
Abstract
Objective:
Transurethral resection of bladder tumour (TURBT) is a common urological procedure. With improvements in technology, technique and community support, our unit was able to implement a dedicated day-case pathway for patients undergoing TURBT. The aim of this study was to prove that this has been a safe and cost-effective improvement to our urology service.
Patients and methods:
A retrospective audit was carried out of 312 elective TURBT cases performed in one centre between 2011 and 2014 (36 excluded for lack of data/emergency status). Data were gathered regarding length of stay, causes of delayed discharge, readmissions and resection quality.
Results:
In 2011, 11% of TURBTs were performed as day cases, and 66% had an overnight stay. After introduction of the TURBT pathway, by 2014, 68% patients went home the same day, and 21% had an overnight stay. The 30-day readmission rate in 2011 was 7% (mostly following overnight stays), whereas 6% were readmitted in 2014. Resection quality was comparable across the two groups.
Conclusion:
Our experience suggests that day-case TURBT can be widely implemented without compromising quality or patient safety.
Level of evidence:
Not applicable for this multicentre audit.
Introduction
Almost 11,000 new bladder cancers are diagnosed each year in the UK,1,2 with 25,000 transurethral resection of bladder tumours (TURBTs) performed in 2012–2013. TURBT for a new transitional cell carcinoma (TCC) treats the primary tumour and provides tissue for accurate pathological staging and risk stratification.3,4 A single postoperative administration of mitomycin C is given to reduce recurrence.4,5,6 Pathological markers indicating quality resection include presence of detrusor muscle and separate biopsies to exclude associated carcinoma in situ.4,7 These markers can be assessed to ensure quality is maintained when service changes are made.
Surveillance and repeat endoscopic treatments make non-muscle invasive bladder cancer (NMIBC) a costly malignancy to treat. 8 The Healthcare Commission (HCC) proposed that TURBT could be performed as a day case, 9 increasing day-case rates from 19.1% to 40% and releasing nearly half a million inpatient bed days each year. 9 The British Association of Day Surgery (BADS) also identified target day-case rates for common urological procedures, with the aim of up to 60% as day case. 10 Due to ‘long-stay payments’ for patients who stay longer than expected following TURBT, optimising this pathway is cost-effective. BADS and the Department of Health developed a Best Practice Tariff (£300 per case) to incentivise day surgery. 11 Release of hospital beds gives an opportunity cost of performing concurrent procedures and efficient bed management benefits acute admissions, enabling the transfer of patients out of the emergency department within the four-hour target.
A TURBT pathway was implemented in 2013, filtering all appropriate patients into a day surgery pathway at the point of diagnosis, subject to surgical, anaesthetic and social suitability (Appendix I).
This study assessed whether the introduction of this new pathway reduced length of stay without subsequent adverse effects on quality, complications or readmissions.
Patients and methods
The pathway was developed in 2012 by consultant staff and a nurse practitioner and was implemented in 2013 with trust clinical governance approval. Mitomycin C was administered in theatre, where appropriate, and drained and disposed of safely after an hour in recovery, before a new catheter bag was attached for discharge. Community support was provided to all patients using a local ‘health care at home’ service, and all patients were reviewed in hospital postoperatively to ensure they were suitable for same-day discharge. The patients were provided with contact details and were visited as required until a trial without catheter planned for the second day post discharge, unless stated otherwise (in the operation notes due to deep resection). This catheter removal was booked for the patient with the health-care-at-home team or in a diary based in the day-case unit. Patients who underwent surgery on a Friday waited an extra day for catheter removal on a Monday (day 3 post discharge). Although there were no fixed exclusion criteria for patients being on the pathway, social factors preventing same-day discharge were identified at the time of diagnosis and noted on the front page. Subsequently, any anaesthetic concerns related to same-day discharge were noted. These were reviewed on the day of surgery, and the patient was not discharged if there were any ongoing respiratory or cardiac issues.
