
Abstract
Objective:
Numerous publications describe the management of stent encrustations, but few address long-term risks. The purpose of this study is to analyze the incidence of new chronic kidney disease attributed to retained ureteral stents in a large multi-institutional patient population.
Materials and methods:
A retrospective chart review of stone disease patients with ureteral stent placement was done in the nation-wide Cerner Health Facts database between 10 July 2009 and 7 June 2018. The estimated glomerular filtration rate was calculated using serum creatinine and the Modification of Diet in Renal Disease Study equation. The study focused on patients with stent duration longer than 6 months and an estimated glomerular filtration rate above 60 ml/min/1.73 m2 before stent placement.
Results:
A total of 1234 stent placements were documented in the Cerner database, 108 patients had a normal estimated glomerular filtration rate prior to the retained stent. The median duration of retained stents was 12.1 months (range 6.1 to 77.7 months), and 33 (30.6%) patients developed new onset chronic kidney disease compared to 8.3% in patients with non-retained stents.
Conclusion:
A new onset of chronic kidney disease was observed in 30.6% of patients with retained ureteral stent, emphasizing the importance of patient counseling and preventive measures to ensure patient compliance and follow-up.
Level of evidence:
Not applicable in this multi-institutional cohort study.
Introduction
First described in 1967, ureteral stent placement is now a common urological procedure establishing drainage from the kidney to the bladder when there is obstruction. 1 Ureteral stents alleviate obstruction and allow for earlier patient discharge from hospitals avoiding percutaneous nephrostomy tubes, but complications can arise such as suprapubic and flank pain, and irritative voiding symptoms. Vesicoureteral reflux is almost inevitable with a patent stent in place. 2 If not removed in a timely manner and left indwelling for more than 6 months, morbidities due to stent migration, ureteral obstruction, urinary tract infections and encrustation may result.3–5 Stent encrustation has been a common complication and correlates with indwelling duration. One study followed patients with stent duration times ranging from days to 18 months showing 9.2% of stents encrusted with retrieval of less than 6 weeks, 47.5% between 6 and 12 weeks, and 76.3% thereafter. 6 Severe complications can even cause death (as reported in one study) due to advanced renal disease and infected hydronephrosis secondary to retained ureteral stents. 7 The treatment and management of stent encrustation have been widely studied, but reports of the rates of renal complications that arise with retained stents are needed.8–11 A previous study from 2019 defined a decrease in the estimated glomerular filtration rate (eGFR) to below 60 ml/min/1.73 m2 as chronic kidney disease (CKD) in patients with retained stents for more than 6 months. This single-institutional study showed that nine of the 34 patients with retained ureteral stents developed a new onset of CKD (26.5%). 12 Other studies show CKD as a possible complication of retained stents, but very few have investigated the percentage of patients that are affected. 13 The purpose of this study was to analyze the incidence of new onset CKD in a large multi-institutional patient population with retained ureteral stents.
Materials and methods
A retrospective review of all records of patients with a ureteral stent placement in the Cerner Health Facts database was done using the Clinical Research Data Warehouse. Cerner is an international information technology company used widely as an electronic medical record (EMR). Data in Health Facts are extracted directly from the EMR of hospitals in which Cerner has a data use agreement. Encounters may include pharmacy, clinical and microbiology laboratory, admission and billing information from affiliated patient care locations. All admissions, medication orders and dispensing, laboratory orders and specimens are date and time stamped, providing a temporal relationship between treatment patterns and clinical information. Cerner Corporation has established Health Insurance Portability and Accountability Act-compliant operating policies to establish de-identification for Health Facts. Inclusion criteria were: (a) patient EMR charts between 10 July 2009 and 7 June 2018; (b) International Classification of Disease (ICD) version 10 codes N20.0, N20.1, N20.2 for kidney or ureteral stone; (c) current procedural terminology (CPT) code 52332 for ureteral stent placement and 52310 for ureteral stent removal. Exclusion criteria were: (a) patient charts outside the time frame 10 July 2009 and 7 June 2018; (b) stent placement for other reasons than obstructing urolithiasis (such as ureteral strictures and obstructing malignancies of the pelvis and retroperitoneum).
