
Abstract
Objective:
This study aims to assess the use of primary X-ray beam collimation during ureteroscopy and its effect on patient radiation dose.
Methods:
A retrospective review of images and radiation doses of patients undergoing ureteroscopy.
Results:
The use of primary X-ray beam collimation during ureteroscopy is associated with lower radiation doses to the patient. Only 3% of images had evidence of collimation.
Introduction
Ureteroscopy is a common procedure in the United Kingdom, with >60,000 performed annually. 1 European Association of Urology guidelines state that fluoroscopy equipment should be available during every ureteroscopy. 2 Although the radiation dose absorbed by urologists is substantially lower than that of the patient, there are concerns regarding cumulative dose during a urologist’s career. 3 Median X-ray dose during a ureteroscopy case on non-obese males was estimated to be 1.13 mSv. 4 However, some studies of endourology cases have found patient exposures of up to 7.6 mSv. 5 Based on a patient dose of 1.13 mSv, the median calculated occupational dose from scattered X-ray radiation is 0.0113 mSv per case (or one abdomen X-ray dose per 100 cases). 6 Ureteroscopy is getting more complicated, cases are getting longer and patients BMI is increasing, all resulting in a dose to staff that is up to three times higher than this baseline.7,8 One study of an abdominal fluoroscopically guided procedure detected doses of up to 2.5 mSv to the operator. 9 Radiation dose to staff is expected to be proportional to the patient’s absorbed dose, although there is significant variation.3,9,10
Common radiation protection techniques for staff include increasing the distance from the X-ray source, shielding the body with lead aprons and keeping exposure time low.5,10,11 All of these contribute to the ALARA (as low as reasonably achievable) dose philosophy.10,11 In the UK, the majority of image intensifiers in theatres are operated by a radiographer. It is their responsibility as the operator to use their knowledge to keep the dose as low as possible whilst maintaining diagnostic image quality.11–13 In theatre, surgeons, radiographers and theatre staff should have knowledge of radiation protection techniques. Surgeons in theatre are acting as both the ‘requestor’ and occasionally the ‘operator’, and hence have responsibility for the protection of the patient and staff from radiation risks.
The set-up and placement of the image intensifier can affect the dose, and constant revision is required as a case evolves. Collimation of the primary beam is one method to reduce the dose (see Figures 1 and 2). Best practice guidelines state that it should be used at all times to reduce the primary beam size to that of the area of interest. 11 Collimation is achieved when electronically adjusted lead leaves are positioned to restrict the X-ray beam as it exits the tube housing. This in theory will reduce the radiation dose delivered to a patient and hence the occupational dose that staff receive.
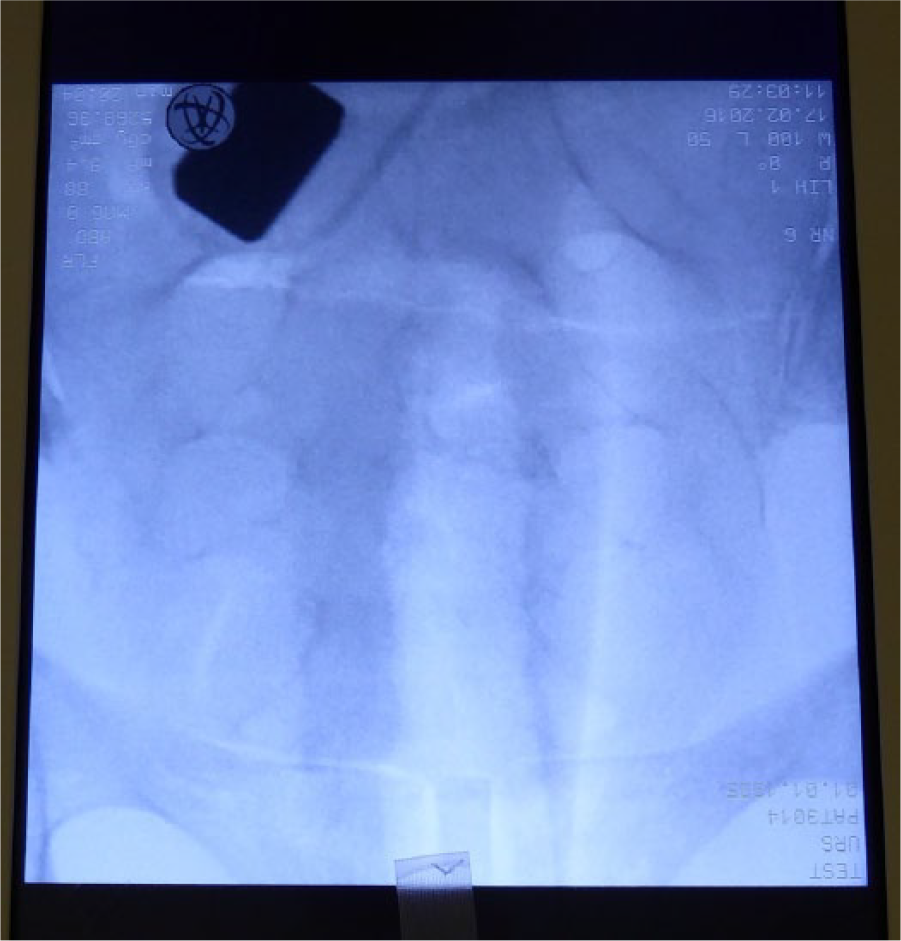
Image intensifier image of an anthropomorphic phantom pelvis without collimation.
