
Abstract
Objective:
To determine the rate of incidental urological findings in patients undergoing computed tomography (CT) colonography/CT colonoscopy (CTC) for investigation of suspected colorectal cancer.
Methods:
Retrospective analysis of patients undergoing CTC between January 2011 and December 2013. All patients with new incidental urological findings were included with their type and number of urological findings. These were stratified as per the colonography reporting and data system (C-RADS) criteria, and a note made of any further imaging, intervention and histology where appropriate.
Results:
Within the time period, n = 1891 CTCs were undertaken. Of these, n = 333 (17.6%) had an incidental urological finding and n = 41 of these patients had dual incidental urological pathologies. In total, n = 49 had significant pathology which required monitoring, further imaging, and medical or surgical intervention; n = 12 required further imaging. In n = 1, the imaging result led to a decision to operate and in n = 9 the results excluded the need for surgical intervention; n = 24 underwent operative intervention. The rates of incidental urological findings were similar to those quoted in literature.
Conclusion:
Our study demonstrates a 17.6% rate of incidental urological findings. Of all findings, 13.1% were deemed significant to warrant further investigation or intervention, and 7.2% of patients with urological findings required intervention. CTCs can adequately image renal masses and further imaging of renal masses did not change management.
Introduction
Computed tomography colonography/CT colonoscopy (CTC) has become an established efficacious technique for colorectal cancer screening in the last 10–15 years, with high interobserver reporting correlation and good patient acceptance. 1 It is frequently utilized as an alternative to colonoscopy where the patient is deemed unsuitable to undergo the procedure.
CTC is a minimally invasive imaging technique of examining the colon and rectum for endoluminal pathologies. In addition to this, it can provide crucial locoregional staging information. CTC requires patients to consume a faecal tagging agent with or without the use of full purgative laxatives. 2 Patients then undergo a CT scan with intravenous contrast. This provides excellent cross-sectional imaging of the lower thorax, abdomen and pelvis, which allows for staging of colorectal cancers but also highlights underlying extracolonic abnormalities.
Incidental findings are defined by being unrelated to the purpose of the requested investigation. In the instance of CTC, this includes the lung bases, and all the pelvic and abdominal contents. Whilst many are benign and inconsequential, a small number will be serious or potentially serious for the patient, which increases with age and symptomatic indication for the CTC.3,4