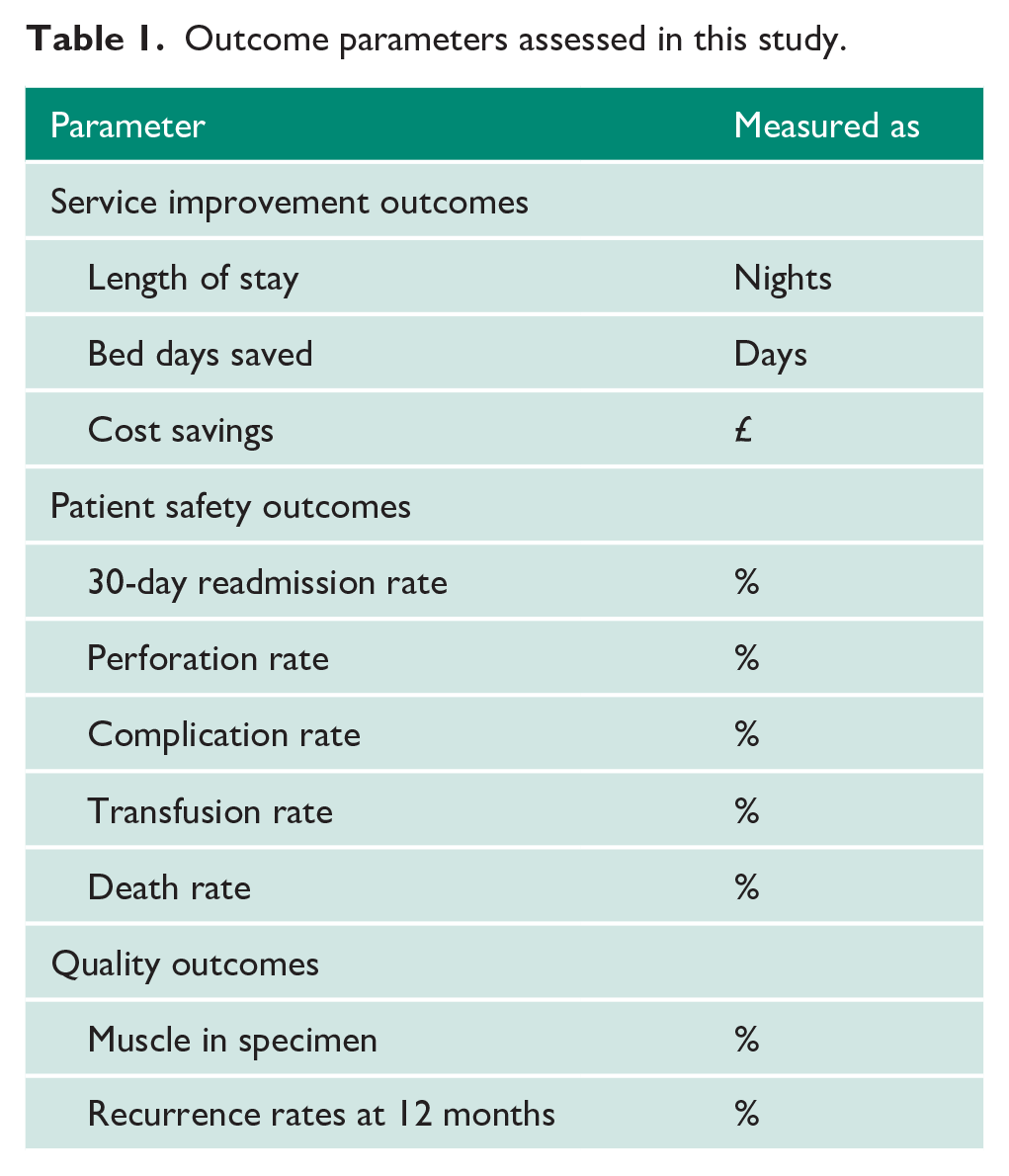
Data were collected retrospectively to audit the patient outcomes from 2011 (pre pathway) to 2014 (post pathway). Our local electronic operative log database was interrogated using the subheadings ‘urology’, ‘all surgeons’ and ‘TURBT’, with all TURBT procedures during each year recorded from 1 January to 31 December. All emergency cases were excluded, as it is well documented that outcomes are different for this group of patients when compared to the elective population. 12 All cases were analysed for indicators of the quality of resection, such as the presence of muscularis propria and recurrence rate at 12 months (Table 1).
