
Abstract
Trainee and established urologists are familiar with ‘generic mentoring’ as a potpourri of helping aids that include supervision, coaching, buddying, career advice, counselling and patronage to enable mentees to develop professionally. However, most are unfamiliar with ‘developmental mentoring’ as a highly specific learnt technique through which mentors help mentees, by interactive dialogue, to choose their own agendas and arrive at their own solutions to career/professional/personal opportunities or difficulties as distinct from the paternalistic mentor approach typified by the downward flow of information generated by ‘generic mentoring’. This paper is a systematic review of developmental mentoring as pertains to urologists in the UK, and reports outcomes of 1-hour taster sessions between Egan-trained mentors and urologists offered at British Association of Urological Surgeons (BAUS) annual general meetings since 2013. Both the General Medical Council and the Royal College of Surgeons of England imply that ‘mentoring’ is mandatory for both trainees and trained urologists, but fail to clarify what they mean by a ‘mentor’, which potentially creates a void in providing ‘developmental mentoring’ since the later requires specific training and is costly to provide. Currently, most ‘developmental mentoring’ is performed by trained staff in Local Education and Training Boards or National Health Service Trusts. BAUS has an opportunity to offer ‘developmental mentoring’ through a portal on its website to manage opportunities and difficulties experienced by its members.
Keywords
Definitions
For the purpose of this article, urologists are defined as those in the specialty with a national training number (NTN ST 3–7), post-CCT fellows, SAS and consultant urologists. 1
Mentoring is difficult to define, but most clinicians use it as a collective or generic term to describe ‘helping’ mentees, and within this tool box is included supervision, coaching, buddying, career advice, counselling and patronage. This potpourri of helping aids is delivered in an apprenticeship mentoring model with a paternalistic mentor/mentee approach yielding a downward flow of information to the mentee, who is most often junior to the mentor. This style of mentoring frequently ignores the individual mentee’s needs, as solutions to their opportunities or concerns are usually provided or coloured by the experiences of the mentor whose training in ‘generic mentoring’ is usually experiential, non-specific and not based on formal learning. Sometimes that is appropriate but often it is not.
Less well recognised is the term ‘developmental mentoring’, which is distinct from the aforementioned since it is based on the needs of the individual mentee rather than the experience of the mentor. This is a process in which the mentee sets both the agenda of the mentoring conversation and, importantly, provides their own solutions arising from their interactive dialogue with his or her mentor. We know from experience that this approach is more likely to result in moving their issue forward because the mentee has absolute ownership.
Developmental mentoring has been defined as ‘The process whereby an experienced, highly regarded, empathic person (the mentor) guides another individual (the mentee) in the development and re-examination of their own ideas, learning, and personal and professional development. The mentor who often, but not necessarily, works in the same organisation or field as the mentee, achieves this by listening and talking in confidence to the mentee’,
2
and it is about helping someone (the mentee) to manage their opportunities and problems more effectively by developing their own unused resources and potential. Mentors use various frameworks and techniques to guide the mentee in this interactive learning process. Different frameworks exist, but the two commonest are the Egan model and the GROW method. Both of these frameworks consist of establishing where the mentee is with a defined issue, where ideally they would like to be and then exploring how they will make this happen, whilst simultaneously considering the consequences of any action and then implementing a timeline for change to occur. Indeed, change is the quintessential endpoint of the mentoring process.
Importantly, developmental mentoring does not involve giving advice of any kind. The skilled mentor, through advanced communication skills, challenging dialogue, respect and empathy, is tasked with changing how the mentee perceives an opportunity or problem in order for the mentee to arrive at their own novel solutions. This is much more empowering and likely to achieve ongoing improvement of their problem-solving skills and self-confidence than an approach through patronage.
Developmental mentors require specific, dedicated training with an initial recognised course consisting of 2–4 days of lectures, interactive practical sessions, video simulation training, literature review and written course work. Thereafter, a commitment to providing a service in developmental mentoring with quality control peer review is necessary.
