
Abstract
Objective:
This study aimed to determine the effect of template transperineal (TTP) compared to transrectal (TR) biopsy on surgical and functional outcomes after robotic-assisted radical prostatectomy (RARP).
Methods:
From 2014 to 2018, 280 patients underwent RARP by a single surgeon. Of these, 184 had TR, and 96 had TTP biopsy. Primary outcomes were continence and erectile function recovery (EFR) rates up to 24 months postoperatively. Secondary outcomes comprised positive margin rates and markers of a difficult operation, including operative time, estimated blood loss (EBL), urethral preservation quality and ability to perform planned nerve-sparing surgery.
Results:
The median age was greater in the TTP group (64 vs. 62 years, p=0.028). The proportions of men with preoperative erectile dysfunction and men undergoing nerve-sparing surgery were not different between groups. Operative time, EBL, urethral preservation quality, proportion of men undergoing intended nerve-sparing procedure, positive margin rates and continence recovery rates were not different among the groups. At 24 months, men in the TR group had a higher EFR rate on univariate analysis (p=0.036), and multivariate analysis (p=0.03).
Conclusion:
TTP biopsy was not associated with markers of a more difficult RARP or worse oncological and continence recovery outcomes but did appear to impact upon long-term rates of EFR.
Level of evidence:
Level 4.
Introduction
Prostate cancer is the most common non-cutaneous cancer in men in many parts of the world.1,2 Prostate biopsy remains the cornerstone of diagnosis. 3 Historical transrectal (TR) prostate biopsy is associated with significant false-negative rates due to under-sampling of anterior and apical segments of the prostate, 4 which in some areas has resulted in the widespread adoption of transperineal template prostate (TTP) biopsy. TTP ‘mapping’ biopsies are typically reserved either for patients with previous negative investigations (multi-parametric magnetic resonance imaging of prostate (mp-MRI) or TR biopsies) and an ongoing suspicion of prostate cancer, or as confirmatory biopsy to avoid misclassification in men with low-risk prostate cancer. 5
TTP biopsies are usually performed under general anaesthesia and have been shown to have higher cancer detection rates 6 and lower sepsis rates compared to TR biopsies.7,8 This is at the expense of higher urinary retention rates following TTP biopsies. 9 They are also associated with significant rates of periprostatic fibrosis on radical prostatectomy specimens. 10 As a result, some clinicians have raised concerns that TTP biopsy may render radical prostatectomy more difficult and adversely affect functional outcomes, although evidence to support such a hypothesis is conflicting.10–14 One factor lacking from all of the published studies to date is long-term functional follow-up. Previous studies have shown that spontaneous recovery of continence can occur up to 12 months following prostatectomy, 15 and recovery of erectile function up to 24 months postoperatively.16,17 Therefore, the purpose of this study was to determine if TTP biopsy adversely affects long-term functional outcomes up to 24 months after robotic-assisted radical prostatectomy (RARP).
Methods
Patients receiving RARP were identified from a prospectively maintained single-surgeon database. The surgeon was experienced and beyond his learning curve at the initiation of this study. Patients were divided into two groups: those receiving TR biopsy for primary diagnosis, and those who received TTP biopsy, either for primary diagnosis or as a confirmatory biopsy during active surveillance. All TR biopsies were performed using a standard 12-core technique. TTP biopsies were performed using a Hitachi Arietta V70 transperineal probe (Hitachi Medical Systems, Wellingborough, UK) and Classic STEPPER™ device (CIVCO, Kalona, IA) according to a previously published novel 10-sector template. 18 Systematic biopsies were taken using a Bard Max-Core™ 18G needle directed at 5 mm intervals via a standard brachytherapy grid. Targeted biopsies were not performed.
Clinicopathological data were collected prospectively and included age, prostate biopsy technique, preoperative prostate-specific antigen (PSA), biopsy tumour grade, MRI findings, clinical stage, American Society of Anesthesiologist (ASA) grade, body mass index (BMI), history of abdominal surgery, history of transurethral resection of prostate (TURP) or bladder neck incision (BNI), preoperative erectile dysfunction (ED), preoperative nerve-spare intention, total operative time, console time, estimated blood loss (EBL), nerve-spare quality (rated on a scale from 1 to 5 as per Schatloff et al. 19 ), urethra preservation quality (rated on a Likert scale of 1 to 5; 5=100%, 4=75%, 3=50%, 2=25%, 1=0%), extended pelvic lymph node dissection status, surgeon assessment of dissection difficulty, length of stay, length of urethral catheterisation, pathological findings (weight, grade, stage, extra-prostatic extension, seminal vesical invasion), positive surgical margin (PSM), Sexual Health Inventory For Men (SHIM) score, number of continence pads used per day and the insertion rate of artificial urinary sphincter. Assessment of surgical difficulty, urethral preservation quality and nerve-spare quality was recorded prospectively by the operating surgeon immediately following completion of each RARP.
