
Abstract
Introduction:
The aim of this regional audit was to gain an understanding of the different approaches to prostate cancer diagnosis across the northwest of England. This often complicated area of urological practice has undergone many changes in recent years and this audit will attempt to evaluate the degree of diversity in diagnostic pathway across one region.
Methods:
Electronic questionnaires were distributed to consultant urologists across the northwest. Over a 2-week data collection period 48 responses were received from 19 urology units. Responses were grouped by centre to evaluate practice per urology unit.
Results:
Written consent was taken for transrectal ultrasound and biopsy in 54% of centres. All centres used a prophylactic antibiotic regime that included ciprofloxacin; however, the duration varied across the region. Units used a 3-day course, 1-day course and single dose at the time of biopsy in 69%, 5% and 21%, respectively. Rectal swabs to detect fluoroquinolone-resistant organisms were not used in 15 of 19 units (79%). Magnetic resonance imaging was not used before the first biopsy in 42% of units. Twenty-one per cent used this study on all men undergoing a first biopsy, while 37% of centres used a more targeted approach. All centres routinely sampled 12 cores during TRUS and biopsy. The majority (74%) sent cores for histology in two containers by side (left/right). The remaining sent two samples from each geographical area in one container. For repeat biopsy indications 42% of units reported they would proceed straight to transrectal ultrasound and biopsy. The remaining 58% utilised another modality such as multiparametric magnetic resonance imaging or transperineal template biopsy in the first instance.
Conclusion:
This audit has highlighted a wide variation in practice within one UK region. Although there have been measurable advances in prostate cancer management, more standardisation of diagnostic pathways may facilitate data collection and reduce variation in outcomes.
Level of evidence:
Not applicable in this multicentre audit.
Keywords
Introduction
The northwest of England has a population of 7.1 million residents and accounts for 13% of the population of England. It is the second most densely populated region after London. 1 It was, however, deemed significantly worse than the rest of England for 75% of the key indicators for health in 2012. 2 Consequently, men in the northwest will live 2.9 years less than their counterparts in the southeast of the country. 2
It is nevertheless encouraging that the mortality rate of prostate cancer has fallen year on year since 2000 despite the age standardised incidence increasing by 6.3% between 2004 and 2013.3,4 In the northwest there was an overall improvement, although it was of the smallest in magnitude in the UK. In our region, there was an 11% improvement in mortality between 1995 and 2009. By way of comparison the southeast showed an improvement of 22% in the same period, double that of the northwest. 4
There have clearly been measurable advances in the management of prostate cancer over the past decade. Many would argue that there is room for further improvement in order to bring the reduction in mortality in line with other regions. In addition, we hypothesise that there is still considerable variation in diagnostic pathways across our region despite the publication of key guidance documents.5,6
The aim of this audit was to gain an understanding of the different approaches to the diagnosis of prostate cancer across the northwest of England. This snapshot will allow us to take stock of current practices which have undergone considerable change in recent years. It will also act as a benchmark from which future studies can evaluate change.
Methods
Data collection and quality
Local practice was audited by way of an electronic questionnaire distributed to consultant urologists working within 19 units in the northwest region in November 2015. Two weeks were allowed for responses.
The questionnaire asked questions relevant to prostate cancer diagnosis and concentrated particularly on the following six domains: (a) patient information and documentation; (b) antibiotic prophylaxis; (c) pre-biopsy imaging protocols; (d) transrectal ultrasound (TRUS) and prostate biopsy: logistic details; (e) TRUS and prostate biopsy: technique; and (f) follow-up after a negative result and repeat investigations.
The electronic questionnaire was configured to encompass all responses and questions could be left unanswered.
Geographical area and institutions audited
Institutions ranged from large university teaching hospitals to smaller district general hospitals (Table 1). There was a range of inner city institutions and centres serving more rural areas. Geographically, the area was bordered north to south by the towns of Blackpool and Crewe; east to west the region ranged from Tameside to the Isle of Man.
Summary of key responses.