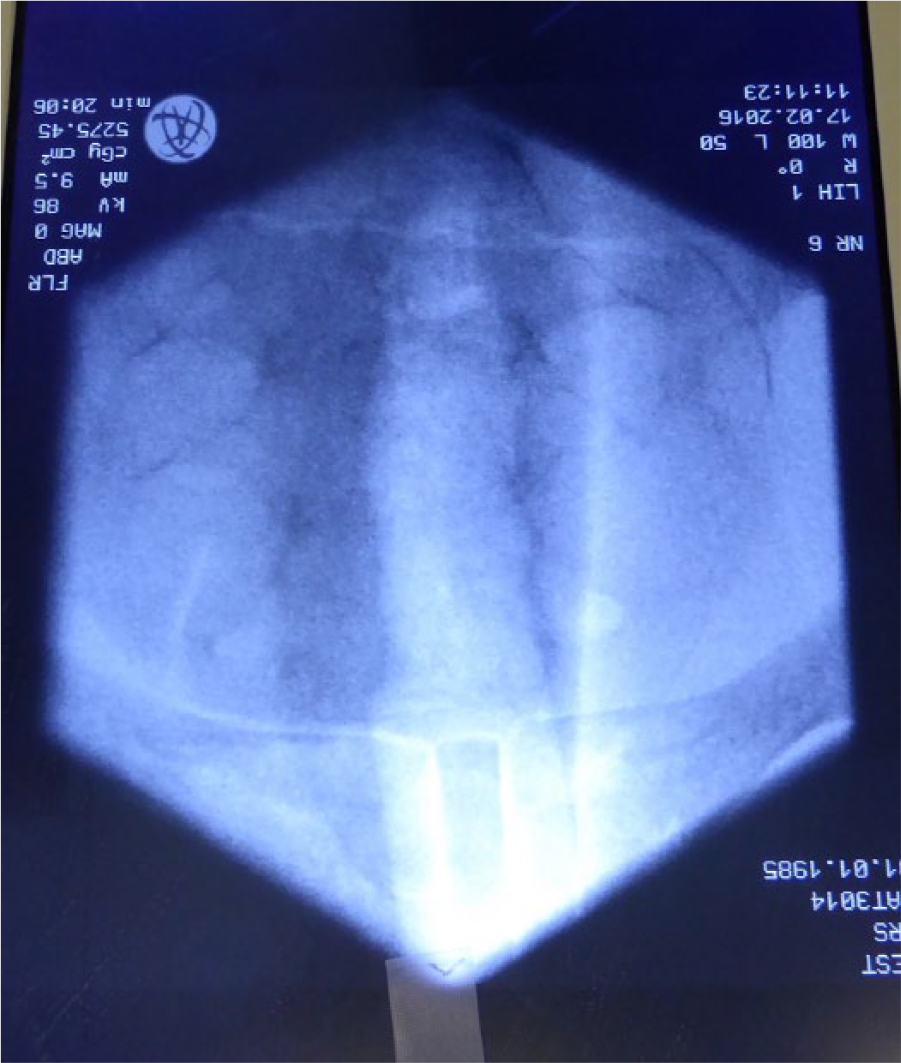
Image intensifier image of an anthropomorphic phantom pelvis with collimation.
This study aims to assess the use of collimation and its correlation with patient dose.
