
Abstract

Introduction
Melanosis bladder is a rare cause of pigmented urothelium. Presenting symptoms vary, and can include non-visible haematuria and offensive-smelling urine. A distinctive discolouration of the urothelium is seen at cystoscopy. The diagnosis is made from histological analysis of bladder biopsy specimens. We describe two cases of melanosis bladder managed in our institution, review other reported cases and suggest a follow-up strategy comprising annual cystoscopy.
Case 1
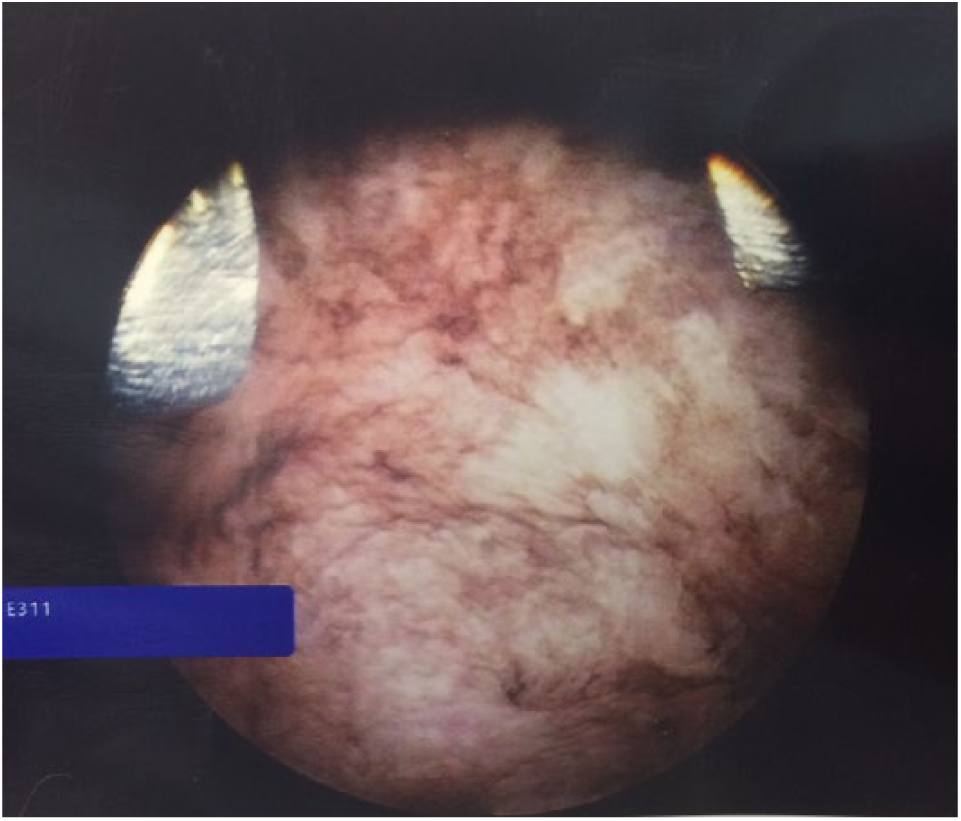
A 45-year-old man presented via his general practitioner with storage lower urinary tract symptoms and recurrent episodes of sterile pyuria. A flexible cystoscopy revealed black deposits throughout the bladder (Figure 1). Biopsies taken at rigid cystoscopy confirmed melanosis of the bladder. As part of the histological investigations, Masson Fontana staining for melanin was positive. After staining with melanin bleach, the Masson Fontana stain was repeated, and found to be negative, confirming the pigmentation was melanin. Perl’s stain for iron was negative.

Cystoscopic appearance of melanosis bladder.
Further biopsies of bladder mucosa taken at the same procedure confirmed normal urothelium with foci of keratinizing squamous metaplasia, with lymphoid aggregates and chronic inflammation of the lamina propria.
He is being followed up with annual flexible cystoscopic surveillance.
Case 2
A 78-year-old woman presented with offensive-smelling urine with negative mid-stream urine cultures, and non-visible haematuria. There was no relevant medical history. Black discolouration was noted throughout the bladder at cystoscopy (Figure 2). Histological analysis of the urothelium showed pigment, positive for melanin on Masson Fontana staining (Figures 3 and 4), and negative for iron staining, consistent with melanosis bladder. Bleaching with hydrogen peroxide removed the melanin (Figure 5). No melanocytes were seen in the bladder biopsies.
Cystoscopic appearance of melanosis bladder.