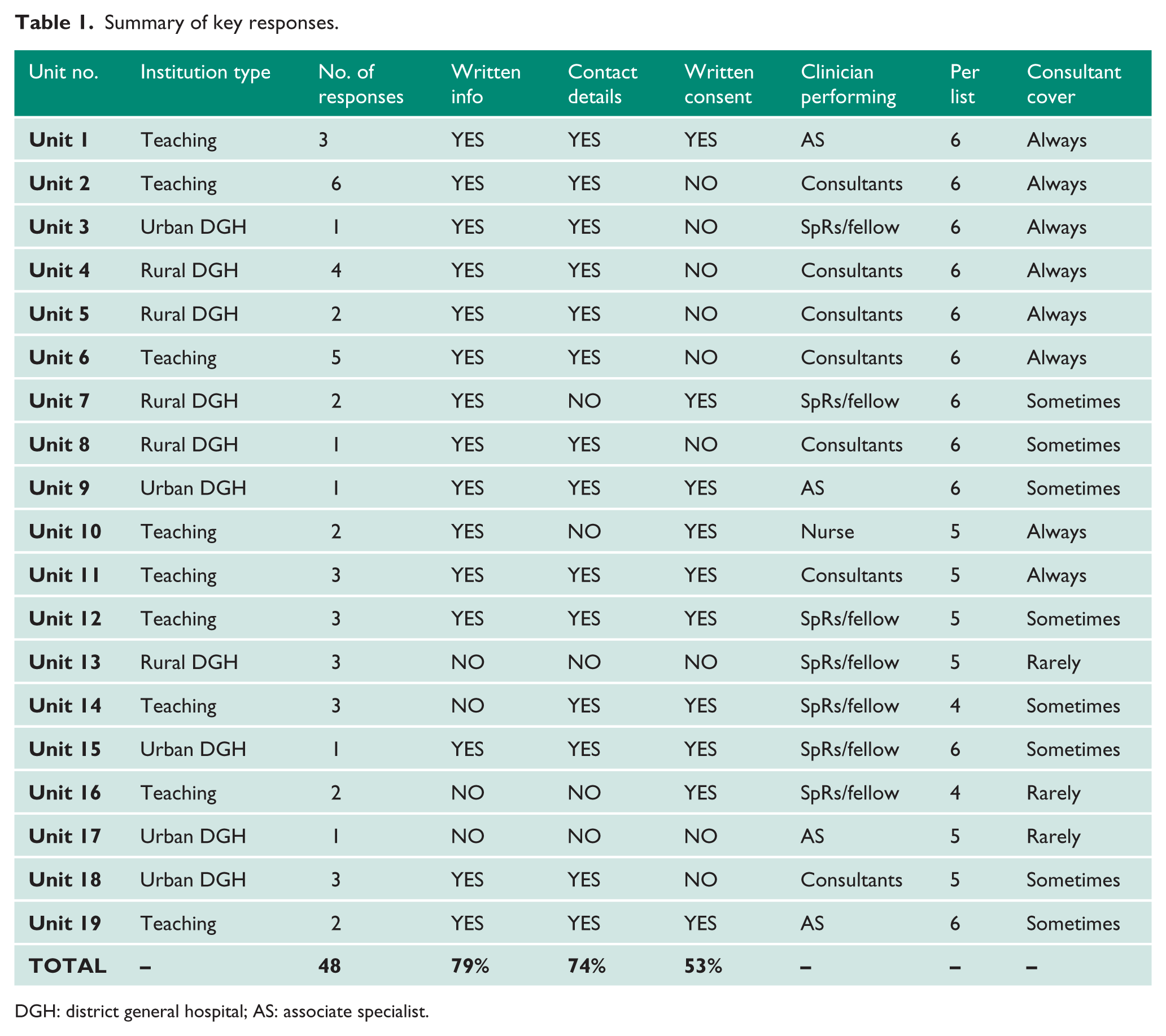
DGH: district general hospital; AS: associate specialist.
Data analysis
Individual consultant responses were grouped according to centre, and an average practice for that unit was determined and reported in this paper. There was little in the way of deviation in practice from consultants employed by the same institution, probably because of standardised multidisciplinary team pathways and protocols.
Informed consent and ethical approval
Informed consent and ethical approval were not sought for this audit. As this regional audit focuses on a consultant’s broad urological practice as opposed to individual patient data it was not deemed necessary.
Results
Data acquisition
At the end of the data collection period 48 individual consultants had responded. Responses were received from all 19 units (Table 1). The total number of consultants practising at each unit and the number specifically involved with prostate cancer diagnosis were not audited.
Patient information and documentation
Responses indicated that 79% of centres provided written information in the form of a patient information leaflet given to patients prior to undergoing prostate biopsy. The contact details of an appropriate healthcare professional who could be contacted in case of complications or concerns was included in all but five centres’ information packs (74%). Written consent was taken in 53% of centres (Table 1).