While searching through the patients’ EMR database it became apparent that many stent patients were not accounted for stent removal. The main explanations for this phenomenon are: first, the stents were removed at another institution (in particular outpatient clinics) that did not use the Cerner EMR system. In this context it has to be mentioned that Cerner is mainly a hospital-based EMR system and more than 75–80% of outpatient clinics use alternative systems. Secondly, many patients removed their stents themselves within days post-stent placement by pulling a string attached to the stent externally accessible outside the urethra. For these patients no procedural codes for stent removal would be documented in any EMR system. These patients were excluded from the analysis.
For the purpose of our study a retained ureteral stent was defined as a stent left in place for longer than 6 months.
Baseline patient characteristics including age, gender, race, duration of stent placement, comorbidities of diabetes and hypertension, serum creatinine, blood urea nitrogen, and eGFR before and after stent placement were collected. The objective was to determine the percentage of patients who were diagnosed with a new onset of CKD. CKD is defined as eGFR less than 60 ml/min/1.73 m2. Each patient’s eGFR was calculated using the serum creatinine and the Modification of Diet in Renal Disease Study equation: (60 ml/min/1.73 m2) = 175 × (SCr)–1.154 × (age)–0.203 × (0.742 if female) × (1.212 if African American). 14
Results
During the period from July 2009 to June 2018, there were a total of 1234 stent placements documented in the Cerner database, among them 108 patients with a retained stent and a normal eGFR prior to stent placement. The median age of the patients was 52.5 years and the median duration of ureteral stent in situ was 12.1 months (range 6.1–77.7 months). Of these patients who started with a normal eGFR, 33 (30.6%) suffered from a new onset of CKD. Before stent placement, five of these patients were diagnosed with diabetes mellitus, 29 with hypertension, and 27 with both diabetes and hypertension. Twenty-two patients with one or both comorbidities developed CKD (36.1%). Of the 47 patients who did not have documented comorbidities, 11 developed new CKD (23.4%) (Figure 1). There was no significant difference in developing new onset CKD for patients with a retained stent less than a year versus more than a year (threshold set at P<0.05).
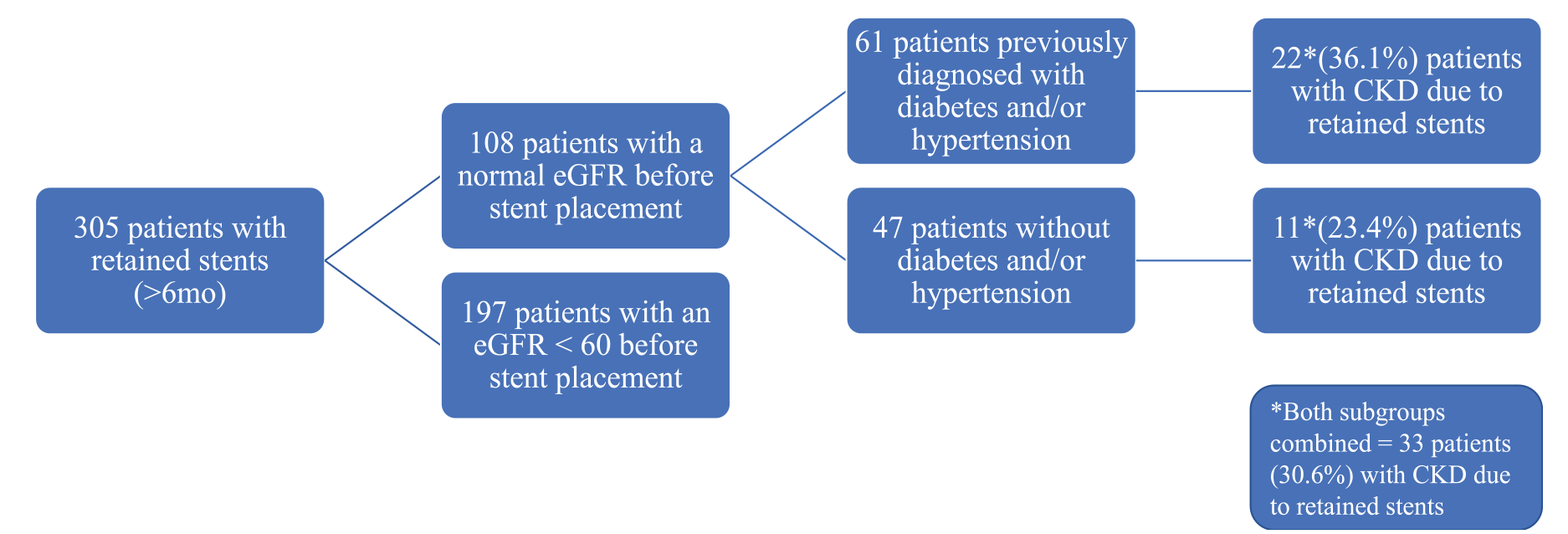
Chronic kidney disease in patients with retained stents (>6 months).
