ePoster Session 1: Prostate Cancer 1, Paddy O’Reilly, June 15, 2026, 16:30 - 17:30
P1-1 The Role of an AI-based Model to Predict Long-Term Oncological Outcomes in Prostate Cancer Treated with Radical Prostatectomy
Dr Davide Farinati1, Dr Alexandre Calado1, Dr Alejandro Granados3, Dr Nicholas Raison2,3, Dr Prokar Dasgupta2,3, Dr Giorgio Gandaglia1, Dr Alberto Briganti1
1Unit of Urology/Division of Oncology, URI, IRCCS Ospedale San Raffaele, Milano, Italy, 2Department of Urology, Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom, 3School of Biomedical Engineering & Imaging Sciences, King’s College London, London, United Kingdom
Introduction: Accurate prediction of long-term outcomes after radical prostatectomy (RP) for prostate cancer (PCa) remains challenging. Existing prognostic tools rely on static clinicopathological variables and cannot incorporate longitudinal follow-up data. We developed and internally validated BertPCa, an artificial intelligence (AI) model for dynamic prediction of oncological outcomes after RP.
Patients and Methods: We analyzed 4,634 RP patients treated between 1990 and 2024 with ⩾2 years of follow-up. For biochemical recurrence (BCR) analysis, 3,971 patients were included; all patients were analyzed for cancer-specific mortality (CSM). Follow-up extended to 15 years. Patients were split into training (80%), validation (10%), and test (10%) sets. BertPCa is a deep learning model that integrates longitudinal follow-up data to continuously update risk predictions. Its performance was compared with Dynamic DeepHit, Cox regression, Random Survival Forest, and the CAPRA-S and MSKCC nomograms using time-dependent concordance indices.
Results: Key predictors of CSM were follow-up PSA, clinical recurrence, percentage of positive lymph nodes, adjuvant hormonal therapy, and intra-operative transfusion. Predictors of BCR included follow-up PSA, pathological ISUP grade, positive surgical margins, percentage of positive biopsy cores and lymph nodes, PSA at diagnosis, and seminal vesicle invasion. BertPCa achieved the highest accuracy for both outcomes, with mean concordance indices of 78% for BCR and 96% for CSM, outperforming all comparator models.
Conclusions: BertPCa provided superior dynamic prediction of BCR and CSM compared with established tools. Integration of follow-up data allows continuously updated risk assessment and may improve personalized postoperative surveillance.
P1-2 Variation in PSA testing rates across ethnic and socioeconomic groups in Northwest London
Mr Nikhil Mayor1, Dr Victoria Vickerstaff2, Ms Beth Graham3, Professor Rhian Gabe2, Professor Hashim Ahmed1
1Imperial College London, London, United Kingdom, 2Queen Mary University of London, London, United Kingdom, 3North London Regional Research Delivery Network, London, United Kingdom
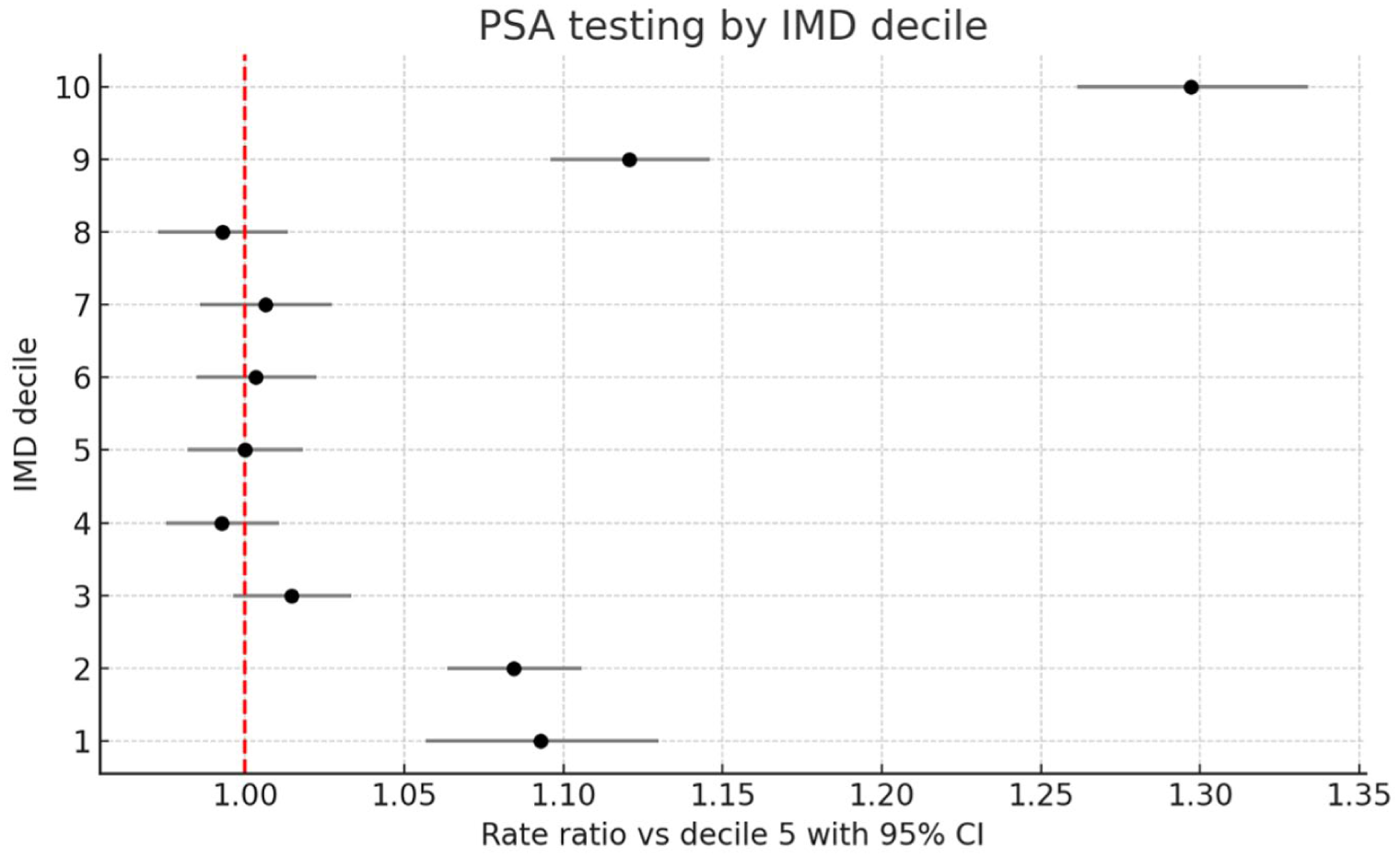
Introduction: Contemporary data describing variation in opportunistic PSA testing is lacking. We examined patterns of PSA testing by age, ethnicity, and deprivation status in northwest London (NWL).
Methods: We performed a retrospective analysis using the Whole Systems Integrated Care dataset in NWL (data obtained 31/03/25). Aggregated primary care data were analysed for 330,579 men aged 50-74 years across NWL (2020-2025).
Results: PSA testing increased with age, rising from 20.0% (95% CI 19.7-20.2) in men aged 50-54 to 50.5% (50.0-51.0) in those 70-74 (RR 2.53, 2.48-2.57). Compared with White men (33.5%, 33.3-33.8), uptake was higher in Black or Black British men (43.8%, 43.2-44.4; RR 1.31, 1.29-1.32) and Mixed ethnicity (37.3%, 36.2-38.3; RR 1.11, 1.08-1.14), similar in Asian men (32.8%, 32.5-33.1; RR 0.98, 0.97-0.99), and lower in Other ethnic groups (30.0%, 29.5-30.4; RR 0.89, 0.88-0.91). PSA testing showed modest variation across IMD deciles (range: 31-41%). Testing was lowest in the middle deciles (3-8) and higher at extremes of deprivation status (deciles 1-2 and 9-10). Testing in the least deprived group was higher compared to the reference group (41.1%, 40.1-42.2; RR 1.30, 1.26-1.33).
Conclusion: PSA testing in NWL shows marked variation across demographic and socioeconomic groups. Uptake increased steeply with age, with over half of men aged 70-74 tested between 2020 and 2025. Black men were around 30% more likely to be tested than White men, and testing was highest among the least deprived. These patterns suggest that the lack of formal PCa screening may exacerbate inequities in PCa detection by socio-economic status.