Currently, it is costly and poorly funded by the National Health Service (NHS) for clinicians in secondary care.
The term ‘coaching’ is often used synonymously with mentoring, largely because each process has overlapping elements. Coaching is generally accepted to be concerned with performance, is short-term and directed at achieving a prescribed level of a defined skill or skill set determined by the coach. A coach need not necessarily be more senior to the coachee or even in the same career structure.3,4
Requirement of developmental mentoring for urologists
The General Medical Council in Good Medical Practice acknowledges the importance of mentoring for the younger doctor, ‘You should be willing to take on a mentoring role for more junior doctors and other healthcare professionals’, 5 and in Leadership and Management it states: ‘You must make sure that staff who are new to an organisation or are moving into a new role have access to an appropriate mentoring arrangement, where relevant, depending on the nature of their clinical practice and their responsibilities’. 6
In Improving Surgical Training’, a proposal for a novel surgical training programme, the Royal College of Surgeons of England states in recommendation 6 of their document that, ‘trainees should have a consistent relationship with a trained educational supervisor and should have a separate and consistent relationship with a trained mentor’. 7
All three statements are ambiguous in using the respective terms ‘mentoring role’, ‘appropriate mentoring arrangement’ and ‘consistent relationship with a trained mentor’. This has potential implications regarding resource allocation, since training and utilising developmental mentors is a costly process compared with using assigned clinical and educational advisors. Certainly, all surgeons, especially trainees and newly established SAS and consultant urologists, need supervision, coaching, buddying, career advice, counselling and patronage, in other words ‘generic mentoring’, but clearly not all require formal developmental mentoring. However, they should know about it and where to self-refer when necessary.
Established SAS and consultant urologists in the NHS work in a complex environment where their resilience is tested on a daily basis. In a recent publication, 1380 urologists in Ireland and the UK were sent a questionnaire on stress in their jobs. Of 575 (42%) who responded, 15% reported using non-prescription drugs or alcohol to alleviate symptoms of burnout and 8% sought professional help. Of respondents, 80% said that burnout should be actively evaluated in their profession and 60% said they would avail themselves of counselling if it were available. 8 These findings clearly indicate the need for both ‘generic mentoring’ as well as developmental mentoring for established urologists in Ireland and the UK.
Interestingly, this has been identified as a generic problem for secondary care consultants for some time. A survey of a large DGH in 1995 showed that nearly 90% of consultants regarded having a mentor as a sign of strength, not a weakness. 9 Negative perceptions of mentoring are now redundant in the modern workplace.
Mentoring at the British Association of Urological Surgeons Annual General Meeting
Free taster sessions in developmental mentoring have been provided by trained Egan mentors (authors of this paper and others) for meeting delegates at each British Association of Urological Surgeons (BAUS) Annual General Meeting (AGM) from 2013–2018 .
In total, 145 1-hour 1:1 sessions were completed with a mean satisfaction score of 7.8 (range 5–10) on a scale of 1 (not helpful) to 10 (very helpful). Mentees comprised of 125 urology trainees, 10 SAS urologists, 8 consultant urologists and 2 medical representatives. Of these, 90% of mentees were not previously aware of the process of developmental mentoring.
Themes featured primarily on career opportunities (85%), which invariably led to an exploration into work–life balance issues. Not infrequently, trainees found the challenge of finding quality personal and family time versus time for training in a performance-regulated career advancement environment very stressful. Most trainees seeking mentoring sessions were ST 5–7 and largely concerned with consultant placement. Career problems for trainees featured less often (10%), and mostly concerned lack of surgical experience and Annual Review of Competency Progression decisions. Personal issues were infrequent (5%) .
Trainees found these mentoring opportunities useful and there was always competition for the limited number of slots at each AGM. Given the reported number of established consultant urologists reporting burnout in their professional lives, 8 it is rather surprising that their utilisation of the taster sessions was so low. This may have been because of difficulties matching mentees with mentors and concerns of confidentiality, or more likely competition with the very-full teaching component of the AGMs.
