
Abstract

Introduction
Prostatic artery embolization (PAE) to treat obstructive benign enlargement of the prostate (BPE) is a safe, effective and validated technique. Recognized risks are post-embolic syndrome, non-target embolization and ischaemic bladder detachment. 1 This case report highlights a rare complication of sloughed prostatic necrotic tissue causing retention and recurrent catheter blockages which needed cystoscopy extraction. We hope this report will lead to early recognition and intervention in the future.
Case report
A 79-year-old male with failed medical therapy for BPE presented with high-pressure chronic retention on computed tomography (CT) scan which showed a residual volume (RV) of 1.5 L and bilateral hydronephrosis (Figure 1). After initial catheterization improved kidney function, he underwent magnetic resonance imaging (MRI) of the prostate, which estimated a prostate volume of 143 cc and showed no evidence of malignancy, with a prostate-specific antigen (PSA) density of 0.07 (PSA=10 ng/mL).
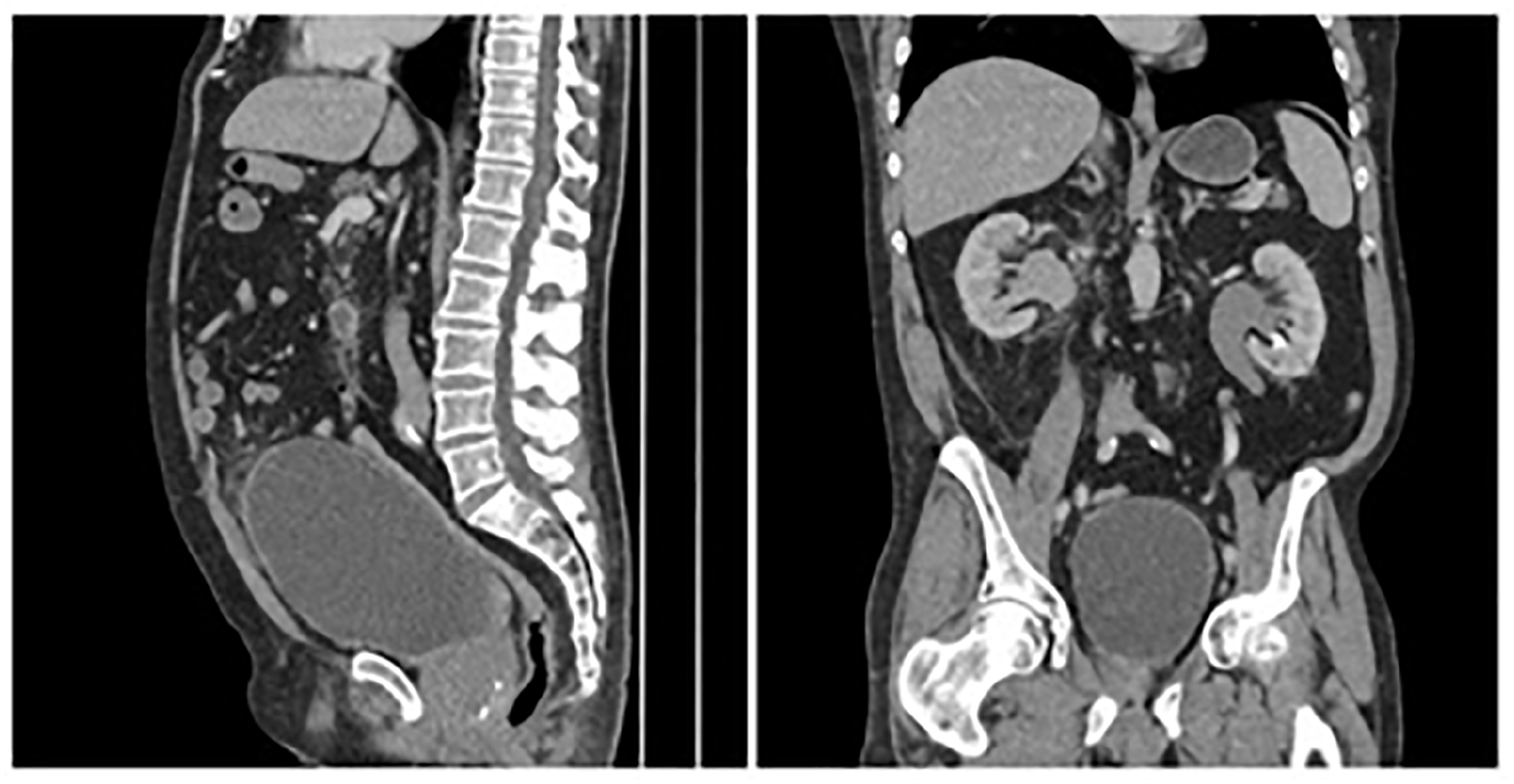
Sagittal and coronal sections of the computed tomography scan, showing features of high-pressure urinary retention.