P1-3 Oncological and functional outcomes following salvage robot assisted radical prostatectomy following radiation or ablation failure
Miss Deepika Reddy1, Luis Ribeiro1, Paul Cathcart1
1Guy’s and St Thomas’ Hospital, London, United Kingdom
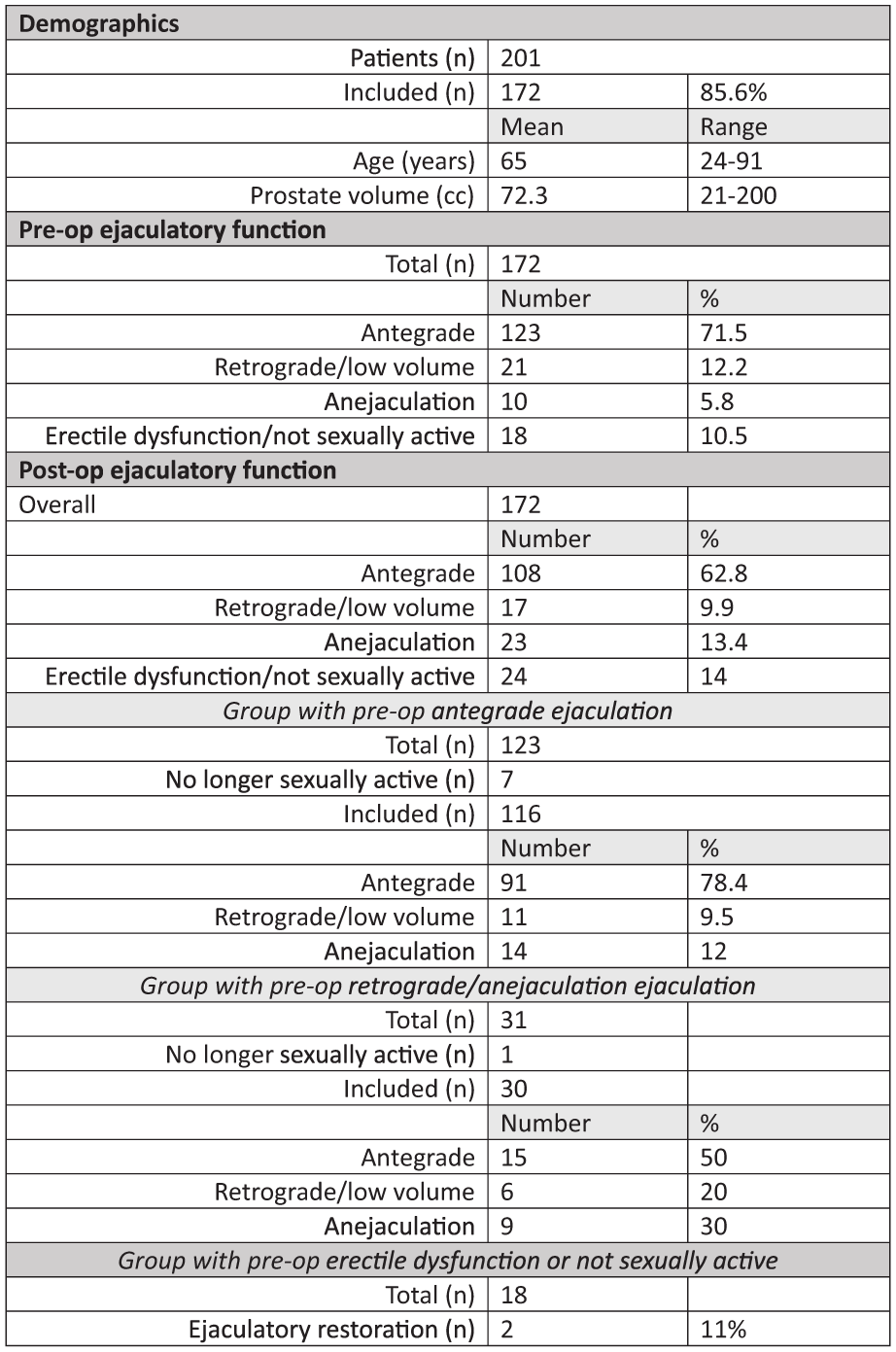
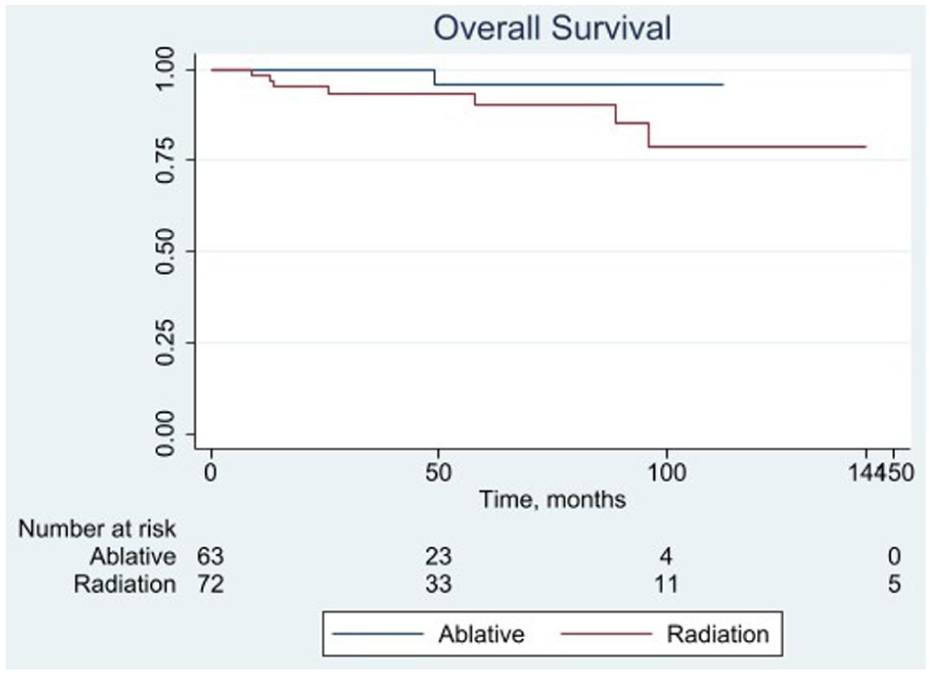
Introduction: Patients diagnosed with recurrent prostate cancer following focal ablation or radiotherapy treatment have limited options with curative intent. Salvage robot assisted radical prostatectomy(sRARP) is becoming more common for patients with localised recurrent disease. We report sRARP outcomes from a single surgeon.
Methods: Patients treated with sRARP following primary treatment with ablative therapy(any modality), radical brachytherapy or radical radiotherapy and received sRARP were included. Primary outcome was overall survival(OS), secondary outcomes were rates of urinary continence (in those continent pre-sRARP) and erectile function at 1-year were reported according to retrospective review of case notes.
Results: 136 patients were included: 63 had primary focal therapy, 52 had radiotherapy, 21 had brachytherapy. Median(IQR)age, PSA prior to sRARP, time from primary treatment to sRARP and median follow-up time was 67 years(61-71), 4.6ng/ml(3.4-8.5) and 72 months(40-122) and 34 months(18-84). 12-year OS was 78%(95% CI 55-91) following radiation/brachytherapy, only one patient died following sRARP for ablative therapy failure.
Following radiation/brachytherapy treatment 35/67(52%) were dry, 13/67(19%) reported terminal dribbling only, 19/67(28%) required ⩾1pad/day. 9/73(12%) reported spontaneous erectile function +/- PDE5 inhibitors, 28/73(38%) required penile vacuum pump use. Following focal therapy 56/62(90%) were dry, 2/62(3%) reported terminal dribbling only, 3/62(5%) patients required ⩾pad/day. 17/50(34%) reported spontaneous erectile function +/- PDE5 inhibitors, 31/50(62%) required penile vacuum pump use.
Conclusions: 80% of patients were alive by 12-years following treatment. Continence rates were well preserved at 1-year. In high volume centres, sRARP can provide oncological control for patients that would otherwise be subject to systemic treatment or watchful waiting regimes.
P1-4 Implementation of the Hugo™ robotic platform for radical prostatectomy: comparative 1-year functional and oncological outcomes from a UK high-volume centre
Ms Isabel Sanz Gómez1, Mr Findlay MacAskill1, Mrs Cynthia O’ Sullivan1, Ms Beatrice Ehrrooth2, Professor Prokar Dasgupta2, Mr Paul Cathcart1, Mr Jonathan Noël1, Mr Alastair Lamb1, Mr Kalyan Gudaru2, Mr Arun Shai1, Mr Majed Shabbir1, Mr Samuel Davis1, Professor Ben Challacombe2
1Guy’s And St Thomas NHS Fundation Trust, London, United Kingdom, 2Guy’s and St Thomas’ Hospitals & King’s College London, London, United Kingdom
Introduction: Use of the Hugo robotic platform for radical prostatectomy has expanded, yet data on functional outcomes remain limited. This study aimed to compare one-year functional and oncological outcomes in an initial cohort of Hugo cases with a contemporary cohort of da Vinci patients at a high-volume UK centre.
Materials and methods: Patients undergoing primary Hugo RARP were prospectively collected and subsequently propensity-matched to contemporary da Vinci cases based on age, PSA and body mass index. Functional and oncological outcomes were assessed at 3, 6 and 12 months. Urinary continence was defined as pad-free status. Erectile function was evaluated using erection hardness score (EHS), International Index of Erectile Function and need for intracavernosal injections. Oncological outcomes included positive surgical margins (PSM) and undetectable PSA (<0.03 ng/mL).
Results: A total of 112 matched pairs were analyzed. Urinary continence outcomes were similar between both groups across follow-up. At 12 months, 67% patients in the Hugo group and 61% in the da Vinci group were pad-free. Erectile function recovery also followed a similar course in the two platforms, with comparable potency rates (EHS ⩾3) at 12 months of 35% and 36%, for Hugo and da Vinci, respectively. No differences in PSM rate (20% Hugo vs 17% da Vinci) or in undetectable PSA rate at 3, 6 and 12 months.
Conclusions: Functional and oncological outcomes at 1 year were comparable between the Hugo and Da Vinci platforms, suggesting that the Hugo system may represent a valid alternative to established robotic platforms.
