
Abstract
Objective:
The objective of this study is to describe how the use of digital rectal exam to triage patients to standard transrectal ultrasound (TRUS) biopsies or magnetic resonance imaging (MRI) then MRI fusion biopsies impacts cancer detection rates, departmental resources and the diagnostic journey.
Patients and methods:
A retrospective analysis of all patients undergoing prostate biopsies in a 15-month period following the introduction of triage digital rectal exam (DRE) and MRI at Ayr University Hospital was conducted. MRI usage and patient journeys were also examined.
Results:
A total of 95.5% of patients proceeding directly to TRUS had malignant histology and less than 1% required further investigation. Forty-nine per cent of patients who underwent triage MRI avoided biopsy and over one-third of patients with previously benign TRUS biopsies had clinically significant malignancy on MRI fusion biopsies. The pathway eliminated repeat TRUS biopsy and the number of biopsies a month decreased. MRI usage doubled and waiting times to diagnostic biopsy increased when compared to a one-stop diagnostic clinic.
Conclusion:
Triaging according to DRE avoided delays in cases of overt malignancy and increased the detection rate of standard TRUS. For those patients with a benign DRE, MRI enabled half to avoid biopsy. The increase in demand on MRI was mitigated, in part, by using a shorter detection protocol but institutions must be aware of the potential for delays to diagnosis.
Level of evidence:
4
Introduction
Prostate cancer is a common malignancy and, with the increased use of prostate-specific antigen (PSA) testing, efforts have been focussed on limiting over-diagnosis and overtreatment of clinically insignificant cancers. 1
Multiparametric magnetic resonance imaging (mpMRI) can be used as a triage test to avoid primary biopsy and potentially reduce the number of clinically insignificant cancers identified. 2 A five-point scoring system (prostate image reporting and data system, PIRADS) is used to stratify MRI scans and, although still a subject of some debate, biopsy is generally recommended in lesions classified as PIRADS 3, 4 or 5.2,3 MRI/ultrasound (US) fusion technology allows targeted transrectal biopsy of the lesion identified on MRI, and this has been shown to increase detection of malignancy on the first biopsy.4,5
There is not yet a consensus, however, on where these techniques should fit into the prostate cancer diagnostic pathway.2,6,7 In addition, most studies to date have failed to comment on the implications on departmental resources and the diagnostic time line. Here we report on our experience of integrating MRI and MRI fusion biopsies into the diagnostic pathway in a District General Hospital.
Ayr University Hospital has been using triage mpMRI followed by targeted and systematic biopsies for men presenting with a raised PSA and benign digital rectal exam (DRE) since 2014 (Figure 1). To rationalise this resource patients are triaged to MRI based on DRE findings. Patients with overt malignancy proceed directly to standard transrectal ultrasound (TRUS) biopsy. We ask how the introduction of this pathway impacts the diagnostic journey, departmental resources and biopsy detection rates.
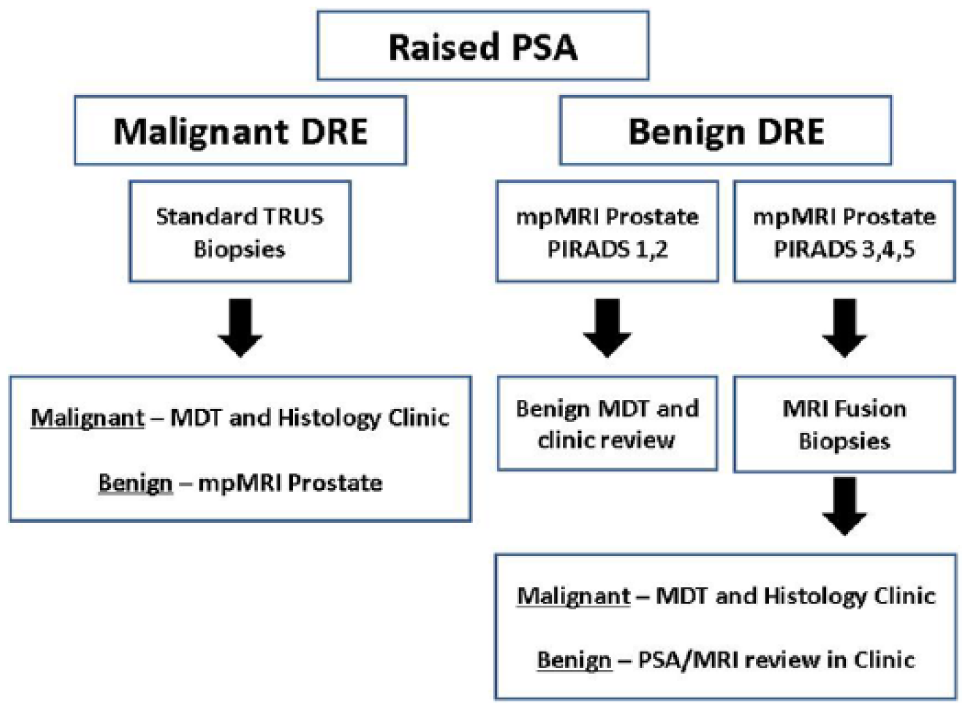
Prostate cancer diagnostic algorithm.