The colonography reporting and data system (C-RADS) classification has been developed to stratify colonic and extracolonic findings by potential seriousness (Figure 1). 5 Although there is perceived benefit of earlier detection, and therefore potential treatment of significant findings at an asymptomatic stage, there is also patient anxiety whilst waiting for further tests or intervention.1,6
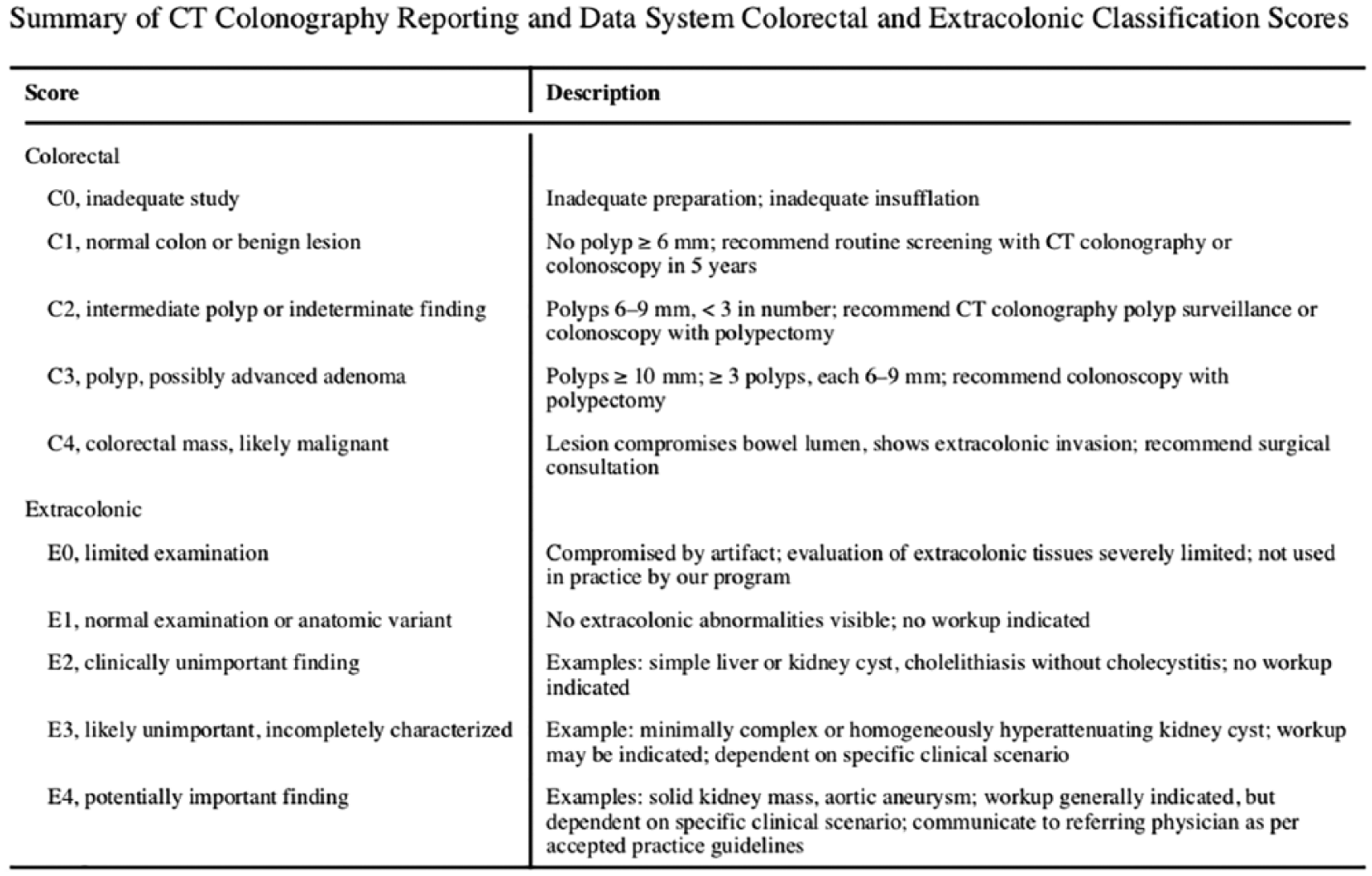
Summary of colonography reporting and data system criteria as per Zalis et al. 5
Here, we describe the incidental rate of new urological findings in patients undergoing CTC for the assessment of colorectal cancer in a medium-sized teaching hospital.
Our aim was to determine the incidence of urological findings in patients undergoing CTC, and determine the incidence of significant urological findings requiring further diagnostic workup and treatment.
Method
Retrospective cohort analysis was undertaken of patients undergoing CTC for suspected colorectal cancer at a medium-sized teaching hospital from January 2011 to December 2013.
All patients undergoing CTC were included. All scans were reported by one of three consultant radiologists. All patients with extracolonic non-urological abnormalities were excluded. Where patients had more than one urological abnormality, they were classified as two separate abnormalities within the data. All urological findings reported within the CTC report were correlated with all prior abdomino–pelvic imaging reports and any previous findings were excluded. Where a change was reported in previous findings, this was classed as a new finding.
All urological abnormalities were then stratified by the authors as per the C-RADS criteria5,7 (Figure 1). All patients with E3 or E4 abnormalities were reviewed to assess if any further diagnostics or therapeutic intervention had been undertaken, and a note made of any relevant histology.
Unless otherwise stated, all diagnosis mentioned should be assumed to be radiological.
We did not document the colorectal findings from the outset as, whilst interesting, they would not change the focus or message of this paper, which concerns incidental urological findings.
Results
In total, 1891 patients underwent CTC during the time period. The mean age of the cohort was 69.2 and 58% were female.
Of the patients, n = 333 (17.6%) had incidental urological findings, with n = 41 having two separate urological findings equating to a total of 374. The C-RADS criteria for the findings are displayed in Table 1.
Tabulation of colonography reporting and data system criteria and associated frequency of findings.
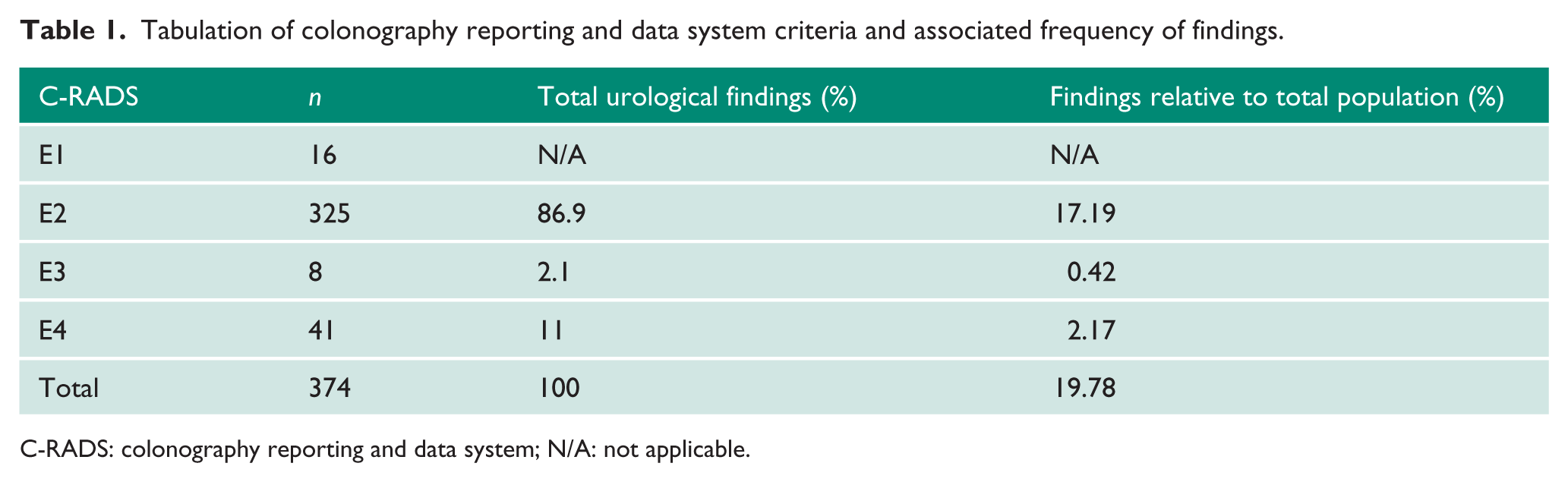
C-RADS: colonography reporting and data system; N/A: not applicable.
