
Abstract
Objective:
To establish current views of British Association of Urological Surgeons (BAUS) members and non-members on global urology and compare findings with its 2016 Urolink survey, to inform future strategic priorities.
Methods:
A 2025 cross-sectional survey, adapted from one carried out in 2016, collected demographic data, global surgery experience, suggested Urolink priorities, and barriers to global health work on a 5-point Likert-type scale, with further suggestions as free text. Quantitative data were analysed descriptively, and subjective data responses, thematically.
Results:
One hundred urologists responded. 38% had previously undertaken urological work in low- and lower-middle-income countries (LMIC), consistent with the 2016 survey. Activity, mentoring, and in-country training were rated the most important Urolink functions at means of 4.5/5 and ~4.5/5, respectively. Advocacy, regional training hubs, equipment support, and reciprocal training opportunities scored means of ⩾ 4.0/5. Key barriers included lack of time, insufficient professional leave, family commitments, and financial constraints. 90% of respondents believed professional leave was important for humanitarian work. 89% of respondents viewed Urolink as important to BAUS’s international profile and 79% expressed interest in remote engagement.
Conclusion:
UK urologists show sustained commitment to global health and have clear preferences for partnership-based, educational, and sustainable models. The findings support expanding long-term institutional links, structured remote training and mentorship, and advocating formal professional leave to facilitate global health activities. Respondents also endorsed reciprocal training opportunities for LMIC and UK trainees, providing a focused framework for Urolink’s future strategy.
Keywords
Introduction
Persistent disparities in surgical care remain a major global health challenge, particularly in low-resource settings with limited essential services. The 2015 Lancet Commission on Global Surgery highlighted the substantial unmet surgical need in low- and lower middle-income countries (LMICs). 1 In sub-Saharan Africa, the urology workforce is extremely limited 2 despite a high burden of urological disease, 3 some nations having as little as a few urologists per million people, in contrast to far higher ratios in high-income countries (HICs) such as the United Kingdom. 4 This reflects wider patterns of surgical inequity,5,6 contributing to avoidable morbidity, mortality, and economic loss when urological conditions go untreated. 3
The Lancet Commission, and subsequent initiatives, emphasise capacity building, workforce expansion, and sustainable cross-system partnerships as key to closing these gaps, 1 although these may be considered unachievable within the health budgets of many LMICs. BAUS established Urolink more than 30 years ago to support urological care through training, mentorship, equipment support, and institutional partnerships, delivered with sensitivity to local cultural, religious and operational contexts in LMICs. 7 The UK urological commitment to Urolink’s ethos has been strong, with a 2016 survey showing over 40% of members that completed the survey participated in some form of overseas working. 8
Global surgery has progressed since 2016. There is now far greater emphasis on sustainable, bidirectional partnerships and on building local capacity through longer term relationships. Twinning, establishing long-term institutional links between high- and low-income centres, has been central to Urolink’s approach since its inception and is now a widely adopted model in global surgery.9,10 Technological advances have also complemented existing models with remote mentorship and virtual multi-disciplinary team meetings (MDTs), both during and after visits, now commonplace. 11 Since the COVID-19 pandemic the delivery of virtual webinars has provided sustained benefit by allowing teaching and training to be delivered when face-to-face visits were, or are, not possible and encouraging a further generation of young urologists to become involved with global urology. 12
In 2025, Urolink surveyed the UK urologists again to assess their current view of global health and compare those results with those results from 2016. The intention was to help shape Urolink’s strategy for the next decade and to determine its ongoing priorities.
Methods
Study design and survey instrument
A cross-sectional online survey was conducted in mid-2025 of UK urologists, both members and non-members of the British Association of Urological Surgeons (BAUS). No exclusions were made dependent upon protected characteristics or occupational status. The survey instrument was adapted from the 2016 survey, retaining the core domains: demographic data, global surgery experience, reasons for involvement, barriers to involvement, and opinions on Urolink’s relevance to its parent organisation, BAUS. In addition, it included novel questions about individuals’ interest in virtual engagement, such as online teaching or hosting overseas colleagues remotely, and preferred methods for receiving Urolink news and updates.
The survey had both quantitative and qualitative components. Closed-ended questions included multiple-choice items and 5-point Likert-type-scale ratings. These assessed respondents' perceptions of each Urolink activity (from 1, ‘not at all important’, to 5, ‘very important’). Respondents also rated the significance of barriers to participation. Open-ended free-text fields were added to collect comments, suggestions, and explanations of motivations or obstacles.
Data collection and analysis
The questionnaire was distributed electronically to all BAUS members via newsletters and informally to non-members through social-media communication channels. Participation was entirely voluntary, and responses were anonymised. No identifiable data were collected, and informed consent was implied by the act of responding to the survey.
Quantitative data were analysed descriptively. Categorical variables are reported as percentages. For Likert-type scale items, mean scores were calculated, which allowed a comparison of respondents' priorities and challenges. Where appropriate, data from 2025 were compared with the 2016 survey to show trends over time.
