
Abstract
Objective:
To evaluate the clinical utility of the Decipher genomic classifier in prostate biopsy specimens and its association with National Comprehensive Cancer Network (NCCN) risk stratification, metastatic outcomes, and racial differences.
Patients and Methods:
We retrospectively reviewed 88 patients with prostate adenocarcinoma who underwent Decipher testing on diagnostic biopsy tissue between 2021 and 2023. Clinical variables, Decipher risk categories, and NCCN risk groups were compared using chi-square, t-test, analysis of variance (ANOVA), and logistic regression to assess their association with distant metastasis.
Results:
Decipher risk categories showed moderate concordance with NCCN classification (Phi = 0.46, p < 0.001). Forty-five percent of patients were Decipher low risk, 30% intermediate risk, and 25% high risk. During follow-up, seven patients (8%) developed distant metastasis; four had high-risk, two intermediate-risk, and one low-risk Decipher scores. Decipher high-risk classification was more common among African American patients than Caucasian patients (44% vs 19%, p = 0.04). The receiver operating characteristic (ROC) curve showed moderate discriminative performance (area under the curve (AUC) = 0.70).
Conclusion:
Decipher testing on prostate biopsy specimens provides prognostic information beyond NCCN classification and may help identify biologic differences across racial groups, supporting its integration into personalized risk assessment.
Level of evidence:
3
Keywords
Introduction
Prostate cancer is the second most common cancer in men and displays considerable clinical variability, ranging from indolent tumors to highly aggressive disease. 1 The National Comprehensive Cancer Network (NCCN) risk classification system, based on prostate-specific antigen (PSA) level, Gleason score, and tumor stage, 2 remains widely used but lacks the resolution to identify which patients are truly at high risk for metastatic progression. 3
To address these limitations, genomic assays such as the Decipher test have emerged. Decipher evaluates the expression of 22 RNA biomarkers to calculate a score reflecting the probability of metastasis. 4 While its prognostic value has been validated in prostatectomy specimens, its utility in the biopsy setting, where most treatment decisions are made, continues to be studied. 5
Moreover, prostate cancer exhibits racial disparities in both incidence and outcomes. 1 African American men are more likely to develop aggressive disease and die of prostate cancer compared to other populations. 6 Whether genomic classifiers capture this biologic risk more effectively than clinical models remains an open question.
In this study, we evaluate the clinical utility of Decipher testing in prostate biopsy specimens. We determined the correlation between Decipher score and the development of distant metastasis; assessed the relationship between Decipher and NCCN risk categories; and explored effect of race in Decipher risk assignment and outcomes.
Methods
This retrospective cohort study included prostate cancer patients who underwent Decipher genomic testing on diagnostic biopsy tissue between January 2021 and December 2023 at a single academic institution. Demographic, clinical, pathological data, and Decipher genomic data were extracted from electronic medical records and pathology reports. This included age, self-reported race, PSA level, Gleason grade group, NCCN risk category, and Decipher risk scores, which were stratified into low (<0.45), intermediate (0.45–0.60), and high (>0.60) categories. Follow-up data were reviewed to assess the development of distant metastasis.
For comparison and analysis purposes, NCCN risk groups were consolidated as follows: low (including very low and low), intermediate, and high (including high and very high). This grouping was used consistently throughout the study to enable clearer comparison with Decipher risk categories.
Comparative analyses between Decipher risk groups, NCCN categories, and metastatic outcomes were performed using chi-square tests, one-way analysis of variance (ANOVA), and Student’s t-test, as appropriate. Logistic regression was used to identify independent predictors of metastasis. Receiver operating characteristic (ROC) curves were generated, and area under the curve (AUC) values were calculated to evaluate predictive performance. All statistical analyses were conducted using SPSS (version 28), and a p-value < 0.05 was considered statistically significant.
Results
The cohort comprised 88 patients, with a mean age of 66.5 ± 7.8 years (range, 49–82 years). Race data was available for 84 patients, among whom 67 (79.7%) were Caucasian and 16 (19%) were African American. Serum PSA levels ranged from 1.12 to 36.83 ng/mL. According to consolidated NCCN classification, 21 patients (24%) were high risk, 64 (73%) intermediate risk, and 3 (3%) low risk. In comparison, Decipher testing categorized 22 patients (25%) as high risk, 26 (30%) as intermediate risk, and 40 (45%) as low risk.