Antibiotic prophylaxis for TRUS and biopsy
All units prescribed prophylactic antibiotics for TRUS and biopsy and all units’ antibiotic regimes included ciprofloxacin. Ciprofloxacin was used in isolation in 42% of units, in combined with gentamicin in 32% and in combination with metronidazole in 10% of centres. Sixteen per cent of units used ciprofloxacin, gentamicin and metronidazole (Figure 1).
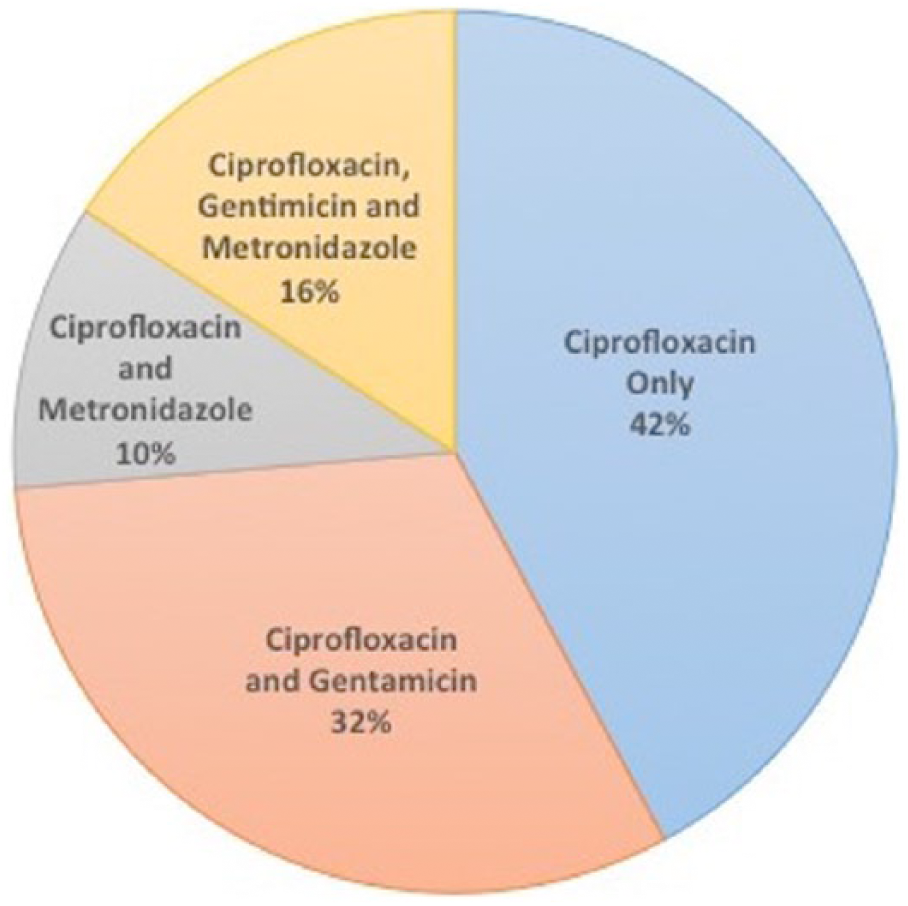
Pie chart to show the variation in prophylactic antibiotic regimes for transrectal ultrasound and biopsy across the region.
The dose of ciprofloxacin ranged from 500 mg (74%) to 750 mg (16%). Ten per cent of centres did not provide information on ciprofloxacin dose. The duration of ciprofloxacin post-procedure was audited. Most prescribed a 3-day course of ciprofloxacin (69%). A 1-day course was given in 5% of centres and a stat dose was administered in 21%. Five per cent of centres did not state the duration of ciprofloxacin. Centres started ciprofloxacin 1 day before biopsy, 1 hour before biopsy and at the time before biopsy in 16%, 63% and 16%, respectively. One unit (5%) did not provide this information.
Rectal swabs prior to TRUS and biopsy were performed in all patients at two units (11%). Two centres utilised rectal swabs in specific patients (11%), and the remaining 15 units (78%) did not perform rectal swabs at all.
Prostate cancer diagnostic imaging
Participants were asked whether patients underwent multiparametric magnetic resonance imaging (mpMRI) prior to initial prostatic biopsy. Responses indicated that 21% of centres performed a mpMRI prior to biopsy for all patients. A more targeted approach was utilised by 37% of centres who performed a mpMRI in patients who met a predefined selection criteria. This selection criteria was based around the patients’ suitability for radical treatment and those deemed to be high risk should cancer be confirmed. The majority of units (42%) did not perform prebiopsy mpMRI on any patient.
