
Abstract
Objective:
Investigate whether prostate volume is a moderating variable for the incidence of prostate cancer (PCa).
Methods:
Study participants in the control arm whose cancer status was verified per biopsies during the 7-year study period were included for analysis. Simple and multivariable logistic regression analyses including parameters such as age and race were applied.
Results:
PCa was diagnosed in 1132 (24.3%) of Prostate Cancer Prevention Trials (PCPT) participants. Simple logistic regression demonstrated a statistically significant reduction in PCa incidence for patients with prostate volumes larger than 60 cc. Risk of aggressive cancer (Gleason grade ⩾ 7) was also significantly lower in men with prostate volumes greater than 60 cc (aOR = 0.585, p = 0.000) when controlling for age, family history of cancer, and race.
Conclusions:
Stratifying the PCPT data by prostate size with considerable statistical power revealed a highly significant (p = 0.000) difference between the incidence of PCa in large (⩾60 cc) and moderate to small (<60 cc) prostates, not only for general PCa but also for high-grade cancer. These results support the clinical hypothesis that prostate/benign prostate hyperplasia size may have a protective effect on the incidence of PCa.
Level of evidence:
Not applicable.
Introduction
According to the American Cancer Society, 1 one in eight men will be diagnosed with prostate cancer (PCa) during their lifetime, making it the second most common cause of cancer death in men. In addition, benign prostate hyperplasia (BPH) also presents a notable health burden, affecting more than 50% of men aged 50 and over, with the incidence increasing as men age. 2 Given the significant prevalence of both disease entities, investigations have been done exploring potential relationships between them; however, their interaction is still not well understood. In the contemporary scientific literature, an evolving hypothesis suggests that large BPH prostates may have a lower incidence of PCa. 3 This theory stems from histo-anatomical observations indicating increased fibrosis and glandular atrophy of the peripheral zone (PZ) of large prostates, which is noteworthy as 80–85% of PCa originates in this zone.3,4
The prospective and randomized Prostate Cancer Prevention Trials (PCPT) is a large and exceptional dataset. It comprehensively documented patient-specific parameters such as the incidence of PCa under both placebo and finasteride treatments, as well as prostate volume. Notably, many patients who were not diagnosed with PCa during the study underwent biopsies at the conclusion of the study. 5 However, to date, no comprehensive study has stratified the PCPT data by prostate volume to verify its function as a relevant moderating variable influencing the incidence of prostate cancer in untreated patients (control group). After gaining access to the PCPT dataset by the SWOG Cancer research group, we tested the hypothesis of large prostate volumes being protective against the incidence of PCa (Table 1).
Listing of used abbreviations.
Methods
Sample selection
Participants were included in the analytic sample if they had biopsies with a confirmed cancer status and were randomly assigned to the placebo/ control group. Participants were excluded if they did not have a prostate volume documented in the dataset or the documented volume was improbably low (<10 cc) or high (>400 cc).
Variables
The primary outcome was development of prostate cancer. Patients were diagnosed with cancer during or at the conclusion of the trial via biopsy, prostatectomy, transurethral resection of the prostate (TURP), or other methods not disclosed. Patients were confirmed to be cancer free at the conclusion of the trial via elective biopsy. The secondary outcome was development of aggressive cancer defined as cancer scored with Gleason grade ⩾ 7. This variable was ordinal and included three tiers – no cancer, low-grade cancer (Gleason grade < 7), and aggressive cancer (Gleason grade ⩾ 7).
The primary predictor was prostate volume included as a continuous variable measured in cubic centimeters (cc) and categorical variable stratified as follows: small prostate ⩽ 35 cc, mid-size 36–60 cc, and large > 60 cc. Additional variables reported include treatment group (placebo, Finasteride), age in years, body mass index (BMI), race (white, black/African American, other), ethnicity (non-Hispanic, Hispanic), and family history of prostate cancer.