Methods
Patients undergoing ureteroscopy were identified through the hospital coding department. Picture archiving systems on Cerner Millennium were analysed for each patient. The number of images saved during the operation with and without collimation present was recorded. The electronic record of DAP (dose area product in cGy/cm2) and fluoroscopy time (seconds) were noted, and cGy/cm2/s was calculated. The number of images with collimation was divided by the total number of images for each patient. Medical records were analysed to note if the ureteroscopy procedure was for stone treatment or other pathology. For patients who had a ureteroscopy procedure for urolithiasis, the stone burden using the Denver Colorado S.T.O.N.E score, 14 side of procedure, type of ureteroscope used and degree of stone clearance were recorded from online records.
Dose as cGy/cm2/s was correlated with the percentage of images with collimation, S.T.O.N.E score and percentage of images with foreign bodies using the Spearman rank coefficient. Comparison of the dose with stone clearance and grade of surgeon was tested using an unpaired t-test.
Results
All patients undergoing ureteroscopy for any indication between June 2013 and May 2015 were included. Of the 260 patients, two-thirds were male. The median age was 59.5 years (range 17–94 years).
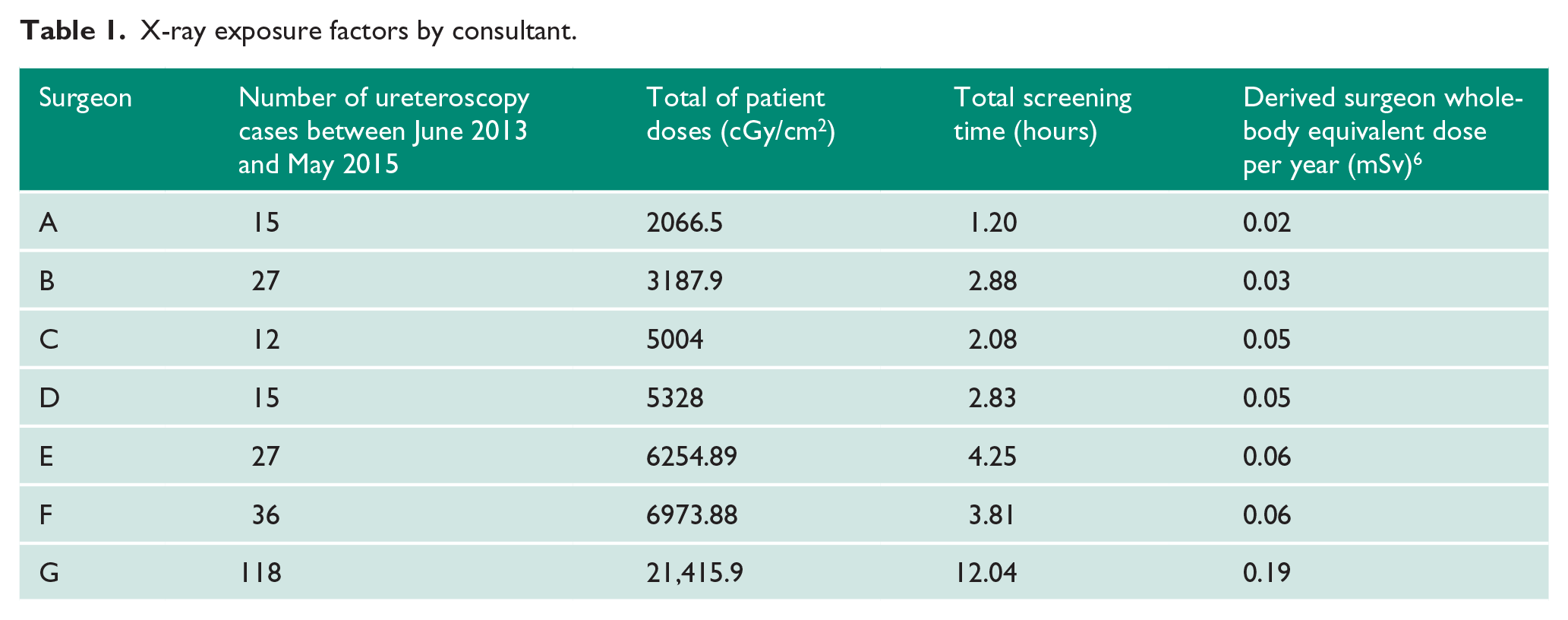
An image intensifier was used in 96% of cases. Eleven cases did not use an image intensifier. Six cases were emergencies, and the remaining cases were for imaging of the distal ureter following bladder tumour resection. A total of 206 (79%) procedures were performed for stones, 39 (15%) for tumours, and the remaining 11 (6%) for strictures, RPF and trauma. Procedures were performed bilaterally on seven patients (3%), on the right for 114 (44%) and on the left for 137 (53%). A flexible scope was used in 15 (6%), semi-rigid ureteroscope in 151 (59%) and both scopes were used in 92 (36%). Consultants performed 76% of procedures, and trainees performed 24%. Table 1 demonstrates the cumulative exposure factors split per consultant and the derived occupational dose.