Of the 21 patients classified as NCCN high risk, 12 (57%) were also Decipher high risk, 5 (24%) were intermediate risk, and 4 (19%) were low risk. Among 64 NCCN intermediate-risk patients, 10 (16%) were reclassified as Decipher high risk, 21 (33%) remained intermediate, and 33 (52%) were reclassified as low risk. All three NCCN low-risk patients were also Decipher low-risk. Figure 1 shows the reclassification of patients between these systems using a Sankey diagram.
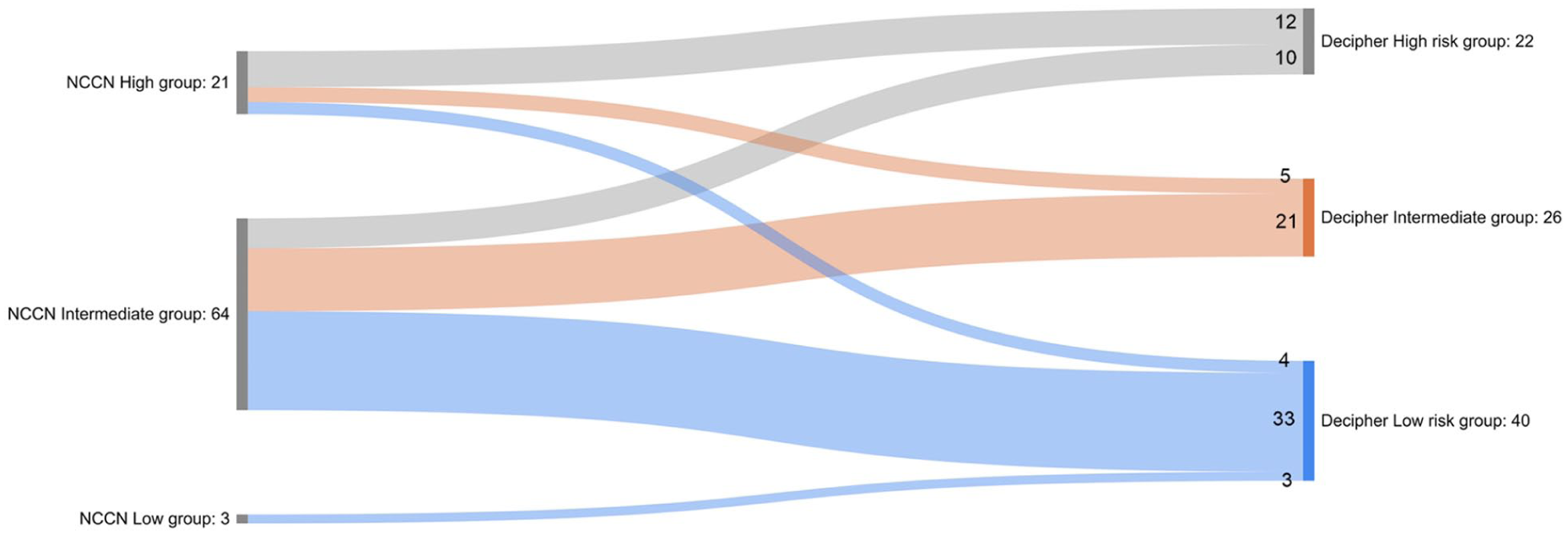
Comparison of risk stratification across decipher and NCCN risk categories using a Sankey diagram.
Concordant classification was observed in 36 patients (40.9%), while 52 (59.1%) were discordant. Concordance rates by NCCN category were 57% in high risk (12/21), 33% in intermediate risk (21/64), and 100% in low risk (3/3). Most discordant cases occurred within the NCCN intermediate-risk group. Among the 64 NCCN intermediate-risk cases, 33 were downgraded to low risk by Decipher, while 10 were upgraded to high risk by Decipher. Figure 2 elaborates the concordance and discordance between the two methods in form of comparison map.