E1 findings were anatomical variants, which included the retroaortic vein (n = 3), duplex kidney (n = 3), extrarenal pelvis (n = 3), horseshoe kidney (n = 6) and cross-fused renal ectopia (n = 1). These are anatomical variants as per C-RADS and are thus not included as pathological incidental findings.
E2 scans comprised the majority of the findings. This was predominantly due to simple renal cysts that accounted for 44.9% (Table 2) of the total urological abnormalities. In addition, they include the following: adrenal adenoma, renal atrophy benign prostatic enlargement (no evidence of outflow obstruction), prostatic calcification, renal calculi, angiomyolipoma, mild hydronephrosis (unilateral), dilated renal pelvis, adrenal lipoma, cortical scarring, bladder calculi, bladder diverticulae, benign adrenal nodule, adrenal inflammation and adrenal infarct.
Tabulation of number of incidental urological findings in descending order of frequency.
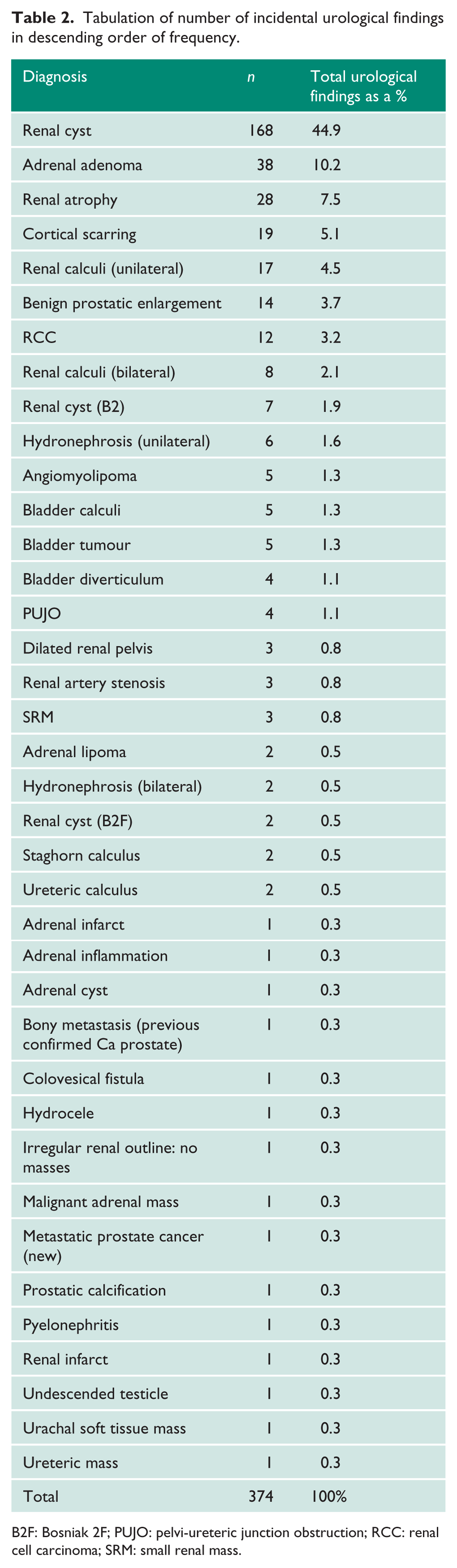
B2F: Bosniak 2F; PUJO: pelvi-ureteric junction obstruction; RCC: renal cell carcinoma; SRM: small renal mass.
Some findings where they would have otherwise been E2 were classed as either E3 or E4 due to associated significant complications from them.
