
Abstract
Introduction:
Over the last decade, simulation-based education (SBE) has evolved from a supplementary training modality into an essential core component of early urology specialty training in the United Kingdom. Introduced in 2015, the ST3 urology simulation bootcamp was designed to address heterogeneity in trainee experience, constrained operative exposure and the heightened anxiety associated with transition into specialty training.
Objective:
The main aim is to evaluate the evolution, structure, educational outcomes and explore the wider impact of 10 years of SBE on early urology careers in the United Kingdom.
Methods:
This narrative review amalgamates published literature, programme evaluations and the longitudinal experience of the UK ST3 urology bootcamp. The development of the bootcamp model, its educational framework, simulation modalities, assessment rubrics and integration within the national training structures are described. Educational and professional outcomes over 10 years are evaluated.
Results:
The urology bootcamp has consistently demonstrated improvement in trainees’ knowledge, technical skills, confidence and preparedness at the point of specialty entry. Multimodal simulation addressing both technical and non-technical skills has supported smoother transitions into clinical practice, earlier engagement in operative opportunities and professional identity formation. Iterative refinement informed by trainee and faculty feedback has enhanced curricular relevance and alignment with real-world needs and demands. The bootcamp model has also been successfully adapted internationally, including in low-resource settings.
Conclusion:
Over the decade, simulation-based urology bootcamp training has become a foundational element of early specialty education in the United Kingdom. By mitigating transitional uncertainties, addressing educational heterogeneity and supporting essential skills acquisition, the bootcamp model offers a scalable, reproducible, evidence-based framework with relevance across surgical specialties and training programmes.
Introduction
Over the past decade, simulation-based education (SBE) in urology has evolved from a novel adjunct to clinical training into a core component of early specialty education.1–4 What began in 2015 as an experimental educational tool, the ST3 (Specialty Trainee) urology simulation bootcamp has transformed into an established, valuable and indispensable element of the UK urological training programme. The traditional Halstead’s learning adage, ‘see one, do one, teach one’, has been refined and supplemented with the advancement of technology, simulation tools and newer surgical education models. 5 This transition reflects broader structural changes in healthcare delivery, surgical training paradigms and societal expectations regarding patient safety and trainee supervision. 6
Over the last decade, urological training has undergone a profound transformation, and multiple factors, such as service pressures (exacerbated by the backlog from the COVID-19 pandemic), increasing subspecialisation and regulations imposed by the European Working Time Directive (EWTD), have resulted in reduced overall clinical and operative exposure.7–10 As a result, early-stage trainees frequently enter specialty training with heterogeneous experience, variable confidence and competencies to manage common urological emergencies and procedures. 11
SBE offers a compelling solution to these challenges. It provides a structured and reproducible environment in which trainees can acquire and rehearse both technical and non-technical skills in a realistic setting without the risk to patients.6,12–15 Educational theories support simulation as an effective modality for learning, especially when it is aligned with principles of active practice and immediate feedback.16,17
After competitive national selection and appointment, the UK urology trainees start their 5-year training programme. The initial period is traditionally associated with increased stress, reduced confidence and heightened risk of errors as this group of trainees’ transitions from supervised core surgical training to the specialty trainee role with greater responsibilities and logistical uncertainties. The ST3 urology bootcamp sought to mitigate this by providing intensive training for both technical and non-technical skills for all newly appointed early-stage trainees, irrespective of their previous experiences, to equip them with the required skill set to begin their specialty training safely. 2
This article aims to evaluate how 10 years of rigorous, simulation-based ‘entry-level’ urology training has evolved and explore the development, structure, outcomes and wider impact of urology bootcamp training and its role in shaping confident and competent urologists.
