
Abstract
Objective:
The objective of this study is to evaluate the utility of routine loopogram follow-up three months after cystectomy and urinary diversion in the early detection of benign ureteroileal anastomotic stricture (UAS).
Materials and methods:
A loopogram was incorporated into our standard follow-up three months after cystectomy and conduit urinary diversion in August 2010–December 2015. Data were maintained prospectively in a database.
Results:
A total of 250 patients (181 male; 69 female); median age of 70 years (range: 38–83) underwent cystectomy and conduit urinary diversion during this period. Of these, 167 (66.8%) had a routine loopogram at three months. Seven of 167 were confirmed to have a benign UAS. Twenty-three of 250 (9.2%) had an early loopogram prior to the planned three-month study in response to symptoms. Nine of 23 were diagnosed with benign UAS. Sixty of 250 (24%) did not have a routine loopogram for a variety of reasons. Five patients with normal three-month loopograms developed late strictures after a median time of 22 months (range 5–38).
In total 21/250 (8.4%) patients developed UAS. Stricture rates for the open, robotic and laparoscopic modalities were 8/129 (6.2%), 12/111 (10.8%) and 1/10 (10%) respectively. Five of seven of patients with early, asymptomatic UAS diagnosed on routine loopogram received treatment; four of five had improvement in renal function.
Conclusion:
Overall stricture rate in this series was 8.4%. The majority of UAS occur early and are more likely to be symptomatic. A policy of routine loopogram benefitted only 4/250 (1.6%) patients. We advocate the use of loopograms in cases with a high index of suspicion rather than for routine screening.
Level of evidence:
Not applicable for this multicentre audit.
Introduction
Benign uretero-enteric anastomotic stricture (UAS) is a significant complication after cystectomy and urinary diversion, with a reported incidence of up to 13%.1–3 Left untreated, these can lead to severe consequences including loss of renal function and morbidity secondary to recurrent infections or pain. Although benign UAS can present at any time after surgery, many studies have shown that these tend to present early, with the greatest risk within the first post-operative year.1–4 Studies have also shown that the majority of benign UAS are asymptomatic and detected only incidentally on imaging.4,5
Most studies published so far on benign UAS after cystectomy and urinary diversion are based on patient populations pre-dating minimal access surgery. There have been concerns that certain technical aspects of laparoscopic and robotic-assisted cystectomy and urinary diversion may result in an increased risk of benign UAS. 6 Only one unit has specifically investigated the rate of stricture occurrence between open and robotic cystectomy, and found no statistically significant difference (open – 8.5%, robotic – 12.6%, p = 0.21). 2
Based on published findings that most benign UAS develop early, but are often asymptomatic, our group initiated a policy of performing routine ‘loopogram’ studies on all patients three months after cystectomy and conduit urinary diversion, with an aim to detect strictures before the irreversible loss of renal function. We report on the utility of this regimen in influencing the clinical management of patients after cystectomy and urinary diversion, particularly in an era of minimally invasive surgery.
Methods and materials
A routine loopogram study performed three months after cystectomy and conduit urinary diversion was incorporated into our standard follow-up protocol in August 2010. Clinical and pathological details for all cystectomy patients at our institution have been entered into a prospectively maintained database since 2004. The data were analysed from August 2010 to December 2015 for the purposes of this study. We included all patients who had either radical or simple cystectomy with ileal or colonic conduit diversion for both malignant and non-malignant disease. Patients were excluded if they underwent any other type of urinary diversion.
Operative technique
At our centre, patients underwent open, robot-assisted or laparoscopic cystectomy with ileal or colonic urinary diversion. Patients with extensive T4 disease, a history of extensive pelvic surgery, or those with severe cardiopulmonary comorbidities who were unlikely to tolerate the Trendelenberg position were advised to have open rather than minimal access surgery.
Open cystectomy was performed in the standard fashion. Robotic cystectomy and laparoscopic cystectomy were performed as previously described. 7 For the minimally invasive procedures, all conduits were constructed via the extracorporeal approach, apart from four patients who had robotic cystectomy with intracorporeal ileal conduit formation. For all uretero-enteric anastomoses, we used a spatulated, end to side, Bricker anastomosis over a 6 or 8 Ch feeding tube or a 6 or 7 Ch single-J stent. The feeding tubes or stents were removed two to three weeks post-operatively.
