Each presenter will be required to present for 7 minutes in total (4 minutes presentations and 3 minutes for questions and answers). The order of presentations will be as follows:
1. Sotonye Tolofari
2. Richard Jones
3. William Fowler
4. Mahmoud Marei
5. Atif Khan
6. Susannah La-Touche
7. Kelvin Adasonla
8. Branimir Penev
9. Niyukta Thakare
10. Aman Harbias
11. James Jenkins
1. Patient-reported outcomes (PROMs) in stone surgery: a multicentre study of patient experience of flexible ureteroscopy versus extracorporeal shockwave lithotripsy
Sotonye Tolofari1, Benjamin Starmer2, James Broome4, Huw Garrod4, Ketan Agarwal5, Kee Wong5, Morkos Iskander1, Saqib Javed2, Pat Kelly1, Henry Lazarowicz1and Robert Calvert1
1Royal Liverpool and Broadgreen NHS Trust
2Mid Cheshire NHS Hospitals Trust
3St Helen’s and Knowsley NHS Trust
4Wrexham Maelor NHS Trust
5Arrowe Park NHS Hospital
Abstract
Introduction: Patient-reported outcome measures (PROMs) assess the quality of care delivered from a patient’s perspective. There is a paucity of evidence reporting PROMs in the treatment of urolithiasis. In this study, we aimed to assess the impact of urological stone procedures on patients’ morbidity.
Methods: Data were prospectively collected over 12 months using the Cambridge renal stone PROMs questionnaire. Patients undergoing flexible ureterorenoscopy (fURS) or a first session of extracorporeal shockwave lithotripsy (ESWL) for renal stones were asked to complete a preoperative questionnaire. This questionnaire was repeated at one, 6 and 12 weeks postoperatively.
Results: Across five NHS trusts, a total of 106 patients was collected over the 12-month period. Sixty patients underwent ESWL with 46 patients having fURS. The mean age was 51 years. Median stone size in the fURS cohort was 10.43 mm; 86% of fURS patients were stented. Complete stone clearance was 77%. Of the ESWL cohort, median stone size was 6.53 mm. Only 3% of patients had a ureteric stent in situ; 74% of patients required more than two sessions.There were no significant differences in preoperative PROMs scores for both treatment groups. At one week, the fURS PROMs were significantly higher than ESWL (P<0.01). However, at both 6 and 12 weeks ESWL had significantly higher PROMs scores (P<0.05).
Discussion: The fURS cohort had a significantly higher PROMs score at week one, suggesting a higher initial morbidity. However, PROMs scores at 6 and 12 weeks postoperatively were significantly higher with ESWL. This may be be due to factors including ureteric stent symptoms in the immediate postoperative period. Repeated sessions with ESWL perhaps explain the higher PROMs score at 6 and 12 weeks, which may lead to continued symptoms or anxiety associated with repeated treatment.
2. National snapshot audit on the surgical management of LUTS/BPE: what has changed over the past two decades?
Hrishikesh Joshi1, R Jones2, H Lazaowicz2, G Sali1, M Kujawa3, R David4, A Pandit4, K Wilson5, C Bates5, C Wilson6, I Shergill6, C Gan7, B Mukhtar8, T Appanna8, R Veeratterapillay9, C Harding9, J Cobley10, M Crockett10, M Madison11, C Dawson11, R Simpson12, B Zelhof12, B Starmer13, R Mukherjee13, S Dhanasekaran14, S Khashaba14, J Jelski15, H Hashim15, E Fishleigh16, J McCabe16, N Pavan17, G Shaw17, T Gunendran18, K Chow18 and C Betts19
1University Hospital of Wales
2Royal Liverpool and Broadgreen University Hospitals NHS Trust
3Stepping Hill Hospital, Stockport NHS Foundation Trust
4Abertawe Bro Morgannwg University Health Board
5Aneurin Bevan University Health Board
6Betsi Cadwalader University Health Board
7Charing Cross Hospital, Imperial College Healthcare NHS Trust
8 Cwm Taf University Health Board
9Freeman Hospital, the Newcastle Upon Tyne Hospitals NHS Foundation Trust
10Gloucestershire Hospitals NHS Foundation Trust
11Good Hope Hospital, Heartlands Hospital and Solihull Hospital, University Hospitals Birmingham NHS Foundation Trust
12Lancashire Teaching Hospitals NHS Foundation Trust
13Leighton Hospital, Mid Cheshire Hospitals NHS Foundation Trust
14Sandwell and West Birmingham Hospitals NHS Trust
15Southmead Hospital, North Bristol NHS Trust
16St Helens and Knowsley Teaching Hospitals NHS Trust
17University College London Hospitals NHS Foundation Trust
18Wythenshawe Hospital, Manchester University NHS Foundation Trust
19Salford Royal NHS Foundation Trust
Abstract
Introduction: Surgical treatment for lower urinary tract symptoms (LUTS)/benign prostatic hyperplasia (BHP) has experienced changes over the years, with the addition of new treatments. There are limited data on the current national practices when compared with historical data.
Method: A national audit (audit of surgical management of benign prostatic enlargement; BPE) was conducted for patients undergoing surgery for LUTS/BPE over an 8 week period (March–April 2018). A two-part proforma, examining processes (eight items) and patient outcome (25 items), was designed and completed at participating sites. The results were analysed and compared with those from the larger national often (59%) or always (18%); 24% of centres reported that training needs impacted the type of treatment.
Conclusion: Monopolar transurethral resection of the prostate still forms the commonest surgical intervention with other technologies being available. There are variations in patient selection, pathways and treatments. Overall complication rates and hospital stays have significantly improved when compared with the results from the national prostate audit. There might be the need for longer evaluation of outcomes with the newer technologies.
