
Abstract
Objective:
The COVID-19 pandemic has had a profound impact on the provision of surgery across the NHS. Despite the challenges, the uro-oncology surgical provision at our centre in the northwest of England, a COVID-19 hotspot, has continued throughout.
Patients and methods:
We report a 26-patient case series performed following national lockdown. Patients were initially screened for COVID-19 symptoms and later all patients required a negative swab pre-operatively. Personal protective equipment using aerosol precautions was used for all cases. A post-operative ‘cold’ COVID-19 critical-care ward was created. Patients who developed possible symptoms of COVID-19 were isolated and swabbed. A telephone questionnaire was completed two weeks following discharge.
Results:
Three out of 26 patients developed post-operative pyrexia, but all tested negative for COVID-19. Non-COVID-19-related complication rates were consistent with our previous results. Telephone follow-up confirmed that none had experienced symptoms suggestive of COVID-19 infection. Overall, patient satisfaction with hospital COVID-19 precautions was high. All patients were satisfied with their decision to undergo surgery during the pandemic.
Conclusions:
Our results indicate that during the peak of the COVID-19 pandemic, with appropriate precautions, a safe surgical service can be continued.
Level of evidence
Level 3
Introduction
The impact on the provision of elective surgery during the current COVID-19 pandemic across the country has been dramatic as the main focus for hospitals shifted to the management of acutely unwell patients with COVID-19. Nationally this has had a significant impact on the provision of surgical cancer care with delays accessing treatment or modifications in management.
The impact of the virus and mitigation planning has had a wide ranging effect on surgical provision. Operating theatres have been closed to free up staff and ventilators for delivery of increased critical-care capacity. Staff members have also been redeployed to help operate critical-care departments.
Additionally, recently published data has shown that peri-operative COVID-19 infection has a high pulmonary complication rate which is associated with a high mortality. 1
Despite these challenges, the national guidelines recommended that urgent cancer care should continue throughout the pandemic. There is currently no published information from the UK on the outcomes of patients undergoing complex urological surgery during the pandemic.
We present a case series of patients operated on during the COVID-19 pandemic in a tertiary urology unit in the northwest of England during a time when the region had one of the highest incidences of COVID-19 cases in the UK outside of London. We describe the steps taken to allow urgent complex cancer surgery to continue during the pandemic and show their short-term follow-up.
Materials and methods
A prospective data collection of all major uro-oncology procedures was undertaken from 23 March 2020, the date of ‘National Lockdown’ in the UK. These cases were performed with special measures put in place at all stages of the patient journey to reduce the risk to patients and staff with regards to COVID-19 infection and transmission.
Pre-operative precautions
During the lockdown, all patients on the Northern Care Alliance (NCA) cancer waiting list were categorised into priority groups for surgery as per NHS England guidance (Levels from I-IV). 2 All category I and II patients (those that required treatment within four weeks) were considered for surgery during this time.
In the initial period following lockdown, patients were screened by telephone for symptoms of COVID-19, including cough and temperature. The procedures of patients reporting symptoms were delayed. Patients were carefully counselled by senior clinicians regarding the benefit and risks associated with surgery during the pandemic period. The uncertainty regarding the risks of exposure to COVID-19 during hospital attendance was discussed in general terms based on the level of knowledge at the time and available national guidance.
With the increased availability of testing in April 2020, a policy was introduced to screen all pre-operative patients for COVID-19 three days prior to planned surgery. Only patients with a negative nasal and oropharyngeal swab proceeded to surgery.
Patients were mandated to strictly self-isolate for 14 days prior to their procedure. Adherence to this policy was assessed by the surgical and anaesthetic team on the morning of surgery. Patients who did not follow this policy were advised beforehand that they would be cancelled.
Intra-operative precautions
On the morning of surgery all patients were admitted to a dedicated COVID-19 negative area within the hospital (green area). All patients that were admitted to this area were COVID-19 screened (initially via questionnaire and later with COVID-19 swabs with increased availability) prior to surgery and had been strictly self-isolating for 14 days pre-admission. The flow of patients to the operating theatre was through the COVID-free green area.
All patients were intubated in the operating theatre with all staff wearing full personal protective equipment (PPE) using aerosol precautions.
Standard of equipment for theatre staff included FFP3 masks with all staff members having been formally fit tested. All staff members wore full-length sleeve surgical gowns, a visor and gloves during the procedure. The surgical team wore full FFP3 masks, a visor, a hood as well as a surgical hat and double gowned and double gloved. The theatre staff were divided into two teams: one team in theatre wore full PPE for the whole case as described and the second team remained in the ante-room to supply any additional materials and equipment to the theatre staff to avoid staff leaving the theatre for the duration of the procedure.