On-site imaging facilities were audited. The majority of units (89%) had a nuclear medicine department with provision for a bone scan on site. Only 11% of institutions had the facilities to provide positron emission tomography–computed tomography, the remainder (89%) referred patients to other trusts for this investigation.
TRUS and prostate biopsy: Logistic details
Biopsies take place in the outpatient department in 58% of centres. The remainder are performed in theatre/endoscopy unit (26%) or a specific procedures unit (16%). Responses indicated that most biopsies are performed equally by consultant urologists (37%) and middle grade doctors (specialist registrars or equivalent non-training grades) (37%). The remaining centres utilised associate specialists (21%) and 5% of centres had specialist nurses who routinely perform TRUS and biopsy.
The majority of units biopsy six patients per list (58%). The remaining centres perform five (32%) or four (10%) per list. A list was defined as a half-day session. One-stop clinics for prostate biopsy were offered by 37% of units in our region.
When asked if there was consultant cover available during a biopsy list, 47% of centres indicated they always had cover, 16% sometimes had cover and 37% rarely had cover (Table 1). Consultant cover was defined as a consultant present within the department for the duration of the biopsy list. All units performed biopsies on specific TRUS and prostate biopsy lists, and four (21%) units had the capacity to provide biopsy lists dedicated to 2-week rule referrals.
TRUS and prostate biopsy: technique
All centres routinely sampled 12 cores during TRUS and biopsy. Samples were sent by side (i.e. six cores from the left in one container and six cores from the right in a second container) in 74% of centres. The remaining 24% of centres sent two cores in a container for each of six geographical areas of the prostate (i.e. left base, left mid-zone, left apex and right base, right mid-zone, right apex). No unit sent each core in a separate container (Figure 2).
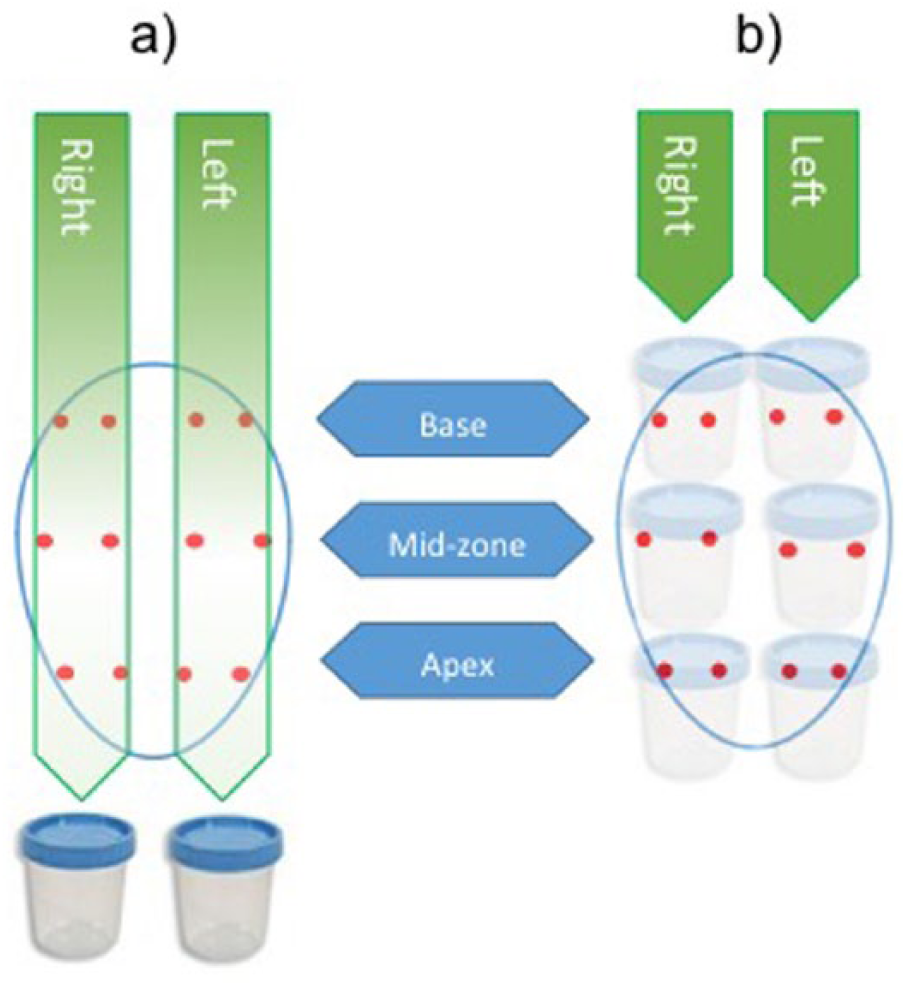
Diagram to show the two methods used across the region to send histological samples from transrectal ultrasound and biopsy. (a) Six cores from the left lobe are sent separately from six samples from the right lobe. (b) Six sample containers are sent for analysis, each containing two cores from each geographical location of the prostate.
