domains reliably measured the same latent variable. Variability and bias was assessed using a Bland Altman plot.
Results: The baseline PROM was self-completed pre-operatively in a test-retest fashion by 46 men. All questions had response rates >85%. Cronbach’s alpha for the penile curvature construct was 0.78 ranging from 0.68 to 0.8 with any single item removed.
Wilcoxon Signed Rank test for the penile curvature construct indicated no significant difference between the test and re-test scores (P<0.62).
Conclusions: The PC questions were answered consistently well. We demonstrated the content validity and reliability of these items. The next step is to validate a PROM containing the most robust items from this analysis. Deployment of the PROM, pre and post-operatively, across healthcare providers will establish its responsiveness, validity and generalisability.
P7-6 Modified protocol using collagenase clostridium histolyticum (CCH) for the treatment of Peyronie’s disease
AM Abdel Raheem, M Capece, G Garaffa, N Christopher, D J Ralph
University College London Hospital
Introduction: This study evaluates the efficacy and safety of collagenase clostridium histolyticum (CCH) (Xiapex®) in the treatment of Peyronie’s disease (PD) at a single centre using a new, NHS friendly, protocol.
Patients and Methods: Thirty patients with PD had treatment with CCH. Patients with active disease, complete plaque calcification or ventral curvature were excluded. The angle of curvature, IIEF and Peyronie’s disease questionnaires (PDQ) were performed at baseline and 4 weeks after every treatment. A total of 3 intra-lesional injections of CCH (0.9mg) were given at 4 weekly intervals, 4 patients requested an additional 3 injections. Patients then used a combination of home modelling and a vacuum device on a daily basis.
Results: So far 16 patients have completed all 3 treatment cycles, 4 of which had a total of 6 cycles. The mean penile curvature was 56° (25°-90°). Overall, 13 patients (81%) had an improvement in curvature with a mean value of 14.6° (0°-40°) or 23.2% from baseline (0°-50%). The end mean curvature was 43° (25°- 75°; p⩽ 0.001). There was a statistically significant improvement in the IIEF intercourse satisfaction and overall satisfaction domains. There were improvements in all 3 PDQ domains that did not reach statistical significance. The 4 patients who had 6 injections continued to have additional curvature improvement, mean 8.75° (0°-30°; p=0.6).
CCH was well tolerated by all with mild penile swelling and bruising in all but no systemic adverse events.
Conclusion: The new shortened protocol using CCH treatment is safe, effective and cost efficient.
P7-7 High flow priapism is associated with high risk of erectile dysfunction and corporal fibrosis
O Kalejaiye, C Fontaine, S Larsen, J Langston, M Walkden, N Christopher, S Minhas, A Muneer, G Garaffa, DJ Ralph
UCL Hospital
Introduction: High-flow priapism is characterised by a prolonged non-painful erection secondary to the formation of an arterial-lacunar fistula usually following perineal blunt trauma. This leads to high arterial blood flow into the lacunar spaces, as the high-resistance elicine arteries are bypassed. The condition is therefore not considered an emergency as blood remains oxygenated and cellular damage is not expected. Current management includes conservative measures or angioembolization of the cavernosal artery.
Methods: Eighteen patients were identified from a prospective database between 2008 and 2015. Diagnosis was based on blood-gas analysis, clinical and radiological findings. Patients were managed either conservatively (n=4) or with superselective angioembolization of the cavernosal artery (n=14). Outcome measures studied were resolution of priapism, number of embolizations and development of erectile dysfunction.
Results: All patients had high flow priapism confirmed on colour penile Doppler studies. Trauma was the causative factor in 72% of cases. In 9 patients (69%) 2 or more embolizations were necessary to achieve persistent detumescence. Erectile dysfunction was reported in 50% of patients. All men managed conservatively developed erectile dysfunction compared with 42% in the group who underwent angioembolization. An MRI scan of the penis was performed in 6 patients and showed the presence of corporal fibrosis in all cases.
Conclusion: Our data suggests that angioembolization has a high success rate in producing detumescence but also that, if not promptly treated, high flow priapism leads to corporal fibrosis and ultimately erectile dysfunction. Therefore a conservative approach should be discouraged and patients should proceed to early angioembolization.
P7-8 Penile prosthesis implantation after female to male total phallic reconstruction: a single-center retrospective analysis on 247 consecutive patients
M Falcone, G Garaffa, A Gillo, A Raheem, M Capece, AN Christopher, DJ Ralph
St. Peter’s Andrology and The Institute of Urology, University College of London Hospital (UCLH)
Aim: to report the outcome of penile prosthesis (PP) implantation in a neophallus in female-to-male transsexuals (FTM).
Material and Methods: Between January 2001 and October 2015, 247 consecutive patients underwent PP implantation as a final stage of total phallic construction. The mean age at the time of the implantation was 38 years [range: 21-69]. Including revision surgery, a total of 328 PP were implanted. All PP were 3 pieces (AMS 700 CX=226, AMS 700 CXR=31, Coloplast Titan=58) and 2 pieces (Ambicor=13) inflatable devices. In 208 patients (63.4%) a single cylinder was implanted while 2 cylinders were fitted in the remainder. In all patients a Dacron envelope was fitted around the proximal and distal aspect of the cylinder(s) to anchor the device to the pubic bone and to prevent apical protrusion.
Results: At present, 133 patients (53.8%) have their original implant still in place, while the remainder needed revision surgery. After the first PP implantation, 21 patients (8.5%) required removal of the device for acute infection and 38 PP (15.4%) were revised for mechanical failure. Causes of mechanical failure were rupture of the cylinder (69%), aneurysm (18.9%) and rupture of the connecting tubing (12.1%). Repositioning of the cylinder(s) or insertion of a second cylinder were necessary in 48 patients (19.4 %). At the multivariate analysis there was no correlation between age, type of phalloplasty, surgeon, number of cylinders, the use of silver impregnated Dacron or antibiotic coating and the risk of infection or mechanical failure. Revision rates were higher in patients with pubic phalloplasty, possibly because this technique of phalloplasty yields poorer cosmetic results (p=0,013). Overall, the 5-years survival rate of the implant was 78%.
Conclusion: Despite the high rate of complication, PP implantation represents the only solution in patients keen to engage in penetrative sex and it yields satisfactory results in the hands of high volume surgeons.
P7-9 The significance of close surgical margins in organ sparing surgery for penile squamous cell cancer
D Sri, A Sujenthiran, W Lam, C Corbishley, BE Ayres, N Watkin
St Georges Hospital
Introduction: Organ sparing surgery (OSS) for penile squamous cell cancer (pSCC) is established. A 5mm margin has previously been considered oncologically safe. This study evaluates the significance of close surgical margins in OSS and clinico-pathological factors that may influence local recurrence.
Patients: Analysis was carried out on an on-going prospective database, which includes accurate recording of surgical margins. Between March 2001 and September 2012, 332 patients treated with OSS for pSCC had clear surgical margins. Local recurrence was defined as residual invasive disease not identified at first surgery. Fisher’s exact test was used to analyse the impact of close surgical margins on local recurrence.
Results: Of 332 patients 64% had < 5mm clear deep surgical margin with 16% clear by <1mm. Overall, 15 patients (4%) had local recurrence, with a median time to recurrence of 6 months. Eight were embolic spread and 7 residual contiguous disease. Lymphovascular invasion (LVI) was present in 67% and cavernosal involvement in 27%.
There was a statistically significant relationship between cavernosal involvement (p = 0.04), LVI (p = 0.0001) and local recurrence. There was no significant relationship (p= 1.00) with close surgical margins (<5mm vs. >5mm). However a margin of <1mm did show increased risk of local recurrence (p=0.0003).
Conclusions: Recurrence due to contiguous residual disease in margin clear OSS in our experience is very low (2%). Tumour embolism is as likely to occur. We conclude that a deep clear margin of 1mm or more is sufficient in the absence of LVI and/or cavernosal involvement.
P7-10 Prospective study comparing videoendoscopic radical inguinal lymph node dissection (VEILND) with open radical inguinal lymphnode dissection (OILND) for penile cancer in 51 consecutive patients over a five year period
V Kumar
Norfolk and Norwich University Hospital
Introduction: Survival in penile cancer is closely linked to the lymph node metastasis status. Open radical inguinal lymphnode dissection (OILND) is a standard treatment option for patients with suspected groin lymph node metastasis. Multiple studies from high-volume centres have shown the complication rate to be 50% or higher following OILND. VEILND is a minimally invasive alternative to traditional open lymphadenectomy. The technique maintains an oncologically sound dissection of the lymph nodes whilst minimizing wound-related morbidity.
Materials and Methods: The wound related, non-wound related complications and oncological safety between OILND and VEILND groups are compared using a prospectively collected database from a tertiary referral centre. The lymph node yield and positivity rate are used as a surrogate for oncological safety.
Results:
Conclusion: VEILND has a favourable length of stay, immediate and short-term complication rate with comparable oncological results as OILND for penile cancer patients requiring ILND. Further follow-up is necessary to confirm long-term oncological safety of VEILND. (P7-10)
Parameter
OILND
VEILND
P Value
Baseline Characteristics
Number of groin basins
18
33
NS
Number of patients
11
20
NS
Age
69.3
65.7
NS
Stay (mean No of days)
7.95
1.56
0.0001, Significant
Complications
Wound related complications
6/11
0/20
0.0006, Significant
No of readmission <30 days
6/11
2/20
0.01, Significant
No of pts with Permanent Lymphoedema
6/11
1/20
0.003, Significant
Oncological safety
Mean No of Lymph nodes per groin
7.75
8.6
NS
No of groins with Positive lymph nodes
5/18
19/33
0.076, NS
Recurrence
0/18
0/33
N/A
Follow-up in months
30-60
1-30
N/A
P7-11 Surgical management of fungating inguinal masses in penile cancer with myocutaneous flap reconstruction
T Mahesan, A Coscione, D Sharma, M Soldin, N Watkin, B Ayres
St George’s Hospital
Introduction: Patients with advanced penile cancer present a severe challenge with fungating inguinal tumour deposits. Surgical excision with pedicled myocutaneous flap reconstruction is one treatment option. We evaluated our experience at a specialist penile cancer centre over a 12 year period.
Patients and Methods: 19 patients were identified from a prospectively collected database. Complications, length of stay and survival data were analysed.
Results: 21 myocutaneous flap reconstructions were performed for fungating inguinal masses. Two patients underwent bilateral procedures. Median length of stay was 18 days (range 7-161). 13 patients (68%) suffered complications (10 x Clavien II, 2x Clavien IVa and 1x Clavien V). 16 patients (84%) had additional treatment with either chemo or radiotherapy.
13 patients (68%) died of their disease with a median survival of 186 days following surgery (18-937). 6 patients are still alive with a mean follow up of 866 days (145-1919). Accounting for readmission stay, either for further procedures or deteriorating health, patients spent a mean of 21.5% of their survival or follow up time in hospital.
4 of the 6 patients alive completed a validated lymphoedema quality of life questionnaire (LYMQOL) and report similar outcomes to patients who have had groin and/or pelvic node surgery without flaps.
Conclusion: Surgical excision and myocutaneous flap reconstruction is associated with a significant complication rate and length of hospital stay. However, 84% of our cohort lived for more than 3 months without a discharging and painful fungating lesion and 32% are alive with a mean follow up of 28 months.
P7-12 Dynamic Sentinel Node Biopsy of inguinal nodes in squamous carcinoma of the male urethra
T Mahesan, A Coscione, C Corbishley, T Yap, B Ayres, S Heenan, N Watkin
St George’s Hospital
Introduction: Squamous Carcinoma of the Male Urethra (SCCmu) is a very rare condition. In the absence of evidence based guidelines, our specialist genital cancer centre multi-disciplinary team (treating a defined population of 11 million people), agreed to manage SCCmu as for penile carcinomas. This included the assumption that SCCmu first metastasised to the inguinal nodes.
Methods: Since 2001 all confirmed primary SCCmu (pendulous, glanular and meatal) were recorded on a prospective database. From 2004, clinically inguinal node negative (cN0) patients were offered dynamic sentinel node biopsy (DSNB) as part of their staging. The cohort was validated by 2 members of the team independently to exclude cases of confirmed or suspected penile cancer involving the urethra. Lymphoscintigraphy was performed as per a previously described protocol for penile cancer.
Results: 80 SCCu were identified. 52 patients with cN0 inguinal nodes underwent DSNB to 93 inguinal basins. Mean follow up was 28.9 months. 15 patients and 18 basins had positive nodes identified. No patients had a false negative study. No patient was shown to develop pelvic node or distant metastases in the absence of a positive inguinal node.
Conclusion: In this pilot study, we have shown that SCCmu first metastasises to the inguinal nodes and that staging with DSNB identifies patients at risk of micro-metastatic disease.
P7-13 Do alcohol, smoking and male age affect semen parameters and IVF/ICSI outcomes?
K Almekaty, FA Al-Mashat, S Abumelha, C Poullis, TL Yap, N Rushwan, H Abdallah, MY Thum, S Minhas
University College Hospital
Introduction: Determine the effects of alcohol, smoking and male age on semen parameters (SP) and outcomes from IVF/ICSI.
Methods: Records of couples attending an IVF Unit were retrospectively reviewed (2013 to 2014). The age, number of cigarettes smoked/day and number of units of alcohol consumed/week were recorded with semen parameters performed on the day of IVF/ICSI. Multivariate analysis of the effects of age, alcohol consumption and smoking on SP and outcome from IVF/ICSI was performed.
Results: 1257 couples attended for fertility assessment. 13% (n=162) of males were smokers. 77% (n=964) had a history of alcohol consumption. 35.8% (n=450) of couples underwent IVF treatment, 57% (n=717) underwent ICSI and 7.2% (n=90) had failure of embryo development.
Increasing male age was associated with a reduction in SP (p< 0.05). Fertilization rate (FR), pregnancy (PR) and live birth rate (LBR) were unaffected (p=0.603, p=0.895 and p=0.088 respectively).