3. Predictors of failed trial without catheter following holmium laser enucleation of the prostate (HOLEP)
William Fowler, Kenneth MacKenzie and Rajan Veeratterapillay
Freeman Hospital
Abstract
Background: Holmium laser enucleation of the prostate (HOLEP) is effective at relieving bladder outlet obstruction with benefits of reduced blood loss, catheter time and length of stay compared to traditional transurethral prostate resection. Some patients are, however, unable to void following catheter removal postoperatively. We aimed to identify predictive factors for failed trial without catheter (TWOC).
Methods: Patients undergoing HOLEP at our institution from January 2016 to December 2017 were identified. A retrospective review was conducted to capture demographic data, indication for surgery and postoperative outcomes. Preoperative clinical data for non-retention patients included international prostate symptom score, peak flow rate (Qmax) and the use of pharmacotherapy, and for retention patients included residual volume and catheter time. Patients had their first TWOC within 24–48 hours. Failure to void was recorded and multivariate analysis undertaken to identify predictive factors.
Results: A total of 219 patients was included; median age was 72 years (range 42–92). Indication for surgery was acute retention (n=77, 35%), chronic retention (n=27, 15%) and refractory lower urinary tract symptoms (n=115, 50%). Twenty patients (9%) failed to void and had a second TWOC at a median time of 10 days. Following the second TWOC, 16 were catheter free and four required intermittent self-catheterisation, therefore 98.2% were catheter free. Predictors of failed initial TWOC for patients in retention were residual volume greater than 2 litres.
Conclusions: HOLEP results in over 98% of patients voiding spontaneously. A delayed TWOC may be considered for patients with residual volume greater than 2 litres.
4. A multidisciplinary approach for paediatric and adolescent urolithiasis highlighting the twin-surgeon model: initial experience and preliminary outcomes
Mahmoud M Marei1,2, Mohan Shenoy3, Supul Hennayake2and Benjamin R Grey1
1Department of Urology, Manchester Royal Infirmary
2Department of Paediatric Urology, the Royal Manchester Children’s Hospital
3Department of Paediatric Nephrology, the Royal Manchester Children’s Hospital
Abstract
Introduction: Urolithiasis in children and adolescents is characterised by a rising incidence, tendency for recurrence and a changing epidemiology. Metabolic and genetic predisposing factors are becoming less commonly identified and the pattern is shifting to become more akin to adult stones. We present the multidisciplinary experience of our tertiary centre in managing paediatric and adolescent urolithiasis, for the initial 3 years (2015–2018).
Methods: A multidisciplinary approach with expertise from paediatric nephrology, paediatric urology and adult urology was adopted. A combined multidisciplinary team clinic was conducted monthly. A twin-surgeon model involving a paediatric and an adult urologist (senior authors) performed the scheduled stone surgeries in combined theatre lists on the paediatric site.
Results: The multidisciplinary team clinic offered 125 appointments for 57 patients until November 2018 through this channel. Fifty-two paediatric and adolescent procedures were performed encompassing nine cases of percutaneous nephrolithotomy (PCNL) (17%) including five prone and four supine with one endoscopic combined intrarenal surgery; 17 cases of uretorenoscopy (URS)/retrograde intrarenal surgery (RIRS) (33%) including six flexible URS; and 26 cases of shockwave lithotripsy (50%). The mean age was 8.3 years (median 7.8 years, range one year 5 months to 16 years 8 months). Complicating factors were noted in 14 cases that were operated on; significant medical comorbidities in two/14 (14.2%), urosurgical or anatomical abnormalities in four/14 (28.6%), e.g. vesicoureteric junction obstruction or urinary diversion and significant metabolic abnormalities in nine/14 (64.3%). The stone-free rate was 77.8% for PCNL and 66.6% for URS/RIRS with 100% clearance when the ureter was successfully accessed. The re-operation rate for residual calculi was 16.7%.
Conclusion: Urolithiasis is an increasingly challenging problem for the paediatric and adolescent population requiring dedicated services. The twin-surgeon model including paediatric and adult endourological expertise is ideal due to the steep learning curve. Support from endourology-competent theatre staff and back-up from paediatric interventional radiology is crucial during PCNL. Miniaturisation of equipment allowed the shift from shockwave lithotripsy towards URS/RIRS and PCNL.
5. Is there a correlation between urolithiasis in horseshoe kidneys and isthmus thickness or renal angulation?
Nicola Lee1, Atif Khan1, Ese Adiotomre1, Michael Kimuli2, Simon Burbidge1 and Chandra Biyani2
1Department of Radiology, St James’s University Hospital
2Department of Urology, St James’s University Hospital
Abstract
Introduction: Stone disease is a common complication of horseshoe kidneys, thought to be brought about by an impedance to normal urinary flow which can also promote infection and obstruction. There are currently limited studies which examine the relationship between horseshoe kidney anatomy and stone formation. We aimed to determine if there is such a relationship by measuring the isthmus size and renal angulation in both stone and non-stone-forming horseshoe kidneys using computed tomography.
