
Abstract
Artificial intelligence (AI) is a set of computational methods that interprets the data given, uncovers the underlying patterns associated with the complexity of data, and provides the prediction of outcomes that have become increasingly relevant in urology. The current application of AI in urology predominately focuses on disease diagnosis and risk factor analysis in urologic oncology and male infertility. While many candidate models have been proposed in the literature, efforts to construct clinically meaningful data by incorporating patient-specific and multidisciplinary approaches should be carried out to improve the clinical applicability of AI in driving personalised treatment planning and disease prognosis. Looking forward, AI has the potential to drive targeted training in urology, from surgical techniques to patient-specific surgical procedure simulation, in combination with other technologies such as augmented reality. In order to achieve this, patient involvement should be considered in the model development stage, which also addresses issues surrounding the ethical deployment of AI in the clinical environment. It is possible to see AI playing a collaborative role with surgeons in improving clinical efficiency in the future.
Artificial intelligence (AI) is a form of advanced computational methods poised to reshape medical data analysis in the era of big data. Its superiority over traditional analysis, such as logistic and linear regression, lies in its ability to process multimodal data, including clinical, laboratory, and imaging data, which simulates the multidisciplinary clinical decision-making process. 1 The potential use of AI in urology spans from diagnosis and prognosis prediction in the clinical setting to simulation training in surgical specialities and accommodating the educational needs of surgeons in training. Although it is apparent that the current benefit of AI lies in increasing diagnostic accuracy and enhancing efficiency in the clinical workflow, essential issues surrounding the large-scale deployment of AI in urology, such as the explainability of the technology and the ethical implications, should be addressed.
Current involvement in urology
The current use of AI in urology largely falls into two purposes: the diagnosis of diseases and the prediction of patient outcomes, with urologic oncology and male fertility being the focus of the use of AI in urology.2,3
AI’s diagnostic applications involve pathological lesion identification, radiological imaging recognition, and risk stratification. Namely, Campanella et al. 4 employed around 25,000 prostate core biopsy slides to train a computer-aided system that allows pathologists to exclude more than 75% of disease-negative slides while retaining a 100% sensitivity in detecting clinically significant prostate lesions. This would increase the efficiency of slide processing and aid non-subspecialised pathologists in their training. When considering the generalisability of AI predictions in prostate cancer biopsies, Bulten et al. 5 maintained a quadratically weighted kappa agreement of over 0.860 when validating their AI model in cross-continental cohorts.
Computer-aided multiparametric magnetic resonance imaging (mpMRI) prostate cancer diagnosis is currently a significant focus in AI research, with more than 30 articles published.6,7 Promising results were reported in AI identifying predefined lesions. However, its limitation to clinical deployment lies in the limited number of disease-positive cases in the training data sets, such as transitional zone cancers. 7 Poor adherence to reporting data sets used in the development of models was highlighted, which hinders the cross-validation of models with similar data sets. 6
In other urological cancers, Hattab et al. 8 proposed an AI-powered soft-tissue registration system to better visualise tumours and vascular structures for robotic-assisted renal cell carcinoma surgeries. When considering the use of non-imaging data in the detection of bladder carcinoma, Sapre et al. 9 reduced the cystoscopy rates in the validation cohort by 30% with the aid of AI-based analysis in the microRNA profiling of urine when comparing its performance characteristics to that of cystoscopy.
When considering the use of AI in outcome predictions, common involvement includes predicting treatment outcomes and disease prognosis.
To increase patient involvement in prostate cancer treatment planning, Auffenberg et al. 10 developed a machine-learning model from a quality improvement consortium. The model demonstrated high accuracy for predicting prostate cancer treatments based on patient characteristics (area under the curve (AUC) = 0.81) to deliver personalised treatment planning. Moreover, factors influencing surgical success and hospital length of stay prediction may also contribute to patient-focused treatment planning in urological cancer treatment. 11
Fertility outcome prediction has received much interest in AI research over the past decade. Girela et al. 12 employed a neural network system to study the combined effect of environmental, modifiable, and non-modifiable risk factors in determining fertility potential in men. Furthermore, Ramasamy et al. 13 investigated preoperative clinical parameters for men with non-obstructive azoospermia multivariable logistic regression. Both studies pioneered the field of AI research in male fertility, although the accuracy of the prediction models was limited.