Methods
Patients investigated on the prostate cancer diagnostic pathway (Figure 1) between January 2015 and March 2016 were included in the analysis. Age-specific PSA ranges were used by the clinicians assessing patients. 8 Clinically significant disease was defined as Gleason 7 and above.
The study was approved as a local audit of service.
DRE
DRE findings were established in the clinical notes, and for the purposes of this study we distinguish two groups of patients: those recorded as benign or smooth and those described as malignant/T3/T4 disease. DREs were performed both by consultants and trainee.
MRI
A single 1.5T MRI scanner was used for all patients. Two protocols are used, both multiparametric using intravenous (IV) contrast. A detection protocol for pre-biopsy patients (30 minutes, excluding pelvic nodes) and staging protocol for those with a diagnosis of prostate cancer (45 minutes, including pelvic nodes). MRI scans were reported by one of two dedicated uro-radiologists according to PIRADS guidelines. 3
Prostate biopsies
TRUS biopsies were performed by or under the supervision of consultant urologists. Standard 10 cores were taken in patients with benign DREs. Fewer cores were taken at the discretion of the operator in patients with overt malignancy.
MRI fusion biopsies were performed under local anaesthetic using Artemis (Eigen, USA) by two consultant urologists in a day-surgery setting. Three to nine targeted biopsies were taken according to the size of the lesion, at the discretion of the operator. Standard systematic biopsies were also taken contemporaneously and did not include the target site.
The pattern of prostate biopsies within the department was reviewed from July 2013 to July 2016. The time frame was altered due to the absence of retrospective data before July 2013.
Timeline analysis
Two groups of patients, before (January 2013 to March 2014) and after (January 2015 to March 2016) the introduction of the new pathway, were identified from multidisciplinary team audit data. All patients had a new diagnosis of prostate cancer. Timeline analysis was carried out in the first 150 patients from each group. The patients were identified chronologically. A case note review was then carried out for each patient.
Results
Pathway outcomes
A total of 151 TRUS biopsies and 156 MRI/TRUS fusion prostate biopsies were performed between January 2015 and March 2016. Twenty-two TRUS and 18 MRI fusion biopsies were excluded as they were either performed as part of active surveillance or were not part of the pathway (e.g. DRE was benign and MRI contraindicated). An additional MRI biopsy was excluded as histology was insufficient.
Prostate MRI
During the first time period 441 MRI prostates were carried out, of which 161 were detection scans. This increased to 672 in the second time period, of which 348 were detection scans. The remaining scans were either staging scans or formed part of the active surveillance protocol.
Performing an initial shorter detection scan was time efficient. In the second time period 75 patients needed detection and staging scans. This additional 45-minute scan accounted for 56 hours of extra scanning time. However, if all detection scans had been carried out as staging scans initially there would have be 68.25 hours of unnecessary scanning time.
Of the 348 detection MRI scans performed 170 patients did not undergo prostate biopsy. Prostate biopsy was therefore avoided in 48.8% of patients referred for MRI.