E3 findings totaled n = 8 and consisted of: n = 1 segmental renal infarct with no cause found on the scan, n = 4 pelvi-ureteric junction obstructions (PUJOs) that were incompletely characterized on the CT, n = 2 Bosniak 2Fs that required further imaging and n = 1 angiomyolipoma that required a further scan for complete characterization.
E4 findings are as tabulated (Table 3), but equated to either having a new malignancy or significant radiological abnormality warranting intervention, or further clinical or radiological follow-up.
E4 lesions divided by regions of the urinary tract with associated modality and frequency of findings.
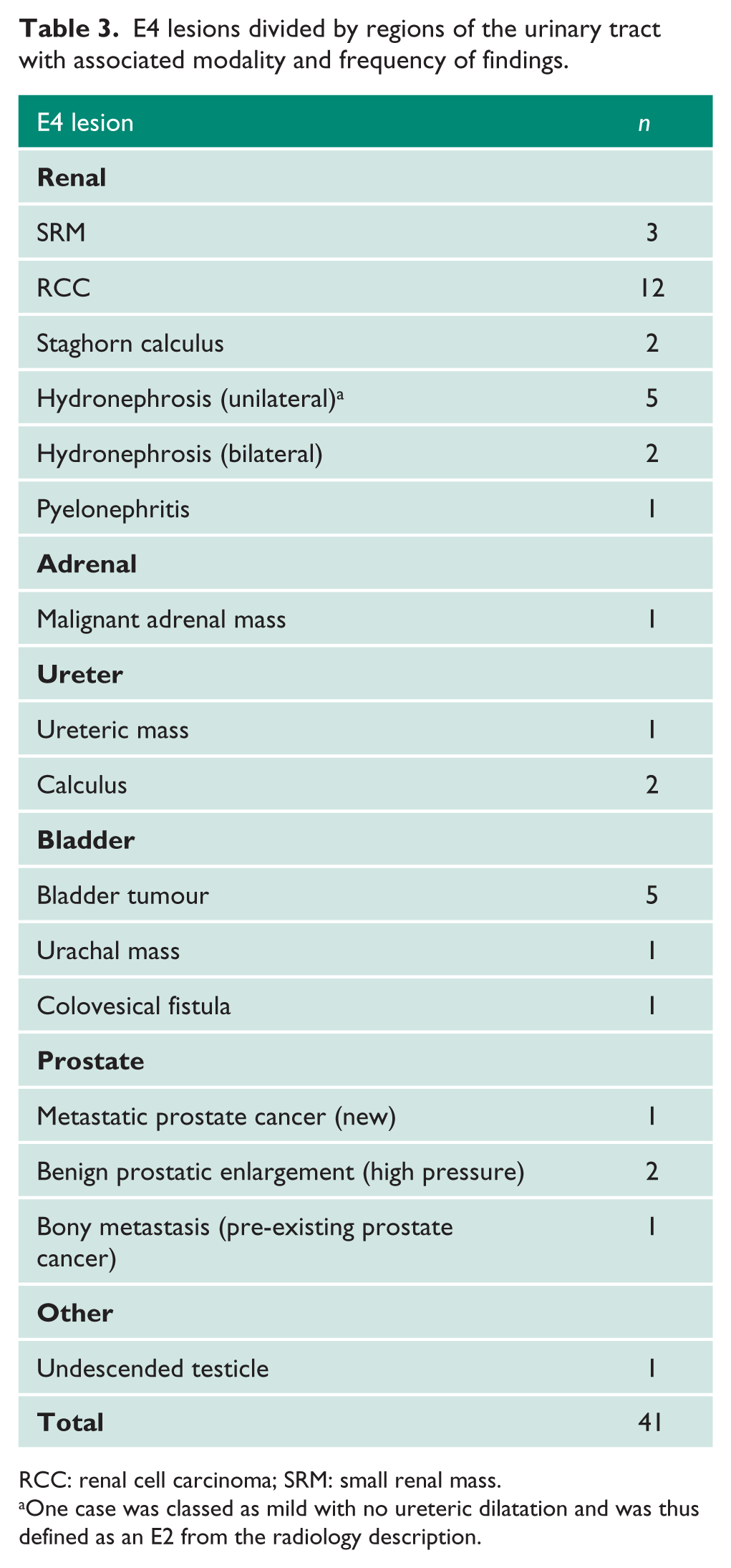
RCC: renal cell carcinoma; SRM: small renal mass.
One case was classed as mild with no ureteric dilatation and was thus defined as an E2 from the radiology description.
Significant renal pathology
In total, n = 12 were reported as renal cell carcinomas (RCCs). Of these, n = 10 underwent radical nephrectomy and n = 1 underwent a partial nephrectomy, while n = 1 was unfit for surgery and went on radiological surveillance.
