
Abstract
Background:
The presence of lower urinary tract symptoms (LUTS) is described as an early symptom of prostate cancer in some patient guidelines; however, a statistical association has never been established.
Methods:
This study was conducted using a prospective electronic database at a single tertiary institution between January 2015 and November 2017. LUTS were assessed using the International Prostate Symptom Score (IPSS), and prostate cancer was graded according to the International Society of UroPathologists (ISUP) grading system. The association between IPSS and Grade Group was tested using parametric one-way analysis of variance (ANOVA) with post hoc analysis using Tukey’s honestly significant difference (Tukey’s HSD).
Results:
A total of 611 men attended the One-Stop Prostate Clinic (OSPC) and IPSSs were available for 557 men. Overall, 46% had mild LUTS (IPSS: 1–7), 38% had moderate LUTS (IPSS: 8–19) and 16% had severe LUTS (IPSS: 20–35). Almost 85% proceeded to have transrectal ultrasound (TRUS) prostate biopsies, and clinically significant prostate cancer (CSPC) was detected in 37% with mild LUTS, 35% with moderate LUTS and 42% with severe LUTS. Correlation between histopathology and IPSSs was assessed in all 78.8% of men who had IPSS data available and underwent prostate biopsies.
Conclusion:
This large series did not establish any correlation between LUTS and prostate cancer in men undergoing investigation for the suspicion of prostate cancer.
Level of evidence:
Not applicable
Introduction
Prostate cancer is the most diagnosed cancer in Australia, accounting for an estimated quarter of cancer diagnoses and 12% of cancer deaths. The incidence of prostate cancer increases with age. 1 Likewise, the incidence of male lower urinary tract symptoms (LUTS) increases with age. This relates to several factors, including the rising incidence of benign prostatic hyperplasia (BPH) and overactive bladder with age.2–4
The concurrent increases in the incidence of both LUTS and prostate cancer with age cause difficulty in determining a definite association between the two. Another confounding factor is that the prostate cancer diagnostic pathway includes both asymptomatic men who undergo prostate-specific antigen (PSA) screening, as well as men who present with symptoms that may be related to prostate cancer, which traditionally has included LUTS, who undergo PSA testing. The majority of prostate cancer detected from needle biopsy is located in the peripheral zone, 5 while symptomatic BPH mainly arises from the transition zone of the prostate. 6 Given these differences in origin, concomitant increased incidences with age, and differences in diagnostic pathways, the link between LUTS and prostate cancer is somewhat uncertain. 7
Methods
A consultant-led same-day prostate cancer diagnostic workup clinic was established in 2011 at a tertiary public hospital in Western Australia called the One-Stop Prostate Clinic (OSPC) to overcome the travel-and-access barriers to prostate cancer diagnostics facing rural and remote men in Western Australia.8,9 Referral criteria to the OSPC were either two age-related abnormal PSA levels (without evidence of urinary tract infection) or abnormal digital rectal examination (DRE) irrespective of PSA level. As part of their urologic assessment at the OSPC, a baseline American Urological Association (AUA) International Prostate Symptom Score (IPSS) method was completed (symptom scores were grouped into mild (1–7), moderate (8–19) and severe (20–35) categories), providing an opportunity to prospectively investigate the link between LUTS and prostate cancer, in men referred regarding a clinical concern of underlying prostate cancer.
Transrectal ultrasound (TRUS)-guided prostate biopsies were performed, and a standard 14-core systematic template was generally employed – two cores from each side of the base, mid and apex of the prostate and a single core from each side of the transition zone. Histopathology results were recorded as the highest Gleason score from all prostate cores taken and assigned a Grade Group as per the 2014 International Society of UroPathologists (ISUP) grading system. 10 Clinically significant prostate cancer (CSPC) was defined as ISUP Grade Group 2 cancers or above. Benign prostatic tissue, high-grade prostatic intraepithelial neoplasia (HGPIN) and atypical small acinar proliferation (ASAP) were all classified as benign for the purposes of this study. All prostate biopsy samples used in this analysis were reported by the same pathology service provider.