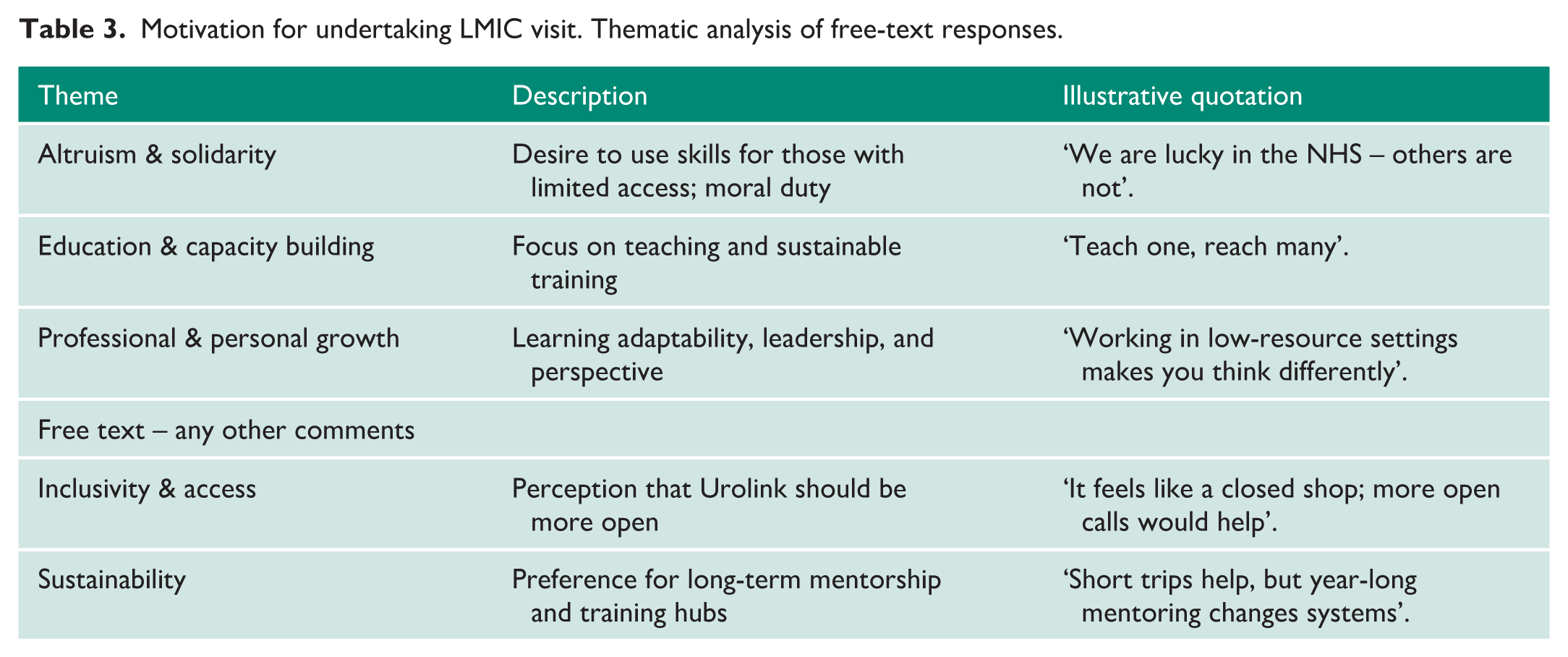
Qualitative data from free-text answers underwent thematic analysis. The research team reviewed responses iteratively to spot recurring themes, motivations, and suggestions. Thematic coding grouped similar answers. Representative quotations are presented to illustrate key themes. Thematic coding grouped similar ideas into five principal categories: (1) altruism and humanitarian motivation; (2) education and capacity building; (3) professional and personal development; (4) inclusivity and access to opportunities; and (5) sustainability and long-term partnership.
Item-level missing data were minimal as all, but free text boxes were compulsory. Analyses utilised all available responses.
This manuscript was prepared in accordance with the STROBE checklist 13 for cross-sectional studies, with all relevant items addressed to ensure transparent reporting.
Results
Respondent characteristics and global surgery experience
A total of 100 urologists completed the 2025 survey (Table 1). Respondents represented all career stages, though most were consultants or senior trainees, with smaller numbers of junior trainees, post-CCT fellows, or retirees. The cohort was predominantly male (about 85%), and over 90% were UK-based.
Respondent demographics and prior global health experience (n = 100).
