
Abstract
Objective:
The study aimed to retrospectively evaluate postoperative results of patients with duplex system ureterocele (DSU) who underwent endoscopic ureterocele incision (UI), lower urinary tract reconstruction (LUTR) or both, and investigate the necessity of upper pole heminephrectomy (UPH) in ureterocele treatment.
Patients and methods:
In total, 44 patients with DSU who were operated on in December 2005 and December 2018 were evaluated for patient characteristics, ureterocele location, differential renal function (DRF), vesicoureteral reflux (VUR), postoperative incontinence, proteinuria, hypertension and urinary tract infection (UTI).
Results:
UI was performed in 27 of 44 cases (61.3%) as the first-line treatment. Ten of them (37%) had no urinary infection or renal function loss at a mean of 3 years (1.5–7 years). LUTR was needed in 17 patients after UI due to VUR in 14 patients and bladder outlet obstruction (BOO) in 3 patients. In total, 34 patients who underwent LUTR, proteinuria or incontinence were not detected in the mean 6 years’ follow-up. Thirty-three patients (97%) had identical renal scans and similar DRF before and after the operation. No patient underwent UPH.
Conclusion:
UI must be considered the first-line treatment in DSU in infancy. In older patients, especially with VUR, LUTR is effective and safe and UPH mostly is not necessary.
Level of evidence:
4
Keywords
Introduction
The underlying anatomical pathology in patients with duplex system ureterocele (DSU) is complicated due to the presence of vesicoureteral reflux (VUR), bladder neck anomaly and outlet obstruction, ureteral dilatation and upper pole dysplasia. The goals of management for patients with DSU include prevention of renal damage, promotion of continence and minimalization of surgical morbidity. Although there are various treatment modalities, accomplishing these objectives is a significant challenge.1–4 Upper pole heminephrectomy (UPH) has been the first-line treatment option to prevent urinary tract infection (UTI) and bladder neck obstruction. 1 But the requirement for a second surgical procedure due to reflux or bladder outlet obstruction (BOO) after UPH increases to 84% when preoperative VUR is associated with the ureterocele.5–7 Long-term follow-up studies showed that the prevalence of de novo ipsilateral lower pole or contralateral reflux following UPH was 40% to 50%.5,7
It was also reported that the nonfunctional upper pole (NUP) left in situ is safe.3,4,6,8
Ureterocele incision (UI) which is a minimally invasive procedure has been the preferred treatment option to prevent ureteral or bladder neck obstruction in patients and is reported to be enough in the definitive treatment for a small, single system, intravesical ureterocele, with no reflux. However, most patients with DSU need a second operation. 2 Lower urinary tract reconstruction (LUTR) corrects the anatomical pathology and reflux at the same time, but it may have the same technical difficulties, especially in patients under 1 year of age.
In this study, we aimed to analyse the results of UI only, LUTR only and UI + LUTR in patients with DSU retrospectively and also evaluate the complications related to surgery or the remaining upper pole.
Materials and methods
A total of 44 patients with DSU who were operated with LUTR only (17), UI + LUTR (17) and UI (10) only were evaluated retrospectively for patient characteristics, ureterocele location, differential renal function (DRF), presence of VUR, postoperative complications, the requirement for additional surgery, hypertension, proteinuria, urinary dysfunction and UTI. Ultrasonography (USG), dimercaptosuccinic acid (DMSA) scintigraphy and voiding cystourethrography (VCUG) were performed in the initial evaluation and postoperative follow-up.
For the patients with high-grade VUR who were admitted older age, LUTR was performed. However, for patients with an extremely dilated upper urinary tract, initial treatment was UI to ensure ureteral reduction. LUTR was performed after a period of follow-up for 6 to 12 months in these patients.
UI was performed in all patients with upper pole dilatation and dilated ureter due to obstruction under 1 year of age and a prophylactic antibiotic was administered. Patients with no VUR or UTI were conservatively followed up after UI. If patients had febrile UTI more than once after UI despite using antibiotic prophylaxis, VCUG was repeated. In patients who had VUR or signs of BOO (hydronephrosis in the contralateral side, voiding dysfunction, postmicturition residue (PMR) than 10% of bladder capacity) with or without functioning upper pole moiety, LUTR was performed (Figure 1).