SPSS Version 25® (IBM, Endicott, NY, USA) was used to perform analysis of associations and statistical significance between mean IPSSs (LUTS) and prostate cancer using parametric and non-parametric tests. The level of statistical significance was set as p < 0.05.
Non-parametric tests were used in the statistical analysis of mean IPSSs for each Grade Group. The Mann–Whitney U-test was used for comparison of IPSS mean scores between Grade Groups in comparison with benign pathology. Kruskal–Wallis testing was used to compare the mean IPSSs of all Grade Groups. IPSSs were categorised into mild, moderate and severe compared with Grade Groups analysed using Pearson’s chi-square test.
The association between IPSS and Grade Group was also tested using parametric one-way analysis of variance (ANOVA) with post hoc analysis using Tukey’s honestly significant difference (Tukey’s HSD).
Human Research Ethics approval was obtained from the University of Western Australia along with institutional governance approval.
Results
Data were available for 611 consecutive men that attended the OSPC between January 2015 and November 2017, and IPSSs were available for 557 (91.1%) of these men. Age, PSA and IPSS data are reported in Table 1. Both IPSS and histopathology results were available for 482/611 (78.9%) men. In total, 223 men (46%) reported mild symptoms, 187 (39%) men reported moderate symptoms, and 72 (15%) men reported severe symptoms.
Age, PSA and IPSS data.
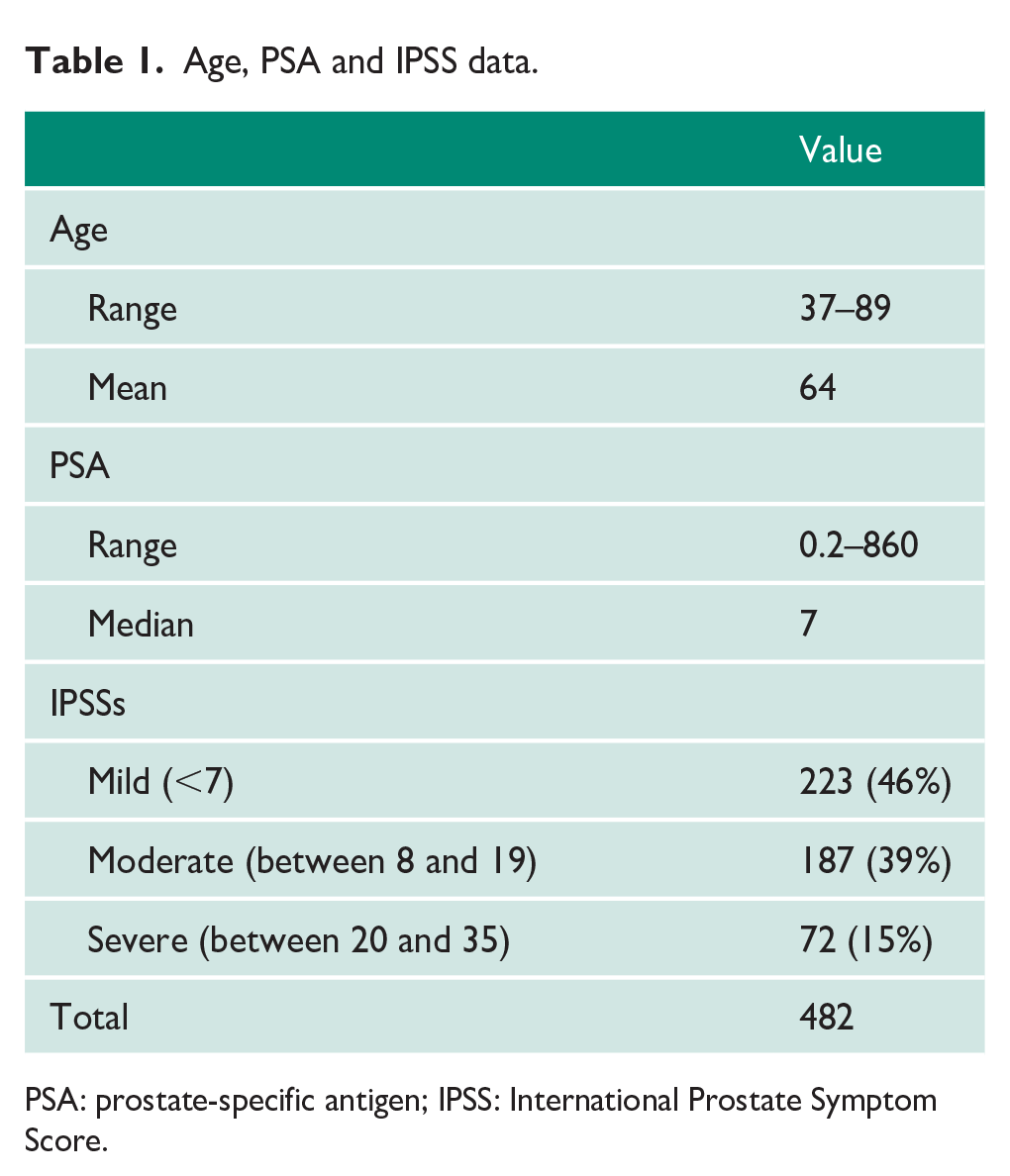
PSA: prostate-specific antigen; IPSS: International Prostate Symptom Score.
IPSSs across histopathology groups were assessed for normality of distribution. Table 2 reports the ANOVA descriptive analysis of mean IPSSs against each histopathology group.
One-way ANOVA analysis testing IPSS for prostate cancer Grade Group.
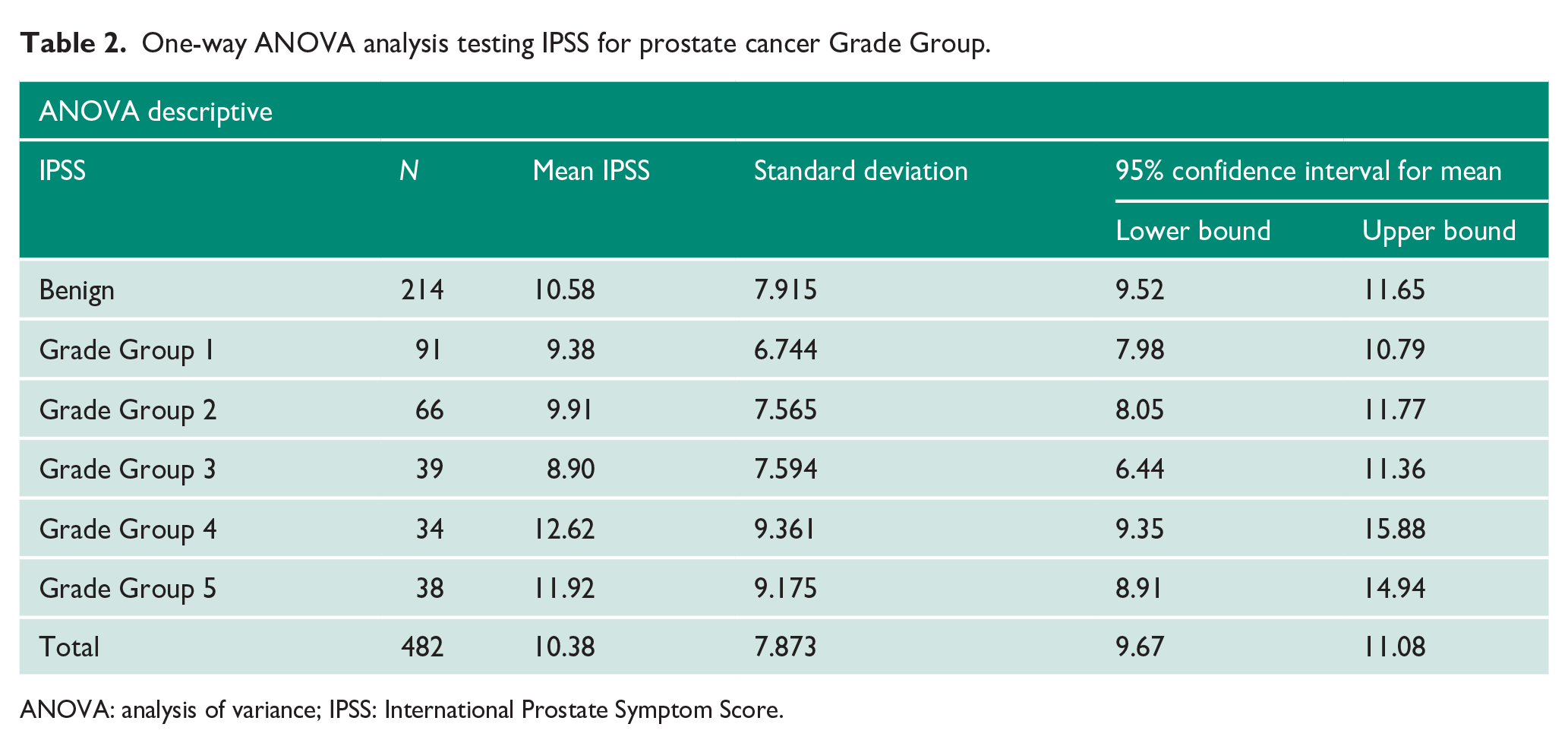
ANOVA: analysis of variance; IPSS: International Prostate Symptom Score.
Comparison of IPSS categorical groups (mild, moderate and severe) with ISUP Grade Groups using Pearson’s chi-square analysis did not reveal any statistically significant differences (p = 0.243).
Correlation between the IPSS and the histopathological outcome for men who underwent prostate biopsies and had IPSS data available is reported according to ISUP Grade Group in Table 3. Mann–Whitney U analysis comparing mean IPSSs of benign histopathology against all prostate