Of the 33 patients who had a normal eGFR before stent placement and an eGFR below 60 after removal of the retained stent, six had a documented permanent eGFR below 60 for more than 3 months after stent removal. For the remaining cases no long-term data (>3 months) were available due to follow-up in clinics that are not Cerner based or due to loss of follow-up.
Calculation of the baseline risk for CKD in patients with non-retained stents: in the Cerner EMR database 929 patients had a stent for less than 6 months. A total of 198 patients were documented to have a stent removal code and correlating labs. As mentioned above, many of patients with non-retained stents did not come back to the hospital for stent removal but rather extracted the stent themselves or went to an outpatient clinic that did not use Cerner EMR. A total of 108 of these patients started with a normal eGFR prior to stent placement. The median age of the patients was 50 years and the median duration of the ureteral stent in situ was 0.8 months (range 0.2–4.8 months). Nine patients (8.3%) suffered from new onset of CKD at the time of stent removal.
Discussion
The complications of retained ureteral stents are well documented through case studies and retrospective reviews.2–7 After systemically reviewing the literature, only a few single-institutional studies have determined the long-term sequelae of retained stents on renal function.8–11 These single-institutional studies reported numbers of patients with retained stents in the range of nine and 38, the calculated risk of developing CKD was ranging between 18% and 33%.15–18 As far as we know, this is the first multi-institutional study analyzing the risk of CKD in more than 100 patients with retained ureteral stents placed for obstructive urolithiasis. We included only stone disease patients, ruling out other indications for stent placement such as cancer and ureteral strictures as the latter conditions carry intrinsic factors potentially affecting renal function. After assessing the 108 patients with retained stents who had a normal eGFR prior to stent placement, 33 (30.6%) were found to have a decreased eGFR below 60 ml/min/1.73 m2 or CKD secondary to retained stents. This 30.6% risk of developing CKD correlates with the previously reported numbers of 18% and 33%, but in a much smaller patient cohort.15–18 In our multi-institutional study, we found that 23.4% of patients without any documented comorbidities developed CKD after retained stents. This result is consistent with the clinical studies reported so far (Table 1). Furthermore, patients with retained stents, whether for less than a year or longer than a year, were found to have no statistically significant difference in developing new onset CKD. Six of the 33 patients had a persistent eGFR less than 60 more than 3 months after the removal of the retained stent, which is considered permanent. For the remaining cases no long-term data (>3 months) were available due to follow-up in clinics that are not Cerner based or due to loss of follow-up. This suggests that up to one-third of patients with retained stents longer than 6 months are at risk of developing CKD as also reported in previous single-institutional studies with smaller cohorts (Table 1).
Reported risk of CKD with retained stent (according to Pubmed search, timeframe year 2000 until October 2020).