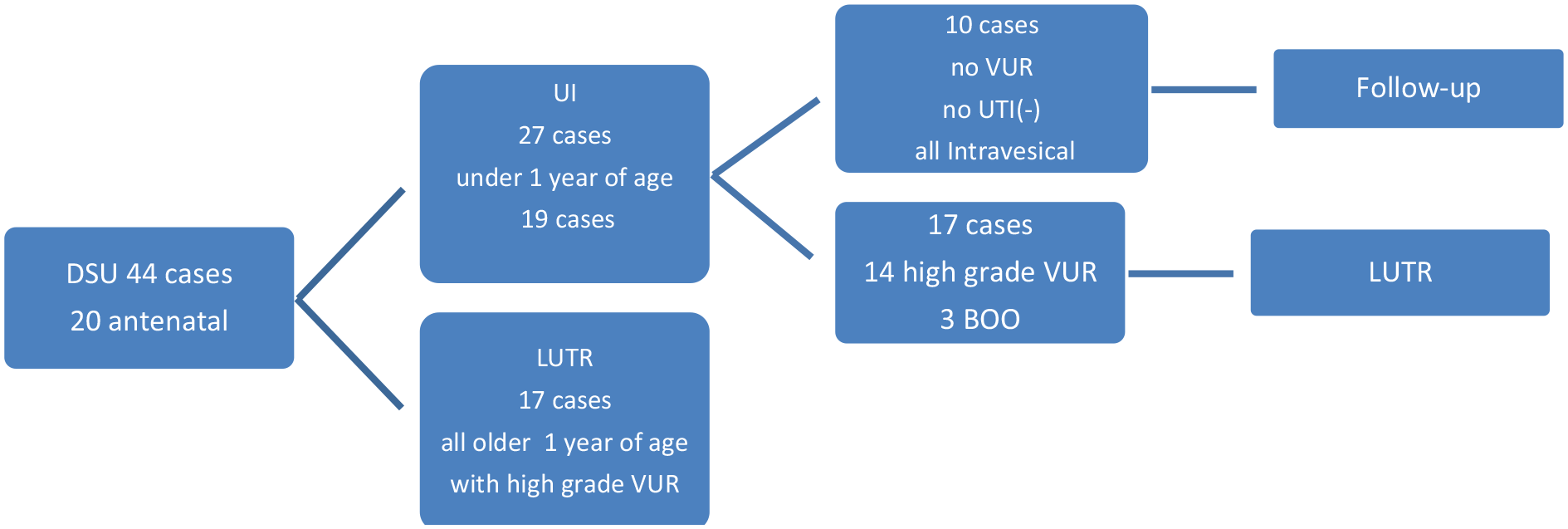
Management of patients with DSU.
UI was performed with a cold knife using an 8 Fr resectoscope. LUTR included ureterocele excision, bladder base reconstruction and common sheath ureteral reimplantation (Cohen). Tapering was performed by the Hendren technique for ureters over 1 cm in diameter.
Urodynamic studies, for patients with UTI after LUTR, were performed. PMR, greater than 10% of bladder capacity, indicated abnormal emptying. For patients who suspected BOO before the operation, PMR was measured by only post-voiding USG.
Data are shown as the mean ± standard deviation. The outcomes were compared between the two groups (preoperative and postoperative values of DRF) using a paired-sample Student’s t-test. All values of p < 0.05 were accepted as statistically significant.
Results
DSU was detected by antenatal USG in 20 patients (45%) and was diagnosed in the other 24 (54%) patients after birth because of febrile UTI. The male to female ratio was 21/23. DSU was left sided in 20, right sided in 24, intravesical in 27 and extravesical in 17 patients.
UI-only group
UI was performed in 27 cases (61%) (extravesical ureterocele/intravesical ureterocele (E/I): 9/18). Nineteen of them were under 1 year of age (70%). Ten patients (37%) (mean age = 19.4 months) who had intravesical ureterocele without reflux were followed up conservatively after UI (UI-only group) (Table 1). Mean preoperative DRF was 42.85 ± 9.1 and was found similar (mean 41.75 ± 8.6) (p = 0.308) in a year follow-up. There was no infection, proteinuria, incontinence or DRF loss at a median of 3.5 years (1.5–7 years).