Follow-up
Standard follow-up was as follows: All patients were routinely followed up two weeks after discharge, then three, six and 12 months after their operation. Immediately prior to the three-month visit, patients had a loopogram. Prior to the six- and 12-month visits, patients had follow-up computed tomography (CT) of the chest, abdomen and pelvis with intravenous contrast, depending on their disease stage and final histology. Subsequent follow-up was tailored according to the disease stage. Patients who had cystectomy for benign diseases had less stringent follow-up. Some patients deviated from this standard follow-up schedule for various reasons.
Loopogram technique
All loopograms were performed in our radiology suite and reviewed by a specialist consultant uro-radiologist (GR). Following a dose of intravenous antibiotic (Gentamicin, 3 mg/kg) a size 6–8 Ch Foley catheter is inserted into the conduit and the balloon is inflated with 10 ml water. Fifty to 100 ml of contrast is then manually instilled with a syringe while radiographs at anterior-posterior and oblique projections are taken. The loopogram is considered normal if there is prompt reflux of contrast along the ureter up to the renal pelvis bilaterally. A loopogram is suggestive of a uretero-enteric anastomotic stricture in the absence of complete opacification of the ureter or renal pelvis. All patients who have an abnormal loopogram go on to have a further confirmatory scan (either CT urogram or a delayed repeat loopogram) before establishing a diagnosis of benign UAS.
Results
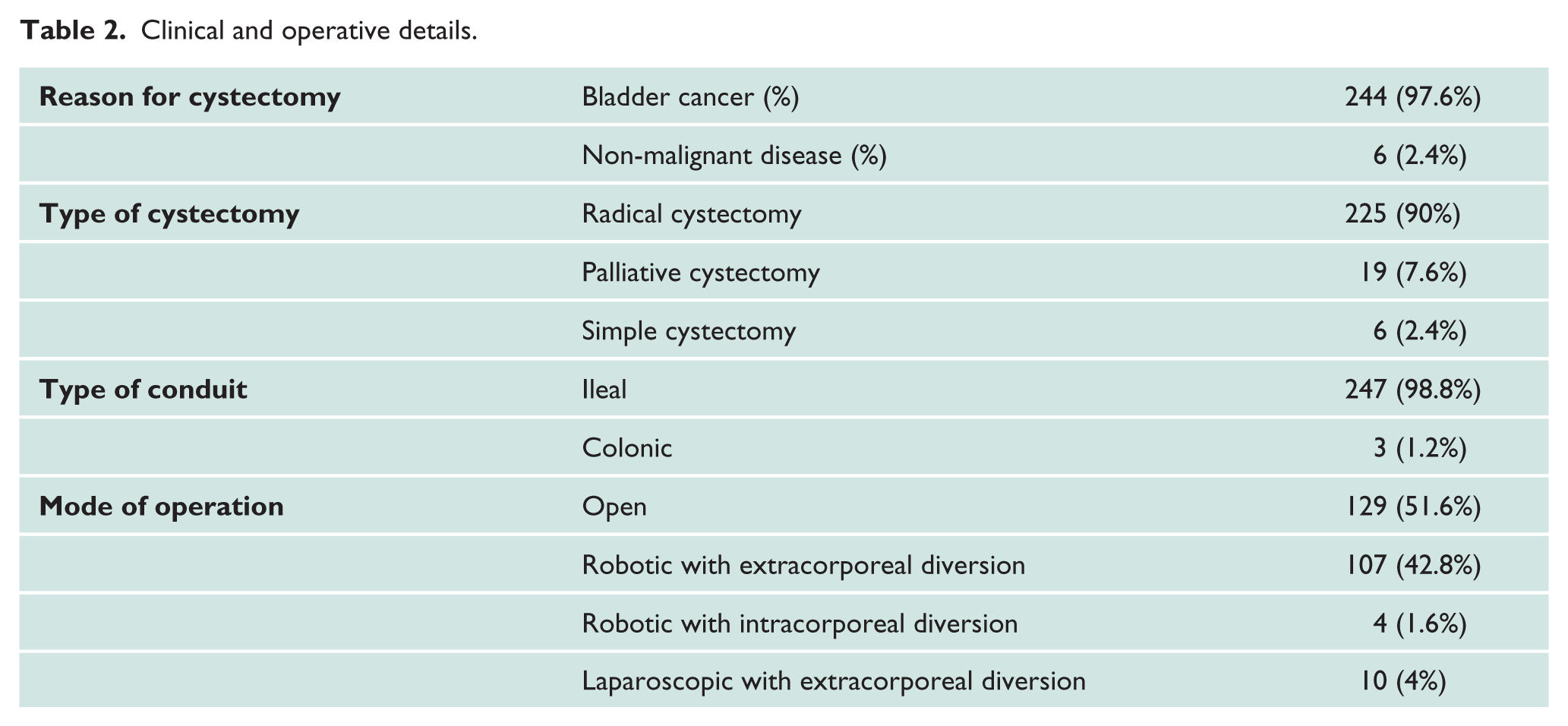
A total of 250 patients had a cystectomy and conduit urinary diversion between August 2010 and December 2015. Patient demographics and clinical and operative details are presented in Tables 1 and 2. Median follow-up duration was 18 months (range 2–54 months).
Patient demographics.

M: male; F: female; BMI: body mass index; ASA: American Society of Anesthesiologists.
Clinical and operative details.
