
Abstract
Proximal migration of stones during ureteroscopic lithotripsy is a common problem that faces many urologists and reduces stone-free rates, which translates into higher costs and longer operative times. In a bid to increase stone-free rates, there are several anti-retropulsion devices on the market, to help urologists during ureteroscopic lithotripsy. We previously reviewed these anti-retropulsion devices and wish to update what is currently available on the market.
Keywords
Introduction
Advances in endoscopic and intra-corporeal lithotripsy technology have made endoscopic treatment of urinary tract calculi commonplace and an effective treatment. 1 The use of ureteroscopy is rapidly eclipsing other modalities of treatment across the world,2,3 supported by high-quality evidence showing higher stone-free rates and lower retreatment rates, compared to extracorporeal shock wave lithotripsy. 4 Proximal migration of stones during ureteroscopic lithotripsy is a common problem that faces many urologists and reduces stone-free rates. Stone retropulsion has been reported to occur in 5–40% of ureteroscopy cases. 5 Stone retropulsion most commonly occurs in dilated ureters, when high pressure irrigation is used. 6 Stone retropulsion results in increased operative times, as well as costs due to an increased need for flexible ureteroscopy. Furthermore, additional procedures may be required to treat residual migrated fragments, in order to render patients stone free. In a bid to minimise such occurrences, there are several anti-retropulsion devices on the market to help urologists overcome this problem during ureteroscopy. We previously reviewed these anti-retropulsion devices 7 and wish to update what is currently available on the market, including:
Mechanical wire basket;
Mechanical balloon basket; and
A gel-based plug.
Mechanical wire baskets
Mechanical wire baskets are currently the most common type of anti-retropulsion devices available commercially. These include devices such as: Stone Cone™ (Boston Scientific Corporation, Natick, MA, USA), Accordion™ (Accordion Medical, Indianapolis, IN, USA), Escape™ (Boston Scientific Corporation, Natick, MA, USA) and NTrap™ (Cook Medical, Bloomington, IN, USA). These mechanical baskets carry an additional advantage over other anti-retropulsion devices, as they can also be used to retrieve stone fragments once sufficiently small (by trawling), negating the need for a basket. Their use may therefore be more cost-effective.
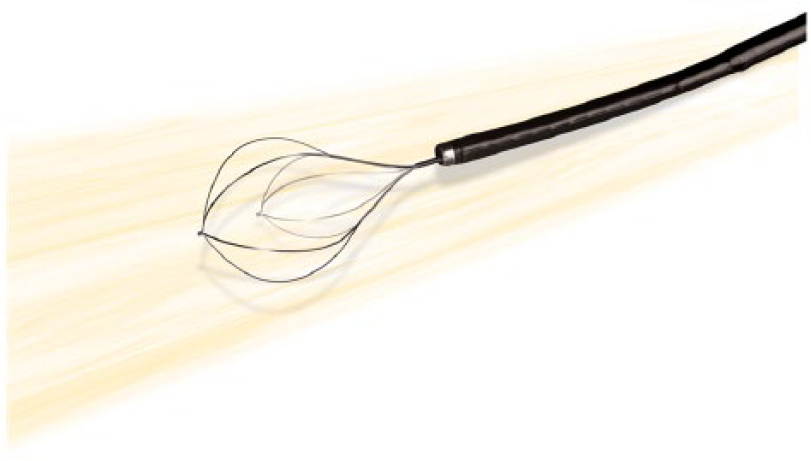
The Stone Cone™ (Figure 1) is a collapsible conical coil that is deployed above the stone in the ureter, prior to endoscopic lithotripsy. The coil of the Stone Cone™ contains an opening that allows fragments up to 3 mm to pass through. The coil of the device is available in either 7 mm or 10 mm. Compared to a flat wire basket, Desai et al. reported that 6 out of 50 patients had residual fragments < 3 mm and none required any auxiliary procedures. 5 A further retrospective review of the Stone Cone™ by Eisner et al. showed that only 2 out of 133 patients (1.5%) who had residual retropulsed fragments of > 2 mm required an additional procedure. 8 Of the 91 patients who were subsequently followed up after 3 years, none had ureteral strictures or hydronephrosis upon subsequent imaging. 8 This suggests that the Stone Cone™ is effective in preventing stone retropulsion during lithotripsy, with no adverse long-term effects on the ureter.

