
Abstract
Objective:
We aimed to evaluate the role of intra-tumoral CXCR1 expression in predicting prognosis and treatment response in metastatic clear-cell renal cell carcinoma patients receiving tyrosine kinase inhibitors.
Materials and methods:
Patients with metastatic clear-cell renal cell carcinoma presented between February 2018–December 2019 were studied for the CXCR1 expression in tumor tissues before starting tyrosine kinase inhibitors. Primary outcome measure was progression-free survival. Secondary outcome measures included overall survival and prediction of treatment response.
Results:
The study included 35 patients with a mean age of 53.6±9.6 years. At a mean follow-up of 12.2±4.1 months, 17 (48.6%) patients had disease progression including eight (22.9%) deaths. Patients with high CXCR1 expression, compared to those with low CXCR1 expression, had a significantly shorter 12-month progression-free survival (35.4% vs 77.9%, p=0.01) and an insignificant impact on 12-month overall survival. The CXCR1 expression scores significantly differed between patients with progressive and nonprogressive disease (20.1 vs 15.1, p=0.01) and patients with high CXCR1 expression had a reduced benefit from tyrosine kinase inhibitors. The multivariate Cox regression analysis showed CXCR1 expression as a significant predictor of progression-free survival.
Conclusion:
High intra-tumoral CXCR1 expression before tyrosine kinase inhibitors can be an independent prognostic factor for progression-free survival and predictor of reduced benefit in patients with metastatic clear-cell renal cell carcinoma.
Level of evidence:
Level 2b.
Introduction
About a third of renal cell carcinoma (RCC) patients have metastasis at the time of initial presentation. 1 The therapeutic options of metastatic renal cell carcinoma have been drastically expanded from several anti-angiogenic agents to novel immune checkpoint inhibitors. 2 However, the selection and sequence of various agents has been a difficult task for clinicians. Various biomarkers were explored by researchers, not only in prognosticating the disease, but also to predict and guide treatment selection. 3
In this line of study, the immunohistochemistry (IHC) of intracellular cell signaling receptors has been explored as a potential biomarker in RCC. One such marker, C-X-C motif chemokine receptor 1 (CXCR1) in tumor tissues has been evaluated in in-vitro and retrospective studies.4,5 However, prospective studies evaluating the role of CXCR1 are lacking. This study aims to evaluate the prognostic and predictive role of intra-tumoral CXCR1 expression in patients receiving tyrosine kinase inhibitors (TKIs) for metastatic clear-cell renal cell carcinoma (mCRCC).
Materials and methods
Study design
This prospective study was conducted at a single tertiary care center between February 2018–December 2019 after institutional ethical committee approval (reference number: IEC/366/6/2018). Patients presenting with synchronous or metachronous mCRCC before the initiation of TKIs were included in the study. Exclusion criteria were non-clear cell histology and a prior use of targeted therapy for mCRCC. Patients with sarcomatoid or rhabdoid differentiation were also excluded. All of the patients had Eastern Cooperative Oncology Group (ECOG) scores of 0–2 and provided written informed consent.
Outcomes analyzed
The primary outcome measure was progression-free survival (PFS), defined as the period between date of TKI initiation and the date of the first documentation of disease progression or death. The secondary outcome measures included overall survival (OS) and prediction of treatment response to TKIs.
A dedicated genitourinary radiologist blinded to the clinical details of the patients interpreted the cross-sectional images using Response Evaluation Criteria in Solid Tumors (RECIST 1.1) and classified each assessment as a complete response, partial response, stable disease or progressive disease (PD). 6 Patients with complete response, partial response and stable disease were categorized as nonprogressive disease (NPD) whereas those with progressive disease or death were categorized as PD.