Two courses on developmental mentoring using the Egan model were held in 2013 and 2016.
Mentoring frameworks
Egan Skilled Helper model
The Egan Skilled Helper model 10 of developmental mentoring is based on a Standard Problem-Management Framework, which consists of three stages, each with three steps (Figure 1):
a) What’s going on?: current picture;
b) What does a better future look like?: preferred picture;
c) How do I get there?: action strategies.
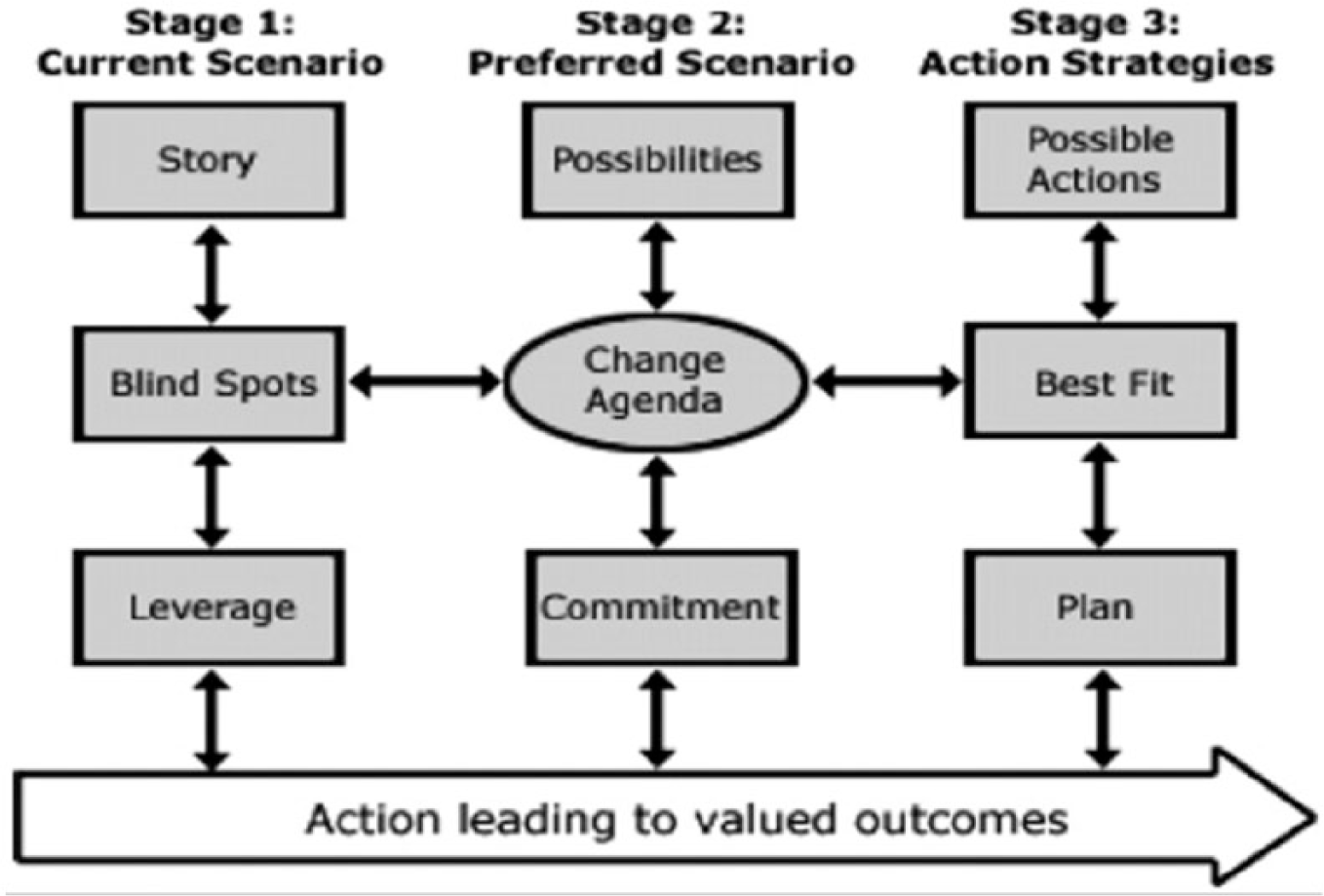
The Skilled Helper model. Source: http://www.vle.eastmidlandsdeanery.nhs.uk/course.