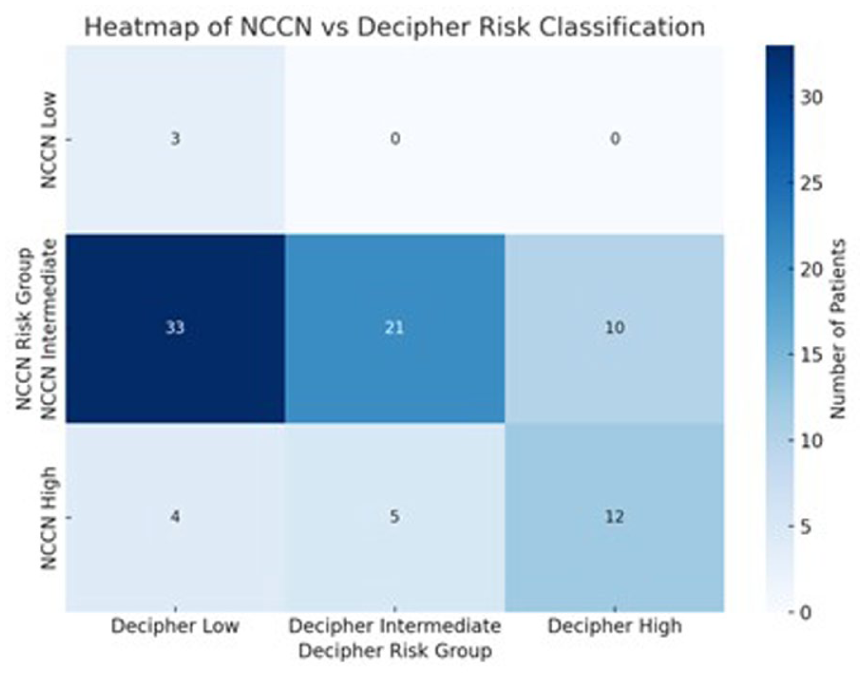
The concordance and discordance between the two methods in form of comparison map.
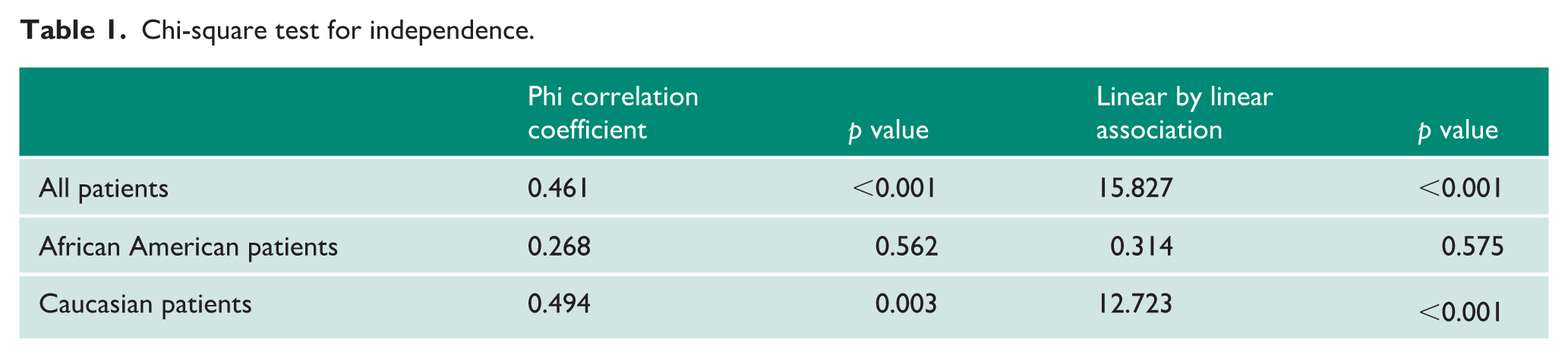
A chi-square test for independence showed a moderate and statistically significant association between NCCN and Decipher risk groups (Phi coefficient = 0.461, p < 0.001). The linear-by-linear association was 15.8 (p < 0.001), indicating a significant trend whereby increasing NCCN risk was associated with increasing Decipher risk. Despite this correlation, only 36 patients (41%) were concordantly classified. A total of 52 patients (59%) were reclassified by Decipher relative to NCCN, with most of these involving down-classification from NCCN intermediate to Decipher low risk.