P1-5 Skeletal muscle index as a prognostic and predictive biomarker in de novo hormone sensitive prostate cancer: an exploratory analysis of the STAMPEDE ARPI trials
Mr Struan Henry Gray1,2, Dr Donal McSweeney1, Mr Omar El-Taji2, Dr Peter Dutey-Magni3, Mr Craig Jones4, Dr Mick Brown1, Professor Louise Brown3, Professor Max Parmar3, Professor Gert Attard3, Professor Nick James5, Dr Alan McWilliam1, Professor Noel Clarke1,2, Mr Ashwin Sachdeva1,2
1The University of Manchester, Manchester, United Kingdom, 2The Christie Hospital, Manchester, United Kingdom, 3University College London, London, United Kingdom, 4Stockport NHS Foundation Trust, Stockport, United Kingdom, 5Royal Marsden Hospital and The Cancer Institute, , United Kingdom
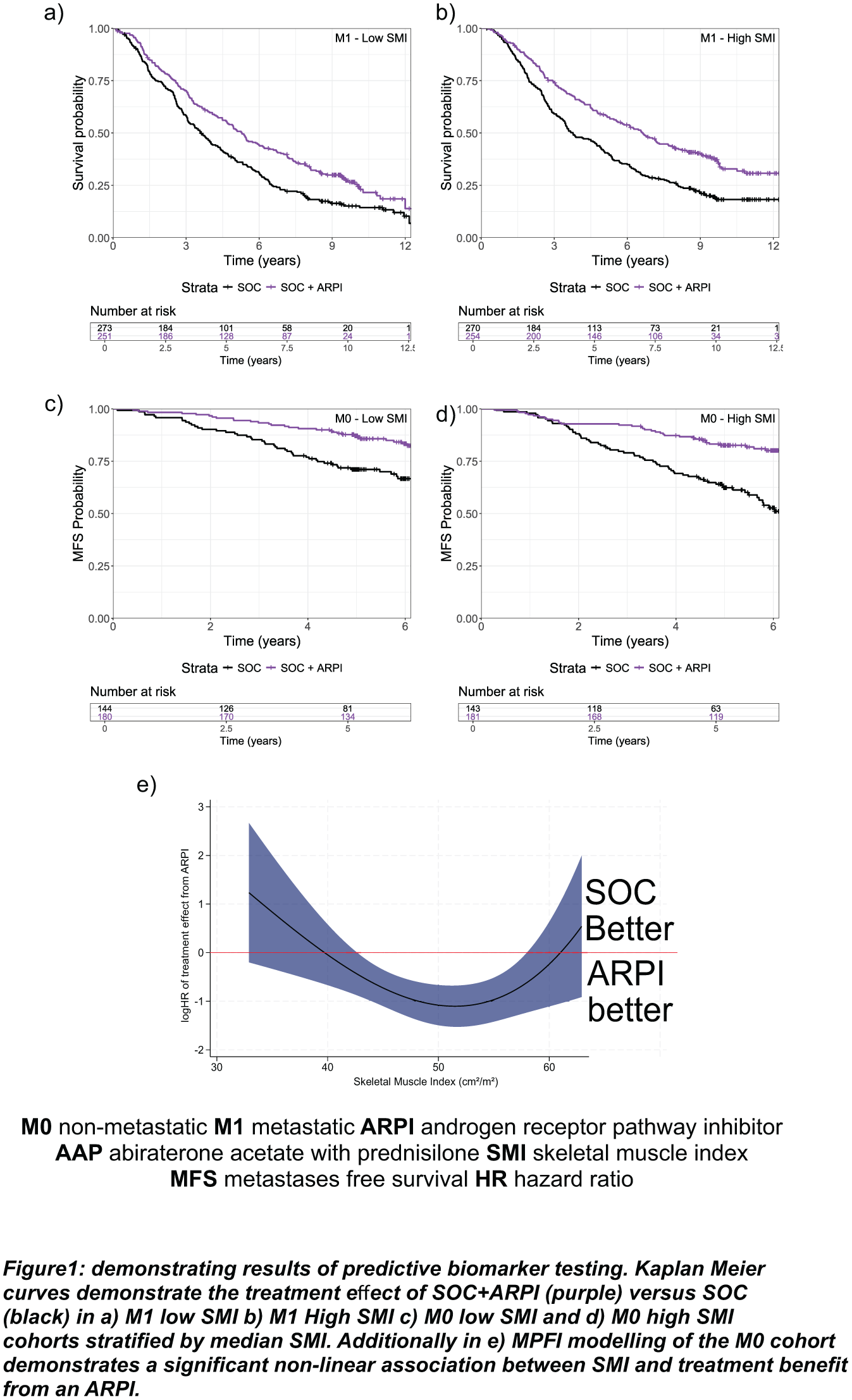
Background: Sarcopenia is common in advanced prostate cancer and exacerbated by androgen deprivation therapy (ADT). We evaluated CT-derived skeletal muscle index (SMI) as a prognostic and predictive biomarker in the STAMPEDE androgen receptor pathway inhibitor (ARPI) trials.
Methods: Men with newly diagnosed non-metastatic high-risk (M0) or metastatic (M1) hormone-sensitive prostate cancer (HSPC) were included. Trials compared standard of care (SOC) with abiraterone acetate plus prednisolone (AAP) ± enzalutamide (Enz). SMI (cm²/m²) was calculated as mean skeletal muscle area divided by height squared. Outcomes were overall survival (OS) in M1 disease and metastasis-free survival (MFS) in M0 disease. Prognostic value was assessed using Kaplan–Meier analyses and Cox regression. Predictive value was evaluated by comparing treatment hazard ratios across high/ low SMI cohorts and testing for treatment–SMI interactions using likelihood ratio tests. Continuous predictive effects were explored using multivariable fractional polynomial interaction (MFPI) models.
Results: 1,696 patients were included (1,048 M1; 648 M0). Each 10 cm²/m² increase in SMI was associated with a 15% reduction in risk of death (HR 0.85, 95% CI 0.79–0.92; p<0.001). In M0 disease, SMI was an independent predictive biomarker for MFS benefit (figure 1) from AAP±Enz. MFPI modelling demonstrated increasing MFS benefit with rising SMI (χ²=9.95, p=0.006), limited to an SMI range of 41–63 cm²/m²; 20% of patients lay outside this range and did not benefit.
Conclusions: SMI is an independent prognostic biomarker and predicts MFS benefit from AAP±Enz in M0 HSPC, showing promise as an accessible biomarker guiding treatment intensification requiring real-world validation.
P1-7 The added value of diffusion-weighted imaging and dynamic contrast-enhanced sequences in the diagnosis of localised radiorecurrent prostate cancer: an analysis from the FORECAST trial
Mr Alexander Light1, Ms Abi Kanthabalan2, Professor Shonit Punwani3, Professor Mark Emberton2, Professor Hashim U. Ahmed1, Mr Taimur T. Shah1, FORECAST Study Group
1Imperial Prostate, Imperial College London, London, United Kingdom, 2Division of Surgery & Interventional Science, University College London, London, United Kingdom, 3Division of Medicine, University College London, London, United Kingdom
Introduction: mpMRI is highly sensitive for detecting localised recurrent prostate cancer post-radiotherapy. This exploratory analysis aimed to assess the additive value of DWI and DCE sequences for detecting localised radiorecurrent cancer.
Patients and methods: FORECAST (NCT01883128) was a phase 2b UK multicentre prospective paired-validating cohort study assessing the accuracy of mpMRI compared to 5mm transperineal template mapping biopsy. Patients were recruited between 2014-2018 from 6 UK centres with biochemical failure after previous EBRT and/or brachytherapy. Radiologists, blinded to other data, first assessed the T2W sequence, then T2W and DWI together, then T2W, DWI, and DCE together. MRI Likert scores 3-5 were considered a ‘positive’ MRI. The diagnostic accuracy and proportions of cancer detected with each sequence combination were assessed.
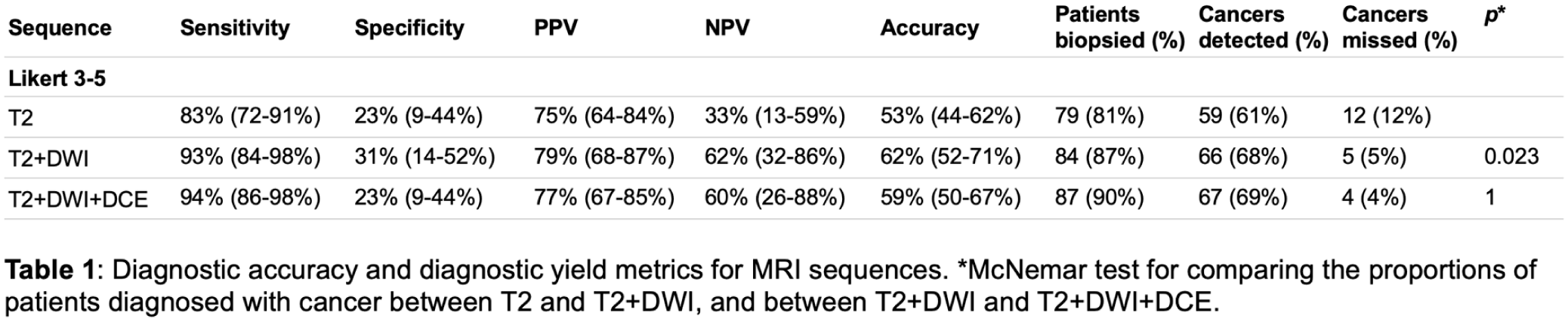
Results: Of 97 included patients, 73 (75%) had radiorecurrent cancer identified. The T2W sequence alone only had sensitivity 84% (95%CI 73-91%), specificity 25% (95%CI 10-47%), PPV 77% (95%CI 66-86%), NPV 33% (95%CI 13-59%), and accuracy 54% (95%CI 45-54%; Table 1). Adding DWI significantly increased cancer detection (difference 7%; p=0.023), conferring sensitivity 93% (95%CI 85-98%), specificity 33% (95%CI 16-55%), PPV 81% (95%CI 71-89%), NPV 62% (95%CI 32-86%), and accuracy 63% (95%CI 53-73%). Adding DCE did not significantly increase cancer detection (difference 1%; p=1), conferring sensitivity 95% (95%CI 87-99%), specificity 25% (95%CI 10-47%), PPV 79% (95%CI 69-87%), NPV 60% (95%CI 26-88%), and accuracy 60% (95%CI 51-60%).
Conclusions: A biparametric MRI incorporating T2W and DWI sequences may be sufficient for detecting localised radiorecurrent prostate cancer; evaluation in a well-powered prospective study is required.
P1-8 Concordance between local and central MRI reporting for prostate cancer diagnosis: an analysis from the PRIME trial
Ms Aqua Asif1, Dr Alexander Ng1, A/Prof Louise Dickinson1, Dr Giorgio Brembilla1, A/Prof Francesco Giganti1, Dr Clare Allen1, Prof Veeru Kasivisvanathan1, on behalf of the PRIME Study Group1
1University College London, London, United Kingdom
Introduction: Prostate MRI interpretation varies between readers, potentially affecting biopsy decisions and downstream patient management. Understanding agreement between routine local reporting and central review is important to contextualise diagnostic decision-making and identify where standardisation or feedback may improve consistency of care.