Of the 250 patients, 167 patients (66.8%) had the planned routine loopogram performed at a median of 94 days (range 56–207). Of these, 19/167 patients had a loopogram suggestive of a benign UAS. After further radiological evaluation with a CT urogram, or a delayed repeat loopogram, only 7/167 patients (4.2%) were eventually diagnosed with a benign UAS. One patient in this group with an initial abnormal loopogram went on to have a CT scan which suggested unilateral hydronephrosis secondary to lymph node recurrence causing external ureteric compression but subsequent positron-emission tomography scan was negative. Of the remaining 148 patients with normal routine loopograms, five subsequently developed late benign UAS at 5, 8, 22, 26 and 38 months respectively.
Twenty-three patients (9.2%) had an early loopogram prior to the planned three-month study in response to symptoms, most commonly of sepsis and acute kidney injury. Two of these patients had been diagnosed with a urinary leak on CT scan a few weeks post-operatively, and therefore had repeat loopograms to monitor the state of urinary leak. Within this group, loopograms were performed at a median of 42 days after surgery. Of these 23 patients, nine (39%) were ultimately diagnosed with a benign UAS.
A total of 60 (24%) patients did not have a routine three-month loopogram or an early loopogram. Of these, 32 were either too frail or had died before three months, seven were followed up at their local unit, one was allergic to contrast, and 20 patients were not booked to have a loopogram as a result of administrative lapses. Supplementary Figure 1 summarises the flow and outcomes of patients as described above.
In total, 21 patients of the 250 in this series (8.4%) developed benign UAS – seven (2.8%) had early asymptomatic strictures, nine (3.6%) had early symptomatic strictures, and five (2%) developed late strictures. The median time to stricture development was 103 days (range 15–1140). Details including the management of all patients who were diagnosed with benign UAS in our series are shown in Table 3.
Details of all patients diagnosed with benign UAS.
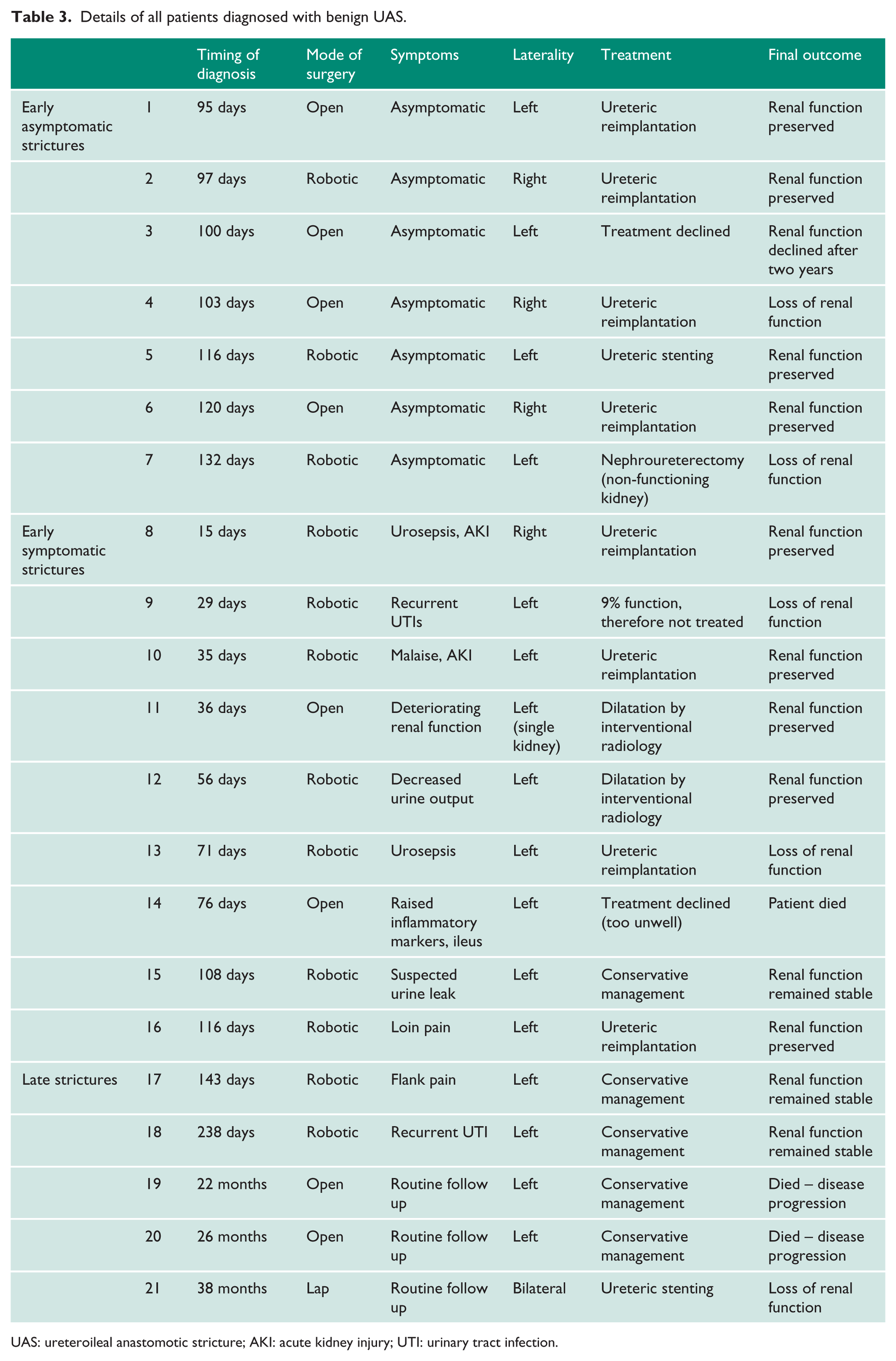
UAS: ureteroileal anastomotic stricture; AKI: acute kidney injury; UTI: urinary tract infection.
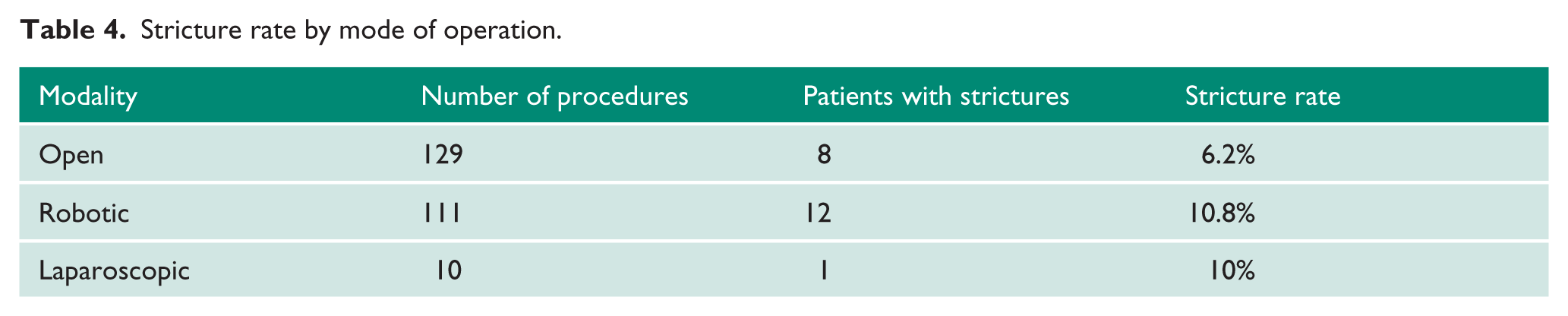
Of a total of 129 open operations performed, eight (6.2%) patients developed strictures. Of a total of 111 robotic procedures performed, 12 (10.8%) developed strictures. One out of a total of 10 patients who had received laparoscopic cystectomy developed a stricture (10%). Table 4 shows stricture rate according to operative mode.
Stricture rate by mode of operation.
Discussion
The value of clinical research is elevated when findings are translated into modifications in clinical practice. Subsequent auditing of the outcomes of these changes can provide further feedback as to the validity of the research findings. In this study, we made use of prior published findings that benign UAS tend to occur early and are frequently asymptomatic, to develop a policy of routine three-month loopograms for all our patients who have had cystectomy and conduit urinary diversion. Our aim was to detect benign UAS early, in order to prevent the irreversible loss of renal function and to reduce morbidity from recurrent infections.
In our cohort of 250 patients, 21 (8.4%) developed benign UAS after a median follow-up period of 18 months. Of these, 16 were early strictures, but only seven of these early strictures were asymptomatic and therefore picked up by the routine three-month loopogram. The other nine patients were found to have developed early symptomatic strictures before the planned three-month loopogram. A further five patients developed late strictures.
Amongst the seven patients with early asymptomatic UAS diagnosed on routine loopogram at three months, five patients underwent treatment for the stricture – four were treated with open ureteric reimplantation and one had a ureteric stent insertion. The renal function of one of the five patients remained impaired despite surgical intervention, while the other four patients had preserved renal function following intervention. The sixth patient had severely impaired renal function when his stricture was detected and subsequently underwent nephroureterectomy. The final patient was found to have mild narrowing in the distal ureter on loopogram, and mild hydronephrosis on CT urogram, but did not have any renal function impairment despite having a solitary kidney and declined treatment for the stricture. Interestingly, this patient subsequently presented back to us two years post-operatively with renal failure secondary to obstruction of her solitary kidney, and was then treated with ureteric stenting. Thus, our policy of routine early loopogram after cystectomy and conduit in 250 patients ultimately benefitted only four patients (1.6%).
Tal et al. 4 studied 221 patients who underwent radical cystectomy and urinary diversion, and found that of 28 patients who developed benign UAS, 75% were asymptomatic. Similarly, in a study of benign UAS after continent urinary diversion, Pantuck et al. 5 found that seven out of nine patients (78%) who developed strictures were asymptomatic. In contrast to these published findings, 9/16 (56.2%) of the early strictures in this series and two of five (40%) of the late strictures presented with symptoms. One reason that more patients in our study were found to be symptomatic with their strictures could be our practice of actively encouraging all patients who have problems after their cystectomy to present directly to the Urology unit where they are rapidly seen by the operating team. As a result, seemingly innocuous symptoms such as malaise or a urinary tract infection, which may have been overlooked by clinicians with less experience, are more promptly investigated by the operating team.
A second notable finding from this study is the difference in stricture rates between the different modes of cystectomy and conduit operations. In our study, the stricture rates after robotic (10.8%) and laparoscopic cystectomy (10%) were higher than that after open cystectomy (6.2%). There have been concerns that the reduced ability to robotically or laparoscopically mobilise the left ureter can lead to ureteric kinking, or inadvertent devascularisation injury to the distal ureter. However, we believe the risk of this is reduced with new robotic systems which provide multi-quadrant access. 8 In addition, the vast majority of the urinary diversions in the minimally invasive procedures in this series were performed extracorporeally. It is thought that extracorporeal uretero-enteric anastomosis formation could place undue tension on the anastomosis, leading to distal ureteric ischaemia and an increased likelihood of stricture formation. 9 With the increasing shift in practice towards performing intracorporeal urinary diversion which allows the uretero-enteric anastomoses to be formed in situ within the abdomen, the risks of excessive ureteric mobilisation and tension on the anastomosis are minimised, which should then lead to a reduced risk of stricture formation. Indeed, Chan et al. 10 recently reported that using an intracorporeal instead of an extracorporeal approach has reduced their stricture rate from 7% to 3%. Only one study so far 2 has specifically investigated the difference in stricture rates between open and robotic radical cystectomy and found no significant difference. Clearly, further prospective studies on larger cohorts are necessary to determine conclusively whether operative approach affects rates of benign UAS.
An important limitation of this study is its retrospective nature. We acknowledge that the lack of randomisation has resulted in inevitable selection bias between patients who did and did not undergo a routine loopogram as planned. However, this reflects genuine difficulties faced in the management of patients who have undergone cystectomy, who are sometimes too unwell even several months after the operation to undergo investigations. We feel that presenting an observational study such as this remains valuable, not only in evaluating the utility of a loopogram in diagnosing benign UAS, but also in assessing the practicality of a policy of routine loopograms in this group of patients.
A further limitation of this study is the relatively short length of follow-up such that the true prevalence of late benign UAS might not have been fully captured. This is especially important as in some series, benign UAS have presented as late as 25 years post-operatively. 1
Having completed this study, we would advocate that rather than routine screening, the most effective way of detecting benign UAS after cystectomy and urinary diversion is to maintain a high index of suspicion, especially in patients presenting with urosepsis, recurrent urinary tract infections, acute kidney injury, or loin pain. This should especially be the case for patients with potential risk factors for stricture formation, such as obesity, a history of pelvic radiotherapy, severe peripheral vascular disease, diabetes, smoking, or malnutrition and technical difficulties during the procedure. 11 Close surveillance is also necessary for patients who develop urine leaks as they are at increased risk of developing benign UAS after resolution of the leak. 12
Irrespective of the operative modality, steps should be taken intraoperatively to minimise the risk of stricture formation. In a recent publication from our team based on our experience of performing the procedure using open, laparoscopic and robot-assisted techniques, we critically appraised all the potential risk factors and recommended certain technical measures to reduce the risk of the stricture formation. These include avoiding excessive ureteric mobilisation, preserving the peri-ureteric blood supply, avoiding the use of diathermy near the ureter, excising the redundant ureter, fashioning the stoma including performing stoma to skin closure before anastomosing the ureters, anastomosis of ureters using interrupted sutures over stents or feeding tubes, testing the anastomosis for a leak prior to closure, and leaving a sump drain in the conduit to further avoid tension on the anastomosis. 11
Conclusion
The rate of benign UAS within our study of 250 patients is 8.4% at a median follow-up of 18 months (range 2–54 months). Although the majority of benign UAS in our series developed early, it is difficult to predict the occurrence of this complication, and they can present with or without symptoms. Benign UAS also appeared to be more common with the minimally invasive approaches but with increasing experience and recognition of potential risk factors, surgical approach is likely to become less relevant. A policy of performing routine three-month loopogram after cystectomy and conduit urinary diversion benefited only four out of 250 patients (1.6%). Rather than as routine surveillance, we would therefore advocate the use of loopograms in highly select patients: (a) those with suspected or proven urinary leak; (b) technically challenging anastomosis; (c) dubious ureteric vascularity, for example, post-radiation; (d) following re-implantation surgery; or (e) symptomatic patients (infection/pain).
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
All applicable international, national, and/or institutional guidelines for the care of humans were followed.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Guarantor
SK
Contributorship
Professor Shamim Khan researched literature and conceived the study. All authors were involved in protocol development and data analysis. Christine Gan and Kawa Omar wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.