Race-stratified analysis revealed that this association varied by demographic subgroup (Figure 3). Among the 67 Caucasian patients, NCCN categorized 3 (4%) as low risk, 47 (70%) as intermediate risk, and 17 (25%) as high risk. Decipher classified the Caucasian group into 33 (49%) low risk, 21 (31%) intermediate risk, and 13 (19%) high risk, indicating a notable shift toward lower genomic risk within the same clinical strata. In contrast, among the 16 African American patients, 13 (81%) were classified as NCCN intermediate risk and 3 (19%) as high risk. However, Decipher assigned only 4 (25%) of these patients to intermediate risk, while 5 (31%) were down-classified to low risk and 7 (44%) were up-classified to high risk. The correlation between NCCN and Decipher classifications was statistically significant among Caucasian patients (Phi = 0.494, p = 0.003) but not among African American patients (Phi = 0.268, p = 0.56). These results are summarized in Table 1.
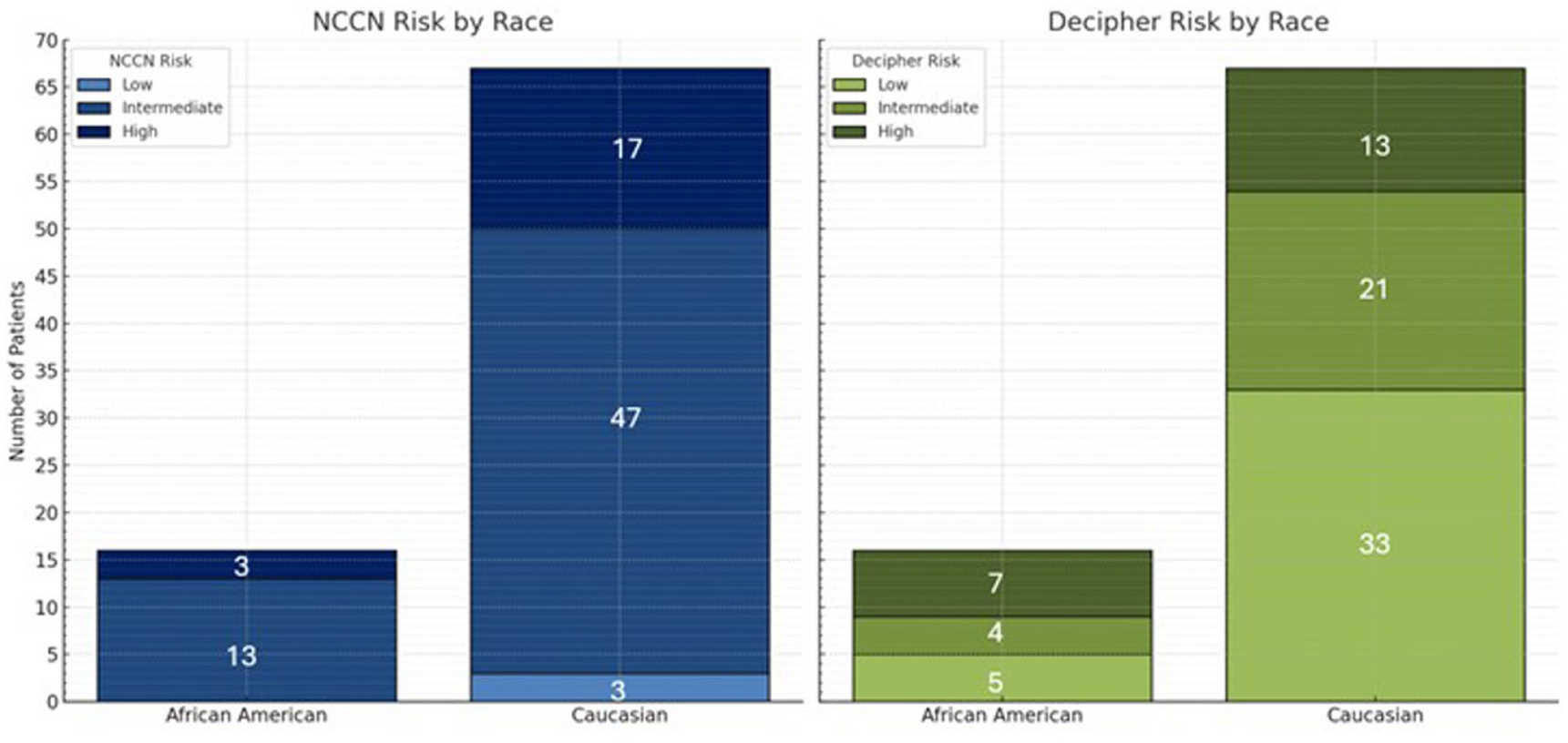
Distribution of decipher and NCCN risk groups by race.