Follow-up after a negative result and repeat investigations
Participants in the audit were asked how patients with a negative initial TRUS and biopsy were followed up. All units indicated that prostate-specific antigen (PSA) kinetics and digital rectal examination (DRE) was the mainstay of follow-up. Furthermore, three units also included free total PSA in their follow-up protocol.
If concern arose on follow-up necessitating further investigation, 42% of units would proceed directly to a second TRUS and biopsy. The remaining 58% of centres indicated they would use an alternative diagnostic method at that point. A mpMRI would be used in 63% of centres for that purpose and 37% of units use transperineal template biopsy (Figure 3).
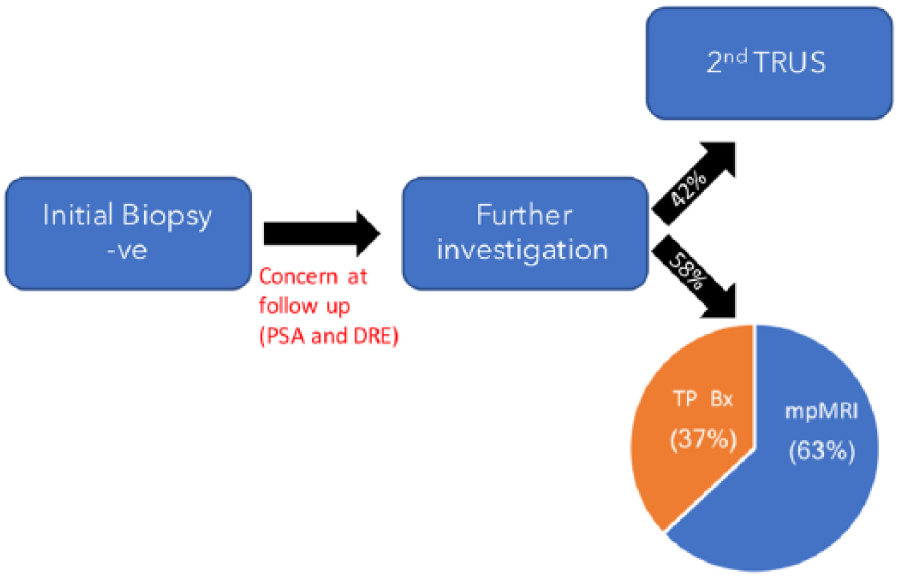
The average practice across the northwest for follow-up after initial negative first biopsy. TP Bx: transperineal prostate biopsy (template); TRUS: transrectal ultrasound and prostate biopsy; mpMRI: multiparametric magnetic resonance imaging prostate; PSA: prostate-specific antigen; DRE: digital rectal examination.
Eight of the 19 units audited (42%) offered transperineal biopsy. Of those units providing that service six units eluded to how template biopsy was performed. Four of the six (67%) performed pan-prostatic biopsy and two out of six (33%) practised targeted biopsy for lesions deemed sufficient risk on mpMRI.
Discussion
The Prostate Cancer Risk Management Programme (PCRMP) has produced a guideline on how centres should perform a TRUS and biopsy. 7 This document advocates written consent, which is not currently routinely practised by half the units in our region. If a region-wide diagnostic pathway were to be created, then written consent would be likely to be mandatory.
Guidelines recommend antibiotic prophylaxis with a quinolone antibiotic for TRUS and biopsy.5,8 All centres in our region utilised prophylactic antibiotics, with ciprofloxacin either alone or in combination. A Cochrane systematic review failed to demonstrate any improvement in sepsis rates with a 3-day course compared to a single dose. It also failed to show superiority of any individual antimicrobial agent. 9 Despite this high-quality evidence, the majority of units (69%) in our region routinely use a 3-day course of antibiotics post-TRUS and biopsy.
