
Abstract
Objective:
British Association of Urological Surgeons (BAUS) is the subspecialty organization for urologists in the United Kingdom. BAUS implemented structured equality, diversity, and inclusion initiatives to improve representation at its annual scientific meetings (ASM). Scientific meetings play a critical role in academic visibility, leadership development, and professional networking. Historically, women, ethnic minority clinicians, and international medical graduates (IMGs) have been underrepresented in conference leadership roles. This study evaluated demographic representation among Chairs and Speakers (C&S) at BAUS ASMs from 2022 to 2025 and compared these data with membership demographics.
Methods:
A retrospective observational analysis of publicly available BAUS ASM programs from 2022 to 2025 was conducted. Demographic variables including gender, ethnicity, and primary medical qualification (PMQ) region were extracted and compared with BAUS membership data. Descriptive statistics and trend analyses were performed.
Results:
A total of 682 C&S were identified. Women comprised 31.2% of participants and were significantly overrepresented relative to workforce proportions. Minority ethnicity representation increased significantly from 34.3% in 2022 to 48.7% in 2025 (p < 0.01). However, Caucasian clinicians and UK-trained doctors remained predominant overall. IMGs accounted for 25.1% of C&S and remained significantly underrepresented compared with workforce data, with only a modest upward trend.
Conclusion:
Representation among BAUS ASM C&S has improved, particularly for ethnic minority clinicians and women. Nonetheless, disparities persist for IMGs and minority groups. Continued targeted strategies and longitudinal monitoring are required to achieve sustained equity in academic participation.
Level of evidence:
4
Keywords
Introduction
Scientific meetings are the cornerstones for sharing latest scientific information, collaborating, and developing networks to innovate and progress. They play a critical role in shaping academic careers by providing opportunities for professional recognition, networking, and leadership development. Historically women, ethnic minorities, and international medical graduates (IMGs) have remained disproportionately underrepresented in leadership positions, academic visibility, and conference participation. Lack of female representation has been reported across various specialties and globally.1–4 Literature on Black and minority ethnic (BAME) representation in this field is also sparse. Ensuring diverse representation among Chairs and Speakers (C&S) is essential for fostering an inclusive professional culture that allows overall development of the historically underrepresented groups.
British Association of Urological Surgeons (BAUS) is the subspecialty organization for urologists in the United Kingdom. It has taken proactive steps to embed equity, diversity, and inclusivity (EDI) principles within its governance and scientific program planning. In recent years, structured efforts have been implemented to ensure that annual scientific meeting (ASM) panels better reflect the diversity of the UK urology workforce. By comparing this data against its membership demographics, we aim, through this study looking at the C&S at the BAUS ASM from 2022 to 2025, to evaluate progress made toward addressing the differential representation and reflecting the workforce mix.
Methods
This retrospective observational study analyzed publicly available BAUS ASM final programs from 2022 to 2025. All listed C&S were identified, and demographic variables were extracted, including gender, ethnicity, and primary region of medical qualification. Gender and ethnicity data was inferred from publicly available professional profiles, institutional websites, and regulatory registers. The primary region of qualification was determined from medical registration data. Two authors independently reviewed all entries. Discrepancies were resolved by a third reviewer. General Medical Council (GMC) workforce statistics for UK-registered urologists were used as comparator data, including gender distribution and IMG status.
Descriptive statistics were used to summarize demographic representation. Trends across years were assessed using appropriate statistical tests, with significance thresholds defined prior to the analysis. Statistical analyses were conducted using a standard statistical software program.
Study design and data sources
This study was a retrospective observational study. Final published programs for 4 years ending 2025 were reviewed to identify all listed C&S. Each individual’s gender, ethnicity (Caucasian or ethnic minority), primary region of medical qualification (UK or non-UK), and role (Chair or Speaker) were collated from publicly available professional profiles, institutional websites, and regulatory registers. Primary region of qualification was determined from medical registration data.
Data extraction and validation
Two authors independently extracted data for all C&S. Discrepancies were resolved by a third reviewer after discussion. If demographic information could not be confidently inferred, the variable was coded as missing and excluded from category-specific analyses.