Functional outcomes were assessed at six weeks and at 3, 6, 9, 12, 18 and 24 months following surgery. Continence recovery was defined as absolute pad usage (0 pads, 1 pad, >1 pad), and erectile function recovery (EFR) was defined as SHIM ⩾17 for each time point.20,21
Secondary outcomes comprised PSM rates and intraoperative markers of a difficult operation, including total operative time, console time, EBL, surgeon-rated subjective difficulty of operation, urethral preservation quality and ability to complete planned nerve-sparing surgery.
Statistical analyses were performed using Stata v16 (StataCorp LLC, College Station, TX). Median values were compared using the Wilcoxon rank-sum test. Proportions between groups were compared using the chi-square test or Fisher’s exact test. Multivariate analysis using multiple logistic regression was used to determine if biopsy group was an independent predictor of EFR, taking into account known predictors, including age, preoperative erectile function and nerve-spare status. 22
Formal ethics approval for this study was not required, as the data were collected as a part of the routine standard audit conducted by our institution on prostatectomy patients. This study conformed to the provisions of the Declaration of Helsinki (as revised in 2013). 23
Results
Baseline demographics and disease characteristics
From February 2014 to May 2018, 281 consecutive patients underwent RARP by a single surgeon. Of these, 184 received TR biopsy (two on active surveillance), and 96 received TTP biopsy (50 on active surveillance). One patient was diagnosed with prostate cancer following TURP and was therefore excluded from the study. Baseline demographics and disease characteristics for each group are shown in Table 1. Patients in the TTP biopsy group were older (median age 64 vs. 62 years, p=0.028) and had a higher ASA score (grade 2 vs. grade 1; p=0.001). There were no statistically significant differences in preoperative PSA, International Society of Urological Pathology (ISUP) grade group and clinical T stage between the groups to suggest higher risk disease as a