Following guidance from the Royal College of Surgeons regarding concerns that laparoscopic procedures may be aerosol generating, all surgery was initially undertaken open. 3 Following further guidance in April suggesting that laparoscopic cases could be safely undertaken with appropriate precautions, laparoscopic nephrectomy cases were reinstated with systems that facilitated smoke evacuation and filtration with 0.01µ ultra-low particulate air (ULPA) filters.
Extubation took place in theatre and before transfer to the recovery area. The operating theatre was taken out of use for 20 minutes before staff were allowed to re-enter to clean and prepare for the next case.
Post-operative precautions
Following surgery, all patients were managed in a dedicated post-operative COVID-19 negative ‘green’ critical-care area. No emergency admissions were permitted to this ward. Any patients who may have developed symptoms suggestive of possible COVID-19 infection post-operatively were isolated in a side room and swabbed for the virus.
Post-operative follow-up
Two weeks following discharge from hospital, a post-operative telephone review and questionnaire were undertaken. Patients were assessed for post-operative surgical issues, COVID-19 symptoms and patient satisfaction
Data was collected on patient demographics, performance status and co-morbidities. Intra-operative data was recorded including operating time and blood loss. Post-operative histology and staging was recorded.
Results
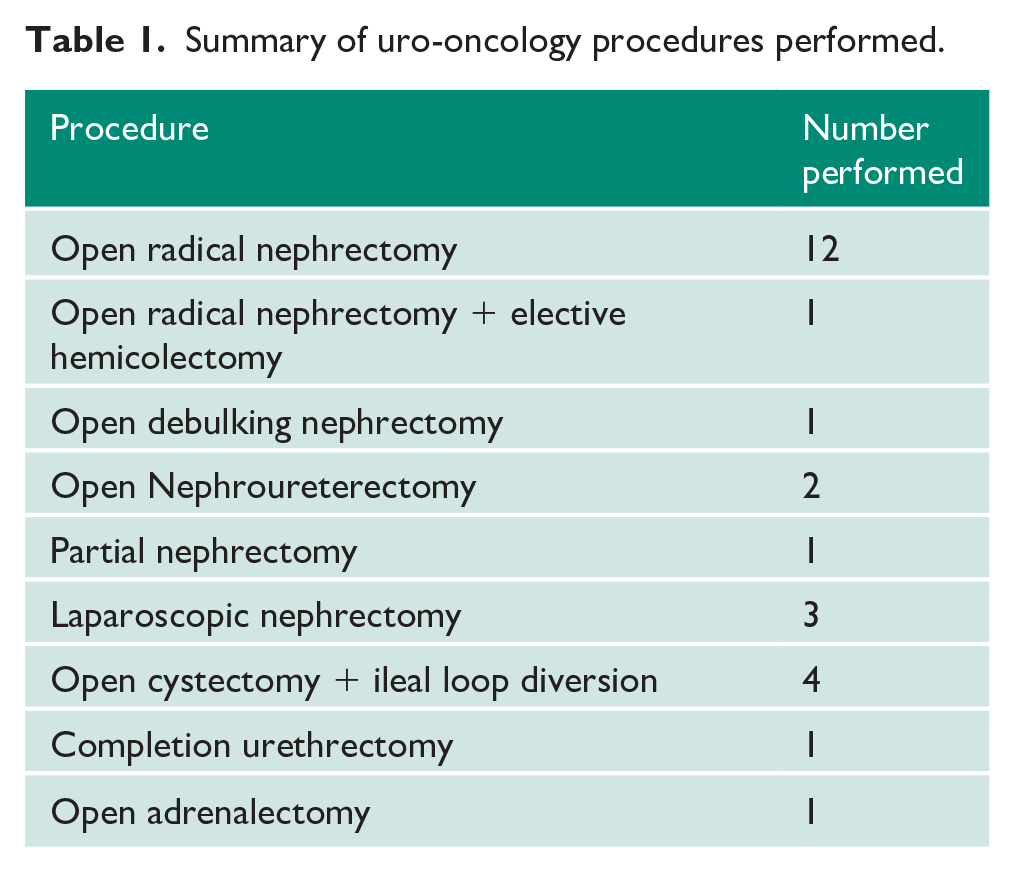
Between 24 March and 19 May 2020, 26 major uro-oncology procedures were performed, coinciding with the peak of the COVID-19 crisis in the northwest of England (Figure 1) and within the hospital (Figure 2). The procedures that were undertaken are listed in Table 1.