Demographics and postoperative findings of patients with DSU.
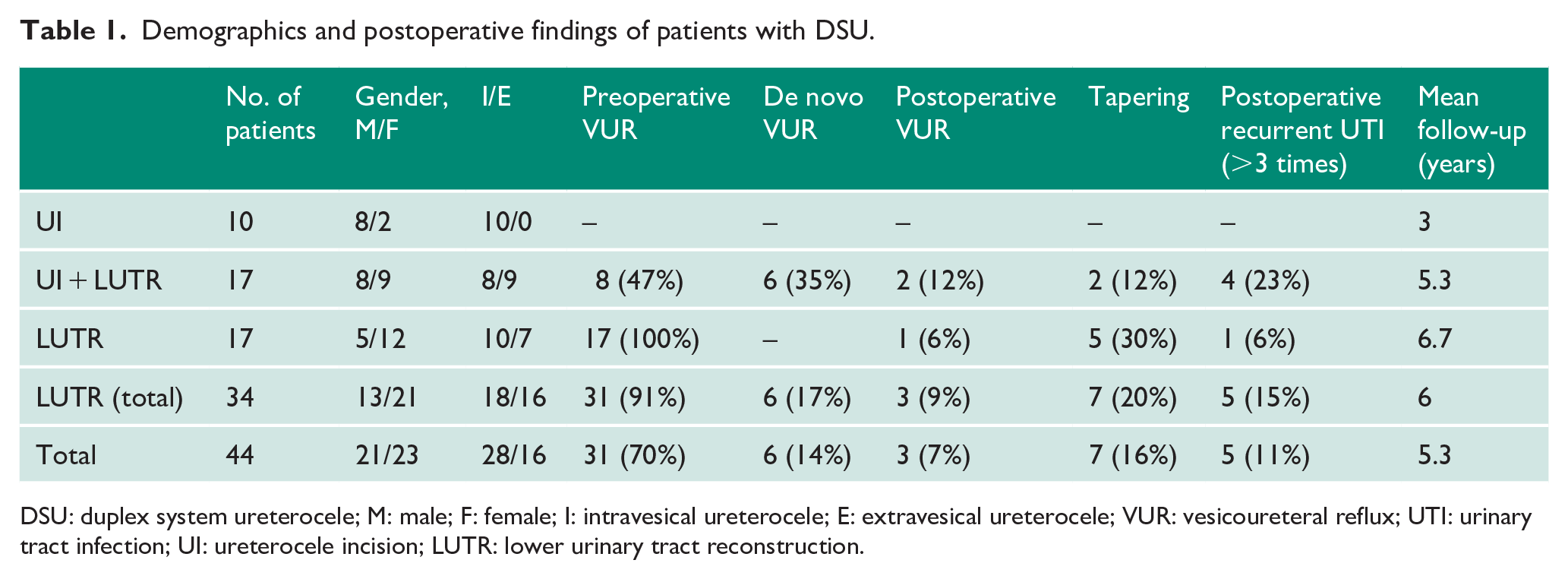
DSU: duplex system ureterocele; M: male; F: female; I: intravesical ureterocele; E: extravesical ureterocele; VUR: vesicoureteral reflux; UTI: urinary tract infection; UI: ureterocele incision; LUTR: lower urinary tract reconstruction.
LUTR + UI group
LUTR was performed at a mean of 14 months after UI in the other 17 cases (E/I: 9/8) (Table 1). VUR was detected in grade 5 in nine patients, grade 4 in four patients and bilateral grade 3 in one patient. The other three patients had bilateral grade 4 hydronephrosis and post-voiding residue in USG with febrile UTI. De novo reflux to the upper pole developed in six of nine patients who had no VUR before UI and two of six patients who had VUR to lower pole. Eight of 27 patients developed de novo reflux after UI in total (29%). LUTR was performed due to VUR in 14 patients (new onset in 6 cases) and BOO in 3 patients with UTI. The mean DRF was found similar before (36% ± 10.4%) and 1 year after the operation (35.5% ± 11.2%) (p = 0.785). For patients with BOO, counterpart hydronephrosis and voiding problems disappeared in postoperative follow-up.