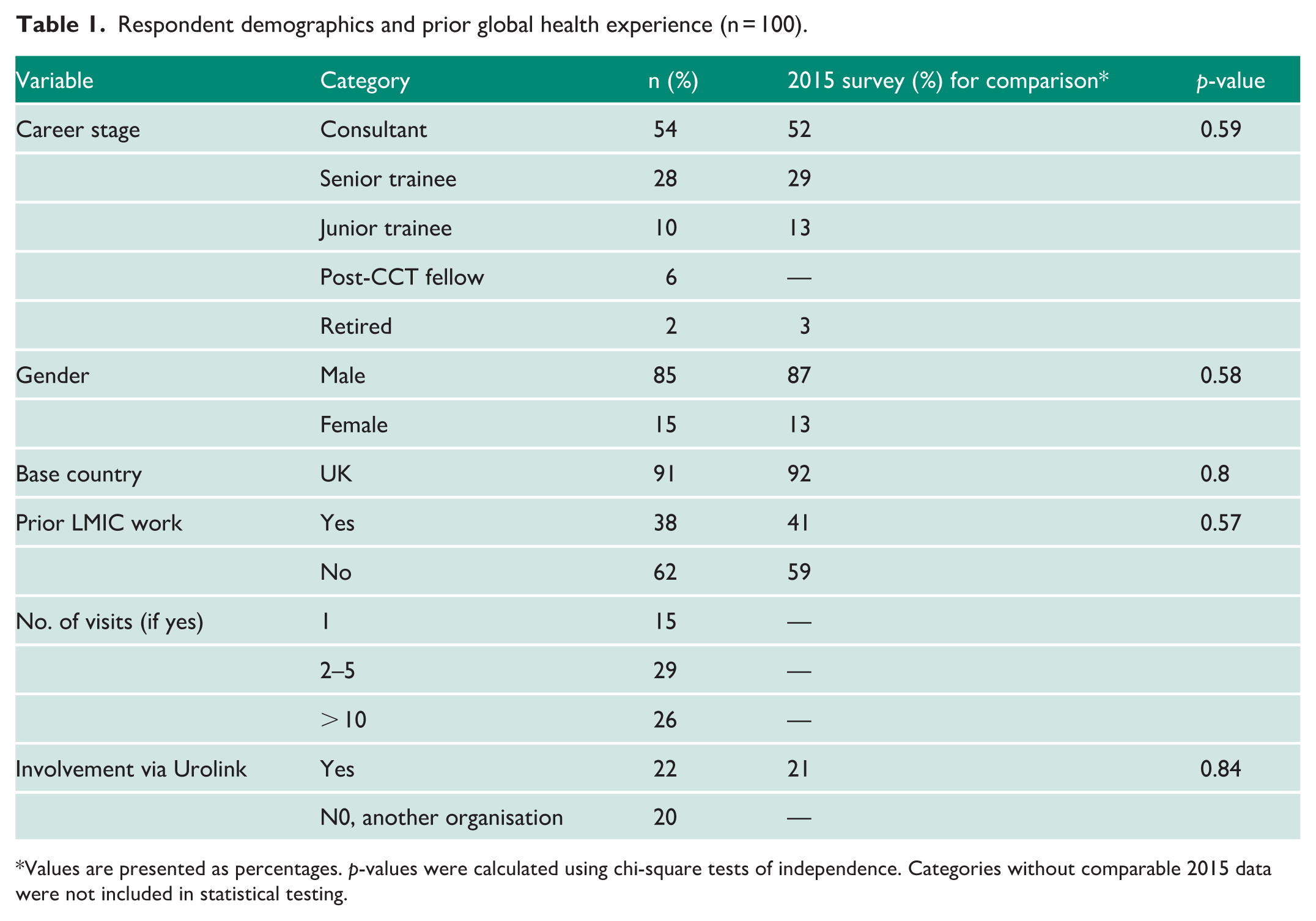
Values are presented as percentages. p-values were calculated using chi-square tests of independence. Categories without comparable 2015 data were not included in statistical testing.
Overall, 38% had undertaken urological work for or had visited LMICs compared against the 41% reported in 2016, indicating sustained UK engagement in global surgery. Among those with overseas experience, 49% had participated in Urolink facilitated activity (n = 22, including four via The Urology Foundation), while others engaged independently or through different organisations. Notably, 34% had completed more than two visits and 29% more than 10%.
56% of overseas visits occurred during consultant careers; however, 39% of those who had participated in overseas activity were specialist trainees.
Of the 35 respondents who had participated in global health work through Urolink in the last 10 years, 17 (48.6%) had been active within the past year, 5 (14.3%) had been active between 1 and 5 years and 13 (37.1%) had not participated for over 5 years.
Perceived priorities for Urolink activities
Survey respondents rated a range of Urolink activities, demonstrating a strong preference for sustainable education and capacity building (Table 2). Mentoring overseas surgeons was the highest-scoring activity (mean 4.5/5), with clear support for structured mentorship programmes linking experienced UK urologists with LMIC colleagues.