Statistical analysis
Stata/MP version 17.0 was used for all data management and analyses (StataCorps, LLC., College Station, Texas). Descriptive statistics were calculated via mean with standard deviation or frequency with percentage, depending on level of measurement. Most missing data was handled during sample selection. However, any additional missingness was accounted for via listwise deletion. Chi-square or independent Student’s t-test were used to assess differences in demographic and clinical characteristics between outcome groups (e.g. those with and without cancer). Normality was confirmed for continuous variables prior to use of parametric statistics. An alpha of 0.05 served as threshold for statistical significance.
Simple and multivariable logistic regression tested the hypothesis that cancer risk is inversely associated with prostate size. Prostate size was modeled as both a continuous and categorical predictor. Multivariable logistic regression included the categorical iteration of prostate size, as well as variables hypothesized to be associated with cancer risk: age, race, and family history of cancer. Finally, generalized ordered logistic regression tested the hypothesis that risk for aggressive cancer, as compared to no cancer or low grade (Gleason grade < 7), is lower in patients with large prostate volumes. Constraints for parallel lines were imposed and the Wald test of parallel lines was done to verify the assumptions were met prior to interpretation. 6
Results
Participants
The PCPT dataset included 18,880 men that participated in the clinical trial. However, 12,435 (65.9%) did not have biopsy results confirming the presence or absence of cancer at the conclusion of the trial, and thus were excluded from the analysis (Figure 1). Of those remaining in the cohort, 1014 were randomized to the finasteride group and 728 of the remaining patients did not have prostate volumes documented. Another 35 patients were excluded due to improbably small or large prostates suggesting data error. The final analytic sample included 4668 men.
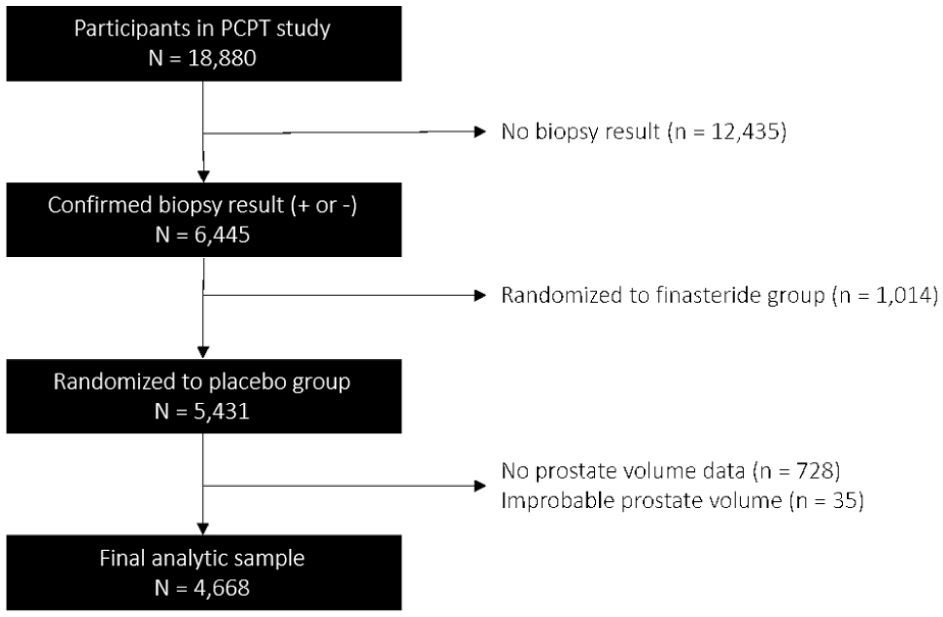
PRISMA diagram of sample selection and exclusion for analysis of placebo group.
The majority of participants were white (95.4%) and non-Hispanic (97.5%) with a mean age of 63 years. Cancer was diagnosed in 1132 (24.3%) patients while the remaining patients had negative biopsies at closure of the study. There were statistically significant differences in age, prostate volume, race, and family history of cancer between the two outcome groups (Table 2). Patients diagnosed with cancer had a mean age approximately 1 year older than those without, while mean prostate volume was approximately 2 cc smaller in cancer patients. There was a significantly larger proportion of African American patients with the diagnosis of cancer (p = 0.002) as well as a significantly higher proportion of patients with a positive family history of cancer (p = 0.000).