Development of the urology bootcamp model
The initial drivers for urology bootcamp development were multifactorial, the most notable reasons being the lack of structured skills-based course and greatly varying urology training exposure during early years of training across various regions. Furthermore, the newly appointed urology ST3 trainees can come from a variety of backgrounds and experiences and over the years, with increasing competition for urology higher surgical training, 18 a fair proportion of appointed trainees come directly from core training. Some trainees may have had the experience of a urology resident as a trust grade either within or outside the United Kingdom. While this heterogeneity in urological exposure and experience exposed educational gaps, which were increasingly apparent at the interface between core surgical training and higher specialty training. 19 New urology trainees are expected to manage acute urological emergencies, perform basic endoscopic procedures and demonstrate leadership within multidisciplinary teams from the outset, often without prior structured exposure to these competencies. Needs assessment conducted among early specialty trainees consistently highlighted deficiencies in confidence, procedural familiarity and non-technical skills such as communication and decision-making. 20 These findings provided the impetus for a more formalised, curriculum-based, standardised preparatory programme. 21
Curriculum design for the urology bootcamp was grounded on an established educational theory of ‘Adult learning principles’ which emphasise relevance, self-direction and experiential learning.16,17 Deliberate practice was operationalised through repeated hands-on simulation with expert faculty feedback, allowing trainees to progress towards a pre-defined benchmark rather than relying on time-based exposure alone. A breakdown of the bootcamp model is shown in Figure 1.
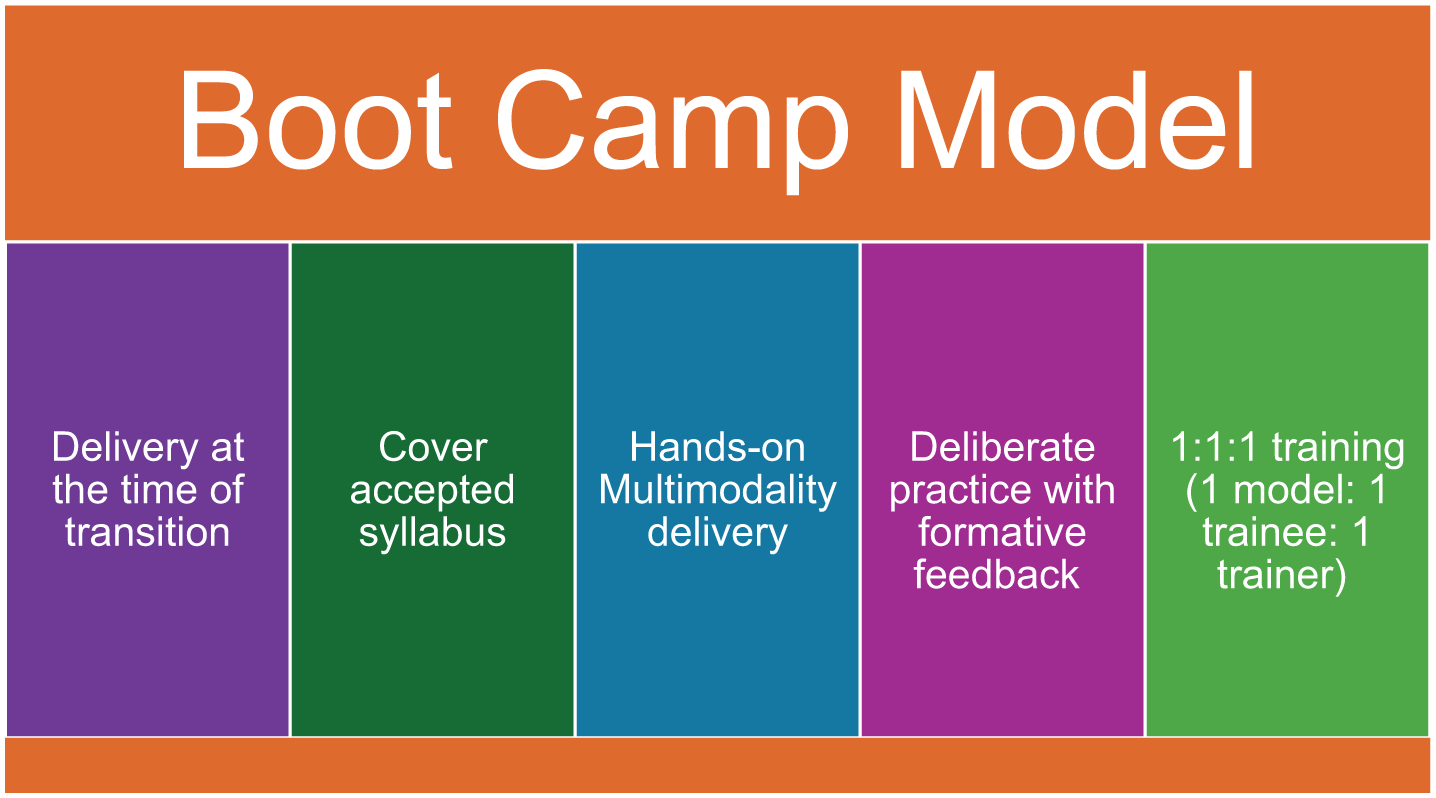
Pillars of the bootcamp model.