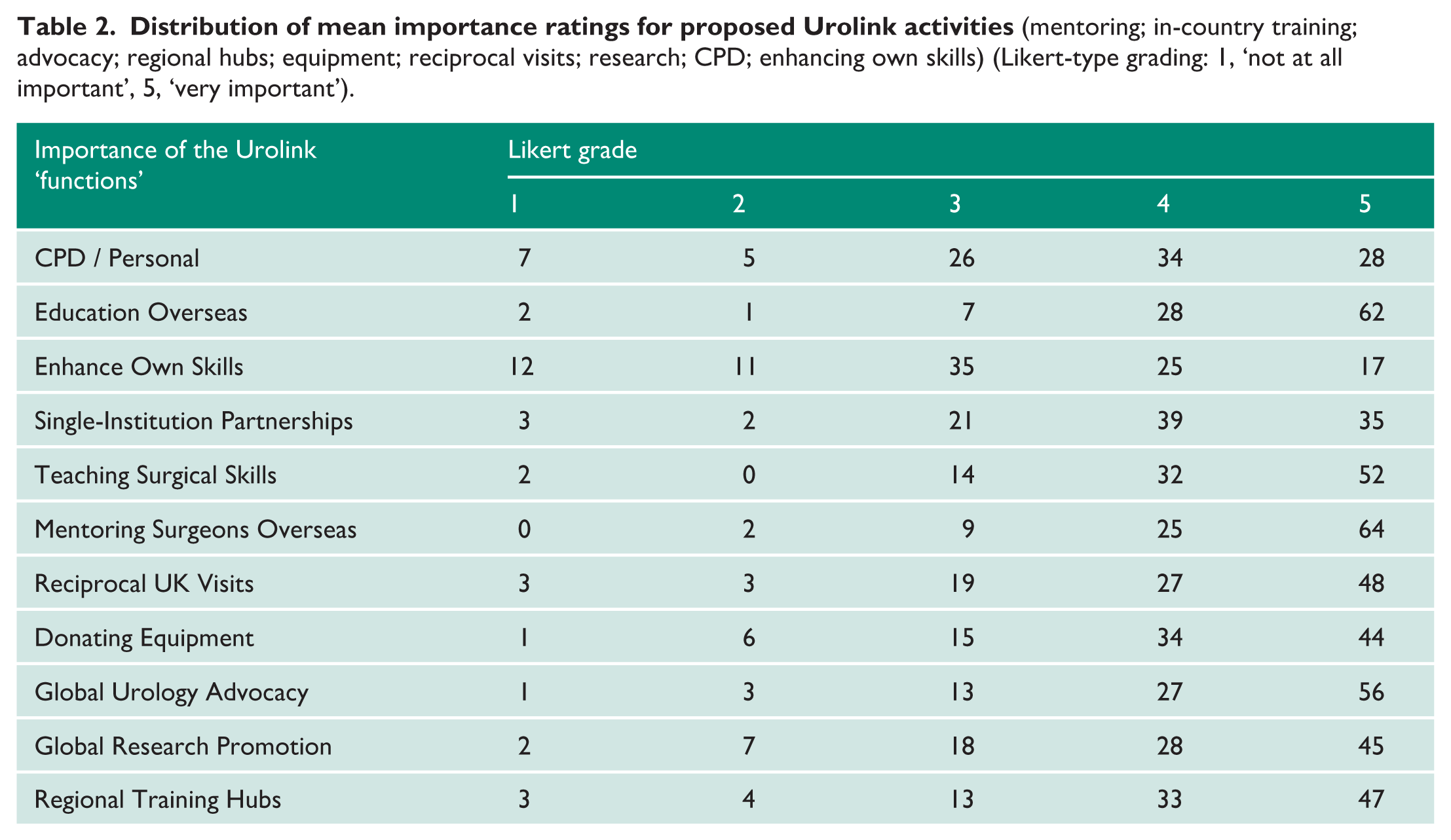
Education and in-country training were also highly valued (mean ~4.5), including lectureships, workshops, and formal surgical skills courses. Teaching operative skills specifically received a mean rating of 4.3, confirming that educational initiatives remain central to members’ expectations of Urolink.
Advocacy for global urological care was rated important (mean 4.3). Establishing regional training hubs (mean ~4.2) and equipment donation (mean 4.1) were likewise strongly endorsed. Free-text comments frequently emphasised the need for sustainable, locally led training centres supported by appropriate and durable equipment provision.
Reciprocal training opportunities were also prioritised. Enabling LMIC trainees to gain exposure in UK centres received a high mean score (~4.1). Similar ratings were given for UK-based exchange opportunities.
Forming long-term institutional partnerships received a mean score of 4.0, reflecting strong endorsement for structured, enduring collaborations. Global urology research was moderately prioritised (mean ~4.1), with over 40% rating it ‘very important’, indicating growing interest in developing an evidence base for global surgical practice.
CPD and professional development for UK surgeons scored lower (mean 3.7), and enhancing personal surgical skills overseas was the lowest-ranked activity (mean 3.2). This suggests that respondents view Urolink’s primary mission as supporting LMIC partners rather than advancing UK surgeons’ technical development.
When asked about Urolink’s contribution to BAUS’s international profile, 89% of respondents rated it ‘important’ or ‘very important’, and only 3% rated it minimally important. Perceived impact on global urological care was also positive, with 37% selecting ‘high’ impact and 40% ‘moderate’.
Regionally, sub-Saharan Africa was identified as the highest priority for Urolink’s work, followed by South Asia. Other regions mentioned included East and Central Asia, the Caribbean, North Africa, and the Middle East. Several respondents emphasised that geographical focus should ultimately be determined by partner-led needs assessments rather than predetermined criteria.