Prostate biopsies
Figure 2 demonstrates the number of prostate biopsies performed per month; this includes those performed as part of active surveillance.
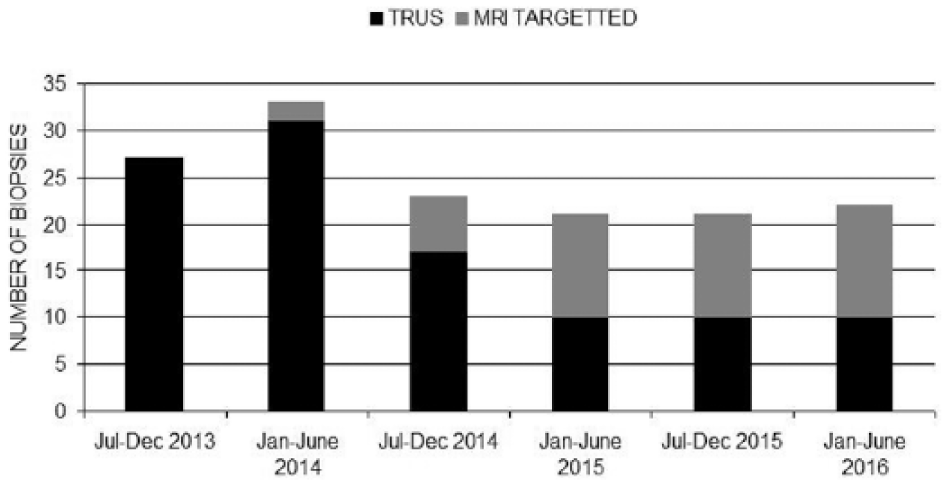
Number and type of prostate biopsies performed per month.
Following the introduction of the pathway, there were no repeat diagnostic TRUS biopsies performed. Four patients underwent repeat MRI fusion biopsies. Two patients underwent biopsy as part of the active surveillance protocol and two patients had high-grade prostatic intraepithelial neoplasia on the first biopsy and Gleason 3+3 disease on the repeat biopsy.
Complications associated with MRI fusion biopsies were assessed. Nine patients required admission and treatment with IV antibiotics after biopsy. There were no cases of urinary retention or bleeding requiring admission. The prophylactic antibiotic regimen was optimised during the study period to 750 mg ciprofloxacin, 240 mg gentamicin and three days of ciprofloxacin 500 mg twice daily (BD) (Supplementary Data S1).
Detection rates
All diagnostic biopsy results are detailed in Table 1. A total of 83.5% of standard TRUS biopsies and 40.1% of MRI fusion biopsies demonstrated clinically significant disease. All bar three clinically significant cancers identified on MRI fusion biopsies were identified in the targeted biopsies (Supplementary Data S2).