LUTR-only group
In 17 patients who were older than 1 year of age (mean age: 60.7 months) with high-grade VUR, LUTR was performed as first-line treatment (5 males, 12 females; E/I: 8/9). Mean initial DRF was 32.4% ± 12.8% and was found unchanged (mean 32.7% ± 12.8%) in postoperative follow-up (p = 0.631).
Total results of LUTR
LUTR was performed in 34 patients (21 females, 13 males; 20 left sided, 14 right sided) with DSU (77%) in total (mean age: 43.6 months) (Table 2). The mean follow-up period was 6 years (1.5–13 years). Eighteen of the ureteroceles were intravesical and the other 16 were extravesical. Twenty-three (67%) patients had DSU with the upper pole obstruction and lower pole reflux. Two of 34 (6%) patients demonstrated reflux to upper and lower poles. Nine patients (26%) had no radiological evidence of reflux at the time of admission. Six of them developed de novo reflux to the upper pole after UI.
Demographics and operative outcomes of the patients with DSU for whom LUTR was performed.
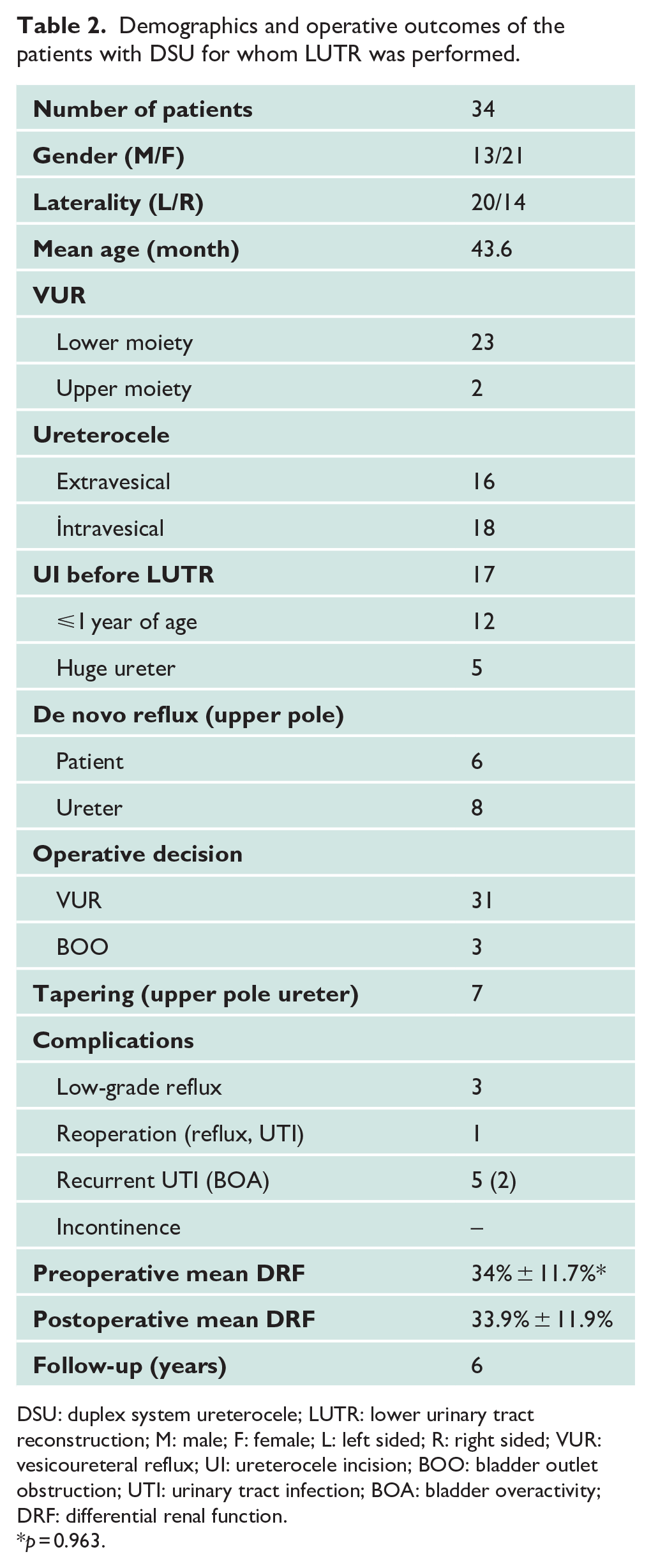
DSU: duplex system ureterocele; LUTR: lower urinary tract reconstruction; M: male; F: female; L: left sided; R: right sided; VUR: vesicoureteral reflux; UI: ureterocele incision; BOO: bladder outlet obstruction; UTI: urinary tract infection; BOA: bladder overactivity; DRF: differential renal function.
