
Abstract

The true incidence of pancreatic complications, although uncertain, would seem to be approximately one in 600 cases as reported by Liapis et al. 1 This incidence reflects our experience at Portsmouth Hospitals NHS Trust. Analysis of the BAUS 2014 Nephrectomy Dataset reveals three pancreatic injuries out of 7703 upper tract procedures performed (two occurring in patients undergoing minimally invasive surgery). 2
Given the increasing complexity of renal surgery being tackled retroperitoneoscopically, we wanted to highlight this as a rare but potential complication to be considered in patients with a protracted postoperative course and non-specific abdominal pain.
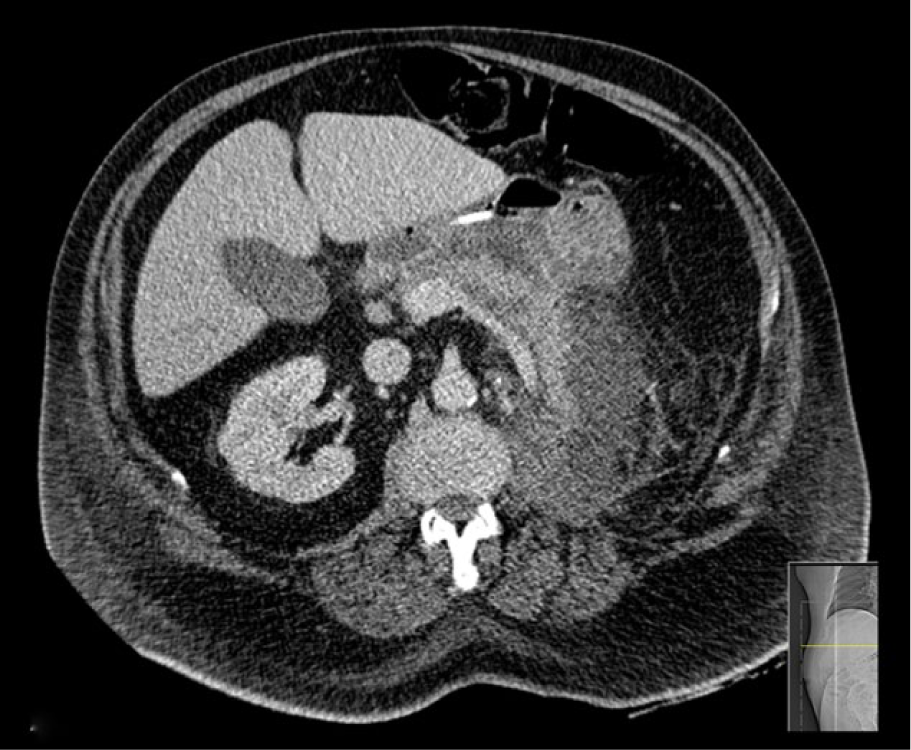
We present two cases of pancreatitis occurring after retroperitoneoscopic nephrectomy, one of which was further complicated by pancreatic pseudocyst development. Both patients were successfully managed conservatively. The first patient was a 76-year-old man with an 8 cm renal tumour, suspicious for renal cell carcinoma (RCC) identified on renal tract ultrasound scan (USS) as part of investigations into painless visible haematuria (see Figure 1 for preoperative computed tomography (CT)). His comorbidities consisted of diabetes and hypertension, for which he was taking insulin, lisinopril, simvastatin and felodipine. He did not drink any alcohol and had no history of gallstone disease. Histological analysis of the left kidney specimen confirmed a Fuhrman grade 2/3 pT3bN0M0 tumour. The operation itself was uneventful. However, two days postoperatively the patient complained of non-specific abdominal pain, nausea and sluggish bowel action. Physical examination revealed generalised upper abdominal tenderness, without peritonism. Laboratory tests are shown in Table 1. An abdominal CT was performed which showed a large collection in the left renal bed (9 cm × 10 cm × 15 cm), which was presumed to be haematoma (Figure 2). However, low attenuation of the pancreatic tail, raising the possibility of pancreatitis (Figure 3), was also noted and on further radiological review the collection was attributed to a large pancreatic pseudocyst. The patient was commenced on Creon and improved symptomatically.