Histological outcome from diagnostic prostate biopsies (%).
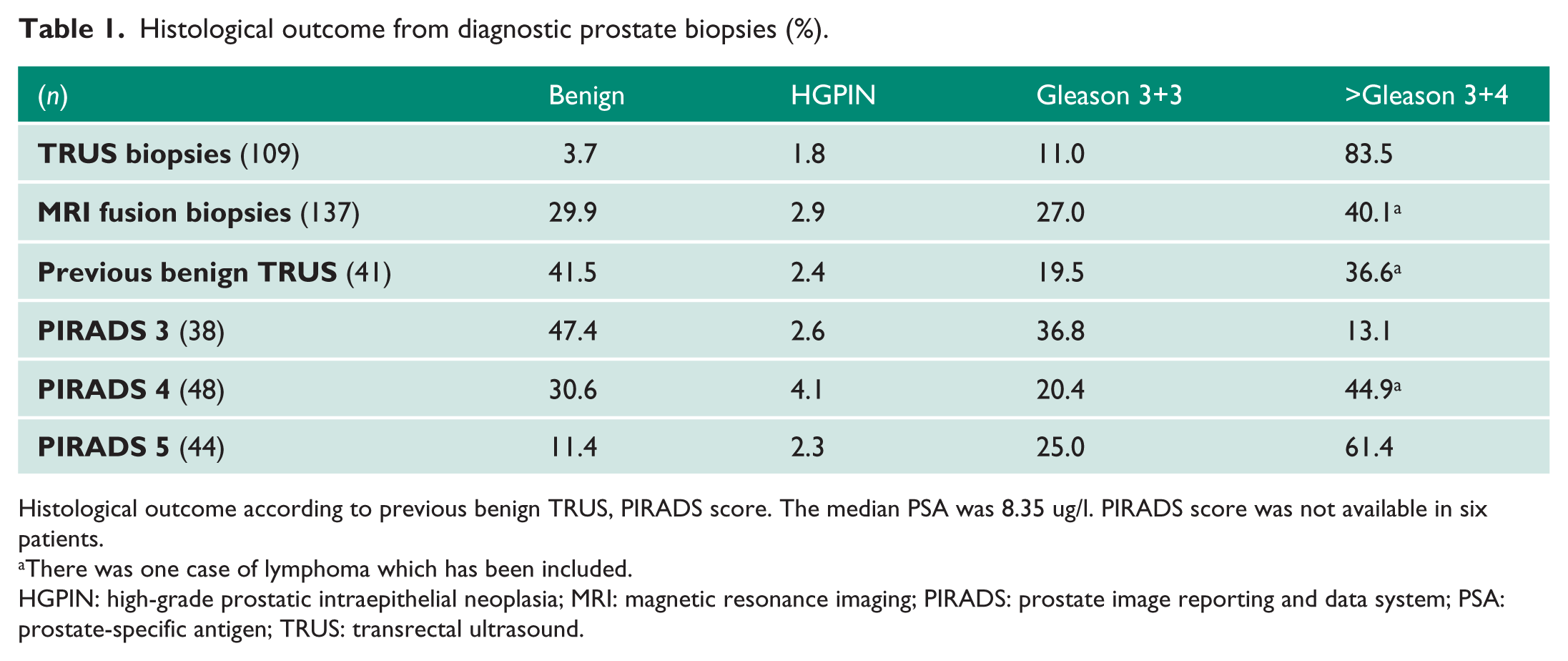
Histological outcome according to previous benign TRUS, PIRADS score. The median PSA was 8.35 ug/l. PIRADS score was not available in six patients.
There was one case of lymphoma which has been included.
HGPIN: high-grade prostatic intraepithelial neoplasia; MRI: magnetic resonance imaging; PIRADS: prostate image reporting and data system; PSA: prostate-specific antigen; TRUS: transrectal ultrasound.
There were four benign standard TRUS biopsies: No further biopsies were undertaken in two patients; one patient was found to have a bladder tumour invading the prostate and one patient underwent an MRI and then targeted biopsies; they were found to have clinically significant disease.
Time to diagnosis
The time from first clinic review to diagnostic biopsy was established in a cohort of 150 patients in each time period. Biopsies were not performed on 41 patients in the first cohort and 48 patients in the second time period. The time to diagnostic biopsy is shown on Figure 3. In the first cohort 17 patients underwent multiple biopsies; in the second cohort this had fallen to four patients.
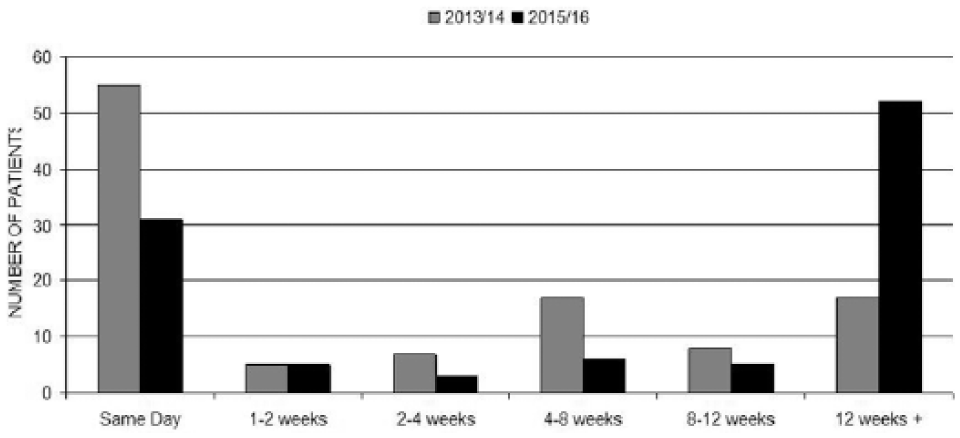
Time from first clinic review to diagnostic biopsy.