Descriptive statistics for placebo group.
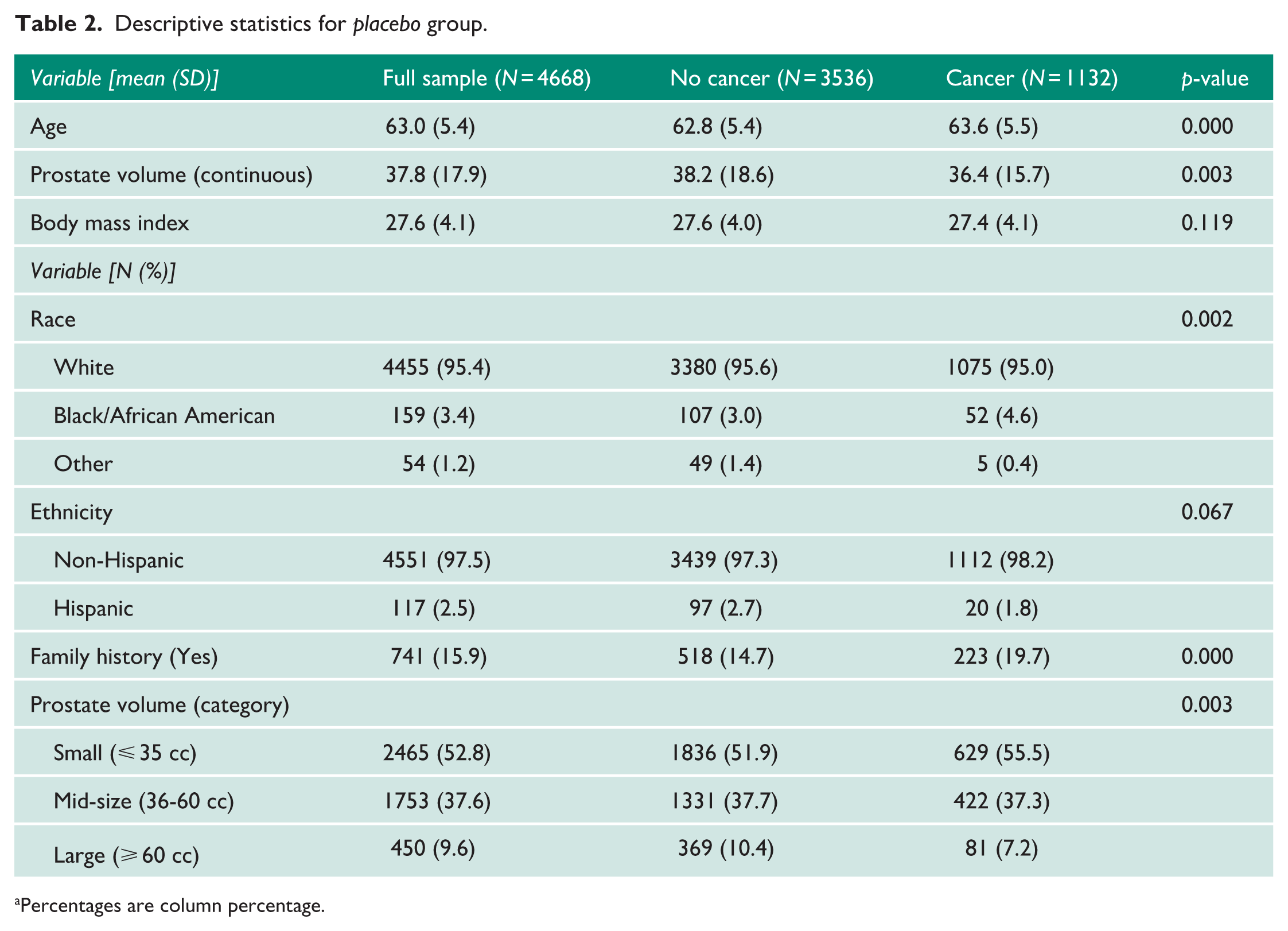
Percentages are column percentage.