The GROW method
The GROW method, 11 conceived and popularised by Sir John Whitmore in ‘Coaching for Performance’ can be used to structure developmental mentoring conversations. It is particularly useful when a mentor is new to mentoring as it provides a framework that is easier to use than the Egan model.
GROW has four stages:
G – Goal setting for the session as well as for the short and long term: what do you want?
R – Reality checking to explore the current situation: what is happening now?
O – Options and alternative strategies, or course of actions: what could you do?
W – What is to be done: what will you do?
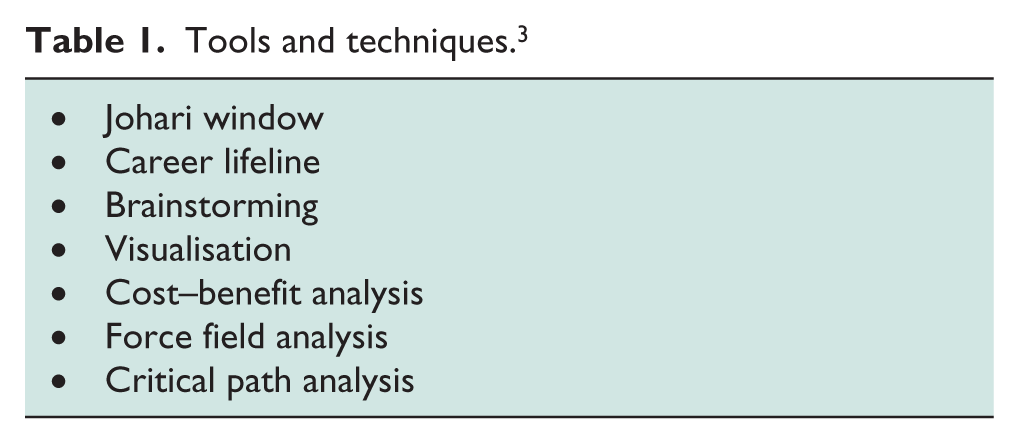
Within developmental mentoring conversations, mentors use various tools and techniques in whichever framework they are using to enable mentees to tell their story, explore possibilities, set goals, and develop and manage action plans (Table 1) .
Tools and techniques. 3
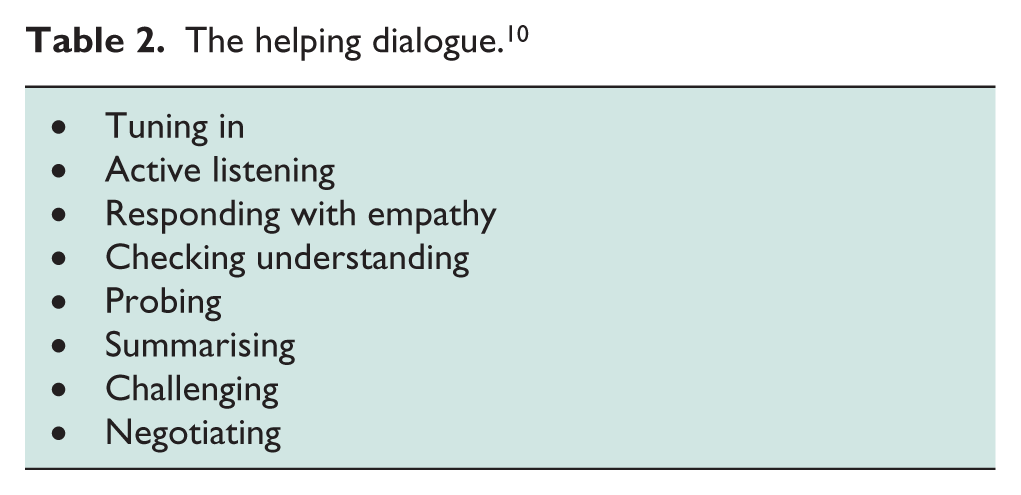
The developmental mentoring conversation requires the mentor to be an advanced practitioner in communication skills (Table 2)
The helping dialogue. 10
How effective is mentoring?
