
Abstract
Nocturnal polyuria (NP) is characterised by increased urine production overnight in comparison to daytime. It has significant adverse events in adults including reduced quality of life, increased risk of falls and increased mortality.
Although NP can be a manifestation of other significant conditions like heart failure and sleep apnoea, there are lots of unanswered questions about NP. What is the underlying pathophysiology? Is NP a physiological manifestation of ageing? Is the circadian change of vasopressin release the primary pathology? Or is it a secondary phenomenon to a low diurnal production of urine? Is the primary pathology at the kidney level or is there another humoral, cardiac, or endovascular element? In this article, we summarise the available English-language literature on the subject of NP, including its epidemiology, pathogenesis, diagnosis and treatment.
Level of evidence: Not applicable for this multicentre audit.
Nocturnal polyuria (NP): Background and definition
NP is an important cause of nocturnal enuresis in children and of nocturia in adults. 1 The latter is defined as the complaint that the individual has to wake at night one or more times to void. 2 There are multiple definitions of NP in the literature:
International Continence Society (ICS) definition: Nocturnal urine volume >33% (NUV33%) of total 24-hour voided volume
This is the most commonly used definition based on the 2002 consensus definition by the ICS: “an age-dependent nocturnal urine volume (normally during the 8 hours whilst the patient is in bed)” of more than 20% of 24-hour urine volume in younger people (20 to 35 years old), and more than 33% of 24-hour urine volume in older people (>65 years old). 3 However, this definition is based on limited evidence. 4
Nocturnal urine production (NUP)90 definition and the Krimpen study
The Krimpen study is a large population-based study in the Netherlands in which 1396 frequency/volume charts (FVCs) from men aged 50–78 years from the general Dutch population were collected at baseline. The NUP was estimated as the mean hourly urine production from 1 a.m. to 6 a.m., during which 90% of the men were asleep. Based on the Krimpen study, Blanker et al. 5 proposed an NUP of 90 ml/h as the threshold for NP (NUP90), as this would be the best predictor for nocturia in older men in a general population.
NUP >10 ml/kg definition
More recently the highest nocturnal voiding frequency was found using the NUP >10 ml/kg definition by Goessaert et al., 6 suggesting that this definition correlates with the largest clinical impact on the patient. It is also the strictest definition with a prevalence of 27% of the general population, for example, compared to a prevalence of 69% with the NUV33% definition. 6
NUV53% definition
Based on a study with healthy volunteers, van Haarst and Bosch 7 challenged the ICS definition by proposing a different threshold value for the nocturnal polyuria index (NPi), which is by definition the nocturnal urine output as a percentage of the 24-hour urine output. In that study, the NPi was normally distributed and they used the upper limit of the 95% confidence interval (CI) (this being 53% of the 24-hour urine volume) to be the threshold value for NP. 7 Although this seems a logical way to define NP, it results in only a very small proportion of the population (<5%) having NP. In various other conditions (e.g. obesity and hypertension), definitions differentiate in clinically relevant deviations instead of 95% CIs of the general population. 8
Problems with the ICS definition
There is significant amount of criticism of the ICS definition in the literature and the need for more discriminative and a better validated definition. We summarise here the six main points of criticism:
The NUV33 definition is based on an assumption of an average eight hours of night sleep; however, most patients over 65 probably sleep fewer than eight hours. 9
There is no clear consensus on the best definition of night: In some studies nighttime is the intended sleeping time while in others it is defined as between 12 and 8 a.m. 10
The NUV33 definition was based on a small number of low-quality studies, including small groups of patients. For example, one study contained nine enuretics and nine healthy controls, 11 while another had 24 young and 21 elderly individuals. 4
Based on the NUV33 definition, NP was present in most patients with nocturia participating in drug trials 12 and the majority of both community-dwelling men and women without nocturia. 13 This leads to overestimating NP and consequently underestimating other disorders. 7
The first morning void is included in the nighttime urine production calculation, but not in the nocturnal voiding count. Therefore, people with a large first morning void, who do not necessarily wake up at night, can easily be classified as having NP without having nocturia.
The NUV33 definition is not based on normal distributions and is not properly validated. 14
Epidemiology, incidence, prevalence and natural history of NP
The incidence and prevalence of NP in the general population depends largely on which definition has been used. There is also a remarkable resolution of incidence over time stressing the need to determine chronicity of NP before starting any treatment.
