
Abstract
We present the case of a 70-year-old female who was incidentally found to have a right angiomyolipoma extending into the renal vein, terminating 1 cm from the inferior vena cava. Due to the invasive nature of the angiomyolipoma in this case, surgical removal via a right laparoscopic nephrectomy was performed. This revealed an un-encapsulated but well-circumscribed fatty mass in the superior pole invading into the inferior vena cava, histologically consistent with a classic angiomyolipoma. Traditionally, patients with tumours extending into the inferior vena cava have been managed with an open surgical approach. Tumours with renal vein thrombus can be managed via an open or laparoscopic approach depending on the extent of vein invasion and local expertise. This is only the third reported case of angiomyolipoma with vascular invasion being treated laparoscopically. Despite the shorter length of the renal vein on the right side, this case demonstrates that a laparoscopic nephrectomy for the management of angiomyolipoma with renal vein thrombus is a feasible approach and would allow the patient faster recovery.
Introduction
A 70-year-old female was incidentally found to have a right renal lesion on an upper abdominal ultrasound. Computed tomography of her abdomen was performed to further characterise this, which showed two fatty lesions, consistent with angiomyolipomas (AML) in the superior pole of the right kidney (Figure 1). The larger lesion extended into the renal vein for 4 cm, terminating 1 cm before the inferior vena cava (IVC). Multiple treatment options were discussed in a multidisciplinary meeting. A laparoscopic nephrectomy was recommended due to the potential risk of fat embolism with embolisation of the AML in this case. Prophylactic IVC filter placement prior to embolisation was not considered as the patient was fit for surgery and there is uncertainty regarding ideal timing of filter removal post embolisation. Nephron-sparing surgery was considered but thought to be difficult and require an open procedure due to the location of the tumour and the degree of renal vein involvement. The patient proceeded with laparoscopic nephrectomy and tumour thrombus excision, recovered well and was discharged day three post-operatively.
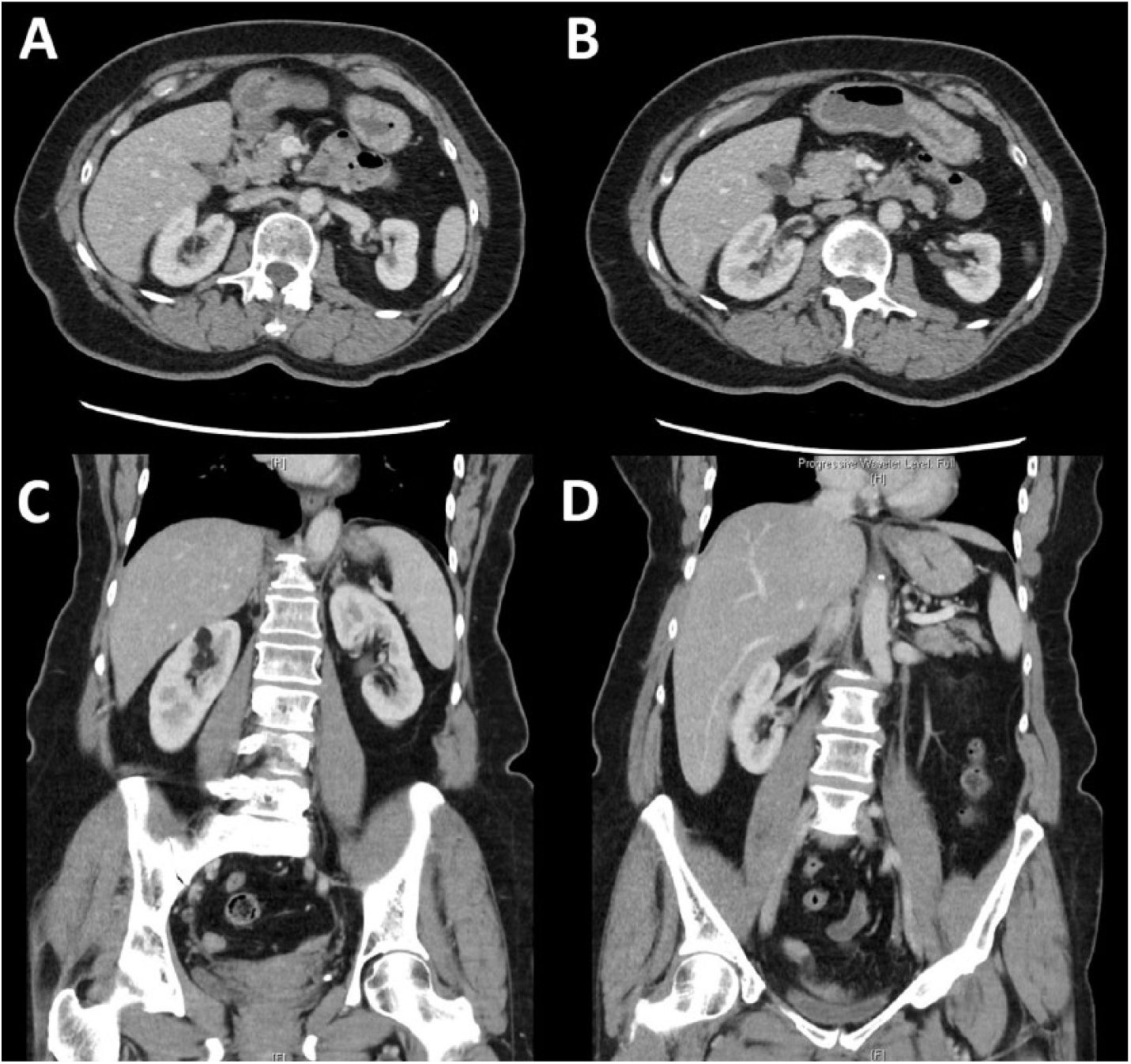
Computed tomography scans showing the right renal angiomyolipoma and the associated renal vein thrombus. The sizes of these lesions were 1.3 cm and 5 mm, with the larger lesion extending into the renal vein for 4 cm, terminating 1 cm before the inferior vena cava (IVC).