Outcome parameters assessed in this study.
Results
After an initial data download from the local operating database, 179 cases were identified in 2011 and 167 cases in 2014. These included first and repeat resections. Initial analysis looked at length of stay (our primary end point), subsequent readmissions and complications (secondary end points).
Length of stay
A summary of data can be seen in Figure 1. For the purpose of analysis, 12 cases from 2011 were excluded from analysis due to no recorded length of stay in their electronic documentation, and nine emergency cases were excluded, leaving 158 data sets for analysis. In 2014, 21 cases were excluded, as they had no recorded length of stay, along with 10 emergency cases, leaving 136 complete data sets. In 2011, the majority of patients (105/158; 66%) stayed one night in hospital after TURBT. Only 18/158 (11%) went home on the same day as the procedure. The median length of stay in 2011 was one night, with a maximum length of stay of 14 days for social reasons. By 2014, most patients were discharged the same day (93/136; 68%), with a maximum length of stay of 11 days and a median length of stay of 0 nights.
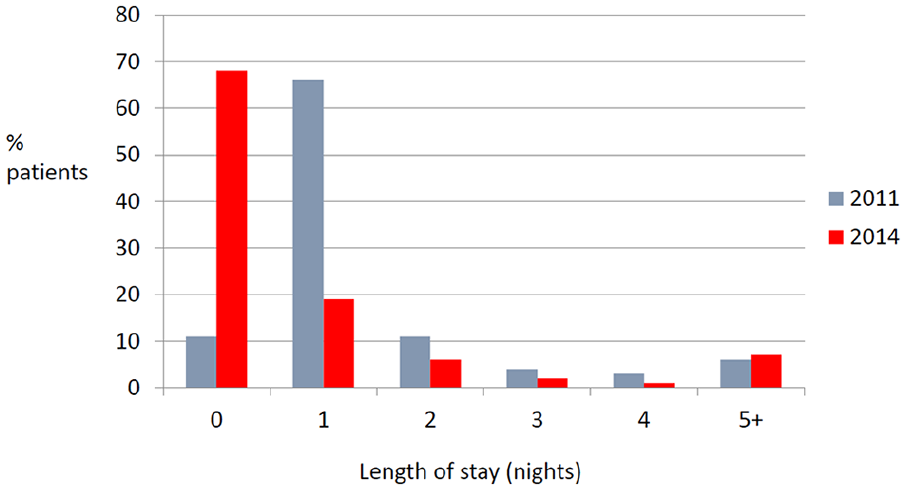
Comparison of length of stay following transurethral resection of bladder tumour in 2011 versus 2014.
The total number of bed days used for TURBT patients in 2011 was 309. This reduced to 134 by 2014, giving a total saving of 175 bed days. With an overnight bed in hospital costing approximately £225, this equates to a potential saving of £39,375.
Readmissions
In 2011, the overall 30-day readmission rate was 7% (11/158) compared to 6% (8/136) in 2014 (Figure 2). All of these readmissions were for Clavien–Dindo grade I or II complications only.
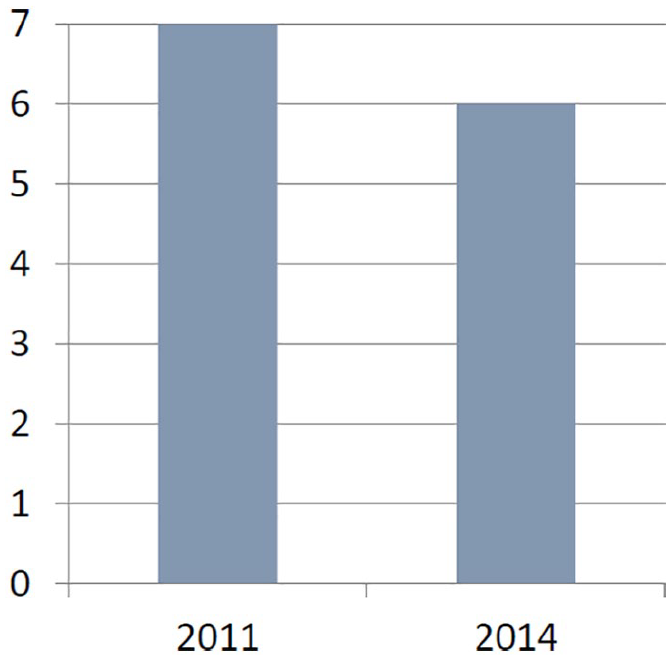
Thirty-day readmission rates (%) per year.