The best available literature is provided by the Krimpen study; van Doorn et al. 13 reported the incidence and prevalence of NP at 13.6% and 27.7% respectively using the NUP90 definition and at 60.3% and 77.8% using the NUV33% definition in men aged 50–78 years. 13 Very high prevalence was noted in other studies using the NUV33% definition.12,15
Based on the NUP90 definition, the prevalence increased from 27.7% to 55.9% in men with nocturia and from 8.0% to 19.8% in men without nocturia at six years of follow-up. The overall incidence at baseline was 13.6% and of these 57.0% resolved after 2.1 years of follow-up. 13
Different mechanisms and causes of NP
Decreased plasma vasopressin (AVP) levels overnight (water diuresis)
Traditionally NP was thought to be associated with low urine osmolality (Uosm) and AVP insufficiency overnight. This phenomenon has usually been felt to be desmopressin responsive. 16 However, recent studies have been unable to demonstrate clear disturbances in circadian rhythm of AVP in therapy-resistant cases. 17
Therefore, decreased nocturnal levels of plasma AVP may play a less important pathophysiological role in adult NP, except for a minority of patients with a decreased osmoregulatory function. 18
Impaired response to AVP (water diuresis)
This results in the excess production of poorly concentrated urine due to a decrease in the osmolarity gradient in the renal medulla. 19
Causes of impaired response to AVP include:
Solute diuresis 23
Sodium diuresis is represented by increased sodium clearance (sodium clearance = (urine sodium × urine flow)/plasma sodium) during the night. 24 This is seen in patients with obstructive sleep apnoea (OSA) and patients with heart failure due to increased atrial natriuretic peptide (ANP) and brain natriuretic peptide (BNP), respectively. 25 It has also been reported in 1-deamino-S-D-arginine vasopressin (DDAVP)-resistant cases.20,26
Other causes of solute diuresis include excessive filtration of a poorly reabsorbed solute such as glucose (for example, in patients with poorly controlled diabetes mellitus), mannitol, radiocontrast media and urea (for example, in patients eating protein-rich foods leading to increased urea production).27,28
Third-space fluid sequestration (solute and water diuresis)
Many patients with NP have third-space fluid sequestration, which is migration of fluid from the intravascular space into the interstitial or third space. This is confirmed by bio-electric impedance analysis in these patients. 29 It results in a low diurnal production of urine as a compensatory mechanism 18 and subsequently high nocturnal production of urine to stabilise the hydration balance as fluid returns back to the intravascular space when the patient is recumbent. 30
Common causes of third-space sequestration include cardiac impairment, autonomic neuropathy, renal impairment, nephrotic syndrome, hepatic failure, malnutrition, and venous stasis secondary to chronic venous insufficiency. 31
Age (solute and water diuresis)
Patient age is an independent predictive factor for nocturia and NP. 32 Ageing is associated with a fivefold increase in the concentration of ANP, making the elderly more susceptible to NP. 33
It has also been noted that ageing is associated with loss of urinary concentration ability secondary to failure of normal renal responsiveness to antidiuretic hormone (ADH). It is not clear whether this failure results from a decreased medullary solute gradient 34 or a decreased tubular response to ADH at the receptor level. 35 Furthermore, renin and aldosterone secretion as well as the tubular responsiveness to aldosterone is also blunted in the elderly leading to loss of water and sodium (salt wasting). 35
Sleep apnoea (solute diuresis)
There has been a remarkable rise in the prevalence of OSA of up to 50% in recent population-based studies 36 and of these up to 90% were not diagnosed by patients’ primary care physicians. 37
The association between sleep apnoea syndrome (SAS) and NP was demonstrated in previous studies, 38 especially in relatively younger men, 39 and there have been few suggested mechanisms for the association. See Figure 1:
Rostral fluid shift: Shifting body fluid from the lower half to the upper half of the body during sleep may induce neck oedema and upper airway obstruction. 40
Negative thoracic pressure due to airway obstruction increases venous return to the right atrium, which increases ANP and leads to an increase in urinary sodium excretion and nighttime urine production. 41
Intermittent hypoxia induces pulmonary vasoconstriction and increases right atrial transmural pressure, causing ANP release. 42 Notably, intermittent hypoxia also contributes to detrusor overactivity, which may cause nocturia. 43
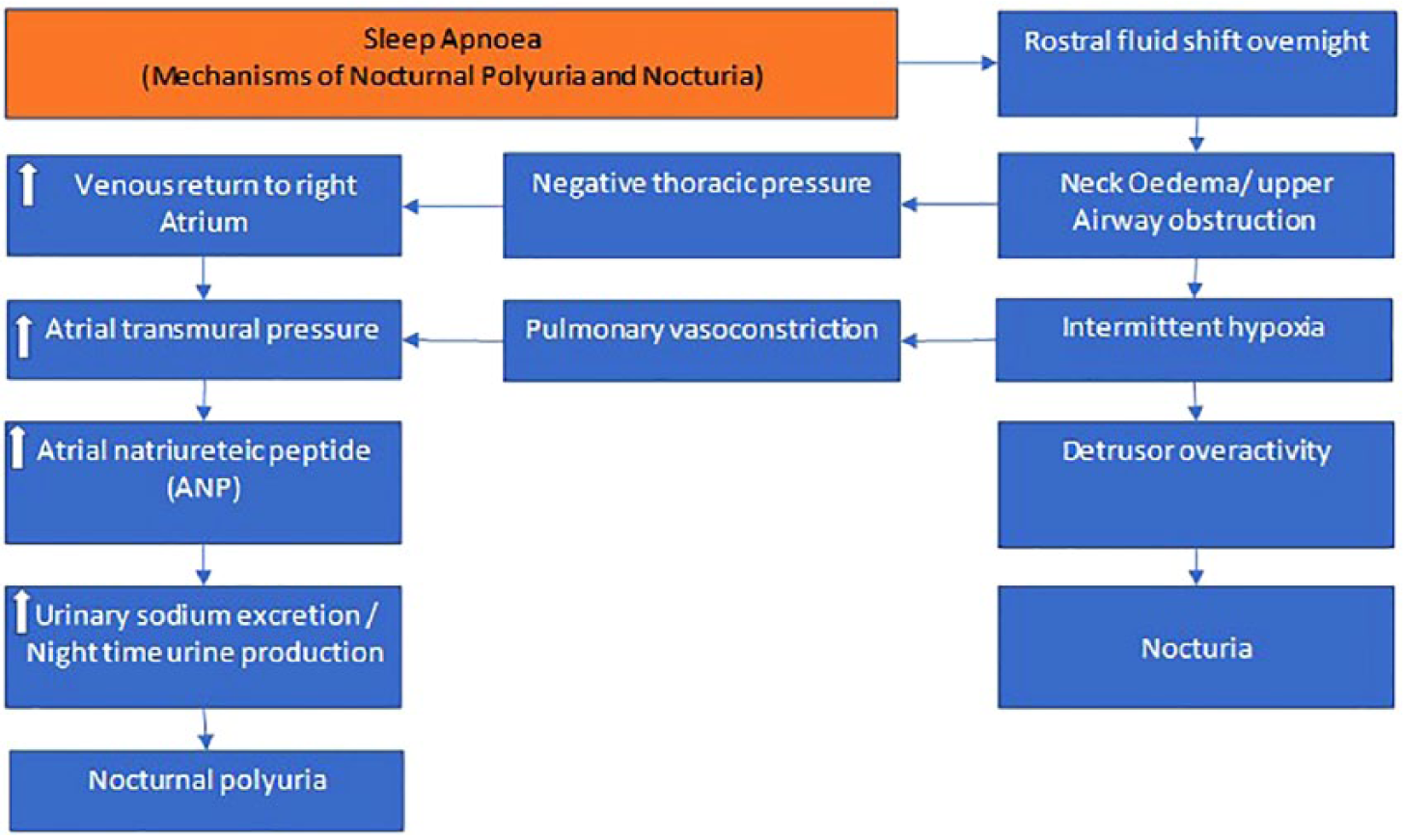
Suggested mechanisms of nocturia and nocturnal polyuria in patients affected by sleep apnoea.