Methods: PRIME (NCT04571840) enrolled men with suspected prostate cancer (PSA⩽20 ng/mL, no prior biopsy) undergoing MRI across 22 centres in 12 countries. Local radiologists reported MRI suspicion using both Likert and PI-RADSv2.1 scoring systems. All scans underwent blinded central review by genitourinary radiologists, each with ⩾10 years’ prostate MRI experience. Agreement was assessed for biparametric MRI (bpMRI) and multiparametric MRI (mpMRI). Concordant biopsy decisions were defined as agreement on whether biopsy was indicated (score ⩾3 vs ⩽2).
Results: 488/490 patients had MRIs accessible for central review. Agreement in biopsy decision was 88.1% (430/488) for bpMRI Likert, 88.3% (431/488) for mpMRI Likert, 88.3% (431/488) for bpMRI PI-RADS, and 88.9% (434/488) for mpMRI PI-RADS. Discordance occurred predominantly at intermediate suspicion thresholds. Central readers assigned lower suspicion scores overall: for bpMRI Likert, 45.1% (220/488) of local reads were scored ⩾3 versus 40.2% (196/488) centrally, with similar patterns across other assessments. More cases were downgraded than upgraded by central review.
Conclusions: Agreement between local and central readers was high across scoring systems and MRI protocols. Discordance clustered at intermediate suspicion levels, where inter-reader variability most influences biopsy decisions. These findings support continued emphasis on prostate MRI training, standardised reporting, and structured feedback to improve consistency in clinical practice.
P1-9 Unified PSA Follow-Up Pathway within an NHS Urology Service: A Standardised Flowchart for Consistent Post-Referral Management and Post-Treatment PSA Monitoring
Mr Saeid Haghdani1, Mr Ehab Abusada1, Mr Ketan Agarwal1, Mr Mohan Pillai1
1East Lancashire Hospitals NHS Trust, Blackburn, United Kingdom
Introduction: Prostate-specific antigen (PSA) testing underpins prostate cancer detection and longitudinal monitoring, yet follow-up protocols differ widely across NHS centres. We aimed to design a unified, evidence-based PSA follow-up pathway applicable to all clinical scenarios, including initial referral, post-biopsy, active surveillance, post-radical therapy, and watchful waiting, to enhance consistency and efficiency within our trust.
Materials and Methods: A departmental review of NICE NG131, European Association of Urology (EAU), and NHS England follow-up recommendations was conducted. Existing local protocols were benchmarked against national standards. A unified algorithm was then developed through multidisciplinary meetings, detailing PSA monitoring intervals, re-referral thresholds, and discharge criteria. The resulting flowchart was ratified by the departmental governance committee for implementation in clinician-led follow-up clinics.
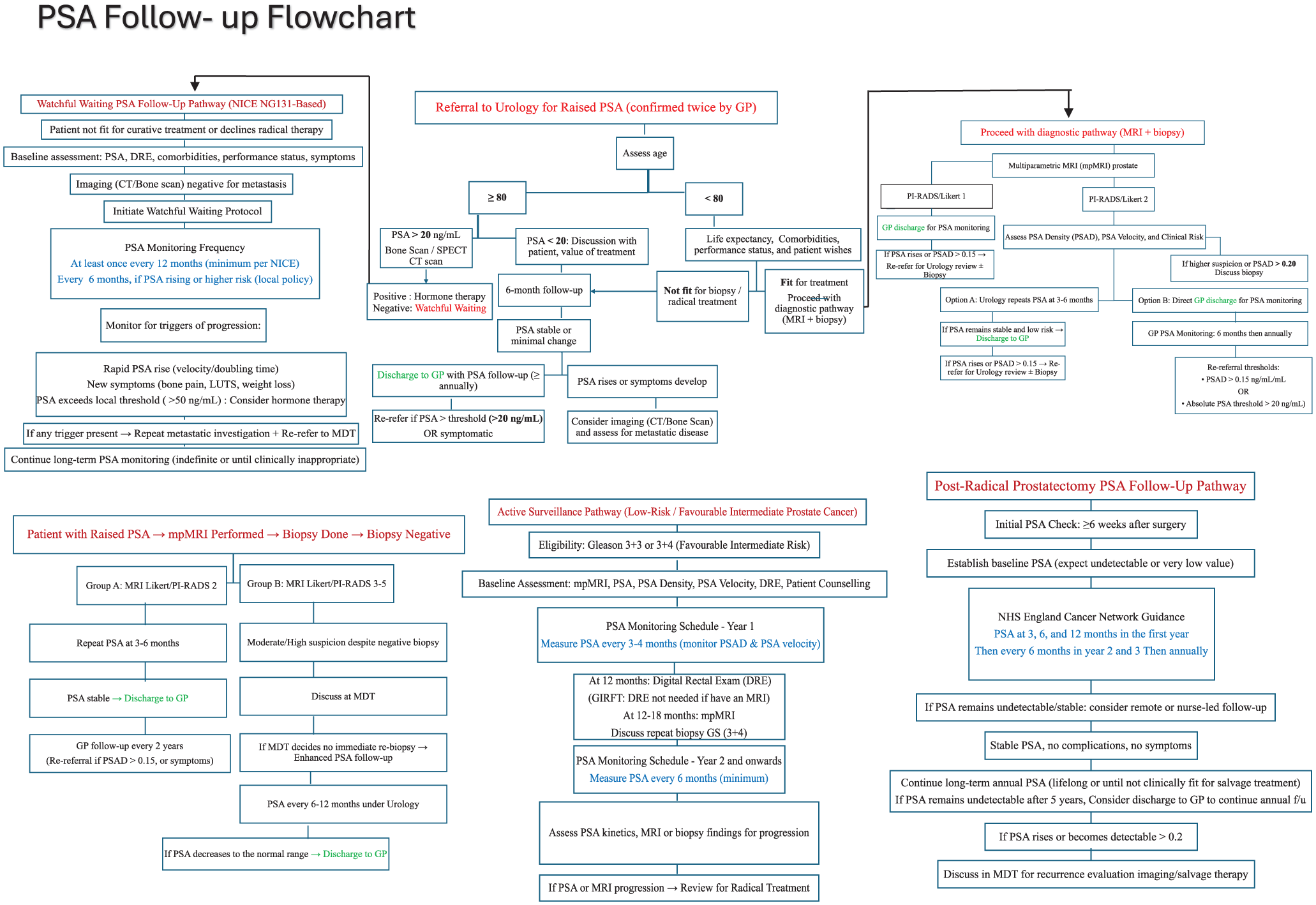
Results: The unified PSA Follow-Up Pathway integrates five clinical branches: (1) referral for raised PSA, (2) MRI Likert 1–2 or 3–5 with/without biopsy, (3) active surveillance, (4) post-radical prostatectomy, and (5) watchful waiting. It defines evidence-based PSA intervals (3–6 monthly in early surveillance, 6-monthly post-radical treatment for 2 years, then annually) and re-referral triggers (PSA density > 0.15 ng/mL/mL or velocity > 0.75 ng/mL/year). This approach promotes consistency, reduces unnecessary hospital reviews, and supports safe discharge to primary care.
(Figure 1: Unified PSA Follow-Up Flowchart)
Conclusions: This clinician-led, unified PSA follow-up pathway provides a standardised model for PSA monitoring across diagnostic and post-treatment settings, ensuring alignment with NICE and EAU guidance, improving communication between secondary and primary care, and optimising resource utilisation.
P1-10 ePoster Session 1: Prostate Cancer 1, Paddy O’Reilly, June 15, 2026, 16:30 - 17:30
Objectives: There is ongoing debate on the value of DRE as a primary care test for prostate cancer. Here we compared cancer yields of abnormal DRE with/without a raised PSA
Patients & Methods: A prospective database of 1395 men referred to our centre for suspected prostate cancer (Jan-Dec 2025) was interrogated. Data was collected for referral reason, age, PSA and detection of ⩾Cambridge Prognostic Group (CPG) 2, ⩾CPG3 and metastatic disease. Two criteria for raised PSA were used – NICE CKS age adjusted PSA (https://cks.nice.org.uk/topics/prostate-cancer/diagnosis/assessment/) and a single PSA ⩾3ng/ml threshold.
Results: 290 abnormal DRE referrals with a concurrent PSA was available for analysis. Median age and PSA was 71years (35-94) and 3.7ng/ml (0.12-1618) respectively. Using age-referenced PSA thresholds, 92/290 men had concurrent raised PSA. In these men with an abnormal prostate DRE and raised PSA,⩾CPG2, ⩾CPG3 and metastatic cancers was detected in 45.6% (43/92), 36.9% (35/92) and 18.4% (18/92) respectively. In comparison for men with a normal age-referenced PSA this was 3.5% (7/198), 2.0% (4/198) and 0% respectively. Using a blanket PSA ⩾3ng/ml threshold, 165/290 men were classed as raised PSA. In these men ⩾CPG2, ⩾CPG3 and metastatic cancer detection was 29.1% (48/165), 23.6% (39/165) and 10.9% (18/165). For men with PSA<3 however, these rates were 1.6% (0/125), 0% and 0% respectively.
Conclusions: A raised PSA referral without the DRE in this cohort would have detected >96% of significant cancers without missing metastatic disease. Removing DRE from national guidance would reduce referrals by 9-14% without impacting cancer survival outcomes.
ePoster Session 2: General - Management, Governance, Education and Quality Improvement 1, Olympia, June 15, 2026, 16:30 - 17:30
P2-1 Factors predicting surgical opportunities among Urology Higher Specialty Trainees (ST3-ST7) in the UK: A Retrospective Analysis from 2010-2024
Miss Justina Cheh Juan Tai1, Miss Kelly Ong1, Mr Stuart Graham2, Miss Justine Royle3, Mr Tony Tien2
1Royal London Hospital, London, United Kingdom, 2Whipps Cross University Hospital, London, United Kingdom, 3Aberdeen Royal Infirmary, NHS Grampian, Aberdeen, Scotland
Objectives: To characterise national trends in operative experience among UK Urology Higher Specialty Trainees (HST) over time, and to identify demographic, training, and institutional factors associated with operative volume.
Methods: This national, retrospective study analysed Intercollegiate Surgical Curriculum Programme (ISCP) and eLogbook data for all UK Urology HSTs from 2010-2024. The following factors were analysed against operative volume: gender, age at ST3 start, ethnicity, training grade, and hospital type, i.e. district general hospital (DGH) versus tertiary centre (TC).