Importantly, successful bootcamp models were integrated with national training structures rather than operating in isolation. 21 Endorsement by Specialty Advisory Committees (SAC) and alignment with national curricula ensured relevance, legitimacy and sustainability. Over time, bootcamps evolved from pilot initiatives to recurrent, centrally supported educational events embedded within urology training pathways. 22
Structure and delivery of bootcamp training
The format of urology bootcamp training is intentionally designed to be intensive and immersive high-volume, hands-on simulation intertwingled with didactic teaching over 5 days. E-learning modules at the course and short lectures prior to each module provide foundational knowledge, which is immediately reinforced through practical stations. 22
A wide range of simulation modalities are utilised starting with bench-top models for simple procedures such as suprapubic catheterisation and scrotal examination. 23 More complex simulation tools such as Lap Mentor, Uro Mentor and TUR Mentor (Surgical Science, Sweden) used to teach procedures such as ureteroscopy, basic laparoscopic skills, transurethral resection of prostate (TURP) and transurethral resection of bladder tumour (TURBT).24–26 Animal tissue models were used to allow higher-fidelity rehearsal of open techniques ranging from scrotal exploration to ureteric re-implantation. Other simulators, such as RobotiX Mentor, Intuitive and Medtronic simulators, provide exposure to robotics basic skills and offer objective performance metrics with the opportunity for repeated practice. 27 Figure 2 illustrates the breakdown of skills and models used in the bootcamp.
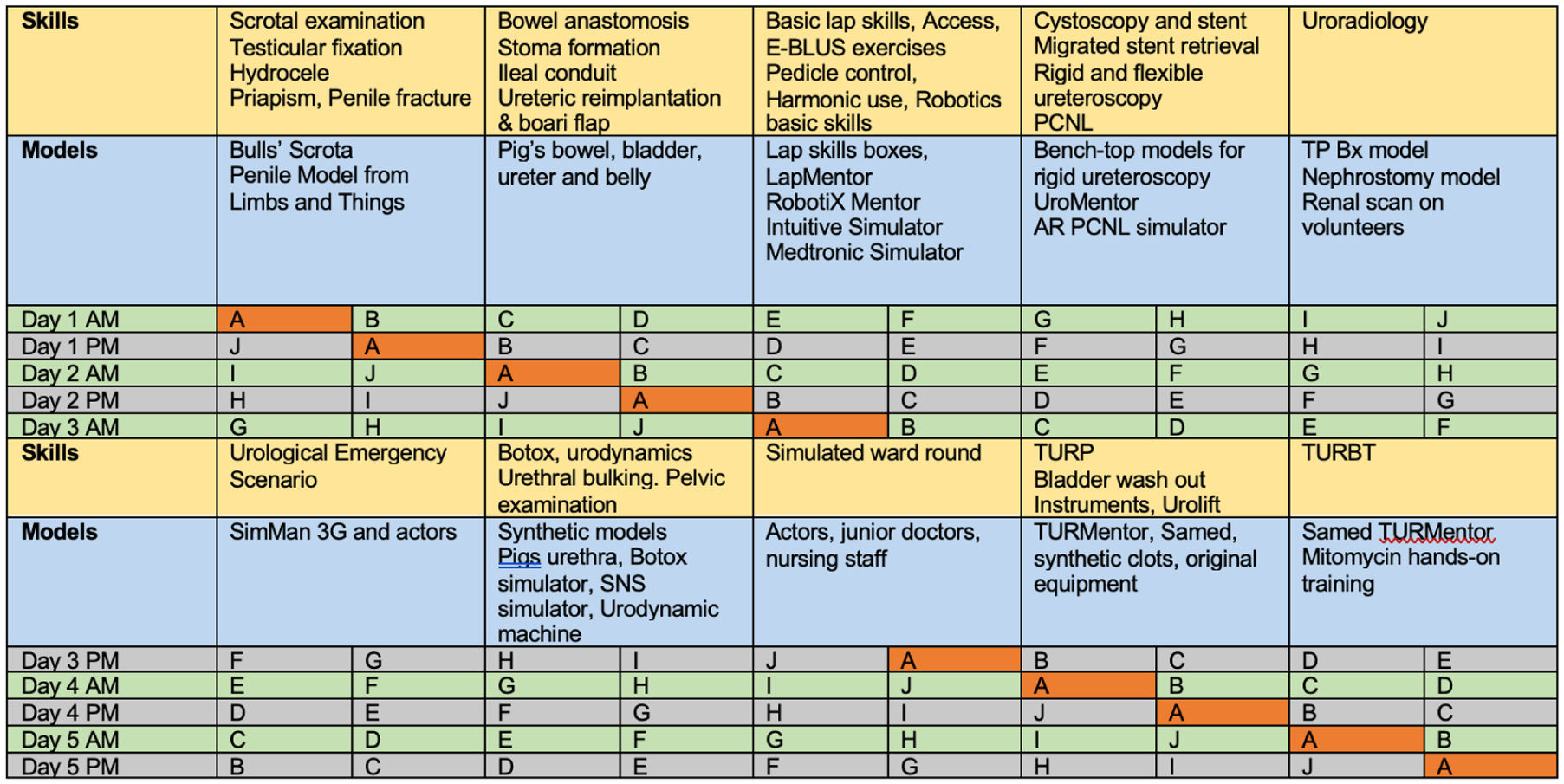
Illustration of curriculum and models used in Bootcamp.
Non-technical skills are addressed through scenario-based simulation using high-fidelity mannequins and trained actors. These sessions focus on emergency management, communication with patients and colleagues, leadership and human factors, reflecting the realities of modern urological practice. 28 In recent years, the importance of surgeon well-being and performance has translated into the inclusion of a session with a surgical life coach to incorporate valuable skills and tools that can be used to enhance performance in a high-pressure, high-stakes environment. 29
