
Abstract
Purpose:
The purpose of this study was to have an accurate estimate about the sexual function of sickle cell disease adult men with previous history of recurrent attacks of ischemic priapism in childhood. We assessed the studies for their precise documentation for the erectile function in this group of patients.
Materials and methods:
We performed a systematic review of the literature by querying PubMed, Medline, and Cochrane. We included original studies on adult patients with sickle cell disease and history of ischemic priapism.
Results:
We identified 15,057 publications, of which 10 met the study inclusion criteria. The incidence of erectile dysfunction was reported up to 69.20% in one study.
Conclusion:
More extended prospective studies are required as multicenter studies to find the exact incidence of erectile dysfunction in men with sickle cell disease and priapism.
Level of evidence:
Level of evidence is not applicable for this systematic review.
Introduction
Priapism is the condition of partially or completely erect penis which is not associated with sexual stimulation and persists for 4 h and more beyond that stimulation. 1 Ischemic priapism is regarded as an emergency condition and delay in evaluating and treating this condition can lead to ischemic necrosis and complete loss of the function of penile tissues. 2 Ischemic priapism accounts for 63% of all cases of priapism in children with sickle cell disease (SCD). It is the main etiology in 23% of adult cases of priapism with a lifetime chance of having ischemic priapism reaching up to 29–42% in SCD men.3,4 More than 70% of SCD patients who have a history of severe priapism have a history of stuttering priapism. 5 A number of factors contribute to the development of priapism in SCD patients including low-flow state, anatomical factors, and decreased penile venous nitrous oxide (NO) concentration which results in vasoconstriction, reduced blood flow, reduced oxygen saturation, and development of sickling. 6 Stuttering priapism is seen in patients with SCD with prevalence rates of 40%. 4 Priapism may have devastating sequelae on the sexual function of men if not treated appropriately. Regardless of the type of treatment of priapism, recurrence of the condition is quite common due to the chronic nature of SCD.
The aim of the study is to assess the outcome of sexual state in adolescent and adult sicklers who experienced attacks of priapism in childhood.
Methodology
This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement guidelines (http://prisma-statement.org/) (Figure 1).
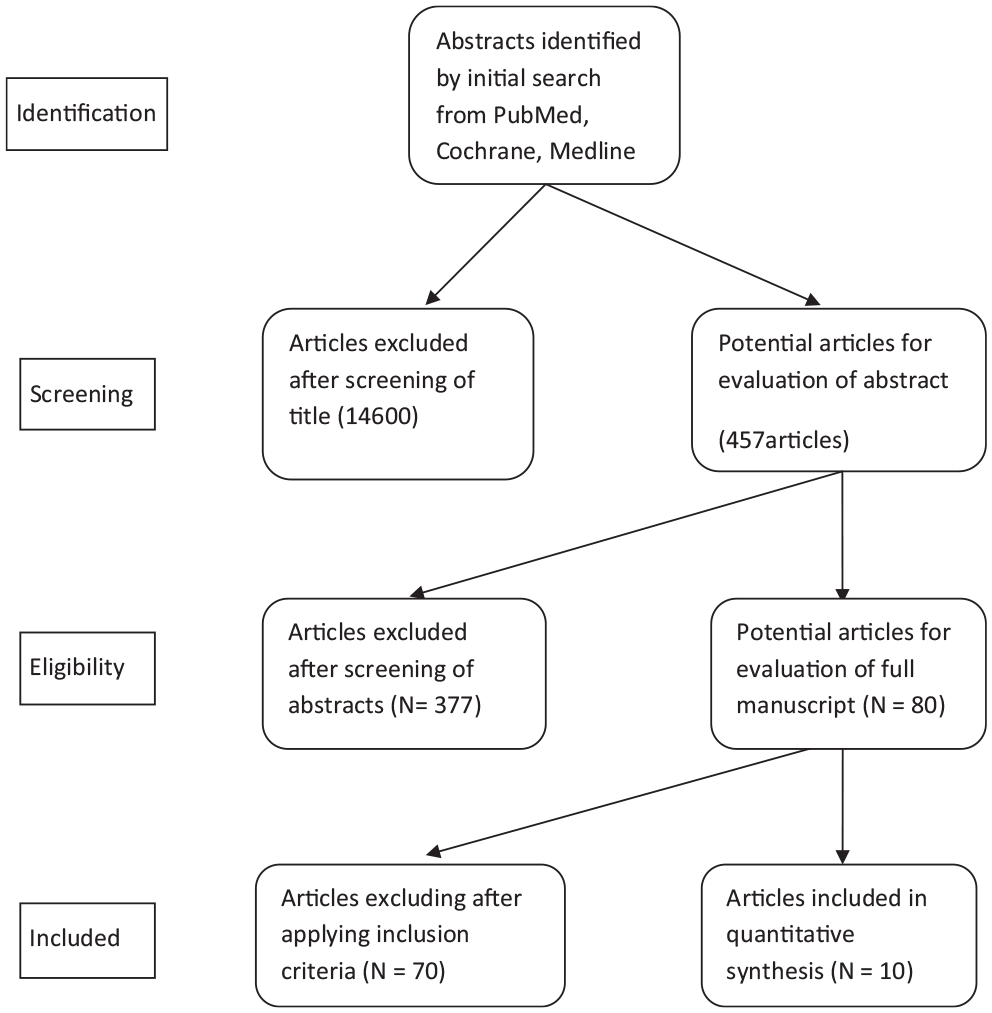
Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram.