Comparator data
BAUS and GMC workforce statistics for UK-registered urologists were used. Completed data set from the BAUS workforce was finally used as comparator data for gender distribution and IMG status. These data were used descriptively to contextualize ASM representation and for final analysis. The GMC data explorer has 1942 urologists on the specialist register and 403 trainees. Forty-four percent of specialists and 29% of trainees obtained their primary medical qualification (PMQ) from outside the United Kingdom. 5
Statistical analysis
All analyses were performed using the standard statistical software. Statistical methods applied include proportions and 95% confidence intervals (CIs) for gender, ethnicity, and PMQ status; chi-square tests to compare proportions across years; Cochran–Armitage trend tests to assess linear trends from 2022 to 2025; and absolute and relative percentage changes and ratios (male:female, UK-PMQ:non-UK PMQ, Minority:Caucasian)
Results
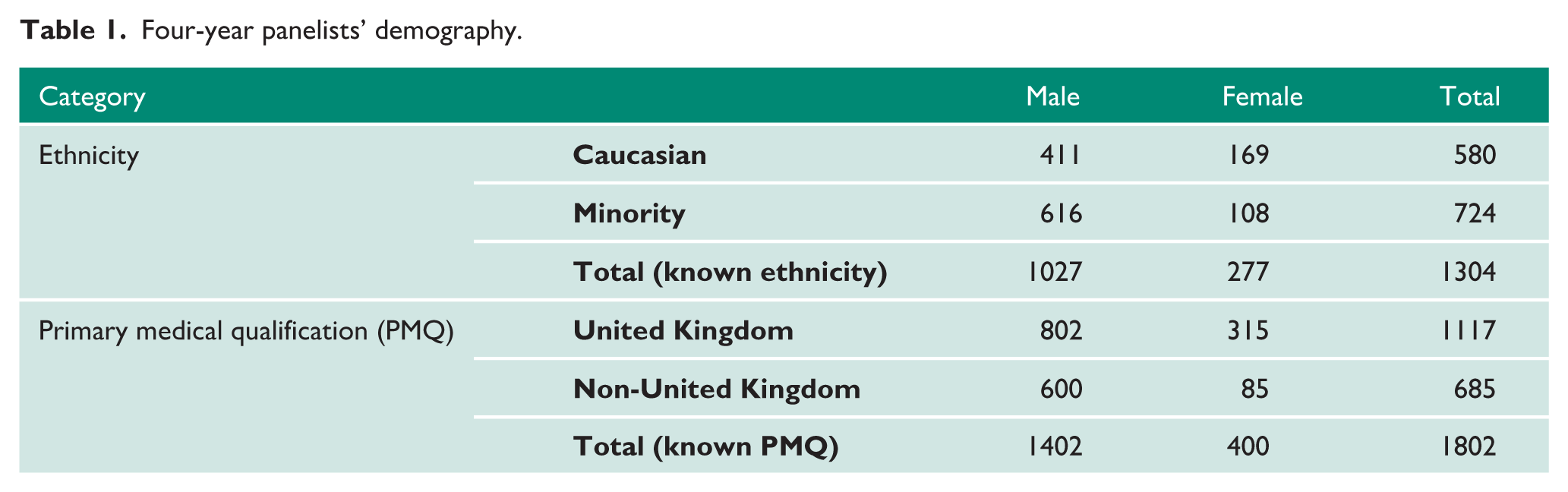
A total of 682 C&S were identified across the study period. This comprised of 187 Chairs and 495 Speakers (Table 1). Annual representation increased from 99 in 2022 to 228 in 2025, with a maximum of 232 panelists in 2024 due to comparatively increased number of sessions. This was compared against the known denominator from BAUS workforce (Figure 1(a) to (c))
Four-year panelists’ demography.