Structured assessment is integral to bootcamp delivery, with pre- and post-course multiple-choice questionnaires (MCQs) assessing knowledge acquisition, while self-reported confidence scales capture perceived preparedness. Objective structured assessment of technical skills (OSATS) and global rating scales were used, where feasible, to evaluate procedural competence. 4
Faculty development represented a critical component of early bootcamp programmes. Trainers required not only procedural expertise but also skills in simulation facilitation, feedback delivery and assessment. 30 Many programmes invested in faculty training workshops to ensure consistency, educational rigour and alignment with regularly updated and relevant learning objectives.
Educational outcomes over 10 years
Since the implementation of the urology bootcamp, it has consistently demonstrated educational benefits to trainees. Studies reported significant improvement in knowledge and technical competence31–33 with trainees showing enhanced familiarity with equipment, procedural steps and emergency protocols. Confidence and preparedness for their urology training are among the most robustly reported outcomes. Delegates describe reduced anxiety and increased readiness in fulfilling the clinical expectations in this new role with expanded responsibilities. It also enhanced their willingness to engage in operative opportunities early in training. Faculty feedback corroborates these perceptions, noting smoother transitions and more effective early performance among bootcamp-trained trainees (personal communication).
Iterative refinement has been a hallmark of urology bootcamp. Structured, consistent feedback from trainees and faculty has shaped curriculum adjustments, station redesign and the integration of new technologies. Longitudinal trends indicate that bootcamp has become more focused, outcome-driven and aligned with real-world clinical demands over time. Figure 3 demonstrates the overall feedback on the urology bootcamp over the years.