X-ray exposure factors by consultant.
The median number of images saved during an operation was four (range 0–29), and the median number with collimation was 0 (range 0–6). When all images in this study were assessed, 3% had evidence of primary beam collimation (n=1229). Images had evidence of unnecessary foreign bodies (hands, table, etc.) on 11% of those assessed.
Stone burden as assessed by the S.T.O.N.E score; the mean score was 6.9 on the right and 7.6 on the left (range 0–15 bilaterally). Stone clearance was clinically assessed as complete in 71% of ureteroscopies. This rate of stone clearance is lower than the 86% quoted in the published literature. 15 When managing ureteric stones, retropulsion or synchronous intra-renal stones may require adjuvant procedures, as some consultants in the unit do not perform flexible ureteroscopy. When the data were reanalysed, the median operating time in the complete clearance group was found to be lower than in the incomplete clearance group (47 vs. 65 minutes; p=0.013). This suggests that there is a threshold past which surgeons favour repeat procedures to avoid prolonged ureteroscopy.
The median screening time was 36 seconds (range 0–474 seconds; n=165). Median DAP was 169 cGy/cm2 (range 0–3651 cGy/cm2; n=174). Not all patients had complete records of exposure factors. The median dose per second was 5.72 cGy/cm2/s (range 0.00–23.5 cGy/cm2/s; n=134). Spearman rank score was r=−0.19491 (p=0.032), demonstrating a weak but statistically significant relationship between cGy/cm2/s and the percentage of each patients images that were collimated. There was no correlation between dose when compared with the S.T.O.N.E score (Spearman rank score=0.18) or the presence of foreign bodies (Spearman rank score-0.08). Derived surgeon dose correlates with caseload (Spearman rank score=0.97). 6 An unpaired t-test did not demonstrate a significant difference in mean dose between patients who had ureteric or intra-renal procedures (p=0.48), complete or incomplete stone clearance (p=0.98) or grade of surgeon (p=0.87).
Discussion
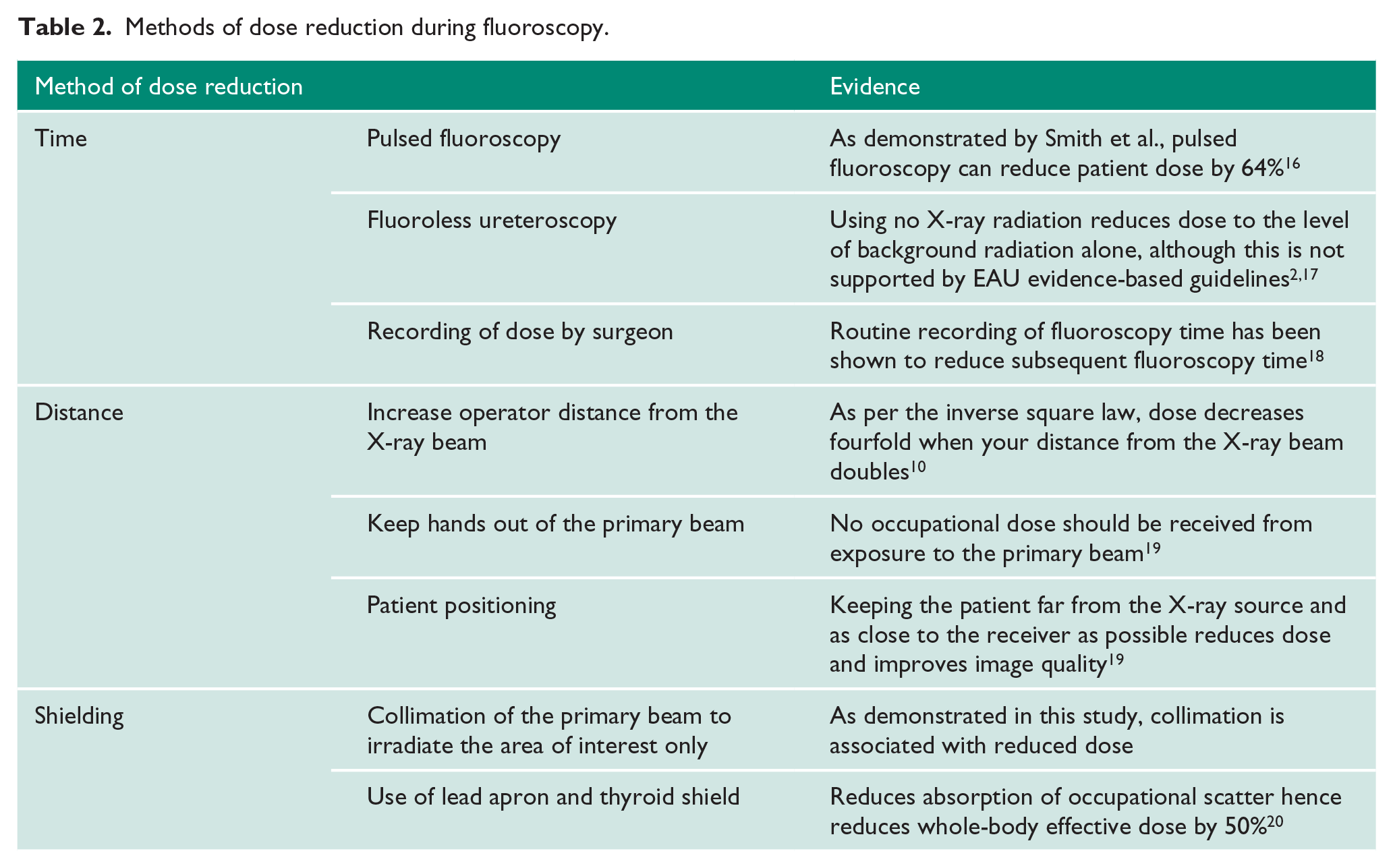
This preliminary study demonstrates a correlation between increasing use of collimation and decreased radiation dose during ureteroscopy. This is based on the retrospective presumption that the proportion of collimated images is reflective of the frequency of collimation use throughout the case. A well-designed prospective assessment of collimation use during an operation would allow for more accurate correlation with patient and staff dose. Collimation is therefore a method of shielding that should always be used. Table 2 demonstrates the methods that can be employed in urology to reduce X-ray dose during fluoroscopy.
methods of dose reduction during fluoroscopy.