Future development and applications
In the next decade, specialties with strong technological involvement such as urology will likely see an increased application of AI. However, as AI starts to be widely incorporated into clinical applications, several critical ethical and practice considerations should be addressed for patients and clinicians. 14
Clinically meaningful AI prediction relies on the quality of input data reflecting a disease’s diagnosis, treatment and prognosis. Therefore, during the data selection stage (Figure 1), clinicians should identify all factors relevant to a specific prediction task involving clinical, laboratory, imaging, and patient-reported data. The AI models based on these would better mimic the clinical decision-making process, advising results more generalisable to real-life clinical tasks. 1 To illustrate, Auffenberg et al. 10 have emphasised patient demographics, Prostate Specific Antigen value, and biopsy score in their prediction model to aid the patient’s diagnosis. However, imaging, treatment, and patient preferences were lacking in the data set, limiting its role in driving more patient-specific predictions. When considering the trustworthiness of AI-generated results, one key drawback may come from the patient groups, perhaps the most significant stakeholders in AI. In order to improve the trust surrounding the AI model, the earliest involvement of the patients is desirable to ensure a thorough review of the data inputted truly reflects on the patient journey, which specifies the treatment expectations and the perceptions of the impact on the quality of life. 15
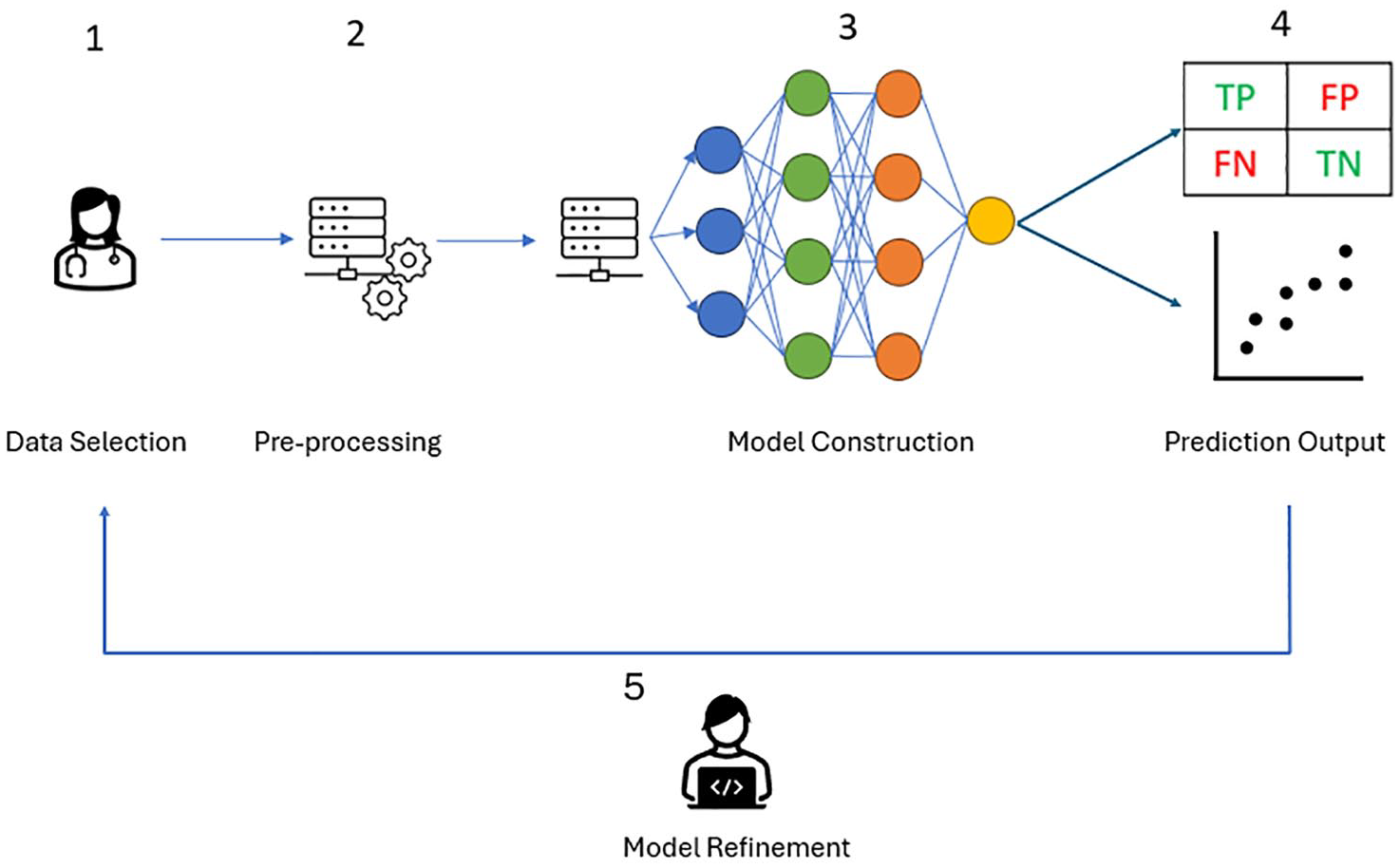
Overview of AI model construction. A human physician selects the data relevant to the prediction problem (1). The data is then preprocessed manually better to prepare the data for AI construction (2). Then, the AI model automatically disseminates the data inputted and learns the connection (lines) between different features (circles) of the data (3). The predictive performance is compared with the ground truth to generate true positive, false negative, true negative, and false positive results for diagnostics or regression-based prediction for multiple predictive factors (4). Finally, the development team should review the model performance and the inputted data to achieve clinically meaningful predictions (5).