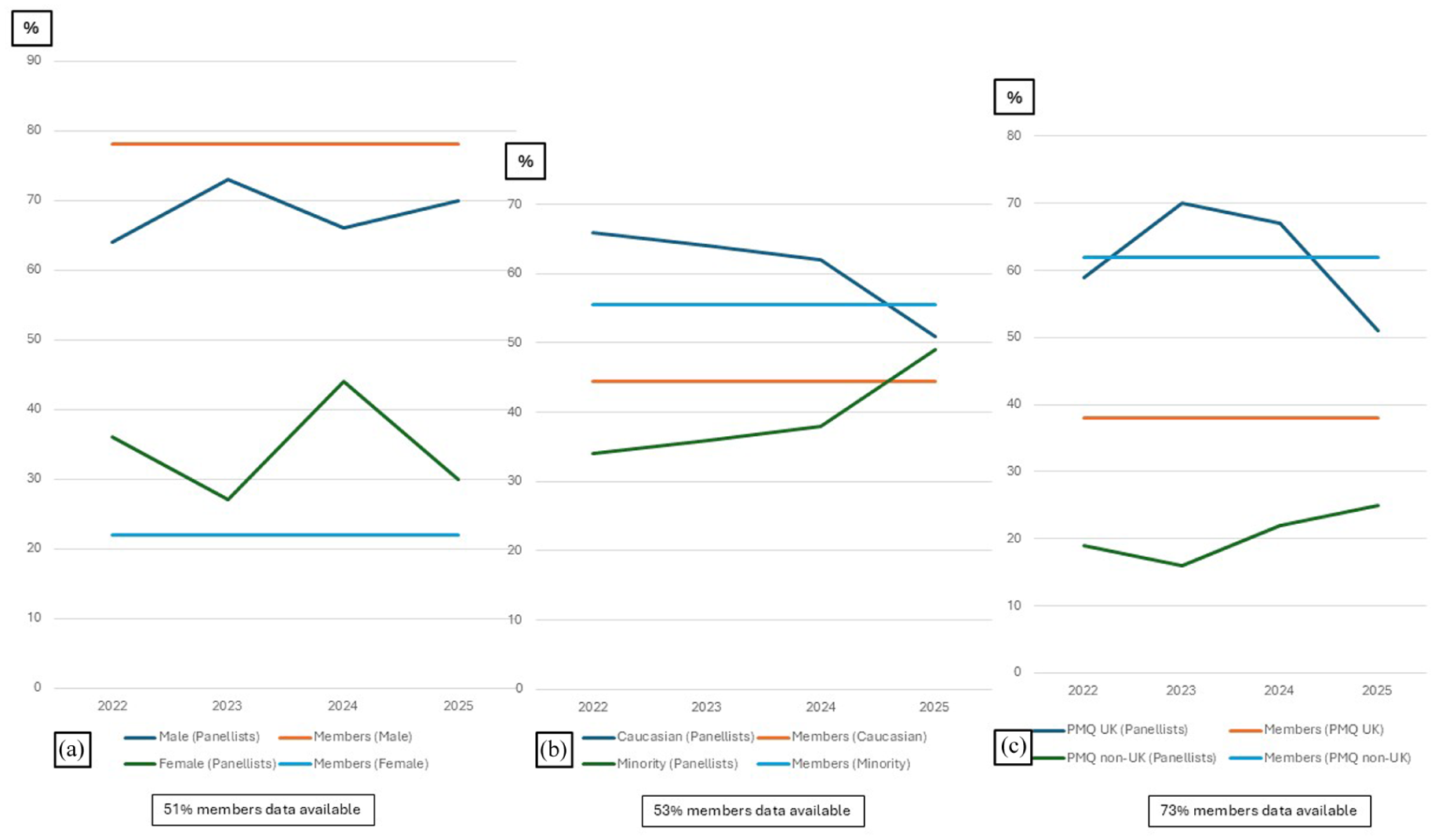
Representation compared with membership profile, (a) gender, (b) ethnicity and (c) primary medical qualification country.