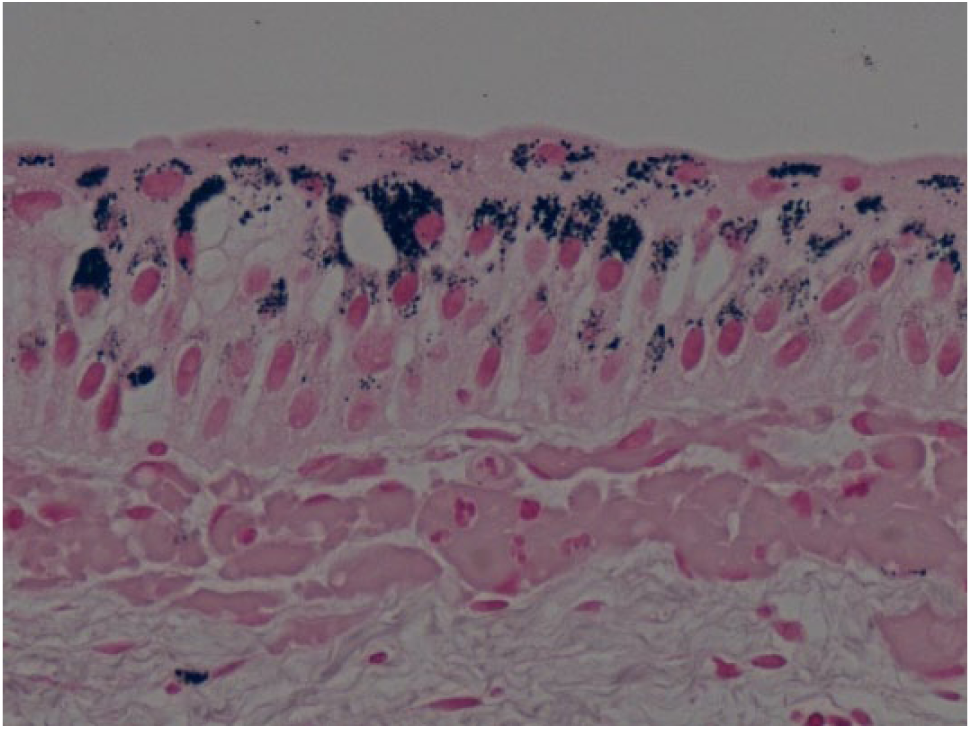
Masson Fontana staining revealed melanin within the urothelium.
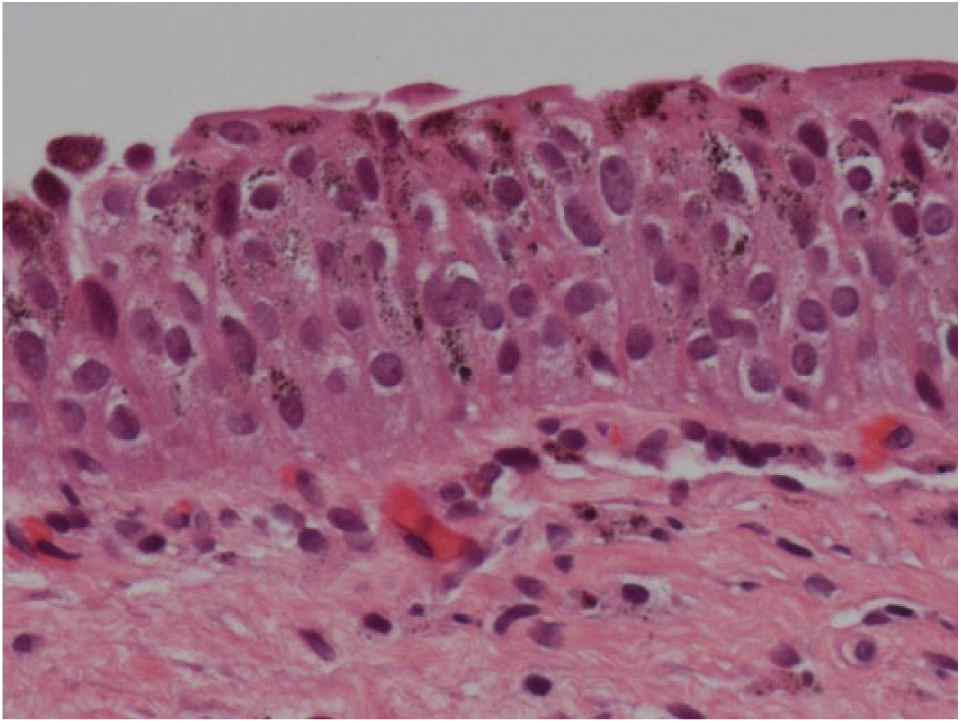
Haematoxylin and eosin staining revealed melanin within the urothelium.