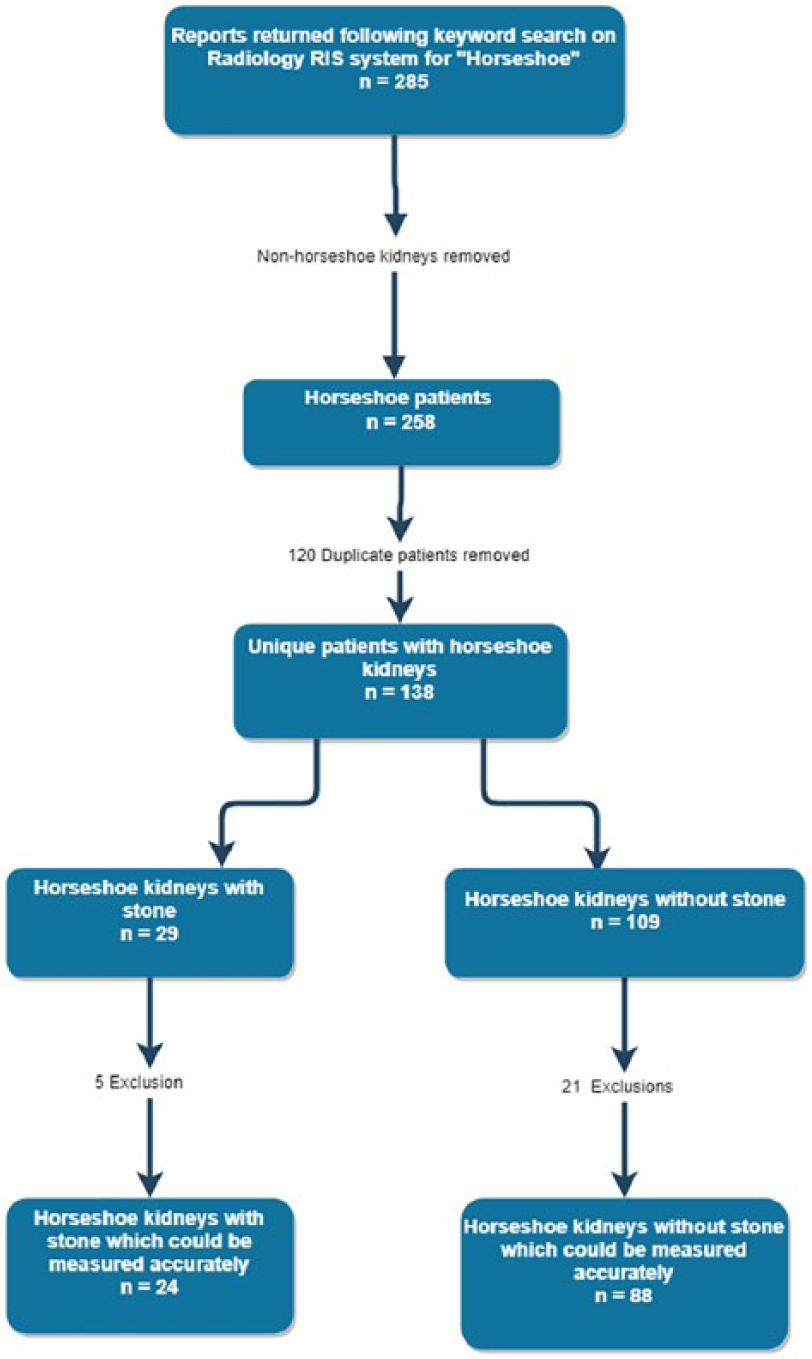
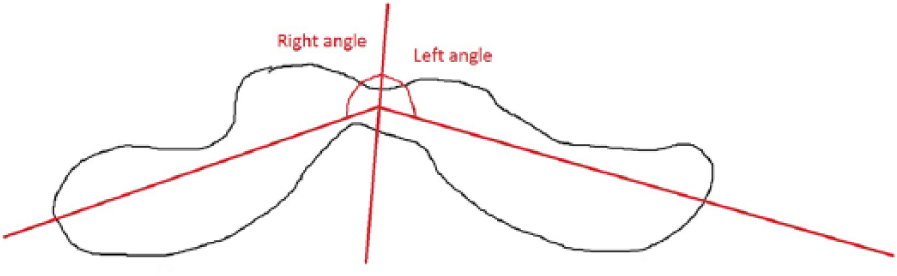
Methods: This was a retrospective study performed at a single tertiary centre. Using the radiological information system, all computed tomography reports between a 5-year period starting from 1 January 2010 to 31 December 2015 were searched for the keyword ‘horseshoe’ on the radiological information system. This produced a list of 285 reports. Each report and image packet of these 285 studies were reviewed to confirm the presence of a horseshoe kidney, and duplicate patients from multiple examinations were highlighted. A total of 138 unique horseshoe kidney patients was obtained and the studies were assessed for the presence or absence of stones (Figure 1). This left a total of 112 horseshoe kidneys; 88 of which contained no stone and 24 with stone. Angle measurements and isthmus size were measured in these kidneys. As axial images are obtained as standard in all cases, these measurements were all obtained on the axial plane (Figure 2). All parameters were measured and recorded manually by one person so as to reduce interobserver variability.
Study inclusion and exclusion flow diagram.
Renal angle measurements as obtained on axial plane.