Of the n = 3 small renal masses (SRMs), n = 2 were put on surveillance; n = 1 had previously had a partial nephrectomy and underwent a biopsy, which demonstrated a benign lesion. Of the SRM patients, n = 2 died within 1 year of the scan from unrelated causes.
Whilst there were a total of n = 6 unilateral hydronephrosis cases, n = 1 was classed as mild with no ureteric dilatation and was thus defined as an E2 from the radiology description, n = 5 were new moderate to severe hydronephrosis and n = 4 were associated with a subsequent causative pathology: n = 1 due to benign prostatic enlargement, n = 1 due to ureteric mass, n = 1 due to bladder tumour and n = 1 due to an abdominal aortic aneurysm.
There were n = 2 cases of bilateral hydronephrosis. Of these, n = 1 had concurrent radiological benign prostatic enlargement and underwent endoscopic resection of the prostate, while n = 1 had concurrent new metastatic prostate cancer radiologically that, on biopsy, was proved to be metastatic bladder cancer; for the purposes of the article, we have included the radiological diagnosis.
There were n = 2 incidental staghorn calculi. Of these, n = 1 underwent a DMSA at the time the data was collected and had a non-functioning kidney; n = 1 was discussed by the multidisciplinary team (MDT) and was for a PCNL for symptomology, while n = 1 had a radiological pyelonephritis and was treated accordingly.
Significant adrenal pathology
On initial CTC, n = 1 adrenal mass was deemed malignant. Further characterization required through a dedicated adrenal CT after 6 months demonstrated a benign lesion with an absolute washout of 78%. However, biochemistry was suspicious for a functioning adenoma causing Cushing’s disease and the patient was referred for intervention.
Significant ureteric pathology
There were n = 3 significant ureteric pathologies, of which n = 1 was a ureteric mass with an associated hydronephrosis requiring surgical intervention. Ureteric calculi represented n = 2: n = 1 was a proximal ureteric calculus that required ureteroscopy and laser lithotripsy, and n = 1 was a renal pelvis stone that underwent stone follow-up.
Significant bladder pathology
Within this cohort, n = 5 bladder tumours were noted. All patients underwent a rigid cystoscopy, with n = 1 having had a cold cut biopsy and n = 4 having formal resection.
The urachal mass underwent a flexible cystoscopy, which demonstrated a normal bladder and, after discussion in the MDT, had an interval CT scan to reassess status (Table 4). They subsequently died from a mesothelioma.