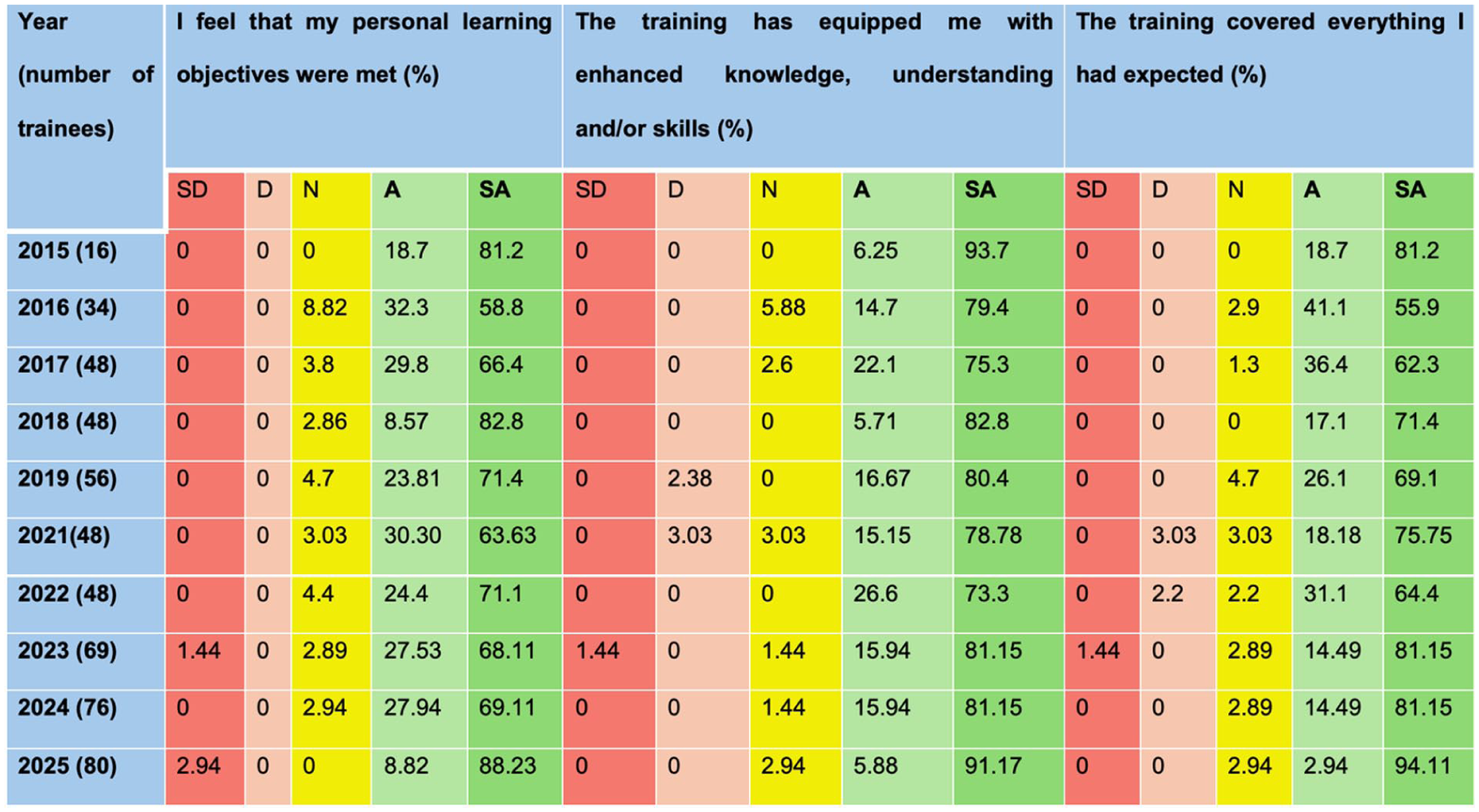
Delegate feedback on the urology bootcamp over the years.
Impact on early urology careers
The influence of bootcamp training extends beyond immediate educational outcomes. Trainees who enter clinical practice with baseline procedural familiarity are better positioned to capitalise on learning opportunities in theatre. This can subsequently translate into a snowball effect on confidence and progression. 4
Professional identity formation is another important impact and bootcamps provide early socialisation into the urological community, fostering a sense of belonging and shared standards. 34 The peer support network formed by meeting a group of people at the same stage of training who share the same fears and challenges should not be underestimated. Exposure to enthusiastic faculty role models can inspire and spark positive emotional valence when faced with this transition.
Leadership, communication and teamwork skills developed through simulation scenarios translate directly into clinical environments. These competencies are increasingly recognised as essential for safe surgical practice and form part of the assessment for their urological curriculum.