No differences in ICSI outcome between smokers and non-smokers. With IVF, smoking reduced PR (p=0.049) but not FR or LBR.
Alcohol affected sperm motility and morphology (p < 0.0001) but not volume or count (p=0.544 and p=0.232 respectively). In IVF, PR was reduced (p<0.048) but not FR and LBR (p=0.847 and p=0.063 respectively). In ICSI, FR were reduced (p<0.013) but not PR and LBR.
Conclusion: Age, smoking and alcohol impair SP. The number of cigarettes and amount of alcohol consumed did not correlate with IVF/ICSI outcome. LBR from IVF/ICSI are not affected by these factors suggesting that these technologies improve fertility outcomes by optimising sperm selection.
P7-14 Live birth rates in men with Non-Obstructive Azoospermia (NOA) undergoing microdissection testicular sperm extraction
CA Poullis, S Abumelha, FA Al-Mashat, K Almekaty, N. Rushwan, TL Yap, MY Thum, H Abdallah, S Minhas
University College London Hospitals
Introduction: Sperm acquisition is often used as a primary end point in reporting outcomes from mTESE in men with NOA. The aim of this study was to report live birth rates following mTESE and analyse factors affecting outcome.
Methods: A retrospective review of patients undergoing a primary mTESE for NOA by a single surgeon was conducted, reporting on outcomes from the first cycle of ICSI. The primary outcome measures were pregnancy (PR) and live birth rates (LBR).
Results: A total of 230 patients were included. The mean age of male and female patients was 42.8 and 33.4 respectively. Sperm was retrieved in 105 of 230 (45.7%) of men. 83 patients had ICSI cycles. The mean number of embryos implanted was 1.8 and pregnancy rate was 43.8%, with a primary LBR of 17.3%. 28 (33.7%) of patients had a further 43 ICSI cycles performed with a cumulative live birth rate of 23.3%. There was no significant difference in pregnancy (p = 0.37) or live birth (p = 0.82) rates between fresh and frozen sperm. Age of male or female partners, Johnsen score or histology did not predict success. In 4 (4.8%) patients sperm was non-viable on the day of egg retrieval.
Conclusion: Sperm can be retrieved in 46% of all men with NOA, although only 17.3% are able to achieve paternity at first cycle, which is independent of the histological diagnosis. There is no difference in outcomes between fresh and frozen sperm, although in a small number, sperm won’t survive cryopreservation.
P7-15 Human spermatogonial stem cell culture and effective cryopreservation – a step towards clinical application
RK Sandher, H O’Keefe, K McEleny, M Herbert, RS Pickard
Newcastle University
900 boys are diagnosed with cancer each year but happily survival rates are high. One of the harms of chemo-radiation treatment is depletion of spermatogonial stem cells (SSCs) leading to subfertility in adulthood. Some centres are cryopreserving testicular biopsies prior to treatment with the hope of auto transplantation, requiring viable and stable SSCs. An alternative approach considered in our laboratory is to perform preliminary separation and ex-vivo culture of SSCs to then be cryopreserved for subsequent re-population of seminiferous tubules. The aim of this work was to develop rapid, reliable and reproducible method for human SSC culture and cryopreservation.
SSCs were isolated from testicular biopsies taken from azoospermic men undergoing sperm retrieval. Co-culture with testicular somatic cells facilitated SSCs clumping as chains and finally colonies. Immunofluorescence-labelling using antibodies against stem-cell markers GFRα1 and PLZF combined with confocal imaging, confirmed SSC signature. To date cultures have been maintained for up to 20 weeks. SSCs colonies were cryopreserved using vitrification. Post-thaw proliferation and cell death was assessed using Ki67 and TUNEL immunofluorescence-labelling; demonstrating an average post thaw viability rate of 90%.
Findings indicate our novel technique of firstly establishing a niche-like environment in-vitro is successful in maintaining long-term cultures of human SSCs. Subsequent cell-based cryostorage can then be used until the patient is ready for subsequent re-population of damaged seminiferous tubules. This work is an important practical step forward in the male germline stem cell field, and undoubtedly will advance the future clinical application of SSCs restoring fertility to male childhood cancer survivors.
Wednesday 29 June 1330-1515 Room 4 ePoster Session 8 – General Urology Chairs: Gurpreet Singh and Rajeev Sood
P8-1 An emerging HoLEP reality: 50W HoLEP outcome data in the UK and predictive use of TRUS volume on operating room times
FA Khan, MA Saleemi, S Taneja, A Alam, BJR Barrass, M Al-Sheikh, I Nunney
Luton & Dunstable NHS Foundation Trust
Introduction: Holmium laser enucleation of the prostate (HoLEP) is commonly performed with high powered laser machines (100 & 120 Watt (W)). Many agree this is achievable at reduced power settings. Interest is gaining in 50W HoLEP surgery given its lower capital cost making this financially attractive. Discussion continues about the efficacy of 50W HoLEP surgery. We report our series of over 250 50W HoLEPs undertaken in a single centre to see if 50W HoLEP surgery is a viable option, clinically and financially, for hospitals wishing to develop such a service. Additionally, the use of pre-operative TRUS volume was used to predict theatre operating room times across the series to enhance theatre utilization for HoLEP surgery.
Materials & Methods: Two HoLEP naïve surgeons (FAK, MAS) completed 263 HoLEPs over 27 months using a 50W holmium laser (Auriga XL, Boston Scientific Inc., Piranha morcellator, Richard Wolf). Pre and post-operative data including TRUS volume, flow rate (Qmax), residual volume (RV), international prostate symptom score (IPSS), quality of life score (QoL), surgical time, hospital stay, histology, haemoglobin (Hb), creatinine (Cr) and catheter times were accurately recorded. Enucleation, morcellation and total operating room (OR) times were plotted against TRUS volume to use as a predictive tool for planning HoLEP theatre lists. Mentorship was provided by a senior 100W HoLEP surgeon.
Results: Statistical analysis using SAS statistical software v9.3. The mean difference was tested using either a paired t-test or a non-parametric Wilcoxon signed rank test. Mean age was 70.1, mean TRUS volume 62.8cc and a mean pre-operative PSA of 3.91 ng/ml with 43% of cases in retention noted. Mean enucleated weight (excluding bladder neck incision (BNI) cases) was 43.3g (95% CI 39.3,47.3) with mean operating room times (enucleation & morcellation) of 99.1 mins with an enucleation rate of 0.68 g/min (95% CI 0.61,0.75). Mean IPSS fell by 12.8 (95% CI-14.3,-11.3, p<0.0001), QoL scores improved by 2.8 points (95% CI -3.2, -2.5, p<0.0001) with a mean increase of Qmax 11.0 ml/s (95% CI 8.8,13.3, p<0.0001). Mean hospital stay was 1.04 days with 12.1% performed as day case surgery. Residual volume fell by 129.1 mls (95% CI -165, -93.2, p<0.0001) and an observed reduction in Hb of 1.5 g/L (p<0.0001) and a small clinically insignificant rise in Cr of 3.8 mmol/l were noted. A stricture rate of 2% and a bladder neck contracture rate of 1.9% was observed. Post-operative irrigation use reached 31% and intraoperative diathermy 12.9%. All patients were rendered catheter free. Two transfusions were recorded in our series. Cancer detection rate was 6.8% with return of the financial outlay by the 16th month.
Regression and correlation analysis was performed to determine any linear relationship with TRUS volume reporting both the coefficient of regression and Pearson’s correlation coefficient. Complete data was available for 249 cases, 4 patients did not have a TRUS volume.
A more efficient rate of enucleation with larger prostates was noted. There was a high correlation between TRUS volume and grams/min enucleated (r=0.6019, 95% CI 0.4772,0.7028) and a significant coefficient of regression (p<0.0001) suggesting a fairly strong linear relationship that was matched by total OR times versus TRUS volume (Pearsons correlation 0.6235, 95% CI 0.5418,0.6935, coefficient of regression p<0.0001). Enucleation, morcellation and OR times all had a strong linear relationship with TRUS volume on plots. (P8-1)
Conclusion: 50 Watt HoLEP surgery is emerging as an efficacious and financially attractive alternative to the 100 and 120 Watt holmium systems. Using pre-operative TRUS volume data predicts enucleation times and OR times guiding theatre list planning and management.
P8-2 Feasability and favourable factors for day-case Holmium laser enucleation of the prostate (HoLEP)
SM Lee, F Crystal, S Kapoor, A Tasleem, P Acher
Southend University Hospital
Introduction: A best practice tariff is available for carrying out transurethral resection of the prostate surgery as a day-case procedure with a target caseload of 30%. The purpose of this study was to determine the feasibility of Holmium laser enucleation of the prostate (HoLEP) as a day-case procedure and identify factors that influence length of stay.
Patients and Methods: Consecutive men presenting for HoLEP between September 2013 and February 2015 were included. Data was collected concerning length of stay, indication, age, weight of enucleated tissue and time of procedure (morning/afternoon). Continuous and categorical variables were compared using Mann-Whitney U and chi-square tests, respectively.
A 22Ch irrigating catheter was placed at the end of the procedure. Patients were discharged with catheter in situ when considered medically fit, and underwent a voiding trial 3-7 days post-operatively.
Results: A total of 108 men were included with median age 70 (range 51-93) years and enucleated weight 39 (range 1-220) grams. Indications were LUTS in 57 (53%) and urinary retention in 51 (47%). 76 (70%) cases were carried out on morning lists.
Median length of stay was 1 (range 0-11) night, with 42 (39%) men discharged the same day and a further 42 (39%) within 23 hours. Day-case and non-day-case patients differed significantly on: lower enucleated weight (p=0.002) and time of surgery (morning list, p=0.003).
Conclusion: HoLEP is feasible as a day-case procedure, attracting the enhanced tariff and improving inpatient bed capacity. Advanced assessment of prostate size and planning of theatre lists will maximise potential for best practice.
P8-3 Evaluation of the learning curve for thulium laser transurethral vaporesection of the prostate (ThuVARP)
AS Sharaf, JM Worthington, H Hashim UNBLOCS TEAM
Bristol Urological Institute
Introduction: TURP has been the standard operation for voiding LUTS for 40 years. The thulium laser technique (ThuVARP) vaporises and resects the prostate similar to TURP. For patients undergoing BPO surgery, NICE guidelines recommended offering TURP or holmium laser enucleation (HoLEP). The objective was to assess the surgical learning curve of ThuVARP, as part of a prospective, randomised, multicentre, controlled trial to determine the clinical and cost effectiveness of ThuVARP versus TURP in the NHS (UNBLOCS trial).
Methods: The UNBLOCS trial is funded by the NIHR HTA program. Consultant urologists were mentored to perform ThuVARP. All participating surgeons observed the chief investigator performing 1 to 2 cases. The lead surgeon then observed the principal investigators (PIs) performing 2 to 5 cases. The surgeons then performed cases without supervision. Competency was assessed with the Intercollegiate Surgical Curriculum Programme work-based assessments by an independent assessor and the PIs were signed off once competency criteria were met.
Results: Nine surgeons were involved form 6 different centres. All of the surgeons have performed at least 150 TURPs. A mean of 2.1 cases were observed by each surgeon and a mean of 2.2 cases were performed by each surgeon under supervision. A mean of 7 cases were performed by the PIs before being signed off as competent.
Conclusions: The study has shown that ThuVARP has a short learning curve not exceeding 12 cases for surgeons already experienced in performing TURPs. Results of the non-inferiority trial are awaited to see if outcomes are comparable to TURP
P8-4 Thulium-Laser Enucleation of the Prostate (ThuLEP) as a technique for treatment of benign prostatic hyperplasia: Evaluation of a six-year experience in an urban teaching hospital
IN Noaman, KL Lee, JA Anderson, HK Krasnowski
Russells Hall Hospital
Introduction: THULEP is a well established alternative to traditional TURP in the treatment of BPH. It has been previously demonstrated to be safe and effective in the treatment of symptomatic prostatic obstruction. In this study we examine whether this trend continues with continued use of the technique over time.
Methods: Analysis of data from electronic records, case notes and dictated clinic letters of all the patients who had undergone THULEP using a 70 W thulium laser (Revolix) for symptomatic outflow obstruction over a 6 year period was done. Data collected included the pre procedure PSA, maximum urinary flow rate (Qmax), Post void residual (PVR) and haemoglobin, comparing it with postoperative haemoglobin, PVR and Qmax. In addition, we assessed the total operative time and the mass of prostatic tissue removed, and the incidental prostate carcinoma pickup rate. Patients were followed up to 3-6 months post-operatively.
Results: 581 patients were analysed: aged between 48 and 93 (mean = 72). Preliminary results show a 147% improvement in Qmax and 91% reduction in PVR. The post-operative fall in Hb was 0.4% with only 1 out of 581 patients requiring post-operative transfusion.
Conclusion: THULEP remains a safe and effective intervention with good outcome in relief of outflow obstruction even as the cohort of patients who undergo the procedure expands.
P8-5 Photoselective vaporization of the prostate by 180-W GreenLight Laser versus Bipolar Transurethral Resection: A subset analysis of the GOLIATH trial
JA Thomas, P Zanteck, A Bachmann, N Barber, G Muir, J Benejam, J-U Stolzenberg, F Bruyere, A Thorpe, R Morton
Princess of Wales Hospital
Introduction & Objectives: GOLIATH is a multicentre trial designed to assess efficacy and safety of photoselective vaporization of the prostate (PVP) versus TURP (Monpolar M or Bi-Polar B) in patients with LUTS /BPO. This analysis mimics prospective randomization and compares efficacy, safety, and day case suitability between PVP and B-TURP.