cancer (Grade Groups 1–5) did not reveal any statistically significant differences (p values: 0.161–0.569). Furthermore, the Kruskal–Wallis U test did not demonstrate any statistically significant differences between mean IPSSs across individual Grade Groups (p = 0.414).
IPSS and Grade Group comparison.
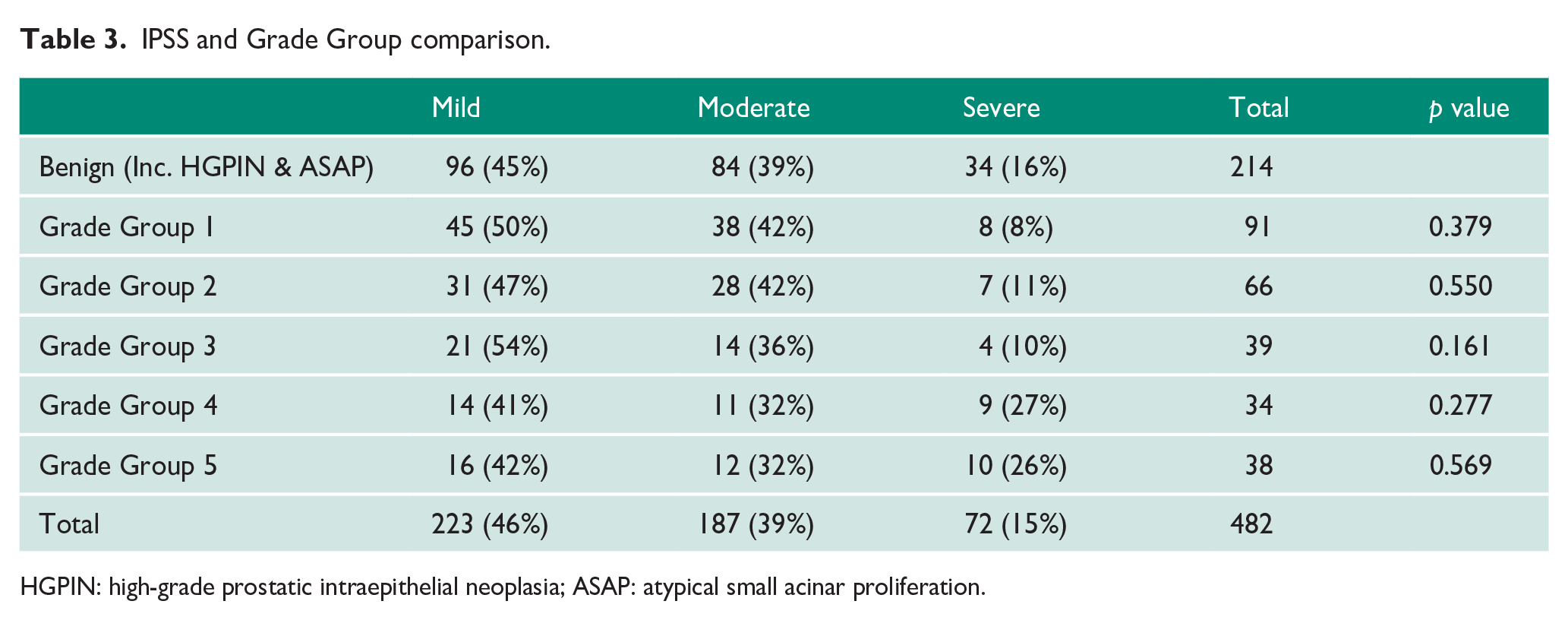
HGPIN: high-grade prostatic intraepithelial neoplasia; ASAP: atypical small acinar proliferation.
Parametric testing comparing IPSS means across histopathology groups were also undertaken. The one-way ANOVA test demonstrated no statistically significant differences in mean IPSS between prostate pathology groups (p = 1.91).
Multiple comparisons with Tukey’s HSD post hoc analysis did not find any statistically significant differences in mean IPSS between histopathology groups with p values ranging between 0.317 and 1.
Discussion
It is appropriate that men presenting with LUTS should undergo DRE and PSA testing, given that prostate volume of ⩾31 mL and a PSA of ⩾1.5 ng/mL are at a significantly higher risk of symptoms and clinical progression of BPH. 11 It may also help in the detection of CSPC. In a small but significant number of cases, abnormal DRE detected by the primary care physician, despite a normal age-related PSA, drives referral and subsequent diagnosis of CSPC. 9
Men with LUTS who present to their general practitioner (GP) are frequently concerned that their symptoms are suggestive of prostate cancer and may benefit from assessment, including identification of risk factors such as family history of prostate or breast cancer along with a conversation about the rationale for PSA testing.2,7,12,13 Our study was completed in Western Australia before widespread use of multiparametric magnetic resonance imaging (mpMRI) in prostate cancer diagnosis. Of course, it is now established that if prostate cancer is suspected, mpMRI of the prostate demonstrates high sensitivity in detecting CSPC radiologically informing the necessity for subsequent biopsy. 14
The presence of LUTS and prostate cancer are intertwined, linked to age and hormonal influences. 15 Numerous studies have suggested that there is no statistically significant relationship between LUTS and prostate cancer.16–20 Our data analysis supports no statistical link between LUTS (using IPSSs) and prostate cancer, in men referred due to a clinical suspicion of prostate cancer.
