
Abstract

Introduction
Idiopathic partial thrombosis (IPT) of the corpus cavernosum is an uncommon condition characterised by thrombosis of the proximal segment of the corpus cavernosum from uncertain pathogenesis. Young men are mostly affected and usually present with perineal pain, a palpable perineal mass with or without partial priapism.1–3 Diagnosis is predominantly based on clinical symptoms in combination with imaging.2–4 We report on a case of IPT of the corpus cavernosum that was managed successfully with a conservative approach.
Case report
A 27-year-old man with no significant past medical history presented to the emergency department with a two-week history of worsening intermittent deep scrotal pain on the right side with no other symptoms, history of penile trauma or sexual activity. On examination, he had normal vital signs with a tender perineum and thickening at the right base of the penis. The remainder of his genitourinary examination was unremarkable. After an initial ultrasound assessment showed no abnormality of the penis or testes, computed tomography (CT) scan of the pelvis with intravenous contrast was performed to exclude a deep collection. A 73 × 20 mm peripherally enhancing hypodensity was observed within the right corpus cavernosum suspicious for partial segmental thrombosis (Figure 1). A subsequent magnetic resonance imaging (MRI) examination confirmed a segmental thrombosis in the proximal right corporal cavernosum (Figures 2, 3 and 4). A conservative management approach including 10 days of low molecular weight heparin (Clexane 80 mg) and an