Materials & Methods: In this analysis, randomization to B-TURP and PVP was simulated by including only subjects randomized and treated at the centers where B-TURP was performed. For centers where B-TURP but not M-TURP was performed, all subjects were selected for analysis; for centers where both M-TURP and B-TURP were performed, a PVP subject was selected for each B-TURP case using propensity score matching. Outcomes included IPSS, IPSS-QoL, Qmax, PVR, and prostate volume (PV) and complication free rate at 2 years. Day case suitability was assessed by catheterization time, length of stay and time to stable health status.
Results: 53 subjects treated by B-TURP and 50 matched PVP subjects were analysed. Similar Improvements in IPSS, Qmax, IPSS-QOL, PVR, PV and PSA were observed in both groups. The proportion of subjects free of complications through two years was 79.2% and 82.0% in PVP and B-TURP, respectively. Time to stable health, catheterisation time, and length of stay were all statistically significantly shorter for PVP.
Conclusion: PVP and B-TURP have similar efficacy and safety outcomes at two years. The significantly shorter recovery times for PVP suggest that day case surgery would more frequently be accomplished by PVP compared to B-TURP.
P8-6 Initial outcomes for prostate artery embolisation, an alternative to surgery for BPH
KA Wong, A Parthipun, A Garcia, S Sohel, S Pandian, S Van Rij, B Challacombe, T Sabharwal, R Popert
Guys and St Thomas’ NHS Foundation Trust
Introduction: Lower urinary tract symptoms (LUTS) secondary to Benign Prostatic Hyperplasia (BPH) are a growing problem. Failure of medical treatment leads to surgical intervention in 1/5th of cases. Surgical treatment such as transurethral resection of prostate and holmium laser enucleation of prostate have recognised complications such as bleeding, stricture formation, incontinence, and impotence. We report on our initial results of prostate artery embolization (PAE) as an alternative to surgery for men with LUTS secondary to BPH.
Patients and Methods: We prospectively looked at consecutive patients who underwent PAE between 1st Jan 2014 to 15th August 2015. Data on PSA, prostate volume, pre and post treatment IPSS, qoL, flow rate and residual volumes, IIEF scores were collected.
Results: A total of 59 patients underwent PAE. Mean age 67.31 +/- 11. The mean prostate volume pre-treatment was 148.52mls (45-540mls). Bilateral embolization was technically successful in 96.7%. There was a mean reduction of 19.98% in prostate volume at three months. Mean IPSS reduced from 22.2 to 7.6 at one year. Mean PVR reduced from 276mls to 92.1mls at one year. There were no major complications and two patients had urinary infections post procedure.
Conclusion: Our data demonstrates that PAE is a safe and feasible treatment option with a high initial success rate at reducing symptoms and improving qoL. It can be offered to those patients not suitable for general anaesthetic and avoid some of the side effects of operative intervention.
P8-7 ’One-stop’ LUTS clinic: providing patient satisfaction and cost effectiveness in benign urology
C Dunford, S Watts, S Kuruvilla, A Zachou, T Rashid
Imperial College Healthcare Trust
Introduction: ‘One-stop’ clinics are well-establised in the investigation of haematuria in the UK. Patient satisfaction is high, but in benign urology, convincing Healthcare Commissioners of cost effectiveness is a challenge.
Patients and Methods: We analysed prospectively collected data on new patients seen in a ‘one-stop’ LUTS clinic. Patients were offered consultation and investigation (MSU, flow rate, post void residual, flexible cystoscopy, video/urodynamic studies) in one outpatient episode. We analysed the cost of providing this service and outcome data.
Results: 141 new patients were seen from May-December 2015.Over half were offered definitive management (19% added to surgical waiting list, 32% treated and discharged). 170 appointments were saved performing investigations on the same day.
The total cost of a new outpatient appointment, four investigations and administration in our Trust is £1570 per patient. The tariff assigned to a ‘new patient’ episode in the one-stop clinic is currently £532 reflecting the most expensive investigation (flexible cystoscopy). This is due to be renegotiated. The potential saving to the Trust per annum by reducing appointments and DNAs is £127,656- £357,912.
93.3% patients rated the service as very good or excellent.
Conclusions: Patient experience and large cost savings support a one-stop approach in benign urology. We have demonstrated this is feasible but requires negotiation of an appropriate tariff to be cost-effective for the Trust. Commissioners and Trusts should work together to promote this approach with the joint aim of improving patient care whilst reducing costs. (P8-7)
Current Practice
‘One-stop’ Practice
DNA Rate New OPA
19%
-
DNA Rate Urodynamics
18%
-
DNA Rate Flexible cystoscopy
14%
-
DNA rate ‘one-stop’ clinic
-
11%
P8-8 The early and late effects of cancer on male fertility
CA Poullis, S Abumelha, FA Al-Mashat, K Almekaty, TL Yap, E Williamson, DJ Ralph, S Minhas
University College London Hospitals
Intoduction: The effects of cancers on male fertility are under reported. The aim of this study was to analyze the impact of different cancer pathologies on spermatogenesis.
Materials and Methods: A retrospective review of patients (2010 -2014) diagnosed with cancer undergoing sperm cryopreservation prior to medical or surgical intervention. The semen volume, sperm concentration, overall motility and morphology were reported in accordance with WHO 2010 values. The main tumour groups analysed were testis, leukaemia, lymphoma, prostate, sarcoma and central nervous system (CNS).
Results: A total of 1067 consecutive patients were included. The median age was 31 (IQR 25 – 39). Azoospermia was reported in 7/1067 (0.7 %) patients, severe oligozospermia (⩽1 million (M) sperm/ml) 64/1067 (6.0%) of patients and oligospermia (<15M sperm/ml) in 325/1067 (30.5%). An additional cohort of 102 patients who relapsed post medical/surgical intervention had a rate of azoo/oligozospermia of 48.02% (n=49).
Median sperm concentration was significantly different between tumour groups (p<0.005 Kruskal Wallis), with testis tumours (pre-orchidectomy) having the lowest concentrations (14 million/ml) and CNS tumours having, the highest (29 million/ml) despite having no significant difference in age between the two groups.
Conclusion: Sperm cryopreservation prior to treatment is mandatory and an important aspect of survivorship management and planning, with up to 0.7% of men potentially requiring surgical sperm retrieval for azoospermia. Up to 40% of men with cancers are subfertile, increasing to 48% presenting after relapse. Further research is required to understand the pathogenesis and target future fertility therapies in this cohort of relatively young men.
P8-9 Post vasectomy semen analysis (PVSA): changing sample timing may have unexpected consequences on outcomes
A Zreik, N Smyth, J Taylor
Forth Valley Hospital
Objectives: Semen analysis is an essential part of vasectomy follow up. Traditionally guidelines recommended two samples, but most have now changed to a single sample, although timing of this sample varies. In 2012 our PVSA protocol changed from 2 PVSA at 8 and 12 weeks to a single PVSA at 12 weeks. We anticipated similar clearance rates at 12 weeks in both groups. This study was designed to confirm this.
Materials and Methods: We retrospectively reviewed our vasectomy database and analysed PVSA results for one calendar year before (Group A – 351 patients) and after (Group B – 391 patients) the change in PVSA protocol. Compliance in sample return and time to first clearance were assessed.
Results: Compliance with requested PVSA protocol was 80.6% in both groups. In Group A azoospermia rates at 8 weeks were 64.7%. This rose to 92.8% at 12 weeks. In Group B the initial azoospermia rate did not match the Group A 12-week rate as expected, but instead was equivalent to the 8-week rate(71.0%, p=0.93). This 4-week difference persisted over follow up with Group B azoospermia rates not rising above 90% until week 17. There were no changes in operative technique, or sample collection and analysis to explain this difference.
Conclusion: A sufficient number of ejaculations are needed to achieve azoospermia. Our results suggest allowing more time until first PVSA request may change patient sexual behaviour with consequent effects on clearance rates. Delaying initial PVSA may not necessarily result in expected increases in azoospermia rates.
P8-10 Age of boys at time of orchidopexy surgery, a single practice review
STM Rizvi
South Tees NHS Foundation Trust Hospitals
Introduction: Recently, the age limit to carry out orchidopexy surgery in boys has been revised down to 12 months. This is to minimise the risk of failure of spermatogenesis later in life. BAUS has also issued guidelines to CCGs in August 2015 for an early referral of boys with undescended testes and recommends a maximum age limit of 18 months for the boys to achieve completion of the treatment.
Patients & Method: A prospective evaluation of data on 140 subjects was carried out by the same surgeon between the period of April 2011 to July 2015. Standard of care measured were based on review by the physicians and the allied health professional from the time of the birth.
Results: A total number of 167 orchidopexies were carried out. Of these 27 (16.2%) were bilateral and were performed simultaneously. Of the total 140 patients 101 (72%) were between the ages of 3 to 16 years. Remaining (28%) were 6 months to 2 years of age. It was evident that in majority of the cases, the concerns were raised by the parents and rarely the older boys.
Conclusions: We do not seem to be meeting the standards of completion of orchidopexy surgery even by the previous age limit of 2 years. Further clarity may be useful of the definition of cryptorchidism/undescended testes as these terms encompass testes which are maldescended, retractile and ascended. There is an urgent need to improve awareness about this important issue among the primary and secondary health care professionals.
P8-11 Outcomes of emergency scrotal exploration for acute scrotal pain: Contemporary series from tertiary care hospital
A Anwar, GM Nandwani, R Singh, R Chahal, AB Stewart, JA Forster, SK Addla
Bradford Royal Infirmary
Introduction: Testicular torsion (TT) is a urological emergency that needs urgent scrotal exploration and detorsion. Testicular damage is dependent on duration of ischemia, degree of twisting of spermatic cord (SC) and raised intra testicular pressure (ITP). We determined the surgical outcome of scrotal explorations performed on patients presenting with acute scrotalpain suspicious of testicular torsion.
Patients and Methods: The data was collected retrospectively from case notes of patients who underwent emergency scrotal exploration from January 2006 to May 2014.The main outcome measures were age, duration of pain, pathology found during scrotal exploration, rate of orchidectomy and histology results.
Results: In total, 309 scrotal explorations were carried out during this period. The median age was 16.5 yrs and duration of symptoms was 8 hours. 50.2% (n=155) had true TT, 33.6% (n=104) were torsion of testicular appendages, 9.3% (n=29) showed inflammatory changes and no obvious cause was found in 6.8% (n=21). Orchidectomy was performed in 9.4% (n=29) patients. Histology revealed necrosis in 62% (n=18), and 38% (n=11) showed viable testicular tissue.
Conclusion: Our results were comparable to published series. It supports the practice of urgent exploration for acute scrotal pain with a clinical suspicion of TT. Testicular torsion was the most common finding, followed by torsion of testicular appendages. As significant number of orchidectomy specimens showed viable tissue on histology, multiple tunica albuginea incisions could be made before planning orchidectomy.
P8-12 Management of high grade blunt renal trauma: A 10-year single UK paediatric centre experience
KY Wong, R Jeeneea, A Healey, L Abernerthy, S Kenny, HJ Corbett, HF McAndrew, PD Losty
Alder Hey Children’s Hospital
Introduction: To report the management and outcome of high grade blunt renal trauma in the paediatric population at our centre over the last decade.
Patients and Methods: Retrospective case-note review of all grade III to V blunt renal trauma admitted from 2005 to 2015. Data collected include demographics, imaging modalities, management, length of hospital stay, complications and follow-up outcomes.
Results: 18 children (12 males, 6 females) with mean age 11 years (4 - 15) were included. According to AAST grading criteria, 39% (7/18) had grade III, 50% (9/18) grade IV and 11% (2/18) grade V injuries. 44% (8/18) had concomitant injuries. 89% (16/18) were managed conservatively although 2/16 subsequently needed JJ stent insertion during inpatient stay for symptomatic urinoma. 11% (2/18) required emergency selective embolisation for significant haemoglobin loss on presentation. Blood transfusion rate for renal injury exclusively was 11% (2/18).
89% (16/18) had at least one repeat imaging prior to discharge; the majority (13/16) had ultrasound only apart from 3/16 who required inpatient repeat CT. Length of hospital stay was median 11 days (4- 31). 17% (3/18) had readmission within 30 days for complications and all required intervention: 1 JJ stent for urinoma, 1 embolisation of renal arterio-venous fistula and 1 embolisation for pseudoaneurysm with frank haematuria. Median follow-up was 6 months (2 - 60 months). 72% (13/18) so far have had follow-up DMSA (1 still awaiting); 11/13 (85%) had reduced relative function (range 3% to 44%).
Conclusions: Our series support conservative management of high grade renal injuries. However, there can be associated relative function loss, especially with higher grade injuries.
P8-13 Outcomes of renal trauma from a major UK trauma centre: 3-year retrospective review
Maxim Johnston, D McDonnell, B Somani
Royal Hampshire County Hospital
Aims: To retrospectively evaluate the outcomes of all renal injuries within a Major Trauma Centre (MTC) in Southern England.
Methods: The patient dataset for all major injuries admitted via the MTC from April 2012-April 2015 was scrutinised for patients who had suffered traumatic renal injury. Data was collected for immediate management, length of stay and any associated mortality from it. Renal trauma was grouped into minor injury (Grade I-II) and major injury (Grade III-V).
Results: 2675 patients were admitted via the MTC of which 197 (7%) suffered an intra-abdominal injury and 39 (1.5%) suffered a renal injury. Twenty-six patients with major (15 grade III, 10 grade IV and 1 grade V) and 13 with minor injuries (6 grade I and 7 grade II) were admitted.
Although none of the patients with minor injuries needed any intervention, six patients (23%) with major injury needed intervention (2 embolization, 2 ureteric stent insertion and 1 nephrostomy). The median length of stay for major and minor injury was 13 days (range: 1-272 days) and minor injury was 10 days (range: 1-37 days). There were no nephrectomy and no mortality reported in this series.
Conclusions: Our review show good outcomes for renal injuries when managed in the MTC. Although major injuries may need intervention, most injuries are managed conservatively without the need for emergency nephrectomy.