Bootcamp beyond the United Kingdom: global and low-resource settings
The urology bootcamp model has been successfully adapted beyond the United Kingdom, including in low- and middle-income countries. 35 In Africa and other regions, bootcamps have focused on essential and emergency urological skills with the utilisation of low-cost, locally sources simulation models. The European School of Urology adopted the USBC because to its success and popularity in the United Kingdom. For first-year European urology residents, the European School Urology Boot Camp is a structured programme that offers excellent technical skills training. 36 Four 2-hour sessions covering laparoscopy, transurethral resection and upper and lower tract endoscopy make up the 1-day training. Similar boot camps were adopted into the training curricula of other specialities, such as general surgery and obstetrics and gynaecology in Yorkshire, as they realised the benefits of this training paradigm. These programmes were designed to address the unique requirements of each speciality while adhering to the same ideals of intensive, practical training (Figure 4).
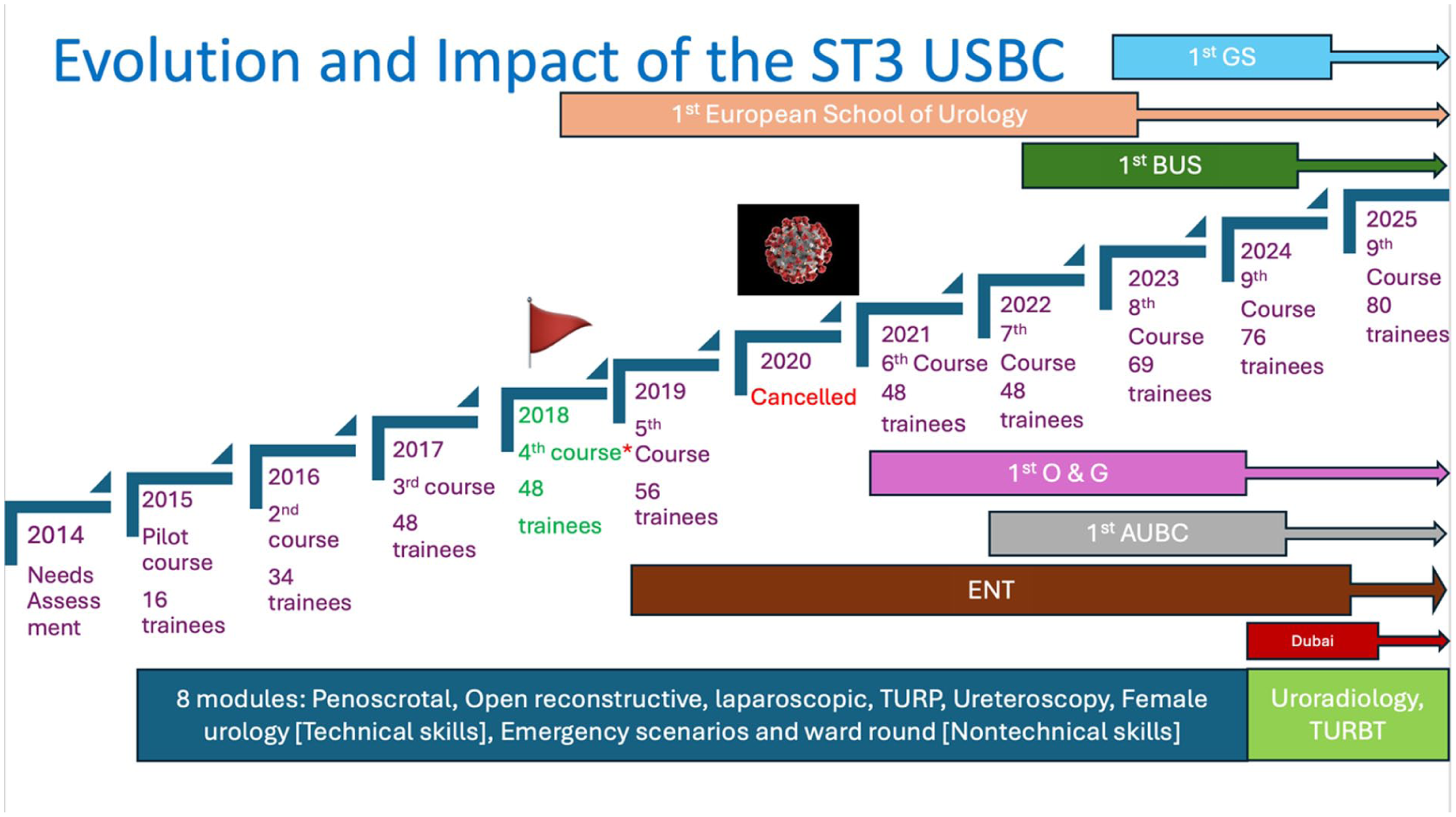
Evolution and impact of the ST3 urology bootcamp.
