
Abstract
Intracavernous injections of vasoactive drugs, such as alprostadil, are widely used as an effective treatment method for erectile dysfunction. Intracavernous breakage of the needle is a very rare complication of self-injections, with only a few case reports available in the current literature. Treatment methods described vary in the literature, ranging from immediate surgical exploration under ultrasound guidance to non-operative management with delayed needle removal once it is easily palpable. We report a case of an 82-year-old man with a retained intracavernous 1 cm 30 gauge needle tip after injection of alprostadil (Caverject; marketing authorisation number PL 00057/0942) and the innovative use of intraoperative X-ray imaging (fluoroscopy) for removal of this.
Introduction
Intracavernous injections were first introduced in 1982 and remain a very effective treatment method in patients with erectile dysfunction resistant to first-line therapies. 1 More common complications of intracavernous injections include bleeding, infection, pain and priapism. Intracavernous breakage of the needle tip during the injection is, however, a rare complication. Only a few case reports discussing this particular complication and the methods for its removal are available in the current literature.1–5 Case reports available in the literature suggest using ultrasound guidance in order to facilitate the removal of the retained needle,1, 2 or instead performing a delayed removal of the needle, after it migrates towards the skin and is directly palpable by the operator. 3
An 82-year-old man presented out of hours to the emergency department at our tertiary referral centre in the west of Scotland, 12 hours after intracavernous injection of alprostadil (Caverject), with a retained 1 cm 30 gauge needle tip. He had complained of some discomfort in the affected area, but was otherwise asymptomatic and was passing urine freely. The patient had been successfully using intracavernous injections for 20 years with no complications prior to this.
The needle tip was not visible or palpable on clinical examination. Pelvic radiograph performed in the emergency department revealed a 1 cm length retained needle in the corpus cavernosum (Figure 1).

Retained needle tip visible in the penis on the pelvic radiograph.
We describe an innovative and, to our knowledge, previously unreported technique of using fluoroscopy (X-ray imaging) to guide removal of a retained intracavernous needle after unsuccessful attempts to achieve this with portable ultrasound guidance.
Methods and results
The patient was admitted to the urology ward and operated on the following morning. Before general anaesthetic induction, the patient himself confirmed the anticipated position of the needle. This was also confirmed by one of the surgeons (ACM) with bedside (portable) sonography and the anticipated incision site was marked. Once anaesthetised, the patient was positioned supine on the operating table, with standard preparation and draping. A vertical incision was made at the anticipated site (dorsal aspect of the inferior half of the penis). Bedside sonography was then used to try and further localise the needle, unfortunately, despite continued attempts, we were unable to grasp the needle due to migration in the soft tissues.
Input from the radiography colleagues was then sought and a C-arm image intensifier (intraoperative fluoroscopy) was brought into theatre. The retained needle tip was triangulated (surgeons AZ and ACM) using two 21 gauge needles with fluoroscopy (Figure 2 (a) and (b)). Both 21 gauge needles were inserted into the corpus cavernosum – one vertically and the other horizontally – with needle tips aimed towards the retained fragment. This allowed precise, three-dimensional localisation and identification of the retained needle tip in between the two larger needles. The retained needle tip was then successfully grasped with mosquito artery forceps after minimal dissection. Haemostasis was satisfactory and the incision was closed with absorbable (4-0 Velosorb Fast) suture. A penile block was performed to facilitate postoperative analgesia and recovery. The patient recovered well and was discharged home the following day with no follow-up required. The patient was willing to try alternative methods of treatment for his erectile dysfunction and this was arranged via his general practitioner.