Qualitative analysis
Qualitative analysis of free-text responses further contextualised these patterns and identified several thematic domains. Respondents emphasised the importance of reciprocal training and bidirectional educational exchange, including opportunities for LMIC trainees to visit UK centres support through BAUS fellowships. A second theme concerned the need for structural support within the UK, such as protected or paid leave, to enable participation in overseas work. Long-term capacity building also featured prominently, with calls for sponsorship of visiting LMIC consultants and the development of enduring mentorship structures rather than episodic visits. Geographic expansion driven by partner-identified need was also raised.
Motivations for global health engagement
Analysis of the 70 free-text responses (Table 3) demonstrated that motivations for overseas engagement were overwhelmingly altruistic. 65 of 70 respondents (93%) articulated motivations rooted in humanitarianism, teaching, or capacity building, most commonly describing aims such as ‘giving back’, ‘supporting local surgeons’, and contributing to sustainable urological service development. Teaching and skills transfer appeared in 48 responses (69%), while long-term mentoring or service development was mentioned in 31 responses (44%). Personal or professional development, such as gaining exposure to different health systems or improving cultural competence, was referenced in 18 responses (26%), but always framed as secondary to partner-focused aims. Only three respondents (4%) expressed motivations centred on enhancing their own surgical skills. These were two specialist registrars (ST3–5 and ST6–7) and one consultant. Adventure, cultural exchange, and opportunities for bilateral learning were occasionally noted, while financial or career-driven objectives were entirely absent. Overall, this motivation profile strongly aligns with Urolink’s values of partnership, sustainability, and equitable global surgical development.
Motivation for undertaking LMIC visit. Thematic analysis of free-text responses.
Barriers to participation
Respondents rated the significance of several potential barriers (Table 4). The highest-rated barriers were:
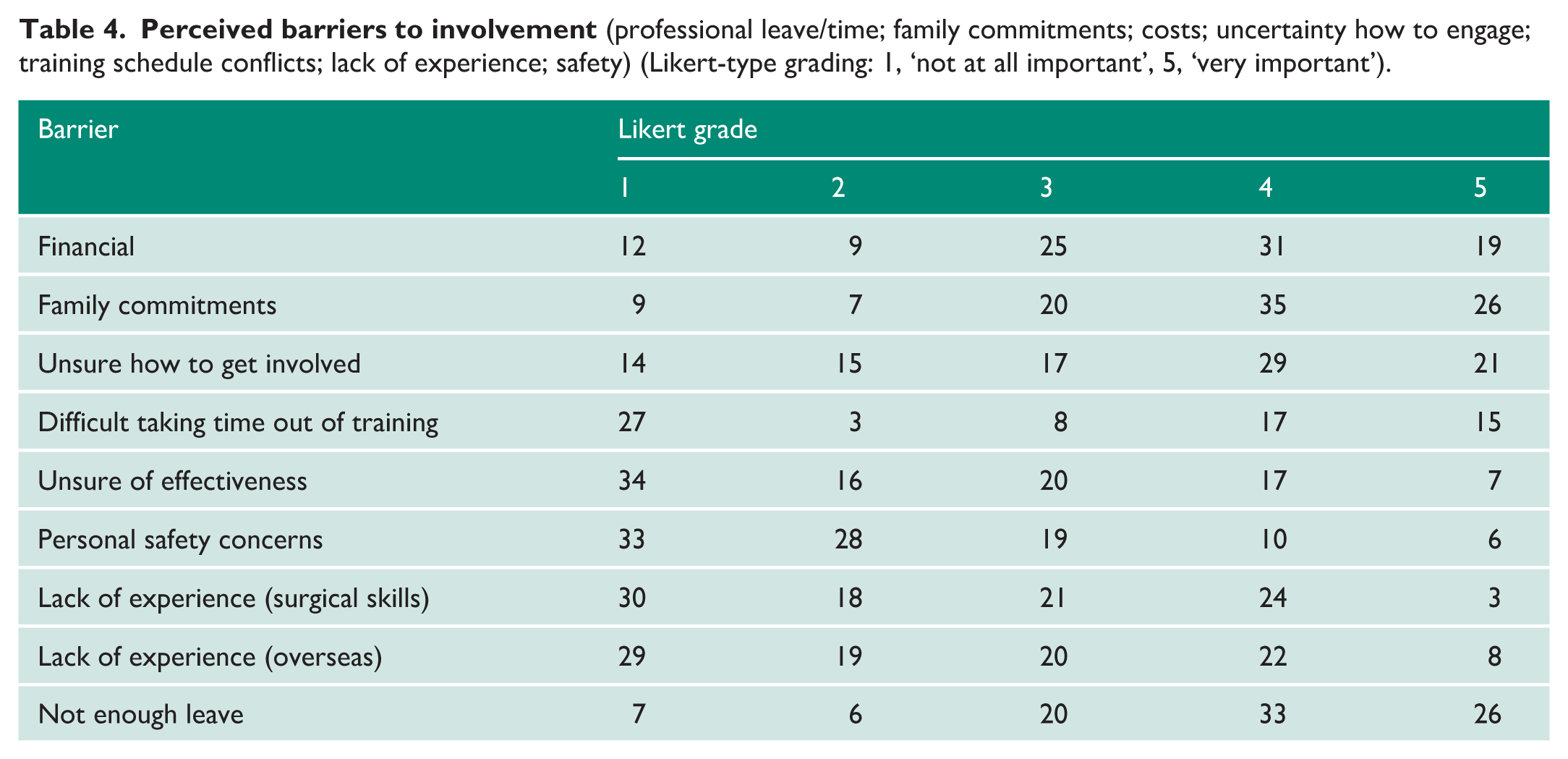
Barriers such as lack of experience or confidence (mean Likert-type grading ~2.6) and personal safety concerns (mean ~2.2) were rated as less significant.