Patients requiring further imaging with outcomes of follow-up where appropriate.
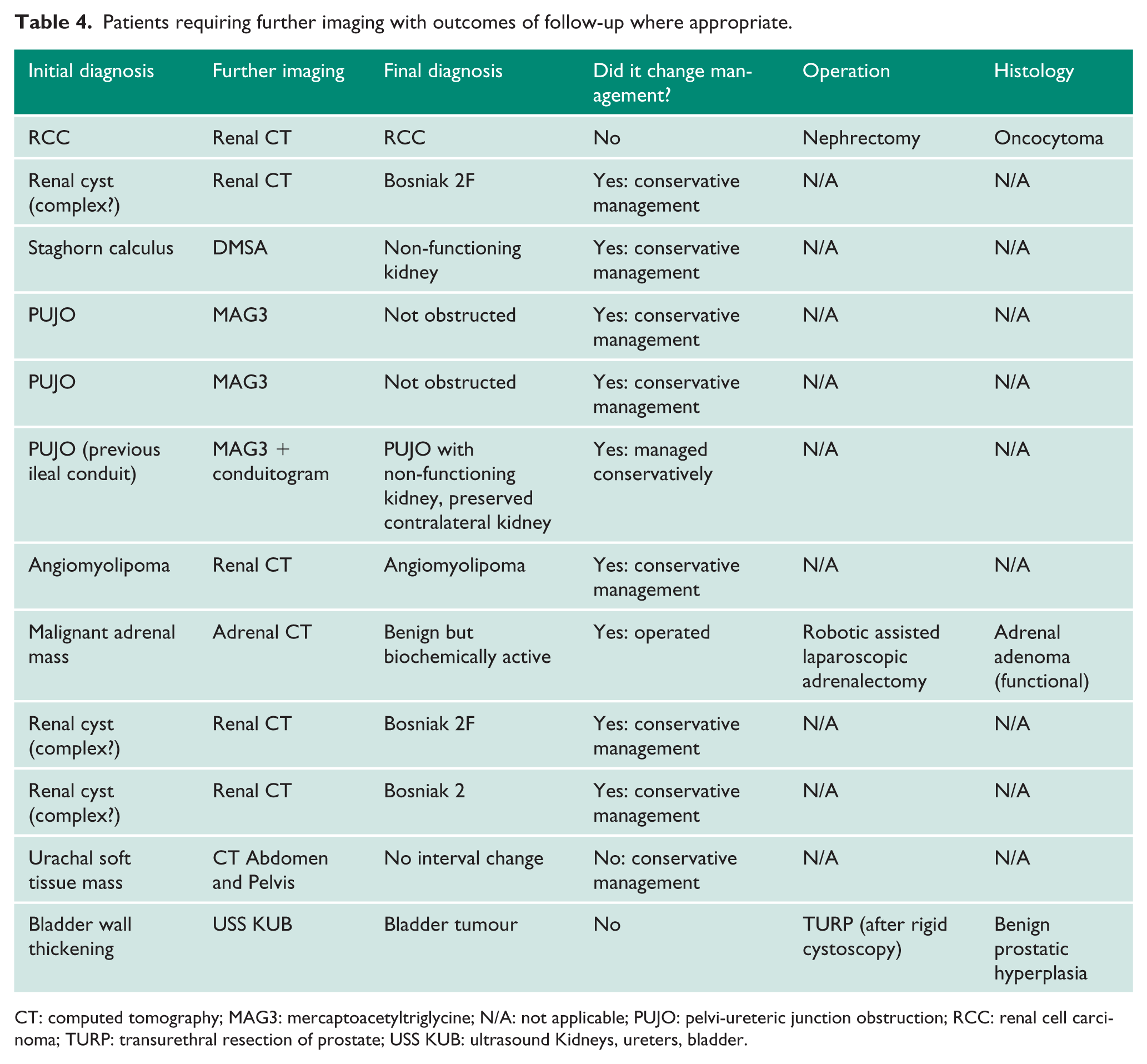
CT: computed tomography; MAG3: mercaptoacetyltriglycine; N/A: not applicable; PUJO: pelvi-ureteric junction obstruction; RCC: renal cell carcinoma; TURP: transurethral resection of prostate; USS KUB: ultrasound Kidneys, ureters, bladder.
A thickened bladder was found in n = 1, with associated intravesical gas that was reported as a colovesical fistula but not completely characterized. The patient subsequently underwent a rigid cystoscopy that confirmed the diagnosis.
Significant prostate pathology
Of the patients, n = 1 had a new radiological diagnosis of metastatic prostate cancer; however, biopsy demonstrated transitional cell carcinoma (TCC) and the patient was treated as a metastatic bladder cancer case.
Radiologically, n = 2 patients had new onset bilateral hydronephrosis with enlarged prostates, and were appropriately assessed and treated as high pressure chronic retention.
A new diagnosis of sclerotic bony metastasis was found for n = 1. The patient was noted to have underlying prostate cancer with a rising prostate-specific antigen level, and this was thus reported as metastatic prostate cancer.
Other significant pathology
An undescended testicle was reported for n = 1 and the patient was referred for assessment accordingly. At the time of data collection, no further scans had been undertaken.
Findings requiring further imaging
In total, n = 12 patients required further imaging to either clarify a diagnosis or for further assessment (Table 4). Of the patients that required additional imaging, n = 9 had a conclusive diagnosis and were managed conservatively. Of note, only n = 3 of the PUJO cases had further scans to confirm diagnosis and split function. One PUJO did not as there was significant cortical atrophy on the original scan and the patient was asymptomatic.
Patients requiring operative intervention
Of the patients, n = 24 required operative intervention (Table 5). Of these, n = 12 underwent nephrectomies (radical: n = 10, partial: n = 1 or nephroureterectomy: n = 1), n = 3 required TURBT, n = 2 required TURP and each subsequent modality had only one patient undergoing the intervention (n = 1) for the following: renal biopsy, ureteroscopy and laser lithotripsy, percutaneous nephrolithotomy (PCNL), robotic assisted laparoscopic adrenalectomy, a flexible cystoscopy and a rigid cystoscopy.
Patients requiring operative intervention with modality, frequency and results, where appropriate.