Preoperative computed tomography (CT) showing proximity of left kidney tumour to the pancreas.
Post-operative serum blood test results for our first patient.
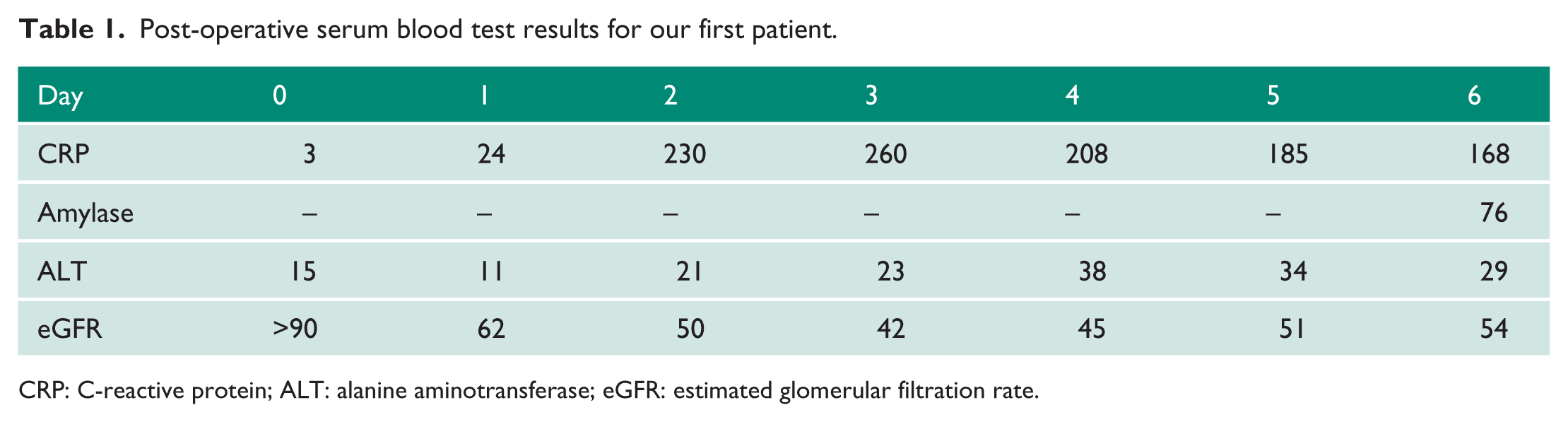
CRP: C-reactive protein; ALT: alanine aminotransferase; eGFR: estimated glomerular filtration rate.