Increased mean arterial blood pressure (water diuresis)
To date, limited studies have indicated an association between blood pressure and NP.44,45 High blood pressure can supress AVP release due to negative feedback from baroreceptors via the vagal and glossopharyngeal nerves. 46
Decreased serum testosterone
Testosterone has been shown to be an independent risk for overall nocturia, and particularly NP, the mechanism of which is unclear. 47
It is still inconclusive whether blunting of hormonal release (i.e. vasopressin) might be the common pathophysiology associating decreased serum testosterone with NP in the elderly. 47
Lower urinary tract obstruction (water diuresis)
Despite lack of high-quality data in the literature, there seems to be a weak causative link between lower urinary tract obstruction and nocturia, yielding a disappointing outcome after prostate surgery in this group of patients. In a retrospective case series, residual/recurrent lower urinary tract symptoms (LUTS) after transurethral resection of the prostate (TURP) were found in 20% of patients, 68% of whom complained of nocturia. 48 Similarly, the third National Health and Nutrition Examination Survey in the United States showed that nocturia (≥ 2 voids per night) persists in 41% and 50% of 60- to 69-year-olds and ≥ 70-year-olds undergoing TURP, respectively. 49
Despite the common belief that NP is not caused by lower urinary tract obstruction, 50 emerging evidence suggests impaired response to AVP in the renal tubules in obstructive disease of the urinary tract. 51 Furthermore, recent studies have shown that medical or surgical treatment of benign prostatic obstruction can reduce nighttime urine production.52,53
Patient-related behavioural factors
This includes medications (e.g. diuretics) and fluid intake at nighttime. 54
Investigations of NP
See Figure 2.
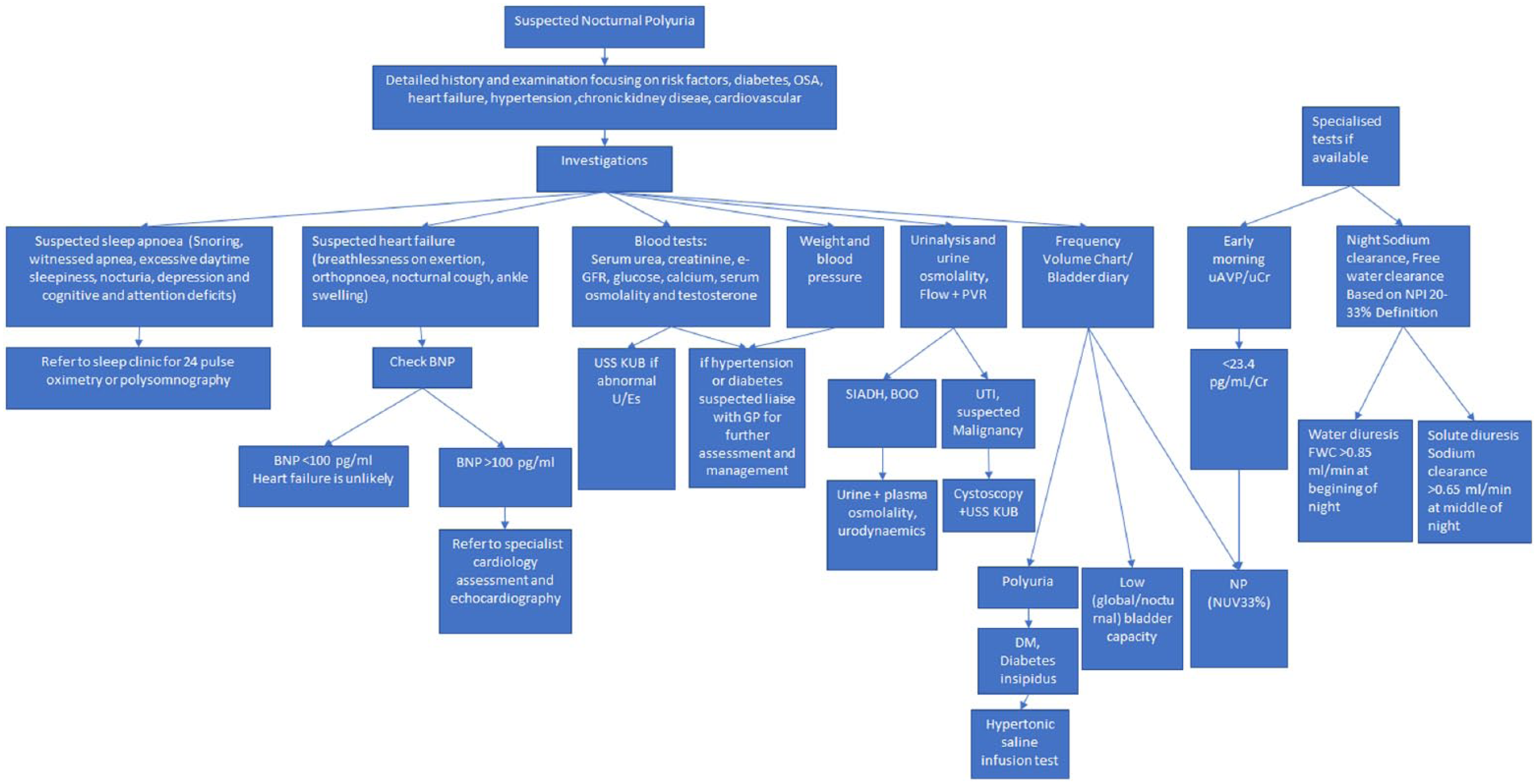
Algorithm for the assessment and investigation of patients presenting with suspected nocturnal polyuria (NP).