Work-up of patients and surgical procedures
All of the patients were evaluated with routine blood investigations. The primary tumor size and metastatic burden were evaluated with contrast-enhanced computerized tomography (CECT) or magnetic resonance imaging scans of the chest, abdomen and pelvis and 18 F-fluoro-2-deoxy-D-glucose-positron emission tomography/CT (FDG-PET/CT). The FDG-PET/CT was performed at baseline and every 12 weeks after initiating the treatment. Patients fit for surgery underwent either laparoscopic or open cytoreductive nephrectomy (CRN) at the discretion of the surgeon. Unfit patients underwent renal mass biopsy (RMB) in order to know the histopathology and CXCR1 expression. A genitourinary pathologist confirmed the histological type and nuclear grade of all the patients based on World Health Organization (WHO)/International Society of Urological Pathology (ISUP) nuclear grading system. 7 In patients presenting with metachronous metastasis, histopathology slides of the radical nephrectomy (RN) specimen were reviewed and used for immunostaining. The 8th edition American Joint Committee on Cancer was used for tumor, nodes and metastases (TNM) staging and the International Metastatic RCC Database Consortium (IMDC) model was used for risk group stratification.8,9
CXCR1 expression and scoring
Two cores of tumor tissues were obtained from each specimen. The primary CXCR1 antibody (1:200 dilution, R&D Systems, Minneapolis, USA) was used for IHC staining. Heat-induced epitope retrieval techniques were used for antigen retrieval. Horseradish peroxidase- 3, 3’ diaminobenzedine (HRP-DAB) Cell and Tissue Staining Kits (R&D Systems, Minneapolis, USA) were used for chromogenic staining. The pathologist evaluated the CXCR1 expression according to immunoreactivity score (IRS) algorithm mentioned previously. 