likely confounding factor for more difficult RARP. Similarly, the distribution of pathological ISUP grade group following RARP was not different between the groups. However, on histopathology, men in the TR group had a higher proportion of T3 disease (34.2% vs. 17.7%, p=0.004) and extra-prostatic extension (34.8% vs. 16.7%, p=0.001) compared to the TTP group. Factors that may contribute to a more difficult RARP, including BMI, prostate volume, history of abdominal surgery and previous TURP or BNI, were not different between the two groups. The proportion of patients with preoperative ED and the number of patients planned for nerve-sparing surgery – both known risk factors for postoperative ED – was also similar among the groups.
Comparison of baseline demographics and disease characteristics between men who had TR versus TTP biopsy prior to RARP.
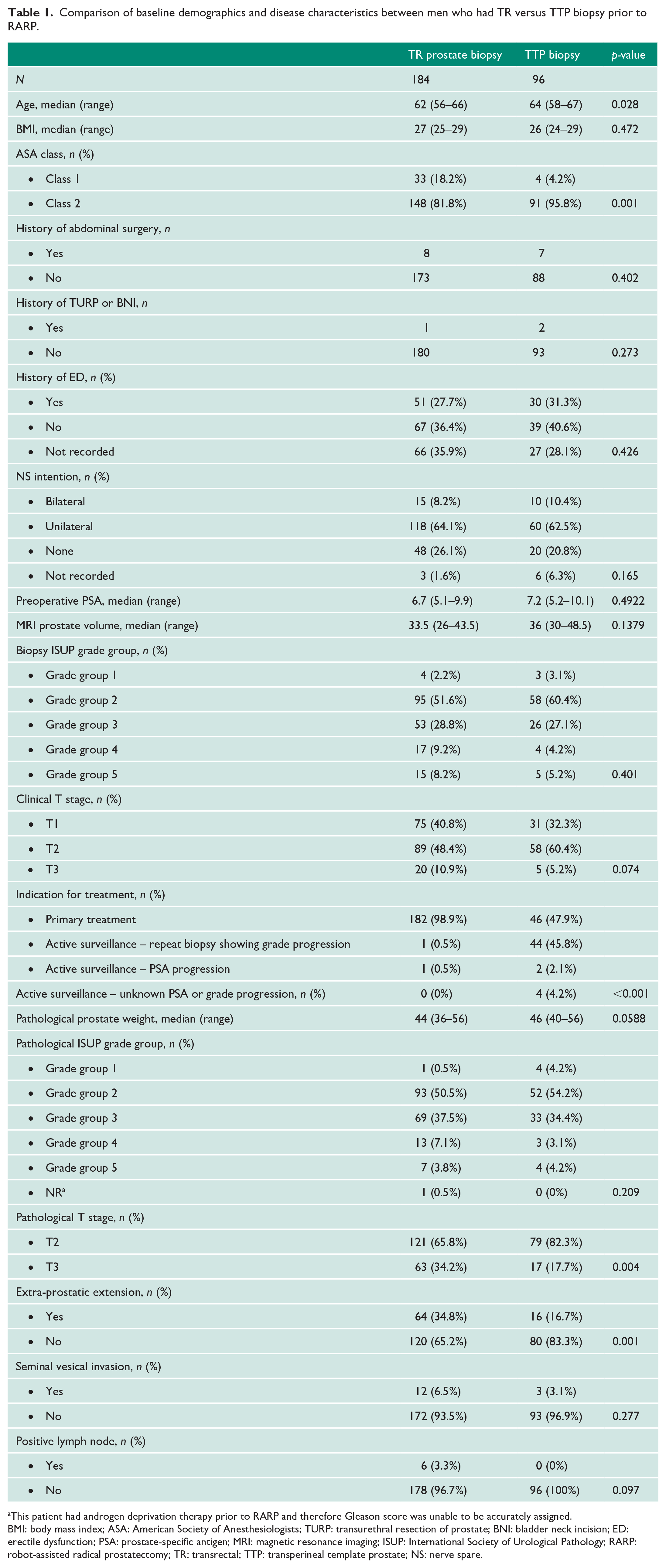
This patient had androgen deprivation therapy prior to RARP and therefore Gleason score was unable to be accurately assigned.
BMI: body mass index; ASA: American Society of Anesthesiologists; TURP: transurethral resection of prostate; BNI: bladder neck incision; ED: erectile dysfunction; PSA: prostate-specific antigen; MRI: magnetic resonance imaging; ISUP: International Society of Urological Pathology; RARP: robot-assisted radical prostatectomy; TR: transrectal; TTP: transperineal template prostate; NS: nerve spare.
Number of biopsy cores and TTP core density
The median number of TR biopsy cores was 12. The median total number of cores taken at TTP biopsy was 42 (interquartile range (IQR) 31–54). The median cores per millilitre of prostate gland was 1.1 (IQR 0.9–1.5).
Continence recovery
There was no difference in the median pad count or proportion of patients who were pad free between the groups of men at any time frame from six weeks to 24 months (Figure 1). The response rate of questionnaire at each of the time frame ranged from 79.2% to 86.1%. At 24 months, the rate of artificial urinary sphincter insertion was not statistically different between the TR group and the TTP group (2.3% vs. 0%, p=0.553).