antiplatelet (aspirin 100 mg) were administered. A thrombophilia screen that assessed APC resistance, antithrombin III, prothrombin factor, factor V Leiden, protein C and protein S was unremarkable. His penile pain reduced and he was discharged from hospital three days later with a plan to continue aspirin indefinitely. Outpatient clinical review one week later revealed improved pain and reduced size of the mass at the base of the right corpora. At follow-up five months and 11 months after presentation, there was complete resolution of symptoms including no erectile dysfunction or urinary symptoms.

Computed tomography (CT) of the pelvis (with intravenous contrast) as seen in axial view. The red arrow is showing a 72.9 × 20.1 mm peripherally enhancing hypodensity within the right corpus cavernosum suspicious for partial thrombosis of the right corpus cavernosum.
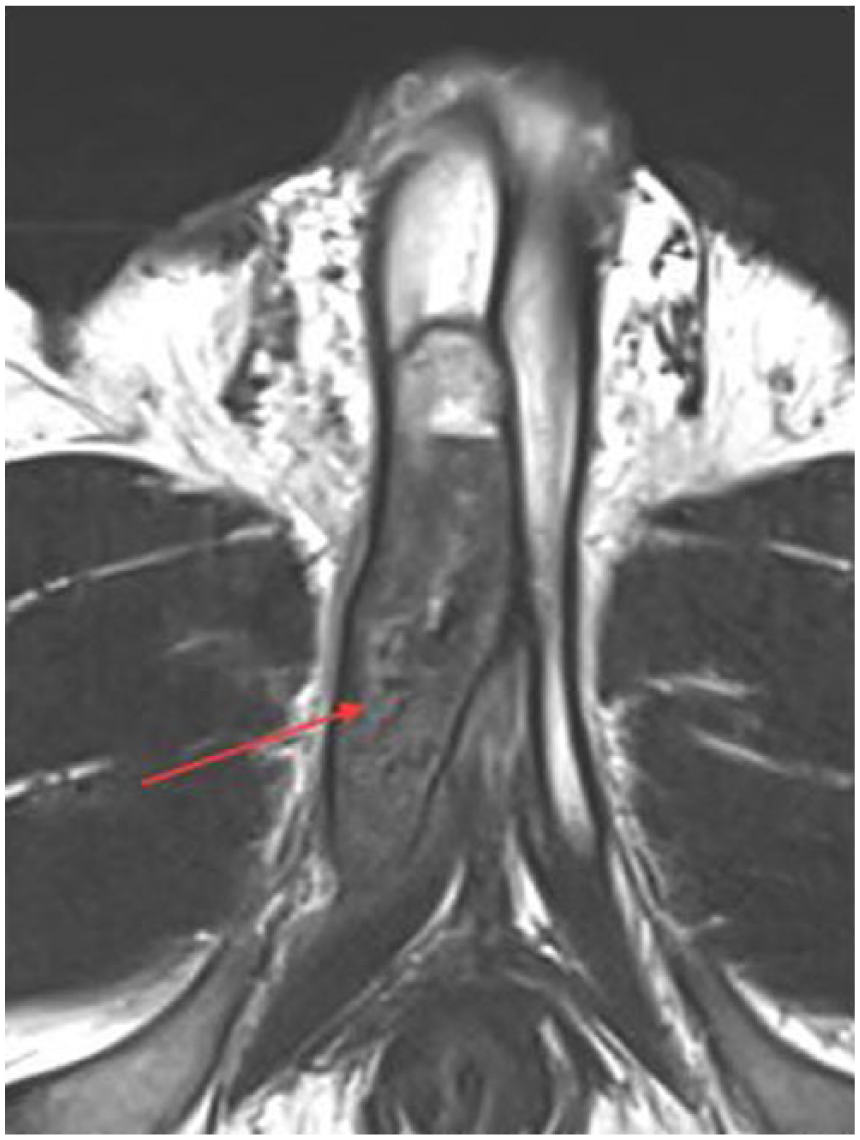
Magnetic resonance imaging (MRI) T2 axial view of the pelvis with the red arrow showing a well-encapsulated collection noted within the right corpus cavernosum with maximal dimensions of 85 mm anterior–posterior × 18 mm craniocaudal × 19 mm transverse. The collection demonstrated a low T2 signal on gradient echo sequences, in keeping with partial thrombosis of the corpus cavernosum. Note the normal corpus cavernosum on the contralateral side.
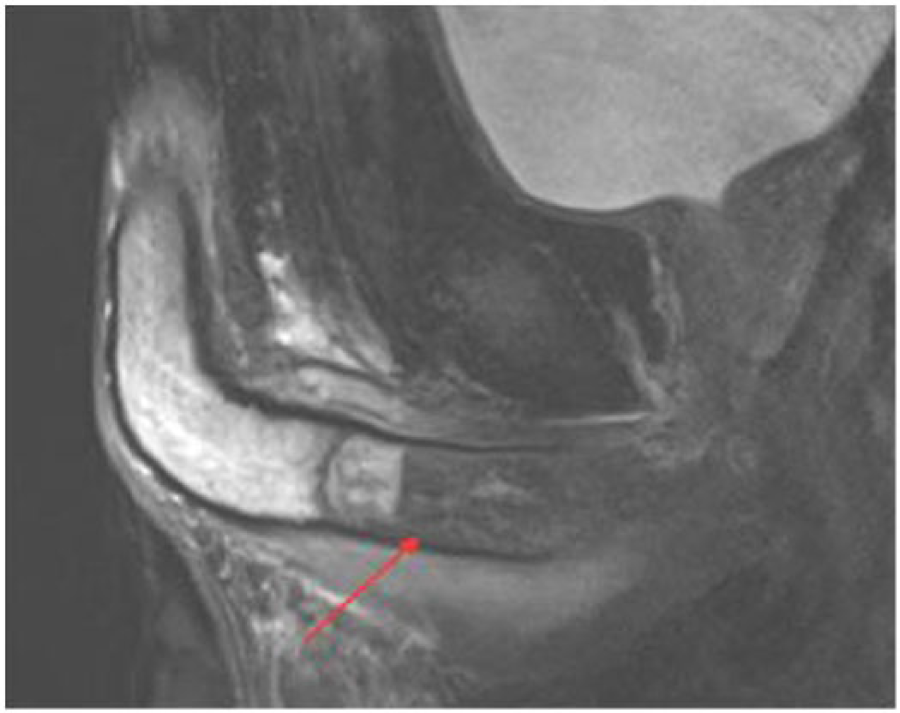
Magnetic resonance imaging (MRI) T2 sagittal view of the pelvis is seen above with the thrombosis demonstrated by the red arrow. The extent of the thrombosis can be clearly visualised by this sagittal view.