Discussion
This pathway aims to reduce the requirement of prostate biopsies while avoiding unnecessary delay in those patients with potentially high risk or advanced disease. Triage to standard TRUS or MRI based on DRE resulted in a 94.5% detection rate from standard TRUS biopsies and less than 1% of patients required further investigations following standard TRUS. In addition, as expected, triage MRI reduced the number of patients requiring prostate biopsies and the overall number of biopsies performed each month. However, as a consequence time to diagnostic biopsy increased.
In our study, 48.8% of patients who underwent MRI avoided biopsy, which is higher than reported elsewhere. 2 This may be because only patients with benign DRE findings underwent MRI or because MRI reporting practices will vary. We saw a higher percentage of malignancy in PIRADS 3 lesions than published elsewhere.2,9,10 This highlights a requirement for local audit and an understanding of variation in reporting between departments when comparing results.11,12
The format of biopsies following MRI remains controversial although MRI fusion has been shown to be superior.4–7 MRI fusion biopsies were well tolerated in our study and the rate of infection following biopsy was 5.5% and comparable to that reported in the literature.13,14 There were no cases of urinary retention, which had been reported to occur in 6.7% of patients undergoing trans-perineal biopsies.13,14 We also suggest that both targeted and systematic biopsies are taken contemporaneously. Although this increases procedure time, three cases of clinically significant cancer were identified in systematic biopsies in this study. Larger studies elsewhere have, however, suggested that this is not necessary and a consensus will be needed if this is approach is recommended nationally. 15
There was an increased time to diagnosis for patients requiring MRI, and this occurs because of waiting times for MRI and then biopsy. We used two approaches to mitigate potential increases in waiting time. Firstly, patients with overt malignancy go straight to biopsy and secondly, we use a shorter detection protocol to increase the number of scans that can be performed.
Currently national recommendations for waiting times for investigations are not cancer specific but ambition exists for 95% of patients referred for testing by a general practitioner are definitively diagnosed with cancer, or cancer is excluded within four weeks.16,17 As the prostate cancer diagnostic pathway changes, departments must be vigilant to patient and institutional expectations while institutional recommendations may need to be adapted given the resource implications of routine triage MRI and the indolent nature of low-risk prostate cancer.
We acknowledge two main limitations of this study: The first that it is a retrospective analysis of patient outcomes and the second that not all patients were biopsy naïve. However, we have been able to demonstrate the utility of this novel triage pathway and hope future prospective studies will validate this further.
Conclusion
Triage to MRI based on DRE avoids unnecessary delays in patients with overt malignancy and allowed half of patients with a benign DRE to avoid biopsy. However, if triage MRI is to become gold standard we need to ascertain recommended wait times for investigations and how departments will absorb the increased demand.
Supplemental Material
Supplementary_Material – Supplemental material for Triaging patients to primary biopsy or prostate MRI based on digital rectal examination improves the detection rate of TRUS biopsy and avoids unnecessary biopsies
Supplemental material, Supplementary_Material for Triaging patients to primary biopsy or prostate MRI based on digital rectal examination improves the detection rate of TRUS biopsy and avoids unnecessary biopsies by Elizabeth Day, Sarika Nalagatla, Je Song Shin, Biju Nair, Murat Gurun, Bob Meddings, George McLaughlin, David Chanock and Ross Clark in Journal of Clinical Urology
Footnotes
Acknowledgements
We would like to thank Prof H Leung for his assistance and guidance in this research.
Conflicting interests
The Authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
RC
Contributorship
ED: data collection, analysis and writing first draft of the manuscript. SN, JSS, BN, MG, BM, GMcL and DC: data collection. RC: conceived the study. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.