Histopathological analysis of the specimen confirmed two, separate, well-circumscribed but un-encapsulated orange-yellow fatty masses within the superior pole, measuring 48 mm and 8 mm. The largest of these lesions extended into the main renal vein with intraluminal tumour identified (Figure 2). On microscopic examination the findings indicated classic AMLs (Figures 2 and 3).
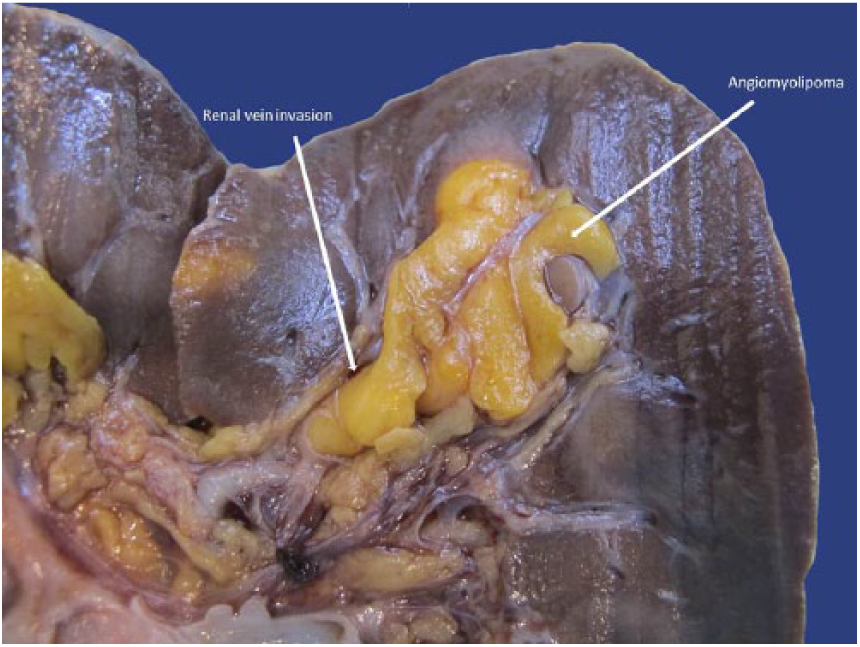
Macroscopic pathological appearance of the right angiomyolipoma invading into the renal vein.
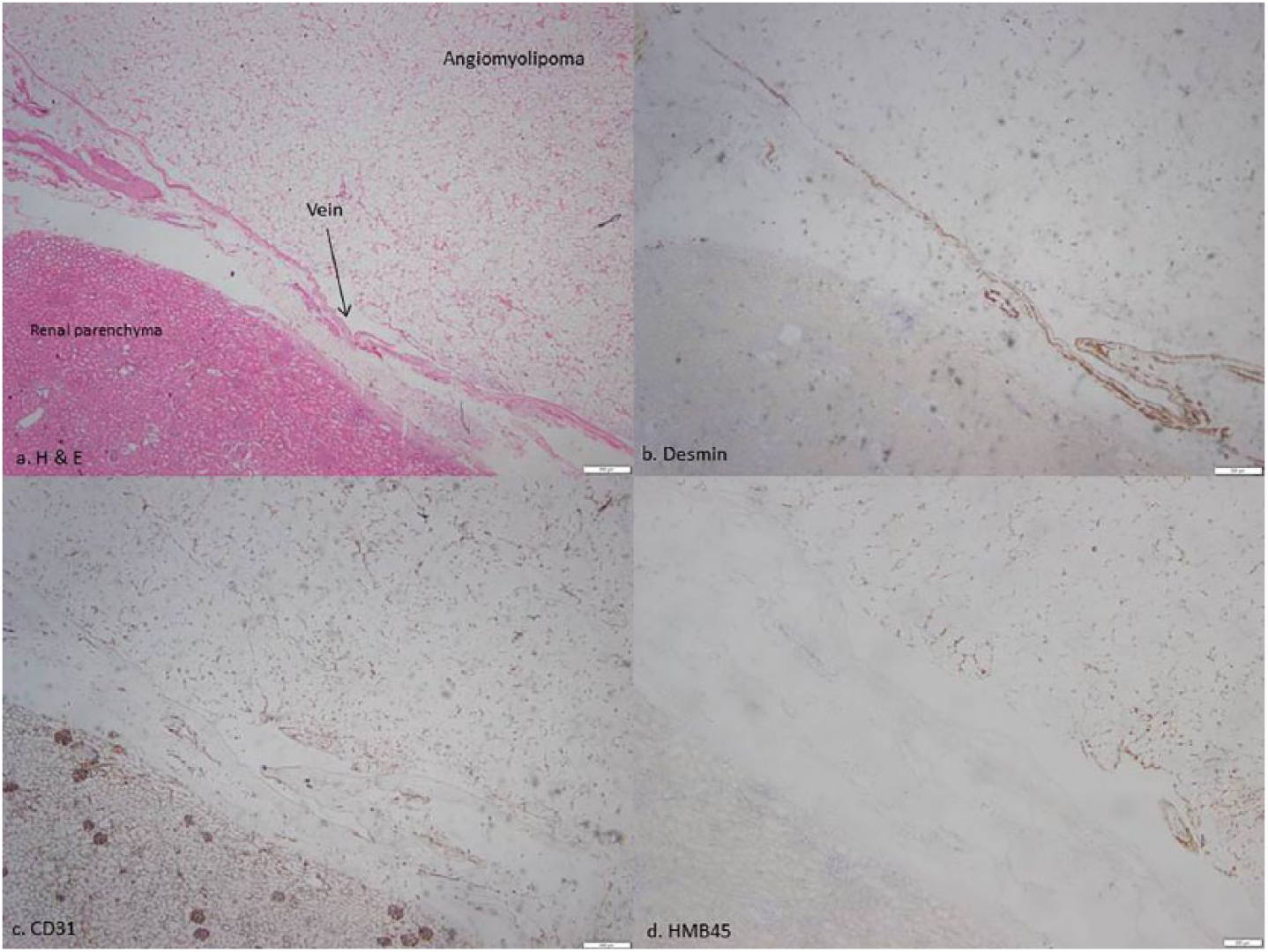
Microscopic images of angiomyolipoma within the renal vein (3(a), hematoxylin and eosin (H&E)), which is highlighted by immunohistochemical stains for desmin (3(b), demonstrating smooth muscle within the vein wall) and CD31 (3(c), demonstrating the venous endothelium). 3(d) An immunohistochemical stain for HMB-45 showing positive staining of scattered tumour cells.
Discussion
Renal AML is an uncommon condition with a reported overall incidence of 0.13%. 1 Histologically, AML are classified as classic variant or epithelioid. 1 Classic AMLs are considered benign. As demonstrated in this case, classic AMLs can rarely be locally invasive into the renal vein or IVC. 2 Conversely, epithelioid AMLs have the potential to undergo malignant changes and to behave aggressively with local recurrence or distant metastasis. 2
There have been 62 cases of reported renal AML with intravascular invasion. 3 Even with classic AMLs, venous invasion is an indication for partial/total nephrectomy and thrombectomy due to the risk of thromboembolic complications. 2 Patients with tumours extending into the IVC have been traditionally managed with an open surgical approach. 