Prostate volume association with cancer
Simple logistic regression demonstrated a statistically significant reduction in the risk of cancer for patients with prostates larger than 60 cc when compared to those with small prostate volumes (Table 3). There was not a statistically significant difference in cancer risk between moderate size (36–60 cc) and small prostates (⩽35 cc) (p = 0.285). On multivariable logistic regression, we found that the relationship between large and small volume prostates held after controlling for other relevant variables including age, family history of cancer, and race. The risk of cancer was significantly lower in men with prostate volumes greater than 60 cc [adjusted odds ratio (aOR) = 0.623, p = 0.000)] compared to men with small prostate volumes though not significantly different in men with mid-size volumes (aOR = 0.912, p = 0.208) (Table 3). The risk of aggressive cancer was also significantly lower in men with prostate volumes greater than 60 cc (aOR = 0.585, p < 0.000) when controlling for age, family history of cancer, and race (Table 4).
Multivariable logistic regression modeling the risk of any prostate cancer in the placebo group given prostate volume (N = 4668).
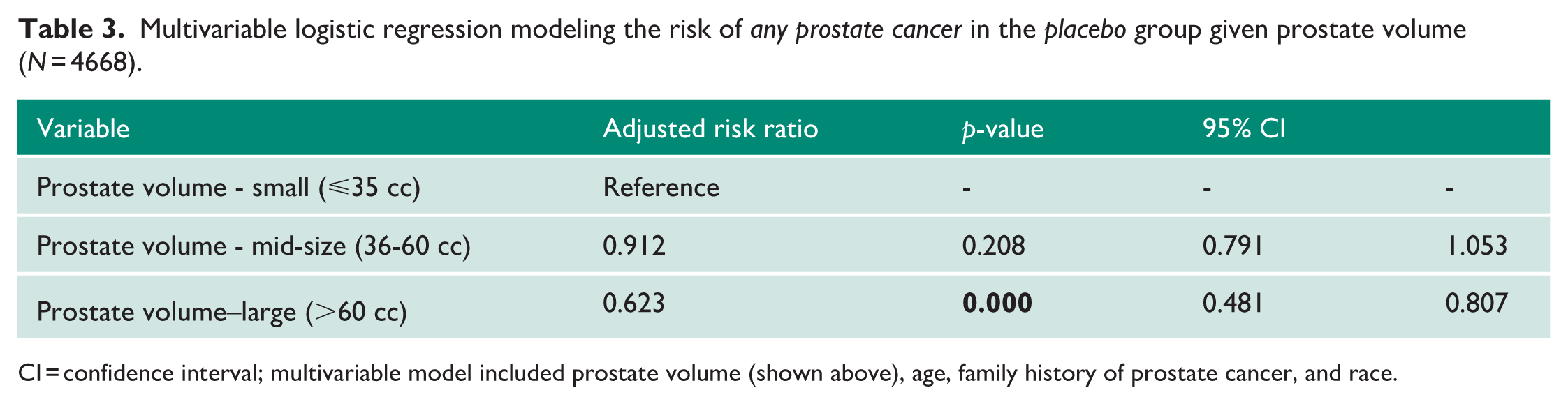
CI = confidence interval; multivariable model included prostate volume (shown above), age, family history of prostate cancer, and race.
Multivariable ordered logistic regression modeling the risk of aggressive Gleason grade (⩾ 7) cancer in the placebo group given prostate volume (N = 4668).