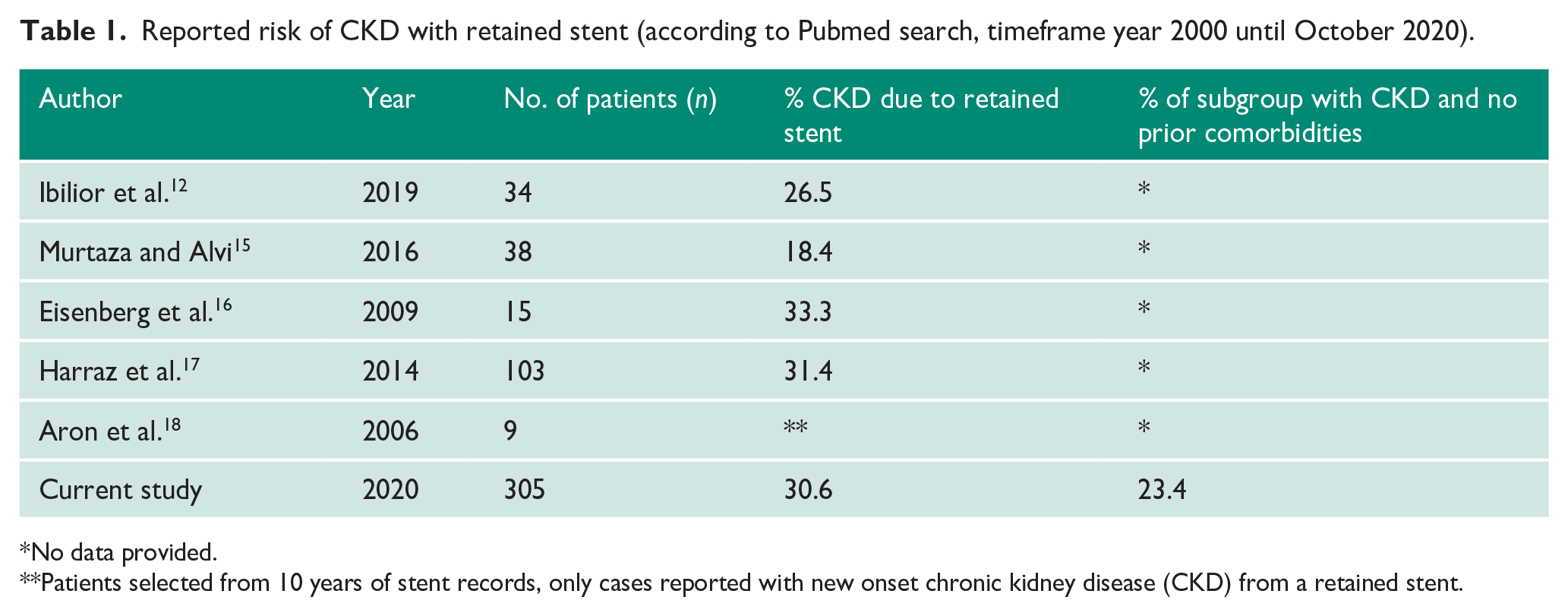
No data provided.
Patients selected from 10 years of stent records, only cases reported with new onset chronic kidney disease (CKD) from a retained stent.
In our study the baseline risk of CKD in patients with non-retained ureteral stents (<6 months) was 8.3% (9/108). Ibilibor et al. found a similar small rate 3.3% (four/120) of new onset CKD in their baseline group of stone patients. 12 Therefore, it can be assumed that the natural rate of new onset CKD is small in comparison to that of retained stent patients, signifying stents to be the plausible cause of decline.19,20
Previous reports have listed many causes for delayed stent removal, but inconsistent patient follow-up and non-compliance are among the main ones. As patients are at significant risk of CKD due to retained stents, the questions arise as to how to avoid this long-term complication and who is primarily responsible: is it the urological surgeon placing the stent or the patient not complying with the follow-up appointment? Previous studies recommended to take preventive measures and to identify patients at risk of stent retention. For instance, Medicaid and uninsured patients are considered to be at increased risk. 12 Several institutions have implemented computer-based stent registries to keep track of patients with stents for that purpose.21,22 Some studies have investigated the use of dissolvable ureteral stents as a solution to chronic retention. 23 A study recently found that patients who use a smartphone stent tracking application had fewer overdue times and lost to follow-up than patients who did not use the ‘app’, 24 but despite tracking systems, some patients still get lost to follow-up. Clearly, patient follow-up is key to decreasing renal complications from retained stents.
One of the main limitations of this study is the process of data extraction from the Cerner database. As mentioned earlier, different hospital and clinic-based EMR systems cause logistic and documentation-related shortcomings in obtaining a complete patient count and follow-up for stent placement and definitive removal. Studying further clinical details such as degree of CKD, time of occurrence, and impact of coexisting conditions is difficult due to the nature of this clinical problem in which randomized and/or prospective clinical trials are not feasible.
Conclusion
Retained ureteral stents are associated with a decrease in renal function emphasizing the importance of thorough patient counseling and proactive measures to ensure patient follow-up and compliance. This multi-institutional study confirms that new onset CKD is developing in 30.6% of patients with a retained ureteral stent for more than 6 months.
Footnotes
Acknowledgements
None.
Conflicting interests
The author(s) declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
WTdR.
Contributorship
Werner T de Riese, Justine R Yamashiro and Cornelia S de Riese contributed to the study conception and design. Material preparation, data collection and analysis were performed by Justine R Yamashiro, Travis J Cole, Chip Shaw and Werner T de Riese. The first draft of the manuscript was written by Justine Yamashiro, the revisions of the manuscript were done by Werner T de Riese, Cornelia S de Riese and Chip Shaw. All authors read and approved the final manuscript.