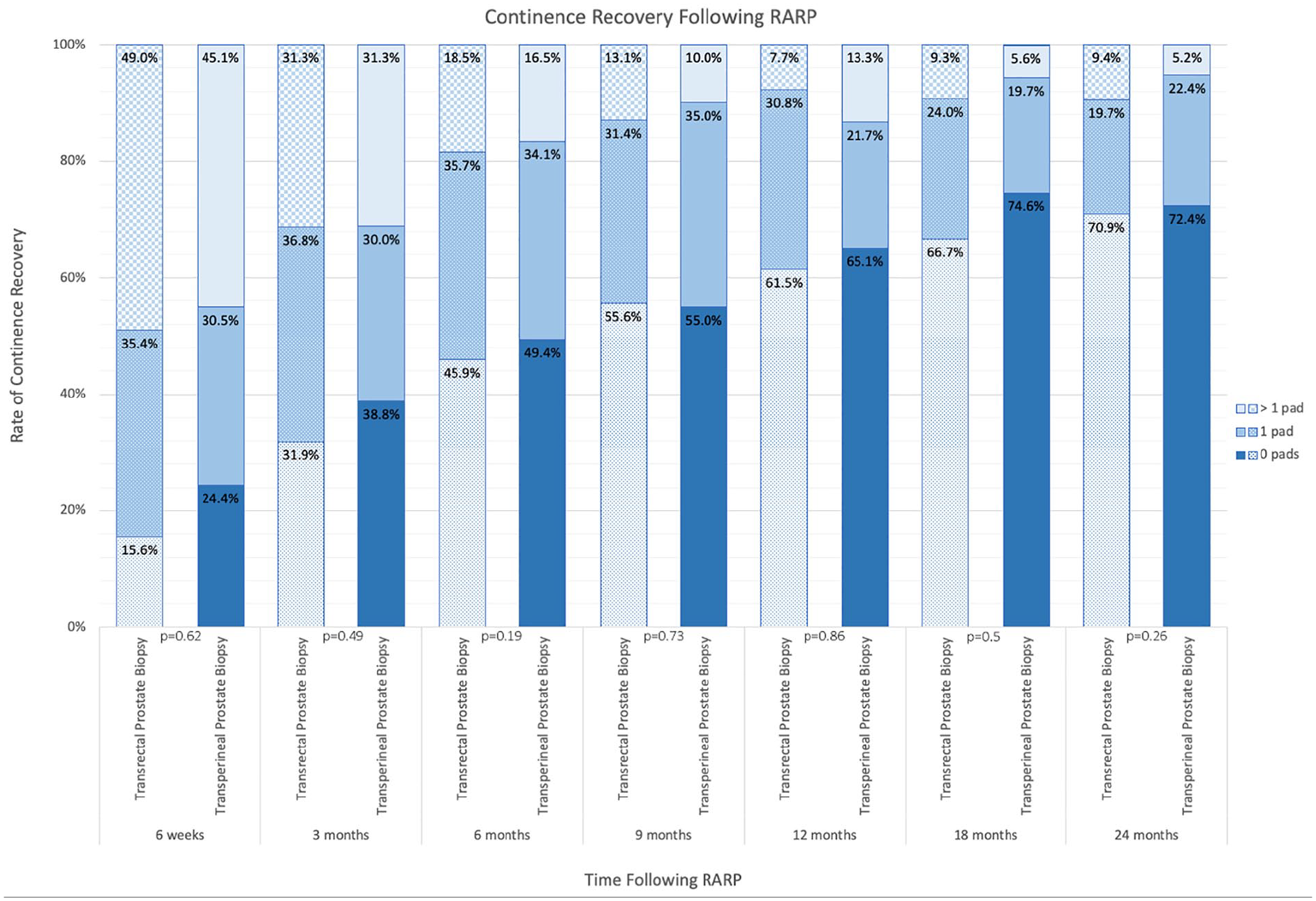
Comparison of continence recovery rates for men who had transrectal (TR) versus transperineal template prostate (TTP) biopsy prior to robot-assisted radical prostatectomy (RARP).
EFR
The rate of EFR as determined by SHIM score at 3–24 months is shown in Figure 2. The response rate of the questionnaire at each of the time frames was 63.7%, 70.5%, 68.7%, 64.4%, 59.5% and 53.0%, respectively. At 24 months following RARP, men who received TR biopsy had a higher rate of EFR compared to men who received TTP biopsy (32.9% vs. 12.0%, p=0.036). Biopsy group remained a predictor of EFR at 24 months on multivariate analysis, taking into account age, preoperative ED status and nerve-spare grade (Table 2).