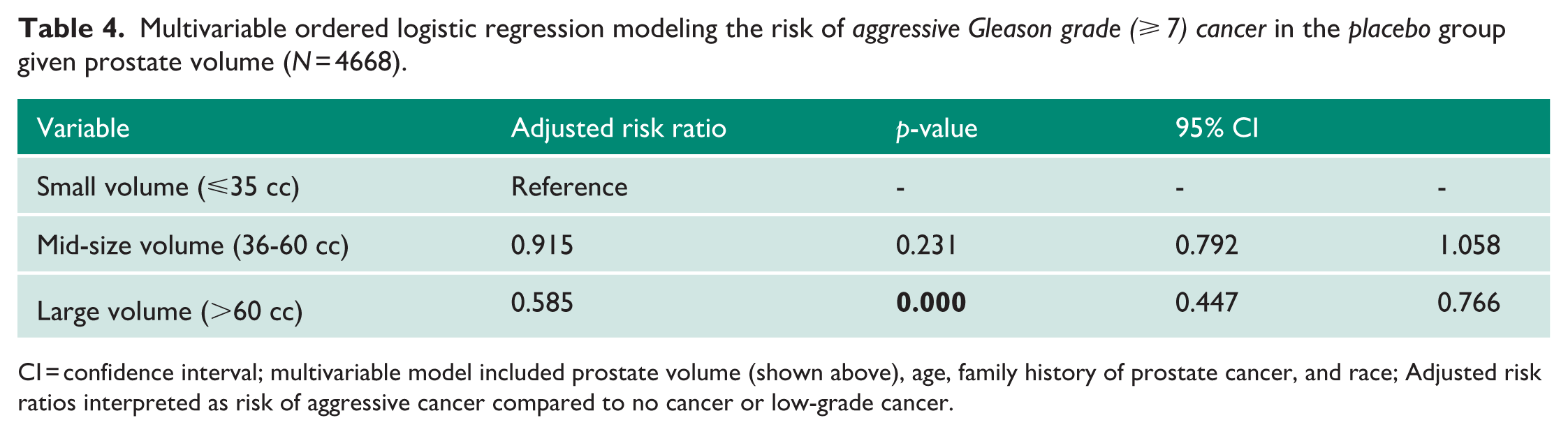
CI = confidence interval; multivariable model included prostate volume (shown above), age, family history of prostate cancer, and race; Adjusted risk ratios interpreted as risk of aggressive cancer compared to no cancer or low-grade cancer.
Table 2 also illustrates in absolute terms the varying cancer rates based on prostate volume. In the smaller prostate group, 629 out of 2465 patients developed cancer during the study, whereas in the larger prostate group, 81 out of 450 patients were diagnosed with prostate cancer. Based on these numbers the relative risk reduction is 29% in men with larger prostates compared to those with smaller prostates: ERS-ERL/ERS = (0.255–0.18)/0.255 = 0.294; ERS = event rate in small prostates, ERL = event rate in large prostates. These findings suggest that prostate volume may play an important role in future risk stratification for prostate cancer.
Discussion
Prostate cancer (PCa) and benign prostatic hyperplasia (BPH) are two of the most common urologic conditions, with autopsy studies indicating a high likelihood of PCa developing in aging men. 7 Although PCa and BPH frequently coexist, their exact pathophysiologic interaction is currently not well understood. Based on results from previous clinical studies, a hypothesis has recently evolved suggesting that large BPH prostates may have a protective effect against PCa.3,4 The prospective and randomized Prostate Cancer Prevention Trials (PCPT) offer a large dataset of BPH patients with well-documented prostate volumes and the incidence of PCa under placebo and finasteride.
With a participant pool exceeding 18,000 in the PCPT study, the data in this report has substantial statistical power. The results reveal a highly significant difference (p = 0.000) in the incidence of PCa between large (⩾60 cc) and moderate to small (<60 cc) prostates in patients assigned to the control (placebo) group. These results support other clinical studies showing an inverse relationship between BPH-size and the incidence of PCa.3,4 To our knowledge, this is the first report based on the PCPT data, where patients with large prostates had nearly a 40% reduction in the incidence of PCa compared to those with moderate to small-sized prostates.