p = 0.963.
Ureteroneocystostomy was done bilaterally due to contralateral VUR in four patients and due to contralateral ureterovesical junction obstruction in one patient. Seven patients (33%) required tapering of the upper pole megaureter. In five patients, a UI was not performed before the surgery. In the other two patients, tapering was necessary despite a slight decrease in ureteral diameter after UI.
Postoperative follow-up
Postoperative ultrasound showed either complete resolution or a decrease in upper tract dilatation in all patients. Follow-up VCUG revealed low-grade reflux (grade 1 or 2) in 3 of 34 patients (9%). Two of them did not have an infection and additional renal damage. In one patient with recurrent UTI and diminished DRF, reoperation was needed (3%).
Twenty patients (59%) were infection-free after the operation. Six patients had afebrile UTI in the early postoperative period once (18%), and three patients had twice (9%). Urodynamic studies were performed in other five patients (15%) with recurrent febrile UTI. Bladder overactivity (BOA) was detected in two patients. The other three patients’ urodynamic studies were found normal. Patients with BOA became infection free with anticholinergic medical therapy and antibiotic prophylaxis. The other two patients have no urodynamic dysfunction detected, but they were incompatible with antibiotic prophylaxis. One patient with recurrent VUR and diminished renal function was reoperated.
Thirty-three patients (97%) had identical total renal scans and similar DRF before (34% ± 11.7%) and after (33.9% ± 11.9%) the operation (p = 0.963). The patient, who underwent reoperation, was the only patient with diminished DRF of more than 5%. Mild hypertension was detected in only one patient with morbid obesity. Thirty-three patients (97%) were continent except for a 2.5-year-old patient who has not gained urinary control yet. The urgency was observed in two patients with BOA. These patients responded well to medical therapy. No patient had development of proteinuria. The follow-up period was with a mean of 6 years.
Discussion
The aim of treatment in DSU can be summarized as prevention of infection and obstruction, elimination of reflux, preservation of DRF and minimization of the morbidity. In the case of DSU, UPH was perceived as one of the first treatment methods chosen for many years.1,7 However, studies of patients with ureterocele treated with UPH revealed that the additional LUTR rate to treat the anatomical abnormality was 15% to 20% if VUR was absent, but increased to 84% to 90% when VUR was present.5,7,9 The indications for secondary surgery are most often persistent or delayed onset VUR, stasis of urine in the ureteral stump, BOO and recurrent UTI. 10
As UI alone allows the drainage of the upper pole and no complications related to the remaining upper pole have been reported, the need for UPH has been less and the efficacy of this procedure has been questioned.4,8,11 Furthermore, UPH does not correct the anatomical defect and this procedure alone will not cure reflux to the lower pole, bladder neck obstruction or detrusor defect in the trigone in large, extravesical ureterocele. Wang et al. 12 reported that treatment-free status most often required ureterocele excision. Shimada et al. 13 concluded that the hypomuscularity of the trigone and the bladder outlet that backs the ectopic ureterocele should be repaired and a high reoperation rate following the UPH has been considered to result from leaving these anatomical defects at the bladder level.