History, examination and bedside tests
A comprehensive assessment of the patient is mandatory. This includes detailed history focusing on any underlying conditions and risk factors for NP, such as diabetes, sleep apnoea, hypertension, chronic kidney disease, heart failure or cardiovascular dysfunction. Focused clinical examination including abdomen, lower limbs and digital rectal examination in males is mandatory.
A full drug history is essential to rule out any pharmacological reason (diuretics, lithium, alcohol, caffeine, vitamin D).
Bedside tests should include measurement of blood pressure, weight, urinalysis, urine osmolality, flow test and post-void bladder scan to look for evidence of bladder outlet obstruction.
Blood tests
This should include serum urea, creatinine, estimated glomerular filtration rate, glucose, calcium, serum osmolality and testosterone measurement.
FVC/Bladder diary
This is a key instrument in the evaluation and diagnosis of nocturia in which patients record the volume and timing of daytime and nighttime voids for one to three days. Based on analysis of the 24-hour FVC, the patient may be categorised as having any of the following: (1) NP; (2) low bladder capacity (nocturnal and/or over 24 hours); (3) mixed (a combination of NP and low global or nocturnal bladder capacity); and (4) polyuria.
Renal function profile (RFP)
This is a useful test that is rarely performed by urologists in the United Kingdom (UK). It entails measurement of free water clearance (FWC) (FWC = urine flow - (urine osmolality × urine flow)/plasma osmolality) and sodium clearance at different time points during 24 hours to help reveal the underlying mechanism of NP and distinguish between water diuresis and solute diuresis. This requires repetitive measurements and good patient adherence making it a somewhat impractical test outside the research lab.
Based on the NUV33% definition, Goessaert et al. demonstrated that FWC at the beginning of the night (12–2 a.m.) exceeding 0.85 ml per minute correlates to water diuresis while sodium clearance in the middle of the night (3–5 a.m.) exceeding 0.65 ml per minute correlates with sodium diuresis. 24
Polysomnography (PSG)
This is performed in patients with suspected OSA (snoring, witnessed apnoea, excessive daytime sleepiness, nocturia, depression and cognitive and attention deficits). 55 PSG is a sophisticated device that consists of the following (see Figure 3):
Electroencephalogram to sample activity from the frontal, central, and occipital regions.
Electro-oculogram.
Electrocardiogram.
Electro-myogram includes the chin (mental muscle) and bilateral legs (anterior tibial muscles).
Nasal-oral flow (nasal cannula with a pressure transducer and thermal sensor for nasal airflow).
Thoracic and abdominal respiratory strain gauge.
Oxygen saturation (pulse oximetry).
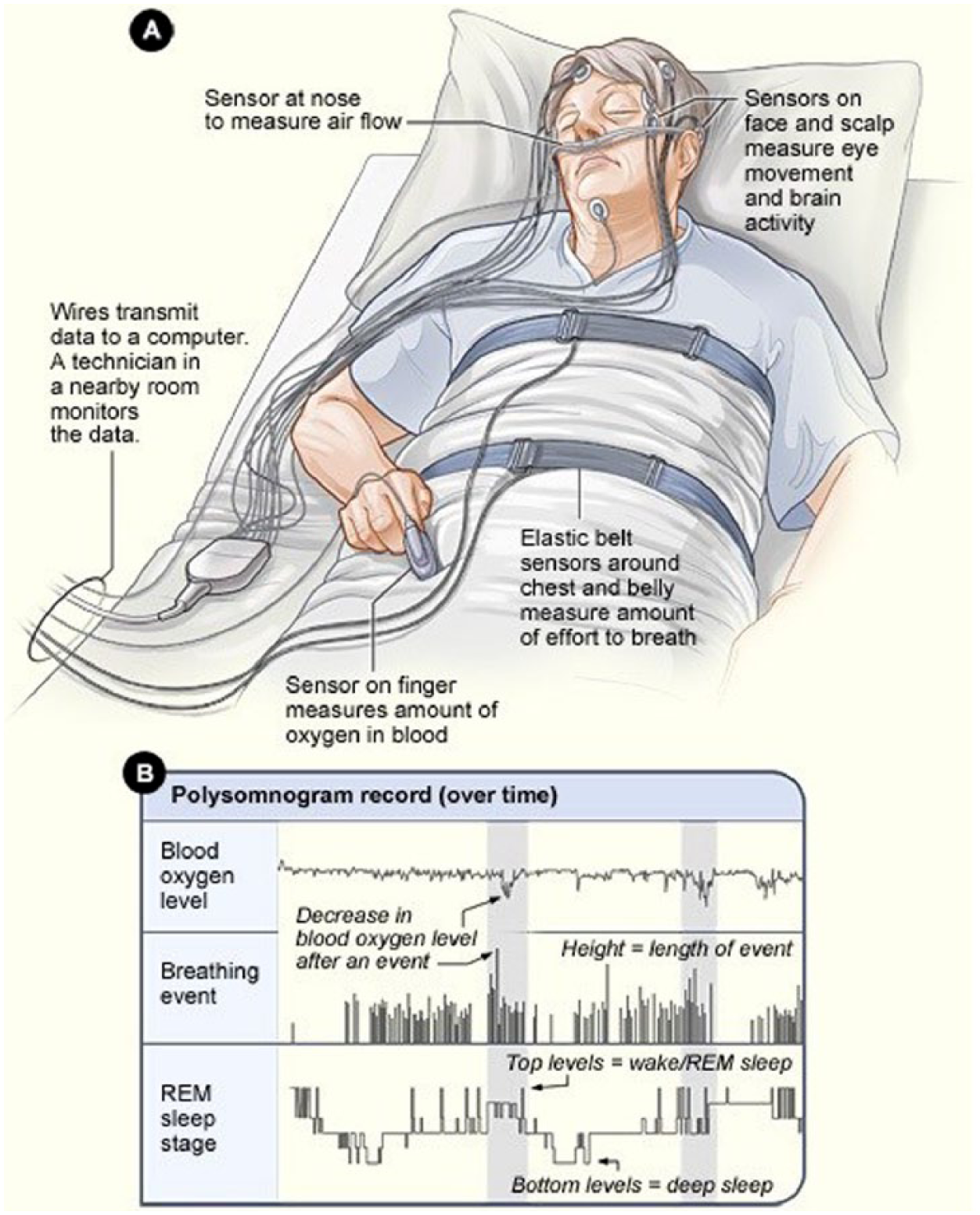
Illustration of the polysomnogram device. (a) Illustration of the components of the device attached to a sleeping patient. (b) An example of polysomnogram record showing blood oxygen levels, breathing events and the stage of sleep (rapid eye movement (REM) or deep sleep).