P8-14 Adopting a ‘one-stop’ approach to all new urology outpatient referrals
J Durrant, S Kamble, B Barrass, F Khan, M Saleemi, A Alam, M Al-Sheik, S Taneja
Luton and Dunstable University Hospital NHS Foundation Trust
Introduction: ‘One-stop’ clinics in urology have been established in several hospitals in the UK. Most centres see only selective patients in these clinics – most commonly haematuria. Our department has recently opened a purpose-built, ‘one-stop’ clinic for all new referrals. We report our experience of the first 10 weeks.
Patients and Methods: A prospective database recorded diagnosis and investigations undertaken in the clinic. Time spent in the clinic and the outcome were logged. Patients were asked to complete a satisfaction survey.
Results: 828 patients were seen in the clinic as new referrals. A total of 642 investigations were carried out, including 193 scans and radiographs and 267 flexible cystoscopies. Mean appointment time was 77 minutes.
A range of different referrals were seen:
21% of patients were suspected cancers referred on 2 week wait.
40% of patients referred for suspected prostate cancer underwent TRUS biopsy in the clinic.
Haematuria patients were offered imaging including CT urogram as part of one stop visit.
34% (n=284) of patients were discharged after one visit.
Extremely high patient satisfaction with 96% of respondents being ‘satisfied’ or ‘very satisfied’ with the service.
Conclusions: It is feasible to see all new urology patients in a one stop set up providing diagnostics including CT urogram and TRUS Biopsy as part of this setup
High patient satisfaction rates are achieved through rapid diagnostics and avoiding multiple patient visits to the hospital. (P8-14)
LUTS
22%
Haematuria
21.2%
Peno-Scrotal
14.5%
PSA / Ca Prostate
9.6%
Stones
8.7%
UTI
8.4%
Renal Mass
3.3%
P8-15 Risk of thrombosis and bleeding in urological cancer surgery (ROTBUS Cancer): Series of systematic reviews and meta-analyses
KAO Tikkinen, S Craigie, A Agarwal, PD Violette, G Novara, R Cartwright, R Naspro, MK Gould, PM Sandset, GH Guyatt
Department of Urology, University of Helsinki and Helsinki University Hospital
Introduction: Pharmacological thromboprophylaxis involves trading off reduction in venous thromboembolism (VTE) against increased bleeding. Here we provide best estimates of absolute risk of VTE and bleeding in urological cancer surgery.
Materials and Methods: We searched for contemporary observational studies reporting symptomatic VTE or bleeding after urological procedures. For each procedure we accounted for use of thromboprophylaxis, length of follow-up, and derived best estimates from the median of included studies. Primary endpoints were 4-week post-operative incidence of symptomatic VTE and bleeding requiring reoperation. We stratified on patient risk factors for VTE (BMI >35, age >75, personal or family history).Quality of evidence was assessed using GRADE.
Results: We included 64 studies reporting on 13 urological cancer procedures, including different approaches of cystectomy, prostatectomy, and nephrectomy. Quality of evidence was moderate for prostatectomy and cystectomy and low or very low for renal procedures. Risk of VTE varied widely between procedures, and between approaches within the same procedure. Cystectomies were high risk for VTE (ranging 2.9%-13.9%) but low risk for bleeding (0.3%). Risks of VTE in prostatectomies showed substantial variation depending on patient risk factors and use of PLND (0.2%-15.7%), with bleeding risks from 0.2%-0.4%. VTE risks in renal cancer surgeries were between 0.7%-6.2% across patient risk groups, with bleeding risks of between 0.1%-1.7%.
Conclusions: Our results suggest that extended thromboprophylaxisis clearly warranted in some procedures. For those operations where the trade-off is less clear, the decision will depend on surgeon and patient values and preferences with regard to VTE and bleeding.
P8-16 Minimising ureteric injury during complex-major colorectal surgery
L Teo, I Jenkins, G Hellawell
London North West Healthcare
Introduction: Complex major colorectal surgery carries a significant risk of urological complicatons that may add morbidity and mortality to an already hazardous procedure. Historical review of urological injury in such cases highlighted the ad-hoc, unplanned nature of urological intervention. At a national centre for complex colorectal surgery, we now minimise urological morbidity by prospectively anticipating urological needs.
Methods: From April 2015, planned urological interventions were prospectively logged and allocated to a designated urological consultant, and discussed at weekly MDTs as part of planned operating by the colorectal service. We evaluated urological outcomes over the past 6 months with a particular focus on minimising unplanned ureteric injuries. We also estimated the costs of prophylactic ureteric stents compared to unplanned ureteric injury.
Results: In six months, 40 requests were made for urological support for complex salvage colorectal operations. 20 requests were for prophylactic ureteric stent insertions to minimise ureteric injuries.
There were no unplanned ureteric transections in the series, with 5 planned ureteric transections in the stented group due to underlying disease processes. The cost for prophylactic ureteric stent insertion and removal is £1700/case, while the estimated cost of unplanned ureteric injury and subsequent reconstruction is £12,000/case.
Conclusions: We did not encounter unexpected ureteric injuries subsequent to the implementation of our advanced planning process for complex colorectal surgery. The tertiary caseload, with previous multiple operations and radiotherapy, presents a challenging cohort with a higher rate of urological morbidity. Careful planning enables the at-risk group to be identified permitting timely urological intervention.
P8-17 Better care at lower cost: Reducing harm from catheter-associated urinary tract infections
L Clarke, J Taylor, D Rowbotham, S Grayson, F Morris, C Blears, R Simpson, B Kadler, K O’Flynn, D Shackley
Salford Royal NHS Foundation Trust
Introduction: Urinary catheter-associated urinary tract infection (CaUTI) results in approximately 3500 deaths/year in the UK. Current data suggests that up to 25% of patients in acute trusts have a catheter inserted which may be unnecessary in 30-50% of cases. 70% of CaUTIs are preventable with current evidence-based strategies. The additional cost associated with treating a CaUTI is estimated to be £1000-£2500.
We postulated that developing a strategy to avoid inappropriate catheterisation would reduce the incidence and harm associated with CaUTI.
Materials and Methods: Following an audit of catheter utilisation and CaUTI in the trust, we undertook a quality improvement initiative to reduce CaUTI rates. Two main strategies were adopted, namely avoiding unnecessary catheter insertion and removing catheters as early as possible. We devised and implemented several novel trust-wide measures including:
Standardised indications for catheterisation
Daily nurse-led review of the appropriateness of catheter indication for all catheterised patients
A nurse-led trial without catheter protocol
Results: In the last 12 months we have achieved:
A fall in the mean inpatient CaUTI rate per 10,000 bed days from 17.5 to 9.4 (46% reduction)
A fall in the mean percentage of catheterised inpatients from 22% to 18% (17.8% reduction)
A fall in the percentage of inappropriate catheters from 20% to 10% (50% reduction).
Conclusion: Our work demonstrates that implementing a range of simple measures can effectively reduce CaUTI. Adoption of these measures in UK healthcare settings has the potential to reduce the serious avoidable morbidity and potential mortality that CaUTI presents.
P8-18 Flexible cystoscopy for the investigation of recurrent Urinary Tract Infection (UTI) – How helpful is it really?
N Smyth, A Zreik, J Taylor
Forth Valley Royal Hospital
Objectives: To investigate the clinical benefit of flexible cystoscopy for the investigation of recurrent urinary tract infections (UTIs). Does this investigation add any diagnostic benefit that cannot be achieved with non-invasive investigations such as flowometry and ultrasound?
Patients and Methods: Retrospective analysis of a database of patients who underwent flexible cystoscopy for the investigation of recurrent UTIs at a single centre between January 2011 and September 2012.
Results: A total of 408 patients underwent flexible cystoscopy for the investigation of recurrent UTIs – 285 women and 123 men. 22 (8%) of female patients had a significant abnormality detected. The majority of abnormalities were found on ultrasound scan with 3 (1%) detected at cystoscopy alone.
No significant abnormalities detected in women under 55 years.
30 (24%) of men had a significant abnormality, 8 (2.8%) of which were detected on flexible cystoscopy.
27 red patches were detected, of these all had either resolved at GA cystoscopy or had benign histology on biopsy. Two bladder tumours were detected, one of which was visible on ultrasound.
Conclusions: In our cohort, only 2.9% of patients had a significant abnormality detected on flexible cystoscopy that could not have been detected with ultrasound or uroflowometry. Our findings suggest that flexible cystoscopy is rarely helpful in the assessment of recurrent UTIs. The majority of significant pathology can be detected through careful clinical history + ultrasound +/- flowometry. Our findings also suggest that flexible cystoscopy is probably not necessary for female patients with recurrent UTIs under the age of 55 years.
P8-19 Penile fracture: Conservative versus surgical; a meta-analysis
T Amer, R Wilson, P Chlosta, S AlBuheissi, O Abomarzouk
Glasgow Royal Infirmary
Objectives: To review the causes and management of penile fracture and to compare between surgical and conservative management as well as immediate and delayed interventions in terms of overall and specific complications.
Methods: A search of all reported literature was conducted for all articles reporting on the management and outcomes of penile fractures. Full texts of relevant articles were obtained and screened according to the inclusion criteria.
Outcomes measures were: numbers of patients receiving surgical or conservative management, aetiology of fracture, length of admission, complications as well as the specifics of diagnostic approaches and operative management. Data was collated and where possible meta-analysed using Revman software.
Results: A total 58 relevant studies involving 3213 patients demonstrated that intercourse accounts for only 48% of cases with masturbation and forced flexion accounting for 39%. Meta-analysis shows that that surgical intervention was associated with significantly fewer complications versus conservative management (P <0.000001). Surgical intervention results in significantly less erectile dysfunction, curvature and painful erection than conservative management. There was no significant difference in the number of patients developing plaques/nodules (P = 0.94). Meta-analysis shows that overall early surgery is preferable to delayed surgery but that rates of ED are not significantly different.
Discussion: Early surgical intervention is associated with significantly fewer complications than conservative management or delayed surgery. Rapid diagnosis by history and clinical examination and swift surgical intervention is key for reconstruction with minimal long-term complications.
P8-20 How confident do general practitioners feel about urology?
NE Boxall, DJ Rosario
Royal Hallamshire Hospital
Introduction: Urological problems account for around 10% of primary care encounters. Referral rates of general urology to secondary care are rising every year and confidence in clinical assessment in primary care might be a factor in this. The aim of this study was to evaluate factors contributing to General Practitioners’ (GPs’) confidence in assessing urological conditions.
Methods: A paper survey of GPs surgeries across England assessing self-evaluated confidence in performing and interpreting digital rectal examination (DRE) and scrotal examination based on two clinical scenarios, grading responses on a five-point Likert scale.
Results: Of 357 respondents (226 male, 131 female), 88% were confident in performing DRE and scrotal examination with fewer reporting confidence in interpreting the findings (72.8% and 69.2% respectively). Female respondents were less confident in both performing and interpreting DRE and scrotal examination (p<0.0001). Neither age nor prior urological training impacted on confidence performing or interpreting urological clinical examination. Participants had mixed views on whether further training on DRE or scrotal examination would improve their confidence (45.3% and 61.6% respectively). There was no statistically significant difference between gender, age or prior urological experience with respect to the perceived impact of extra training on confidence.
Conclusions: Females made up 37.1% of the GP workforce in 2003 increasing to 48.5% in 2013. Despite possible underrepresentation of female respondents, a gap between male and female GPs’ confidence at performing and interpreting urological examinations was identified in this survey. Prior urology training does not appear to impact on confidence in urological clinical examination.
Wednesday 29 June 1430-1530 Room 12 ePoster Session 9 – History of Urology Chairs: Jonathan Goddard & Nick Gill
P9-1 Showmen in Urology
AO Auer, D Hodgson
Queen Alexandra Hospital - Portsmouth Hospitals NHS Trust
Introduction: There are many instances where dramatic demonstrations of pathology or therapy have significantly influenced medical practice. We explore examples in Urology.
Methods: We identified, and reviewed the pertaining literature on, three key “showmen” in our specialty.
Results:
Terence Millin (1903-1980). This Irish surgeon trialled TURP but favoured his own modification of the retro-pubic approach, hence “Millin’s prostatectomy” still performed today. He demonstrated the effectiveness of this at a meeting of the Royal Society of Medicine when he had a patient, who he had operated on a week before and had plied with beer, to demonstrate his improved flow to the audience of stunned Urologists.
Giles Brindley (1926-). This British physiologist made a very dramatic demonstration of the pharmacological effects of Papaverine on the penis by revealing his own, previously injected organ during a lecture at the Urodynamics Society in Las Vegas in 1983. According to leading Andrologist John Pryor “the impact was tremendous”, and went a large way to herald the era of pharmacological treatment of impotence.
Christian Chaussy (1945-). This German Urologist was instrumental in developing the first ESW lithotripter. He even volunteered to be the first human subject on this then very much experimental machine. His open door policy, inviting colleagues to live surgical demonstrations, did much to win over the initially sceptical Urological community.
Conclusion: “Showmen” can have a dramatic effect on the development of medicine, as demonstrated by the three presented here who changed the course of Urology.
P9-2 Alexander Randall: A major contributor to the understanding of the genesis of renal calculi
M Hadjipavlou, MJA Perry, KM Anson
St George’s Hospital
Introduction: Urinary tract stones have been tormenting humans since the ancient times with the true aetiology remaining a mystery until the past century. We review the life and pioneering work of Alexander Randall who paved the way to the understanding of stone formation.
Methodology: A comprehensive search was performed on the life of Alexander Randall and his work on the pathogenesis of urolithiasis.
Results: Alexander Randall (1885–1951) started his career in urology at John Hopkins in 1907. His research focused on the origin of stones by studying the renal papilla and investigated by inducing stones in animal models, however inconsistent results changed his methodology to using human cadavers. In 1937, Randall described a hypothesis that renal calculus formation is due to renal papillary damage resulting in deposition of crystalline urinary salts. He reported vascular abnormalities and atherosclerosis associated with these plaques as degeneration of tissue overlying the calcium plaques would enhance subsequent stone formation. He published his most well-known series of over one thousand pairs of kidneys where he found that 20% showed evidence of early calcified plaques in at least one renal papilla, to which he gave his name.