A ‘train-the-trainer’ approach has proven crucial in the sustainability of the bootcamp training model. By equipping local faculty with simulation and educational expertise, programmes reduce reliance on external support and promote long-term capacity building. International delivery has highlighted the importance of contextual adaptations. Curriculum content, simulation faculty and assessment methods must reflect local disease patterns, resource availability and training structures. Lessons learned from global implementation have, in turn, inspired innovations within high-income settings.
Challenges and limitations
Despite their success, the urology bootcamp faces ongoing challenges, with funding being a significant barrier, particularly given the costs associated with simulation equipment, faculty time and venue requirements. Resource-intensive simulation models may be difficult to scale equitably across regions, especially in healthcare systems with variable institutional resources and reliance on high-fidelity equipment and specialist faculty may inadvertently disadvantage trainees in smaller centres or resource-limited settings.
Balancing simulation fidelity with accessibility is an enduring challenge. High-fidelity virtual reality and cadaveric simulation offer educational advantages but may exclude programmes with limited resources. Conversely, low-fidelity models, while more accessible, may not fully replicate clinical complexities.
Measuring long-term career impact remains challenging. While short-term educational outcomes are well-documented, robust data linking bootcamp participation to long-term operative competence, patient outcomes or career progression is logistically challenging. Most evaluations rely on self-reported confidence measures and short-term assessments, and longitudinal, multicentre outcome data remain limited.
Future directions
There has been an expansion of the bootcamp beyond entry-level training into advanced subspecialty-focused training. Targeted programmes in areas such as endourology, functional urology, oncology and emergency urology can support key transition points later in training and address emerging workforce needs. 37 Technology innovation and advancement will play an increasing role in training. Artificial intelligence (AI) and data analytics offer potential for enhanced assessment of both technical and non-technical skills, including automated performance metrics, decision-making analysis and personalised feedback.38,39 Integration of AI into simulation-based non-technical skills training may allow more objective evaluation of situational awareness, communication skills and leadership. 40
Formal accreditation and recognition through continuing medical education (CME), national curricula and international endorsement may further legitimise and validate urology bootcamp as a core educational intervention. This may alleviate the challenges faced with funding from educational bodies. Further research priorities should include longitudinal outcome studies, cost-effectiveness analyses and exploration of the impact of the urology bootcamp across the urology training period.
Conclusion
Over the past 10 years, simulation-based urology bootcamp has evolved from innovative pilot initiatives into a foundational component of early specialty training. By addressing educational gaps at critical transition points, the urology bootcamp has enhanced trainee confidence, competence and preparedness while supporting patient safety and professional identity formation.
Their success has important implications for urology training programmes and offers broader lessons for surgical education in an era of constrained clinical exposure and increasing complexity. As trainees’ needs and expected competencies change, the urology bootcamp model provides a relevant, scalable, evidence-informed framework for preparing the next generation of urologists and may serve as a blueprint for SBE across different stages of training and for other surgical specialties.
Footnotes
Acknowledgements
We would like to thank all participants, faculty and Medical Education Team, Leeds Teaching Hospital, Leeds, for their continued support.
Conflicting Interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Equipment and sponsorship for the Urology Simulation Boot Camp were provided by BJUI, Karl Storz, Boston Scientific, Intuitive, Medtronic, Samed, CMR Surgical, Cook Medical, Coloplast, Ethicon, NovusMed, Dantec, OKB Medical (Simbionix), MediPlus, Teleflex, European Pharma.
Ethical Considerations
Not applicable
Patient Consent
Not applicable
Consent to Participate
All participants provided informed consent during the course for their data to be used in future research and publications.
Consent for Publication
All participants provided informed consent during the course for their data to be used in future research and publications.
Data Availability Statement
Vish Hanchanale and Chandra Shekhar biyani.
Guarantor
CSB, VH
Contributorship
Conceptualisation: KO, CSB
Methodology: KO, CSB
Formal analysis: KO, CSB
Writing–Original Draft: KO
Writing–Review & Editing: CSB, MM, VH
Trial Registration
Not applicable