
Abstract

Case
A 71-year-old woman presented to our service for elective salvage cystectomy. She was diagnosed with muscle invasive urothelial carcinoma of the bladder two years prior and underwent primary chemoradiotherapy. The patient returned for review due to high volume recurrence of bladder urothelial cell carcinoma with secondary bilateral hydroureteronephrosis despite ureteric stents in situ, as well as significant pelvic pain and chronic haematuria. Her adrenal glands were noted to be normal at the time of this computed tomography (CT) scan (Figure 1). Bilateral percutaneous nephrostomy tubes were placed for initial renal tract decompression. Her other past medical history consisted of chronic renal impairment, previous pulmonary embolism and reflux. The patient was charted heparin prophylaxis 5000 IU b.i.d. from day 1 postoperatively during her admission but was on no other anticoagulants or antiplatelets.
High-volume tumour recurrence in bladder causing bilateral hydronephrosis despite bilateral ureteric stents.
She underwent a salvage cystectomy with ileal conduit formation and had an unremarkable postoperative course apart from an ileus requiring total parenteral nutrition for seven days, which resolved by day 14 postoperatively. On the night prior to discharge, the patient reported the sudden onset of bilateral flank pain, and she became hypotensive and febrile. Resuscitation with intravenous fluids and broad-spectrum intravenous antibiotics was commenced, but she remained persistently hypotensive and was transferred to the intensive care unit for vasopressive support.
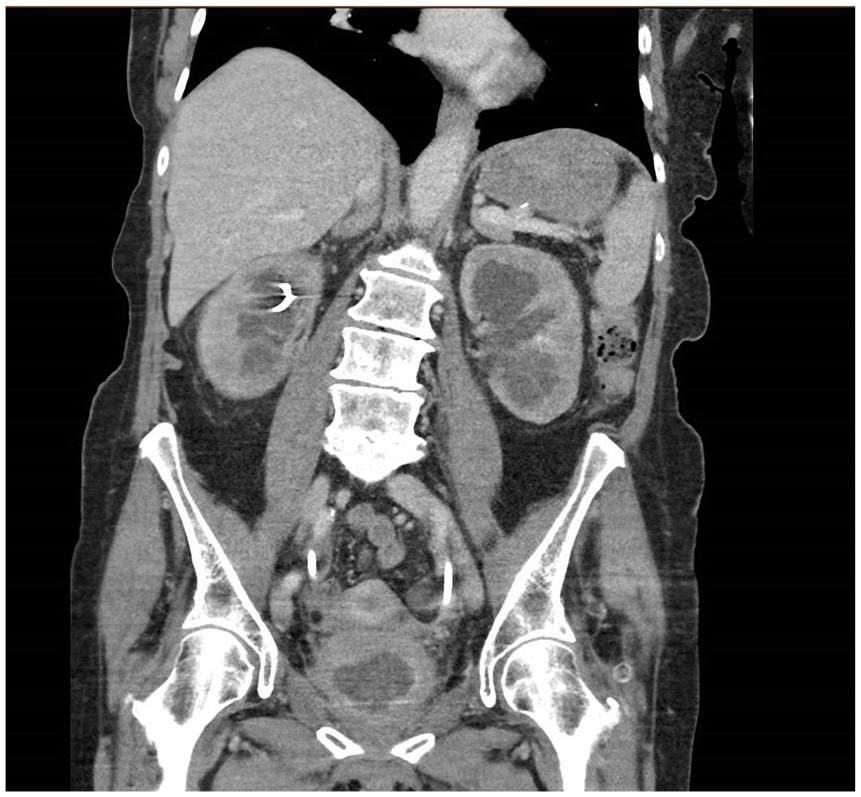
Once haemodynamic stability was achieved, she had a CT scan of her abdomen and pelvis which showed bilateral adrenal haemorrhage (Figures 2 and 3). Her serum cortisol level was critically low at 69 nmol/L (range 200–650 nmol/L morning peak) without any classic electrolyte disturbance or hypoglycaemia. All blood and urine cultures were negative for organisms.

Coronal view of bilateral adrenal haemorrhage (arrows) on computed tomography (CT) scan post salvage cystectomy.