The explainability surrounding the computational process of AI decision-making should be addressed when developing AI models. The complexity of the AI model’s construction means it is difficult to extract the precise methods for its decision-making process, known as the black-box phenomenon. 1 Without clear reasoning from the AI in reaching its conclusions, it contradicts the General Medical Council (GMC) Good Medical Practice rules that a doctor must be prepared to explain and justify her decisions. 16 If she uses an AI model but cannot explain it to the patient or colleagues, impending ethical questions would be raised about patient safety. This caveat is the bottleneck for faster deployment of AI models as more sophisticated AI models handling multidisciplinary data (such as clinical, biochemical, and imaging data) tend to come along with the said black-box phenomenon.
Moreover, if AI models were to be deployed prematurely and mistakes soon followed, the delicate doctor–patient relationship may be broken. In any healthcare setting, a wrong decision may break the rapport between a patient and a doctor. However, suppose an AI-generated mistake occurs, and its developer cannot locate the source of the mistake due to its black-box methodology. In that case, this may damage patients’ confidence in clinicians and the use of AI in medicine.
With a robust development, assessment and deployment strategies in place, the potential of AI in urology may expand beyond clinical applications. AI in surgical education and training has recently rocketed in research and development. In particular, current studies focused on benchtop tasks such as suturing and knot tying with kinematic and video data from the surgeon’s external sensors. 17 The application remains to differentiate operator experiences, such as medical students and senior surgeons. Owing to the restricted methods of motion capturing, the full potential for using kinematic data is yet to be fully explored in surgical technique teaching. Integrating AI in virtual reality (VR) and augmented reality (AR) paves another path for surgical education. Aimed to simulate the three-dimensional view of the real-world environment, VR and AR have already been widely deployed in instrumentation and surgical procedure training in urolithiasis. 18 With the incorporation of AI, AR users may be able to personalise their education needs based on the performance of the training sessions. Even more, when simulating the procedure steps for their patients ahead of the surgery, surgeons may use AI to build a virtual model of the patients to familiarise them with their specific disease characteristics to improve the success rate. Such is possible when considering the application of AI and AR in robotic surgery. 19
For AI technology to be widely deployed in urology, laying the foundation of AI literacy is vital for clinicians, as outlined by a recent National Health Service (NHS) and Health Education England (HEE) report. 20 Training for foundation-level knowledge may start with understanding the updated definition of AI, namely the description of deep learning by LeCun et al. 21 Next, we need to understand the current involvement of AI projects in urology (Supplementary Table 1) and appreciate the data used in the training process to judge the clinical value of the prediction outcomes. This should also involve the understanding of quality assessment matrices extending from the conventional measurements for diagnostic tests such as sensitivity, specificity or AUC values to AI-specific measurements such as F1 score, precision-recall AUC values for machine learning 22 or Dice score for deep learning-assisted imaging recognition system. 23 Factors influencing model prediction bias, such as data imbalance, should be investigated when viewing the data set used to input into the AI model. 22
To conclude, AI is becoming increasingly prevalent in urology. However, before clinicians embrace this newfound technology, key ethical considerations and the clinical feasibility of each AI model should be discussed in the context of the specific prediction task. AI should advocate working alongside clinicians to improve their tasks’ efficiency rather than as a risk to replacing human activities.
Supplemental Material
sj-docx-1-uro-10.1177_20514158241300242 – Supplemental material for Artificial intelligence’s current involvement in urology and future implementation in clinical environments
Supplemental material, sj-docx-1-uro-10.1177_20514158241300242 for Artificial intelligence’s current involvement in urology and future implementation in clinical environments by Yi Zhao, Eva Bolton, Naeem Soomro, Bhavan Rai and Rakesh Heer in Journal of Clinical Urology
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Imperial College London Open Access Fund.
Ethical Considerations
No ethical considerations apply.
Guarantor
Y.Z. is the guarantor of this work.
Contributorship
The author contributions include, but are not limited to, the following: Y.Z. wrote the manuscript; Y.Z. B.R. and R.H. created the study concept; E.B., N.S., B.R. and R.H. provided supervision and guidance; Y.Z. and R.H. checked the manuscript in its current form.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data availability statement
Not applicable
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.