
Abstract
Objective:
This study aimed to analyse a population of men undergoing radical prostatectomy to determine whether a delay to surgery is associated with poorer outcomes. A secondary aim was to analyse whether the introduction of positron emission tomography (PET) imaging using probes labelled with radiotracers targeting prostate-specific membrane antigen (PSMA) was associated with delay.
Methods:
A retrospective chart review was performed for men undergoing radical prostatectomy in Cairns, Australia, between March 2014 and March 2018, who were identified from a prospectively maintained database.
Results:
A total of 332 cases were analysed. Logistic regression analysis failed to show extra time between biopsy and surgery as a predictor for any adverse outcome. Patients who underwent preoperative staging with PSMA-PET had a longer delay between biopsy and imaging (47.1±40.4 vs. 32.3±22.9 days; p<0.01) but a shorter duration between biopsy and surgery (109.5±64.7 vs. 132.5±70.8 days, p<0.01) compared with men staged with computed tomography and a bone scan.
Conclusions:
Delay to surgery was not a predictor for adverse pathological outcomes or the need for further postoperative treatment. Patients staged with PSMA-PET took longer to get their imaging but proceeded to surgery quicker overall, likely because they had a higher-risk disease.
Introduction
There can be delays for men who elect to proceed to radical prostatectomy for curative treatment of clinically localised prostate cancer. Patients are encouraged to take time to consider all their options after diagnosis, and this can involve referral to a radiation oncologist, a specialist prostate cancer nurse and/or a multidisciplinary meeting. In universal health-care systems, resources such as theatre time must be triaged and managed according to urgency. There is also increasing information available on social media platforms intended for prostate cancer patients, which may be misleading and unreliable but which can still create doubt for patients. 1 Any of these factors can contribute to men now taking longer to proceed to treatment.
Preoperative staging for prostate cancer has traditionally been performed using computed tomography (CT) and a radionuclide bone scan. 2 Over the past decade, there has been increasing interest in the use of positron emission tomography (PET) imaging for prostate cancer, specifically using ligands labelled with radiotracers which target prostate-specific membrane antigen (PSMA). PSMA-PET imaging has been shown to have high sensitivity and specificity in detecting prostate cancer metastases in the setting of biochemical recurrence following primary treatment, 3 but its use in primary staging before curative treatment is less clear. A systematic review recently concluded that there are only few high-quality studies assessing its use for staging, but it does appear to outperform traditional imaging modalities (i.e. CT and bone scan) in detecting metastases. 4 Despite a lack of definitive high-level evidence or guidelines to support its use, PSMA-PET is rapidly becoming utilised in Australia as the primary staging modality of choice, replacing CT and bone scan.4 –6
A delay between diagnosis of malignancy and surgical treatment has been clearly associated with poor cancer-specific and overall survival outcomes in many types of cancers. 7 There have been several studies which have aimed to determine whether a delay to radical prostatectomy affects clinical outcomes, but their results have been conflicting.8 –11 A Japanese study concluded that for men treated with robot-assisted laparoscopic radical prostatectomy (RALP), a delay of more than 6 months between biopsy and surgery did not affect the rate of biochemical recurrence. 8 Another recent publication found that for more than 2000 men with high-risk prostate cancer treated in Baltimore, those who waited longer than 3 months for surgery had no difference in biochemical recurrence, adjuvant therapy or metastasis-free survival. 10 Other recent publications have had different conclusions. Another American study including more than 2000 men concluded that men were more likely to have adverse pathological features if they had surgery more than 75 days after biopsy, with the highest-risk patients having worse pathology if there was a delay of more than just 30 days. 11 A Canadian study also showed on multivariate analysis that high-risk patients who waited more than 90 days for surgery had higher rates of biochemical recurrence and further treatment, but this was not the case for low- or intermediate-risk patients. 9
In summary, the evidence as to whether the time taken to proceed to surgery affects clinical outcomes is unclear. The aim of this study was to assess a cohort of Australian men who underwent surgery for prostate cancer in order to determine whether a delay to surgery influenced clinical and pathological outcomes. It was hypothesised that a lengthier time between diagnosis and surgery may be associated with worse pathological outcomes or higher rates of adjuvant or salvage treatment. It was also hypothesised that men undergoing PSMA-PET for staging might experience a delay to surgery.