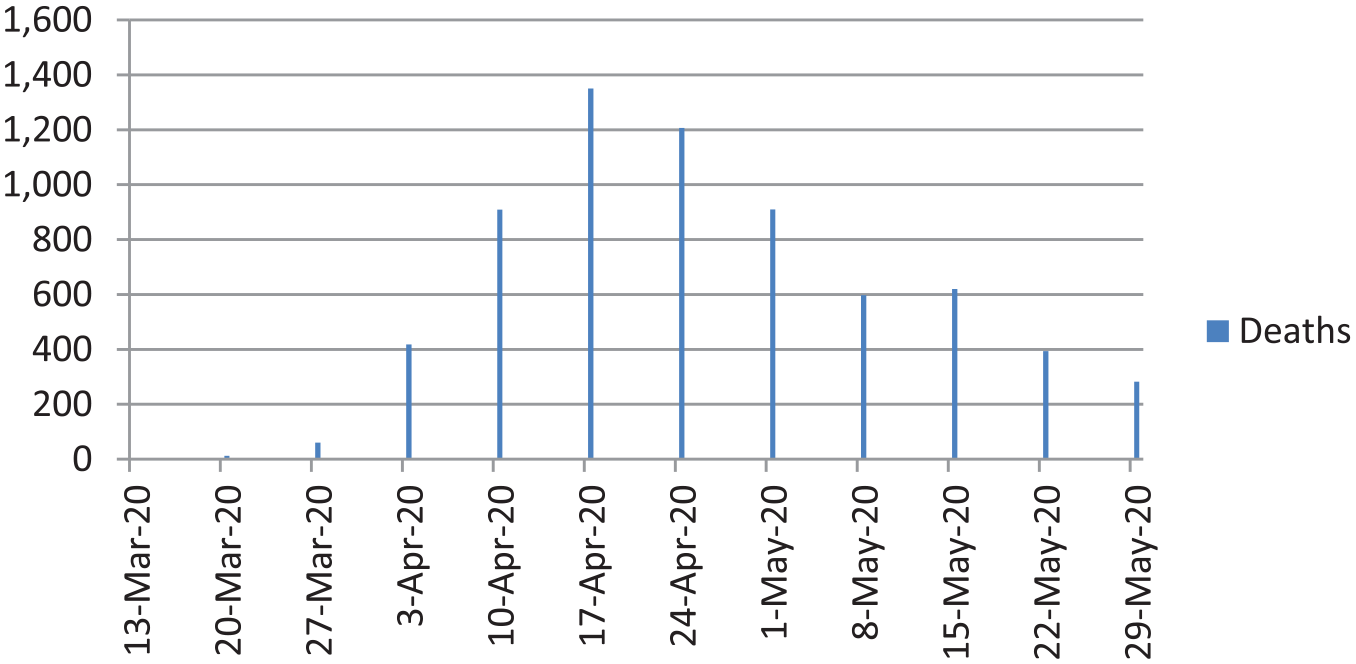
Weekly COVID-19 associated deaths in the northwest of England. 5
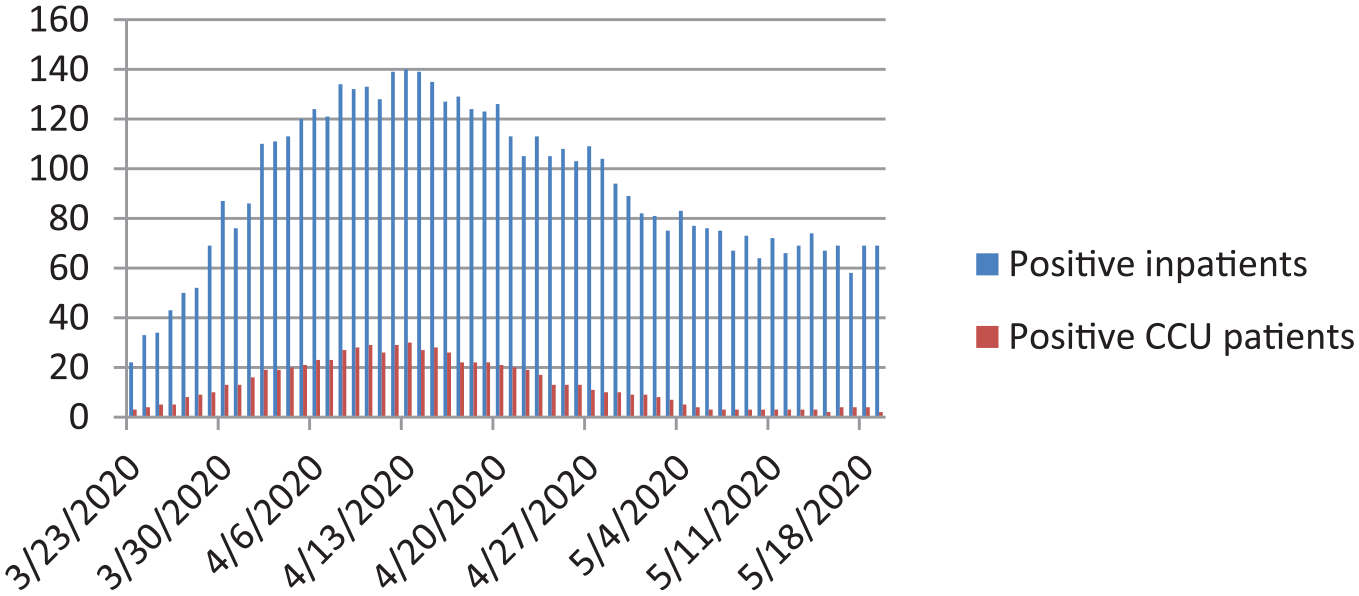
Local hospital COVID-19 numbers showing positive inpatients and positive patients on the critical-care unit (CCU).