Stone Cone™ (Permission for use granted by Boston Scientific Corporation, Natick, MA, USA).
The Escape™ (Figure 2) is a 1.9 F zero-tip, four-wire nickel-titanium alloy (Nitinol) stone retrieval basket, which allows for concurrent stone basketing and lasering. There are two “open” positions for the Escape™ basket: In the standard position, it is 11 mm in diameter; and when fully opened, it can achieve a diameter of 15 mm, to entrap larger stones while lithotripsy is being performed. An advantage of the Escape™ basket over the Stone Cone™ and the NTrap™ basket is the use of the device through the same working channel of the ureteroscope, eliminating the need to have an additional instrument running next to the ureteroscope inside the ureter; however, as both laser fibre and basket are in the same ureteroscope channel, the position of the laser fibre could be restricted by the Escape™ basket and the irrigation flow could be severely reduced, resulting in poor visibility. 7 In a study by Kesler et al., 87% of the 23 patients who underwent ureteroscopic laser lithotripsy using the Escape basket became stone free. 9 Like any other Nitinol basket, laser damage can still occur, thus damaging the basket and in turn preventing proper closure and stone manipulation. 9 The Escape™ basket can also be used to transpose stones from the lower pole to the upper pole, when used during flexible uretero-renoscopy. It can be used as a regular basket to remove stones, as well as function as a holder to stabilize the stone during lithotripsy.
The Escape™ (Permission for use granted by Boston Scientific Corporation, Natick, MA, USA).
The Accordion™ (Figure 3) is a hydrophilic mechanical tool with a film occlusion that expands after negotiating past the stone, to prevent retropulsion of stones during endoscopic lithotripsy. Pagnani et al. reported that patients who were treated with the Accordion™ device experienced significantly less stone retropulsion during fragmentation, as compared to the control group (p = 0.0064). 10 Similarly, Wu et al. reported a significantly higher stone-free rate for the Accordion™ group, compared to the control group (84.2% versus 53.6%, p = 0.001). 11 Moreover, it is also more resistant to laser damage than the Stone Cone™ and NTrap™. 12 The radio-opaque ‘gold tip’ at the end of the device is easily seen on the X-ray image intensifier, making retrieval controlled. 13
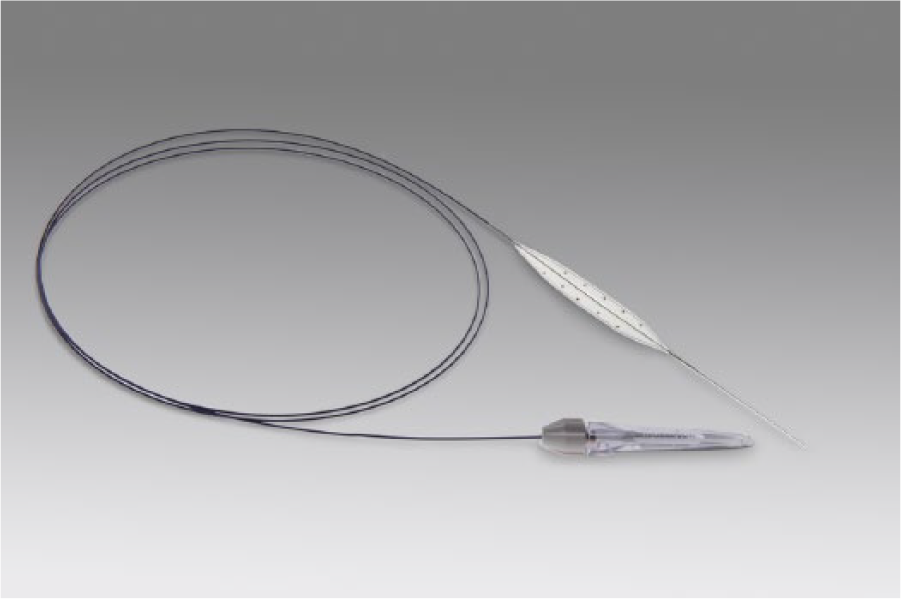
Accordion™ (Permission for use granted by Accordion Medical, Indianapolis, IN, USA).
The NTrap™ (Figure 4) basket is made of tightly woven mesh of “Nitinol” wires, consisting of an inner wire and an outer radio-opaque carrying catheter. The inner wire is a shape memory alloy that has a 7-mm umbrella-design basket. Han et al. and Lee et al. both report a very positive outcome, achieving a high stone-free rate whilst using NTrap™ following endoscopic lithotripsy using pneumatic lithoclast and a holmium:YAG laser lithotripter, respectively.14,15 A randomized trial of NTrap™ by Wang et al. also concludes that the NTrap™ basket is an effective device in reducing the occurrence of stone retropulsion during ureteroscopic lithotripsy of a proximal ureteric stone; but they note that both operative time and analgesic consumption were significantly higher in the NTrap™ group than in the control group. 16

NTrap™ (Permission for use granted by Cook Medical, Bloomington, IN, USA).
In another randomized controlled trial comparing NTrap™ and Stone Cone™, Faharat et al. show that Stone Cone™ significantly lowers rates of retropulsion during semi-rigid ureteroscopy with pneumatic lithotripsy. 17 Out of 180 patients, 63 were randomized to Stone Cone™, 59 to NTrap™ and 5 patients had no device as a control group. The stone-free rates were 95%, 83% and 72%, respectively (p < 0.05). The rate of secondary procedures required was highest in the control group, at 28%, and lower in the NTrap™ group, at 17%; but lowest in the Stone Cone™ group, at 5%. This may provide evidence that the Stone Cone™ was slightly better at preventing stone migration and improving the stone-free rate.
XenX™ (Rocamed, Monte Carlo, Monaco) is the latest anti-retropulsion device on the market that can be found in the literature (Figure 5). It is a multifunctional device: it functions as a normal hydrophilic guidewire when it is closed, and as a “Nitinol” ureteral mesh when it is opened. A small sample size of 15 patients, in a study conducted by Montanri et al., 18 achieved 93% stone-free status without any complications, using XenX™. More recently, Sanguedolce et al. 19 have published a multicentric comparative study on XenX™. In their study, they managed to achieve a 100% stone-free rate intraoperatively with XenX™ in 41 patients; and an 85.4% stone-free rate intraopreatively in the control group of 41 patients (p = 0.017), across nine centres in Europe. As XenX™ was only introduced in 2012, at present there are insufficient clinical trials to comment on its clinical significance and efficacy.
XenX™ (Permission for use granted by Rocamed, Monte Carlo, Monaco).
Mechanical balloon basket
The Passport™ balloon (Boston Scientific Corporation, Natick, MA, USA) is the only mechanical balloon basket on the market (Figure 6). Although the Passport™ balloon is designed primarily as a ureteric dilation balloon, it has been used as an anti-retropulsion device by urologists. It has a balloon dilation catheter mounted on a guide wire. Once it has been negotiated past the ureteric stone, the balloon is inflated to prevent stone retropulsion. Although the balloon dilation catheter is only 3F, one study showed that the failure rate of advancing the balloon dilation catheter could be as high as 31%. 20

Passport™ balloon (Permission for use granted by Boston Scientific Corporation, Natick, MA, USA).
Lidocaine gel-based plug
This anti-retropulsion device utilizes lidocaine jelly as a plug to prevent stone migration. After the procedure, the gel is flushed out with saline irrigation or it is allowed to slowly dissolve over time and be eliminated in the urine.