Methods
A prospectively updated database of all radical prostatectomies performed by three surgeons in Cairns, Australia, was used as the source to identify patients for this study. This included patients undergoing both public and private treatment. All patients undergoing radical prostatectomy between March 2014 and March 2018 were identified from this database and were screened for eligibility. Men were excluded from the final analysis if their biopsy data, including date of biopsy or histopathology from biopsy, was unable to be retrieved. Men without final prostatectomy histopathology available were also excluded. Patients who had neo-adjuvant treatment with androgen deprivation therapy (ADT) preoperatively were excluded, as were men who were treated with salvage radical prostatectomy following previous curative intent treatment.
A retrospective review of the electronic medical record was undertaken. Data including the initial serum prostate-specific antigen (PSA) level, date of biopsy and subsequent biopsy results were recorded. The modality of staging imaging used and the date of these scans were noted. The date of surgery and final pathological data from prostatectomy (specifically grade, margin status and pathological stage) were recorded. Postoperative follow-up outcomes were documented, including PSA results and need for subsequent treatment, including adjuvant or salvage radiation therapy, chemotherapy or ADT. Any detectable postoperative PSA was used as a surrogate marker of adverse clinical outcome, as it has been shown to be associated with poorer outcomes. 12
Statistical analysis was performed using IBM SPSS Statistics for Windows v24 (IBM Corp; Armonk, NY). Univariate analysis between groups was performed with Fisher’s exact test for categorical outcomes and unpaired t-test for continuous variables. A p-value of <0.05 was determined to be statistically significant. Binary logistic regression analysis was performed for adverse pathological and clinical outcomes using time from biopsy to surgery as the variable to assess whether it predicted adverse outcomes.
Results
A total of 343 men were identified from the radical prostatectomy database. Four men were excluded due to unavailable data. In addition, three had no biopsy histology available, and one had no final prostatectomy data available. A further four men were excluded due to neo-adjuvant hormone use, and three men were excluded due to previous treatment (i.e. radiation or cryotherapy).
Of the screened cohort undergoing radical prostatectomy, 332 men were included in the final analysis. The demographics and pre- and postoperative data of the cohort are detailed in Table 1. The mean age of the patients was 63.1±6.4 years. Most patients (82.5%) underwent RALP without lymph-node dissection.
Characteristics of patients included in the study (N=332).
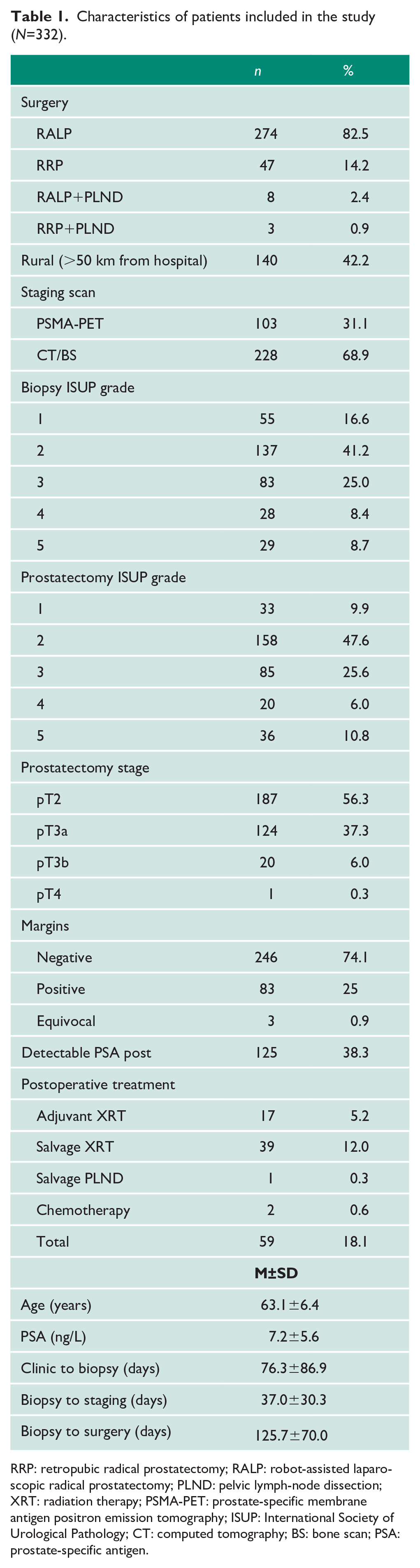
RRP: retropubic radical prostatectomy; RALP: robot-assisted laparoscopic radical prostatectomy; PLND: pelvic lymph-node dissection; XRT: radiation therapy; PSMA-PET: prostate-specific membrane antigen positron emission tomography; ISUP: International Society of Urological Pathology; CT: computed tomography; BS: bone scan; PSA: prostate-specific antigen.