In this context, it is noteworthy to mention the distinctive nature of the prostate, a unique organ consisting of four zones. Among these, the peripheral zone (PZ) and the transition zone (TZ) are pivotal when considering the pathophysiology of BPH and PCa. BPH predominantly affects the TZ, leading to hyperplasia as men age. Large BPH prostates in elderly individuals develop a thickened capsule, termed “surgical capsule,” facilitating enucleation during surgery.3,4 This growth-related expansion in BPH exerts mechanical stress on the PZ, inducing fibrosis and glandular tissue atrophy. Given that about 80% of PCa originates in the PZ, BPH-induced atrophy of the PZ glandular tissue decreases the incidence of PCa, particularly in large prostates. 8
Recent histo-anatomical studies corroborate these findings, demonstrating decreased glandular tissue volume in the PZ of large prostates compared to small prostates. 9 Furthermore, Lorenzo et al. 10 presented mathematical models that further support this, indicating mechanical pressure inhibits PCa expansion within the PZ of large prostates. Consequently, smaller tumor volumes and better prognosis are observed among patients with large prostates.11,12
Other investigators posit the “sampling error” hypothesis, suggesting that large prostates may yield higher false-negative PCa biopsy results. 13 However, several factors mitigate this argument. The PCPT deployed a variable number of biopsy core numbers based on prostate size, with extensive monitoring and repeat biopsies for suspicious cases. Extensive research indicates that additional biopsies performed mitigate the possibility of false-negative biopsies.14,15 Also, PSA levels, which tend to be higher in large prostates, prompt additional biopsies, reducing the likelihood of missed PCa diagnosis. 16
In addition, PSA density (PSAD) and MRI-guided biopsies support the protective effect of large prostates, as higher PSAD values in smaller prostates indicate elevated PCa risk.17–19 MRI-guided biopsies exhibit superior detection rates for clinically significant PCa, further substantiating the inverse correlation between prostate size and PCa incidence.18,19
The PCPT data not only highlight a protective effect of large prostates against general PCa but also demonstrated reduced high-grade PCa (Gleason grade ⩾ 7) incidence in larger prostates compared to small prostates (p = 0.000). Patients with large prostates are nearly 50% less likely to experience clinically significant PCa (Table 4). This clinically important finding provides a possible explanation for the original PCPT study results showing a twofold increase of high-grade PCa in the finasteride group compared to placebo. 5 Finasteride and other 5-alpha reductase inhibitors mainly reduce the volume of the TZ, a phenomenon which is more pronounced in large prostates, thus presumably reducing the mechanical stress on the PZ. Therefore, use of finasteride and other medications in the same class could lead to the recovery and uninhibited proliferation of the glandular tissue within the PZ, negating the protective effects of BPH in large prostates. However, more research is necessary to investigate this phenomenon on the effects of finasteride and other 5-alpha reductase inhibitors on the TZ and PZ in comparison to untreated BPH patients.
We acknowledge several limitations of this retrospective review of the PCPT data. Notably, the exclusion of 12,435 patients from our study arises to the lack of prostate biopsy records, which constituted the main source of obtaining prostate volume data. Potential bias based on differences in training may have affected the data collection by the urologists whose patients participated in this study. Future research should explore how medications like finasteride influence TZ and PZ dynamics, elucidating their role in PCa development.
Conclusion
The presented report on stratifying the large PCPT data set by prostate volume supports previous clinical studies and the hypothesis of an inverse relationship between prostate volume and the incidence of PCa—not only for general, but also for clinically significant PCa. This review of the PCPT data should encourage additional research on the dynamic interactions between the different prostatic zones and their impact on incidence and aggressiveness of PCa. Confirming the outlined hypothesis of the protective effects of large BPH size against prostate cancer will have significant clinical implications on future diagnostics and management of BPH and PCa.
Footnotes
Acknowledgements
None.
Ethical Considerations
Not applicable.
Contributorship
ZJS and WTWdR requested the PCPT data from the SWOG committee. SS completed the analysis of the data. ZJS, JMW, SS, and WTWdR contributed toward writing of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent to Participate
Not applicable.
Trial registration
Not applicable.
Guarantor
W.T.R.