Summary of uro-oncology procedures performed.
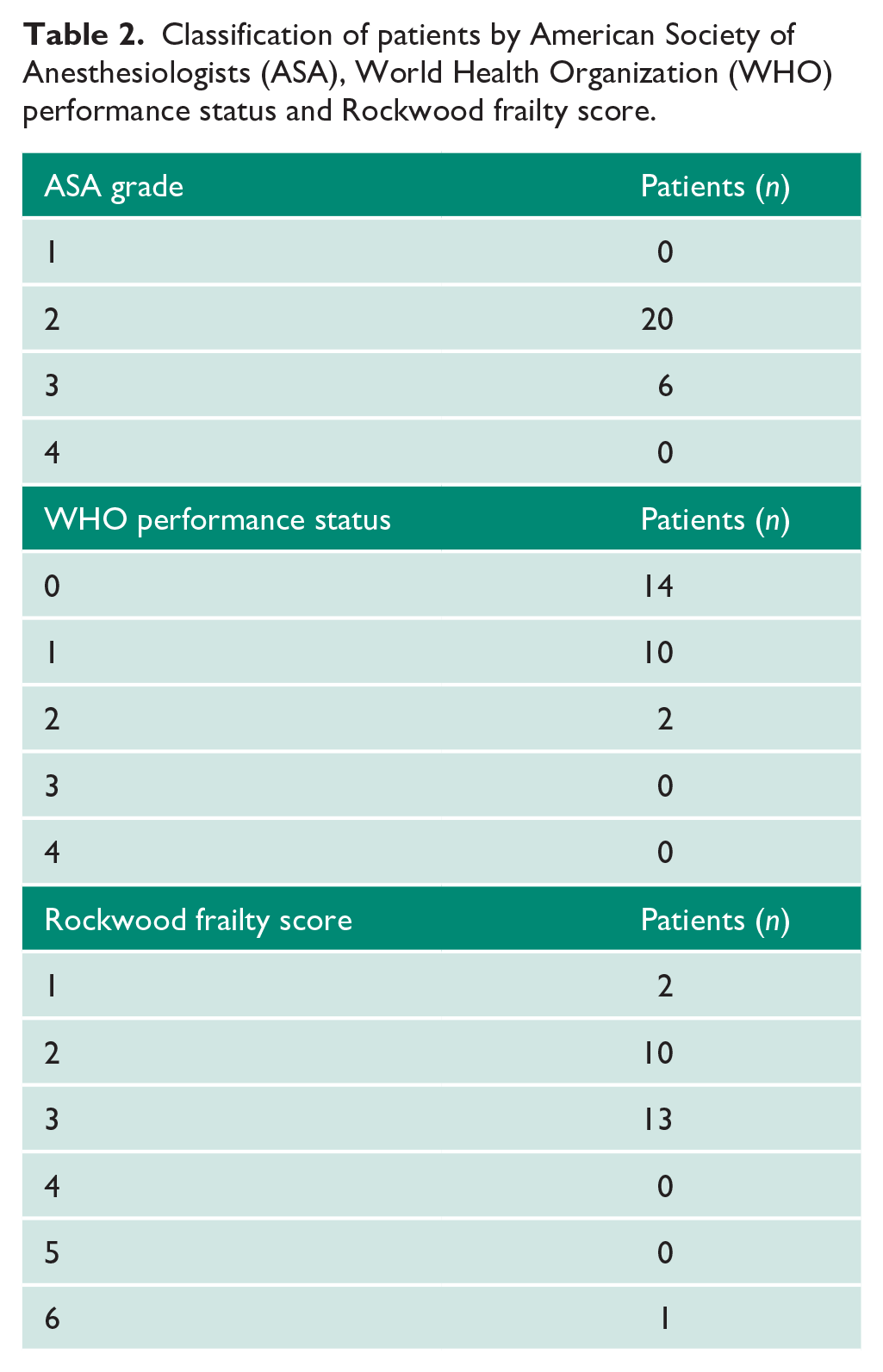
The median age of the patients was 60 (range 50–77). The World Health Organization (WHO) performance status, American Society of Anesthesiologists (ASA) and Rookwood frailty scores 4 were assessed by the surgical and anaesthetic teams (Table 2).