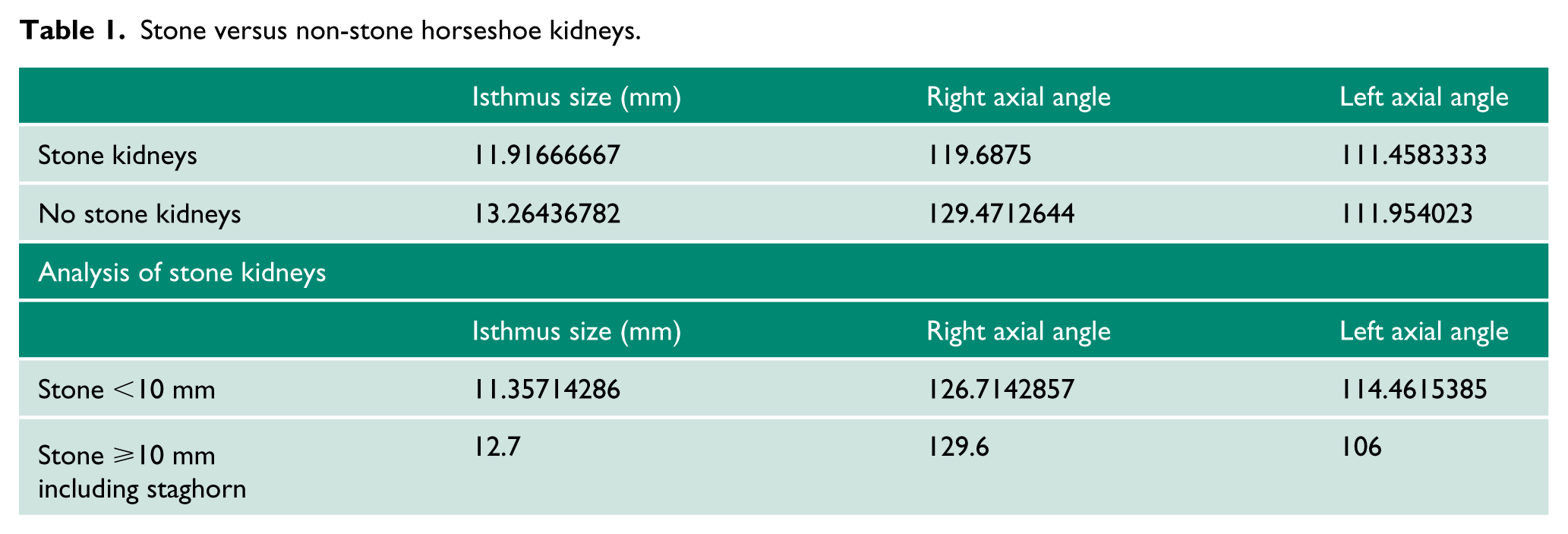
Results: Isthmus size varied widely, measuring from 2 to 39 mm. The right renal angle ranged from 51 to 158 degrees, left 38 to 152 degrees and isthmus size was 11.91 mm (stone kidneys) versus 13.26 mm (no stones) (Table 1).
Stone versus non-stone horseshoe kidneys.
Isthmus size (mm)
Right axial angle
Left axial angle
Stone kidneys
11.91666667
119.6875
111.4583333
No stone kidneys
13.26436782
129.4712644
111.954023
Analysis of stone kidneys
Isthmus size (mm)
Right axial angle
Left axial angle
Stone <10 mm
11.35714286
126.7142857
114.4615385
Stone ⩾10 mm including staghorn
12.7
129.6
106
Conclusion: The isthmus size and renal angle measurements were not found to be significant determinants for stone disease in our patient population.
6. The safety and efficacy of upper pole supine PCNL
Susannah La-Touche and Asad Abedin
Russells Hall Hospital
Abstract
Introduction: Upper pole renal access carries a risk of pleural puncture, liver injury on the right side and splenic injury on the left. Supine percutaneous nephrolithotomy (PCNL) confers advantages of draping once, better airway access and the capacity for combining PCNL with ureteroscopy. Difficulty in upper pole puncture is cited as a possible disadvantage in supine PCNL. We present our experience of the safety and efficacy of upper pole punctures in supine PCNL.
Methods: We performed a retrospective study on all patients requiring upper pole puncture between 2012 and 2018. All cases identified were performed on patients in a supine position in a single institution by an experienced urologist. Standard antibiotic prophylaxis was given at induction. All renal punctures were guided by ultrasound and fluoroscopy. Postoperatively, the stone-free rate was determined principally by computed tomography (CT) and was defined as the absence of any calculi in the urinary tract.
Results: We identified 136 PCNLs, of which 26 upper pole, supine procedures were performed, including punctures for four staghorn calculi and one partial staghorn. The mean age of patients was 59.4 years (range 25–78) and the female to male ratio was 1:1. Stone composition included three (11.5%) triple phosphate and one (3.8%) cystine stone. Follow-up imaging included 19 CTs, three ultrasound scans (USS), three X-rays and one USS and X-ray. Residual calculi occurred in eight (30.8%) patients and complications arose in three (11.5%) patients: One pseudoaneurysm required embolisation and blood transfusion (3.8% transfusion rate). Two patients developed septicaemia. There were no visceral, thoracic complications and no cases of failed access.
Conclusions: Our study demonstrated that upper pole puncture in supine PCNL, under ultrasound and fluoroscopic guidance can be performed safely without increased incidence of thoracic and visceral injury.
7. Are NICE and GIRFT recommendations for the management of acute ureteric colic achievable? A snapshot comparison of a tertiary referral versus district general hospital
Kelvin Adasonla1, Hamid Abboudi1, Narin Suleyman2, Kelvin Adasonla1, Georgios Kazantzis1, Giuseppe Celentano1, Vimoshan Arumuham1,2, Siân Allen1 and Daron Smith1
1Endourology Department, Institute of Urology, University College London Hospitals
2Department of Urology, Watford General Hospital, West Hertfordshire NHS Trust
Abstract
Introduction: We aimed to determine how feasible it is to achieve the National Institute for Health and Care Excellence (NICE) and get it right first time (GIRFT) recommendations for ureteric colic management in 48 hours.
Methods: Prospective data for all acute colic admissions between 1 November 2018 and 31 March 2019 in a tertiary referral unit and a district general hospital (DGH) was evaluated against NICE 2019 and GIRFT recommendations specifically regarding patients with uncontrollable pain or stones deemed unlikely to pass (i.e. patients recommended for treatment within 48 hours).