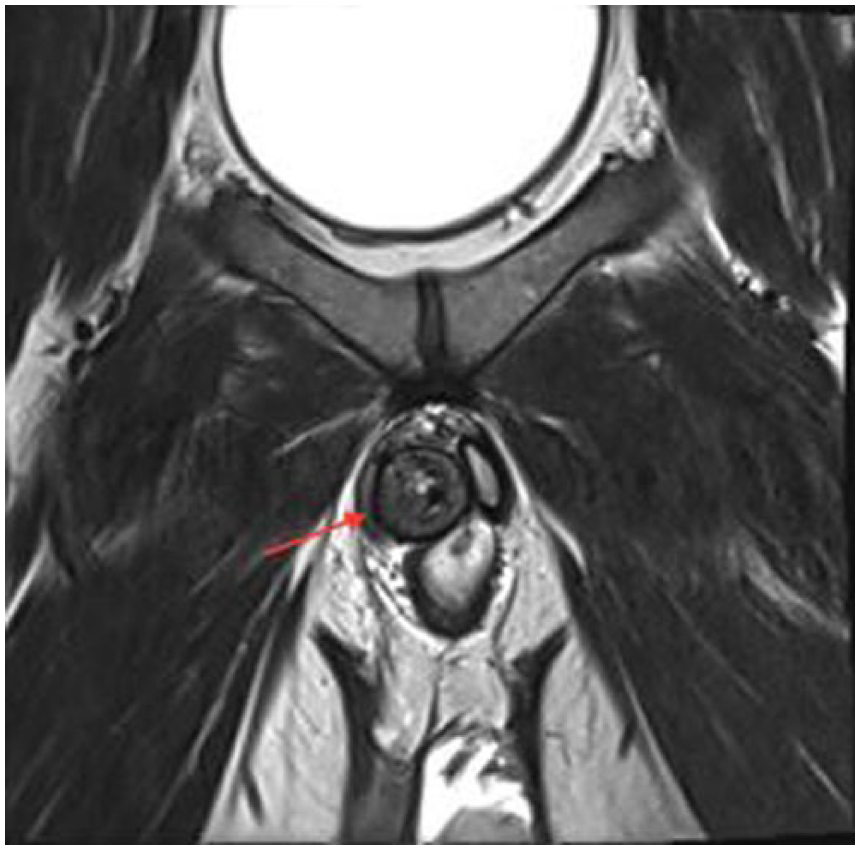
Magnetic resonance imaging (MRI) T2 coronal view of the pelvis is shown above. The red arrow points towards the thrombosis of the right corpus cavernosum, and its compression of the contralateral side is evident here.
Discussion
We report a case of IPT of the corpus cavernosum detected with non-invasive diagnostic methods and managed successfully with conservative medical management. The aetiology of IPT remains unclear, although associations between extensive cycling causing microtrauma, as well as vigorous sexual intercourse have been reported.4,5 In addition, a fibrous web at the level of the cruocavernosal junction, reported in the majority of IPT patients with advanced MRI imaging, may predispose for entrapment of blood in the crura. 5
MRI is used to confirm the diagnosis when clinically suspected, although ultrasonography and/or CT imaging are more commonly performed acutely due to accessibility and consideration of differential diagnoses. 4 MRI is the superior modality due to superior visualisation of penile soft tissue (septum and thrombus) abnormalities and differentiation between IPT and other pathologies such as penile malignancies, Peyronie’s disease and penile abscess. 4 The findings in this case have confirmed that non-invasive imaging methods are sufficient to confirm the diagnosis.3,5
Historically, treatment of IPT consisted of drainage and shunting of the thrombus; however, adverse outcomes such as erectile dysfunction were reported. 5 In a recent case series review, low molecular weight heparin and/or subsequent or simultaneous antiplatelet therapy proved to be successful as first line treatment 73% of the time. 4 In cases in which conservative management failed, surgical incision of the web with saphenal graft repair or Heincke Miculicz reconstruction was performed with good functional outcome. 5
In conclusion, IPT of the corpus cavernosum should be considered among men who present with unilateral perineal swelling and pain. Once confirmed with MRI, conservative treatment with systemic anticoagulation in consultation with specialist haematology opinion is recommended as first line therapy. If conservative management is unsuccessful, surgery should be considered.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Verbal and written informed consent was obtained from the patient for the anonymised information to be published.
Guarantor
SVR.
Contributorship
SVR, JW and MC researched the literature, obtained images and contributed to writing the manuscript. MJR, IT and ND helped to correct and revise the manuscript for submission.