Classification of patients by American Society of Anesthesiologists (ASA), World Health Organization (WHO) performance status and Rockwood frailty score.
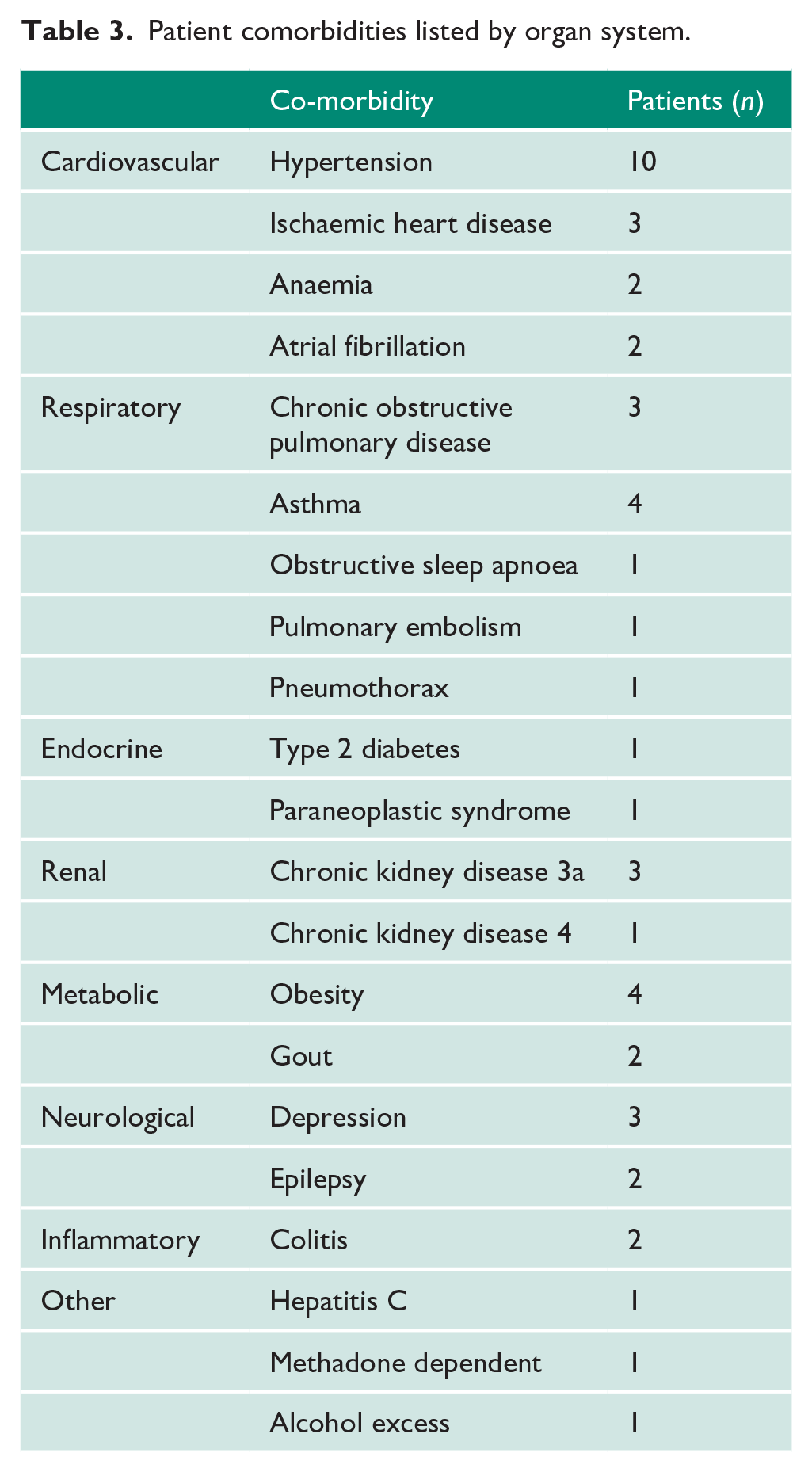
Co-morbidities of the patients are shown in Table 3. Ten out of 26 patients had a documented respiratory comorbidity including asthma (4), chronic obstructive pulmonary disease (COPD; 3), previous pulmonary embolus (1) and obstructive sleep apnoea (1). Patients had a median body mass index (BMI) of 27.6 (range 60.2–18.6).
Patient comorbidities listed by organ system.
All patients were compliant with the pre-operative self-isolation policy and no patients were cancelled on the day of surgery for this reason.