10 The CXCR1 expression was categorized into low and high CXCR1 expression, if the mean IRS scores were <15 and ⩾15, respectively. 10
Statistical analysis
The continuous variables were compared using Student’s t-test or Mann Whitney U-test, and the categorical variables were compared using the Pearson’s Chi-square test or Fisher’s exact test. Survival curves were constructed by Kaplan-Meier estimates and compared with the use of log-rank test. Cox proportional-hazards regression analysis was performed to estimate univariate and multivariate hazard ratios (HRs) for PFS and OS. A p-value of <0.05 was considered as statistically significant. All statistical analysis were performed using Stata, version 14.0 (StataCorp, College Station, Texas, USA).
Results
Baseline characteristics
A total of 35 patients were enrolled during the study period and their baseline characteristics are summarized in Table 1. The mean age was 53.6±9.6 years and 62.9% were men. Synchronous and metachronous metastases were seen in 77.1% and 22.9%, respectively. In this cohort, 54.2%, 22.9%, and 22.9% underwent CRN, RN, and RMB, respectively. The average tumor size was 10.7±3.6 cm and the majority (91.4%) had multifocal metastasis. Patients with high CXCR1 expression had a higher tumor diameter than low CXCR1 patients (11.9±3.7 vs 9.09±2.7, p=0.02).
Baseline characteristics.
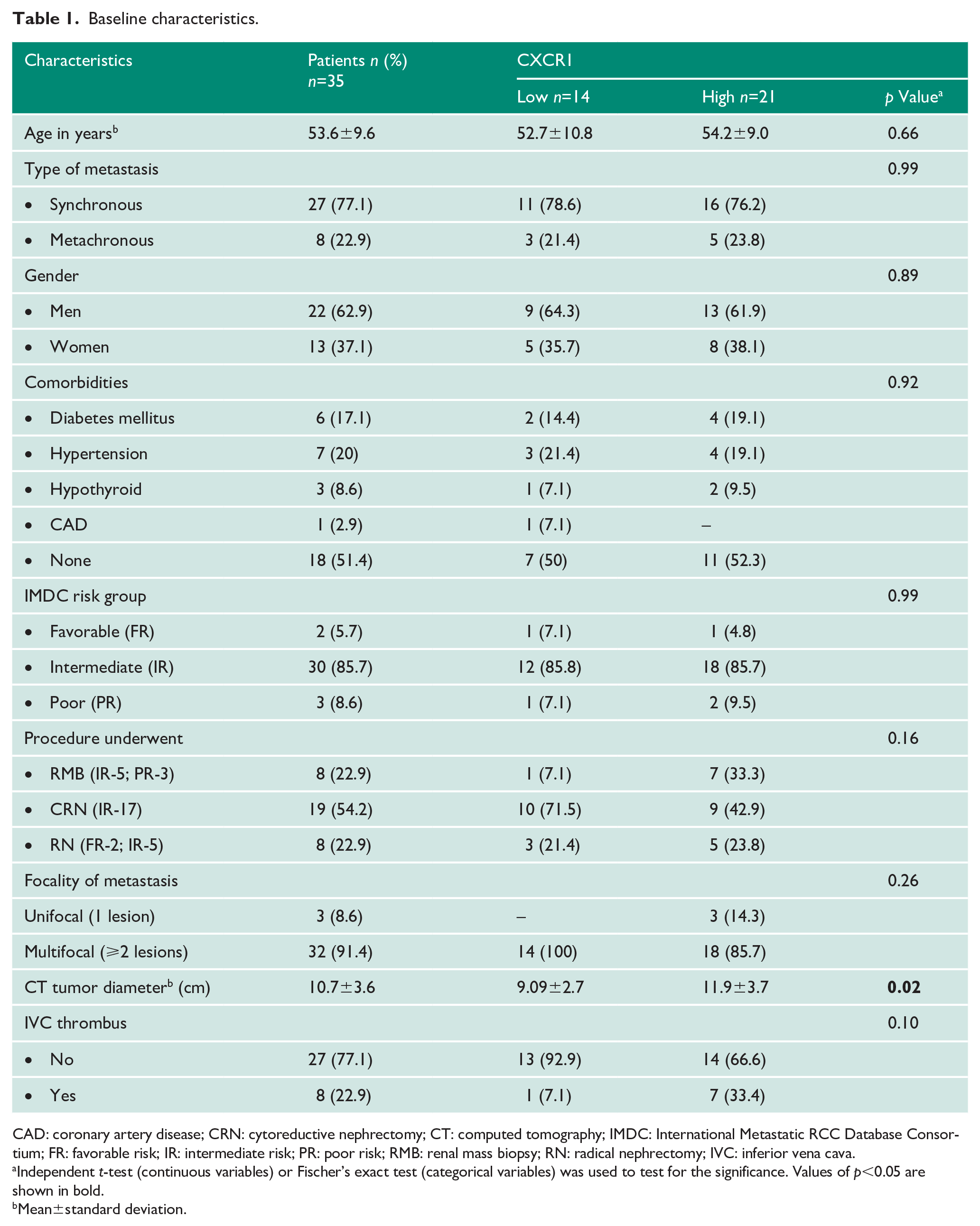
CAD: coronary artery disease; CRN: cytoreductive nephrectomy; CT: computed tomography; IMDC: International Metastatic RCC Database Consortium; FR: favorable risk; IR: intermediate risk; PR: poor risk; RMB: renal mass biopsy; RN: radical nephrectomy; IVC: inferior vena cava.