Results: Overall, 37 of the 106 patients (35%) with acute colic at the tertiary centre were potentially eligible for 48-hour treatment; 19% (7/37) of these were septic and therefore drained (six stented, one nephrostomy) leaving 81% (30/37) suitable for active treatment of whom 53% (16/30) received definitive treatment within 48 hours (12 uretorenoscopy, four extracorporeal shockwave lithotripsy); 81% of these (13/16) were stone free within 48 hours. Three ureteroscopy cases failed due to tight ureters. Five patients underwent primary ureteroscopy the following Monday, such that 70% (21/30) were treated definitively within 72 hours. Temporising stents were inserted in eight patients because of a lack of OR time (three), Friday admission and no ureteroscopy facility over the weekend (four) and failed extracorporeal shockwave lithotripsy (one). The lack of primary treatment options over the weekend accounted for 71% of patients who could not be treated within 48 hours. By contrast 33 DGH patients were eligible for 48-hour management; 94% received an emergency stent.
Conclusion: Treatment within 48 hours is ambitious but provides a good outcome. The weekend effect is problematic, but 72-hour management is more realistic and seems acceptable. Dedicated theatre time and expertise (including over weekends) will be needed to meet the NICE and GIRFT recommendations. DGHs will need either substantial investment or readjustment of services to achieve these targets.
8. Review of the indications for ureteric stents use post ureterorenoscopy
Branimir Penev, Meghana Kulkani and Mark Cynk
Maidstone and Tunbridge Wells NHS Trust
Abstract
Introduction and objectives: The indications for ureteric stenting post ureterorenoscopy (URS) remain controversial. Stent symptoms are a cause of significant morbidity. We evaluated the indications for stent use in large series.
Materials and Methods: A prospective database of 1418 patients undergoing therapeutic and diagnostic URS were retrospectively analysed. Rates of stent insertion were determined stratified by stone size, number, location and density; and by indication for ureteroscopy. Complications were determined by review of patient hospital records.
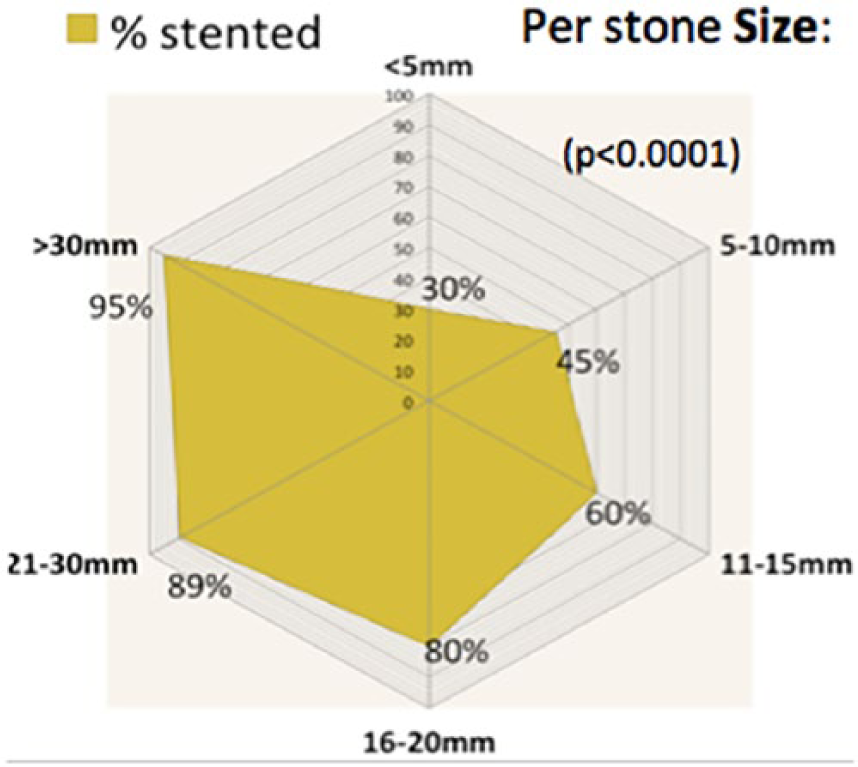
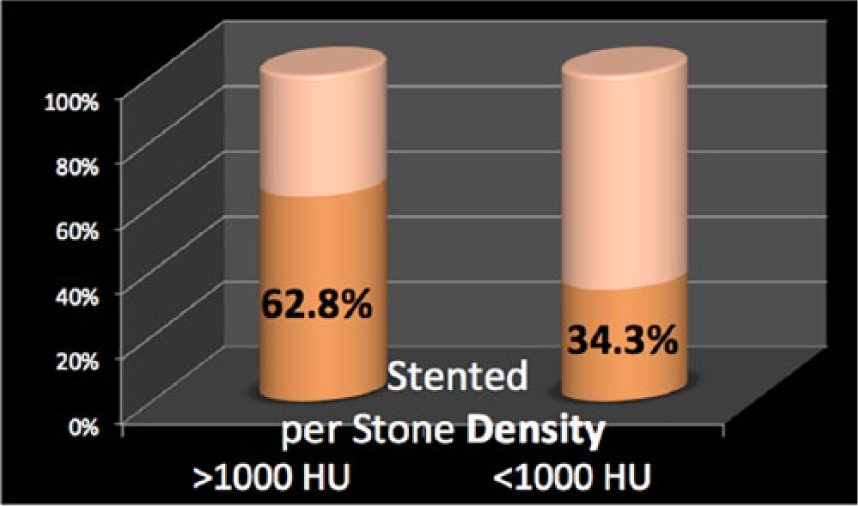
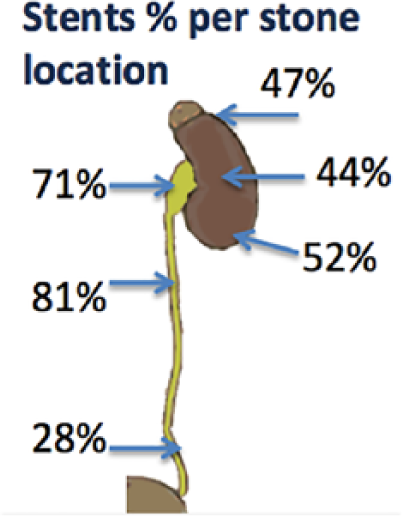
Results: The majority of URS (1198, 84%) were for treatment of calculi. In these, overall half (49.6%) of the patients were stented postoperatively. Multiple stones were present in 45.7% of the cases and stents were used in 61% of these. When stratified by stone diameter, the stenting rate was 30% for less than 5 mm stones; 45% for 5–10 mm; 60% for 10–15 mm; 80% for 16–20 mm; 89.7% for 21–30 mm; and 95% for stones over 30 mm (P<0.0001, chi-squared test). Stents were used in 47%, 44%, 52% and 50%, for stones in upper, mid and lower pole, and calyceal diverticula, respectively, with no difference between these locations (P=0.7856). However, for stones in the renal pelvis, where there was a greater proportion (45.4%) of larger (>15 mm) stones, 71% required stenting. The stenting rate was 81% for proximal and 28% for distal ureteric stones, respectively. Stones with density greater than 1000 Hounsfield units (HU) on preoperative computed tomography scan were stented twice as frequently (62.8% vs. 34.3%) as stones of less than 1000 HU. Following diagnostic URS, or for management of upper urothelial tumours, stents were used in 13.4% and 18.6% of cases, respectively.