With improvements in chemistry and imaging modalities, subsequent research on the pathophysiology of stone formation covered the gaps in Randall’s theory related to his plaques.
Conclusions: Randall gave his name to subepithelial calcified plaques of renal papillae which act as anchors for stone formation. Great tribute is due to his work which has formed the basis of contemporary stone research.
P9-3 The contribution of Sir Thomas Spencer Wells to urology
MS Wanis, JC Goddard
University Hospitals of Leicester
Introduction: Sir Thomas Spencer Wells served in Malta as a naval surgeon before establishing his own practice in London in 1853. He is most notably recognised in the fields of Obstetrics, Gynaecology and Ophthalmology. He was Surgeon to Queen Victoria’s Household from 1863-1896. Although his contribution to Urology is less well known, he was founding member of St Peter’s Hospital for Stone in London in 1860, the first hospital in Britain dedicated to urology.
Methods: A literature review was performed on the contribution of Spencer Wells to urology using Medline, Embase, Public Records Library and other sources.
Results: In 1860 Spencer Wells gathered with Armstrong Todd, Reverend Whatton and TP Aldershaw to discuss establishing a hospital for urinary stones. He subsequently published a paper in the press campaigning for a hospital dedicated to urinary diseases. St Peter’s Hospital for stone was established in 1860. Wells practiced there until 1862 after which he departed to work at the Samaritan Free Hospital For Women. Whilst there, Wells was one of the first surgeons to recognise urinary tract injuries whilst pioneering ovarian cystectomy. After his death in 1897, St Peter’s committee acknowledged Wells for maintaining an interest in the hospital’s welfare throughout his career.
Conclusions: Sir Thomas Spencer Wells was a founding member of St Peter’s Hospital and continued to contribute to urology throughout his career. This was one of the first specialist hospitals in London at the time and its establishment was a catalyst for the development of urology as a specialty.
P9-4 John Wickham - The Godfather
AO Auer, D Hodgson, PM Thompson
Queen Alexandra Hospital - Portsmouth Hospitals NHS Trust
Introduction: John Wickham (JW), it has been suggested, is the godfather not only of endo-urology in the UK, but a key pioneer of minimally invasive surgery internationally.
Material and Methods: The subject was interviewed and the resultant transcript analysed. Former colleagues were questioned and literature written by, or pertaining to, the subject was reviewed.
Results: Having witnessed the finesse of neurosurgery in his training and developed renal cooling for his MD thesis, on being appointed as a consultant in 1968, JW was concerned at the crude surgery for renal calculi which often resulted in nephrectomy. Over the subsequent decades he developed radial nephrotomies and then PCNL. In the face of resistance from his British peers he joined with international colleagues to form the Endourological Society in 1994 and was their first president. He also formed the Society for Minimally Invasive Surgery, with innovators from other specialities in 1989. In the 1980’s he introduced lithotripsy to the UK and with Malcolm Copcoat performed the first laparoscopic nephrectomy. He also led many Endourological research projects and enthused a new generation of Urologists. His most ambitious project was an autonomous TURP robot which, whilst clinically effective, was moth-balled because of cost. However, as a proof of principle, it was invaluable, and foresaw the revolution in robotic urological surgery over the subsequent three decades.
Conclusion: JW can rightly be claimed to be the Godfather of Endourology and the impact of his work on minimally invasive surgery across specialities is still evident today.
P9-5 Reed Miller Nesbit: So much more than a straightening procedure
OC Putt, IP Wharton
University Hospital of Coventry & Warwickshire
Reed Nesbit (1898-1979) graduated from Stanford, before gaining surgical residency at Ann Arbour, Michigan. Under Hugh Cabot’s tutelage, and whilst rooming with Charles Huggins, he published prolifically and progressed to become the first head of the Urology department.
His contribution to paediatric urology was significant. In 1931, Cabot and Nesbit described their single-stage orchidopexy procedure, which included their much citied method of testicular mobilisation. Nesbit (1940) subsequently described a two-stage repair for hypospadias consisting initially of chordee correction and ventral resurfacing using buttonhole transposition of the prepuce. A Z-plasty technique to correct stricture of the interval meatus was also reported (1954).
After a lecture by Theodore Davis (1931), Nesbit first revolutionised and then popularised transurethral resection of the prostate. He modified the Stern-McCathy resectoscope by extending the loop beyond the sheath and spring-loading the mechanism. Observing intravenous haemolysis, he introduced isotonic glycine for irrigation and limited operative time to 60-minutes (1948).
Combining cystometry with neurological examination, Nesbit and resident Lapides concluded that the bladder was controlled by two reflex arcs and then classified neurogenic bladder types (1947).
As ureterosigmoidostomy, the then favoured technique for urinary diversion, was frequently complicated by anastomotic stenosis, Nesbit (1948) developed a method of ureteric spatulation with mucosa-mucosa anastomosis which lowered the stricture rate.
In 1964, Nesbit described the surgical procedure for which he is synonymous. Initially used for correcting congenital penile curvature, it was subsequently adopted by Pryor & Fitzpatrick for the management of Peyronie’s disease (1979).
Prior to retirement (1967), Nesbit became the first urologist to be President of the American College of Surgeons; a fitting finale to his remarkable career.
P9-6 The rise and fall of occupational bladder cancer in the Western World
MS Wanis, M Hadjipavlou
University Hospitals of Leicester
Introduction: One in ten cases of bladder cancer are attributed to occupational exposure to carcinogens. Multiple substances used in the chemical industries have been linked to the disease. We review the milestones that led to the discovery of carcinogens and changes in employment regulations leading to a fall in occupational bladder cancer.
Methods: A literature review on occupational bladder cancer was performed using Medline, Embase and the Archives of the Royal Society of Medicine.
Results: In 1895, German surgeon Ludwig Rehn reported three cases of bladder cancer in workers at the Hoechst aniline factory, Greisheim. However, the association with the chemical was difficult to prove as chemical manufacturers used other coal- and oil-based compounds. Beta-naphthylamine (BNA), produced by distilling coal, was used in the production of dyestuffs, cables and rubber. In 1938, Delaware-based pathologist Wilhelm Hueper showed an increase in bladder tumours when BNA was administered orally to dogs but, being funded by the chemical industry, had difficulty publishing his research. BNA was prohibited worldwide following a landmark study by Case and Holster on British rubber industry workers in 1954 after discovering a 200-fold increased risk of bladder cancer. In 1972 Miyakawa subsequently demonstrated a significantly decreased incidence of bladder cancer.
Conclusions: The groundbreaking discovery of aromatic amines as the most important carcinogens in occupational bladder cancer prompted worldwide regulatory changes to the manufacture of rubber and dyestuffs. The incidence of occupational bladder cancer has decreased in the Western world but is still widely reported in less developed countries.
P9-7 The ‘Holy Stones’
MSV Vedanayagam, K Farrag, I Dickinson, S Sriprasad
Darent Valley Hospital
Introduction: In spite of their divine powers, holy men and women have suffered from urinary stones since antiquity. This presentation explores the fascinating history.
Methods: A search for sources was undertaken using the Internet and library sources.
Results: St Alban of Mainz is said to be the patron saint of kidney stones. The Greek Philosopher Epicurus who preached freedom from fear (ataraxia) and from pain (aponia) died from an obstructing ureteric stone (270BC). Pope Innocent XI underwent surgery for kidney stones and following his death in 1689, he was found to have “stones weighing nine ounces in the left kidney and six ounces in the right”. Martin Luther, a German monk, was also a sufferer of kidney stones. He consequently almost faced death from being ‘unable to urinate’. It was the movement of the carriage on the journey home that prompted spontaneous stone passage and ‘spared his life.’ The Bishop of Chester and founder of the Royal Society, John Wilkins, had the distinction of heading a college at both the Universities of Oxford and Cambridge. To treat his kidney stones, he was fed, “four red-hot oyster shells in a quart of cider and blistering with cantharides.” It is believed that he died from the opiate overdose (1672). Father Thomas in India had a miraculous disappearance of his kidney stone after praying to Mother Teresa.
Conclusion: The historical records of distinguished people give us an insight to the prevailing management of stones in the corresponding period.
P9-8 How intersex children in the Dominican Republic changed the face of Urology
T Mahesan, UR Reddy
Brighton and Sussex University Hospitals
Introduction: With an ageing population, the prevalence of benign prostatic hyperplasia (BPH) is increasing and with it the number of men opting for conservative management over surgery. The concept behind finasteride, one of two main drugs, stemmed from the discovery of a gene mutation causing ambiguous genitalia in childhood. How did research of an intersex disorder go on to become the basis for one of the best known drugs in urology today?
History: In the 1970s Dr Julianne Imperato-McGinley, a consultant endocrinologist travelled to La Salinas in the Dominican Republic to investigate rumours of girls growing penises. Here she found guevedoces (translation: ‘men at twelve’), an inter-related population who carry an autosomal recessive mutation affecting the 5 alpha reductase (5 AR) type II gene. Homozygous carriers are deficient in 5 AR, preventing conversion of testosterone to dehydroepiandrosterone. Until puberty this manifests as the absence of a penis and testes, and as adults these men have little facial and body hair, immunity from male pattern baldness and very small prostate glands.
Application: It is this final property of 5 AR deficiency that is utilised in finasteride, a 5AR inhibitor which mimics the effect of the gene mutation, reducing the size of the prostate and thus lower urinary tract symptoms.
Conclusion: With its introduction, finasteride changed the management of BPH, introducing a viable long term alternative to prostatic surgery. What started as a rumour around gender identity continues as a drug that improves the lives of men worldwide.
P9-9 From death sentance to improved quality of life: The evolution of management of malignant ureteric obstruction
JG Calleary, A Bourdomis, P Naidu, S Khan
Pennine Acute NHS Trust
Introduction: Death from obstructive renal failure secondary to advanced pelvic malignancy was regarded as a possible desirable outcome. (Meyer et al, Cancer1980; 45: 2698-2701). Treatment was reserved for severe pain or new diagnoses. We track changes in attitudes and techniques which have increased survival but especially quality of life.
Methods: Systematic literature review of databases (eg Pubmed) was performed using keywords such as ureteric/ureteral obstruction, advanced pelvic malignancy and obstructive uropathy. Search dates used were 1900 – 2015. Abstracts of retrieved references were evaluated and relevant papers checked. Diversion method, survival, outcome, complications of diversion and quality of life measures were extracted.
Results: Less than 100 relevant papers were identified. From these two basic eras of clinical management are identifiable. The first involved very selective diversion using ileal conduit or cutaneous ureterostomy and lasted to the mid 1980’s. The second era is associated with increased use of diversion and increased minimally invasive techniques. Use of these has led to reduced complications, reduction in hospitalisation time and has contributed to increased survival.
Conclusion: Brin et al (J Urol May 1975; 113(5): 619-22) in a series of 47 “malignant” diversions showed 23% alive at six months and 2/3 of their time was spent in hospital. Currently minimally invasive techniques used in conjunction with prognostic tabulation can improve both survival and quality of life in up to 66 % of diverted patients (Fiuk et al, J Urol. 2015 Apr;193(4):1092-100). Clearly this represents a vast improvement. The challenge is to continue this sterling work.
P9-10 ‘Transgender’: Mythology to modern times!
A Reekhaye, M El-Hadi, M Vedayanagam, J Nariculam, S Sriprasad
Darent Valley Hospital
Introduction: Transgender and transsexualism have fascinated people since antiquity. This study explores the history from ancient to modern day gender reassignment surgery (GRS).
Methods: A search for sources was undertaken using internet and library sources.
Results: In Indian mythology, deities are represented as both male and female at different times or of both genders at once, such as Ardhanarishvara (‘Lord whose half is woman’) created by the merging of the God Shiva and his consort Parvati. In African mythology, the God Mawu-Lisa, formed by a merger of the twin brother and sister Gods Lisa (the moon) and Mawa (the sun). The patron God of transgender is Dionysus, a God gestated in the thigh of his father Zeus. The birth of modern GRS was in Berlin. Rudolph became Dora by GRS performed by Dr Felix Abraham (1931). Lili Elbe had several procedures including a uterine transplant, the rejection of which caused her death and is the theme of a recent Hollywood movie. In Britain, Sir Harold Gilles was the pioneer of GRS. He performed female to male GRS on Roberta Cowell (1951), which became the standard technique. Christine Jørgensen was a famous recipient of GRS (1952). She was a night-club singer and actress and fought for the rights of GRS persons.
Conclusion: Norman Fisk introduced the term gender dysphoria syndrome (1973) to cover applicants seeking GRS. This surgery is complex and has evolved to change the physical characteristics based on a person’s mental belief of his or her gender.
Thursday 30 June 1200-1315 Room 4 ePoster Session 10 – Prostate Cancer Treatment: Choices and Outcomes Chairs: Justine Royle & Jay Smith
P10-1 The BAUS Radical Prostatectomy audit – an update on current practice (2014)
C Miller, A McNeill, N Campain, L Hounsome, S Fowler, JS McGrath
BAUS Section of Oncology
Introduction: As part of the Consultants Outcomes Publications programme, data on radical prostatectomy (RP) practice during 2014 were made ‘public-facing’ for the first time.
Methods: Individual surgeons/units uploaded their data on RP to the electronic BAUS data registry. Once extracted, data were transferred to an Access™ database for validation prior to analysis using Tableau™ software.