90% of respondents agreed that there should be a form of special professional leave for humanitarian work.
Analysis demonstrated clear age-related variation in the impact of family commitments on participation in global urology activity. Among higher trainees and post-CCT fellows aged 25–34, 52% reported a moderate–severe barrier (scores 4–5). The 35–44 cohort showed a similar but slightly attenuated pattern, with 38% reporting scores of 4–5 and most of the remainder indicating a moderate barrier (score 3). In contrast, only 14% of consultants aged 45–54 reported a significant barrier, with 62% scoring 1–2, indicating a substantial reduction in perceived constraint. Among those aged 55–64, 74% reported minimal barrier scores (1–2), and retired respondents almost uniformly described little or no barrier.
Qualitative analysis
Free-text responses highlighted additional barriers. The most frequent themes were limited awareness of how to get involved and perceptions that Urolink operates as a closed or informal network, making opportunities difficult to access. 10 respondents noted mismatches between their subspecialty skills and the reconstructive expertise often required, alongside local service pressures, staffing constraints, and family responsibilities. Concerns were also raised about the risk of trainees displacing local learners and about navigating local professional dynamics and rivalries.
Communication and engagement preferences
The survey revealed that 73% of respondents accessed Urolink’s web pages, and 38% visited them at least occasionally. 48% accessed the latest Urolink news. Alternative means of gaining knowledge of Urolink’s activity are shown in Figure 1.

Respondent preferred Urolink communication channels.
Interest in remote involvement was high (Table 5): 79% expressed willingness to contribute via online teaching or by hosting overseas trainees, highlighting new avenues for engagement that did not require international travel.
Comparison of key indicators: BAUS Urolink surveys 2016 to 2025.
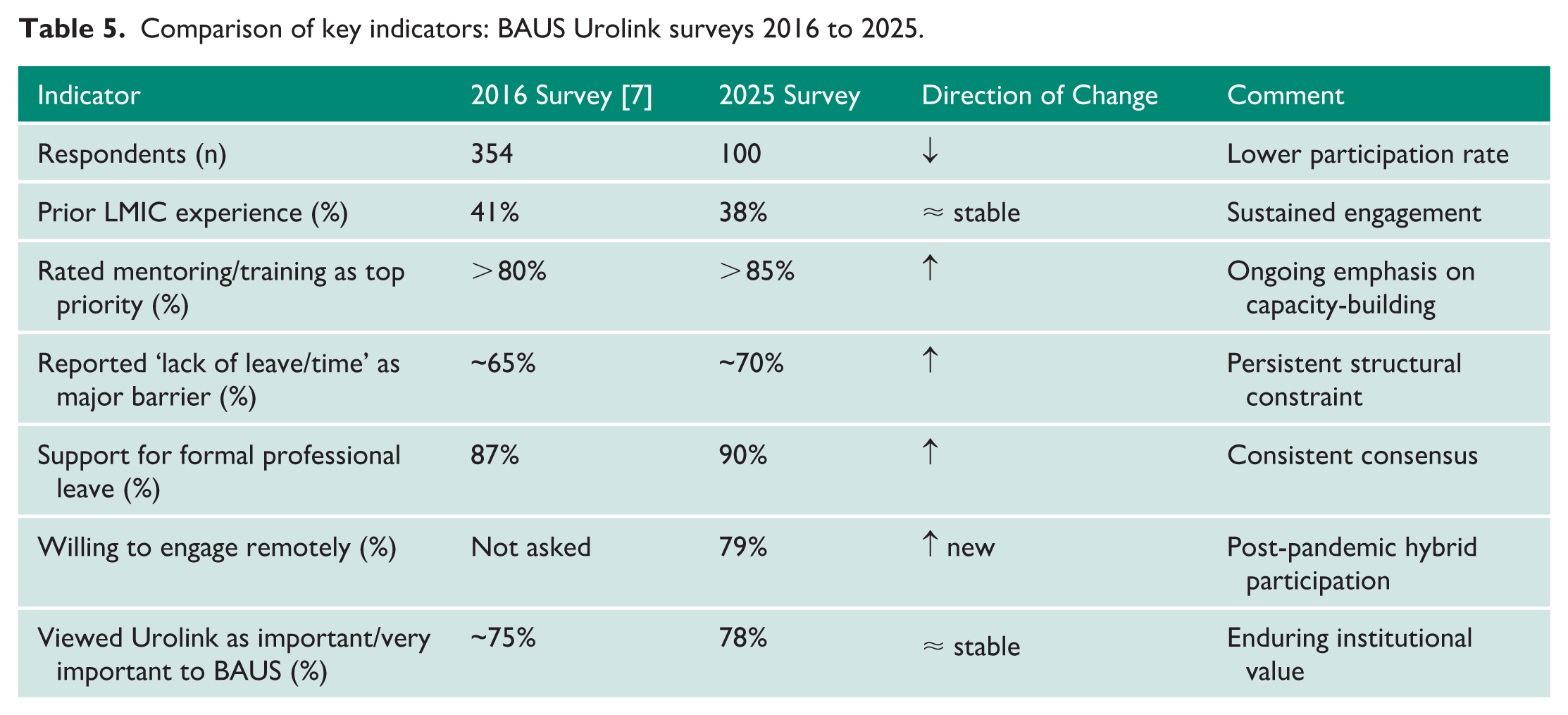
Regarding academic interest, 67% considered research articles on global urology to be ‘Important’ or ‘Very important’, reflecting a supportive climate for the scholarly dissemination of Urolink’s global health contribution.