Systematic search strategy
We performed comprehensive electronic searches for English language publications which were referenced in PubMed, Cochrane, and Medline from 1980–2018. We used relevant terms including “sickle cell disease,” “ischemic priapism,” and “erectile dysfunction.” The study retrieved 75 abstracts.
Evidence acquisition
The abstracts were reviewed by two independent teams to select those for full manuscript review. The criteria for the selected manuscripts included English language, peer-reviewed, retrospective, and prospective studies. Studies that only discussed the impact of priapism in sicklers on sexual function at adolescent and adulthood were included in this systematic review. Studies and abstracts which were not reported in English or discussed other aspects of priapism, were not included in the study. Also abstracts without full-text publications were excluded. A total of 10 abstracts met the inclusion criteria of the study and were selected for full text review.
Results
Study selection
An initial search using the relevant search terms revealed 15,057 titles. After narrowing the search field to meet the inclusion criteria, a total of 457 titles was obtained. When focusing on articles that discussed the development of erectile dysfunction (ED) in SCD men with a history of priapism, only 80 articles were identified. Ten articles studied the development of ED related directly to ischemic priapism in SCD men and were selected for full review.
The included 10 articles were retrospective and prospective articles that evaluated the sexual function of men with SCD and episodes of ischemic priapism. The number of patients who were included in all the studies was 301. The mean age of patients included in the study reached up to 30.5±1.63 years. The follow-up of patients was variable in the studies; the maximum follow-up was 21.9±4.1 weeks. The incidence of ED was reported up to 69.20% in one study (Table 1).
Descriptive statistics of included articles.
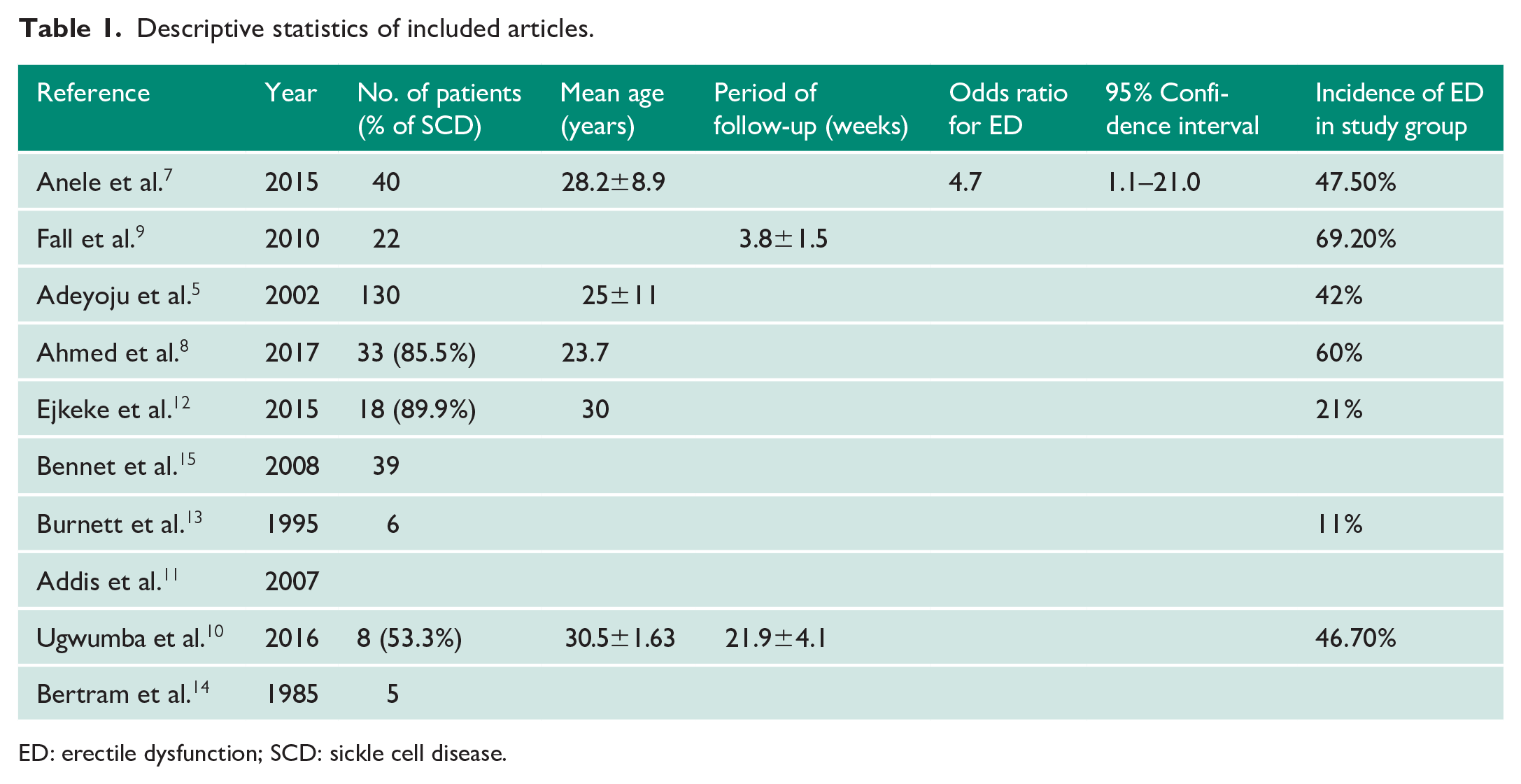
ED: erectile dysfunction; SCD: sickle cell disease.