Ali et al. described the use of lubricant jelly proximal to the stone, before performing lithotripsy through a 6F ureteral catheter inserted through the ureteroscope, to reduce the rate of stone retropulsion. 21 This novel, but off-label use for lubricant jelly was effective in all seven patients described: their stone-free rate was 100%. Zehri et al. 22 performed a randomised clinical trial of lidocaine jelly in 25 patients, and only one stone retropulsion was observed (4%) under those conditions, compared with 28% in the control group. The stone-free rate was significantly higher in the lidocaine jelly group (96%) versus the control group (72%; p = 0.045). One drawback of using lidocaine jelly as an anti-retropulsion mechanism is that the jelly could potentially obscure the view of the surgeon during ureteroscopy. Further studies conducted by Bastawisy et al. 23 and Sen et al. 24 compared the lidocaine method to anti-retropulsion devices, such as the Stone Cone™ and the Accordion™. They concluded that lidocaine jelly was not superior to the Stone Cone™ nor Accordion™ in terms of preventing stone migration, decreasing the stone-free rate, operative time and the need for auxiliary procedures.23,24
BackStop™ (Boston Scientific Corporation, Natick, MA, USA) is a reverse-thermosensitive dissolvable polymer that is deployed proximally to the ureteric stone. At body temperature, it turns to a gel and blocks the ureter beyond the ureteric stone temporarily, to prevent retropulsion of stone fragments during ureteroscopic lithotripsy. After stone fragmentation and extraction of fragments are completed, the polymer is easily dissolved by room temperature saline irrigation and flushed out, rendering the ureter patent again. Rane et al. 25 reported the first randomised study trial on BackStop™. In this study, they managed to decrease retropulsion from 60% in controls to 15%, with no intra-operative complications noted. 25 Similarly, Molina et al. 26 also report no intra-operative complication with BackStop™. Furthermore, all their patients were rendered stone free; 26 however, as of January 2016, distribution of BackStop™ was ceased.
Discussion
The fact that there are so many devices and on differing themes clearly indicates that there is no ideal device that can be used in all patients and situations. The endourologist needs practice in keeping the devices in place, as any lack of concentration can make the device go back to the kidney along with the stone. Like in all surgical procedures, practice makes deployment and successful fragmentation of the stone easier.
Cost is an important factor in considering anti-retropulsion devices. Ursiny et al. 27 did a cost-effectiveness analysis on all commercially available anti-retropulsion devices in the USA. They conclude that devices are considered cost-effective if the retropulsion rate is ⩾ 6.3%. Their estimation was based on retropulsion rates of 1.9% with devices and 16.3% without devices; that the average cost of an anti-retropulsion device was US$278; and that the cost of secondary procedures such as shockwave lithotripsy was US$5290 and ureteroscopy was US$6390.
