
Abstract

Case
A 42-year-old male presented with an impacted, thick stainless steel ring around the base of his penis, allegedly placed four weeks prior by someone else whilst unconscious. Distally, the penis demonstrated oedema and he had difficulty voiding (Figure 1). Under a spinal anaesthetic, with assistance from the fire brigade, a high-speed electronic cutting device was needed to split the ring in two diametrically opposed locations. A wooden tongue depressor was used to separate the ring from the underlying skin and a saline drip used during the procedure to aid cooling (Figure 1). A flexible cystoscopy showed urethral blanching and therefore a urethral catheter was inserted for 24 hours. He initially made an uneventful recovery, but re-presented at day 8 with bacteraemia requiring intravenous antibiotics. He subsequently improved, but failed to attend follow-up appointments.
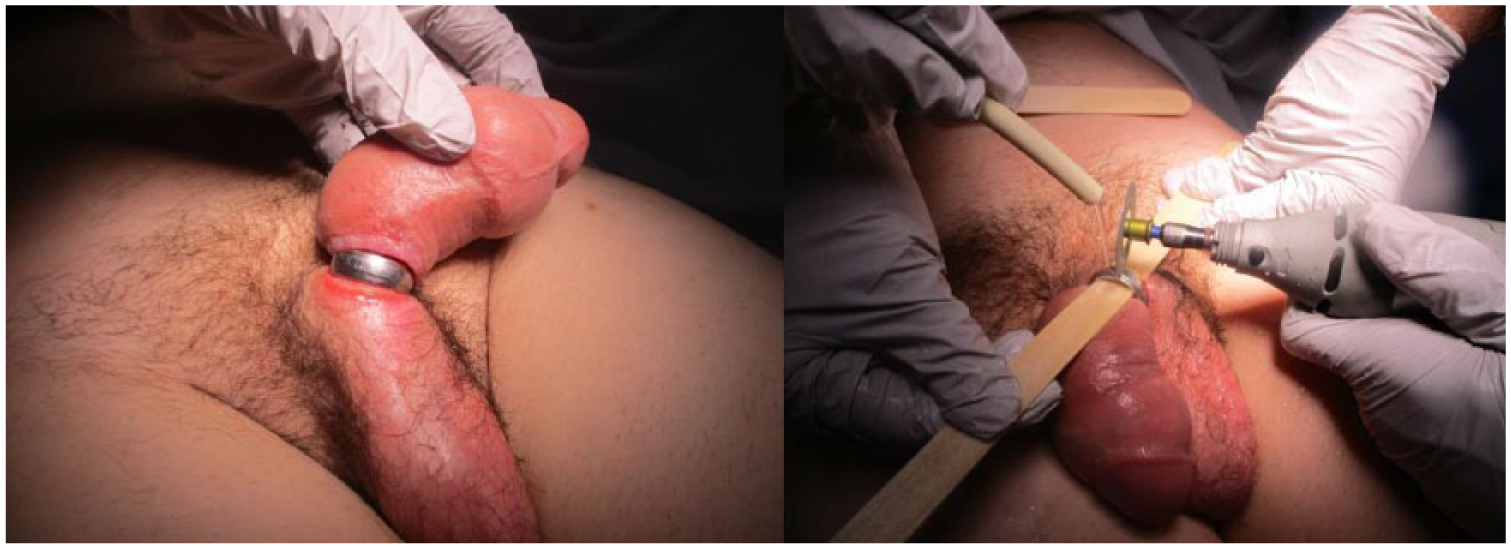
(Left) Stainless-steel ring at the base of the penis causing strangulation, with skin ulceration at the level of the ring and distal penile oedema. (Right) Removal of the penile ring with high-speed cutter, with interposition of a wooden tongue depressor and continuous saline irrigation.