The rate of fluoroquinolone-resistant Escherichia coli in the UK increased by 18% between 2010 and 2013. 10 Numerous papers have shown that over the same period the infective complications of TRUS and biopsy have increased while the non-infective complications have remained static or have fallen.11 –13 It seems clear that antimicrobial resistance represents an increasing risk for prostate biopsy. 14 Taylor et al. 15 reported an improvement in the rate of infective complications after tailored prophylaxis based on rectal swabs taken before biopsy. Interestingly, an overall cost benefit was also seen due to the reduction in the costs associated with reduced hospital admissions. 15 In this era of increasing antibiotic resistance the importance of proper antibiotic stewardship cannot be overstated and rectal swabs may offer another means of achieving this. This would, however, present challenges to those 21% of units in our region which offer a one-stop clinic for prostate cancer diagnostics.
Current guidelines do not recommend the use of mpMRI before an initial biopsy as meta-analysis has suggested that cognitively targeting TRUS-guided biopsies only increases the cancer detection rate by 2%. 5 The authors of the PROMIS trial have recently published their results. 6 This well-designed study has shown that mpMRI is more sensitive than TRUS and biopsy (93% vs. 48%, P < 0.0001). The negative predictive value of mpMRI was also improved compared to TRUS and biopsy (89% vs. 74%, P < 0.0001), suggesting that mpMRI is more accurate when ruling out clinically significant prostate cancer. The authors concluded that approximately one quarter of men may be able to avoid a biopsy altogether. In our region only 21% of centres routinely perform prebiopsy mpMRI. The increase in workload required to perform prebiopsy mpMRI for all men undergoing biopsy would likely be a significant challenge for already stretched radiology departments.
Meta-analysis has shown that adding lateral cores to sextant biopsy significantly increased cancer yield. Schemes with 18–24 cores did not further increase the cancer detection rate but did, however, increase the complication rates. The review concluded that 10–12 cores strike the right balance between cancer detection and complications. 16 This is now routinely practised throughout our region.
The majority of centres audited sent cores for histological analysis by side (Figure 2(a)). This is the minimum requirement and aids decision-making around the suitability for nerve-sparing radical prostatectomy. 7 A quarter of units sent two cores from each geographical location per sample container (Figure 2(b)). This allows for better disease localisation, quantification, and can assist in management decisions.
The National Institute for Health and Care Excellence (NICE) used meta-analysis performed by Mowatt et al. to aid its decision-making over the use of mpMRI after an initial negative biopsy. When compared to systematic extended 14–16 core TRUS for re-biopsy mpMRI had improved sensitivity (88% vs. 83%), a better estimated yield (24% vs. 20%) and lower morbidity. 17 NICE concluded that mpMRI to determine the need for, and direct, repeat TRUS-guided biopsy is cost effective. Our results have indicated that 42% of urology units in the northwest still proceed directly to a second TRUS and biopsy.
This audit is a snapshot of current clinical practice across one region. The quality of the data is dependent upon the responding consultants’ knowledge of the service at their units. Clearly, there are also limitations associated with an attempt to group the complexities of prostate cancer diagnostic pathways into a single response to a questionnaire. This audit was designed as a tool to summarise the more standard practise across our region. Within these confines we wanted to explore and to go into some depth. However, we purposely avoided some other interesting areas of prostate cancer diagnostics which are not recommended by NICE (such as prostate health index and urinary PCA3) for brevity and clarity purposes.
The management of prostate cancer is a challenge for clinicians. It is an area in which there is a healthy and active body of research, reflected by a continually changing landscape. This does, however, present difficulties and a unified diagnostic pathway for a whole region would be challenging. This audit has suggested that future developments may well be clarification of the role of mpMRI and its ability to circumvent prostate biopsy. With TRUS and biopsy now carrying more risk this would be a huge step forward. Other methods of dealing with the increasing incidence of infectious complications such as rectal swabs and tailored prophylaxis may also play more of a role in the future. Further high-quality studies are required in this area for clarification but interventions such as these may be a step in the right direction.
Conclusion
Even within a single UK region there are significant differences in practice. Certain areas, such as antibiotic prophylaxis or the number of biopsy cores used, are evidence based. Other areas are driven by resources and clinician preference. The adoption of a standardised pathway is likely to improve diagnostic standards and reduce variation in outcomes. Further work on how the variation in practice can affect outcomes would be a strong driver to ensure change and is an area to be studied in the future.
Footnotes
Acknowledgements
The authors would like to acknowledge the northwest regional audit group where these data were originally presented.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
JO.
Contributorship
JO designed the data collection tool and collated results. JDB researched the literature, analysed the data and wrote the manuscript. Both authors reviewed and edited the manuscript and approved the final version of the manuscript.