Mean surgical time was 196 minutes (range 70–435 minutes) and mean bloods loss was 205 mls (range 10–800mls).
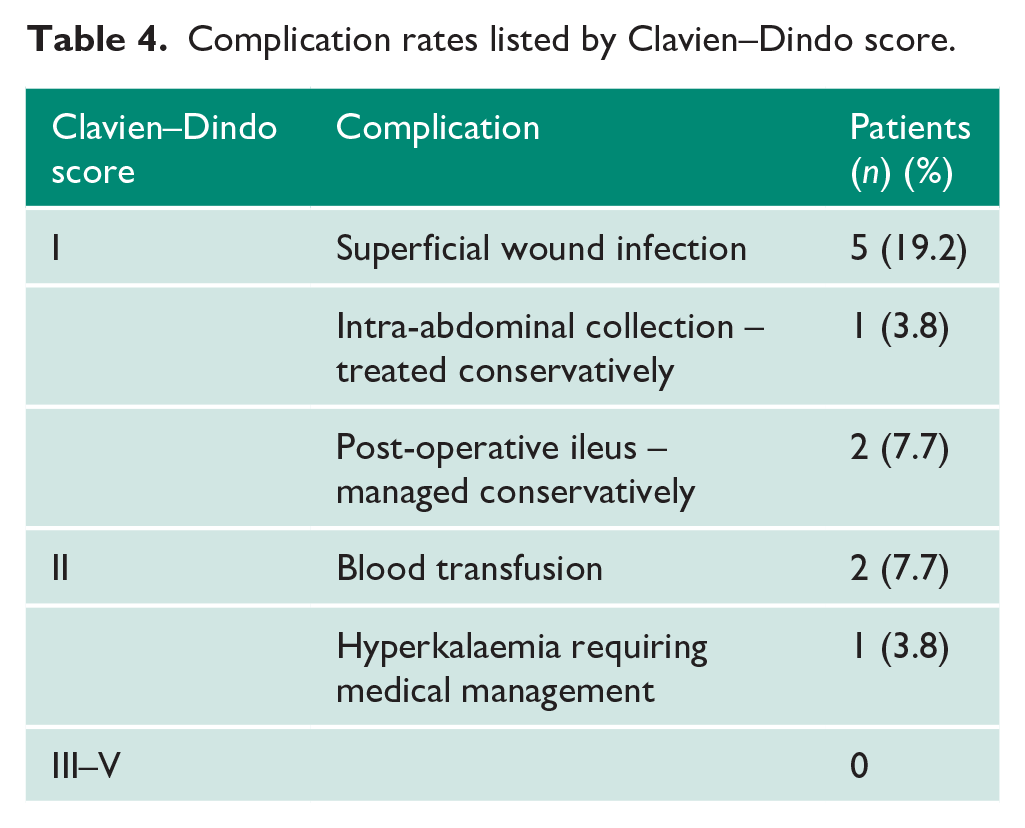
None of the patients had a Clavien–Dindo grade III complication or higher. There were 10 patients (38%) with a minor complication graded Clavien–Dindo I or II (Table 4). There were no recorded hospital readmissions.
Complication rates listed by Clavien–Dindo score.
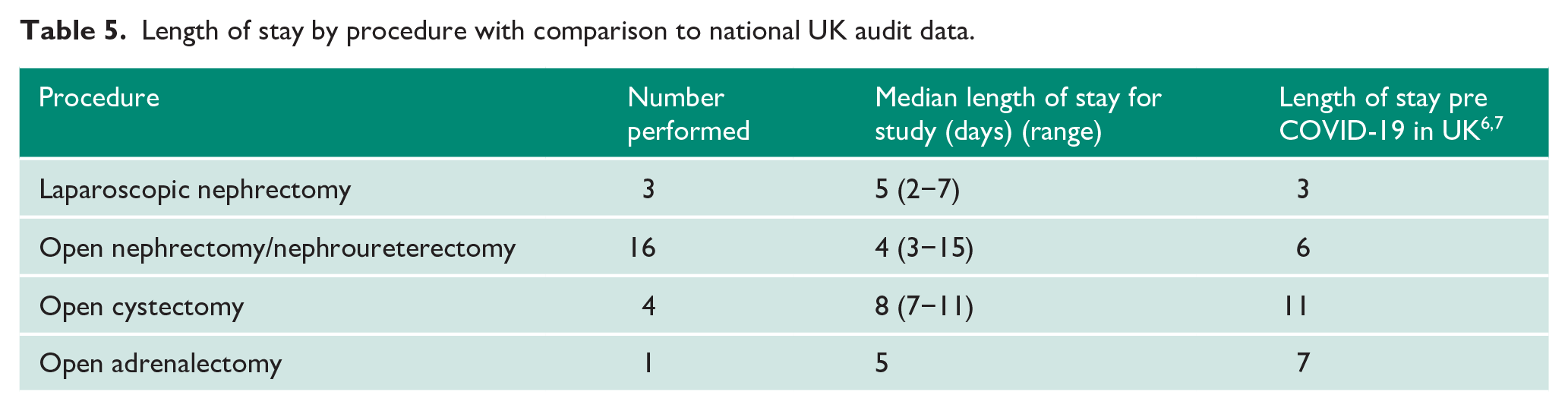
The combined median length of stay for all procedures was five days (range 2–15 days). Table 5 shows the length of stay by operation compared to pre-COVID-19 UK average length of stay for the same procedure.