The lack of correlation between the S.T.O.N.E. score and dose is surprising. Although the score was designed as a tool for predicting stone-free rates at ureteroscopy, it has been used in this study as a marker of stone burden. Surgical intent was not assessed in this study, and hence although stone burden may have been high, the procedure performed may not have intended to render the patient stone free in one sitting. The lack of correlation with grade of surgeon is also interesting. It is suggested that the electronic record of the performing surgeon is not correct, as the majority of lists in this institution would have a trainee operating. When the volume of cases is assessed per consultant, it is noted that exposures in this study would result in an approximate dose of 0.02–0.2 mSv a year to the operating consultant. This value is derived from calculations in interventional cardiology studies. It is suggested that in urology, surgeons are closer to the primary beam and that occupational dose may actually be higher than these derived values. Therefore, this advances the argument for occupational dosimetry studies to be performed focussing on urologists.
Although these data may reassure urologists that their occupational radiation dose is low, there is evidence that extrapolated organ doses from whole-body monitoring is inaccurate. 20 Many studies also demonstrate that knowledge of radiation protection and correct use of personal monitors is lacking.20,21 The staff dose in this study was not assessed, as personal monitors are seldom worn in the institution, and the shared nature of the monitors makes correlation with patient dose impossible. Further studies may benefit from real-time dosimetry assessment of case-by-case dose to staff. Patient doses are increasing, with a subsequent increase in occupational dose to staff. Attention to dose reduction is therefore important, and urologists can be proactive in this by working with radiographers to identify regions of interest on images and hence collimation limits. As urologists are technically acting as the justifier and occasionally the operator of exposure according to IR(ME)ER guidelines, there is a need for regular training on radiation safety and dose reduction.
Conclusion
This study demonstrates the correlation between increasing use of collimation and decreasing radiation dose. Increasing patient dose leads to increased occupational dose to staff. Attention to dose reduction is therefore critical. Further research should quantify both the dose rate urologists receive during ureteroscopy and the dose reduction achieved using the techniques discussed.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Informed consent for patient information to be published in this article was not obtained because this was a retrospective study of unidentifiable information.
Guarantor
BH.
Contributorship
BH researched and devised the study. BH, WB, SA and HC collected the data. BH wrote the manuscript, with additions by WB. All authors reviewed, edited and approved the final manuscript.