Gender representation
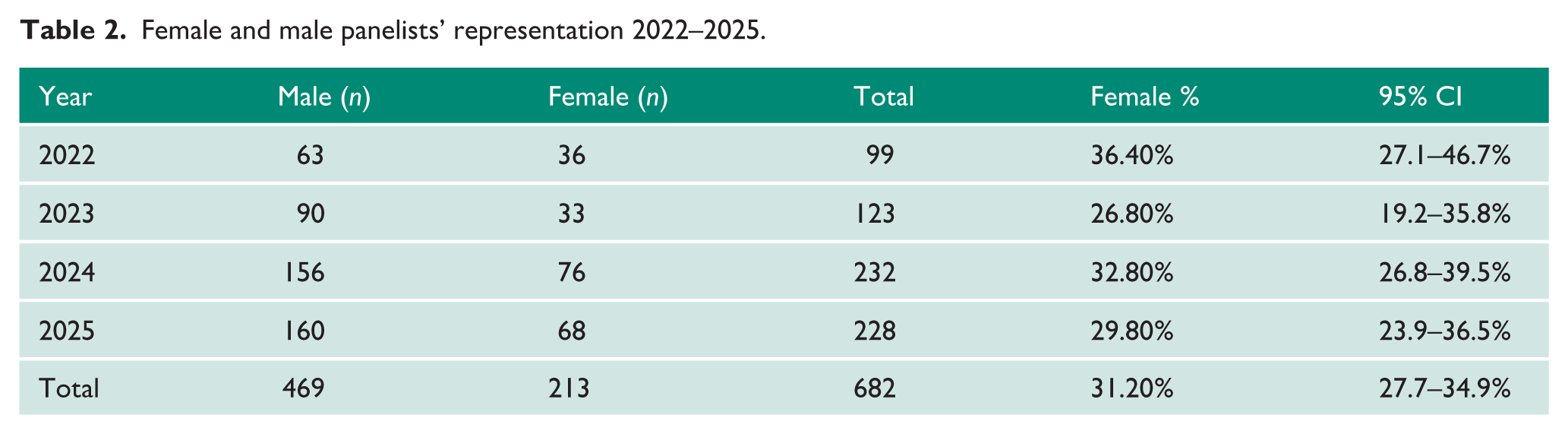
Across all ASMs (N = 682), 469 (68.8%) C&S were male, and 213 (31.2%, 95% CI 27.7–34.9%) were female (Table 2). Compared with membership (81.0% male, 19.0% female), women were significantly overrepresented (χ² = 66.72, p < 0.0001, V = 0.31). No significant linear trend in female representation was observed across years.
Female and male panelists’ representation 2022–2025.
Ethnicity
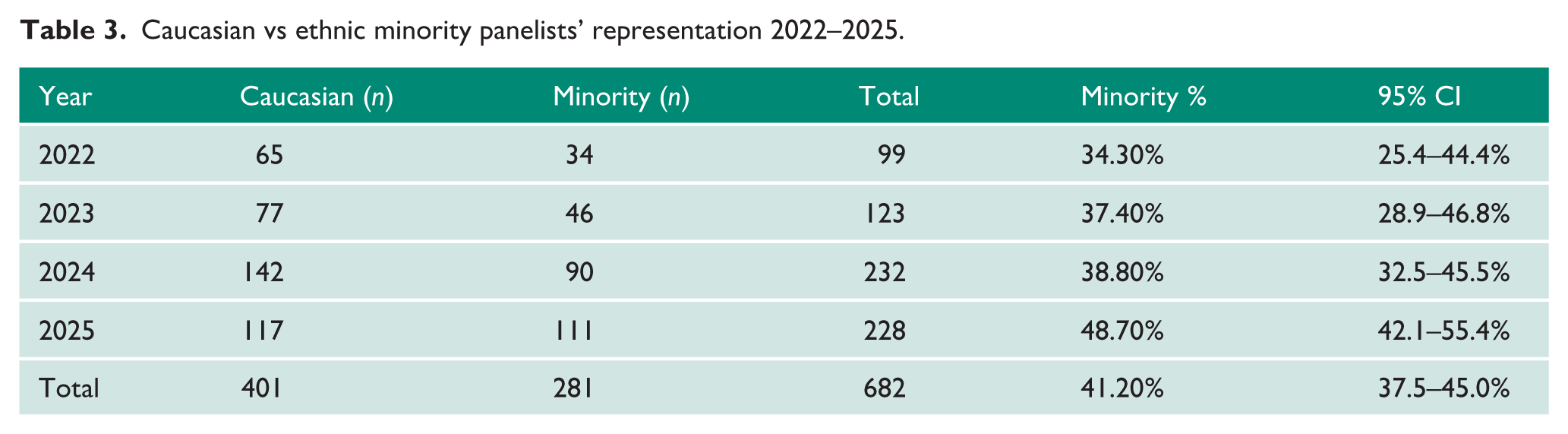
Among C&S with identifiable ethnicity (N = 682), 401 (58.8%), 281 were minority ethnicity, making up 41.2% of the overall sample (95% CI 37.5–45.0%) (Table 3). Compared with membership (44.5% Caucasian, 55.5% minority), Caucasian speakers were significantly