Chi-square test for independence.
Follow-up data were available for 81 patients, with a median duration of 22 months. The ROC curve evaluating Decipher score for metastasis prediction yielded an AUC of 0.70, indicating moderate discriminative performance (Figure 4). All patients were alive at last follow-up, and 7 (8%) developed distant metastases. Of these, four were classified as high risk, two as intermediate risk, and one as low risk by Decipher.
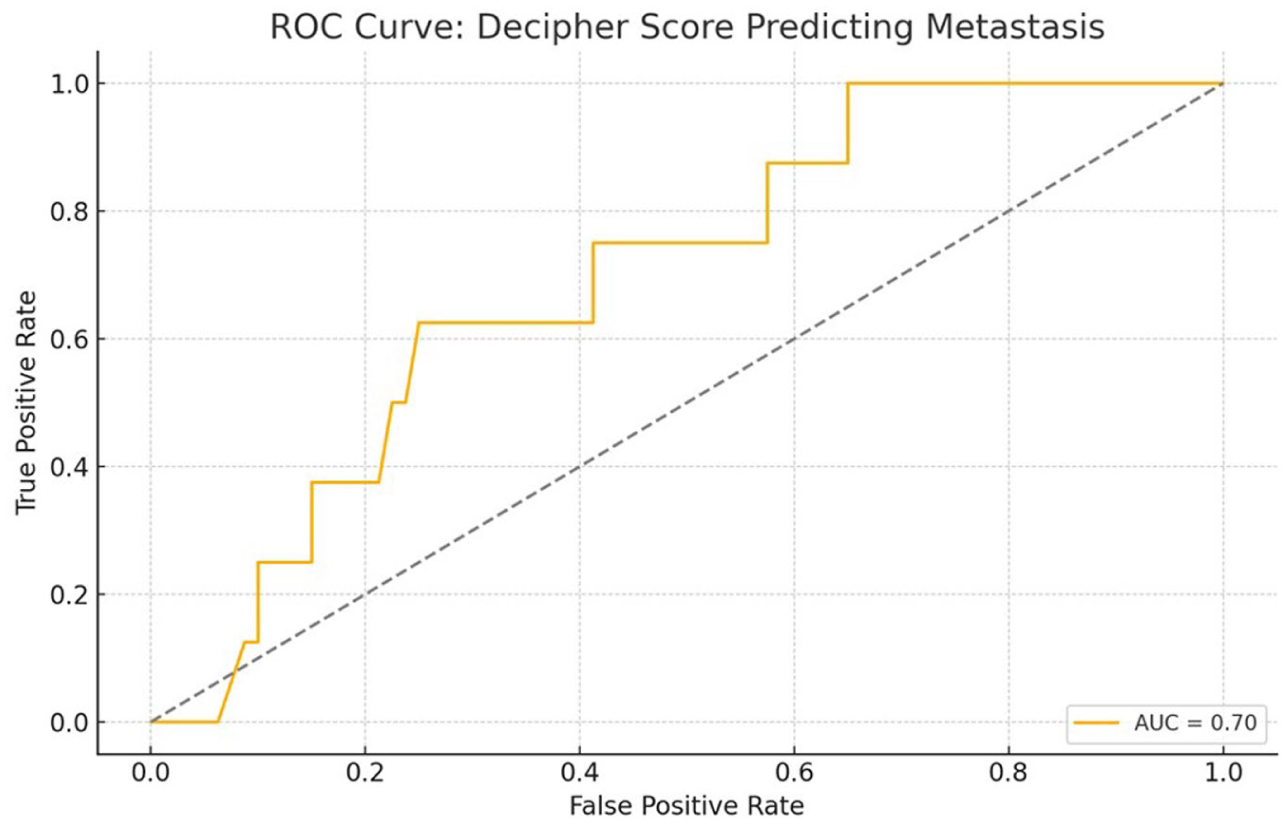
Receiver operating characteristic (ROC) curve illustrating the predictive performance of the Decipher score for distant metastasis.