The patient was counselled on surgical interventions, including transurethral resection of the prostate, holmium laser enucleation of the prostate or PAE, with a CT angiogram showing favourable configuration for PAE. In September 2019, he underwent successful PAE with an uneventful recovery, no shunting and 400 µm Embospheres injected with satisfactory stasis (Figure 2).
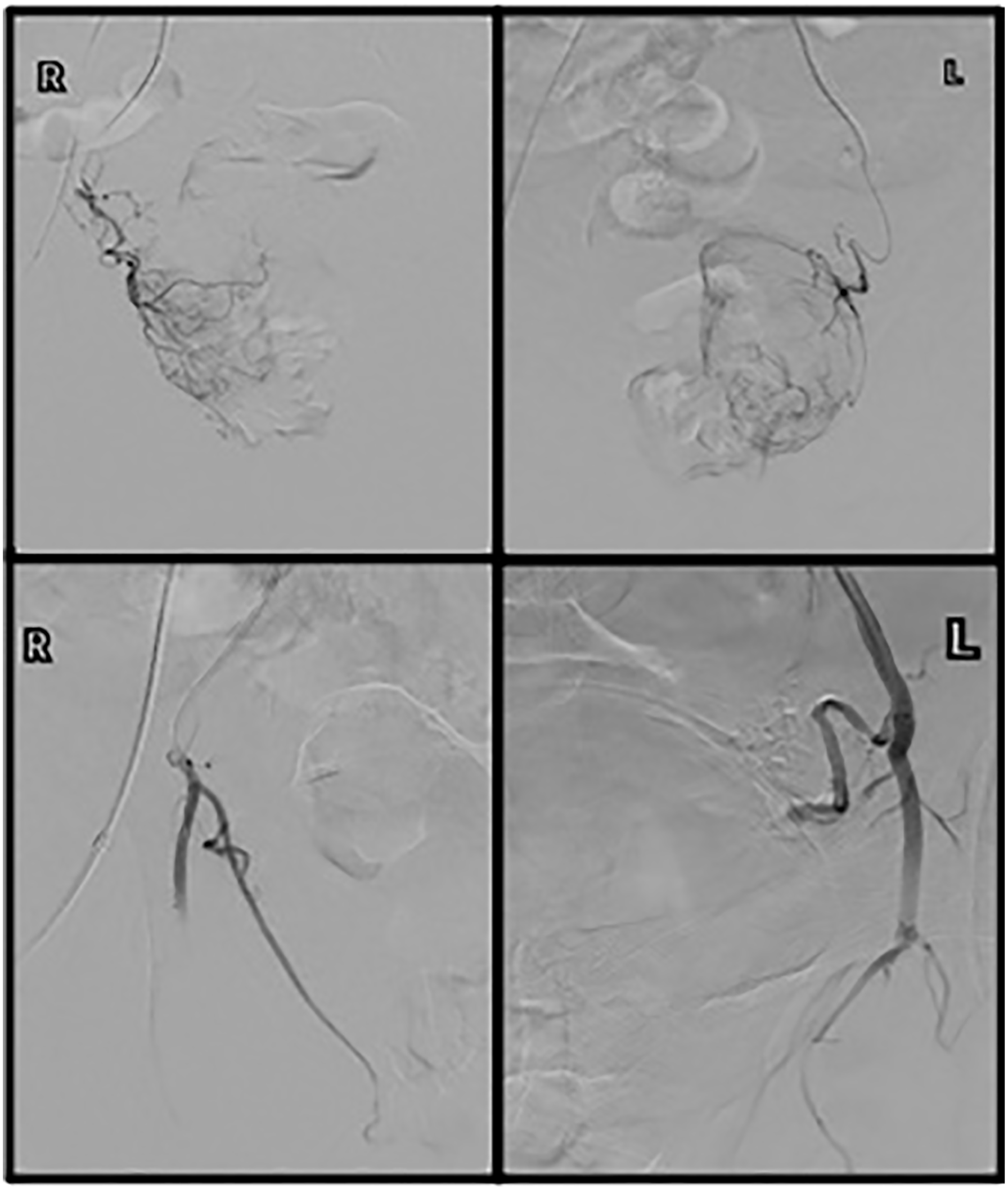
Prostatic artery embolization through the right common femoral artery, showing before and after embolization on both sides.
Eight weeks later, the patient underwent a trial without catheter (TWOC) but re-presented with acute retention and recurrent catheter blockages. A second TWOC failed, even though it was of low RV. A repeat MRI of the prostate showed reduction in prostate size to 45 cc and inflammatory changes to the prostate, but also a 3 cm semi-circular structure near the catheter balloon (Figure 3).