Independent t-test (continuous variables) or Fischer’s exact test (categorical variables) was used to test for the significance. Values of p<0.05 are shown in bold.
Mean±standard deviation.
Pathological and oncological outcomes
Sixteen (45.7%) and 19 (54.3%) patients had a low and high WHO nuclear grade, respectively. All the patients received either pazopanib (91.4%) or sunitinib (8.6%) as TKI therapy. At a mean follow-up of 12.4±4.1 months, 77.1% (27/35) of the cohort were alive and 22.9% (8/35) succumbed to the disease. Disease progression was seen in 17 (48.6%) patients including eight deaths.
Role of intra-tumoral CXCR1 expression
The CXCR1 expression was categorized into low (Figure 1(a)) and high CXCR1 (Figure 1(b)) expression as shown in the IHC image. Low and high CXCR1 expression of the primary RCC specimens were seen in 40% (14/35) and 60% (21/35) patients.
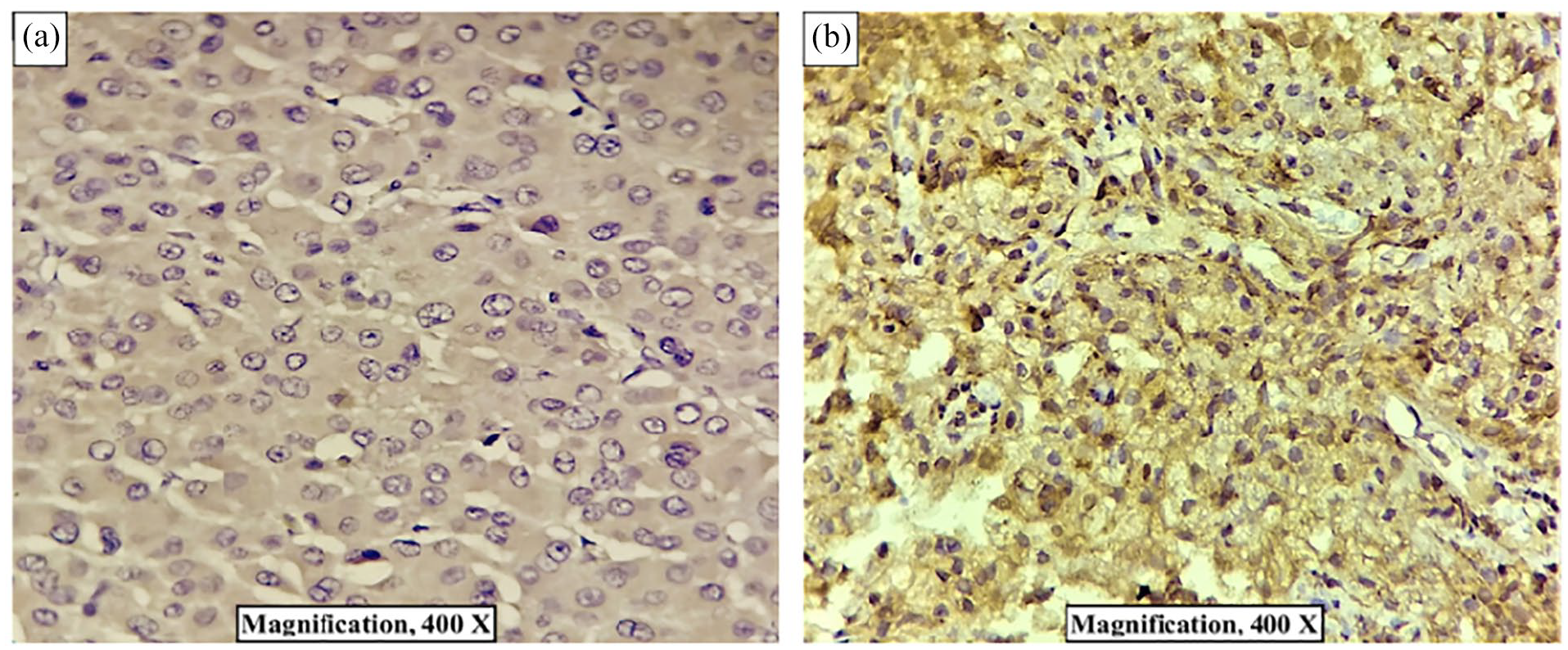
CXCR1 expression.
CXCR1 as a prognostic biomarker
Patients with high CXCR1 expression had a significantly shorter 12-month PFS (35.4% vs 77.9%, p=0.01; Figure 2(a)) as compared to patients with low CXCR1 expression. Although the estimated 12-month OS in patients with high CXCR1 expression was shorter than low CXCR1 patients, the difference was statistically insignificant (70.6% and 85.1%, p=0.31; Figure 2(b)).
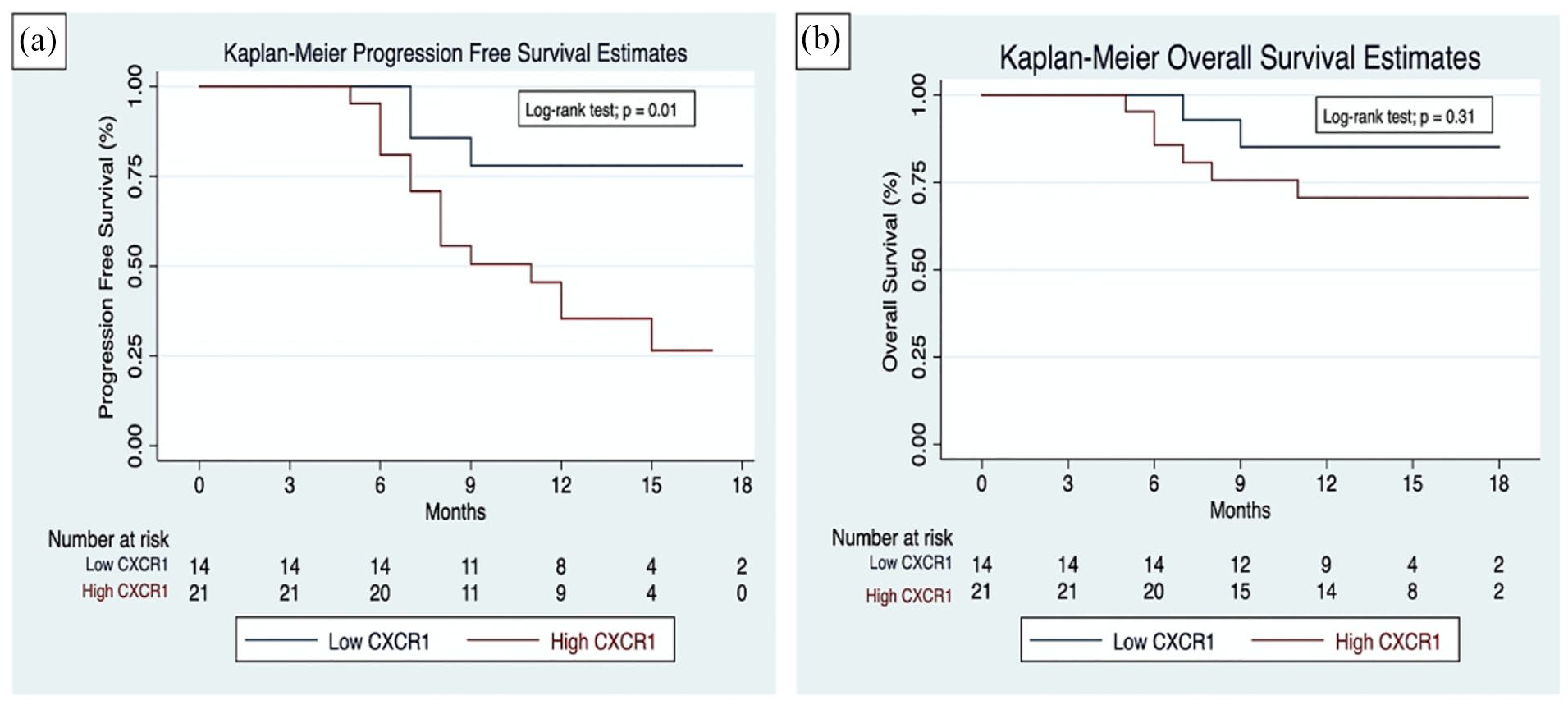
Kaplan-Meier survival curves showing: (a) progression-free survival rates between low and high CXCR1 expression patients; (b) overall survival rates between low and high CXCR1 expression patients.