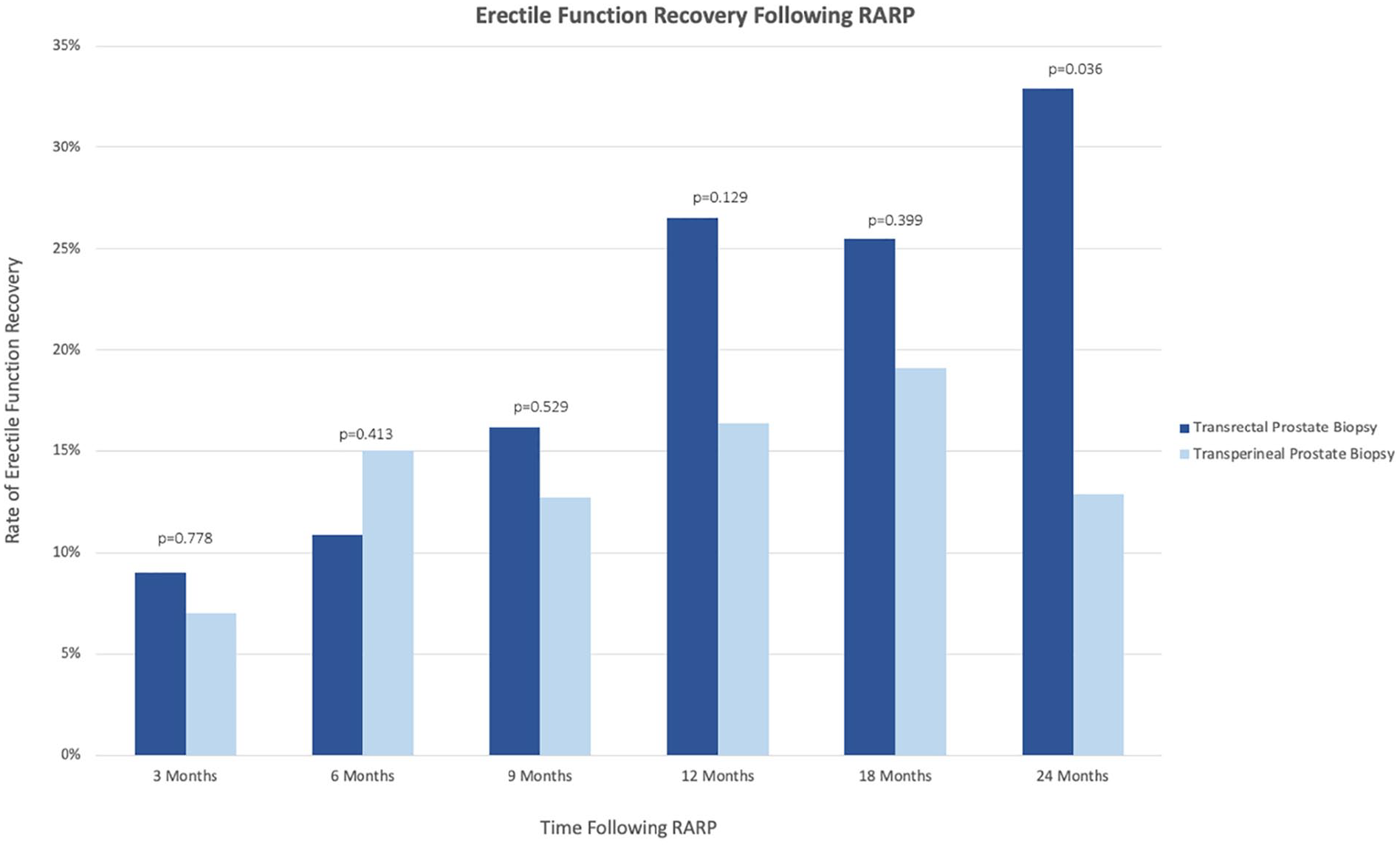
Comparison of rates of erectile function recovery defined as Sexual Health Inventory for Men score of 17–25 for men who had TR versus TTP biopsy prior to RARP.
Multiple logistic regression analysis for factors affecting erectile function recovery following RARP.