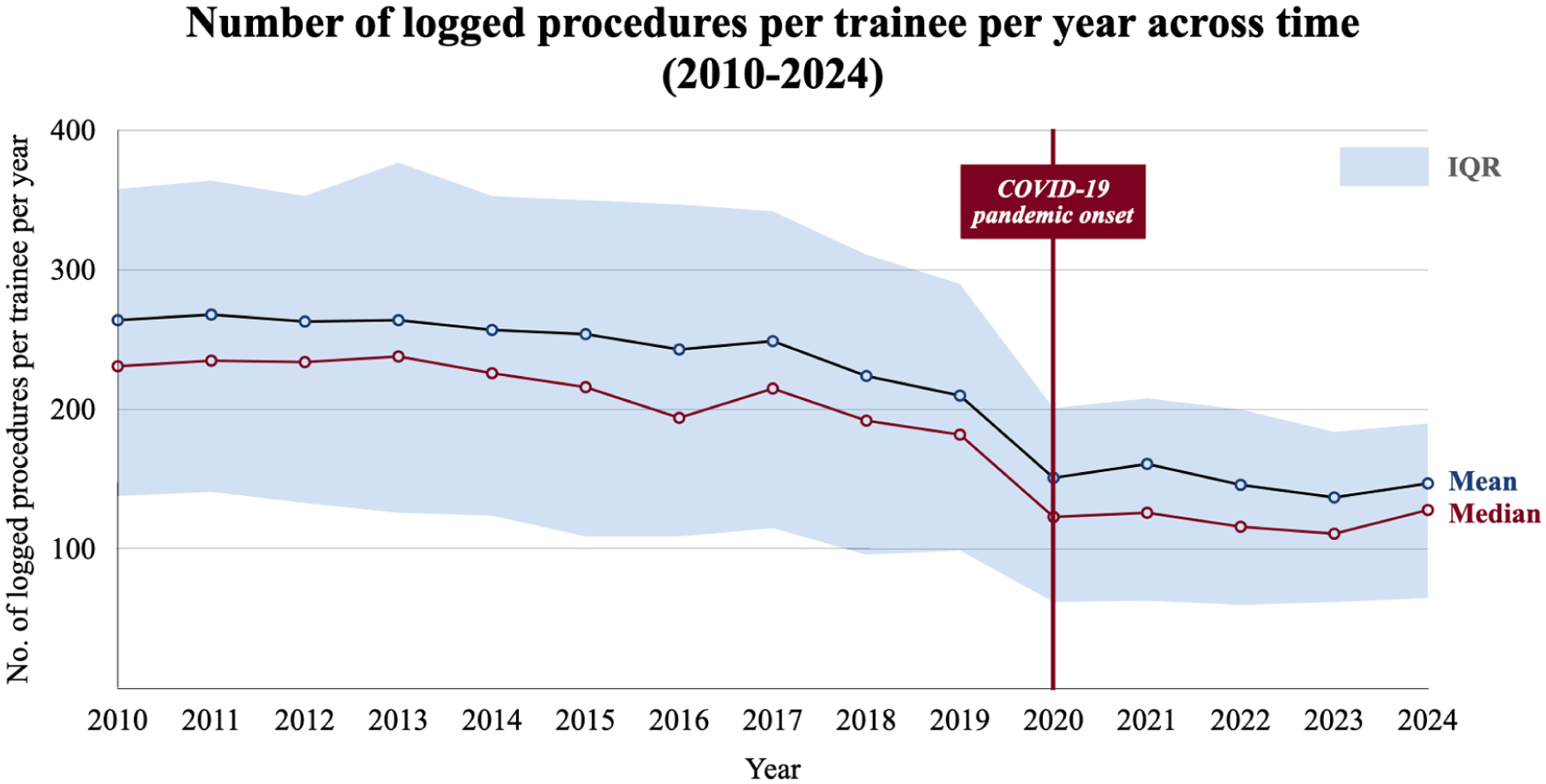
Results: A total of 1,140 trainees were included. There was no significant difference in operative volume by gender or age. A global difference in operative volume across ethnic groups was observed, however no adjusted pairwise differences remained significant. Operative volume declined over 15 years (Figure 1), with trainees performing 10.8 fewer operations each year than the year before (β₁=-10.8 procedures/trainee/year, t=-9.31, p<0.001), with the lowest recorded volume in 2020. Increasing seniority was associated with fewer procedures logged (Rs=-0.284; p<0.001). However, senior trainees logged more fascial sling, percutaneous nephrolithotomy, nephrectomy, radical prostatectomy, radical cystectomy, ileal conduit formation, and penile straightening procedures. Trainees in DGHs logged more procedures overall (U=2x10-47, p<0.001), while trainees in TCs logged more special interest procedures (U=1.6-24, p<0.001).
Conclusion: Operative experience among HSTs in the UK has declined over the past 15 years, with significant variation by training grade and hospital type. Targeted rotation planning and training strategies are required to ensure adequate operative exposure to produce safe and competent consultants who can provide the best possible patient care.
P2-2 Improving MRI Staging Accuracy in Muscle Invasive Bladder Cancer Through VI-RADS Implementation
Dr Mansha Bhiryani1, Dr Lara Jehanli1, Mr Mazen Allam1, Mr Tom Thompson1, Mr Ben Starmer1, Mr Vishwanath Hanchanale1, Dr Sarah Keegan1
1Liverpool University Hospitals NHS Foundation Trust, Liverpool, United Kingdom
Introduction: VI-RADS is a structured scoring and reporting system designed to improve the accuracy of multiparametric MRI (mpMRI) staging in suspected bladder cancer. We aimed to assess local diagnostic performance of MRI in muscle invasive bladder cancer (MIBC) and evaluate the impact of implementing VI-RADS.
Methods: A three-cycle retrospective audit was conducted at a single centre with approval following local guidance, including consecutive patients undergoing MRI for suspected MIBC. MRI T-stage was compared with histopathology from TURBT or cystectomy to determine staging concordance and specificity for differentiating MIBC from NMIBC. 27 patients were included in cycle 1, while 24 patients were included in cycles 2 and 3 respectively. Following Cycle 1, VI-RADS protocol adoption and reporter training were introduced, and multiplanar reformatted DCE became routine during Cycle 2. Secondary measures included patterns of over- and under-staging, timing of MRI, and appropriateness of MRI requests.
Results: MRI–histology concordance improved from 70.4% (Cycle 1) to 87.5% (Cycle 3). Specificity increased from 0.36 to 0.86, with NMIBC overstaging falling from 25.9% to 8.3% and minimal understaging (⩽4.2%). Several cases showed concordance between MRI and cystectomy staging despite discordance with TURBT, suggesting possible under-staging by TURBT. Additionally, in cycle 3, 95% (23/24) of MRI requests were appropriate, and mean time to MRI was 9 days.
Conclusion: Implementation of VI-RADS protocols and optimised imaging reformats improved MRI staging accuracy and reduced overstaging. These findings support progression toward an MRI-first staging pathway, including evaluation of pre-TURBT MRI and its impact on time to definitive treatment.
P2-3 Simultaneous referral triage with communicated pre-appointment diagnostic requests improves decision making in clinic and highlights non-attendances
Mr Abdullah Al-Mitwalli1, Ms C Joo1, Ms H Light1, Mr M Willcox1, Ms P Sangster1, Mr W.G Lee1, Prof David Ralph1
1UCLH, London, United Kingdom
Introduction: There is a delay in triage of referrals from primary care to urology services, compounded by clinic waiting times for outpatient appointments (OPD, which can lead to patient frustration and long waiting lists. During triage, clinicians can order investigations and send a letter acknowledging referral receipt and requested tests. The effect of this enhanced triage on decision-making is not known.
Methods: A quality improvement project was registered and consecutive andrology patients awaiting first OPD were screened for enhance triaging (ET) presenting with selected conditions (erectile dysfunction, infertility as well as scrotal benign issues) and necessary investigation were requested i.e. hormonal profile, semen analysis and testicular ultrasound were order appropriately. A letter was sent to inform the patient of the requested investigation. Data collected on consecutive patient group without this enhanced triage as a control group.