Patients with suspected OSA should be referred to a dedicated sleep clinic under the supervision of a consultant respiratory physician who liaises with the neuro-physiology department to perform PSG if deemed appropriate. PSG is not readily available in all sleep clinics and some units perform 24-hour pulse oximetry instead to diagnose OSA.
Early-morning urinary vasopressin/urine creatinine (uAVP/uCr) level
uAVP/uCr level in the early morning could be a primary noninvasive aetiological screening marker for patients with nocturia and NP. Hirayama et al. 56 showed that nocturnal uAVP/uCr level and urine osmolarity at 12 a.m. and 6 a.m. in patients with NP were significantly lower than those in patients without NP. 57
Despite the usefulness of this test, it is rarely used in practice, perhaps due to the small study population and the lack of appropriate validation.
Treatment
The significant fluctuations in NP suggest that it is advisable to first determine its cause and chronicity before starting any intervention. Every effort should be made ideally in a multidisciplinary setting to optimise and address any risk factors and other medical comorbidities that can contribute to NP in the elderly population. See Figure 4. These include the following:
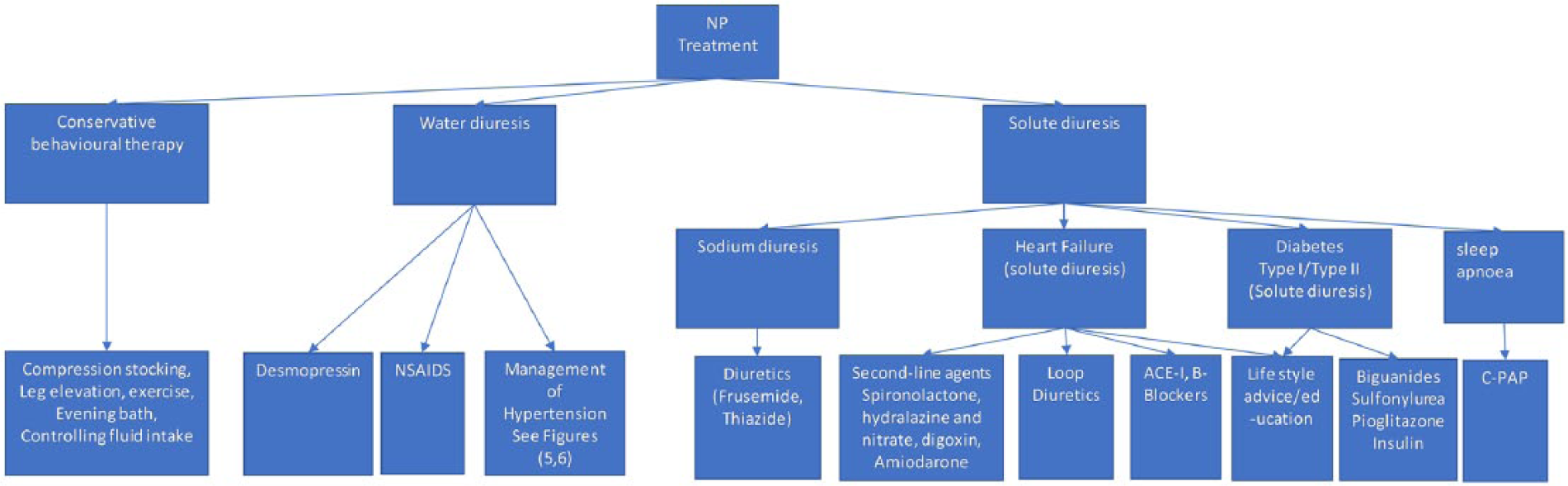
Algorithm for the treatment of nocturnal polyuria (NP) according to the underlying aetiology.
Conservative and behavioural treatment
Simple user-friendly measures that can be recommended include: compression stockings and leg elevation to reduce peripheral oedema, exercise, an evening bath and controlling fluid intake. It has been reported that water immersion with the head out induces a cephalad blood shift and increases the cardiac output, resulting in diuresis and natriuresis, hence the recommendation for an evening bath. 58
Although these measures are widely used, there is little direct evidence for their effectiveness. 59
Water diuresis
DDAVP
Treatment with a vasopressin receptor (V2) agonist is useful in NP patients with excessive water diuresis and suppressed vasopressin.