Length of stay by procedure with comparison to national UK audit data.
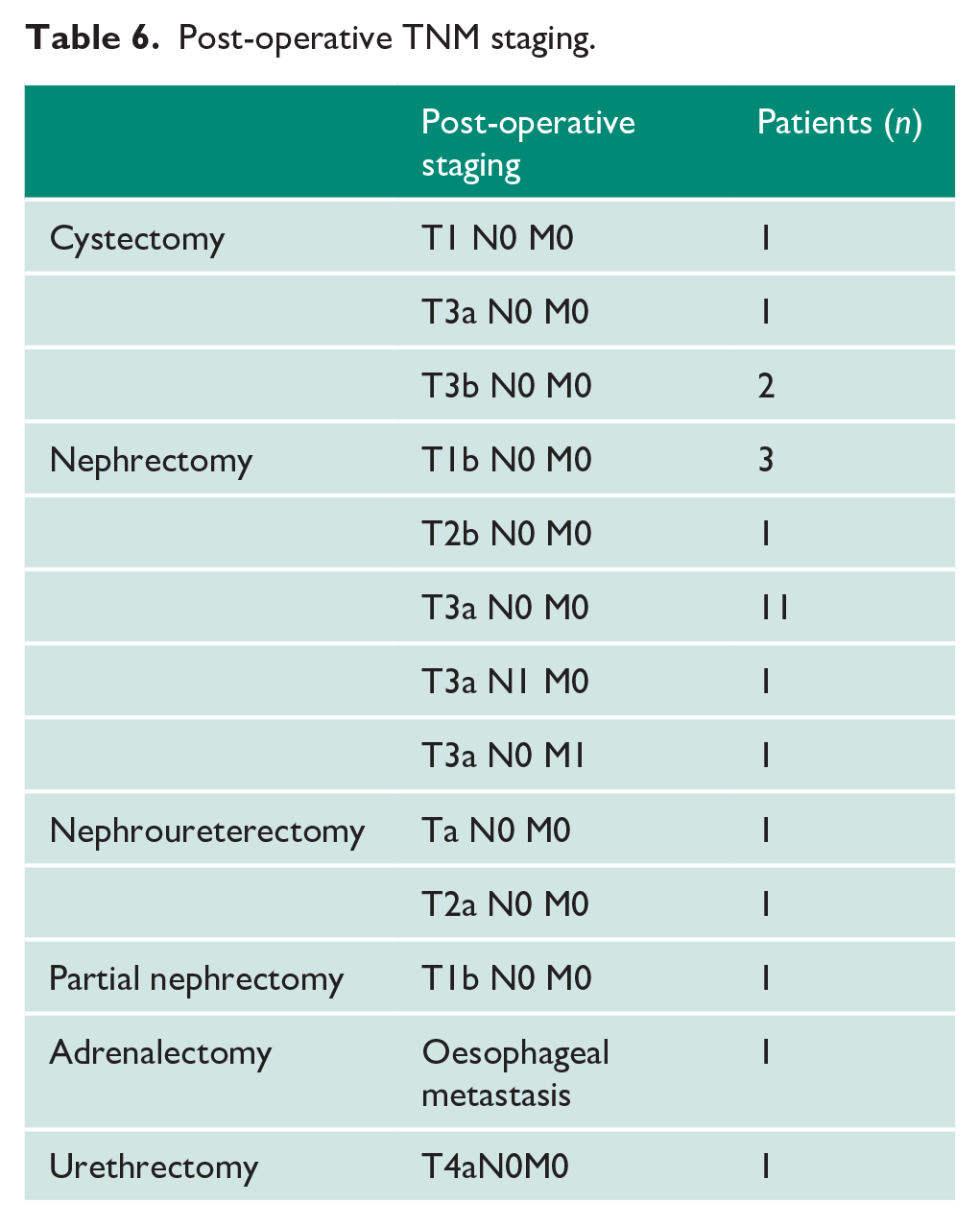
A breakdown of the post-operative staging is shown in Table 6.
Post-operative TNM staging.