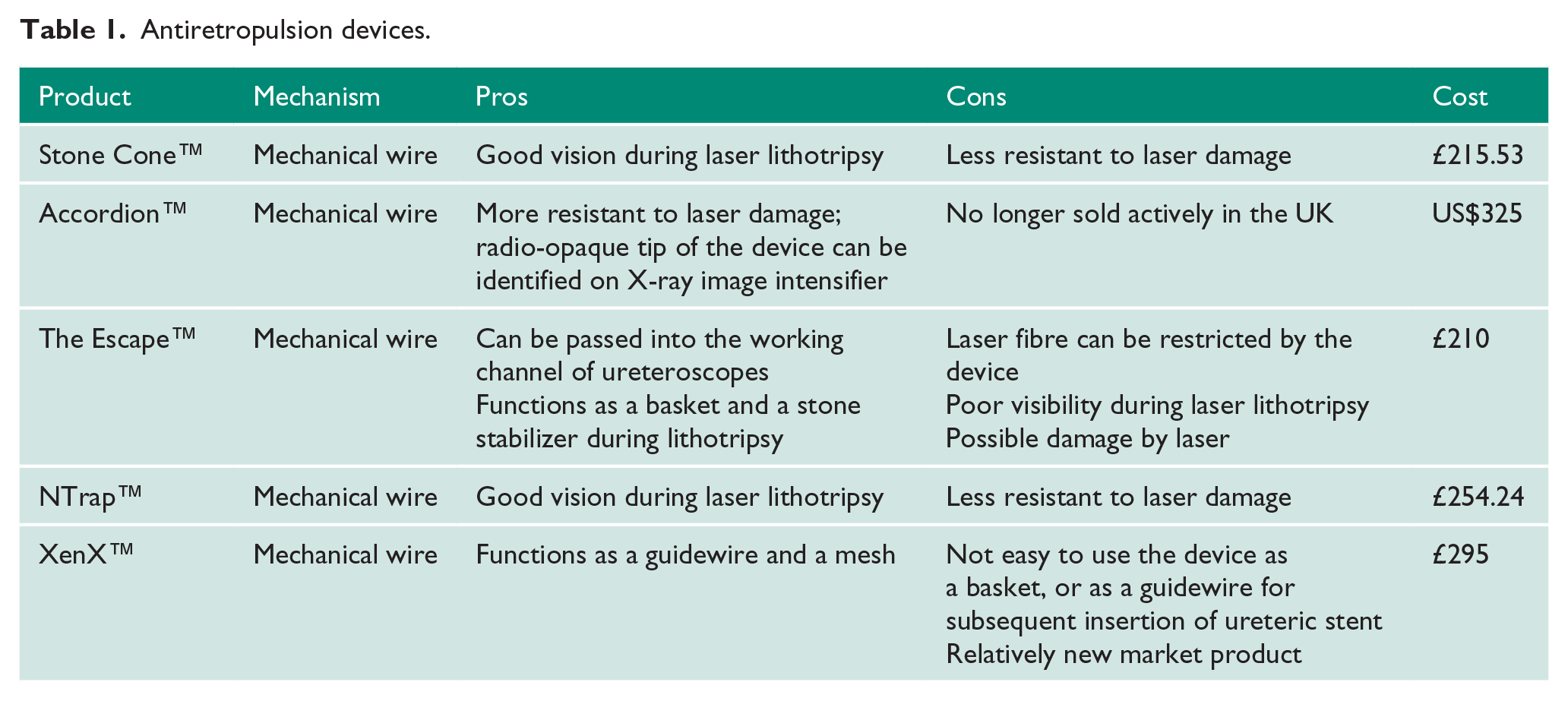
The UK cost of each anti-retropulsion device is shown in Table 1. The choice of anti-retropulsion device ultimately depends on the experience and familiarity of the endourologists.
Antiretropulsion devices.
In their study comparing XenX™ with the standard ureteroscope control group, Sanguedolce et al. 19 found that although it was about £34 more expensive to use XenX™ than not in the control group at the time of the procedure, on average, the latter was more likely to incur a higher cost. This is because the control group is more likely to require further procedures to achieve a stone-free status, require ureteric stents, and require more analgesia to relieve the patients’ stent symptoms; all of which will translate into costs. 19
In institutions where flexible ureteroscopes are not readily available, deploying anti-retropulsion devices has obvious benefits. It was shown that anti-retropulsion devices can reduce operative time, the need for ureteric stenting and the need for further procedures, while they increase stone-free rates; 16 however, it cannot be emphasized enough that a modern comprehensive stone unit should always have a flexible urterorenoscope ready, along with a Holmium laser, as stones can easily go back into the kidney irrespective of the devices used, and these may need fragmentation and retrieval in order to avoid another procedure in the patient.
Conclusions
Each anti-retropulsion device has a specific set of advantages and disadvantages. An ideal anti-retropulsion device should be one that not only serves the purpose of preventing fragment migration proximally, but it should also be easy to use and deploy, as well as concurrently allowing the safe passage of working instruments, such as laser fibers, guide wires and stents. More importantly, such a device should be relatively inexpensive and accessible. The search for a perfect anti-retropulsion device continues.
Footnotes
Acknowledgements
We would like to thank Boston Scientific Corporation, Accordion Medical, Cook Medical and Rocamed for supplying us with the photos of their antiretropulsion devices.
Conflicting interests
BHC is a consultant for Bard Medical, Boston Scientific Corp, Cook Medical, Olympus Medical, and ADVA-Tec. The other authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
YCP.
Contributorship
YCP did the literature search and wrote the first draft. SuS and BHC edited the first draft. SeS edited the second draft. AR supervised the team. All authors reviewed and edited the manuscript and approved the final version of the manuscript.