Desmopressin, a synthetic analogue of AVP, is a selective V2 receptor agonist and is internationally registered in at least 50 countries as a treatment for NP. However, it is not licensed in the UK to treat nocturia or NP and therefore its use is strictly off label. 27
Two double-blind, placebo-controlled studies (the NOCTUPUS studies) investigating the use of desmopressin in the management of nocturia60,61 demonstrated a 50% reduction in nocturnal voids in 46% of women as compared to 34% of men with an 78% increase in mean time to first nocturnal void in women as compared to a 59% increase in men.
A recent randomised, single-blinded, placebo-controlled trial 62 showed that low-dose oral desmopressin (0.1 mg) achieved a good clinical response (decrease of two or more voids per night) in 61.4% of patients. It also delayed the first void by 30 minutes, which is a strong determinant of sleep quality.
On the other hand, there is a lack of long-term data on the safety of desmopressin in adults; the therapy is known to gradually decrease serum sodium and induce hyponatraemia even in patients with normal baseline serum sodium, therefore checking serum sodium one week after initiating treatment and at regular intervals thereafter is recommended. 62 Desmopressin should be used with caution in patients with conditions associated with fluid and electrolyte imbalance such as chronic heart failure and renal impairment due to the risk of hyponatraemia and fluid overload. Furthermore it has been reported that desmopressin decreases renal excretion of potassium and increases excretion of calcium in the short term. 63
Nonsteroidal anti-inflammatory drugs (NSAIDs)
The effect of NSAIDS on nocturia is exerted via inhibiting cyclooxygenase enzymes, which are responsible for the production of prostaglandin H2, an important factor for sustaining renal plasma flow. 64 The latter is noted to decrease by 35% with nadir two hours after administering diclofenac leading to reduced urine production. 65 This explains the analgesic effect of NSAIDs in ureteric colic.
Management of hypertension
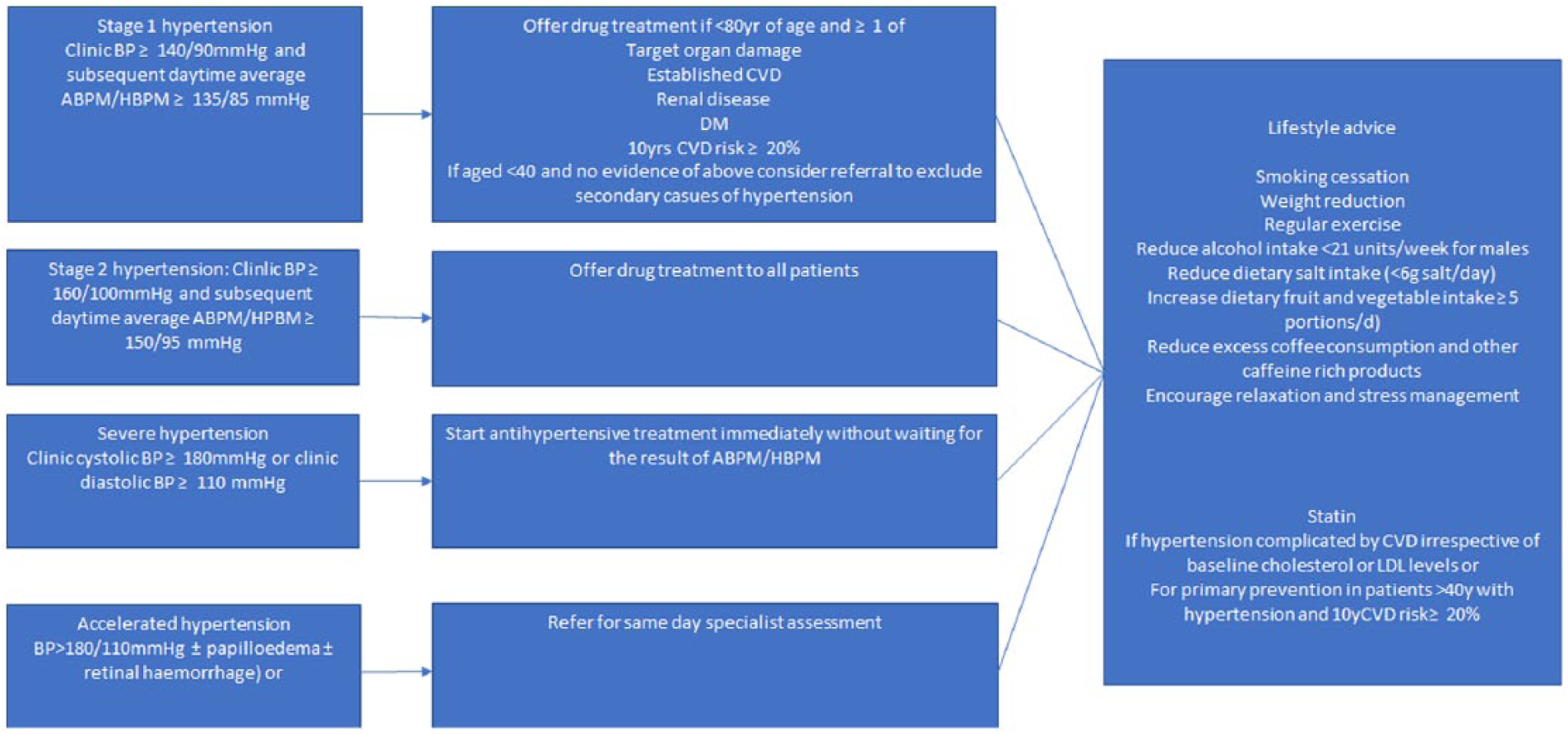
Algorithm for the management of hypertension according to severity.