CXCR1 as a predictive biomarker
A significantly higher CXCR1 expression score was noted in patients with PD than patients with NPD (20.1 vs 15.1, p=0.01; Figure 3). Further, patients with high CXCR1 expression had a higher disease progression while on TKIs as compared to the patients with low CXCR1 expression (66.7% vs 21.4%, p=0.01; Table 2).
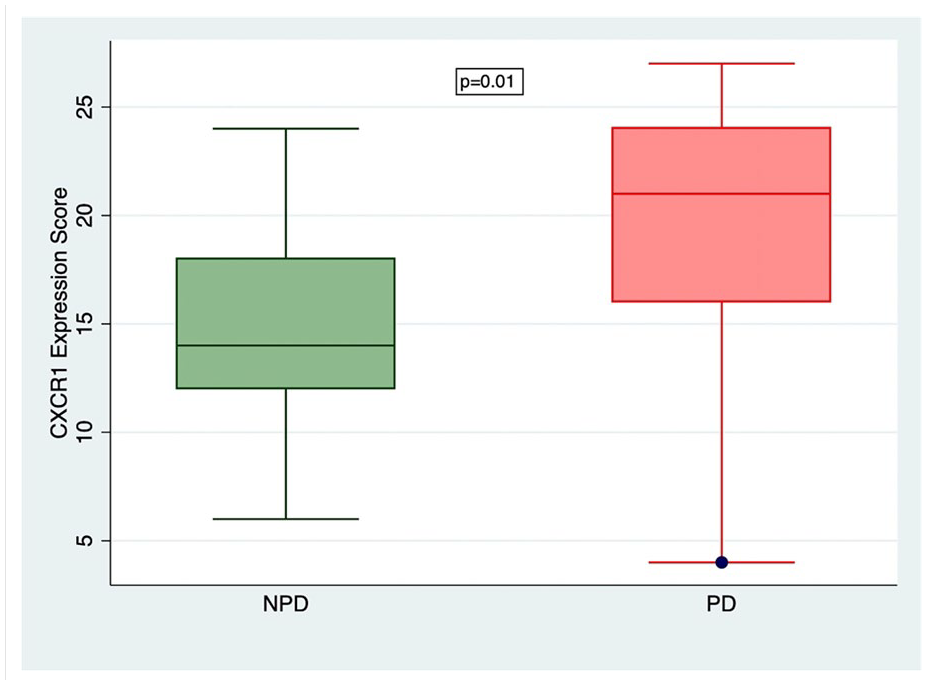
Comparison of CXCR1 expression scores between nonprogressive disease (NPD) and progressive disease (PD).
Role of intra-tumoral CXCR1 expression in predicting treatment response.