The mean PSA level prior to biopsy was 7.2±5.6 ng/mL. The most common histopathological grade of prostate cancer diagnosed at both biopsy and radical prostatectomy was grade group 2 as defined by the International Society of Urological Pathology (ISUP). The distribution of ISUP grade groups at biopsy and final prostatectomy specimen is detailed in Table 1. A total of 103 (31.1%) men were staged using PSMA-PET imaging compared with 228 (68.9%) with CT and bone scan. The median duration between biopsy and surgery for the whole cohort was 107 days (range 14–431 days; M=125.7±70 days).
Patients who underwent preoperative staging with PSMA-PET scans had an average delay between biopsy and imaging of 47.1±40.4 days, which was significantly longer than the wait for men imaged with CT and bone scan (32.3±22.9 days; p<0.01). However, men receiving a PSMA-PET scan had an average duration between biopsy and radical prostatectomy of 109.5±64.7 days, which was significantly shorter compared to 132.5±70.8 days for men staged with CT and bone scan (p<0.01). Men selected for staging with PSMA-PET had higher initial PSA levels and greater proportions of higher-grade disease on biopsy (Table 2). Rural patients (defined as living more than 50 km from urological services) averaged 133.9±72.0 days between biopsy and surgery compared to 120.1±68.1 days for men who lived closer to the treatment centre (p=0.08).
Preoperative characteristics of prostate cancer patients undergoing different types of staging imaging.