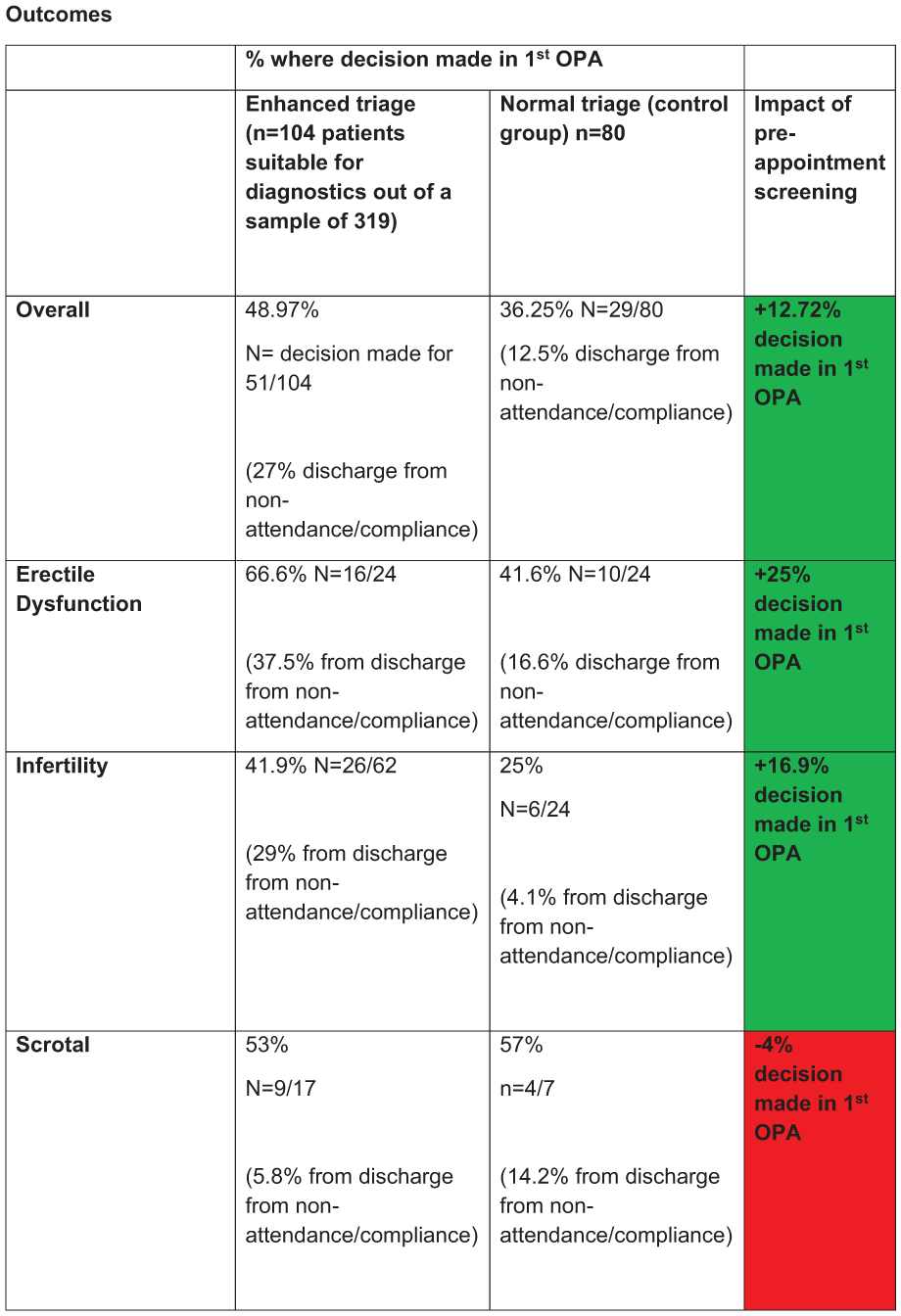
Results: 319 patients were screened, and 104 (33% ) were eligible for ET. In the ET group, there was higher percentage of patients having a definitive decision at first encounter compared with control group 49% vs 36%. Additionally, this allowed patients to be discharged for not attending their investigations therefore DNA rate was reduced in the ET group compared to control.
Conclusion: There is opportunity to shorten patient pathways by completing enhanced triaging with pre-appointment diagnostic screening. This not only allows for quicker decision making with less clinic visits but also flags the patients who do not attend prior to their clinic appointment.
P2-4 Transforming Out-patient ureteric Stent exchanges: From pilot initiative to standard outpatient care – Enhancing value through innovation, patient satisfaction and cost
Ms MF Frascheri, N.C. Grossman, S Fernandes, T Davis, L Tear, B.K Somani, Ms Amelia Pietropaolo1
1University Hospital Southampton Nhs Foundation Trust, Southampton, United Kingdom
Introduction & objectives: Routine stent exchanges are typically performed every 3-12 months. Delays in replacement can result in serious complications.
We implemented a protocol for outpatient ureteric stent exchanges under local anaesthesia (LA).
Materials & methods: LA ureteric stent exchanges were introduced following informed patient consent (audit reference: QI/0093). Procedures were conducted in the outpatient lithotripsy suite using a single-use flexible cystoscope, with lidocaine gel administered for local anaesthesia and fluoroscopic guidance. Visual Analogue Scale (VAS), ranged from 0 (no pain) to 10 (worst pain).
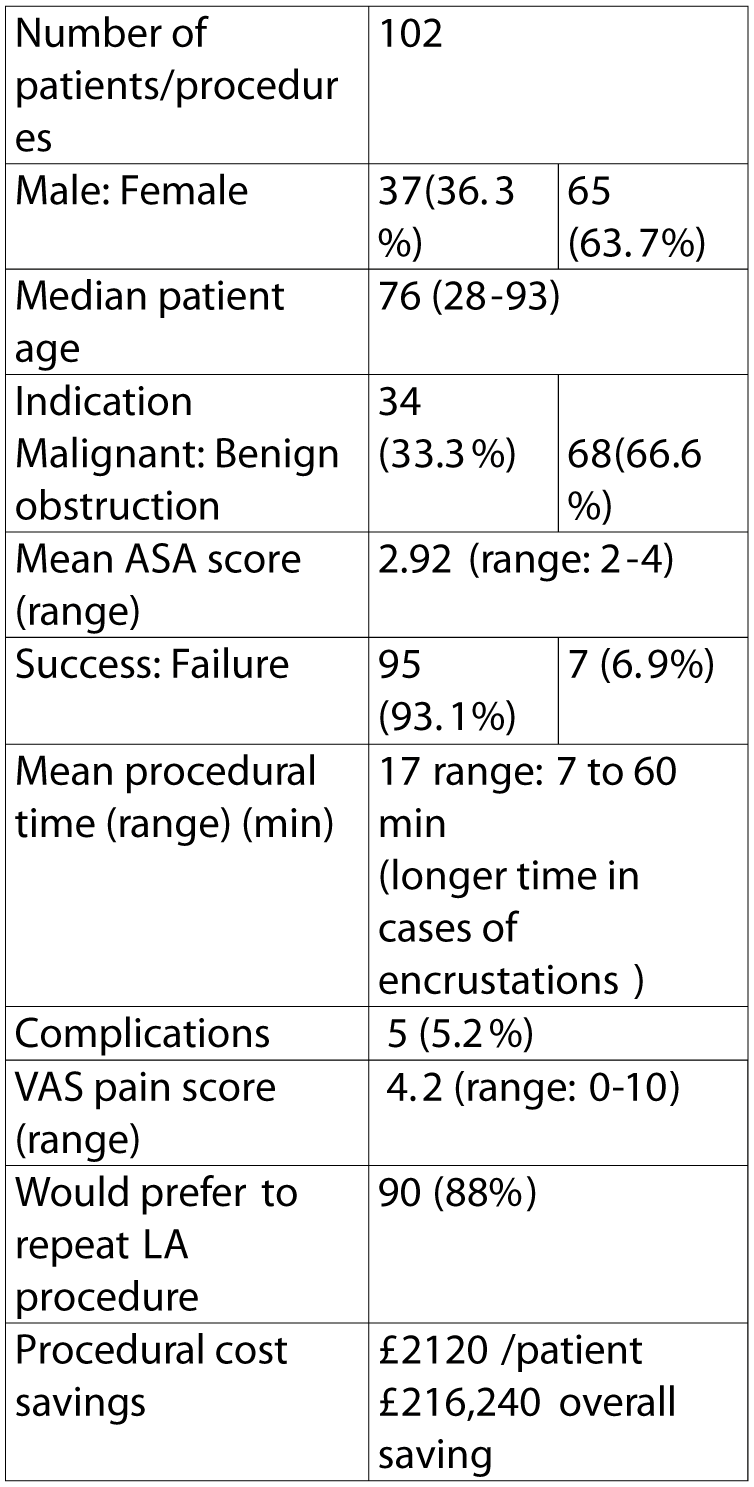
Results: Over a 31-month period (March 2023 – September 2025), a total of 102 ureteric stent exchange procedures were performed under LA. The median patient age was 76 years (IQR: 28–93), with a mean ASA score of 2.92 (range: 2–4). Of the 102 procedures, 95 (93.1%) were successfully completed under LA. Reasons for failure included pain intolerance (n=2), urethral stricture (n=1), a tight PUJ (=2) and stent encrustation (n=2). The mean VAS pain score was 4.2. 88% of patients (n=90) expressed willingness to undergo the procedure again under LA. Only one case of post-procedural UTI was reported (CD II), with no other complications.
The cost saving per procedure was estimated at £2120, yielding a projected total saving of £216,240 across all cases, attributed to reduced use of operating room (OR), anaesthetic input, and perioperative staffing.
Conclusion: Outpatient ureteric stent exchanges under LA represents a safe, effective, and well-tolerated alternative to traditional operating room procedures with significant cost savings while freeing theatre capacity for higher-priority cases.
P2-5 Global outreach for training outside the UK: A 25 year retrospective analysis of Urolink’s activity and the opportunities for UK urological trainees
Mr Abhishek Chandna1, Mr Stephen Payne2
1University Hospitals of Coventry and Warwickshire, Coventry, United Kingdom, 2Manchester University NHS foundation Trust, Manchester, United Kingdom
Introduction: Urolink represents BAUS in low and low-middle income countries, improving education at all levels by a mentoring model for local hosts. This study aims to evaluate the geographical reach, scope of Urolink’s international visits and the demographic evolution of participation over a 26-year period to demonstrate training opportunity for UK urologists in global surgery
Methods: A retrospective analysis of Urolink activity between 1999 and 2025 was conducted utilising visit reports logged on the BAUS/Urolink website. Data were extracted regarding the number of countries and centres visited, total visits, their content and the occupational demographics of participants.