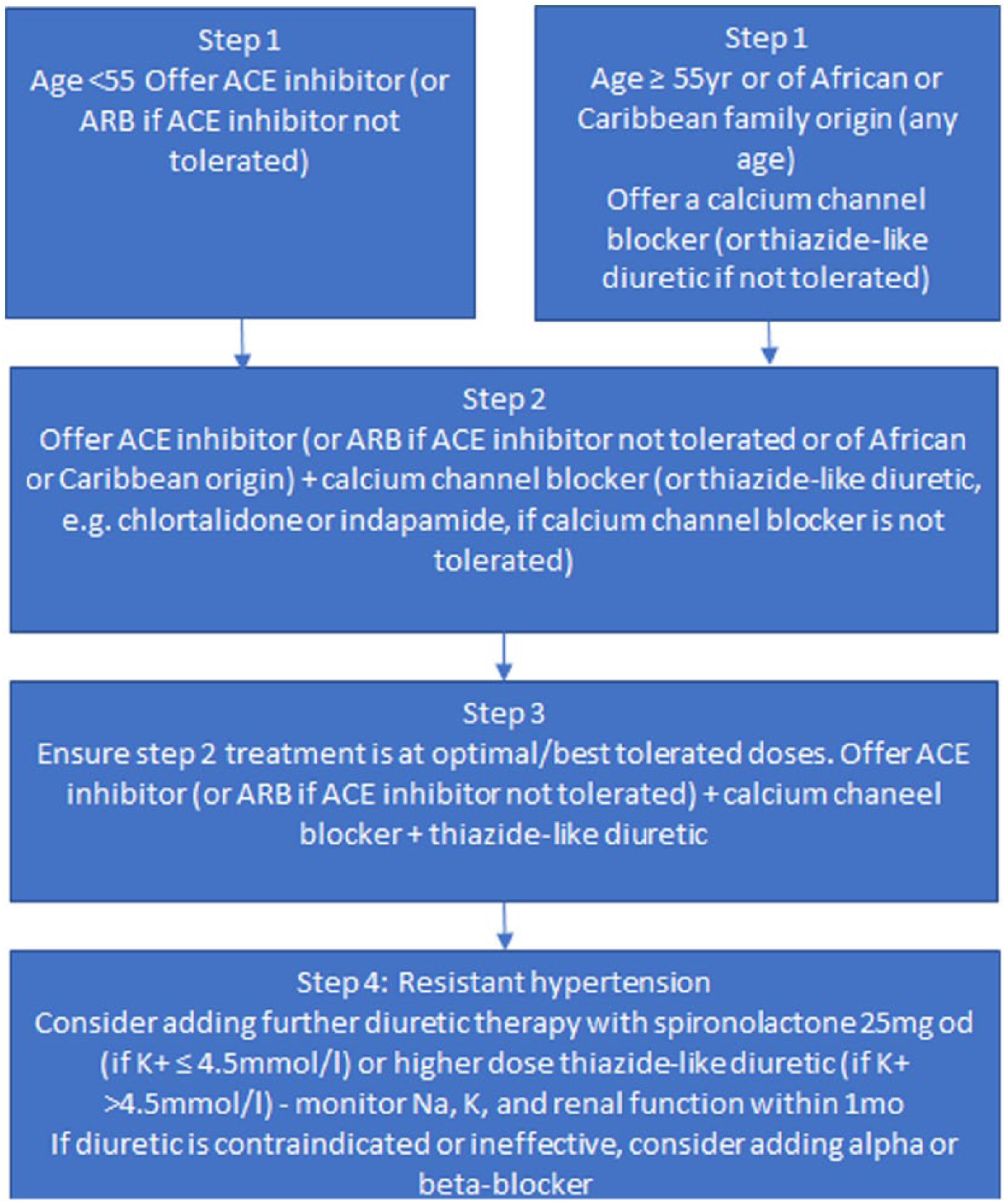
Algorithm for drug treatment of hypertension illustrating the choice of drug based on age and race and suggested treatment escalation in resistant cases.
Tamsulosin
Limited studies showed that tamsulosin reduces NUV in benign prostatic enlargement. 66 It may act via increasing daytime renal blood flow by relaxing the renal artery leading to an increase in the diurnal urine volume and a decrease in NP. 66
Solute diuresis
Management of diabetes
This is best achieved by the primary care physician and entails the following:
Six-monthly review.
Checking haemoglobin A1c (HbA1c) at least twice a year.
Offering lifestyle advice: Dietary behaviours and physical activity.
Diabetes education and referral to structured programme for those newly diagnosed. 67
Drug treatment of Type II diabetes
Biguanides: Metformin is usually initiated if HbA1c remains ≥ 48 mmol/mol after a trial of diet/lifestyle interventions.
Sulfonylureas: Gliclazide is considered first line if patients are not overweight and if hyperglycaemic symptoms require rapid response.
Pioglitazone is usually used in combination with metformin and/or sulfonylurea for patients with poor glycaemic control.
Management of heart failure
Lifestyle advice: Weight loss, reduction of salt, alcohol restriction, stopping smoking and regular exercise. In severe cases fluid restriction might be necessary.
Drug treatment
Loop diuretics (frusemide or bumetanide) to relieve congestive symptoms and fluid retention.
Angiotensin-converting enzyme inhibitors and beta-blockers are recommended in all patients with left ventricular systolic dysfunction.
Second-line agents.
This is usually started under specialist supervision and includes spironolactone, hydralazine and nitrate, digoxin and amiodarone.
Management of sleep apnoea: Continuous positive airway pressure (CPAP)
CPAP is a device that delivers high-flow oxygen via a tight-fitting mask; it applies positive pressure throughout the breathing cycle which helps open the airway and reduces the impedance and oxygen requirement. It is the most effective therapy to reduce symptoms as well as cardiovascular and metabolic complications of SAS. It is also an effective treatment for NP in patients with SAS. 38
Diuretics
The choice is limited to diuretics with a short bioactivity leading to high sodium excretion in a short period of time and allowing full restoration of the medullary osmotic gradient so that sensitivity to desmopressin is maintained. Frusemide seems to fulfil this criterion. It is recommended that diuretics are taken during the day to allow the body’s sodium load to be handled during the day, leading to lower sodium excretion at night and thus lower NUP. 68
Other treatments
Antimuscarinics
These are mainly used in patients with nocturia secondary to an overactive bladder or small bladder capacity, therefore they were not included in this review.