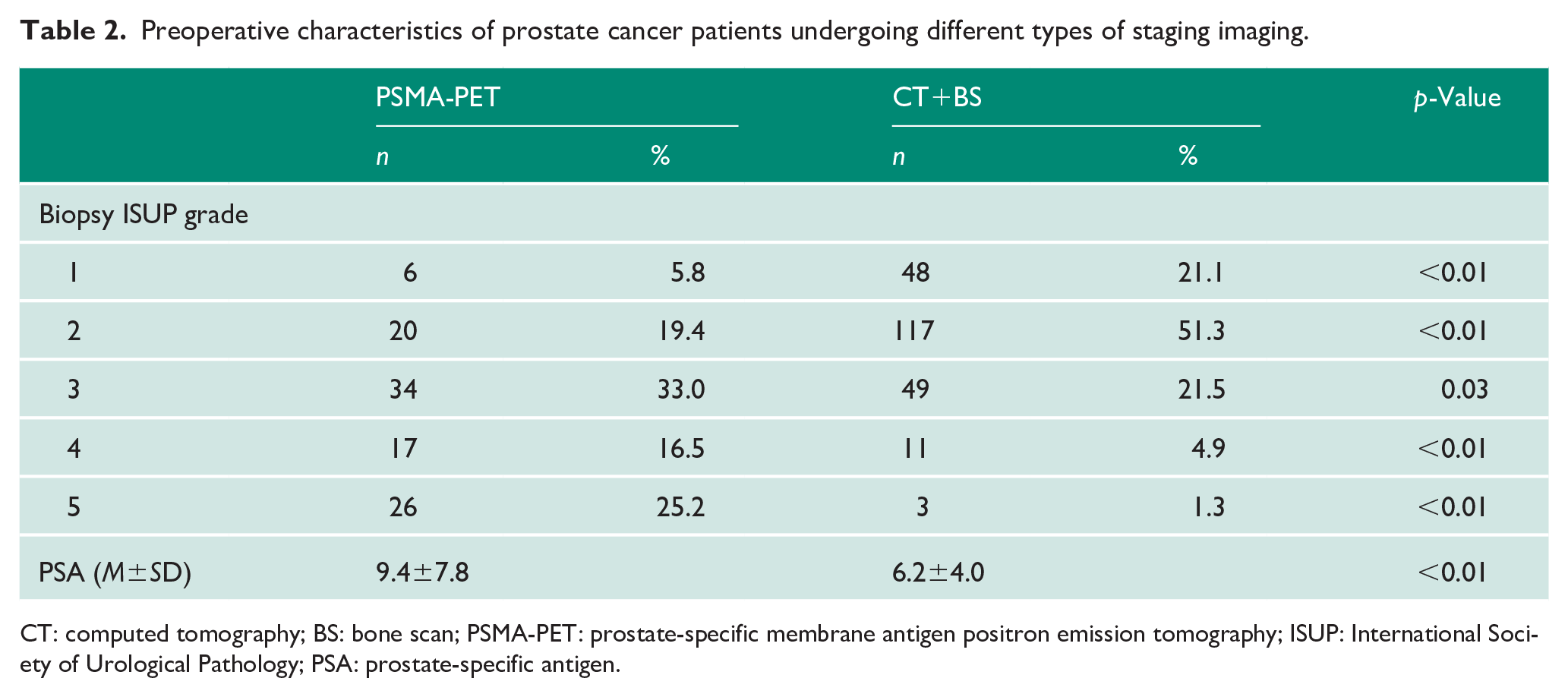
CT: computed tomography; BS: bone scan; PSMA-PET: prostate-specific membrane antigen positron emission tomography; ISUP: International Society of Urological Pathology; PSA: prostate-specific antigen.
The proportions of the total cohort having adverse pathological outcomes, including positive surgical margins and extra-prostatic extension (stage pT3 and above), are outlined in Table 1.
There were 125 (37.8%) men treated with radical prostatectomy within 90 days of biopsy. When compared to men who waited more than 90 days from biopsy to surgery, there was no difference in rates of positive surgical margins or the need for postoperative treatment such as radiation therapy (Figure 1). Of men treated within 90 days, 16.0% experienced an upgrading of their histopathology compared to 24.6% of men waiting more than 90 days between biopsy and surgery (p=0.07). There was a significantly greater proportion of men with pT3 or greater pathological stage in the group who had surgery within 90 days of biopsy (51.2% vs. 39.1%; p=0.04). Logistic regression analysis failed to show time between biopsy and surgery as a predictor for any adverse outcome except for pathological extra-prostatic extension or pT3 disease (Table 3).
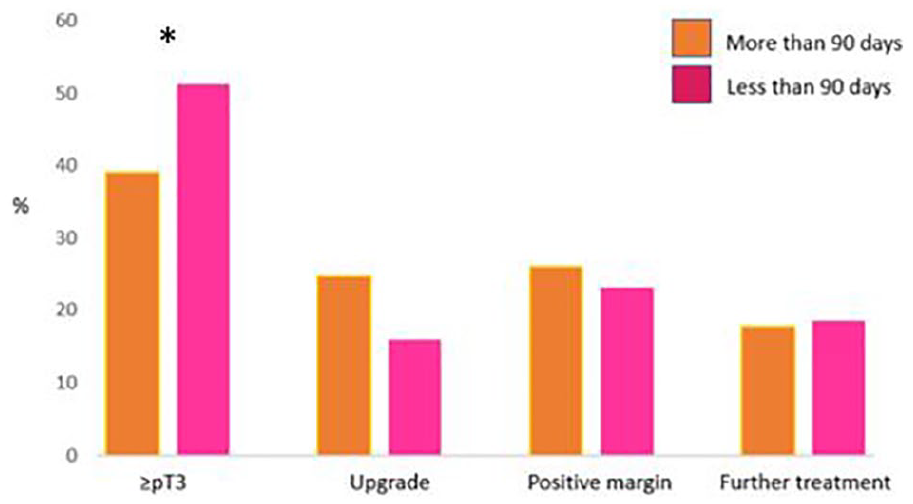
Percentage of patients with adverse pathological or clinical outcomes, separated into groups by time from biopsy to surgery. *p<0.05.