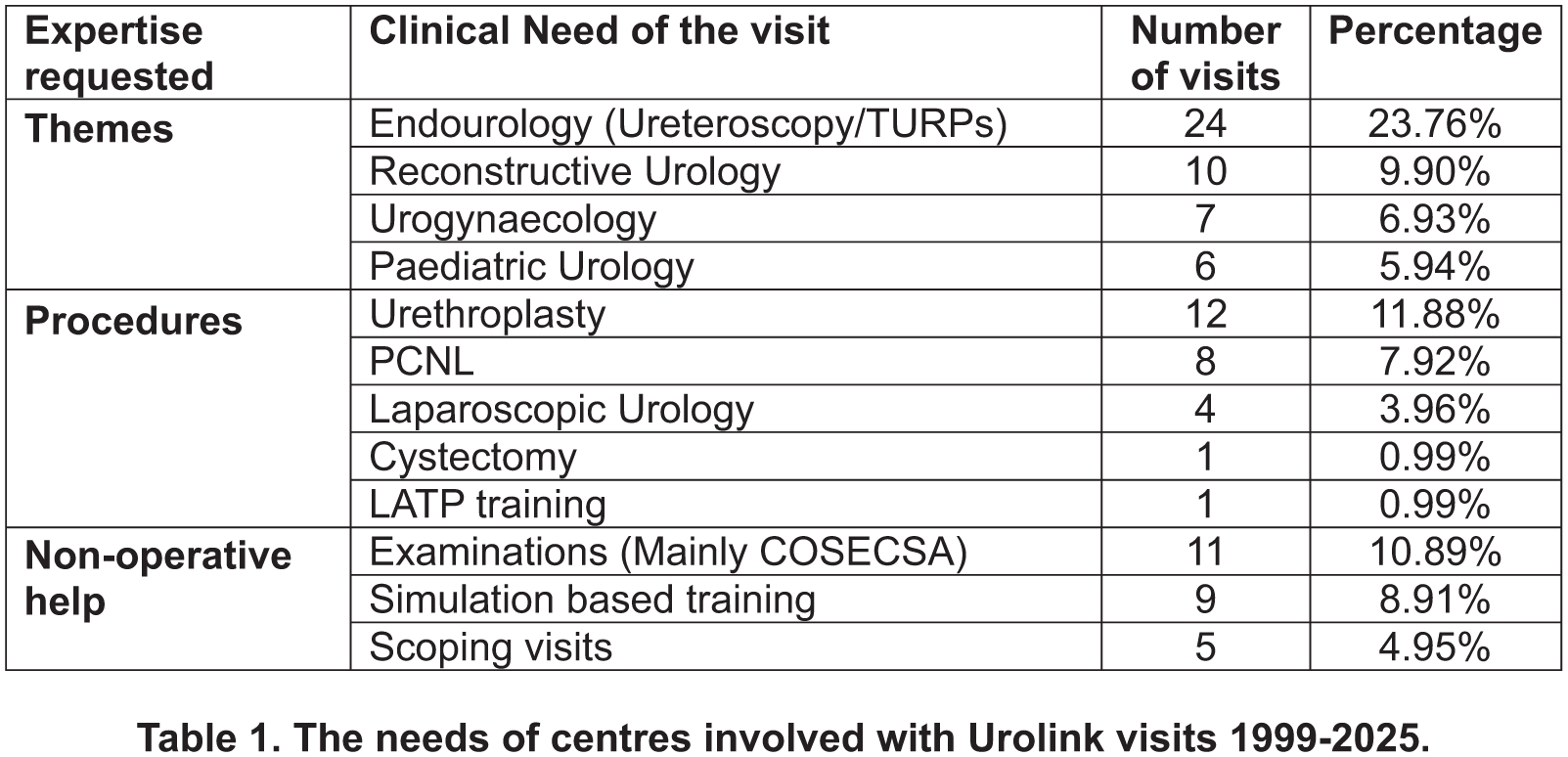
Results: 98 visits took place to 37 centres in 22 countries. Complete data was available for 92 visits attended by 46 urological consultants and 45 trainees. There has been an increase in visits, and involvement during the index period, with median engagement by 6 consultants and 2 trainees/year. Twenty-three consultants and 3 trainees were involved in more than 2 visits, with 9 (31%) of participants remaining engaged for >8 years. Six trainees retained engagement into consultant careers.
Thematically, the content of visits is shown in Table 1. Basic, and advanced endourological procedures were the commonest experience requested by host institutions, followed by reconstructive surgery, paediatric urology and urogynaecology. Quality assurance at examinations and simulation-based training, accounted for 27.7% of all activity.
Conclusion: There has been a growing interest in participating in Urolink’s global urology mandate, with significant scope for highly-supervised trainee involvement in diverse areas of urological sub-speciality experience, in unique healthcare environments.
P2-6 One-stop local anaesthetic circumcision clinic: An evaluation of utility, efficiency and safety of the service
Mr Sagara Ruwan Kumara Maduwe Gedara1, Miss Sandevni Amaya Jayamanne1, Miss Elizabeth Bright1, Mr Mathialagan Murugesan1, Mr Nicholas Munro1
1Royal Cornwall Hospitals NHS Trust, Truro, United Kingdom
Introduction: One-stop surgical pathways aim to improve efficiency, patient experience, and resource utilization within the NHS. This study sought to evaluate the safety, clinical outcomes, operational efficiency, and patient satisfaction associated with a one-stop local anaesthetic (LA) circumcision service delivered in a community-based NHS-commissioned surgical centre.
Patients and methods: Retrospective case note review of all patients attending the adult one-stop circumcision clinic between January 2024 -August 2025, to assess number of patients proceeding with same day circumcision, 30-day complication rate, efficiency of the service and patient satisfaction.
Results: 274 patients attended the clinic of which 219 (79.9%) proceeded to same day LA circumcision. Median wait time from referral to procedure was 113 days and median on day hospital stay was 105 minutes. Complications within 30 days occurred in 10 patients (3.6%), predominantly minor, with no procedure-related mortality. Telephone follow-up of patients demonstrated universal satisfaction and no reported concerns. By avoiding an additional hospital visit inherent in the standard pathway, the one-stop model saved an estimated 60 minutes and 48 km (30 miles) of travel per patient, equating to over 13,000 km of avoided travel across the cohort and estimated reduction of 1.9-3.3 tonnes of CO2 emission.
Conclusion: The one-stop LA circumcision model is safe, efficient, associated with high patient satisfaction, and low complication rates. It significantly reduces waiting times, hospital stay duration, and patient travel burden, while aligning with NHS sustainability goals.
P2-7 Health-economic burden of ureteroscopy-related complications: A national HES-based analysis of 90,807 NHS patients
Professor Bhaskar Somani, Mr Mohammed Boulmani, Mr Alfredo Dell’Isola, Miss Alice Craven
1University Hospital Southampton NHS Foundation Trust, Southampton, United Kingdom
Introduction: Ureteroscopy-related complications result in unplanned admissions and additional NHS cost. Our study aims to quantify Healthcare Resource Group (HRG)-defined economic burden of post-ureteroscopy complications and identify high-risk groups using Hospital Episode Statistics (HES).
Materials & Methods: This retrospective study used HES data to identify patients undergoing ureteroscopy for urolithiasis in NHS England (2018-2023). Patients were stratified into predefined cohorts based on demographics, comorbidities, infection history, and procedural factors. HRG costs were analysed for the index ureteroscopy admission and subsequent complication-related hospital spells within 30 days. Twelve post-operative complications were assessed, including urinary tract infection (UTI), sepsis, deep vein thrombosis (DVT) and myocardial infarction (MI). HES captures confirmed hospital diagnoses, and data use was approved under NHS Digital agreement DARS-NIC-05934-M7V9K.
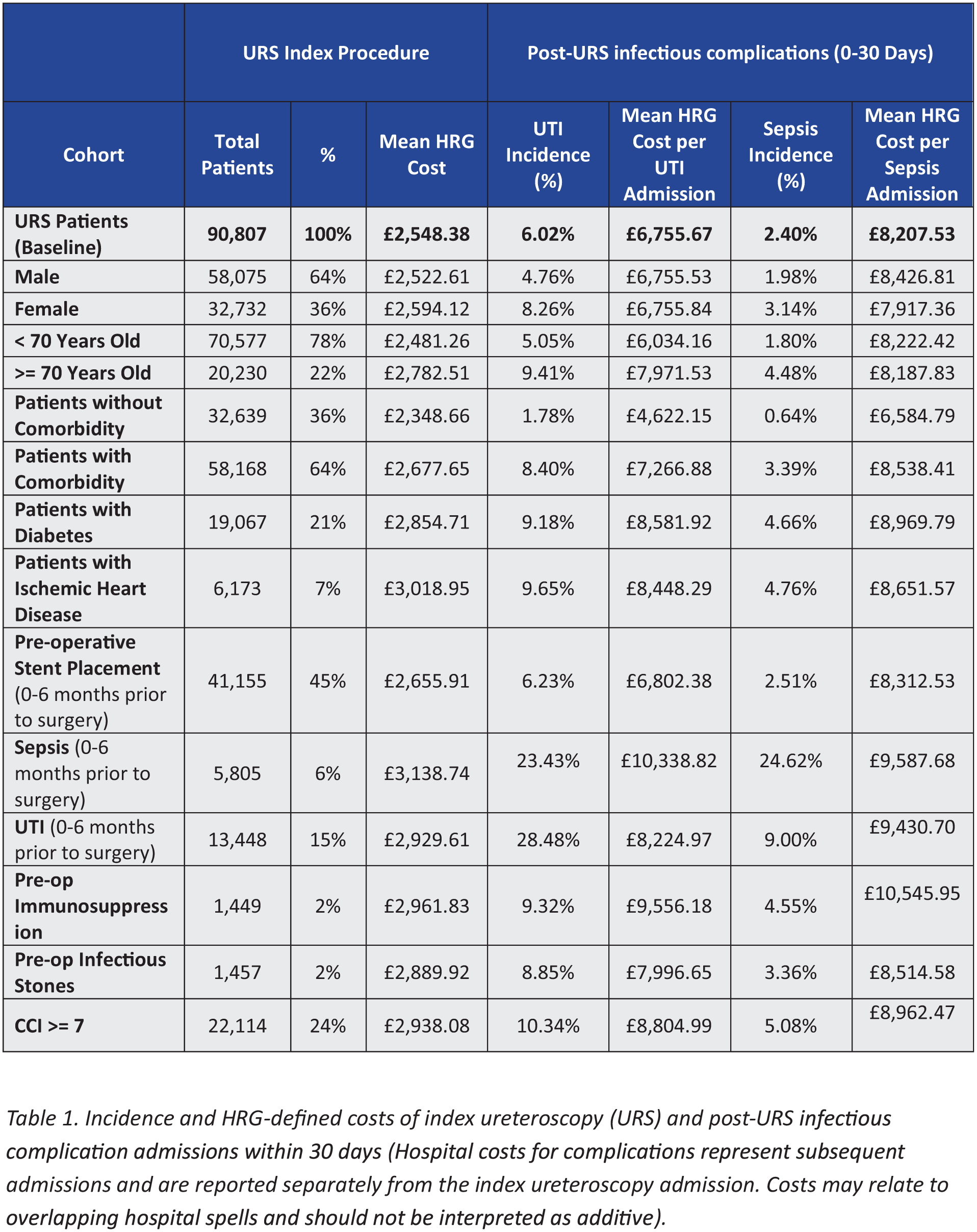
Results: A total of 90,807 patients were included. Within 30 days of ureteroscopy, UTI, sepsis, DVT and MI occurred in 6.02%, 2.40%, 0.22% and 0.08% of patients, respectively, with mean HRG costs of £6,756, £8,208, £5,230 and £6,088 per admission, additional to the index ureteroscopy cost.