Conclusions: Our experience supports the judicious use of ureteral stents. The highest stenting rates were for larger, harder, renal pelvis, or proximal ureteral stones. Stents can be avoided in stones less than 1 cm, in URS for diagnosis, ablation of small upper urinary tract calculi and stones with density less than 1000 HU.
9. Metabolic evaluation of adults with urolithiasis: guidelines versus practice
Introduction: Patients with recurrent stone formation contribute to frequent hospital attendances and are at a higher risk of significant morbidity. Recently published National Institute for Health and Care Excellence (NICE) guidelines do not stipulate the exact extent to which patients should have metabolic investigations. European Association of Urology (EAU) guidelines define clear criteria and pathways for metabolic evaluation. We aimed to assess our current practice with respect to metabolic work-up of stone patients and its impact on stone recurrence.
Patients and Methods: All adult patients who attended stone clinic between August 2017 and November 2017 were retrospectively evaluated. High-risk categories were identified as per EAU guidelines. Data were obtained to determine whether patients had basic evaluation and if extended evaluation was undertaken in high-risk patients. Recurrent stone episodes including new stone formation were noted.
Results: A total of 399 patients was included; age range 19–93 years; men n=247 (62%) and women n=152 (38%). Serum calcium, serum urate and stone analysis were undertaken for 238 (60%), 207 (52%) and 105 (26%) patients, respectively. Four per cent (10/238) had abnormal calcium, 17% (35/207) had abnormal urate and three (6%) of these had a further stone episode; 64/399 (16%) were identified as high risk for stone formation. Only 35 (55%) of high-risk patients were referred for further metabolic assessment including 24 hour urine. Recurrent stone episodes occurred in 13 (20%) high-risk patients, seven (54%) of whom had an extended work-up and six (46%) of those were not fully investigated.
Conclusions: Compliance with metabolic evaluation can be improved. Recurrent stone episodes occurred in a small proportion with abnormal calcium and urate. Performing extended work-up did not significantly impact stone recurrence in the short term. It will be interesting to observe the frequency of recurrent stones after a longer follow-up period and the impact of extended work-up on stone recurrence in high-risk patients in the long term.
10. The importance of stone retrieval in the modern management of urolithiasis: the UroPro stone catcher versus traditional sieving
Aman Harbias, Manoj Ravindraanandan, Adam Jones and Wasim Mahmalji
Hereford County Hospital
Abstract
Introduction: World urolithiasis is increasing, with a 70% increase in hospital admissions between 2000 and 2015. Stone analysis can allow for the identification of metabolic conditions, and stone retrieval may decrease the need for follow-up imaging, reducing costs and patient radiation.