Quantitative evidence that mentoring is effective in clinical practice is lacking, but a recent systematic narrative review searched 12 databases for publications between 2006 and 2016 concerned with relationships between mentoring activities and the health and well-being of doctors. The initial search returned 4669 papers and, after exclusions, a full-text analysis of 37 papers was conducted. From these, 13 papers were selected for review. The findings were that mentoring positively influenced collegiate relationships, networking and aspects of personal well-being, such as confidence and stress management, and was valued by doctors as a specialist support mechanism for professional practice. 12
Ackroyd and Adamson in 2015 published a review paper on ‘Mentoring for new consultants’ to popularise their mentoring scheme at the Royal College of Physicians of Edinburgh. 13 They suggested that mentees acquired increased job satisfaction, greater self-confidence, improved objectivity with problem solving and ability to implement change, and importantly improved work–life balance. They advanced that mentoring new consultants ‘could lead to better care provision and indirectly contribute to the quality of the healthcare delivered’.
Conclusion
Consultant urologists can and do offer generic mentoring to trainees, SAS and other consultant colleagues, largely as a result of their own experiences and a desire to help train the newer generation of urologists. Most do this under the guise of surgical tutor, assigned clinical supervisor, assigned educational supervisor, training programme director, SAC member or clinical director. However, few in these positions are able to offer developmental mentoring since this requires specific training, the acquisition and maintenance of certain skill sets, which needs to be quality assured. Nevertheless, it is imperative that every urologist understands what developmental mentoring means, when it might be needed and how it can be accessed .
To promote a clearer understanding of developmental mentoring by urologists, the authors of this paper delivered 145 1-hour 1:1 taster sessions at BAUS AGMs between 2013 to 2018, achieving a mean satisfaction score of 7.8 on a 10-point scale where 1 = not helpful and 10 = very helpful. Most mentoring conversations primarily featured issues concerning career opportunities.
The importance of resilience is increasingly recognised given the difficulties of training and working in a complex NHS environment, and developmental mentoring has an important role here in the management of personal and professional difficulties. 8 However, developmental mentoring is more commonly used to develop opportunities and potential, especially in trainees and newly appointed consultants, with proven benefits both to them and the organisations in which they work.
A list of regional trained developmental mentors with visible biographies to allow mentee/mentor matching featured on the BAUS website would be one way for potential mentees at any level to self-refer ‘offline’ to secure confidentiality of their mentoring conversations.
In summary, developmental mentoring allows the mentee, through one-to-one confidential conversations with their mentor, to be challenged and encouraged to fulfil their potential and aspirations, or resolve their difficulties using their own solutions. It can be useful at all stages of a career.
Footnotes
Acknowledgements
The authors wish to thank BAUS for sponsoring the taster mentoring sessions at their AGMs, which has allowed developmental mentoring to be more widely appreciated by the urological community.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Contributorship
All authors contributed to content and the revision of drafts. TT conceived the original concept for the paper and wrote the first draft, which was subsequently reviewed by GF and NR, along with subsequent drafts. TT conceived the idea of the article from reviewing experience at the BAUS AGM’s developmental mentoring sessions between 2013–2018, at which GF and NR were the other principal Egan mentors.
Guarantor
TT.