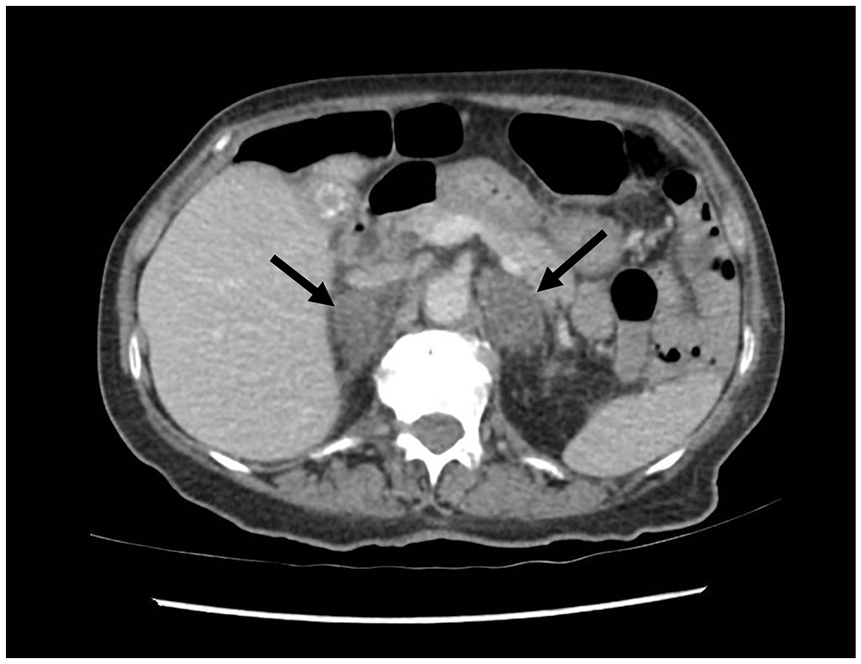
Axial view of bilateral adrenal haemorrhage (arrows) on CT.
She was reviewed by the endocrine team and commenced on intravenous hydrocortisone stress dosing initially, 100 mg every six hours.
Following initiation of corticosteroids, she became normotensive and remained clinically well. During her inpatient stay, she was weaned daily to 50 mg every six hours, then 20 mg every eight hours, then 20 mg orally every 12 hours which she was discharged on (three days later). She did not respond to attempts to down-titrate corticosteroid therapy at her last outpatient endocrine review and was likely to require it indefinitely. She has since died from presumed progressive metastatic disease.
Discussion
Atraumatic bilateral adrenal haemorrhage resulting in adrenal insufficiency is rare, particularly in the postoperative setting. It has a high mortality rate (it has been estimated that adrenal haemorrhage may be present in 15% of individuals who die of shock). However, it is often not recognised early due to its rarity and due to symptoms being contributed to other postoperative complications.1–4 It is characterised by non-specific symptoms – abdominal pain, nausea/vomiting and confusion, hypoglycaemia and electrolyte disturbance (classically hyponatraemia and hyperkalaemia), progressing to shock with profound hypotension.5,6 Therefore, it is important to have a high index of suspicion in order to ensure adequate investigation, and it remains an important differential diagnosis of postoperative shock.
Spontaneous adrenal haemorrhage can be precipitated by septicaemia (Waterhouse–Friderichsen syndrome), gastrointestinal perforation, adrenal tumours, abdominal malignancy or intracranial pathology, coagulopathy, trauma (including burns) and shock.1,2,3–5,7,8 As a postoperative complication, it often occurs within 7–14 days following major surgery; it is unlikely to occur following minor surgery.5,7 One case series of 12 patients describing spontaneous postoperative adrenal haemorrhage reported that eight of these patients had surgery on the gastrointestinal tract or biliary system, and two on the genitourinary tract (a trans-urethral resection of bladder tumour complicated by bladder perforation, and a trans-urethral resection of the prostate with severe postoperative haemorrhage and massive transfusion). 2 Interestingly, in the case we have presented, the cystectomy was performed without any significant intra- or perioperative complications.
Infection (sepsis or pneumonia) and coagulopathies were cited as notable risk factors, but in each case, it was clearly evident that the patients were subjected to severe stress. Overall, it has been estimated that 50% of bilateral adrenal haemorrhage cases occur in the context of an acute stressful illness.2,8 Prompt diagnosis can be made with a non-contrast CT scan of the abdomen. Adrenal haemorrhage is characterised by an ovoid or round mass at the adrenal gland.3–5 Adrenocorticotropic hormone/basal cortisol levels in the acute setting can confirm adrenal insufficiency. 6 Treatment involves corticosteroid replacement. For the haemodynamically unstable patient with suspected ongoing bleeding, angioembolisation or open adrenalectomy can be considered.3,7
Atraumatic adrenal haemorrhage and acute adrenal insufficiency is a rare but important differential diagnosis of shock in the postoperative period (especially in the context of significant morbidity or acute stress). Prompt recognition and timely investigation with imaging (confirmed by serum results) is important, as it carries a high mortality rate unless treated with corticosteroid replacement. This case has prompted our service to have a low threshold for investigation for adrenal haemorrhage as a differential diagnosis in the postoperative shocked patient with poor response to resuscitation.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Informed consent was obtained from the patient.
Guarantor
A.T.
Contributorship
K.L. completed the literature review and drafted the manuscript. A.M. provided critical review and editing. A.T. oversaw the patient case and edited the final version of the manuscript.