
Abstract

Case
A 58-year-old woman presented with right flank pain, dysuria, fevers and vomiting. She reported anaphylaxis to seafood, topical iodine antiseptic and also intravenous contrast. Urine culture grew Escherichia coli, and a computed tomography (CT) scan revealed a small vesicoureteric junction calculus confirming the diagnosis of urosepsis secondary to an obstructed ureteric calculus.
She required out-of-hours ureteric stenting, but there was no alternative contrast agent available and no interventional radiology service out of hours. She was transferred to intensive care for intravenous antibiotics and vasopressors, while an appropriate contrast agent was sourced. The patient received a cystoscopy, retrograde pyelogram and stent insertion six hours later after Gadovist® (gadobutrol, Bayer©, Canada) was sourced from a nearby facility. A total of 7.5 ml of undiluted Gadovist was used for a retrograde pyelogram intraoperatively (Figure 1). This contrast media provided technically adequate image quality for the procedure with no adverse reaction. The patient made an uneventful recovery and received definitive stone clearance at a later date with no long-term sequalae.

Right-sided retrograde pyelogram using Gadovist (gadobutrol) as an alternative contrast media. The image quality from the Gadovist during the retrograde pyelogram was perfectly acceptable to aid ureteric stent placement.
Discussion
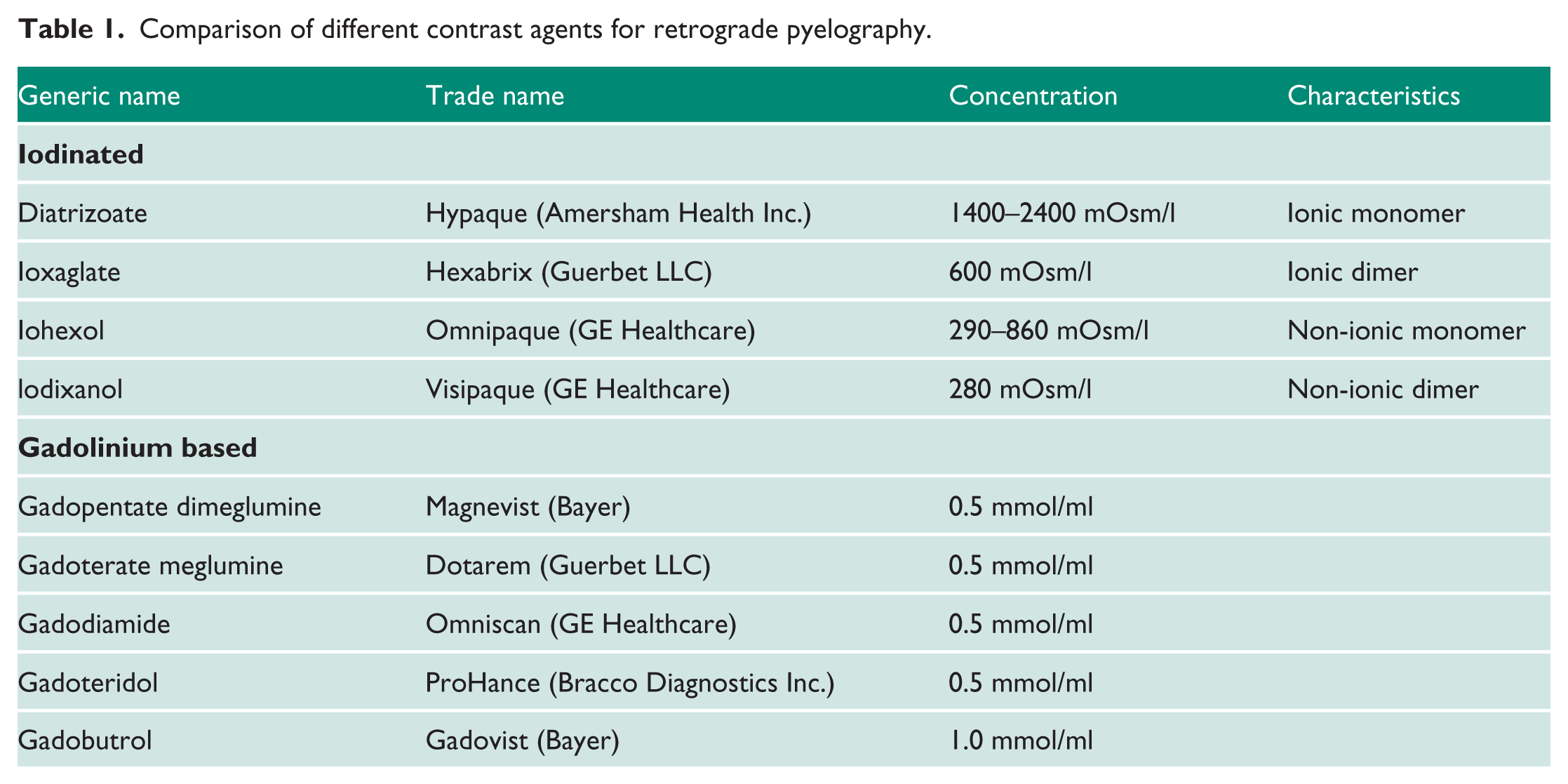
Retrograde pyelography is commonly performed as part of urological procedures to visualize the renal collecting system and to guide diagnosis and management. Many different contrast agents are available, as seen in Table 1. The usual agent used is a non-ionic iodinated contrast such as iohexol. There are reported cases of patients having anaphylactoid reactions to contrast during urological interventions. 1 Whilst insertion of ureteric stents can be performed without contrast, the use of contrast can aid in difficult cases, particularly for less-experienced clinicians.
Comparison of different contrast agents for retrograde pyelography.
There is a common misconception that allergy to iodine or seafood is a contraindication to the use of iodinated contrast. However, studies have shown that the risk of a reaction to iodinated contrast with this history is similar to that in patients with other food allergies or asthma, and even previous reactions to iodinated contrast does not increase the risk of a severe reaction. 2
Therefore, the only contraindication to iodinated contrast agents is anaphylactic reaction to iodinated contrast. Healthcare workers are often uncomfortable using iodinated contrast in the presence of iodine or seafood allergy despite the literature stating otherwise. 3
Gadolinium-based contrast has been shown to be useful in retrograde pyelography, but with older formulations such as gadoteridol, which is lower in concentration than gadobutrol. 4 Gadobutrol (Gadovist) is now commonly used as contrast for magnetic resonance imaging. Knowledge about this alternative contrast agent remains mixed in our experience with regards to dose, dilution and appearance under an image intensifier.
The attenuation for iodinated contrast is three to five times greater than that of gadolinium, meaning gadolinium-based contrast should not be diluted and higher volumes may be required for comparable images. 5 As seen in Table 1, gadobutrol has twice the concentration of other gadolinium contrasts, making it more suitable for retrograde pyelography. To date there are no cases report of nephrogenic systemic fibrosis or gadolinium brain deposition with the use of gadolinium in the urinary tract, which are potential complications of gadolinium contrast.
Gadobutrol is an effective alternative contrast media that should be used if a patient describes an anaphylactic reaction to previous iodinated contrast only. Iodinated agents are safe to use in patients with documented reactions to seafood or iodine, including anaphylaxis. We advocate undiluted gadobutrol at a standard 1.0 mmol/ml concentration with at least 20 ml prepared for use in retrograde pyelograms when needed.
Footnotes
Acknowledgements
None.
Conflicting interests
The Authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Redcliffe Hospital, Queensland, Australia does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Guarantor
M.Y.C.
Contributorship
M.Y.C> wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.