Results: Details on 6,651 RP were uploaded from 157 consultants at 71 sites (87% of all RP in England). Median number of RP per surgeon was 31 (1-157) with a median per centre of 77 RP (compared to 16 and 38 respectively in 2013). 25% of centres perform less than 50 RP per year. Commonest surgical approaches were open (13.4%), laparoscopic (26.7%) and robotic (58.5%). Transfusion rates vary with surgical approach–open (6.5%), laparoscopic (0.8%) and robotic (2.9%). Median length of stay varies markedly – open (3d), laparoscopic (2d) and robotic (1d). Lymph node dissection (LND) is performed in 42% of RP, but only 45% received extended LND. 57% of patients have nerve sparing (28% unilateral/23% bilateral). Approximately 1 in 4 RPs are ‘training cases’, but only 14% are with trainees suggesting a high level of consultant upskilling. Positive margins rates (pT2) are lowest with robotic surgery (13.61%) compared to open/lap (19%).
Conclusions: Compliance with data registry of RP is high in England and, for the first time, allows an accurate ‘snapshot’ of current practice. Most patients undergo RP by high volume surgeons in high volume centres. Length of stay/positive margin rates are lowest with robotic surgery. Reported transfusion rates are lower with minimally invasive approaches.
P10-2 Are there differences in radical prostatectomy practice between centres and surgeons performing differing volumes of surgery?
C Miller, A McNeill, N Campain, L Hounsome, S Fowler, JS McGrath
BAUS Section of Oncology
Introduction: Following centralisation of major urological cancer surgery, median number of cases of RP per surgeon and per centre has increased in recent years but there remain significant differences in volume between surgeons/centres. The current analysis describes differences in RP practice between low, medium and high volume practices.
Methods: Individual surgeons/units uploaded their data on RP to the BAUS Registry. Once extracted, data were transferred to an Access™ database for validation prior to analysis using Tableau™ software. Centres were defined as low (<50), medium (50-100) and high (>100) volume according to annual caseload. Surgeons were similarly grouped into low (<50) and high (>50) volume.
Results: Details on 6,651 RP (Jan–Dec 2014) were uploaded from 157 consultants at 71 sites (87% of all RP in England). Table 1 demonstrates % of RP by volume, % undergoing lymph node dissection (LND) and % of latter that had extended LND (eLND).
Centre
Surgeon
Volume
LND
%eLND
Volume
LND
%eLND
LOW
13.4%
43%
34.2%
40.2%
40%
29%
MEDIUM
28.1%
34.8%
19.8%
−
−
−
HIGH
58.5%
45%
56%
59.8%
43%
53.8%
Only high volume robotic centres achieved a median length (LOS) of stay of 1d – other centres and lap RP had median LOS of 2d. Open RP - LOS 3d. The same effect was seen with surgeon volume. The majority of cases in high volume centres are robotically-assisted.
Conclusions: Patients undergoing RP where surgeon and centre volumes are high are more likely to have an adequate LND, a robotically-assisted procedure and an optimal LOS. (P10-2)
P10-3 Factors that affect decision-making for radical prostatectomy in elderly patients with prostate cancer: Results from the National Prostate Cancer Audit
MG Parry, A Sujenthiran, A Aggarwal, P Cathcart, S Charman, J Nossiter, H Payne, J van der Meulen, N Clarke
Clinical Effectiveness Unit, The Royal College of Surgeons of England
Introduction: There is increasing evidence that older men with prostate cancer (aged over 70 years old) are under-treated. The International Society of Geriatric Oncology developed treatment guidelines to reduce ageism within prostate cancer care. Individual health status, not age, is recommended to drive decision-making for management, with the use of a validated screening instrument (G8) and the assessment of patients’ co-morbidities, dependence status and nutritional status. We aim to report the factors that affect decision-making for radical prostate cancer surgery in elderly patients with prostate cancer.
Patients and Methods: A survey was sent out to all 48 specialist multi-disciplinary teams (sMDTs) within England and all four in Wales. sMDT leads were asked to rank six factors in order of importance (1=most important; 6=least important) when assessing an elderly patient’s suitability for radical surgery: age, expected life-expectancy, co-morbidities, performance status, cardio-pulmonary exercise test (CPEX) result and other.
Results: There was a 100% response rate from sMDT leads. 63% of sMDTs ranked expected life-expectancy as the most important factor, followed by co-morbidities (42%), performance status (40%), CPEX result (26%), and age (6%). Other factors flagged as important included patient choice and disease grade/status.
Conclusion: Chronological age is not regarded as the most important measure of suitability for radical prostate surgery. Clinicians should be encouraged to utilise validated tools to predict life expectancy and performance status when evaluating patient suitability for radical prostate cancer surgery.
P10-4 An improved clinical risk stratification system to better predict cancer specific mortality at diagnosis in primary non-metastatic prostate cancer
VJ Gnanapragasam, A Lophatananon, K Muir, A Gavin, D Greenberg
Academic Urology Group, University of Cambridge
Introduction: Risk stratification is the cornerstone of management for newly diagnosed non-metastatic prostate cancer. Here we developed and tested a new risk stratification system using the number of individual risk factors and the ISUP 2014 prognostic scores.
Patients and Methods: Diagnostic data was derived from 10,139 UK men divided into a training (n=6226) and testing set (n=4113). An external validation cohort (n=1706) was also used. Risk groups were first assigned as low, intermediate and high (NICE 2014) then sub-stratified by the number of risk factors and grade re-classified using the new ISUP scores. A 5 strata criteria was produced and prognostic power compared against the NICE criteria with prostate cancer specific mortality (PCSM) as the outcome.
Results: In both training and testing sets the new classification identified a very low-risk group (Group 1), a subgroup of intermediate-risk cancers with a low PCSM risk (Group 2, HR 1.62[0.97-2.75]) and a further subgroup with an increased PCSM risk (Group 3, HR 3.35[2.04-5.59]) (p<0.0001). High-risk cancers were also sub-classified into a better and worse outcome group: Group 4 (HR 5.03 [3.25-7.80]) and Group 5 (HR 17.28 [11.2-26.67]) (p<0.0001). In comparison to NICE, the new criteria demonstrated improved prognostic performance (Concordance index 0.75 (95% CI 0.72-0.77) versus 0.67 (95% CI 0.64-0.69) (p<0.0001). This was recapitulated in an external cohort (Concordance index of 0.83 (95% CI 0.80-0.87) for predicting PCSM versus 0.67 (95% CI 0.64-0.70) for the NICE criteria.
Conclusion: A novel 5 strata risk classification out-performs the NICE criteria in predicting the risk of PCSM.
P10-5 Medium to long term follow up of a large UK cohort of active monitoring of patients
AJ Bennett, MT Jefferies, O Hughes, K Narahari, H Kynaston
University Hospital of Wales
Introduction: Active surveillance is now an established part of the management of patients with low risk localised prostate cancer. However, long term follow-up data for it is still lacking.
Methods: We reviewed a prospectively collected database of active monitoring (AM) patients within our institution from February 1997 to March 2014. Age, PSA, Gleason grade and D’Amico classification at presentation were reviewed. Time to treatment and survival were assessed.
Results: 506 patients were included with a median follow up of 5.95 years (range 0.83- 18.8 years). Median age was 68 years (range 46 - 92) and median PSA was 7.6ng/ml (range 0.4-35.4) at presentation. 85.4% had Gleason 6 and 14.6% Gleason 7. 63.4% were D’Amico low risk, 32.4% intermediate risk and 4% high risk. Overall, 42.3% of patients received treatment. Median time to treatment was 2.5 years. Percentage of patients receiving treatment at 0-5 years follow-up was 33.6%, 5-10 years follow-up was 40.7% and >10 years was 42.3%. Of these treated patients, 8% chose to withdraw from AM and the remainder had treatment based on PSA rise and/or a combination of grade/volume/stage progression.
A total of 76 patients died (15%). Overall survival at 5, 10 and 15 years was 91.6%, 81.7% and 71.6% respectively. Disease specific survival at 5, 10 and 15 years was 99.4%, 97.8% and 90.0% respectively.
Conclusion: Overall, treatment and survival rates for our cohort are similar to other published data with similar follow-up times.
P10-6 Focal HIFU for Treatment of Localised Prostate Cancer: A Multi-centre Registry Experience
Guillaumier S, Hamid S, Charman SC, van der Meulen J, McCartan N, Shah K, Hindley R, Nigam R, Dudderidge T, Afzal N, Cornaby A, Lewi H, Persad R, Moore CM, Arya M, Emberton M, Ahmed HU
UCL
Introduction: Focal therapy using HIFU has been shown to provide encouraging short-term disease control with a low genito-urinary side effect profile. We report on the medium-term oncological and functional outcomes from our UK prospective academic HIFU registry across 8 centres.
Methods: 625 patients diagnosed with T1aN0MO to T3bN0M0 prostate cancer after multi-parametric MRI, transperineal and/or MR-targeted biopsies and were treated with focal HIFU.
Results: Of 625 patients, 80 (13%), 491 (81%) and 39 (6%) had low, intermediate and high-risk disease. At 1-2 years and 2-3 years post-op, at baseline and follow-up; 305 (97%) and 241 (98%) were pad-free, respectively. At 1-2 years and 2-3 years after focal-HIFU, continence status was 209 (83%), and 156 (80%) were pad-free, leak-free continent.
At 1-2 years and 2-3 years, at baseline and follow-up; 138 (84%) and 87 (86%) maintained erectile function, respectively. Two (0.8%) developed a recto-urethral fistula of which one healed with urinary diversion alone and the second required operative reconstruction.
Overall, 29/625 (4.6%) were found to have in-field recurrence on 12 month post-op biopsies. 16 (2.6) out-of-field de novo disease or progression and 11 (1.8%) had both. 122 (20%) had a further focal-HIFU treatment, whilst 44 (7%) transitioned to radical whole-gland therapy. The metastasis-free survival, prostate-cancer specific survival and overall survival at 5 years were 97%, 100% and 99% respectively.
Conclusions: Focal HIFU has acceptable rates of cancer control in men with clinically significant prostate cancer with a low genito-urinary side-effect profile in the medium-term and across a number of centres.
P10-7 Development and internal validation of a multivariable prediction model for biochemical failure after focal salvage high intensity focused ultrasound for locally recurrent prostate cancer: presentation of a risk score for individual patient prognosis
M Peters, TT Shah, A Kanthabalan, N McCartan, JRN van der Voort van Zyp, MA Moerland, M van Vulpen, R Hindley, M Emberton, HU Ahmed
University Medical Center Utrecht (UMCU) and University College London Hospital (UCLH)
Introduction: Locally recurrent prostate cancer after primary radiotherapy might be curatively treated using focal salvage. Optimal patient selection is essential. This study therefore aims to develop a prediction model for biochemical failure (BF) following focal salvage high intensity focused ultrasound (HIFU).
Materials and methods: A comprehensive registry was used (Nov 2006-Sept 2014). Recurrences were assessed with multi-parametric MRI combined with template prostate mapping biopsies or systematic TRUS-guided biopsies as well as PET/CT and a bone-scan. Quadrant or hemi-ablation was applied. With Cox proportional-hazards regression, the effect of determinants on BF (Phoenix-definition) was assessed. Multiple imputation was used for missing data. Internal validation was performed using bootstrap resampling (500 datasets). Calibration plots and the C-statistic were adopted to assess model performance. Finally, a risk score was created.
Results: 139 patients were identified. Primary treatment consisted of external beam radiotherapy (EBRT, n=134) or EBRT with high dose rate brachytherapy (n=5). Mean follow-up was 37 months (sd 21 months). BF occurred in 71, resulting in 50% biochemical disease-free survival (bDFS) at 35 months. Multivariable, disease-free survival interval (DFSI) after primary radiotherapy, pre-salvage PSA, PSA doubling time (PSADT), prostatic volume and T-stage (both MRI-based) were independent predictors (Table 1). The adjusted C-statistic was 0.69. Calibration was accurate up to 36 months. Our risk score consisted of 4 groups, highly predictive of bDFS at 3 years (88% [95%CI: 75-100%], 68% [51-81%], 33% [18-48%] and 20% [0-40%].
Conclusion: Improved focal salvage patient selection can increase recurrence free rates from 50% to almost 90% at 3 years.
P10-8 Does extended pelvic lymph node dissection increase morbidity and mortality in men undergoing robotic radical prostatectomy?
KE Hughes, T Nambirajan, G Riley, M Kumar
Arrowe Park Hospital
Aim: Extended pelvic lymph node dissection (EPLND) at the time of robotic prostatectomy is controversial despite being the gold standard for identifying microscopic lymph node metastasis (MLNM). Our aim was to determine if appropriate patients had been selected and to compare morbidity.
Method: Retrospective analysis was undertaken of 299 men who underwent robotic radical prostatectomy at our institution between January 2013 and December 2015. Patients were subdivided into 2 groups those who had undergone EPLND (tissue excised from obturator, internal and external iliac region +/- common iliac region) and those that hadn’t (NOLND). Data was collected on demographics, calculated Briganti score, duration of surgery, LN yield, and complications. Results were analysed using the student-t test or chi squared test on spssv23 (p= <0.05 was considered significant).
Results: Eighty Eight men (29.4%) had EPLND; 66 (86.4%) had bilateral EPLND with average LN yield 15.8 (range 4-42) and 12 (13.6%) had unilateral EPLND, average LN yield 6.17 (range 1-9). Two hundred and eleven men had NOLND. Univariate analysis showed statistically significant difference between age at surgery, calculated Briganti score, operating time (mins) and length of hospital stay (p=0.001, p=0.000, p=0.001, p=0.048 respectively). No difference in blood loss (p= 0.872). Twenty-nine patients (6 EPLND vs 13 NOLND) (14.1%) had a post-operative complication none were Clavien-Dindo grade 3 or above (p=0.799).
Conclusion: EPLND will continue to provide therapeutic and diagnostic benefit for suitable patients at risk MLNM. We have shown there is no significant difference in morbidity or mortality contradicting previous studies.
P10-9 Management of pathological lymph node positive prostate cancer post radical prostatectomy: Recent experience from a single UK centre
A Kodera, T King, SA Ehsanullah, A Shafik, A Makar
Worcestershire Acute Hospitals NHS Trust
Introduction: Immediate ADT has previously been shown to improve CSS and OS in N+ disease after RP. In the present era of increased detection of microscopic nodal disease due to increasingly performed ePLND, this may represent over treatment for some patients. We present a series of patients with N+ disease managed either expectantly or with immediate ADT with a focus on early oncological outcomes.