Free-text suggestions emphasised the need for improved transparency and communication, better advertising of overseas opportunities, increased focus on sustainability and long-term impact, and the expansion of the volunteer base. The establishment of formal equipment donation pipelines and recognition of Urolink activities within BAUS were also advocated.
Discussion
The 2025 Urolink survey reinforces the sustained commitment of UK urologists to global health, mirroring percentage engagement levels reported in 2016. Approximately 40% that completed the survey have undertaken overseas urological work in LMICs in the last 10 years. This indicates that global engagement is now an established element of UK urological practice, rather than a transient interest, and there is evidence of sustained activity among a core group. The survey suggests strong current engagement alongside attrition among previously active members and highlights that considerable global surgical activity occurs outside Urolink’s auspices.
There is a clear shift towards sustainable, partnership-driven models. Respondents prioritised capacity-building activities such as mentoring, education, and the development of regional training hubs over short-term clinical service or individual professional gain. This aligns with contemporary global surgery discourse and the wider move towards localisation of expertise.1,7,9 The emphasis on remote mentorship, shown to be effective, 14 and structured training corresponds with the transition away from episodic ‘missions’ to models that strengthen local systems. 15 Advocacy, institutional partnerships, and appropriate equipment support were also highly valued. 16 Respondents endorsed reciprocal exchanges and long-term institutional links, which produce more durable outcomes than stand-alone interventions. 15 Facilitating LMIC trainees’ exposure to UK centres was viewed as valuable for strengthening partner country capacity and for enhancing UK trainee development. 17
A notable finding since 2016 was the strong willingness to contribute remotely through online teaching, virtual mentorship, and remote hosting. This could expand Urolink’s base and enable flexible, sustainable collaboration. Virtual shared learning during the COVID-19 pandemic, including UK-Zambia webinars, demonstrated that cross-continental education can be effective, clinically useful and conducive to the building of meaningful relationships. 12 Other specialties have also deployed virtual simulation and VR-based training to support LMIC education; 18 remote MDTs and online collaboratives are now recognised as being vital prior to visits for surgical workshops and simulation training. Virtual work should complement rather than replace in-person visits, which remain essential for contextual understanding, trust, and the building of durable partnerships 7 and increase productivity among NHS clinicians when in the host’s country. 19
Preferences for partnership-driven approaches align with the Lancet Commission on Global Surgery’s recommendations and others interested in global health. 1 Our thematic analysis has demonstrated predominantly altruistic motivations, centred on humanitarianism, teaching, and capacity building among Urolink-associated urologists. Personal or professional gain was acknowledged but viewed as a secondary motivator, reflecting findings from work in women’s health and the 2016 survey.7,20
Significant barriers do, however, persist. A lack of time or institutional support, family responsibilities, and financial constraints were the most prominent challenges, consistent with earlier surveys and broader global health literature. 21 Family commitments emerged as a pronounced but time-limited barrier, peaking in early and mid-career and declining with age. This suggests Urolink’s programmes must tailor opportunities, particularly for clinicians aged 25–44, through flexible models to avoid systematically excluding this large cohort. The attrition of 13 urologists with Urolink experience needs to be addressed and methods to re-engage and engage cohorts will remain critical.
Some barriers may be mitigated through expanding digital engagement and emerging technologies such as telesurgery. 22 However, a reported lack of awareness about opportunities for engagement and a perception of exclusivity within, Urolink emphasised the need for greater transparency and openness in its activities and methods of financial support. The preference for BAUS newsletters, the website, and direct email as communication channels provides clear guidance to address this desire for improved visibility.
Views on the domestic benefits of global health work were divided, although wider NHS literature indicates substantial professional gains from involvement in global health involvement. As described by Venn and Payne 23 , Urolink’s partnerships strengthen transferable skills among UK urologists, including leadership, innovation under constraint, and cross-cultural communication. These competencies, developed through teaching, mentoring, and adapting to unfamiliar environments, translate directly into improved teamwork, service redesign, and quality improvement within the NHS. 23 Previous trainees also report accelerated clinical maturity, enhanced problem-solving, and improved teaching and leadership capability through global health involvement. 24
Comparison with the 2016 survey highlights stable engagement but evolving modalities, particularly digital tools and a stronger call for institutional support. The growing emphasis on global urology research, 25 with two-thirds rating it important, suggests academic maturation and opportunities to advance evidence-based practice are evolving objectives for Urolink.