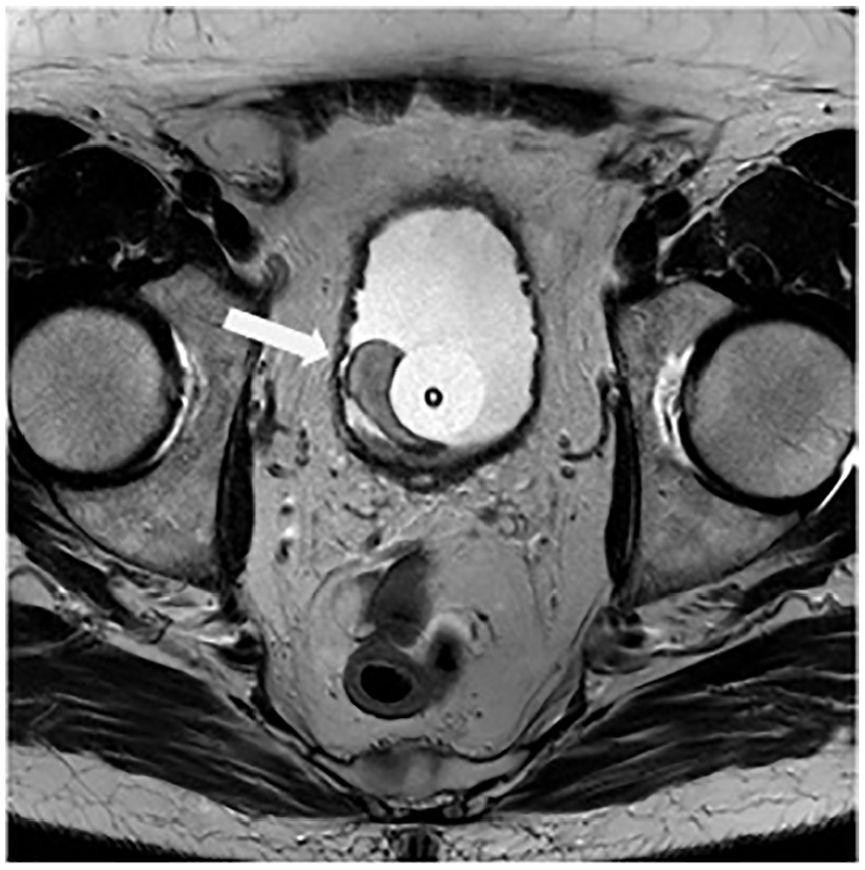
Magnetic resonance imaging of the prostate, showing a semi-circular structure (arrow) near the catheter balloon in the bladder.
Cystoscopy showed the prostatic fossa with a wide-open large cavitation in the residual lateral lobes and 3 cm of large necrotic tissue floating in the bladder that needed resection in order to complete evacuation (Figure 4). Its histology was of remnants of necrotic prostatic tissue (calcified necrotic tissue showing traces of corpora amylacea and no viable tissue). The patient is now catheter free.
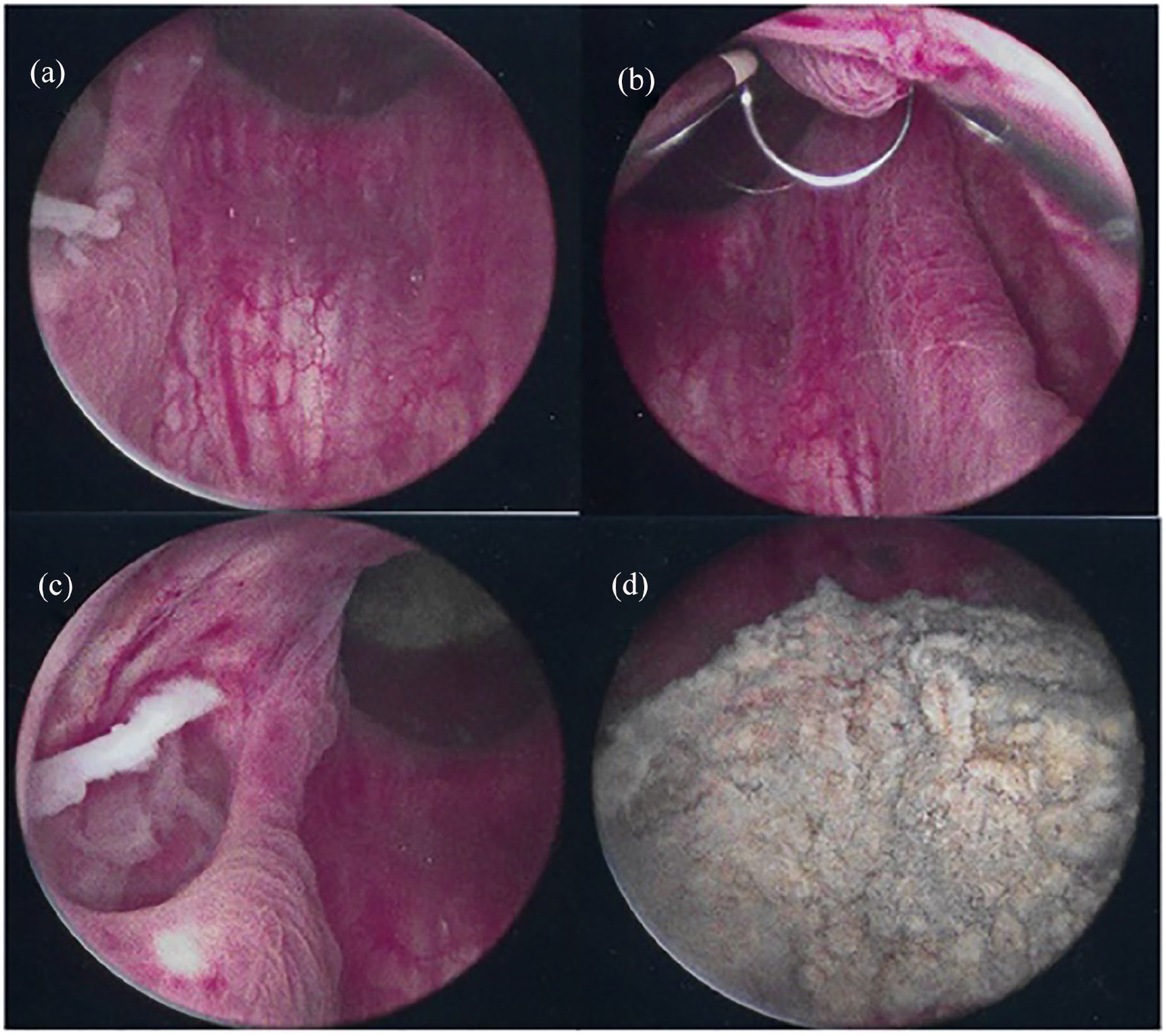
Cystoscopy showing (a)–(c) the open prostatic fossa bed with cavitation in both lateral lobes and (c) and (d) the floating ball of necrotic tissue.
Discussion
PAE is a NICE-approved, safe and non-invasive technique to treat BPE. It is particularly suitable for treating patients with a large prostate volume but who are unfit for invasive procedures. 2 Studies report a 28% reduction in prostate volume, a good success rate 2 and a low complication rate, with most minor complications, such as haematuria, haematospermia, urinary tract infections, post-embolization syndrome and inguinal haematoma, being self-limiting. Major complications are reported in <1% of cases and mainly comprise bladder ischaemia and severe urinary tract infection. 1
A literature review revealed sporadic case reports of prostatic tissue expulsion after PAE, but most were self-limiting.3–5 Although Uflacker et al. warned in his case report of the possibility of acute retention, 5 this the first report to describe retention by sloughed prostatic tissue as a complication and its subsequent management.