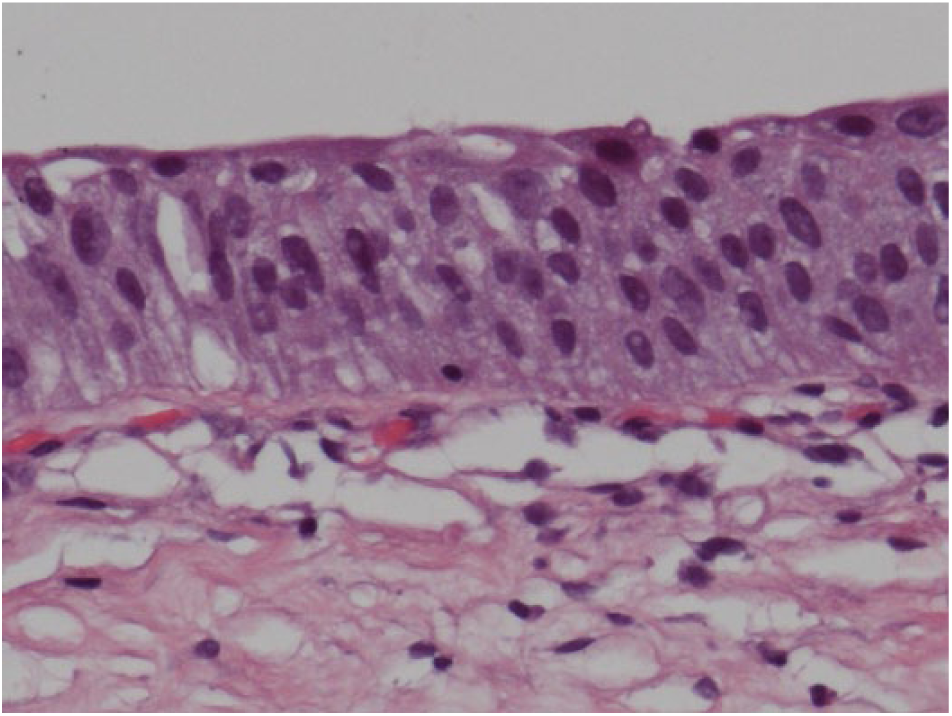
Bleaching with hydrogen peroxide removed the melanin deposition, helping confirm the diagnosis of melanosis bladder.
Her symptoms of offensive urine resolved spontaneously. She is also being followed up with annual flexible cystoscopic surveillance.
Discussion
Melanosis bladder is a rare condition; a PubMed search for ‘melanosis bladder’ or ‘melanosis vesica’ yielded only 18 other cases. Many of these have been detailed previously. 1
Presenting features leading to cystoscopy may include haematuria, 2 overactive bladder symptoms including urge incontinence 3 and dysuria and offensive-smelling urine, 4 similar to Case 2 in our series.
In some cases it has been found associated with urothelial carcinoma at presentation. 5
The putative causes of bladder melanosis include the migration of cells from the neural crest during embryonic development, or metaplasia of the bladder urothelium. 6 Whilst these are only speculative, it is interesting that there was evidence of squamous metaplasia seen in our first case. It is not clear whether this is a related finding and does not seem to have been reported elsewhere.
The differential diagnosis includes malignant melanoma of the bladder, 5 so biopsy is essential. Haemosiderin and lipochrome deposits can also give a similar macroscopic appearance.
Appropriate histological stains help with diagnosis.5,6 Haematoxylin and eosin staining cannot discriminate between the differential diagnoses identified. Staining with Masson Fontana will turn melanin pigment black. Subsequent bleaching, e.g. with hydrogen peroxide, will remove melanin, helping confirm the diagnosis. Perl’s iron stain will turn haemosiderin blue. As in our case, these stains were all used to help identify melanosis.
As this is such a rare entity, formal surveillance guidelines are lacking. Given there have been reports of an association of melanosis bladder and high-grade bladder transitional cell carcinoma, we are performing annual cystoscopic surveillance for our patients, and other groups are doing similar,1,5 with some also surveying the upper tracts.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from both patients for their anonymised information to be published in this article.
Guarantor
ET.
Contributorship
ET wrote the article and performed the literature review. JO commented on the histological findings, and provided the histological slide. FQ was the senior author. All authors have reviewed the final manuscript.