The survey has limitations. The response rate was modest and may reflect selection bias, and survey fatigue among the urological community. The consistency of themes, however, supports the validity of the findings within the cohort which engaged with this study, while the qualitative analysis provides practical insight for organisational development, and strategic restructuring, to embrace the digital world that is omnipresent across the globe (Figure 2).
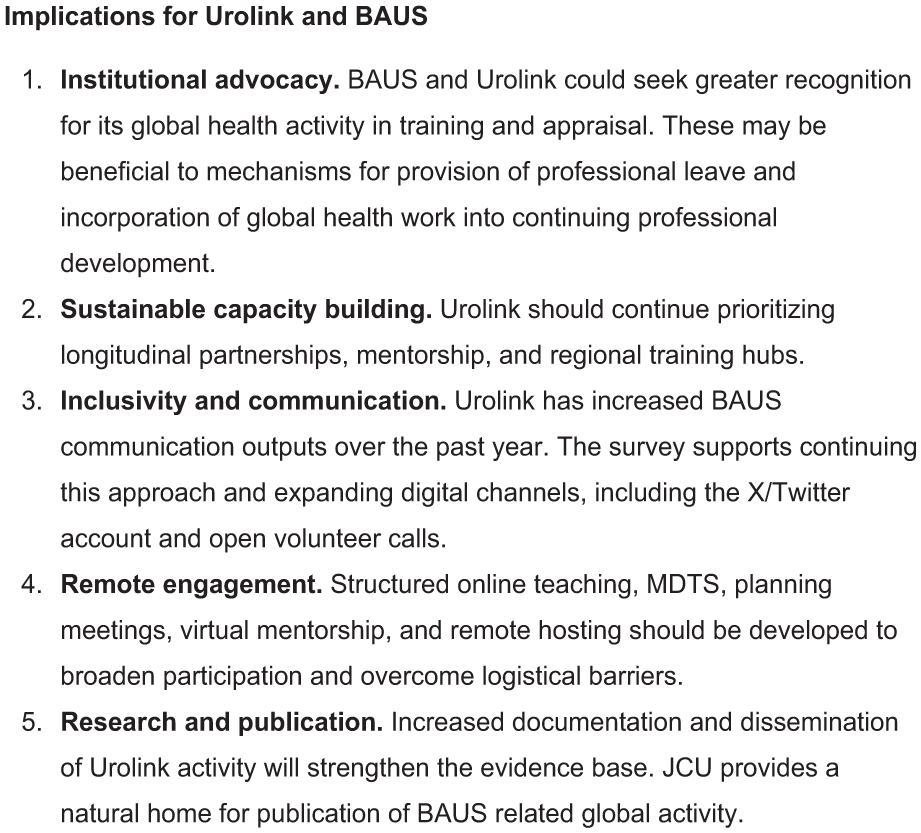
Strategic outcomes for Urolink from the 2025 survey.
Conclusion
The 2025 survey demonstrates sustained enthusiasm for global health among UK urologists, with a strong preference for partnership-based, educational, and capacity-building approaches. Traditional barriers remain. However, there is clear support for developing structures that facilitate participation. Growing interest in digital engagement and global urology research reflects the field’s evolution. To maximise its impact, Urolink should continue aligning strategy with member priorities, advocate for institutional support, and embrace innovative models of collaboration.
Footnotes
Acknowledgements
The authors thank the BAUS secretariat for their assistance in disseminating the survey to members, and the Urolink Committee for their support and oversight. The authors are also grateful to those who completed the survey and contributed free-text responses.
Conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mayur Gami is a funded global health fellow through the Cambridge Global Health Partnerships.
Michael Ng has received funding for a TUF/Urolink Fellowship.
Stephen R Payne has received funding from BJU International, and Urolink, for overseas travel
Shekhar Biyani has received funding from BJU International, and Urolink for overseas travel.
Danielle Whiting has received funding for a TUF/Urolink Fellowship and from the BAUS section of endourology.
Nicholas Campain has recieved funding from Urolink for overseas travel.
Ethical considerations
No formal ethical approval was required for this voluntary, anonymous survey. The project followed standards for professional society surveys. No sensitive or personal data was collected. The purpose was to inform strategy and contribute to the global urology discussion.
This was a voluntary, anonymised professional attitudes survey.
Informed consent
Not applicable.
Consent to participate
Not required.
Consent for publication
Not required.
Data availability statement
Data available on request.
Guarantor
Nicholas Campain.
Contributorship
Mayur Gami and Michael Ng are the primary authors and contributed equally to the conception, data interpretation, and drafting of the manuscript. Stephen R Payne provided senior editorial oversight and critically revised the manuscript for important intellectual content. Susie Venn, Chandra Shekhar Biyani, Danielle Whiting, and Nicholas Campain contributed as senior editors and were responsible for the original concept, study design, and overall structure of the paper. All authors reviewed and approved the final manuscript and agree to be accountable for all aspects of the work.