overrepresented (χ² = 56.52, p < 0.0001, V = 0.29). Minority representation increased significantly from 34.3% (95% CI 25.4–44.4%) in 2022 to 48.7% (95% CI 42.1–55.4%) in 2025 (trend test p < 0.01).
Caucasian vs ethnic minority panelists’ representation 2022–2025.
IMG status
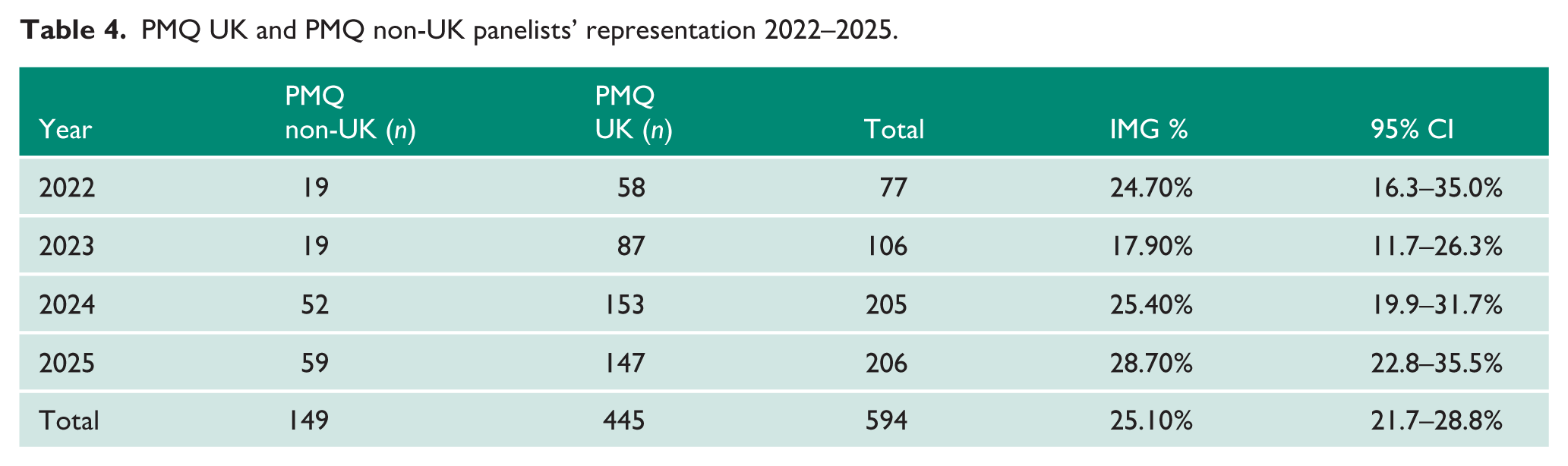
Among C&S with an identifiable qualification status (n = 594), 445 (74.9%) were UK-trained (Table 4). IMG’s accounted for 149, making up only 25.1% (95% CI 21.7–28.8%). Compared with membership (61.9% UK-trained, 38.1% IMG), IMGs were significantly underrepresented (χ² = 42.14, p < 0.0001, V = 0.27). A modest upward trend in IMG representation was observed but did not reach statistical significance (Cochrane-Armitage trend test p = 0.058).