Thirteen out of 26 patients had a negative COVID-19 swab pre-operatively, reflecting the change of practice at the end of April mandating pre-operative swab tests. Until this point, as testing was not available, patients were assessed on symptoms, history and exposure to risk groups.
Three out of 26 patients had inpatient post-operative COVID-19 swabs taken; in all cases this was due to pyrexia. COVID-19 was not detected in any of these three patients.
All patients were successfully contacted to complete the post-operative questionnaire. None had post-operative symptoms in keeping with COVID-19 infection including cough or temperature. Twelve out of 26 consulted a doctor for a non-COVID-19 related issue including superficial wound infection (3) constipation (1), UTI (1) and pain relief (1). None developed symptoms warranting a COVID-19 test.
Patients were asked to score pre-operative concerns about COVID-19 from 0 (no concern) to 10 (very concerned). There was considerable variability amongst the cohort with a median score of 5 (range 0–10). Patients were asked about their satisfaction with the COVID-19 precautions taken during admission from 0 (very unhappy) to 10 (very happy). Satisfaction was high with a median score of 9 out of 10. Overall feeling of safety whilst an inpatient was given a median score of 9 out of 10. All 26 patients felt it had been the correct decision to have their operation despite the COVID-19 pandemic.
Discussion
Our results indicate that during the peak of the COVID-19 pandemic we have been able to continue to provide a safe major uro-oncology surgical service. There is no evidence to suggest that any patients in this cohort went on to develop overt clinical infection with COVID-19 following their surgery. In the three cases where inpatients developed a fever in the post-operative phase, none of them tested positive for COVID-19 and they are recovered rapidly with no other symptoms typical of COVID-19. The six-day median length of stay is higher than expected for our major uro-oncology surgical service, and likely reflects the change from laparoscopic surgery to open surgery during a proportion of this period. Despite the increased length of stay, the complication rate did not differ from our pre-COVID-19 experience and compared well to published literature.8,9
The results of the post-discharge questionnaire also support our results as any COVID-19 complications acquired during admission would have expected to present by 14 days post discharge. With high levels of anxiety in the general population it is also reassuring to find that patients were satisfied with the levels of precautions taken and felt safe during their admission.
The provision of the service was heavily dependent on the critical-care department at our centre. They were able to meet the increased intensive care demands of the COVID-19 pandemic, while still having sufficient resources to provide safe anaesthetic support to allow surgery to proceed. The creation of a ‘cold’ or ‘green’ COVID-19 critical-care ward was also vital in allowing us to continue providing the service safely.
No patients who would have been a candidate for major uro-oncology surgery in the pre-COVID-19 environment were prevented from proceeding to surgery during this period at our unit. Our operative numbers for major cases were higher than the same time period in 2019 (26 v. 21 cases) and time from booking to surgery was reduced from a mean of 24 days in 2019 to a mean of 16 days in 2020.
Not all patients were swabbed prior to surgery; this, however, reflected the testing availability at the beginning of the lockdown when tests were only available for symptomatic patients. When testing capacity increased, pre-operative swabbing became mandatory at three days prior to surgery.
A recent review has summarised the various international guidelines which focus on pre-operative prioritization, pre-operative COVID-19 screening, PPE for staff and post-operative care to limit exposure to COVID-19. 10 There are currently limited published results from patients undergoing elective surgery during the COVID-19 environment. Our protocol is in line with the guideline released in May by the Royal College of Surgeons in England relating to recovery of surgical services during and after COVID-19. 11
Routine pre-operative computerised tomography (CT) scanning has not been recommended for surgical patients and was therefore not incorporated into our protocol. Intercollegiate guidance has advised CT chest for patients requiring post-operative level II/III critical care. 12 Only one patient from our cohort needed level II critical care which was due to the pre-operative diagnosis of obstructive sleep apnoea and the need for non-invasive ventilation. A pre-operative CT was not felt to be required in this case and the patient had an uncomplicated recovery.
As we have now passed the peak of the pandemic, the critical-care requirement from COVID-19 across the country is declining. This will result in the reinstatement of surgical services as resources are reallocated
Conclusion
There is limited published evidence on surgical outcomes in the UK during the COVID-19 pandemic. This case series can serve as an example that, with the appropriate precautions, surgery can be recommenced safely. It also suggests that if a further increase in COVID-19 infection rates were to occur, either locally or nationally, the provision of critical surgery could continue if appropriate steps are taken to safeguard the welfare of staff and patients.
Footnotes
Acknowledgements
We would like to thank Maurice Lau, Euan Green, Helen Doran, John Calleary and Arun Jain who were involved in the surgical procedures.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Not applicable.
Guarantor
SBM.
Contributorship
SBM conceived the paper. SS was involved in data collection and SS wrote the first draft of the manuscript. KJO, NWC and SBM edited and constructed the final manuscript