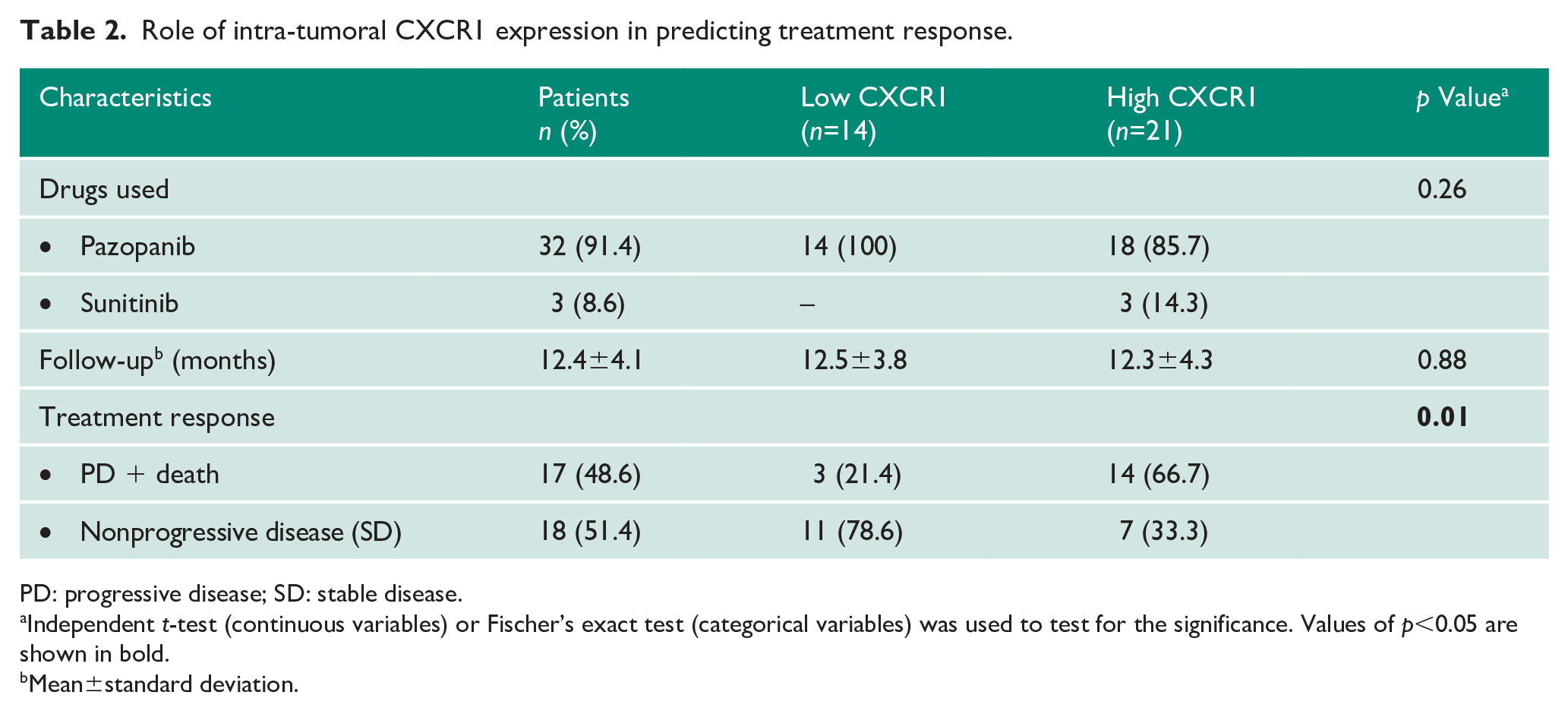
PD: progressive disease; SD: stable disease.
Independent t-test (continuous variables) or Fischer’s exact test (categorical variables) was used to test for the significance. Values of p<0.05 are shown in bold.
Mean±standard deviation.
Cox regression analysis of variables predicting PFS and OS
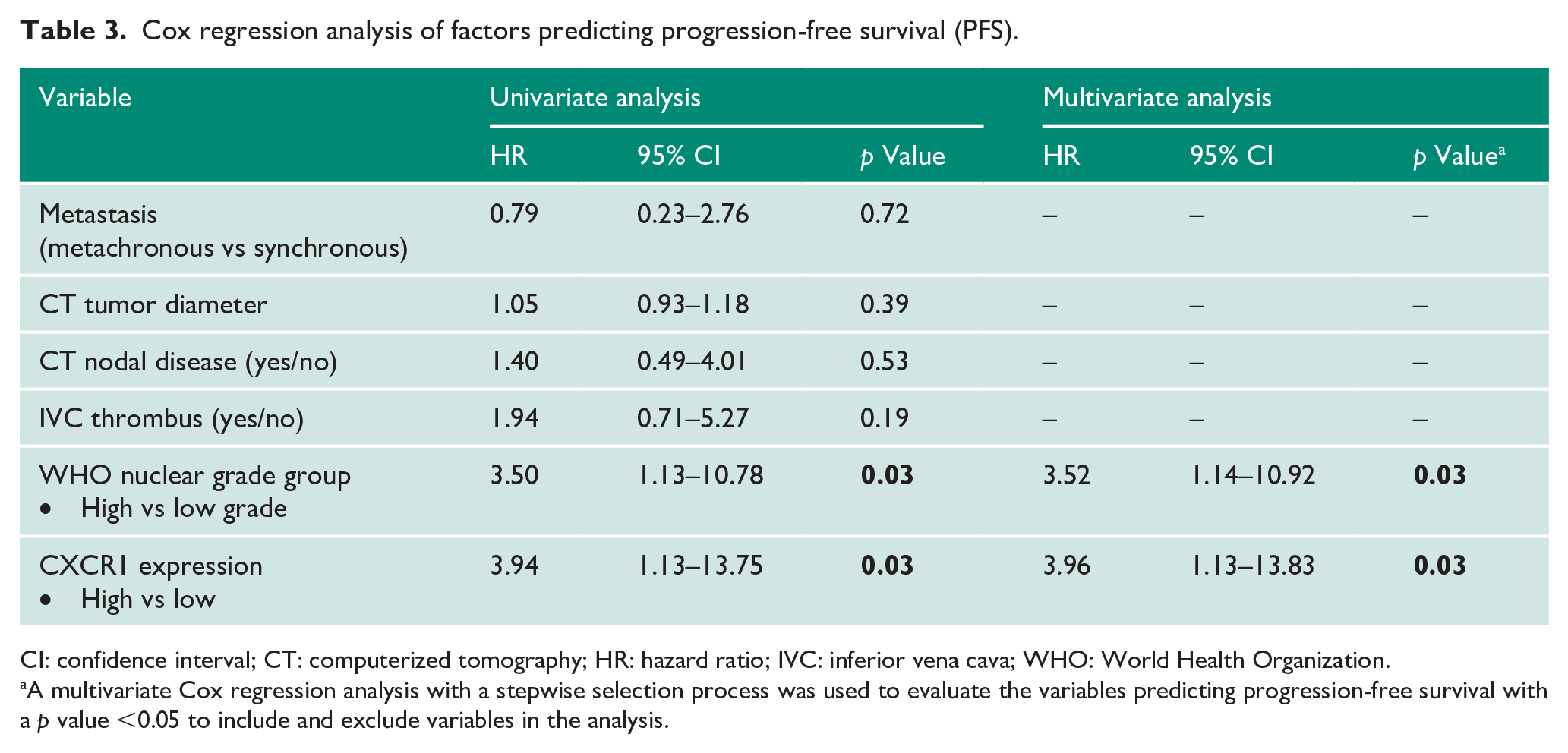
The univariate analysis showed WHO nuclear grades (p=0.03) and CXCR1 expression (p=0.03) were the factors possibly associated with PFS. Further, a multivariate Cox regression analysis with a stepwise selection process with a stringency level p<0.05, revealed CXCR1 expression (HR 3.96, 95% confidence interval 1.13–13.83, p=0.03) to be the most independent factor predictive of PFS (Table 3). However, none of the variables assessed in the model significantly predicted OS (Table 4).
Cox regression analysis of factors predicting progression-free survival (PFS).
CI: confidence interval; CT: computerized tomography; HR: hazard ratio; IVC: inferior vena cava; WHO: World Health Organization.
A multivariate Cox regression analysis with a stepwise selection process was used to evaluate the variables predicting progression-free survival with a p value <0.05 to include and exclude variables in the analysis.
Univariate Cox regression analysis of factors predicting overall survival (OS).

CI: confidence interval; CT: computerized tomography; HR: hazard ratio; IVC: inferior vena cava; WHO: World Health Organization.
Discussion
The better understanding of tumorigenesis in recent years has rapidly expanded the range of therapeutic agents for mCRCC. Despite various agents being available, the optimal selection and sequence of drugs are lacking. Biomarkers may help clinicians to prognosticate the disease as well as to predict and guide treatment selection. 3
The present study indicated that intra-tumoral CXCR1 expression is a useful prognostic marker of PFS in mCRCC. Also, a high CXCR1 expression predicted the poor response to TKIs. In a multivariate Cox regression analysis, CXCR1 expression was found to be the most significant predictor of PFS.