Univariable logistic regression demonstrated that NCCN high-risk classification was associated with higher odds of metastasis (odds ratio (OR) = 9.1, 95% confidence interval (CI) = 1.6–52.4). Decipher high-risk classification showed a similar positive association (OR = 4.2, 95% CI = 0.8–21.0). However, both analyses were limited by the very small number of metastatic events (n = 7), resulting in wide confidence intervals and unstable estimates. Multivariable regression was not performed because the number of events did not meet the minimum threshold for reliable modeling.
In the NCCN high-risk group, 5 of 21(23.8%) patients developed metastasis. Among 22 patients classified as high risk by decipher, 4 (18%) progressed to metastatic disease. Among 12 patients who were high risk by both NCCN and decipher, 3 (25%) developed metastasis. The clinicopathologic and molecular features of these patients are summarized in Table 2. Many patients lacked prostatectomy Gleason or pathologic stage because they either presented with metastatic disease at diagnosis or were managed non‑surgically.
Clinicopathological features in seven patients with metastasis.
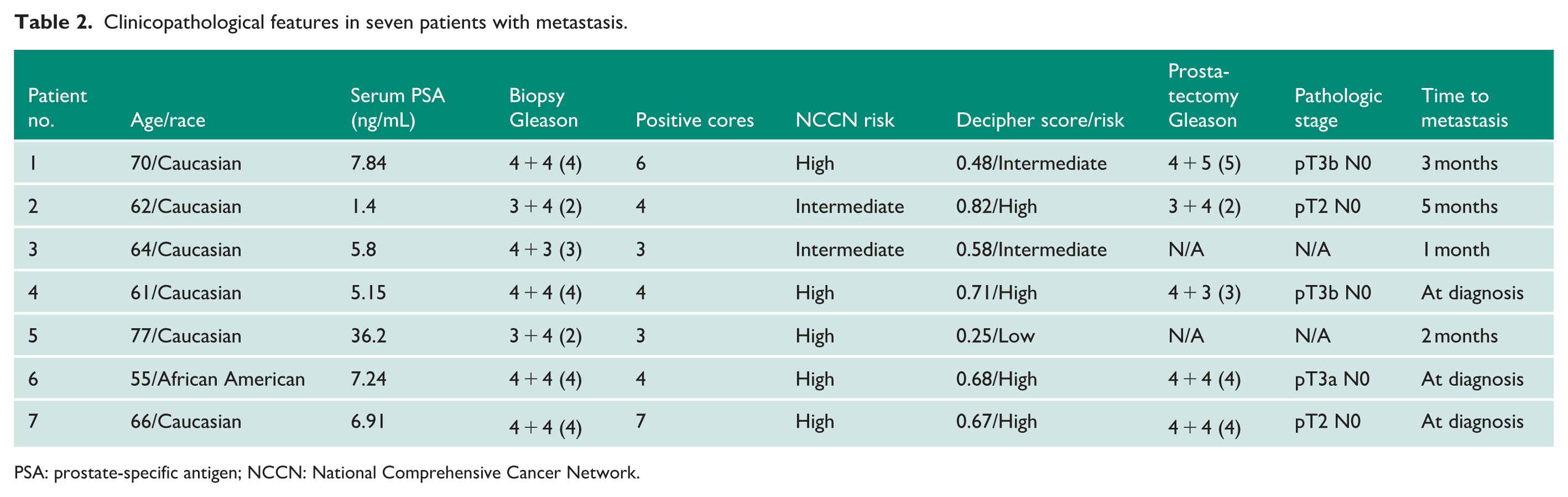
PSA: prostate-specific antigen; NCCN: National Comprehensive Cancer Network.