Discussion
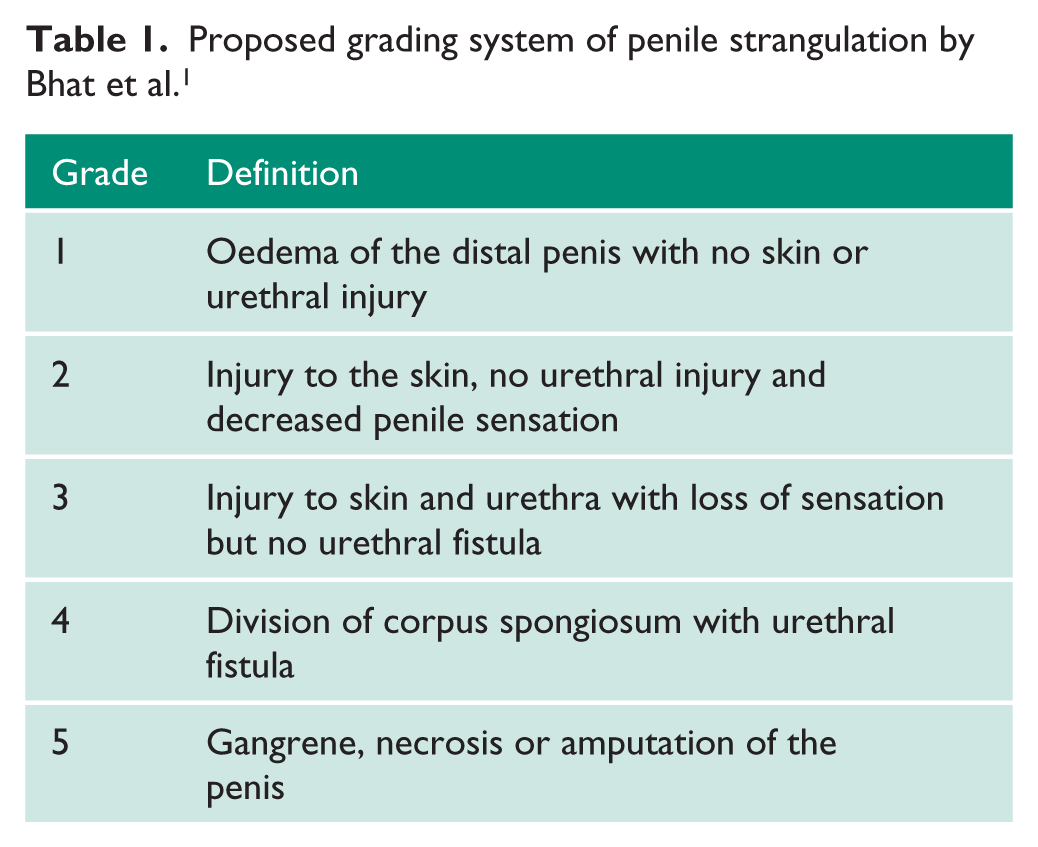
Penile strangulation is a urological emergency requiring urgent intervention. A grading system proposed by Bhat et al. 1 grades the severity of these injuries and is useful in clinical practice (Table 1). The severity of injury varies greatly, but the literature support the view that presentation after 72 hours is associated with higher-grade injuries. 2 The size, position, duration and composition of the ring affect ease of removal. Use of anaesthetic enables any surgical corrections, skin debridement, urethroscopy and catheter placement to be performed. Clinicians should also give tetanus prophylaxis as required.
Proposed grading system of penile strangulation by Bhat et al. 1
This case highlights our preferred surgical method for removing an impacted, thick penile ring and also an unusual case of chronic strangulation. Multiple different removal options are available, often adopting a stepwise progression of techniques. This ranges from removal under local anaesthetic with lubrication to medical ring-cutting devices.
The use of medical ring cutters (manual or electronic – Figure 2) can be the first-line option for smaller rings. Solid, thick or dense rings are often resistant to these devices and need removal with a more powerful electronic, oscillating multifunction tool with a diamond-surface cutting device (Figure 2). Such devices are not routinely available in hospital, but fire departments often have one.

Different commercially available ring-cutting devices.
In our case, the thickness of the stainless steel ring meant a conventional ring-cutting device was ineffective and a high-speed oscillating tool was needed. Previous reports advocate the interposition of a metallic object to protect underlying tissues during removal of penile rings. 3 Heating of the cutting blade or ring can occur with any device; therefore consideration of irrigation is important to avoid thermal tissue damage.
Our case highlights an alternative method, using a wooden barrier tongue depressor and irrigation. We feel this is safer as wood is less likely to conduct heat. Continuous cooling via saline irrigation is a simple addition to reduce the blade/ring/depressor temperature, preventing further thermal injury. Urethral injuries are consistent with grade 3 injuries and above; therefore all removals should have a formal urethroscopy. Postoperative antibiotic cover is important to prevent wound and systemic sepsis, as occurred in our case eight days after the operation.
Footnotes
Acknowledgements
None.
Conflicting interests
The Authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Redcliffe Hospital, Queensland, Australia, does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for his information to be published in this article with identifying information removed.
Guarantor
M.C.
Contributorship
M.C. wrote the first draft of the manuscript. Both authors reviewed and edited the manuscript and approved the final version of the manuscript.