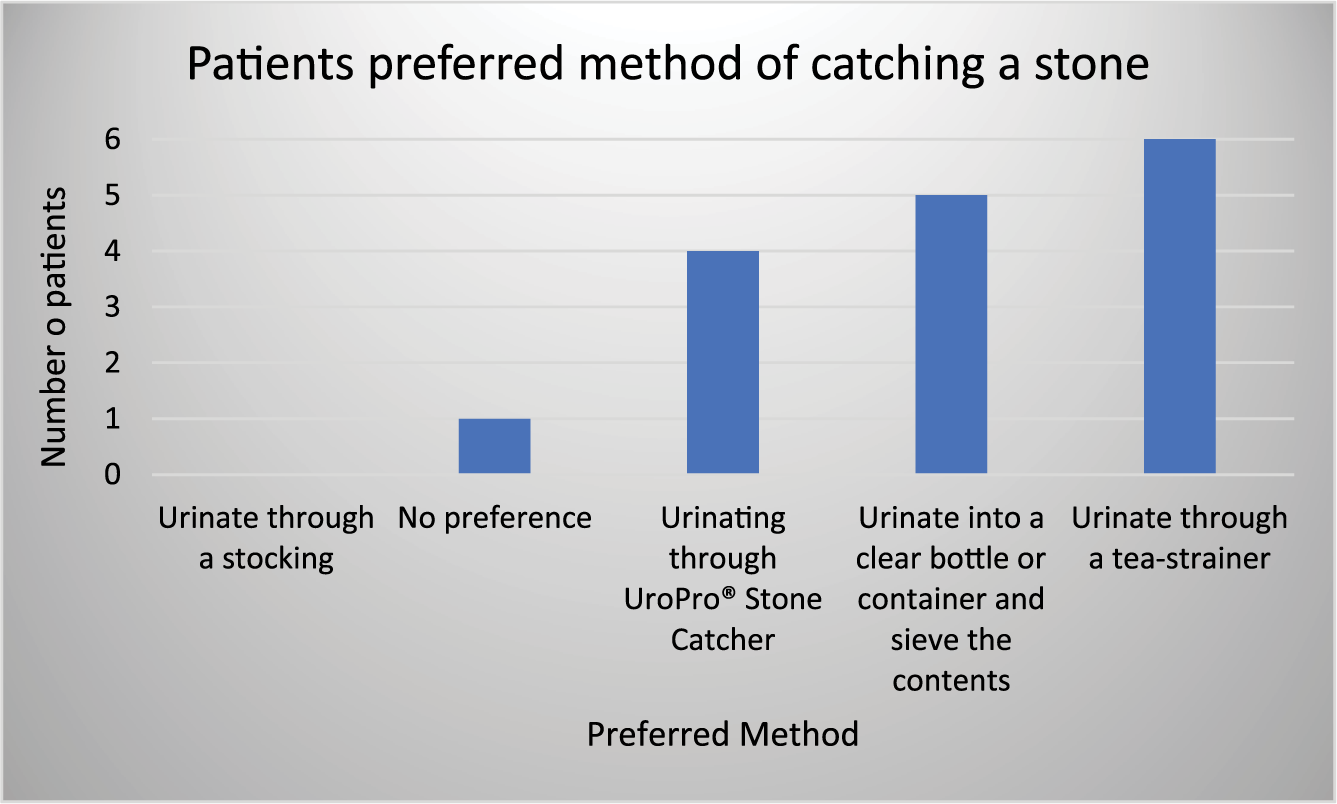
Methods: Between December 2018 and May 2019 patients receiving shockwave lithotripsy (SWL) or being conservatively managed for a ureteric stone were discharged with a Paramount Medical Solutions UroPro stone catcher (Figure 1). Both groups of patients were asked to complete a patient survey regarding the product.
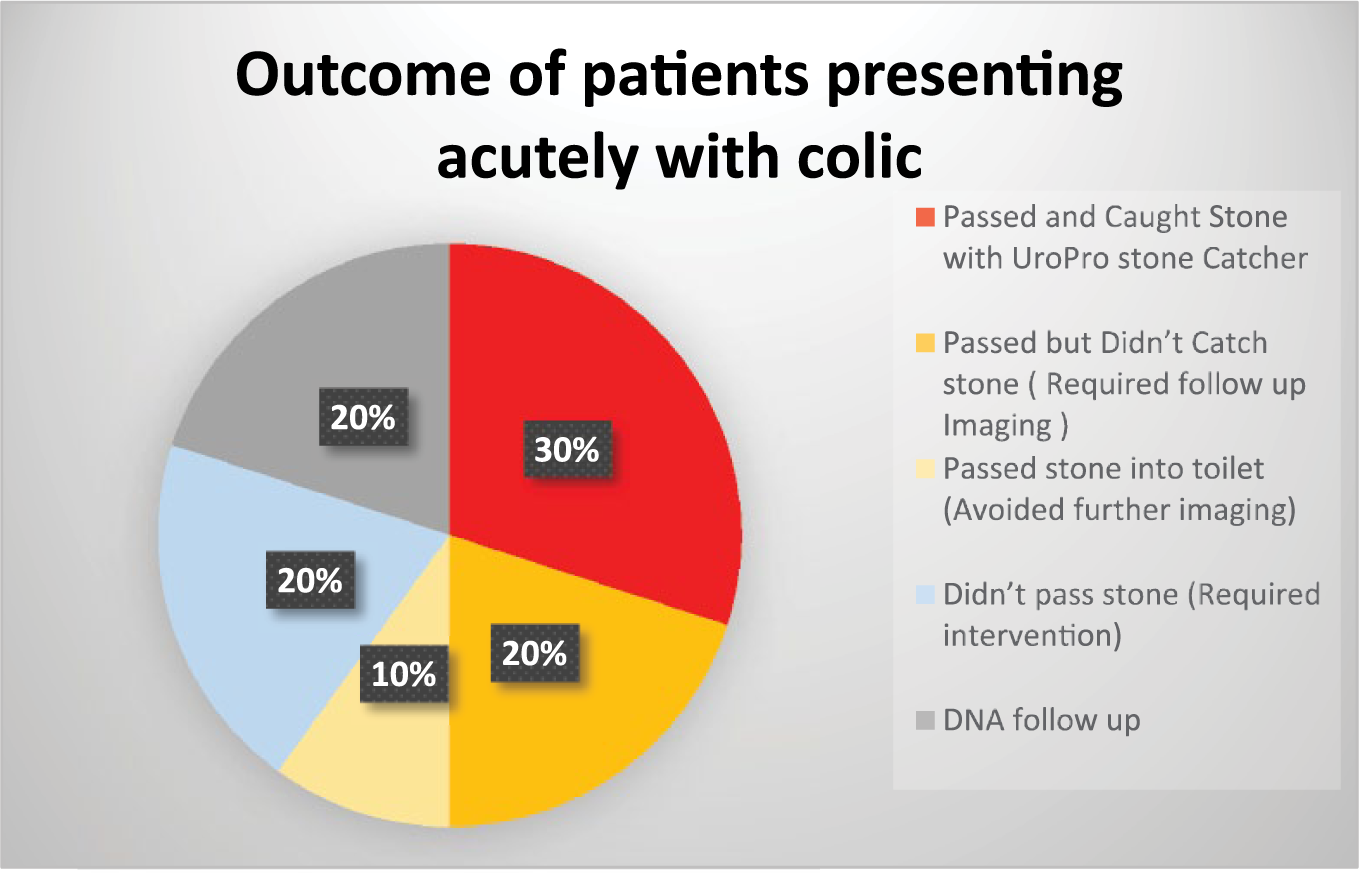
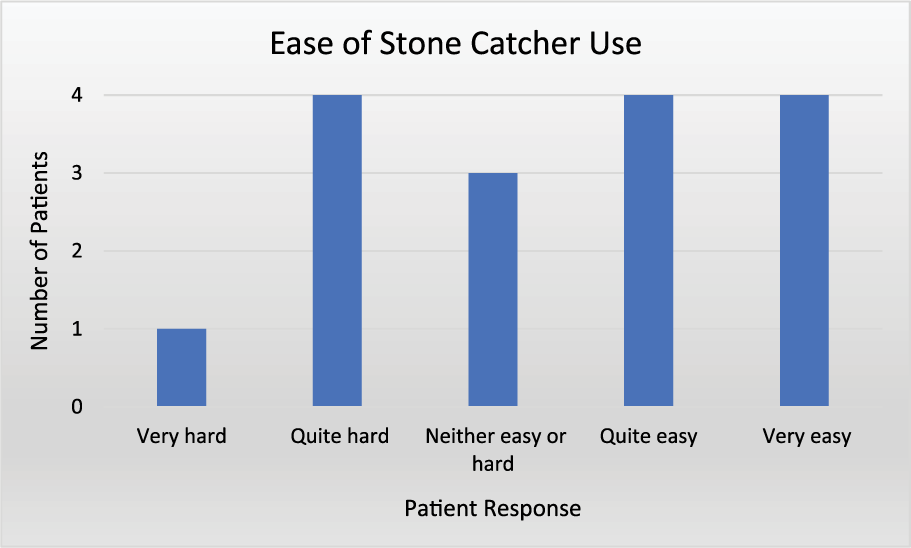
Results: Nineteen patients were recruited. Nine from SWL and 10 from acute admissions. Sixteen responses have been received: eight each from each group. Three patients were uncontactable. Figure 2 shows the outcome of the acute patients, of the eight undergoing extracorporeal SWL only one patient had caught fragments (Figure 3). Figure 4 outlines patient responses to ‘how easy did you find the stone catcher to use’ and Figure 5 highlights how only four of the 16 patients preferred using the UroPro Stone catcher over other methods. Common complaints about the stone catcher were that it was unhygienic due to the short handle and overflow of urine due to the mesh not being porous enough.
Discussion: The UroPro stone catcher did increase the number of stones caught and sent for analysis. However, many patients preferred the older ‘sieving’ methods. Stone catchers retail at £5.50, therefore ‘sieving’ remains more cost effective. Stone retrieval in any form remains advantageous, as confirming stone passage saves the patient 0.5 to 2.8 mSv of radiation from follow-up imaging, the NHS c. £100 per unnecessary follow-up computed tomography scan and aids metabolic analysis. Over time both factors may be substantial. Therefore, emphasising the benefits and importance to patients to sieve their urine regardless of the technique is paramount in the modern management of urolithiasis.
11. Comparison of transperitoneal versus retroperitoneal laparoscopic radical nephrectomy practice and outcomes based on data from the UK BAUS Nephrectomy Audit Database from 2012 to 2017
James Jenkins1, Chris Foy2 and Kim Davenport2
1Bristol Urological Institute, Southmead Hospital
2Cheltenham General Hospital
Abstract