Complications
When assessing complications and quality, we looked at all the patients in each group, namely 179 in 2011 and 167 in 2014. In 2011, 4/179 (2%) patients received a transfusion, with one being intra-operative due to a low preoperative haemoglobin level, and 3/179 (1.7%) required a postoperative blood transfusion. The transfusion rate in 2014 was 1% (2/167). No patients died in the immediate postoperative period in 2011, although one patient died following elective TURBT in 2014 (0.6%) but after the initial 30-day period.
Resection quality
We measured quality of resection by determining whether the detrusor muscle was included in the specimen and through recurrence rates. In 2011, 129/179 (72%) TURBTs were performed solely by a consultant. In 2014, 132/167 (79%) were performed by a consultant. Regarding the histology, 174 cases were included in 2011, and 153 were included in 2014. Cases were excluded if the histological report did not mention whether the muscle was included, or if there was no mention of muscle in the specimen because the histology was clearly benign.
In 2011, 113/174 (65%) included the muscle in the resection specimen. Of the 61 cases without the muscle in the specimen, the vast majority (41/61; 67%) were G1pTa or G2pTa disease, and only six went on to have the muscle involved at a later date. In 2014, 136/153 (89%) resection specimens had evidence of the detrusor muscle being present. Of the remaining 17 cases, two eventually went on to have muscle involvement, and 9/17 (53%) were G2pTa cases.
We also assessed recurrence within the first 12 months following TURBT. In 2011, 22% of cases went on to have a recurrence, reducing to only 16% in 2014.
Discussion
Before HCC and BADS advice to increase day-case rates for TURBT, one article found 50% of TURBT-related ‘near misses’ in the cancer pathway were due to capacity limitations. 13 This supports the use of day-surgery pathways for TURBT, as it removes the need for an inpatient bed and associated health-care demands and costs. It is also more acceptable to patients to avoid a hospital stay, as a Danish study demonstrated that TURBT can impact quality of life. 14 There is also less chance of cancellation and associated impacts on well-being. 11
Our primary goal of increasing day-case rates for TURBT has been achieved, with a new rate of 68% (above the BADS recommendation), 10 resulting in a large number of day-bed and cost savings. Some patients still require a hospital stay: 12% stayed up to six nights for social reasons (30% of all patients requiring an overnight stay). This is comparable to an 11% reported rate of social admissions following urology surgery. 15 Social admissions are difficult to target for change but can be addressed at pre-assessment. Restarting care packages can cause delays, but only if the patient is in hospital for more than 24 hours. Support post anaesthetic could be overcome by not using general anaesthetic, and there have been developments recently in the use of short-acting spinal anaesthetic to enable safe day-case surgery.16,17
Although we do not have complete data on how many patients went home with a catheter, it would approach 100%. The aim was that all patients undergoing TURBT were discharged with a catheter. This helped prevent cautious (and potentially poor-quality) resection in a bid to avoid catheterisation, as surgeons knew that a catheter was accommodated as part of the pathway. Surgeons may have opted not to catheterise patients who only required cystoscopy with cold-cup biopsy, but these patients were not included here.
Readmission rates (unplanned admissions requiring an overnight stay) of 6% here were comparable to published rates of 5%. 18 These excluded attendances for catheter removal. Thirty-day unplanned hospital readmissions contribute to costs and are associated with a higher complication rate. 18 A multidisciplinary approach to the TURBT pathway may target areas associated with poorer outcomes (hypertension, diabetes and smoking). 18 The time-dependent nature of cancer pathways 19 limits the influence we can have on preoperative morbidities, but it is an area of consideration moving forward.