Discussion
It is well-known that patients with SCD are at risk for developing priapism in their childhood and adolescent lives with a lifetime prevalence of ischemic priapism in SCD patients ranging from 2–35%.15,16,17 A considerable number of patients can even experience stuttering priapism that occasionally needs surgical intervention to resolve. The ischemic nature of priapism in patients with SCD makes the incidence of fibrosis of cavernosal tissues so significant. 18 The impact of ischemic priapism on the sexual function in SCD men was one of the reported complications of this hematological disease. However, clear well-documented prevalence for ED in those patients was not obtained.
The incidence of SCD is higher in certain communities than in others and hence the studies discussing different aspect of SCD related priapism vary in their number among different regions. This study tried to figure out the real incidence of ED in adolescent and adult men with a history of SCD. There was a deep literature search to find studies which involved the long-term follow-up of SCD men who suffered priapism to evaluate their sexual function when they were adolescent or adults. This seems to be of importance for many reasons; first to have a clear incidence; second to better review the optimum treatment options which reduce the incidence of ED in those patients; and third to investigate patients with established ED and find the proper way for treatment. 19
The incidence of SCD in our community is relatively high. The total number of SCD patients in Iraq in 2015 was 5124. The prevalence of SCD had slightly increased from 13.1/100,000 in 2010 to 13.9/100,000 in 2015. The highest prevalence of SCD was registered in Basra province (the most southerly province) (124/100,000) and the lowest was in Sulaymaniyah and Salahaldin (0.3/100,000). Most of the SCD patients presented with an ischemic type of priapism which is usually treated conservatively with sedation, intravenous fluids, oxygen administration, use of sodium bicarbonate, and blood transfusion. In some patients a more invasive approach is adapted in the form of corporal injection of diluted epinephrine with aspiration of cavernous blood. Shunt procedures were performed in other refractory cases. 20
Ischemic priapism, also called veno-occlusive priapism, is a form of compartment syndrome that results from blocked venous outflow which in turn prevents oxygenated arterial blood from perfusing the tissues of corpora cavernosa. The hypoxic environment, which is created by the subsequent lack of arterial inflow, damages the smooth muscles of the corpora cavernosa and may lead to irreversible necrosis and fibrosis. 21
Literature studies have extensively considered different aspects regarding ischemic priapism, such as the outcome of early versus late presentation, conservative versus surgical intervention, and comparisons between the outcomes of different surgical procedures. In most studies, the erectile function of patients, which were enrolled, was evaluated using a five-item version of the International Index of Erectile Function Questionnaire (IIEF-5) which consists of five selected items seeking to clearly discriminate between subjects with and without ED. 22 This study showed that searching the Web for articles addressing the long-term effect of priapism on the sexual function in patients with SCD revealed not such an abundance of studies. In most of the cases, the long-term follow-up of sicklers with a history of priapism for the development of ED is not adequate, probably because there was a lack of clear strategy for following up SCD men into adolescent and adulthood life. Some studies discussed the treatment of established ED mainly by the use of penile implants and evaluated this option of treatment as being effective or not.21,22
The presence of variable incidence and prevalence of the SCD among different parts of the world is probably the most important factor that affects the depth of follow-up of patients with ischemic priapism and the length of this follow-up. To our knowledge, this study seems to be the only systematic review that has analyzed ED due to ischemic priapism in SCD men over a long period of follow-up. The absence of good-quality evidence to identify the long-term outcomes of ischemic priapism in SCD men suggests there is a need to conduct good multicenter prospective protocols to investigate the condition.
Conclusion
SCD is well-known in the etiology for the development of ischemic priapism and subsequent ED. Different treatment strategies are present for the treatment of this condition, ranging from conservative medical management to surgical intervention. It is recommended to conduct better quality prospective studies with longer follow-up periods to find out the real incidence of ED in men with SCD-associated priapism.
Footnotes
Acknowledgements
None.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of Basrah College of Medicine approved this study (REC number: 0304093-2020).
Informed consent
Not applicable.
Guarantor
FSA.
Contributorship
MA Mohammed and HHA Almoamin researched the literature and conceived the study. FS Attar was involved in protocol development, gaining ethical approval, patient recruitment and data analysis. FS Attar wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript