
Abstract

Background
Bladder rupture is rare, but most common when the bladder is distended. It is often associated with synchronous major traumatic injuries. 1 A retrograde cystogram is a sensitive and specific procedure for confirming bladder rupture and is considered the gold standard for diagnosis. 2 CT cystography has been shown to have comparable levels of accuracy as conventional fluoroscopy and can be incorporated within a trauma-focussed CT scan. 3 We report a case of retrograde cystography failing to demonstrate an intraperitoneal bladder rupture that later became apparent.
Case report
A 21-year-old female presented to the Emergency Department with a history of lower abdominal pain and frank haematuria following low-velocity, blunt trauma to the lower abdomen when she fell inebriated from her partner’s shoulders. She had no significant past medical history, and was catheterised on admission on account of the haematuria. The catheter drained 700 ml of clear urine. She was haemodynamically stable and her routine blood tests were within normal parameters. Her abdomen was soft and non-tender and, other than mild bruising of her genitalia (onto which she had fallen), examination was unremarkable.
She underwent a retrograde cystogram within 4 h of admission, to determine if any significant bladder injury was evident. Anterioposterior and lateral views were obtained (Figure 1).
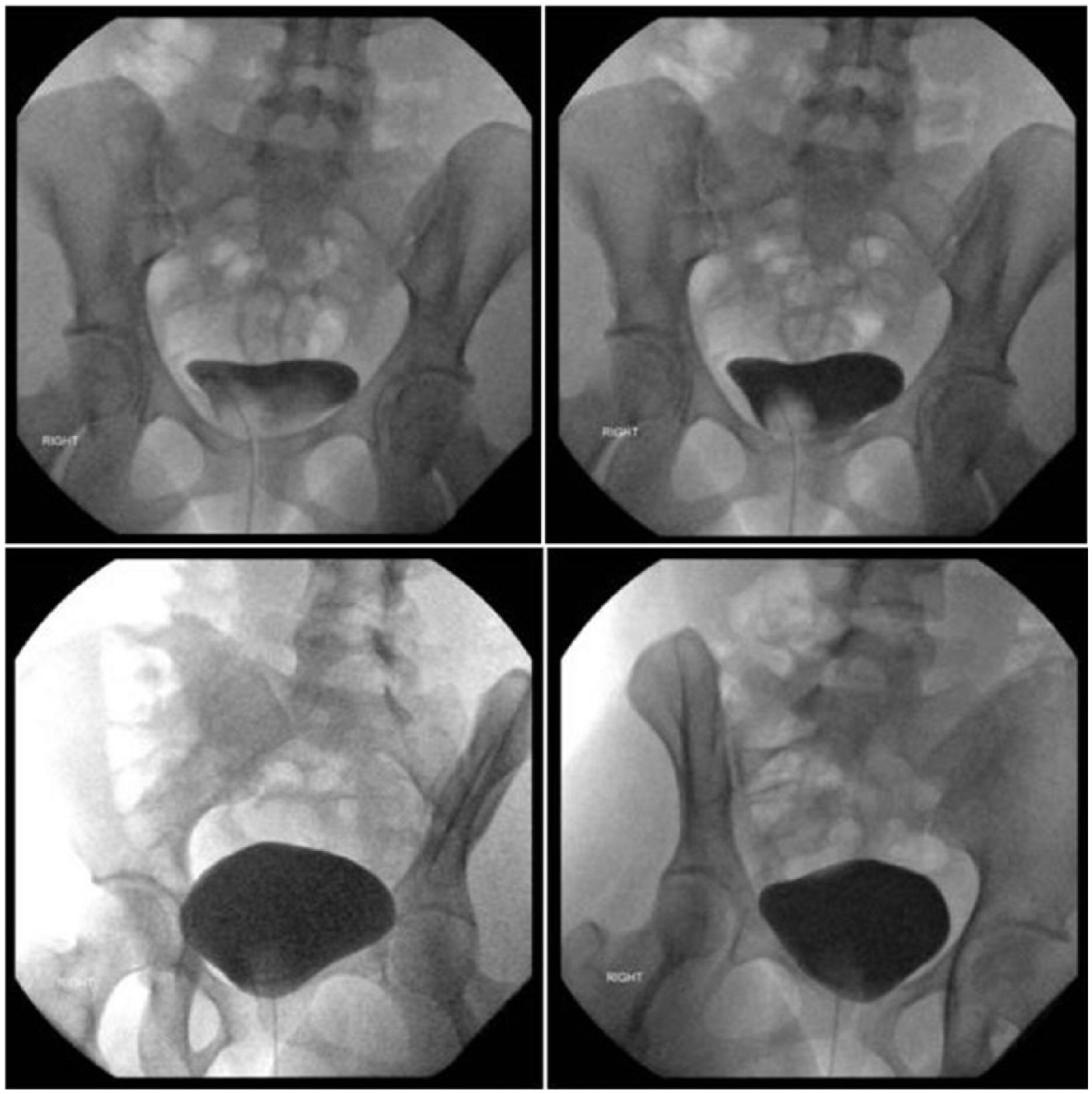
This patient’s conventional retrograde cystogram showing bladder filled with 350 ml of contrast and no leakage.
The consultant radiologist’s confirmatory report stated that there was “no evidence of bladder rupture”. No other imaging was performed and she was discharged with a urethral catheter because of periurethral bruising. She was readmitted to the day ward 2 days later for catheter removal. Shortly after catheter removal she complained of worsening lower abdominal pain and was transferred to the acute admissions unit for reassessment.
On review, her abdomen was peritonitic, and a CT scan of the abdomen and pelvis demonstrated free fluid in her abdomen with a small amount of pneumoperitoneum, but with no obvious damage to the bladder or any other specific organ. The general surgeon on-call performed a laparotomy with the expectation of finding a bowel perforation (postulated to be caused by an ischaemic crush injury). Instead, a 3 cm rent in the dome of the bladder was discovered. It was repaired and her recovery was uneventful.
Discussion
Retrograde cystography is well established and regarded as the gold standard diagnostic tool in the diagnosis of bladder injury.2,3 Many patients in whom bladder rupture is clinically suspected present with polytrauma and undergo abdominopelvic CT imaging. They often have deranged bloods, specifically elevated creatinine in the presence of an intraperitoneal urine leak.4,5
In this case, the patient was systemically well throughout her initial admission, with mild bruising of her genitalia being the only clinical abnormality. Her haematuria resolved immediately and there was no abdominal tenderness, hence conventional cystography was performed to minimise radiation exposure. CT imaging should have been obtained given the initial presentation, despite the rapidly resolving clinical picture; the case highlights that this approach should be adopted, as retrograde cystography is fallible and can provide false reassurance in failing to demonstrate a bladder rupture.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Our institution does not require ethical approval for reporting individual cases.
Informed consent
Verbal informed consent was obtained from the patient for their anonymised information to be published in this article.
Guarantor
PAJ.
Contributorship
MDHS and SDL reviewed the literature and wrote the first draft of the report. PAJ reviewed and edited the report.