Conclusion
See Table 1.
Key points of nocturnal polyuria (NP).
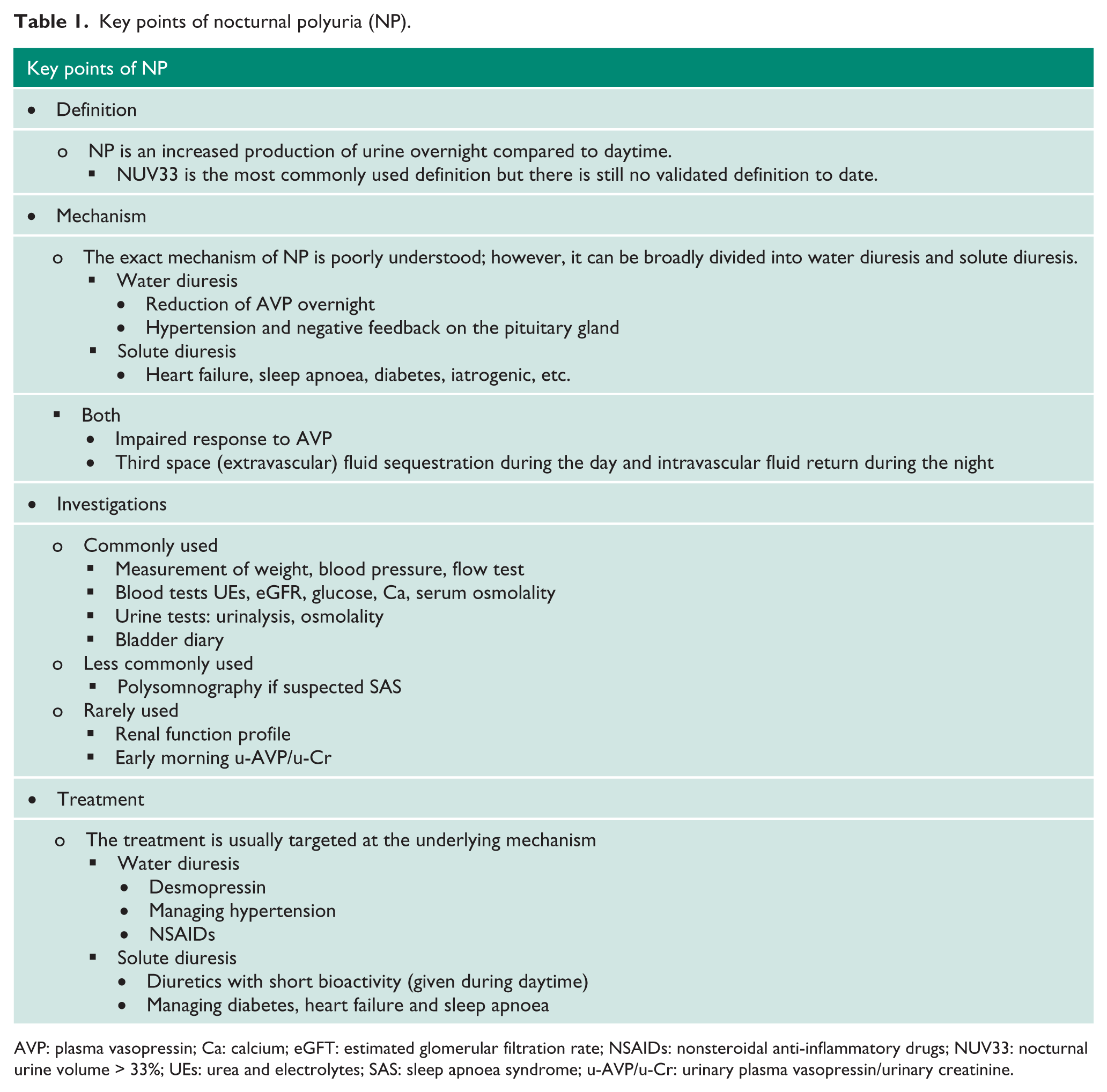
AVP: plasma vasopressin; Ca: calcium; eGFT: estimated glomerular filtration rate; NSAIDs: nonsteroidal anti-inflammatory drugs; NUV33: nocturnal urine volume > 33%; UEs: urea and electrolytes; SAS: sleep apnoea syndrome; u-AVP/u-Cr: urinary plasma vasopressin/urinary creatinine.
NP is the leading cause of bothersome nocturia and a complicated symptom of a multifactorial and potentially serious aetiology and increasing incidence with age. Treatments prescribed by urologists and primary care physicians are often empirical and lack understanding of the underlying pathophysiology of the condition. The latter involves hormonal, endocrinal, renal, cardiac and neurovascular systems.
There is a need to develop primary- and secondary-care algorithms based on multidisciplinary consensus to guide the correct investigations and treatment of this often-bothersome symptom. There is also a need to refine the currently available definitions with improvement in internal and external validity and better understanding of the pathophysiology that underpins NP to be able to advance treatment in this field.
Footnotes
Acknowledgements
None.
Correction notice
At time of publication, low dose desmopressin (Noqdirna) was approved for use in patients with nocturia due to nocturnal polyuria.
Conflicting interests
Mr Hashim: Speaker and advisor for Ferring and Astellas. No other conflicts of interest are declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
AK-I
Contributorship
Antoine Kass-Iliyya performed the literature search and wrote the first draft, modified it according to senior author comments and acted as the corresponding author. Hashim Hashim reviewed the initial draft, suggested changes, and reviewed the final draft before submission.