PMQ UK and PMQ non-UK panelists’ representation 2022–2025.
Discussion
This multi-year analysis provides the first formal evaluation of demographic representation among C&S at BAUS ASMs against known membership demographics. This is also the first reported ethnicity representation review in conference scientific activity, particularly in urology. The findings demonstrate some improvement in representation over time. However, significant disparities remain when benchmarked against BAUS membership data.
Gender representation showed a substantial increase in the absolute number of female C&S across the study period. 6 However, proportional representation fluctuated year on year, without a consistent upward trend. When aggregated across all years, women were significantly overrepresented, relative to the proportion among the BAUS membership. This reflects deliberate efforts by BAUS to increase visibility of women in academic and leadership roles. Bias in academia extends beyond conference leadership 7 and needs to be actively overcome for meaningful progress.
Ethnicity balance demonstrated most notable improvement. Minority representation increased steadily from 34.3% in 2022 to 48.7% in 2025, with a statistically significant positive trend. Despite this progress, Caucasian speakers remained significantly overrepresented relative to the membership denominator. This discrepancy may reflect seniority gradients within the specialty, differential academic engagement opportunities, and historical underrepresentation of minority clinicians in leadership and academic roles. 8 The upward trajectory, however, suggests that BAUS’s EDI strategy is beginning to shift representation toward greater equity.
IMG representation also increased in absolute terms, with a modest upward trend that approached statistical significance. However, IMGs remained significantly underrepresented relative to their proportion in the BAUS membership. This finding aligns with broader literature indicating that IMGs often face structural barriers to academic visibility, including reduced access to mentorship, fewer research opportunities, and slower progression into senior roles.9–11 The increasing IMG participation observed in later years may reflect growing awareness of these disparities and targeted efforts to address them.
The strengths of this study include its multi-year design, independent dual-reviewer methodology, and use of membership data as a denominator for any inferential analysis. However, several limitations must be acknowledged. Demographic data for ethnicity and qualification were incomplete within the membership dataset (membership demographic data at 58% completion), necessitating the use of reduced denominators. Demographic characteristics of ASM participants were inferred from publicly available sources rather than those self-reported, introducing potential misclassification bias. Analysis in this study does not account for seniority, academic ranking/expertise, subspecialty, or prior speaking experience, all of which influence selection for conference roles and the multiple invites for a select few of the C&S. International invited speakers and non-urologists’ UK experts were included in the panelist numbers. As these speakers were not members, this may have inflated apparent disparities in IMG representation.
Conclusion
This study demonstrates measurable progress in ethnic minority and IMG representation at BAUS ASMs between 2022 and 2025, alongside substantial increases in the absolute number of women participating as C&S. However, when benchmarked against BAUS membership demographics, significant disparities remain: Caucasian and UK-trained clinicians continue to be predominant, while minority and IMG clinicians remain underrepresented. These findings highlight both the positive impact of BAUS’s EDI initiatives and the ongoing need for targeted strategies to ensure equitable academic visibility, especially among speaker roles.
The authors, over the 4-year study period, all of whom have led the selection of diverse C&S panels for the ASM, have continued to deliver an excellent scientific conference, both with state-of-the-art content and excellent speakers.
Future work should steer toward incorporating self-reported demographic data, more granular ethnic categories, and intersectional analyses. Qualitative research exploring perceived barriers to academic participation among underrepresented groups would further contextualize these quantitative findings. Longitudinal monitoring of ASM representation should continue to ensure that early gains translate into sustained equity.
This successful BAUS framework for equity and diversity serves as a blueprint for urology organizations in selecting panel members for scientific meetings.
Footnotes
Ethical considerations
No ethical approval required.
Consent to participate
Not required.
Consent for publication
Not required.
Author contributions
All authors contributed to the drafting and review of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data available on request.
Guarantor
J.P.