4 In cases where the AML only invades the renal vein, laparoscopic nephrectomy remains a favourable alternative option to open surgery with a faster recovery time. To our knowledge, there have only been two prior reported cases of laparoscopic nephrectomy for management of AML with vascular invasion.4, 5 In our case, the operation was performed via a transperitoneal laparoscopic approach. The renal vein tumour thrombus was milked back towards the kidney with laparoscopic DeBakey forceps to allow sufficient length of normal renal vein for placement of Hem-o-lok® clips (Teleflex, North Carolina, USA). Despite the shorter length of the renal vein on the right side, this case demonstrates that a laparoscopic nephrectomy for the management of AML with renal vein thrombus is a feasible approach.
In summary, invasive AML associated with tumour thrombus extending towards the renal vein is a rare condition. 2 The presence of a tumour thrombus has significant implications with potential thromboembolic events. Clinicians should be wary of the potential risk of fat embolization associated with conventional minimally invasive management of these AML with angioembolisation. These patients are best managed with a nephrectomy and tumour thrombectomy. In patients where the tumour thrombus stops short of the IVC, a laparoscopic approach to the nephrectomy can be feasibly performed with a good outcome and faster recovery for the patient.
Footnotes
Acknowledgements
Nil.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Alfred Health does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article
Guarantor
EG will accept full responsibility for the content and authorship of the paper.
Contributorship
EG wrote the manuscript and obtained consent from the patient, HHY conceptualized and edited the manuscript and provided Figure 1, GT and RC processed the pathological specimens and provided Figures 2 and ![]() with descriptions, DK contributed to the conceptualization of the article, data collection and editing.
with descriptions, DK contributed to the conceptualization of the article, data collection and editing.