Overall, TURBT complication rates are around 6%. 20 We found a 6% rate of Clavien–Dindo grade I–II complications in patients readmitted after introduction of the new pathway, including a 1% transfusion rate. This compares favourably to a national UK audit which reported 20% Clavien I–II complications. 21 There is a potential risk of bladder perforation, the majority of which are subclinical. So, a period of catheterisation helps to reduce the effect of this, particularly with the use of mitomycin C.
Death rates were low, with no perioperative mortality in 2011. There was a single postoperative death in 2014 at 90 days. This makes the 30-day mortality rate 0% for both years, but the 90-day mortality rate in 2014 0.6%, lower than the reported 90-day mortality rates of 3.3%. 12
There was no reduction in quality of TURBT on the pathway. An increase in detrusor muscle in the specimen from 65% to 89% across the two time periods is consistent with published data. Older series reported rates of muscle as low as 48%, 20 whereas newer series quote rates of 79–90%.22,23 This is in line with guidelines that recommend a target detrusor muscle positive rate of 80%. 24 This increases the quality of resection such that residual tumour at re-resection reduces from 40–44% to 14–21% 7 and ensures patients receive effective treatment based on stage, grade and subsequent risk stratification. 4 However, it is important that surgeons can make a risk–benefit decision at the time of TURBT, as an overly deep resection in small papillary tumours, especially in elderly patients, may increase morbidity without added benefit, as these often do not invade beyond mucosa, and a complete resection can be achieved without the detrusor muscle.
There was a 79% rate of consultants performing TURBT noted – higher than the reported national average of 53.6%. 21 This will improve resection quality, but these results must be replicated by training junior surgeons in order to ensure ongoing provision of good quality TURBT.
There is a proven reduction in early recurrence following TURBT with a single dose of postoperative intravesical chemotherapy. 25 Our centre has trained staff to enable immediate postoperative mitomycin C administration in theatres, with drainage in the recovery area before return to the day unit. The recommended target is that 80% of patients receive postoperative chemotherapy within 24 hours of TURBT. 24 Currently, 73.1% of patients in the UK receive mitomycin C between 2 and 24 hours postoperatively. 21
These data prove TURBT can be performed safely as a day case in the majority of patients, across a range of ages and co-morbidities. This enables us to reassure patients that day-case surgery is safe and gives them confidence that they do not need to stay in hospital, without compromising their safety or outcomes. Anecdotally, patients prefer to recover at home. So, this also potentially improves overall quality of life, particularly in patients who require multiple surveillance procedures for NMIBC.
Conclusion
Our experience suggests that day-case TURBT can be widely implemented without compromising quality or patient safety. In fact, markers of quality and safety were better after moving to a day-case approach. This means we can confidently perform TURBT as a day-case procedure, benefitting the trust and the National Health Service as a whole financially whilst improving the patient experience in those who may require recurrent procedures. This can be further improved by designing new pathways for those patients who require social-care input and through exploring novel regional anaesthesia options, and work is ongoing to establish objective patient satisfaction with this pathway.
Supplemental Material
JCU_Appendix_one – Supplemental material for Applying an enhanced recovery approach to endoscopic procedures: Local experience with progression to day-case transurethral resection of bladder tumour
Supplemental material, JCU_Appendix_one for Applying an enhanced recovery approach to endoscopic procedures: Local experience with progression to day-case transurethral resection of bladder tumour by Hannah L Wells, Abigail Lazenbury, Lucy Fairchild and Mark Harris in Journal of Clinical Urology
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Registered with local audit office.
Informed consent
Included on consent forms used for operation.
Guarantor
M.H.
Contributorship
L.F. and M.H. designed and initiated the pathway and got trust clinical governance approval. A.L. and H.W. did the data collection. H.W. performed the data analysis and was the primary author on the paper with the assistance of M.H.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.