Patients and Methods: Patients with N+ disease at RP were identified retrospectively from our database. Patients were either given immediate ADT or offered a period of PSA monitoring depending on disease characteristics and informed patient choice.
Results: 35 patients were identified with N+ disease, all except 4 had undergone ePLND as part of open RRP. Mean lymph node yield was 16 (2-64). Overall median follow up was 38 months (8-110). 24 patients underwent PSA monitoring, 11 patients were given immediate ADT. Of those undergoing expectant management, median follow up was 25 months during which 29% required additional treatment for biochemical progression. In the immediate treatment group one patient died from PE 2 years post operatively. No other patient in either group developed clinical progression and the median PSA at most recent follow up in patients managed expectantly and with immediate ADT is 0.2 and <0.1 respectively.
Conclusion: In our small series, patients with N+ disease at RP managed with PSA surveillance had a low rate of biochemical progression and need for additional treatment at 2 years. Immediate ADT for N+ disease may be safely avoided in selected cases.
P10-10 Intraoperative frozen section of the prostate during Robotic Assisted Radical Prostatectomy (RARP) improves erectile function rates and decreases positive margin rates - United Kingdom’s first series of 100 cases
N Vasdev, BP Rai, S Agarwal, G Mohan, J Adshead
Lister Hospital
Introduction & Objective: To evaluate functional outcomes and positive margin positive rates (PSMR) for intra-operative frozen section (IOFS) analysis of the prostate during RARP allowing nerve sparing.
Methods: We prospectively analysed the data of 100 patients who underwent an IOFS during RARP from November 2012 to November 2015. Our IOFS technique involved whole lateral circumferential analysis of the prostate with the corresponding neurovascular tissue. Intrafascial nerve spare was performed. The specimen was removed intra-operatively by extension of the 12mm-camera port. Proportion were compared using the 2-tailed z-test (p-value<0.05=significant).
Results: Median time to extract the specimen, wound closure and re-establishment of pneumoperitoneum increased the operative time by 8 min. Median blood loss for IOFS vs. non-IOFS cohort was 130±97 ml vs 90±72 ml (p=NS) respectively. For T2 disease the proportion of patients who underwent a nerve sparing approach (unilateral or bilateral) in IOFS and non-IOFS cohort was 62% vs. 98.7% (p<0.05). For T3 disease the proportion of patients who underwent a nerve sparing approach (unilateral or bilateral) in IOFS and non-IOFS cohort was 28% vs. 91% (p<0.05). The 3 and 12-month continence rates for IOFS vs. non-IOFS cohort was 81% vs. 78%, p=NS and 93% vs.95%, p=NS respectively. The 12-month erectile function rates for IOFS vs. non-IOFS cohort was 31.74 vs.64%, p-0.0001. For T2 disease PSMR were T2-6.4% vs. 16.7% (p=0.02). For T3 Disease PSMR were 9% vs. 44% (p=0.002)
Conclusion: Introduction of the IOFS analysis increased the proportion of patients undergoing a nerve sparing approach, decreased the PSMR and improved erectile function rates.
P10-12 Development of indicators to assess intermediate treatment-related urinary complications following radical prostatectomy
A Sujenthiran, M Parry, S Charman, J Nossiter, A Aggarwal, H Payne, N Clarke, J van der Meulen, P Cathcart
St George’s Hospital
Introduction: Radical prostatectomy (RP) is a common treatment for localized prostate cancer. Data on incidence of intermediate treatment-related complications following RP are lacking. We developed indicators using Cancer Registry (CR) – Hospital Episode Statistics (HES) linked data to capture unplanned interventions following RP.
Patients & Methods: Men with prostate cancer were identified as having undergone RP if their HES record between 2008 and 2012 contained the “M61” Office of Population Censuses and Surveys (OPCS) procedure code. Hospital admissions post-RP were interrogated for OPCS codes related to urinary complications. 3 sub-categories were determined (haematuria-, stricture- and incontinence-related) and validated with associated ICD-10 codes. Cumulative 2-year Kaplan-Meier rates were calculated for all urinary complications and the 3 sub-categories while logistic regression analysis was employed to evaluate predictors of urinary complications.
Results: 17,552 men underwent RP over the study period, 16.5% of whom underwent at least one urological intervention within 2 years. Median time to first intervention was 111 days. 2-year incidence of experiencing either haematuria, stricture or an incontinence related complication was 12.0%, 6.8% and 0.9%, respectively. Charlson score ⩾1 (OR 1.13(95%CI: 1.02-1.25), p=0.02), lower socio-economic status (OR 1.55(95%CI: 1.35-1.77), p<0.01) and length of stay for RP>3days (OR 1.66(95%CI: 1.53-1.80), p<0.01) significantly increased the likelihood of at least one urological intervention.
Conclusions: Approximately 1 in 6 men required an unplanned urological intervention within two years of RP. These data could be used to counsel patients regarding treatment-related complications while adjusted indicators could be used to assess variation in care.
P10-13 What parameters affect continence after radical prostatectomy?
IDN Rudd, R Zakri, B Hearnden, J Pain, M Thomas, B Eddy
East Kent Hospitals University NHS Foundation Trust
Introduction: Urinary incontinence (UI) after radical prostatectomy (RP) has a significant detrimental effect on quality of life. It has been reported that laparoscopic or robotic assisted laparoscopic prostatectomy (RALP) results in better outcomes in the short term and nerve sparing procedures are also associated with a reduced incidence of UI. Little is otherwise known about what parameters influence UI after RP
Patients and Methods: We analysed a prospectively collected database of 605 consecutive RALPs by a single surgeon. All were performed with a posterior reconstruction and a modified Van Velthoven anastomosis. Pad number and ICIQ scores were assessed at 6 weeks, 3, 6, 12, 18 and 24 months. UI outcomes were analysed in relation to age, prostate size, BMI, nerve sparing procedures, bladder neck sparing procedures, previous TURP, training cases and extended lymph node dissections.
Results: Pad usage and ICIQ scores decrease dramatically between 6 weeks post operatively and 12 months. At 24 months mean pad usage is only 0.2 pads and ICIQ score 2.5.
Patients over the age of 70 had significantly worse UI (p=0.0021). Bilateral nerve sparing was associated with reduced pad use (P < 0.001) and ICIQ scores up to 3 months (P =0.0014) but not beyond.
There is no significant difference in outcomes with prostate size, BMI, previous TURP, extended lymph node dissections, training cases or the use of a bladder neck sparing procedure.
Conclusion: Overall continence rates are good after RP. Increasing age is the only parameter that significantly affects long term outcomes.
P10-14 3-month pad use is a reliable predictor of long term continence recovery in men undergoing robotic radical prostatectomy
AN Sridhar, PJ Cathcart, G Basnett, TP Briggs, S Nathan, JD Kelly
University College London hospital NHS trust
Objectives: Although urinary continence (UC) return post RARP can take up to two years, predictive metrics are required for patient counselling and early institution of enhanced rehabilitation. The aim was to evaluate to the accuracy of 3-month UC return as a predictive metric of long term UC recovery.
Method: A prospective cohort study of 740 men undergoing RARP over a 4 year period between September 2010 and Dec 2014 was conducted. The ICIQ-SF was administered pre and post RARP at 3, 6, 12, 18 and 24 months. Multiple linear regression analysis was used to test association between UC scores at different time points.
Results: 61.5% (276/449), 71.0% (282/397), 78.2% (248/317) and 83.3% (185/317) respectively were noted to be pad free at 3, 6, 12 and 18 months after surgery. Median ICIQ-SF scores at similar time points were 5, 4, 3 and 1. 98% of men were continent at 12 months if they required ⩽ 2 urinary pads at 3 months compared to only 14% that required ⩾ 3 urinary pads (p=<0.001). Mean 12 month ICIQ-SF score for men requiring ⩾3 pads at 3 months was 8 (SD 2.04) compared to 3 (SD 2.2) for patients requiring ⩽ 2 pads (OR 2.7, 95% CI 2.1-3.5, p<0.001).
Conclusions: 3-month UC is a good predictor of long term UC return. A high proportion of patients requiring ⩾ 3 pads at 3 months will not regain continence and can be identified as requiring enhanced rehabilitation.
P10-15 Does supersensitive PSA add additional prognostic benefit to predicting biochemical recurrence in post radical prostatectomy patients at medium term follow up?
KE Hughes, T Nambirajan, G Riley, M Kumar
Arrowe Park Hospital
Aim: To determine if supersensitive PSA nadir (SSPSAN) post radical prostatectomy is a significant prognostic indicator for predicting the risk of biochemical recurrence (BCR) and can help identify patients who may be safely managed conservatively.
Method: Retrospective analysis was undertaken of 271 men with a SSPSAN who underwent laparoscopic radical prostatectomy at our institution between 2008 and 2013. Eighteen patients with PSA >0.1 ng/ml were excluded. 253 eligible patients were divided into 2 groups; SSPSAN⩽0.01g/dl and SSPSAN between 0.02-0.1ng/dl. Demographic data, Pre-op PSA, post-operative Gleason score, pathological T-stage, margin status, lymph node involvement and BCR/salvage treatment (BCR/STMT) was recorded. Kaplan-Meier analysis were used to compare time to (BCR/STMT). Multivariable cox regression was used to evaluate the relationships between SSPSAN and identify men at higher risk of BCR. SPSSv23 used for statistical analysis.
Results: Two hundred and fourteen men (85%) had SSPSAN ⩽0.01ng/dl (Group-A) and 39 men (15%) SSPSAN between 0.02-0.1ng/dl (Group-B). At a mean follow up 56.0 months (range 29.2-84.631 (12.3%) had BCR; defined as serum PSA>0.2ng/dl (15/48.4%); or salvage treatment (16/51.6%) for high or rising PSA<0.2ng/dl. Kaplan-Meier estimates showed men with SSPSN⩾0.02ng/dl had a significantly higher rate of BCR/STMT than those with SSPSAN ⩽0.01ng/dl (Log-rank: p=0.00). Multivariable cox regression; backward method showed SSPSAN⩾0.02g/dl was the only significant independent variable for predicting BCR (p=0.000).
Conclusion: SSPSAN is a significant independent predictor of BCR or adjuvant treatment. Men with a SSPSA ⩽0.01ng/dl even in the presence of other adverse pathology could undergo conservative management.
Thursday 30 June 1200-1300 Room 12 ePoster Session 11 – Basic Science Chairs: Imran Ahmad & Ased Ali
P11-1 UroMark - A highly multiplex biomarker for the detection of bladder cancer
A Feber, P de Winter, P Dhami, M Martinez-Fernandez, DS Paul, A Hynes-Allen, WS Tan, P Gurng, S Rodeny, A Mehmood, F Villacampa, F de la Rosa, C Jameson, KK Cheng, MP Zeegers, R Bryan, N James, JM Paramio, A Freeman, S Beck, JD Kelly
UCL Cancer Institute
Introduction: Bladder cancer (BC) ranks the most expensive to manage due to the need for cystoscopic examination. Several studies have shown the utility of epigenetic alterations as urinary biomarkers for the detection of disease, however these have failed to reach the sensitivity required to replace cystoscopy in ruling out BC. The aim of this study is to determine the sensitivity and specificity of a large scale targeted bisulphite-sequencing assay (UroMark) for the diagnosis of BC by using cystoscopy as the reference standard.
Material & Methods: The 150 loci UroMark assay was defined from a cohort of 81 MIBC, 30 normal urothelium, 532 bloods and validated in 179 BCs, 20 normal and 10 non-malignant urines. RainDrop PCR and next generation sequencing (NGS) was used to validate the UroMark assay in urines from 98 non-cancer controls (haematuria cases (n=86), surveillance cystoscopy (n=12)) and 78 BC cases (low grade (n=30), intermediate and high grade cancers (n=48)).
Results: The 150 markers UroMark assay accurately predicted the presence of BC from urinary DNA with a sensitivity of 1 and specificity of 0.97, giving and ROC area under the curve of 0.95.
Conclusions: Epigenetic urinary biomarkers for detection of BC have the potential to revolutionize the management of this disease. We have developed a novel high through put, NGS based assay for the detection of BC specific epigenetic alterations in urine. We show that the sensitivity and specificity as equivalent to cystscopy and outperforms small panel methylation assays for the detection of BC in urinary sediment.
P11-2 The translational potential of cell-free mutant DNA for muscle invasive bladder cancer
KMP Patel, K vd Vos, C Smith, J Morris, C Massie, VJ Gnanapragasam, DE Neal, B v Rhijn, M vd Heijden, N Rosenfeld
Cancer Research UK Cambridge Institute
Introduction: Only 50% of patients with muscle invasive bladder cancer (MIBC) respond to Neoadjuvant Chemotherapy (NAC). Overtreatment of non-responders therefore, represents a major drawback. At present, we are unable to accurately and promptly identify responders. The analysis of tumour-derived mutant cell-free DNA (cfDNA) may identify response promptly due to its short half-life and has hitherto been unreported. For urological cancers, direct shedding of mutant DNA into urine may increase mutant:wild type ratio and more informative than plasma as a non-invasive liquid biopsy.
Methods: Interim analysis was performed on sequential plasma, urine cell-pellet and urine supernatant samples from 8 MIBC patients. DNA was extracted with optimised protocols. Single Nucleotide Variants (SNVs) of multiple genes were assessed by high-throughput Tagged-AMplicon Sequencing, and Copy Number Alterations (CNAs) were analysed using shallow Whole Genome Sequencing (sWGS), based on previous descriptions.
Results: 14 SNVs were detected in 7 patients. When comparing peripheral fluids, SNVs were detected in the plasma 5 times, urine cell-pellet 21 times and urine supernatant 15 times, indicating that for MIBC, SNVs are detected more frequently in urine. CNAs were detected in all tumour samples and were present in the peripheral fluids in 4 of 6 patients analysed to date.