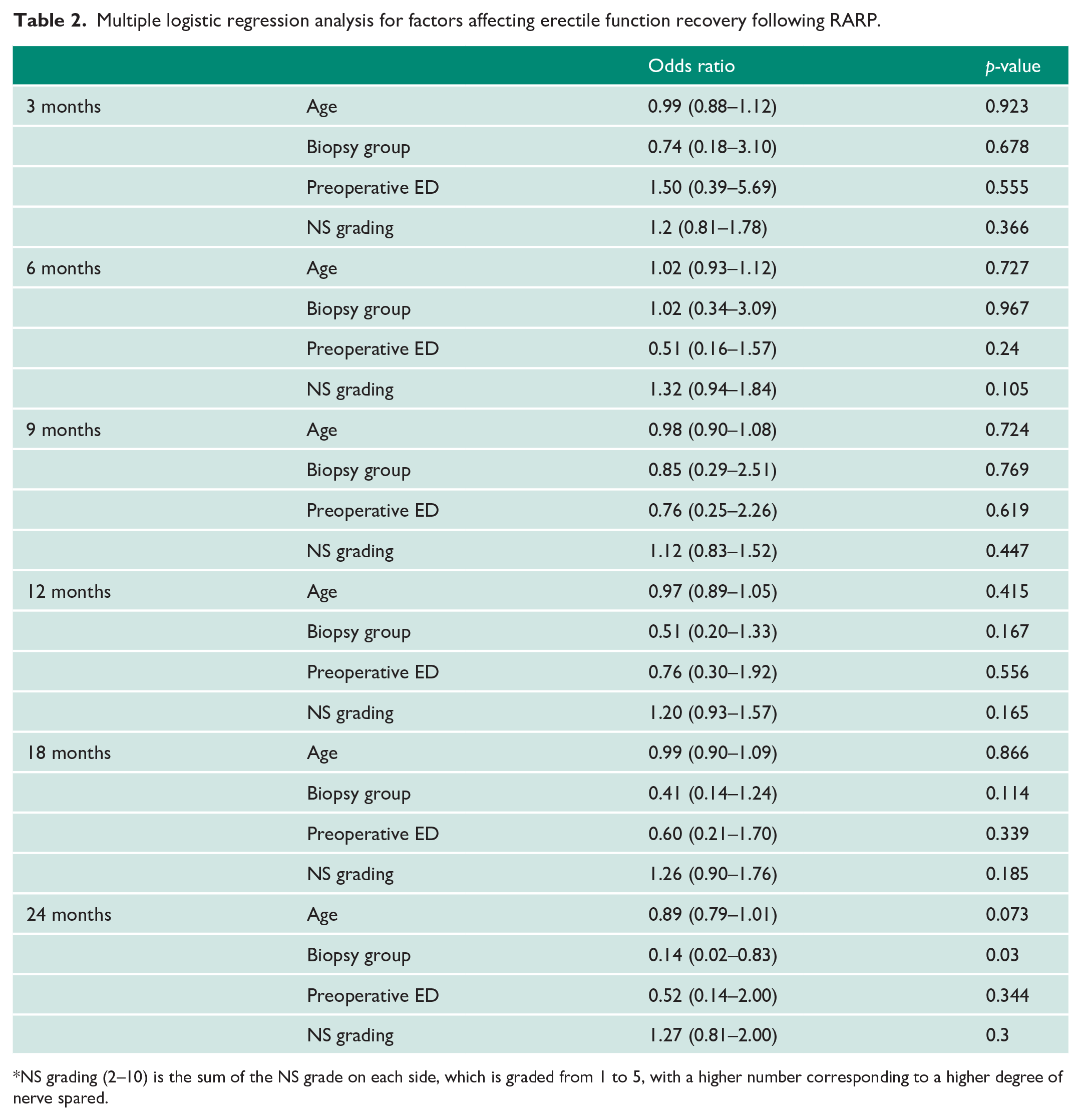
NS grading (2–10) is the sum of the NS grade on each side, which is graded from 1 to 5, with a higher number corresponding to a higher degree of nerve spared.
Oncological outcome
PSM rate was not different between men in the TR group versus those in the TTP group (21.2% vs. 21.9%, p=0.895). On subgroup analysis of T2 and T3 disease, there remained no difference in the PSM rate between the two groups.
Intraoperative and postoperative surgical outcomes
Comparative intraoperative and postoperative surgical outcomes for each group are shown in Table 3. The proportion of RARPs with documented difficult dissection was higher for men in the TTP group for pathological T2 but not T3 disease. Despite this finding, operative times, EBL, intraoperative surgeon-rated urethral preservation quality and ability to complete planned nerve-sparing surgery was not different between the groups.
Comparison of intraoperative and postoperative surgical outcomes between men who had TR versus TTP biopsy prior to RARP.