The prevalence of BPH, overactive bladder and LUTS is known to increase as men age.21,22 The mean male age in our data series was 64; therefore, it is possible that many had BPH, overactive bladder or other pathologies contributing to their LUTS. Similarly, those men diagnosed with prostate cancer may have exhibited LUTS owing to the concomitant BPH or other pathologies rather than the prostate cancer.
Conflicting clinician and patient information resources regarding LUTS and prostate cancer further confuse this issue. In clinical practice, acknowledging a lack of association between prostate cancer and LUTS may alleviate psychological distress in men experiencing LUTS.
Table 4 summarises clinician guidelines from Australia, New Zealand and the United Kingdom with regard to the association between symptomatic (LUTS) and the risk of underlying prostate cancer. It gives an indication that there is clinical inconsistency across jurisdictions as to the relevance of LUTS in the context of prostate cancer risk assessment.
Clinician guidelines from Australia, New Zealand and the United Kingdom demonstrating the association between presence/lack of LUTS and the risk of or presence of prostate cancer.
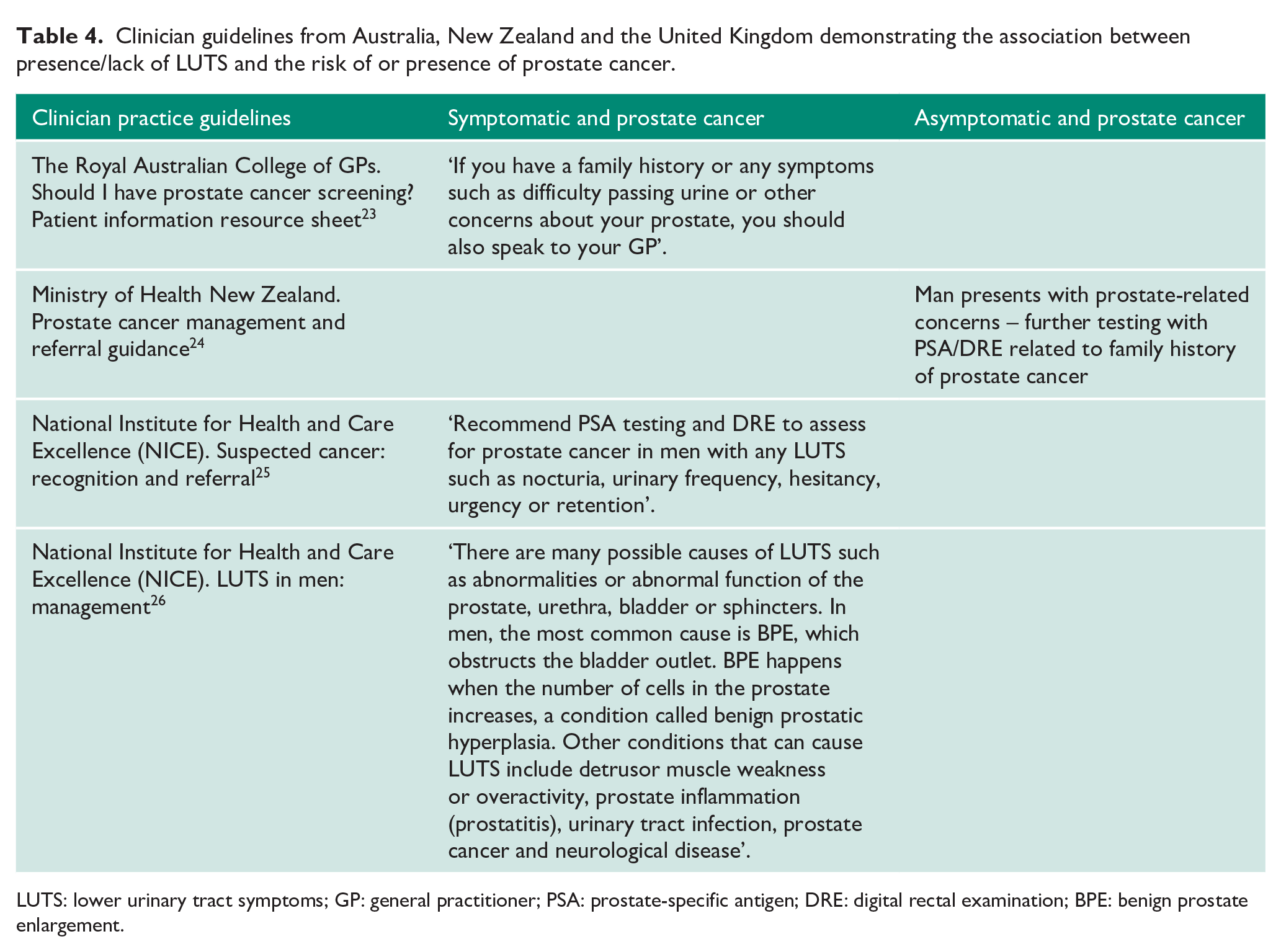
LUTS: lower urinary tract symptoms; GP: general practitioner; PSA: prostate-specific antigen; DRE: digital rectal examination; BPE: benign prostate enlargement.