Logistic regression analysis of prediction of adverse pathological outcomes by time from biopsy to surgery.
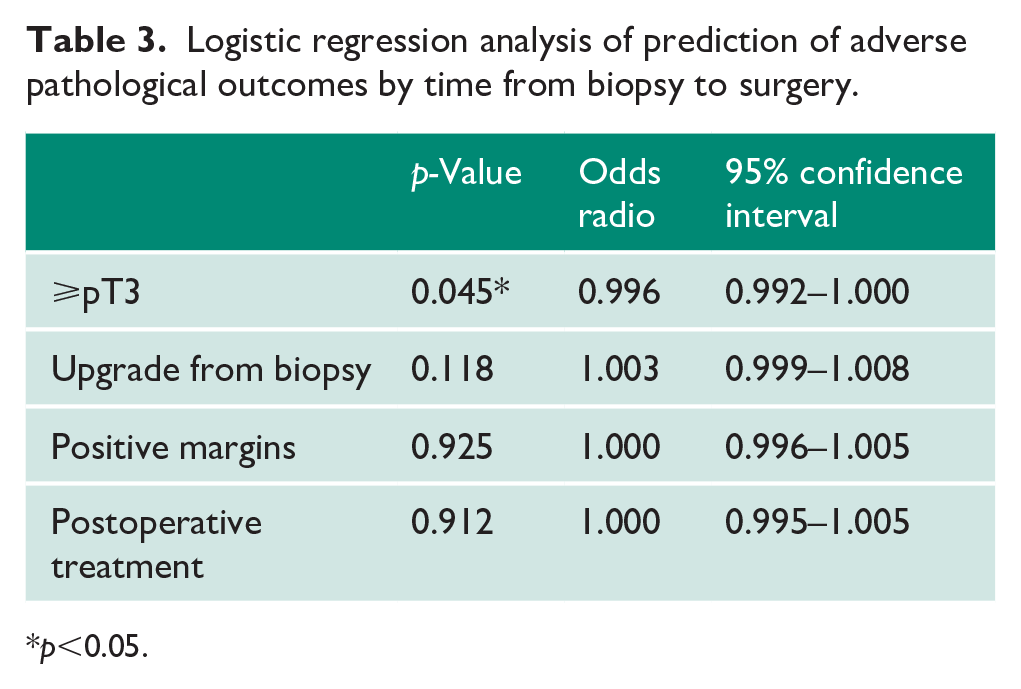
*p<0.05.
Discussion
This retrospective analysis shows that men who waited longer between biopsy and radical prostatectomy in this cohort did not have worse clinical outcomes in terms of needing further adjuvant treatment. There was a higher proportion of men with extra-prostatic extension or pathological stage T3 disease in the cohort of men who waited less than 90 days. This is likely to be due to preoperative concern about extra-prostatic extension based on either digital rectal examination or multi-parametric magnetic resonance imaging of the prostate, which would influence surgeons to book prostatectomy on a more urgent basis. There was a trend towards upgrading of ISUP grade group histology from biopsy to prostatectomy for men who faced lengthier delays, although this did not reach statistical significance. Previous retrospective studies have reported conflicting results in regard to whether delay increases the risk of pathological upgrading. Hirasawa et al. 8 found that delay did not influence the rate of upgrading in their mixed-risk cohort, while O’Brien et al. 13 found a delay of 6 months or more was associated with pathological upgrading. Importantly, their cohort was comprised of men with only low-risk disease.