Of the 88 patients with available treatment data, 74 (83%) received radiotherapy and 14 (17%) did not. Among those who received radiotherapy, 46% were classified as Decipher low risk, 34% intermediate risk, and 20% high risk. In comparison, the group that did not receive radiotherapy included 36% low-risk, 36% intermediate-risk, and 29% high-risk patients. These distributions suggest that treatment decisions were not strictly based on genomic risk, with radiotherapy given across risk categories and some high-risk patients receiving alternative approaches.
Discussion
Risk stratification in prostate cancer remains central to treatment selection and prognostic evaluation. Traditional systems such as the NCCN classification rely on PSA levels, Gleason score, and clinical staging to categorize patients into risk groups. While clinically practical, these models do not always reflect the underlying tumor biology, potentially leading to over or undertreatment. In contrast, genomic tools like the Decipher classifier offer a molecular perspective on disease behavior, quantifying metastatic potential based on gene expression profiles.
Our findings confirm and support that the Decipher genomic classifier provides important prognostic information beyond traditional NCCN clinical risk stratification when applied to prostate biopsy specimens. The use of Decipher on diagnostic biopsy tissue has been increasingly studied in recent years. Several retrospective and prospective studies, as well as registry-based analyses, have confirmed its prognostic value when applied to pre-treatment biopsies. Notably, Nguyen et al. 4 assessed Decipher in biopsy samples from patients treated with radiation or surgery and found it to be an independent predictor of metastasis (hazard ratio (HR) = 1.39; p = 0.001) and prostate cancer-specific mortality (HR = 1.57; p = 0.037), with a 10-year disease-specific mortality of 0% in the low-risk group versus 9.4% in the high-risk group. Similarly, Klein et al. 5 evaluated Decipher in a cohort of 57 patients with a median follow-up of 8 years and found that it was the only significant predictor of metastasis in multivariable analysis (HR = 1.72 per 10% increase in score; p = 0.02). Combining Decipher with the NCCN model improved predictive accuracy, increasing the concordance index from 0.75 to 0.88.
In our study of 88 patients, Decipher classified 45% as low risk, 30% as intermediate risk, and 25% as high risk. These distributions closely align with those reported in prior studies. Nguyen et al. 4 reported 46% low risk, 33% intermediate risk, and 21% high risk; Vince et al., 6 in a prospective statewide registry of 855 men, reported 41%, 32%, and 27%, respectively; and Kim et al., 7 in a cohort of men eligible for active surveillance, observed 53% low-, 28% intermediate-, and 19% high-risk groups. In addition, a systematic review by Jairath et al. 8 summarizing data from over 30,000 patients reported Decipher risk distributions of approximately 52% low risk, 22% intermediate risk, and 26% high risk. The consistency of our findings with these external datasets reinforces the validity of our cohort and supports the broader clinical relevance of Decipher testing in pre-treatment biopsy specimens.
We observed a moderate concordance between NCCN and Decipher classifications (Phi coefficient = 0.461), consistent with earlier reports indicating that these systems assess overlapping but distinct biological dimensions. Although the Phi coefficient demonstrated a moderate association between NCCN and Decipher risk groups (Phi = 0.461), this does not imply high agreement at the individual-patient level. As shown in our cohort, 59% of patients were reclassified by Decipher relative to NCCN, most commonly within the intermediate-risk group. A moderate correlation simply reflects that both systems trend in the same direction across the population, while the high discordance rate highlights that the two models capture different dimensions of tumor biology, leading to frequent patient-level re-stratification. Vince et al. 6 demonstrated similar association rates and highlighted that Decipher contributes independent prognostic value, particularly for refining intermediate-risk patients. Similarly, Gore et al. 9 found that Decipher improved post-biopsy decision-making, including identifying candidates for active surveillance and early definitive therapy, suggesting its role in fine-tuning NCCN risk assignments.
A key observation in our cohort was the high rate of discordance between NCCN and Decipher risk categories whereby 59% of patients were classified differently by Decipher and NCCN. Most of these involved NCCN intermediate-risk patients reclassified as low risk by Decipher. This aligns with findings from Marascio et al., 10 who reported that Decipher can down-classify patients with otherwise ambiguous clinical features, potentially reducing overtreatment. Roidos et al. 11 further validated this utility by showing that Decipher-guided decisions led to de-escalation of therapy without compromising short-term oncologic outcomes.