Conclusions: Interim analysis of MIBC patients suggests that urinary cfDNA is more informative than plasma for mutational analysis. Liquid biopsies can provide continual monitoring of tumour burden and mutational profile. Urinary mutant cfDNA analysis could therefore, play an important role in detecting treatment response in patients undergoing NAC for MIBC.
P11-3 Low INPP4B expression predicts poor prognosis locally advanced and metastatic bladder cancer
WS Tan, PMS Gurung, C Ackerman, S Rodney, P de Winter, A Freeman, C Jameson, T Powles, A Feber, JD Kelly
University College London
Introduction: Traditional prognostic markers such as tumour grade and stage have a limited role in predicting outcomes in bladder cancer (BCa). Inositol polyphosphate-4-phosphatase, type II (INPP4B) is a tumour suppressor gene and loss of INPP4B is associated with a poor prognosis in prostate and breast cancer with limited evidence in BCa.
Patient & Methods: A tissue microarray (TMA) of 105 patients with stage IV (pT4b or N1/2) or metastatic BCa who had stable disease after chemotherapy was stained for INPP4B. All patients did not have radical treatment. Light microscopy was used to examine TMA cores. Primary end point was overall survival (OS).
Results: Median follow-up was 17.4 months (range: 1.4-45.5, IQR: 7.1-20.1). INPP4B was positive in 56 patients (66.7%) while 28 patients (33.3%) had low/ negative INPP4B expression. INPP4B negative patients were significantly associated with shorter OS (HR: 1.97, 95% CI: 1.09- 3.57; p=0.022).
Conclusion: Loss of INPP4B was associated with shorter OS in BCa patients with stage IV or metastatic disease. Further work is needed to determine if INPP4B is a prognostic marker for response to chemotherapy.
P11-4 Uncovering patterns of copy number aberrations in penile cancer
S Rodney, A Feber, M Arya, P De Winter, M Saqib, R Nigam, P Malone, S Tan, M Christodoulidou, V Sahdev, M Lechner, A Freeman, C Jameson, A Muneer, S Beck, J Kelly
University College London
Introduction: In Europe penile cancer (PeCa) is a rare disease, with an incidence of approximately 1.5 per 100,000 males. Due to the rarity of the disease there is a paucity of knowledge of its genetic drivers. Our previous work demonstrated a large range of epigenetic drivers. We now present the role that copy number aberrations play in driving the oncogenesis of penile cancer.
Patients & Methods: High density genome wide methylation arrays were used to assess copy number variation using the conumee package in R. Samples from twenty four patients with squamous cell penile carcinoma were used. Further analysis was performed using GISTIC (a tool to identify genes targeted by somatic copy-number alterations that drive cancer growth).
Results: Significant amplifications were found including 4p15.2, 9p22.3, 19p13.2, 19p12 and 19q13.2. Significant deletions were found at 4q35.2, 6q22.31, 6q27, 7q36.1, 11p15.4, 11q12.1, 11q23.3, 13q13.3, 15q11.2 and 21q22.11. Distinct patterns of copy number gains were noted for both the HPV positive samples (1p36.11, 3q26.2, 6p22.1) and lymph node positive samples (3q26.2 and 11q22.2). These copy number alterations included many known oncogenes including MYC, KRAS and FGFR3 as well as tumour-suppressors CDKN2A, CCND1, RB1 and p53.
Conclusions: This new study interrogated 24 penile cancer genomes using high-density genome wide methylation arrays. We present distinct patterns of copy number variations for both HPV positive and lymph node positive samples. This both corroborates previous findings of a defined amplification at 19q13 but also adds further novel variations in both HPV positive and lymph node negative subsets.
P11-5 Does PIK3CA Copy Number Aberration lead to activation of the PI3K-AKT-mTOR Pathway?
A Adimonye, E Stankiewicz, S Kudahetti, R Rajab, C Corbishley, Y-J Lu, N Watkin, D Berney
Barts Cancer Institute
Introduction: The phosphatidylinositol-4,5-bisphosphate 3- kinase, catalytic subunit alpha (PIK3CA) gene is mutated and amplified in various cancers leading to dysregulation of the PI3K-AKT-mTOR pathway, which is known to regulate cell proliferation and survival. Nobody to our knowledge has evaluated PIK3CA copy number status (CNS) in penile cancer (PC). We aimed to determine the prevalence of PIK3CA copy number gain, its effect on PIK3CA mRNA expression and activation of the PI3K-AKT-mTOR pathway in PC.
Materials and Methods: Fresh frozen tissue specimens and paraffin embedded blocks were obtained from 24 primary penile cancer patients with additional 15 corresponding paired normal epithelial tissue. PIK3CA gene CNS and mRNA were examined using fluorescence in-situ hybridisation (FISH) and Quantitative Real Time PCR, respectively. Phospho-AKT (p-AKT) and phospho-mTOR (p-mTOR) protein expression were assessed using western blot.
Results:PIK3CA copy number gain was found in 11/23 (48%) patients. Penile tumours showed significantly lower expression of PIK3CA mRNA (3.8±2.9 vs 7.4±2.2, P=0.0004), p-AKT (0.3±0.3 vs 1.0±0.7, P=0.0008) and p-mTOR (0.3±0.2 vs 0.7±0.5, P=0.0033) than normal adjacent penile tissue. No association was found between PIK3CA CNS and expression of PIK3CA mRNA, p-AKT or p-mTOR protein. (P=0.4779, P=0.894 and P=0.5095, respectively).
Conclusion: A high frequency of PIK3CA copy number gain was found in PC, suggesting that the PI3K pathway may play a role in penile carcinogenesis. However, surprisingly, we found no association between PIK3CA CNS and PIK3CA mRNA, p-AKT or p-mTOR protein expression. Further work to clarify the link between PIK3CA CNS and activation of the PI3K pathway is needed.
P11-6 EMT markers within M1 diagnostic prostate biopsies correlate with stem like phenotype and loss of AR signalling
K Hiew, SM Bokobza, CA Hart, T Elliott, NR Smith, M Brown, NW Clarke
Salford Royal NHS Foundation Trust
Background & Aims: Epithelial-Mesenchymal Transition (EMT), as characterised by loss of cell polarity and cell-cell adhesion, and the gain of invasion and migratory abilities, stem like characteristics and resistance to chemotherapeutic agents, is critical to metastasis. Our previous work showed Vimentin and E-cadherin were prognostic in diagnostic biopsies. This report examines whether EMT status correlates with altered expression of androgen signalling and stem cell-like genes in primary diagnostic prostate samples with M1 disease at first presentation.
Result: Expression of EMT inducers (ZEB1: r=0.537, p=0.015; ZEB2: r=0.750, p=0.000; SNAI2:r=0.604, p=0.005), the EMT effector a-SMA (r=0.635, p=0.003), CD44 (r= 0.472, p=0.036) correlated with EMT status. AR genes (AR, ARV7) exhibited an inverse correlation with EMT status (AR: r= -0.542, p= 0.013: ARV7: r=-0.502, p=0.024). The kallikrein family showed a mixed response with KLK4 correlating with EMT status (r=0.474, p=0.035) but not KLK2 & KLK3.
Conclusion: Our results suggest EMT status is associated with the expression levels of AR signalling and stem cell like genes in diagnostic needle biopsies of men with primary M1 CaP at first presentation.
P11-7 Exosomal RNA as a source of urine biomarkers for prostate cancer
MYH Yazbek Hanna
Royal Preston Hospital
Introduction: In this study we have exploited the recent development of methods that have enabled the analysis of RNA present in urine exosomes of prostate cancer (PCa) patients. We report RNA expression patterns that contain diagnostic and prognostic information for PCa, and association with response to hormone treatment.
Methods: First catch urine following digital rectal examination were collected from 800 men. 3 groups of patients were used: Low, Intermediate, and High-risk according to NICE stratification criteria, and two control groups: benign and advanced disease. 50-gene transcript expression analysis using NanoString technology was performed on 193 samples. Exosomal RNA Next-Generation Sequencing was performed on 20 samples for novel biomarker discovery.
Results: Expression analysis identified transcripts that were significantly differential expressed: 17 between cancer and non-cancer samples, and another 17 transcripts up-regulated in high-risk and advanced disease in comparison to lower-grade disease. Two gene transcripts were significantly differentially expressed in patients who failed to respond to hormone treatment for high risk/metastatic disease. Three genes were significantly differentially expressed in patients who relapsed within 12-months of treatment initiation.
Next-Generation Sequencing of exosomal RNA samples identified 45 genes to be significantly differentially expressed between non-cancer and cancer samples. 33 out of the 45 genes showed a significant linear trend in association with cancer-risk.
Conclusions: Urine exosomal RNA contains PCa- specific transcripts. Gene expression analysis and Next Generation Sequencing identified genes that are significantly differentially expressed between cancer and non-cancer cases as well as prognostic genes and genes that can predict response to hormone treatment.
P11-8 A urinary peptide biomarker panel to identify significant prostate cancer
MJS Salji, A Latosinska, A McKay, J Clark, H Mischak, HY Leung
CRUK Beatson Institute
Background: Urinary biomarkers which can identify patients with significant prostate cancer (PC) used as an adjunct to PSA testing is an attractive clinical prospect. Capillary electrophoresis coupled to mass spectrometry (CE-MS) is a tool for the discovery of such potential urinary peptide biomarkers.
Methodology: CE-MS was performed on 313 samples of urine obtained from patients with significant PC with Gleason 8-10 or T3/4 disease (n=66) and controls with High Grade -PIN, low volume low grade Gleason 6 disease, Prostatitis, BPH or normal histology (n=247). An initial training set of 236 patients was used to identify a biomarker panel separating controls (n=188) from significant PC (n=48). Performance was then compared to PSA by ROC analysis in a clinical test set (n=77, 18 cases and 59 controls) classified by PSA.
Results: A panel of 94 peptides were identified in the training cohort separating significant PC and controls (p<0.05, using Benjamini and Hochberg adjustment and bootstrapping cross validation). ROC analysis showed an AUC=0.82 for our biomarker panel in the training cohort. As expected the AUC for PSA in the test cohort was almost perfect (0.968) as it was classified by PSA. Our biomarker panel showed AUC of 0.69 in the test cohort which significantly differed from PSA (p<0.001).
Conclusions: Using CE-MS we have generated a 94 peptide urine biomarker panel specifically to identify significant PC from insignificant disease. Our biomarker panel shows differing ROC to PSA in an independent PSA classified test cohort and may provide a useful adjunct to PSA testing.
P11-9 Neutrophil gelatinase-associated lipocalin (NGAL) as a biomarker of renal injury in patients with ureteric stones
M Bolgeri, K Farrag, A Reche, P Manghat, S Sriprasad
Darent Valley Hospital
Introduction: In patients with acute unilateral ureteric obstruction, creatinine and urine output measurement have significant pitfalls as markers of renal injury in the presence of a normal contralateral kidneys.
A biomarker may allow early detection of renal injury. NGAL has shown good performance as predictor of renal injury in different scenarios.
This study analyzes the kinetics of NGAL in patients with acute obstruction secondary to ureteric stones.
Material and Methods: Serum (sNGAL) and urine (uNGAL) levels were measured pre-, intra- and postoperatively in 37 subjects with ureteric colic, and compared with two control groups (13 patients with non-obstructive renal stones undergoing elective surgery and 10 healthy controls). Samples were analyzed with a commercially available turbidometric immunoassay. Multivariate analysis evaluated the correlation of NGAL with routine clinical parameters.
Results: sNGAL decreased significantly after relief of ureteric obstruction (77ng/mL vs 82ng/mL, p=0.01). uNGAL in the urine from the obstructed kidney was significantly higher than in the bladder. In patients who passed their stone, at 4 weeks’ follow-up NGAL levels were significantly lower (p=0.03). NGAL at presentation was significantly lower in healthy controls (p=0.003). Surgery didn’t significantly affect levels of pNGAL and uNGAL (p=0.61 and p=0.09).
Conclusions: Relief of obstruction led to a significant decrease in NGAL levels.
Surgical intervention did not act as a confounder.
These observations suggest that NGAL could help estimating renal injury due to obstructive stones and act as a marker of de-obstruction during follow-up.
Further studies are needed to establish the significance of these for the clinical decision-making.
P11-10 An in vitro model to study cystinuria
HL Rhodes, LK Farmer, T Knight, MN Woodward, GI Welsh, RJM Coward
University of Bristol
Introduction: Cystinuria is an inherited renal stone disease caused by mutations in the amino acid exchanger system b0,+ found on the proximal tubular epithelial cells (PTEC) of the kidney. Defects in either subunit of the transporter, rBAT or b0,+AT, lead to the formation of recurrent cystine stones and significant renal impairment. There are no effective treatments available, and no recent therapeutic advances. Mutation analysis has recently been made available in the UK. This work aims to establish a functional in vitro model to investigate the cellular effects of the common British mutations in rBAT and b0,+AT to enable the identification of new therapeutic targets at the molecular level.
Materials and Methods: Epitope-tagged rBAT and b0,+AT were expressed and characterised in human conditionally immortalised PTEC, and cystine uptake was quantified using radio-labelled cystine assays.
Results: Immunoprecipitation studies confirmed that expressed rBAT and b0,+AT formed dimers in PTEC in vitro. Biotinylation studies confirmed correct trafficking of the dimerised transporter to the plasma membrane. Radiolabelled cystine uptake more than doubled in cells co-expressing both rBAT and b0,+AT compared to untransfected PTEC, or PTEC expressing rBAT or b0,+AT alone.
Conclusions: We have established a functional in vitro model that can be used to further interrogate system b0,+ in the cell type specifically affected in cystinuria. This model can be manipulated to investigate known and discovered cystinuria mutations with the aim of facilitating development of novel disease therapies.