Other studies have used biochemical recurrence, defined as a postoperative PSA of ⩾0.2 ng/mL, as a measure of adverse outcome.8,13 Many patients with biochemical recurrence, however, never go on to have further treatment over many years, and many such patients will never develop symptomatic metastatic disease. 14 There is also a large cohort of patients who are treated with postoperative adjuvant or salvage radiation therapy without ever reaching this definition of biochemical recurrence. These men may be treated with adjuvant radiation in the setting of adverse pathological predictors such as positive surgical margins or ‘early salvage’ radiation in the setting of a detectable PSA which is <0.2 ng/mL. 12 Radiation therapy has been linked with worse quality of life and functional outcomes for men who receive it, 15 and therefore the need for postoperative treatment was judged for this study to be a more relevant definition of adverse clinical outcome than simply detectable PSA. Nearly 82% of patients in this cohort had avoided the need for postoperative treatment, and this proportion is comparable to other cohorts recording ‘biochemical recurrence free survival’.8,9 There were, however, significant differences in these cohorts compared to the current study. Zanaty et al. 9 did not include any patients undergoing adjuvant radiation therapy, while Hirasawa et al. 8 had a relatively small cohort of eligible patients after they performed their propensity score-matching analysis.
A previous study by Abern et al. found an increased rate of positive surgical margins in patients who waited more than 9 months for radical prostatectomy, and this group also had higher rates of biochemical recurrence. 16 However, in this same cohort, patients who waited between 3 and 9 months had no worse outcomes than those who proceeded to surgery within 3 months. 16 These findings were only true for men with intermediate-risk disease, and there was no difference over the same time frame for men with low-risk disease. 16 That study also had much higher rates of positive surgical margins in the order of 50% for intermediate-risk patients. 16
Men in this study who had their prostate cancer staged with PSMA-PET waited longer for their staging imaging but proceeded to surgery faster than their counterparts staged with CT and bone scan. The most likely explanation for this is that men with higher-risk disease were more likely to be staged with PSMA-PET, and these are men who are more likely to be booked for expedient surgery. The benefits of PSMA-PET in the primary staging setting is currently subject to a multi-centre clinical trial in Australia. 17
Like many retrospective studies looking at prostate cancer, this study is limited by its relatively short follow-up which precludes any meaningful conclusions being drawn about survival and long-term prognosis. There are several potential biases, including selection bias which is inherent in all retrospective analyses, but particularly in this study where there was no control for disease risk between patients who waited more or less than 90 days. Patients with low-risk disease may have a period of observation or surveillance before deciding to proceed with prostatectomy, and these men will inherently have more favourable outcomes than high-risk patients. Finally, the decision to use time between prostate biopsy and prostatectomy was used as the main delay variable to be consistent with other previously published studies. This risks not acknowledging that for some patients, there may be a confounder in considerable delay prior to deciding to proceed with diagnostic biopsy, evidenced by the standard deviation seen for the duration between outpatient clinic and biopsy.
Conclusions
In this cohort, time between prostate biopsy and radical prostatectomy was not associated with adverse pathological outcomes or need for further postoperative treatment. Patients who were selected to be staged with PSMA-PET took longer to complete their staging imaging but proceeded to surgery quicker overall – likely because they had higher-risk disease. Patients can be reassured that current wait times for surgery and imaging studies do not appear to compromise outcomes in this cohort, but these results should be cautiously applied to other populations.
Footnotes
Acknowledgements
Thank you to all of the staff at Cairns Hospital, both clinical and non-clinical, who made this project a success. This research was undertaken as part of the third year of the MSc in Surgical Sciences through the University of Edinburgh by Alexander Nesbitt.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
The ethics committee of Far North Queensland approved this study (LNR/2018/QCH/48375 (Nov ver 1) – 1304 QA).
Informed consent
Written informed consent was deemed unnecessary in this retrospective audit by the Ethics Committee
Guarantor
A.N.
Contributorship
A.N. collected the data, analysed the data and wrote the initial manuscript. P.S. conceived the idea for the study, and G.E., S.A. and P.S. together refined the study design, helped in data collection, provided advice on interpretation and edited the manuscript. S.P. supervised the study, performed the literature review and edited the manuscript.