Objective: Since the advent of laparoscopic surgery, there has been progressive sub-specialism among nephrectomists to the retroperitoneal or transperitoneal renal approach. UK comparisons between these methods are outdated and fail to reflect either the growth in experience or the improved completeness of audit data collection. We provide an updated view on laparoscopic radical nephrectomy (LRN) outcomes using the surgeon-reported data of the BAUS Nephrectomy database.
Methods: We performed a retrospective review of BAUS Nephrectomy database entries from January 2012 to December 2017 for all LRN procedures with the approach documented. Entries were analysed for patient characteristics and intraoperative/postoperative outcomes by Mann–Whitney tests and chi-squared analysis.
Results: A total of 15,328 LRNs were logged, with 12,584 (82.1%) transperitoneal and 2744 (17.9%) retroperitoneal procedures. A trend towards lower body mass index in the retroperitoneal group (28.9 vs. 29.4; P<0.003) and larger tumours in the transperitoneal group (6.73 cm vs. 6.27 cm; P<0.001) was seen. There was no statistical variation in mean patient age (64.2 years), Charlson comorbidity score (2.05), preoperative haemoglobin (135g/dL), gender (61.9% male) or lymph node status (4.2% positive). Intraoperative outcomes revealed greater blood loss in the transperitoneal group (178 ml vs. 114 ml; P<0.001) with increased transfusion requirements (3.6% vs. 2.7%; P<0.02). A modest increase in operative time was seen for transperitoneal procedures (2.5 vs. 2.4 hours; P<0.01). No statistically significant variation was seen in open conversion rates (4.4%) or documented intraoperative complications (3.9%). Postoperatively, retroperitoneal LRN resulted in minimally longer inpatient stays (4.7 vs. 4.5 days; P<0.001). No variation was seen in unplanned intensive treatment unit stays (1.8%), hospital deaths (0.3%) or positive tumour margins (2.6%).
Discussion: This represents the largest single study comparing outcomes between these procedures, representing over 90% of all LRNs performed in the UK between 2012 and 2017. Although higher transfusion rates were seen in the transperitoneal procedures, these and other differences are modest and both procedures are seen as viable options.