Patient information sources are summarised in Table 5. There appears to be inconsistency both among different sources and within sources about the relevance of LUTS as an indicator of prostate cancer. These sources often include a distinction about whether the presence of LUTS an early or late symptom of prostate cancer, but overall men could be expected to conclude that LUTS can be indicative of prostate cancer (either as an early or late presentation).
Summary of patient information resources.
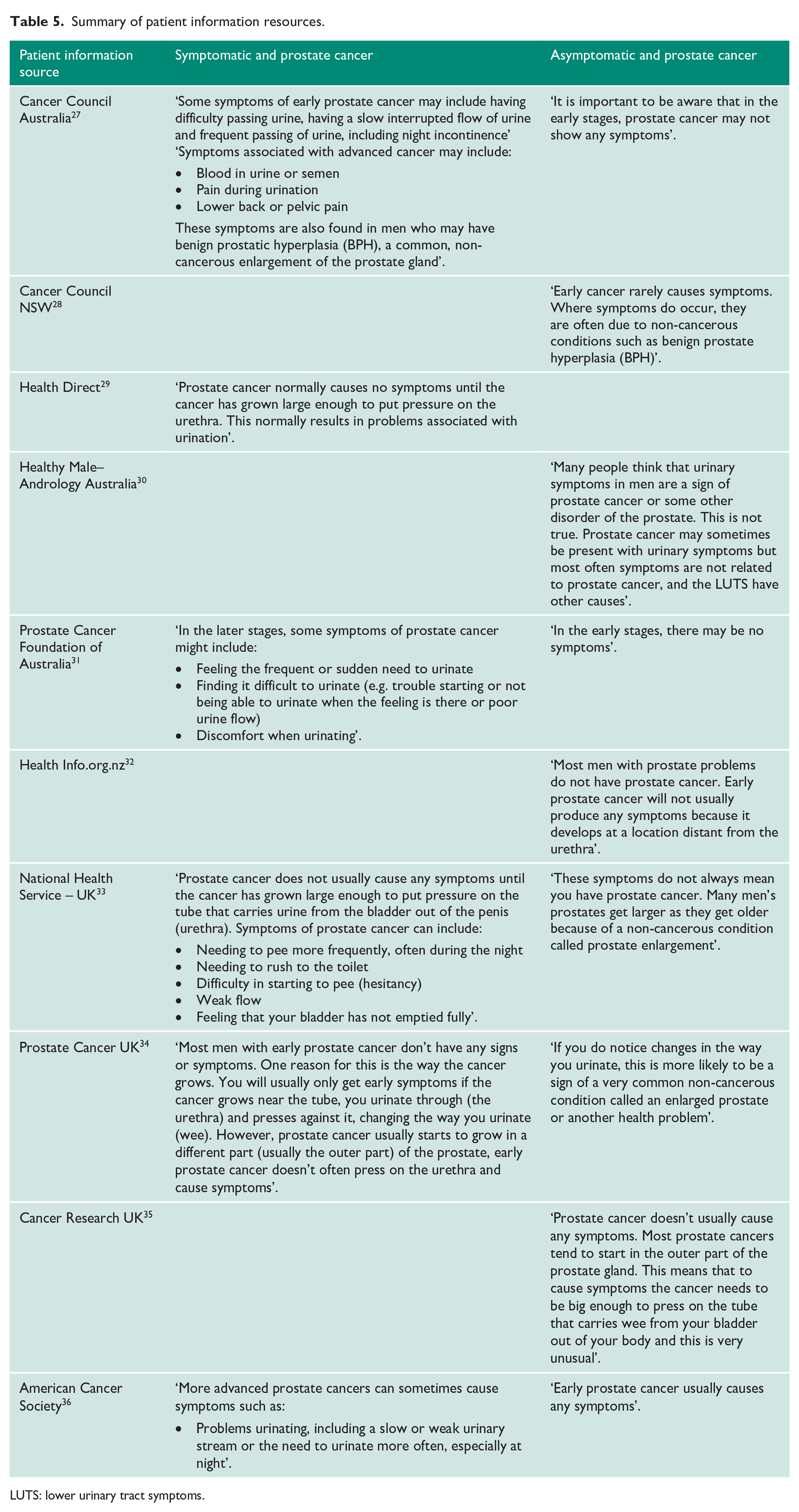
LUTS: lower urinary tract symptoms.
Limitations of the study
This was a prospective study of men referred regarding a clinical concern of underlying prostate cancer; the high incidence of CSPC in this population may therefore have affected the ability of this study to detect a correlation between LUTS and CSPC. Another limitation is that these data cannot be applied to all men with LUTS, as the patients in this study only included men with a clinical suspicion of prostate cancer based on an elevated PSA or abnormal DRE. The association between LUTS and prostate cancer is expected to therefore be even weaker in men without a raised PSA or abnormal DRE. Another limitation is the sample size, which may have been too small to detect subtle associations between LUTS and prostate cancer for sub-analyses for individual ISUP Grade Groups.
Conclusion
Our large prospective data series has not demonstrated any correlation between LUTS and prostate cancer, in men referred due to a clinical suspicion of underlying prostate cancer, which is consistent with other reported studies. Some patient resources may be interpreted as describing a link between LUTS and prostate cancer, and efforts should be made to dissociate this widely considered association that may cause psychological distress for men with LUTS.
Men seeking advice regarding assessment and management of LUTS is an integral part of care in the primary health setting. BPH is the commonest cause for LUTS, but due to its prevalence, prostate cancer may frequently co-exist. It is the authors’ view that DRE and PSA testing are appropriate in all men presenting with LUTS as both PSA and DRE have a genuine role in guiding the management of BPH and may further diagnose a CSPC. These consultations also offer GPs the opportunity to reassure patients, interrogate risk factors for prostate cancer including family history and refer patients to an urologist for further discussion or management.
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Human Research Ethics approval was obtained from the University of Western Australia (RA/4/20/5088). South Metropolitan Health Service Human Research Ethics Committee approval number 15-034-1.
Informed consent
Institutional ethics approval and governance were obtained, and informed consent was not required given all data were unidentifiable.
Contributionship
M.A.Z. reviewed and edited the manuscript. C.H. responsible for data collection, analysis and writing the manuscript. S.F. responsible for data collection and analysis. A.M. responsible for data analysis and writing the draft manuscript. S.P.M. reviewed and edited the manuscript. M.B. responsible for supervision. D.H. responsible for supervision, review and editing of the manuscript.