As more studies show the effectiveness of PAE, we require a better understanding of the complications, particularly as most studies are of patients with a median age of >65 years. 1 This scenario should be considered after PAE in a patient with progressive symptoms, unexplained episodes of catheter blockages and low residual volume retention. Early cystoscopy assessment is recommended, as sloughed tissue may be too large to pass spontaneously.
Supplemental Material
sj-jpg-1-uro-10.1177_20514158211018133 – Supplemental material for Retention by sloughed prostatic tissue: A rare complication after prostate artery embolization
Supplemental material, sj-jpg-1-uro-10.1177_20514158211018133 for Retention by sloughed prostatic tissue: A rare complication after prostate artery embolization by Fouad Maqboul and Salil Umranikar in Journal of Clinical Urology
Supplemental Material
sj-jpg-2-uro-10.1177_20514158211018133 – Supplemental material for Retention by sloughed prostatic tissue: A rare complication after prostate artery embolization
Supplemental material, sj-jpg-2-uro-10.1177_20514158211018133 for Retention by sloughed prostatic tissue: A rare complication after prostate artery embolization by Fouad Maqboul and Salil Umranikar in Journal of Clinical Urology
Footnotes
Acknowledgements
The authors thank Dr Alex Chapman, Interventional Radiologist, Ashford and St Peter’s Hospital, UK
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Informed consent was obtained for patient information to be published in this article.
Guarantor
Fouad Maqboul
Contributorship
Fouad Maqboul: consent, writing – original, editing and final draft, investgation analysis, literature review, visualization; Salil Umranikar: wiriting – review and edit, supervision, visualization
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.