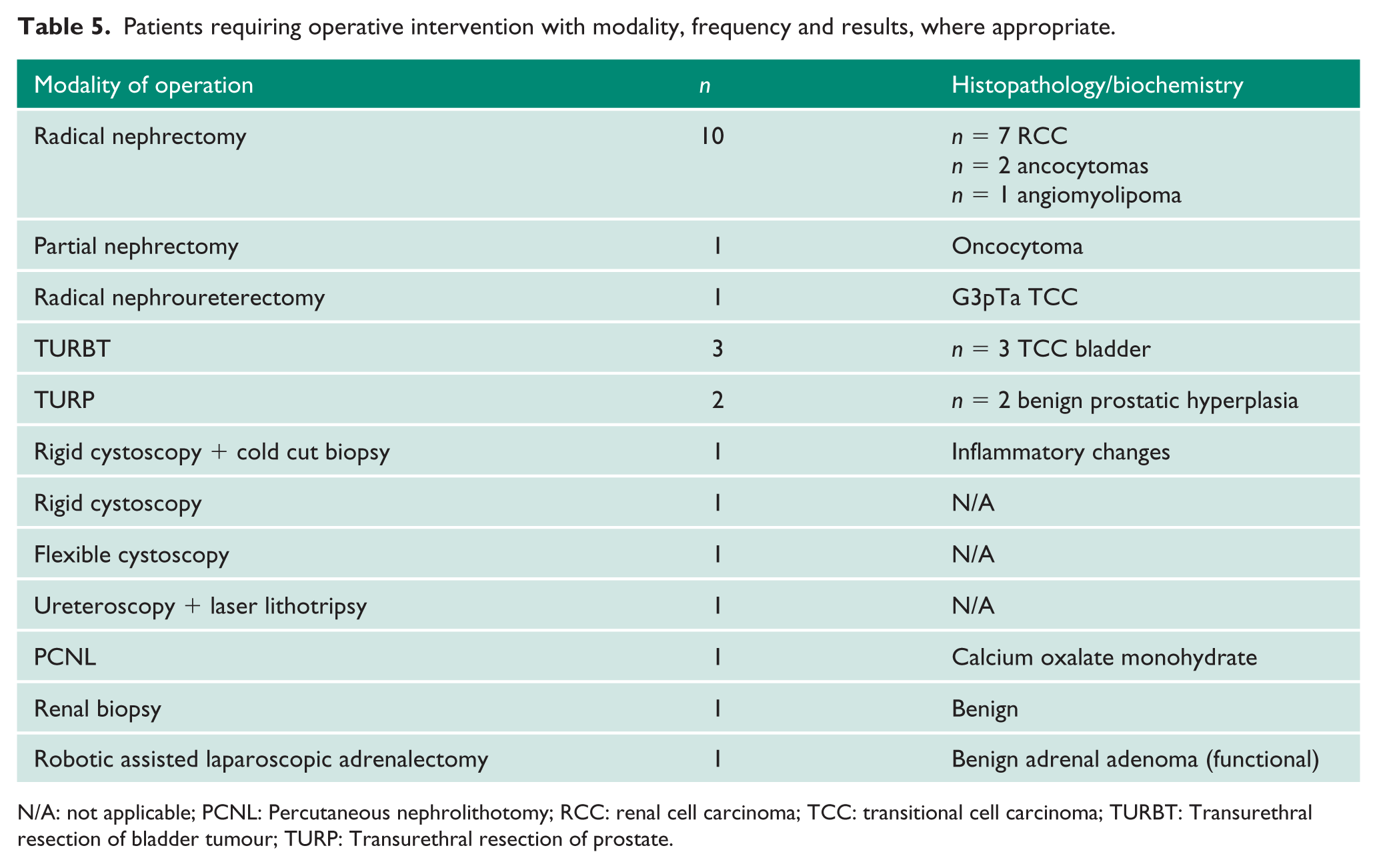
N/A: not applicable; PCNL: Percutaneous nephrolithotomy; RCC: renal cell carcinoma; TCC: transitional cell carcinoma; TURBT: Transurethral resection of bladder tumour; TURP: Transurethral resection of prostate.
Of the n = 10 radical nephrectomies, n = 7 came back as RCCs, n = 2 oncocytomas and n = 1 as an angiomyolipoma. The partial nephrectomy was referred to a tertiary centre for surgical management. Histology demonstrated an oncocytoma. The nephro-ureterectomy was a G3pTa TCC with complete excision and clear margins.
Of the reported bladder masses, n = 3 underwent a TURBT. All the TURBTs had underlying TCCs of varying grades and depths; n = 1 on rigid cystoscopy was thought to be an intravesical prostatic extension but underwent a TURP given the patient’s symptoms. This demonstrated benign hyperplastic changes. Finally, n = 1 had a rigid cystoscopy and cold cut biopsies, which demonstrated inflammatory changes only.
The single urachal mass underwent a flexible cystoscopy, which showed a normal bladder, and was subsequently followed up with an interval CT as mentioned previously. The patient with suspicion of a colovesical fistula radiologically had a rigid cystoscopy, which confirmed the diagnosis.
Both TURPs were undertaken for high pressure chronic retention. Both demonstrated benign histology.
Of the single number interventions, the renal biopsy demonstrated a benign tumour. The ureteroscopy and laser lithotripsy resulted in complete stone clearance. The PCNL resulted in good clearance and stone analysis was reported as calcium oxalate monohydrate.
The patient with a functioning adrenal adenoma underwent a robotic retroperitoneal adrenalectomy at a tertiary centre, which demonstrated a benign adrenal adenoma.
As a percentage, 7.2% of all patients with urological findings (or 1.2% of the entire cohort) underwent operative intervention.
Discussion
At the time of writing, this is the largest single-centre cohort study of its kind. 8 Furthermore, it is also the only study to our knowledge focusing purely on incidental urological findings.
This study highlights how common extracolonic urological diagnosis is following CTC. In total, 17.7% of patients in this predominantly Caucasian population cohort had a urological diagnosis. Of these patients, only 12 (3%) required further imaging to aid diagnosis and discharge. Of the patients whom had extra imaging, only three went on to have surgery. The patient with a suspected malignant adrenal mass on initial CT had an interval scan demonstrating a benign lesion, but was operated on but due to biochemical workup and symptomology. Therefore, one could argue that the imaging did not directly lead to operative intervention.
For those that request CTCs, our study adds to the data on possible unexpected outcomes of completing an investigation, with around 1.3% of the cohort in this study needing urological intervention.
The rates of detection of underlying anatomical variants (horseshoe kidney, cross-fused renal ectopia, extrarenal pelvis and duplex kidney) are in keeping with the rates quoted in the literature, 9 with the exception of duplex kidney and extrarenal pelvis, which demonstrate lower rates.10–12 Rates of extrarenal pelvis have been quoted at approximately 12% in a post mortem series done by Gupta et al., which is in stark contrast to our study rate of 0.15%. 13 It must be noted that these numbers can be highly skewed given that, if these abnormalities had been detected in a prior scan, they would not have been classified as a new incidental finding in our series.
Siddiki et al. 8 conducted a literature review of all CT colonography studies reporting extracolonic findings with a cohort of ⩾ 100 consecutive subjects. Nine studies were included in their review with populations ranging from n = 100–1253. Indications for CTC in each paper differed from screening, surveillance or diagnostics. Interestingly, none of the studies used the C-RADS criteria to stratify the incidental findings and used other means to class severity. ‘Significant’ findings in each study were defined as patients requiring further workup, and/or medical or surgical intervention.
The percentage of incidental findings ranged from 5–8% for those for whom CTC was done for screening purposes and ~16% in the symptomatic population. The percentage of patients requiring medical or surgical intervention for their significant incidental finding ranged from 1.3–2.3% in an asymptomatic population, and 6–19% in a symptomatic population. Our patient population was largely symptomatic rather than screening CTC, which carries a higher incidence of E3 and E4 findings.4,6
It is important to note that we are unable to draw direct comparisons to our data as we have only included incidental urological findings, whereas the comparative studies in the literature review looked at all incidental findings.
Of note the CTC technique employs both non-enhanced and portal venous-phase post contrast sequences, which allows for characterization of most renal lesions by virtue of the presence or absence of enhancement, in addition to the Hounsfield unit (HU) value. 14 Significant enhancement is defined as a change > 20 HU. In cases of equivocal enhancement (10–20 HU), a renal mass will be indeterminate and dedicated triple-phase renal CT (comprising of pre-, cortico-medullary and parenchymal phases) may clarify status.15,16
This has allowed 11 of the 12 renal cancers to be accurately characterized without a need for further investigation. The distinction between a benign renal mass and RCC cannot be reliably made on imaging. The accepted view is that masses < 3 cm with no evidence of nodal or metastatic disease will be termed SRMs. Most will turn out to be RCCs; however, a small but significant proportion are benign. 17 Masses > 3 cm or with aggressive features such as renal sinus/extracapsular extension/venous invasion were classified by the radiologists as probable RCCs. 18
The non-enhanced sequence is valuable for characterizing adrenal adenomas, as a HU value of ⩽ 10 is highly specific. 19
There are some limitations to our study. Recording of incidental findings was by review of the radiological report, rather than radiologist review of examinations. Radiologist reporting of insignificant urological findings such as simple renal cysts will vary widely depending upon reporting style, experience, and local or national guidelines. 20 Thus, the true number of E2 findings may be higher. Patients with multiple incidental urological findings, e.g. hydronephrosis patients, may be linked but were classed as two separate pathologies. This could represent bias and skew the data, but would only be the case for those with the aforementioned pathology. As CTCs are designed to look predominantly at the lower gastrointestinal tract for any significant abnormalities, one could argue that some benign pathological findings may not necessarily be commented upon due to incomplete reporting.
Conclusion
Our study demonstrates an 17.7% rate of incidental urological findings with the majority being non-significant. Of all findings, 13.3% were deemed significant to warrant further investigation or intervention; 7.2% of patients with urological findings required intervention. CTCs can adequately characterize malignant renal masses.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
AA.
Contributorship
Mr Adnan Ahmad: collated and analysed the data set, and was responsible for composition of the manuscript and all supplementary material. Mr Jeremy Nettleton: conceived the idea, helped collate and review data, and provided guidance on composing the manuscript. Mr Matthew Hotston: provided crucial urological guidance on data collection and composition of the manuscript. Dr Alison Bradley: provided a crucial radiological perspective, and was involved in the review and amendment of the manuscript. Dr Giles Maskell: provided a crucial radiological perspective, and was involved in the review and amendment of the manuscript.