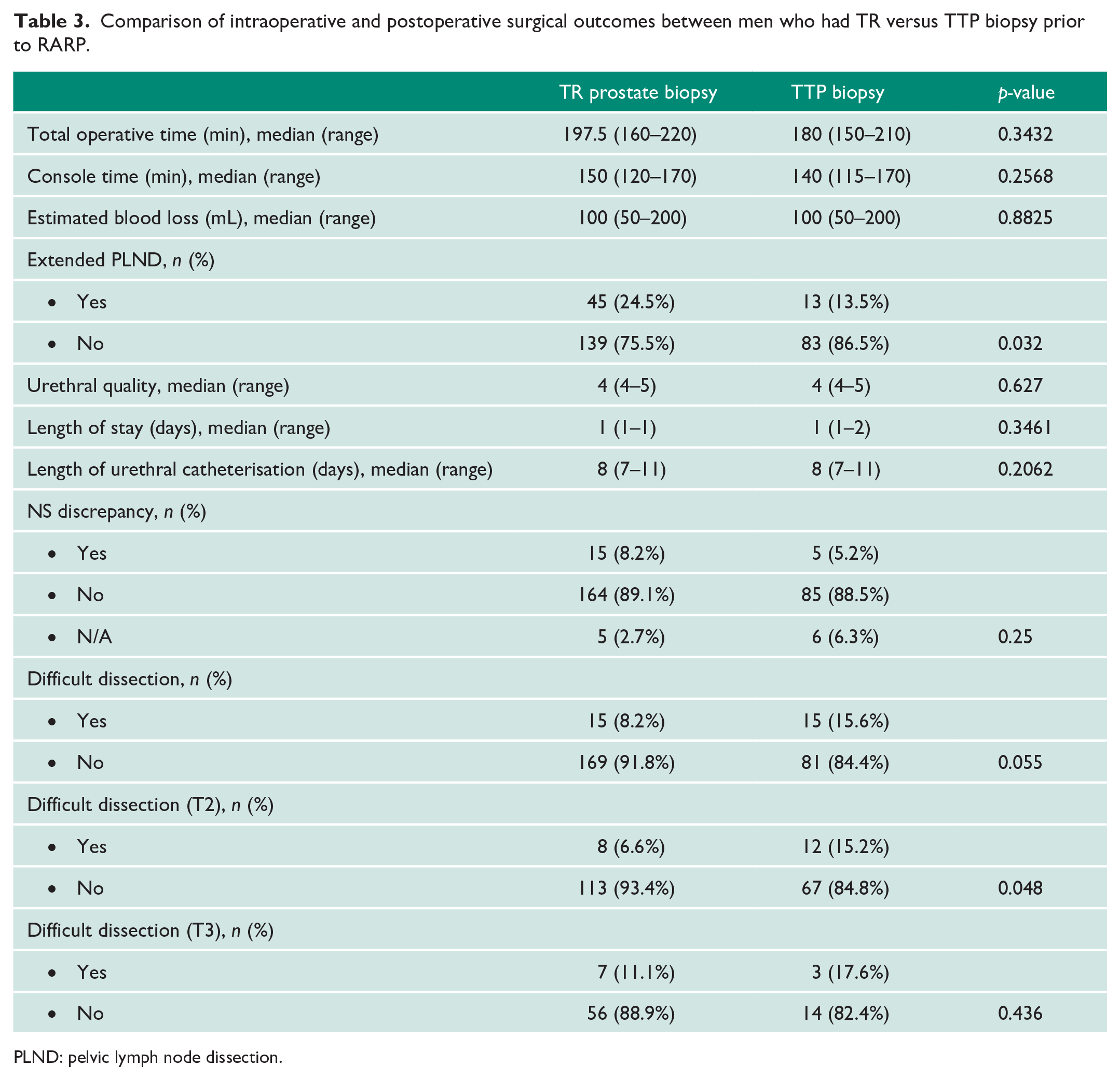
PLND: pelvic lymph node dissection.
Discussion
Previous studies analysing the effect of TTP biopsy on perioperative and functional outcomes have provided conflicting results.10–14 Barzell et al. reported the effect of TTP biopsy on fibrosis encountered intraoperatively, and found that extensive fibrosis was present in 57% of patients, which made preservation of one or both neurovascular bundles (NVB) unachievable. 10 Most of the patients in this study received TR and TTP biopsy concomitantly, which may have adversely affected the amount of fibrosis compared to TTP biopsy alone. 10 In contrast, Huo et al. reported successful intraoperative nerve-sparing surgery following TTP biopsy, despite the presence of a similar degree of fibrosis at radical prostatectomy, and Dimmen et al. reported no difficulties in RARP following TTP biopsies.13,14 The largest study on this topic previously by Wadhwa et al. which retrospectively compared outcomes after transrectal and transperineal biopsies in 181 men from a single institution, of whom 61 received transperineal biopsy, with a median of 27 harvested cores. They found no difference in perioperative complications and oncological and functional outcomes between the groups. However, the study has several limitations. First, it was a retrospectively study with no prospective record of surgical perception of difficulty or nerve-spare quality. Second, follow-up for functional outcomes was limited to only six months, which may not be long enough to assess recovery of continence and erectile function adequately, as multiple studies have shown that continence recovery can take up to 12 months 15 and erectile function up to 24 months16,17 following radical prostatectomy. Third, the number of patients in the transperineal group was relatively small, which may have limited interpretation of the findings.