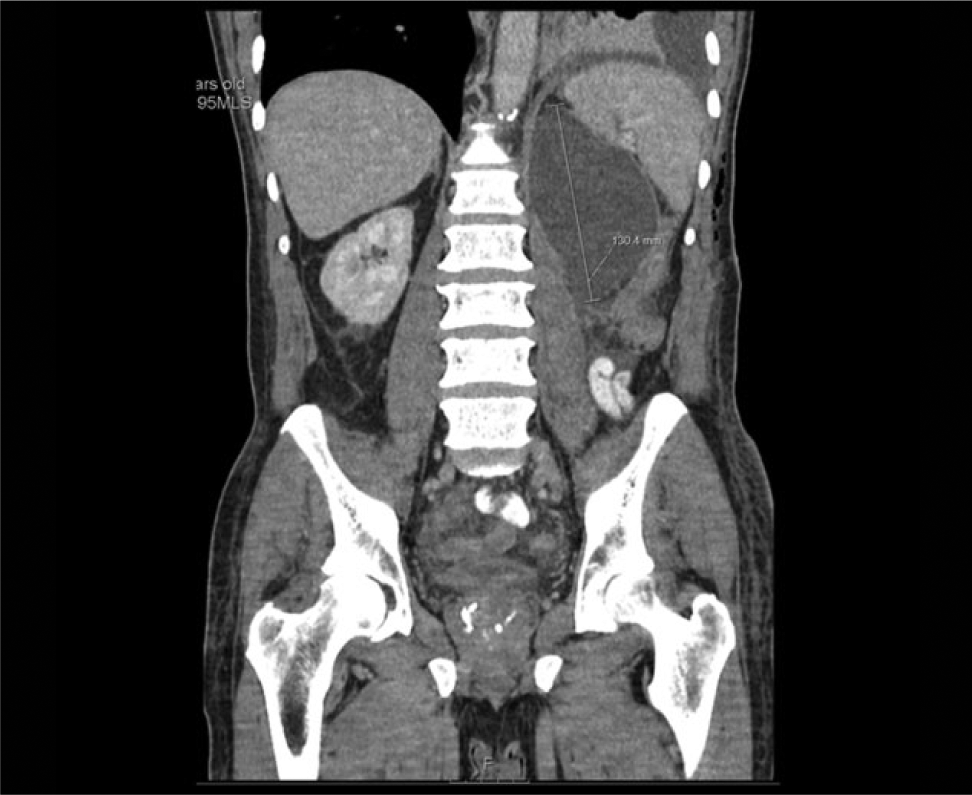
Computed tomography(CT) showing pseudocyst which was initially thought to be haematoma.

Postoperative computed tomography (CT) showing evidence of pancreatitis.
The second patient was a 72-year-old man with urolithiasis referred for nephrectomy for a large pelvico-ureteric junction (PUJ) stone (shown in Figure 4), associated with a large renal collection which had previously been managed with a failed stenting procedure, and subsequent percutaneous drainage. He also had a T2N1 sigmoid tumour and underwent a laparoscopic low anterior resection at the same time as his laparoscopic left simple nephrectomy. His other comorbidities consisted of Type 2 diabetes mellitus and gastro-oesophageal reflux for which he was prescribed saxagliptin, gliclazide and omeprazole. He also did not drink any alcohol and had no history of gallstone disease. His postoperative CT showing the development of pancreatitis is shown in Figure 5. This was associated with an elevated serum amylase, which peaked at 418 U/l on Day 1 postoperatively, and fell back to normal levels by Day 3.

Preoperative computed tomography (CT).
Postoperative computed tomography (CT) showing pancreatitis.
Discussion
Pancreatic injuries are rare complications of laparoscopic urological surgery. Left-sided retroperitoneal nephrectomy is probably the commonest urological cause of such injuries. The close anatomical relationship of the left kidney to the distal pancreas and perinephric tissue reaction (inflammatory and/or desmoplastic), increase the potential for such an injury.
As far as we are aware, there are no previous reports of pancreatic pseudocyst development following laparoscopic nephrectomy. Pseudocysts are surrounded by non-epithelialised fibrous and granulation tissue. They contain pancreatic enzymes, blood and necrotic tissue. Rupture results in a clinical emergency, and diagnosis is based on a high index of suspicion as symptoms are often non-specific with abdominal pain, pyrexia and vomiting predominating.
Conservative management was successful in both our patients; however, their postoperative recovery was significantly prolonged as a result of these complications. The operating surgeon in these two cases hypothesises that use of a fan retractor to elevate the pancreas in these difficult cases may have contributed to inadvertent pancreatic trauma, and thermal injury through the use of vessel sealant devices (LigaSureTM) may also play a role. Our technique has now been modified in light of this report.
Footnotes
Acknowledgements
The authors would like to thank the patients involved in these case presentations for allowing their anonymised data and images to be shared.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Guarantor
LS.
Contributorship
LZ and TD researched literature and conceived the paper. TD and TA were involved in collection of relevant clinical data. TD wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.