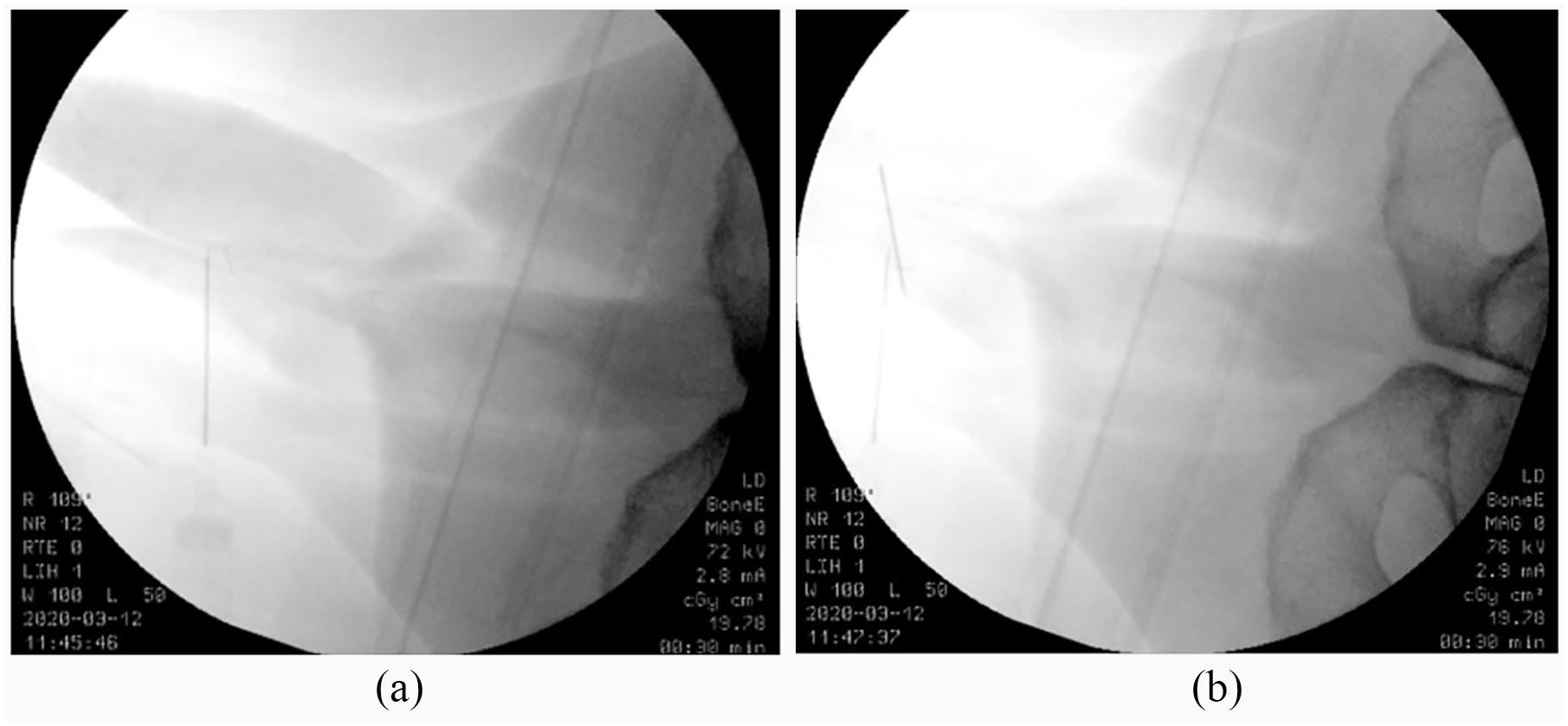
(a) Intraoperative imaging: the first 21 gauge needle placement near the retained needle tip. (b) Intraoperative imaging: triangulation of the retained needle tip with the second 21 gauge needle.
Discussion
Breakage of needle tip during intracavernous injection of erectile dysfunction drugs has been scarcely described in the literature, probably due to the rarity of this particular complication. Most previous case reports have focused on the use of sonography for localisation and removal of retained intracavernous needle,1, 2 while some advocated for a delayed retrieval. 3 No previous reports, to our knowledge, have been published on the use of fluoroscopy for localisation of retained intracavernous needle intraoperatively.
Our initial aim, as described in the methods, was to remove the retained needle fragment under ultrasound guidance. Unfortunately, the needle tip was small and excessively mobile in the soft tissues, making retrieval particularly challenging. We found fluoroscopy very useful in this case, as it allowed for an accurate triangulation of the small retained fragment, therefore easing the identification of the needle and subsequent removal with minimal dissection. This technique might continue to be useful in cases in which the retained needle fragment is particularly small and migrates through the soft tissues easily, therefore making removal under ultrasound guidance difficult.
Challenges faced intraoperatively, while using the fluoroscopy machine, included fairly poor quality and overexposed radiographic images due to the fact that we were imaging soft tissues. Positioning of the patient and the C-arm also took up a significant amount of operative time. Regardless of this, accurate triangulation and removal of the needle was achieved remarkably fast once fluoroscopy was in use. Preoperative preparation, specifically with regard to patient positioning and anticipation of possible need for the image intensifier, would help reduce the risk of delays in the future. Good communication between the surgeon and the radiographer were also essential in this case, as this is not an area of the body that is normally imaged intraoperatively.
We believe our case demonstrates a new technique of localising a retained needle tip in the corpus cavernosum intraoperatively, where other more straightforward methods (e.g. use of sonography) have failed. This fluoroscopy-guided triangulation technique will be useful for other urologists in the future, where similar circumstances (e.g. a small retained needle fragment, easily migrating through soft tissues or difficulty in achieving removal under ultrasound guidance) are encountered.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Informed consent was obtained from the patient for use of both general information in relation to the case and use of X-ray images.
Guarantor
AZ
Contributorship
Gabija Lazaraviciute is the first author and Abdullah Zreik was the supervising author. The rest of the authors contributed to the case report to a similar extent.