In the study presented herein, we report comparative perioperative and functional outcomes for 280 men receiving TR and TTP biopsy, of whom 96 underwent TTP biopsy. In contrast to Wadwha et al., single-surgeon data were used, ensuring that preoperative preparation, nerve-spare intention and operative technique was standardised, thus limiting confounding. In addition, data were harvested from a prospectively maintained database which included immediate postoperative surgeon assessment of nerve-spare quality, urethral preservation and overall difficulty, reducing retrospective bias. Regarding the question of whether TTP biopsy leads to a more difficult radical prostatectomy, we found that subjective perception of increased surgical difficulty was more common in the TTP group with organ-confined disease, but not for T3 disease, although the numbers in each group were small, and care should be taken in the interpretation of the results. Irrespective, in accordance with previous studies, we did not find that nerve-sparing surgery was significantly impaired by the increased difficulty of the operation.11,13,14 Furthermore, there was no difference between the groups in terms of perioperative, oncological and short-term functional outcomes, suggesting that whilst RARP after transperineal biopsy may have been subjectively more difficult from a surgeon’s perspective, this difficulty did not translate into clinically meaningful impaired outcomes.
To our knowledge, this is the first study to compare long-term functional outcomes for RARP after transrectal versus transperineal biopsy. Whilst there was no difference in continence rates between the two groups, we found significantly reduced erectile function in the transperineal group at 24 months. One explanation for this finding is that transperineal biopsy itself contributed to the degree of erectile dysfunction. Certainly, TTP is associated with postoperative impairment of erectile function,24–26 although it is usually temporary and typically recovers within six months. 24 In addition, Garcia et al. showed that TTP biopsy does not impact on erectile function compared to TR biopsy at least in the medium term up to six months. 27 Another possible explanation is that the higher median age in the transperineal group contributed to the findings. However, there was only a small age difference, and the biopsy group remained a predictor of EFR on multivariate analysis accounting for age. Another explanation is that periprostatic fibrosis caused by transperineal biopsy results in impaired nerve-spare quality, leading to reduced long-term EFR. Whilst nerve-sparing completion rates were similar and surgeon perception of nerve-spare quality was no different among the groups (data not shown), it is possible that the degree of intraoperative trauma caused during nerve sparing may have been greater in the transperineal group due to tethering of the NVB. A further consideration is that the transperineal biopsy technique in this trial may have contributed to the observed findings. We utilised a ‘template mapping’ technique, performing biopsies every 5 mm, resulting in a median core number of 42, which is higher than that reported in previous studies.11–14 It is therefore conceivable that a higher than average degree of periprostatic fibrosis may have contributed to the reduced EFR in the TTP group.
This study has several limitations. First, this study is a retrospective analysis of comparative outcomes, and as such is subject to the recognised bias and confounding associated with such studies. A second limitation is that some data fields were incompletely captured prospectively and were therefore supplemented by retrospective review of the medical record. Finally, this is a single-surgeon study, and care must be taken when extrapolating the data. Further multicentre prospective study with baseline and follow-up patient reported outcome measure data to confirm the findings of this study is warranted.
Conclusion
High core density TTP biopsy, as compared to conventional TR prostate biopsy, is associated with increased surgeon perception of surgical difficulty but not with objective markers of a more difficult RARP. Oncological and long-term continence outcomes are also unaffected. EFR at 24 months appears to be impaired in men receiving TTP biopsy, despite reported adequacy of intraoperative nerve sparing. The reasons for the association remain to be fully elucidated.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for the present study because the data were collected as a part of the routine standard audit conducted by our institution on prostatectomy patients. This study was completed in accordance with the Declaration of Helsinki as revised in 2013.
Informed consent
Informed consent was not sought for the present study because the data were collected as a part of the routine standard audit conducted by our institution on prostatectomy patients.
Guarantor
T.J.W.
Contributorship
H.H.Y. and T.J.W. conceived and designed the study. T.J.W., K.B. and A.B. were responsible for data acquisition. H.H.Y., T.J.W., A.B. and T.R.T. undertook the data analysis and interpretation. H.H.Y. and T.J.W. drafted the manuscript. K.B., A.B. and T.R.T. were responsible for the critical revision of the manuscript. T.J.W. and T.R.T supervised the study.