Conversely, some patients in our study were upgraded to high-risk by Decipher despite intermediate-risk classification by NCCN. This mirrors the findings of Marrone et al., 12 who found that Decipher could unmask high-risk molecular features not reflected in standard histopathology. Zaorsky et al. 13 similarly reported that patients with low NCCN risk but high Decipher scores had worse long-term outcomes, advocating for the incorporation of genomic tools in treatment planning to avoid undertreatment.
In our cohort, only four of seven patients (57%) who developed distant metastasis were classified as high risk by Decipher. This highlights a critical limitation: while Decipher enriches for high-risk cases, it may not identify all patients at risk for progression. This underscores the need to interpret genomic classifiers in conjunction with clinical and pathological data, as recommended by Klein et al., 5 who emphasized that Decipher should complement and not replace traditional risk models due to its inability to fully capture the heterogeneity of tumor behavior.
We also observed racial differences in Decipher scoring. Although only one African American patient in our cohort developed metastasis, 44% were classified as Decipher high-risk compared to 19% of Caucasian patients. Jairath et al. 8 conducted a systematic review involving over 30,000 patients and noted that while the Decipher genomic classifier is prognostic across various clinical endpoints, its performance may vary by race, with differences in score distributions observed among Black versus White patients. They emphasized the need for further calibration in diverse populations to avoid biased risk categorization. Similarly, Zaorsky et al. 13 echoed this concern, analyzing Decipher scores in a multi-institutional cohort, and found that Black patients had significantly lower Decipher scores than White patients despite comparable clinicopathologic features, suggesting potential underestimation of risk. The authors stressed the need for ancestry-specific validation to ensure equitable clinical application of genomic tools. 14
The Decipher score demonstrated moderate discriminative ability for predicting metastasis in our cohort (AUC = 0.70), consistent with Leapman et al., 15 who found that Decipher reliably predicted distant metastasis in biopsy specimens when used in combination with clinical variables. However, the presence of metastatic progression in patients with low or intermediate Decipher scores in our study reiterates the multifactorial nature of prostate cancer progression and supports the conclusion from Fuerst et al. 16 that no single classifier is sufficient for comprehensive risk prediction. We found that high NCCN risk group and high decipher risk score combined predict metastatic disease in prostatic adenocarcinoma slightly better than either risk classifier alone. These findings reinforce the value of multi-modal risk assessment strategies. Table 2 shows clinicopathological features in seven patients with metastasis.
While the majority of patients received radiotherapy, the treatment distribution across Decipher risk groups suggests that clinical decision-making was not strictly guided by genomic classification. Radiotherapy was administered to patients across all Decipher risk categories, and some high-risk patients were managed without it. This pattern highlights the variability in real-world treatment practices and underscores the potential utility of Decipher in supporting more personalized, risk-aligned therapeutic strategies.
Limitations of this study include its retrospective design, modest sample size, and the small number of metastatic events. The median follow-up of 22 months is relatively short for assessing metastatic progression in prostate cancer, where distant metastases often occur several years after diagnosis. This limited follow-up likely contributed to the small number of metastatic events (7 of 81 patients), which in turn constrains the robustness of the ROC analysis and limits the statistical power of regression modeling. Nonetheless, our dataset reflects real-world biopsy practice and supports the integration of genomic testing into early-stage decision-making. Molecular classifiers like Decipher hold the potential to personalize treatment, and refine risk stratification, provided they are validated across diverse patient populations and used in conjunction with traditional risk factors.
Footnotes
Acknowledgements
The authors would like to acknowledge the technical and logistical support of the University of Kansas Medical Center pathology laboratory staff for their assistance with Decipher testing and data retrieval.
Ethical considerations
This study was approved by the Institutional Review Board of the University of Kansas Medical Center.
Consent to Participate
The study used de-identified retrospective data and did not require patient consent according to institutional policy.
Author contributions
Hebatullah Elsafy and Ameer Hamza conceived the study design and supervised data collection. Maryam Abdo contributed to data acquisition and statistical analysis. Margaryta Stoieva and Zubaidah Khalaf assisted in data interpretation and manuscript editing. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request. De-identified patient information cannot be publicly shared to protect privacy.
Guarantor
H.E.