CXCR1 is a G-protein-coupled receptor which, when activated by its ligand interleukin-8 (IL-8), results in intracellular signaling leading to neutrophil recruitment. IL-8/CXCR1 signaling was found to promote angiogenesis, tumorigenesis, and metastasis in many solid tumors. 11 CXCR1 also reported inducing the growth of RCC. Tumors with CXCR1 expression are found to have resistance to chemotherapy or targeted agents.12,13 The enriched pathways of hypoxia and angiogenesis in CXCR1-expressing tumors were hypothesized to contribute to a poor response to agents targeting angiogenesis. 10 CXCR1 found on endothelial cells and neutrophils also hindered the anti-angiogenic agents. 5 With a potential target for newer agents, only a few studies have evaluated CXCR1 in RCC.14,15
Zhu et al. demonstrated CXCR1 expression mainly within the epithelial area rather than the stromal region of RCC. In their retrospective analysis of non-metastatic RCC patients, high CXCR1 expression indicated poor OS and recurrence-free survival. 5 Chen et al. showed high CXCR1 expression in metastatic RCC was associated with poor OS (p=0.015) but insignificant impact on PFS (p=0.261). 10 In contrast, we found high CXCR1 expression significantly associated with poor PFS with insignificant impact on the OS. This discrepancy may relate to the inclusion of more synchronous (78.1%) and multifocal metastasis (93.7%) in our cohort, compared with only 54% and 30%, respectively, in their study. 10
High CXCR1 expression with inherent resistance to anti-angiogenic agents influenced few researchers to develop new agents targeting CXCR1. Grepin et al. studied the CXCL7 axis as a potent target for the treatment of clear-cell RCC. In a mice model, agent (SB225002) inhibiting CXCL7 receptors (CXCR1 and CXCR2) affected both the tumor vasculature and the proliferation of tumor cells. 14 Another animal study by Dufies et al., showed compound C29 targeting the CXCR1 axis exerted an anti-proliferation or survival activity on a panel of cancer cells including naive and resistant RCC cells. 15
In the present study, patients with high CXCR1 expression had a poor response to TKIs and the CXCR1 expression scores were significantly higher in patients with PD than NPD. This is in agreement with Chen et al. since they showed a poorer therapeutic response to TKIs (p=0.017) with high CXCR1 expression. 5
To the best of our knowledge, this is the first prospective study to evaluate the role of CXCR1 expression as a prognostic and predictive marker in mCRCC. Our study results may instigate future studies on the role of anti-CXCR1 agents in mCRCC. The other strength of our study was, in contrast to previous studies, that we exclusively included clear-cell type mRCC excluding other confounding histological features like sarcomatoid or rhabdoid differentiation which may affect the prognosis. The study is limited by the heterogenous inclusion of metachronous and synchronous mCRCC patients which may influence the ability to generalize the results to one group. While this heterogeneity may affect the prognosis, treatment response prediction is unlikely to be affected as we evaluated the CXCR1 before starting TKIs. Further, at the start of the study pazopanib and sunitinib were the preferred first-line therapy for any IMDC risk category patients. 16 Though recently immune checkpoint inhibitors with nivolumab plus ipilimumab combination is the recommended first-line therapy in intermediate and poor risk categories, 17 we do not believe it invalidates the data presented herein, as pazopanib and sunitinib are still recommended as optional first-line therapies. Moreover, worldwide, TKIs are still used as front-line therapy in view of their low cost as compared to the newer agents.
Recently Zheng et al. developed a novel nomogram incorporating eight clinical factors like Fuhrman grade, lymph node status, sarcomatoid features, cancer-directed surgery, bone, brain, liver and lung metastases for accurate prediction of overall survival of patients with metastatic RCC. 18 Intratumoral CXCR1 expression on IHC can be incorporated as an additional factor to this nomogram to enhance the prediction of OS rates. However, this needs further validation in future studies.
Overall, the results of our study may provide a rationale for CXCR1 to be considered as a potential prognostic and predictive biomarker in mCRCC patients starting on TKIs. Finally, prospective studies exploring the role of CXCR1 expression in patients starting on immune checkpoint inhibitors are warranted.
Conclusions
To conclude, our study results demonstrated that before the start of TKI therapy in mCRCC, high intra-tumoral CXCR1 expression was found to be an independent prognostic factor for PFS and predicted a reduced benefit with TKIs. This imparts the role of CXCR1 expression as a potential biomarker in mCRCC patients considering TKI therapy.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the institute ‘Intramural Research Grant’ (project number A-621) from the research section of the All India Institute of Medical Sciences, New Delhi, India.
Ethical approval
The present study protocol was reviewed and approved by the Institutional Review Board of All India Institute of Medical Sciences, New Delhi, India (approval number: IEC/366/6/2018).
Informed consent
All patients gave informed written consent to be included in the study.
Guarantor
BN.
Contributorship
BN, SP, SKau and SKar reviewed the literature and planned the study. SP, BN, SKau, and SKar were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. SP wrote the first draft of the manuscript. BN, PS, and AS contributed important intellectual content to the manuscript and data interpretation. All authors reviewed, edited, and approved the final version of the manuscript.