In addition, during the upper pole ablative surgery, the risk of vascular compromise of lower pole moiety was reported.14,15 Sheth et al. 16 reported complications were seen in higher incidence in the UPH and he recommended LUTR. Ipsilateral ureteroureterostomy is recommended, an alternative technique for the treatment of DSU in patients with salvageable upper pole. However, this technique has some limitations like ureteral dilatation and the presence of ipsilateral reflux. New onset of yo–yo reflux, residual ureteral stump infection and lower pole damage are also possible.14,17
UI is a minimally invasive method in terms of decreasing the dilatation of the system to save some time for the definitive treatment. 18 In this study, UI was used as the first-line treatment method in patients whose upper system was overly dilated or small age for LUTR. It was remarkable that all patients who were successfully treated by UI only had intravesical ureterocele with no reflux.
Recent studies suggested that subureteric transurethral injection (STING) should be added to the treatment as a minimally invasive treatment after the incision. 19 We believe that it is difficult to treat reflux with STING in DSU patients because of individual anatomical variation and severe trigonal distortion. Moreover, reflux in DSU cases is generally high grade. The weakness of the bladder wall, which is a component of ureterocele a short intravesical tunnel length may affect the success of STING. 20 Even in duplex system patients without ureterocele, the success rates were reported low.21,22 Long-term complications like obstruction are reported in recent years; open surgery is recommended especially in higher risk groups.23,24 Moreover, STING may complicate further surgeries to the bladder level.
For patients with DSU associated with NUP, concerns have been expressed due to theoretical risks of the development of hypertension, proteinuria and infections. Levy et al. 25 did not find any relationship between the preservation of the upper pole and hypertension. Our data support that nonfunctioning kidneys or upper pole renal moieties do not increase the risk of hypertension or proteinuria. It was also reported that in DSU patients, LUTR can be performed irrespective of the upper pole renal function.6,13 In our series, the renal function of the upper pole did not affect the surgical decision. No evidence leaving NUP in place increased infection or affected the lower pole function negatively.
The primary concern about the LUTR is the risk of a bladder neck injury, especially in young infants. It has not been established whether the ureterocele itself affects bladder development and function or whether interventional surgery causes the dysfunction of the bladder.26,27 No serious complications have been reported in patients with LUTR even under 1 year of age. 28 In our series, incontinence was not detected in any of our patients after toilet training. However, it may be appropriate to postpone the surgery after 1 year of age to avoid complications for such a complex anomaly at this level.
The main limitation of this study is that it is a retrospective review. There is no patient with UPH. We believe that removing an already nonfunctioning upper pole is not beneficial for DSU patients, and we have been managing DSU cases for close to 15 years without UPH. Good results were reported in a limited number of patients without reflux with UPH but in these patients was UPH needed? The procedure alone could not help to resolve obstruction of ureterocele or eliminate BOO and VUR.
Conclusion
DSU is a complex anomaly and it is important to provide the patient with the most accurate, most effective treatment and avoid recurrent interventions. We thought that UI should be performed as the first-line treatment in patients with BOO or severe dilatation of the upper pole. However, UI has limited treatment efficacy in extravesical ureterocele and may cause de novo reflux in patients without VUR which was also confirmed by our data. In cases of high-grade VUR with DSU over 1 year of age, LUTR is the treatment of choice. LUTR is a single-stage and safe procedure, which definitively corrects the main pathology with a single incision. Our results confirmed that UI, LUTR or both of them, if necessary, treat DSU patients of any age, with or without VUR effectively, with low complication rates, and UPH is an unnecessary treatment option for DSU.
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for the study was obtained from SBÜ İzmir Dr. Behçet Uz Children’s Education and Research Hospital Ethics Committee (Approval Number: 437-2020/18-10).
Informed consent
Written informed consent was obtained from the parents for their children’s anonymized information to be published.
Guarantor
A.B.U. is the guarantor of this article.
Contributorship
A.B.U. was responsible for study design, data analysis, writing, editing and gaining ethical approval. A.Ş. was involved in writing and editing. Z.G.T. and Ö.O. were responsible for data collection and searching publish documents. G.S. and M.Ö. were responsible for data collection. All authors reviewed and edited the manuscript, and approved the final version.