Among high-risk groups, pre-operative UTI was associated with a 28.5% post-operative UTI rate while pre-operative sepsis was associated with UTI and sepsis rates of 23.4% and 24.6%, respectively. Across the study period, UTI- and sepsis-related admissions were associated with additional HRG-defined hospital expenditure of £36.9 million and £17.9 million, respectively, noting potential overlap between admissions.
Conclusions: Post-ureteroscopy infectious complications are associated with increased NHS expenditure, particularly among high-risk patients. Targeted risk stratification and infection-prevention strategies may reduce morbidity and economic burden to the NHS.
P2-8 HoLEP Trifecta Achievement in Octogenarians: Single Centre Analysis of Surgical outcomes
Mr Nadeem Iqbal1, Dr Ben Charles Davison2, Mr Simon Holden2
1Newham University University Hospital, London, United Kingdom, 2Whipps Cross Hospital, LONDON, United Kingdom
Introduction: Holmium laser enucleation of the prostate (HoLEP) is increasingly utilised in elderly patients with significant comorbidity and large prostate volumes; however, objective surgical quality benchmarks in octogenarians remain poorly defined. We evaluated the feasibility and clinical relevance of a HoLEP trifecta as a composite surgical quality metric in patients aged ⩾80 years.
Methods: We retrospectively analyzed patients aged ⩾80 years who underwent HoLEP at a high-volume tertiary referral center between 2015 and 2025. Trifecta was defined as the contemporaneous achievement of: (1) no postoperative complications within 3 months; (2) absence of urinary incontinence at 3-month follow-up; and (3) Three-month postoperative maximum urinary flow rate (Qmax) >15 mL/s. Peri-operative characteristics and early functional outcomes were evaluated.
Results: Among all HoLEP procedures performed during the study period, 56 patients were aged ⩾80 years (mean age 82.3 years). Mean prostate volume was 135.7 cc, mean operative time was 197.6 minutes, and mean ASA score was 2.4. Mean length of hospital stay was 1.15 days. Mean IPSS improved significantly from 19.4 preoperatively to 6.3 at 3 months postoperatively (P value<0.001). Postoperative urinary incontinence was observed in 5 patients (8.9%). Minor complications occurred in 11 patients (19.6%), with no major complications. HoLEP was completed successfully in all cases. The HoLEP trifecta was achieved in 39 of 56 octogenarians (69.6%).
Conclusions: HoLEP provides substantial symptom relief with acceptable complications in octogenarians with very large prostates. The HoLEP trifecta offers a standardized approach to assessing surgical quality in elderly patients.
P2-9 Exploring procedure cancellations due to UTI on the day of surgery alongside GIRFT guidelines
Miss Amelia Simenacz1, Mr Muhammad Sanan1, Miss Amy Nagle1
1Royal Free Hospital, London, United Kingdom
Introduction: Same day surgical cancellations due to urinary tract infections (UTIs) lead to significant loss of operating theatre time, prolonged patient waiting lists and reduced patient satisfaction. This audit evaluated the timing and outcome of pre-operative urinalysis in line with Getting It Right First Time (GIRFT) guidelines (April 2025). The primary aim was to determine the number of UTIs identified on the day of elective surgery and highlight systemic errors contributing to same day cancellations.
Methods: Retrospective data were collected for 38 patients scheduled for elective urological procedures, using data sheets provided by the administrative team. Parameters collected included timing of pre-operative urinalysis, availability of results prior to surgery, antibiotic prescribing, urinalysis results on the day of surgery and documentation of urinary symptoms.
Results: 94.7% patients had urine microscopy, culture and sensitivity (MCS) performed pre-operatively. Of these, 55.3% were conducted over 14 days prior to scheduled surgery. 63% of patients had a positive MCS, 50% (19/38) received antibiotics prior to surgery. 92.1% patients had positive urine dipstick on day of surgery, with 94.7% recorded as asymptomatic. Positive nitrate dipstick results frequently resulted in cancellations, contributing to same-day cancellation rate of 21%.
Conclusion: A significant portion of cancellations may be preventable. Contributing factors to same day cancellations included suboptimal timing of pre-operative urine testing, inappropriate action following abnormal results and unclear documentation. Targeted interventions to improve testing, ensuring appropriate antibiotic treatment, clear management plans and education on differentiating asymptomatic bacteruria from true UTI, could help reduce cancellations in elective urological surgery.
P2-10 We need to stop doing pre-operative group and save for a trans-urethral resection of the prostate; an audit of current practice
Miss Iona Fernandes1, Mr Faraz Sharif, Dr Georgina Mussell, Dr George Monaghan, Miss Charlotte Hogg, Mr Chandra Shekhar Biyani
1St James’s University Hospital, Leeds, United Kingdom
Background: Pre-operative group and save (G+S) are currently taken as standard practice for patients undergoing trans-urethral resections of prostates (TURPs), a common endo-urological procedure. This generates a significant use of resources, with a single group and save sample costing up to £12, excluding labour costs. Whilst the use of pre-op G+S have become an obsolete practice in some common laparoscopic procedures such as appendicectomies, we continue to use them for TURPs. The aim of this audit was to determine the need for pre-operative G+S.
Methods and Materials: We retrospectively collected data from online records of patients who underwent a TURP over a 9-month period in 2024.
Results: 148 patients underwent TURPs between the beginning of January and September in 2024 between the ages of 50-95, (mean age 72.0). Of these patients, 127 (85.8%) had 2 G&Ss, 17 (11.4%) had 1 G&S and 4 (2.7%) had none. Out of these patients, 12(8.1%) required an intervention for haematuria including irrigation and bladder washouts or a return to theatre. Only 1 (0.6%) required a blood transfusion post-operatively.
Conclusion: In the vast majority of cases, there is not sufficient reason for mandatory pre-operative G+S; indeed, it may waste time, resources and finances. The cost of the bottles alone cost up to £3552 for our cohort. A tailored approach, such as identifying co-morbidities, pre-operative haemoglobin levels and the concomitant use of anticoagulation would be more prudent to assess patients who may be at high risk of bleeding and should therefore have a pre-op G+S.
ePoster Session 3: Bladder Cancer: Muscle Invasive/Non-Muscle Invasive, Catherine Lewis, June 16, 2026, 08:00 - 09:00
P3-1 Organisational and clinical practice factors associated with early recurrence after TURBT surgery: an analysis of the RESECT study
Ms Aqua Asif1,2, Dr Steven MacLennan3, Ms Nikita R Bhatt2,4, Mr Keiran D Clement2,5, Ms Eleanor F Zimmermann2,6, Mr Sinan Khadhouri2,7, Prof Paramananthan Mariappan2,8,9, Prof Veeru Kasivisvanathan1,2, Mr Kevin M Gallagher2,8,9, on behalf of the BURST-RESECT Global Study Group1,2
1University College London, London, United Kingdom, 2British Urology Researchers in Surgical Training (BURST), London, United Kingdom, 3University of Aberdeen, Aberdeen, United Kingdom, 4St Vincent’s University Hospital, Dublin, Ireland, 5NHS Tayside, Dundee, United Kingdom, 6North Bristol NHS Trust, Bristol, United Kingdom, 7St Andrews University, St Andrews, United Kingdom, 8University of Edinburgh, Edinburgh, United Kingdom, 9Western General Hospital Edinburgh, Edinburgh, United Kingdom
Introduction: We aimed to determine factors associated with early recurrence after transurethral resection of bladder tumour (TURBT).
Methods: This was an international, observational, case-control study. The outcome was recurrence at the first cystoscopy after primary TURBT. Twenty-three factors were selected. “Difficult tumour” was defined as >5 cm; or >3 cm on dome, posterior, anterior wall; or ⩾5 tumours. A dedicated list was a session where most cases were NMIBC. A mixed-effects logistic regression (with random intercepts for centre and surgeon) was fitted, adjusting for age, sex, smoking, stage, grade, continent; with interaction terms: “difficult tumour by experienced surgeon” and “difficult tumour on dedicated list”.
Results: 9800 cases from 232 centres involving 2731 surgeons were included. Early recurrence rate was 2073/9800 (21%). Lower recurrence was associated with in-study cases vs. baseline cases (OR 0.79, 0.71-0.89, p<0.001) and single-instillation intravesical chemotherapy (OR 0.64, 0.54-0.76, p<0.001). Higher recurrence was associated with difficult tumour (OR 1.88, 1.52-2.31, p<0.001) and academic versus non-academic hospitals (OR 1.23, 1.00-1.52, p=0.046). Training cases, surgeon grade/experience, dedicated lists, detrusor sampling, had no significant association with recurrence. “Difficult tumour by experienced surgeon” trended to lower recurrence (OR 0.80, 0.63-1.00, p=0.06), while “difficult tumour on dedicated list” did not (OR 0.94, 0.71-1.23, p=0.64).
Conclusions: Observation within audit can reduce early recurrence. We propose a new “difficult tumour” characterisation associated with higher recurrence. We recommend national audits of practice for TURBTs, and pre-operative risk stratification may aid operative planning.
P3-2 Real-world evaluation the Galeas Urinary Biomarker for Surveillance in intermediate and high-risk NMIBC; experience from a UK TULA clinic with histopathological correlation
Mrs Nidhi Kapadia1, Ms Helma Kolarickal1, Mr Sachin Agrawal1
1Ashford And St Peter’s Hospitals, Chertsey, United Kingdom
Objectives: To evaluate the role of the GALEAS urinary biomarker for surveillance in non–muscle-invasive bladder cancer (NMIBC) with histopathological correlation within a TULA clinic.
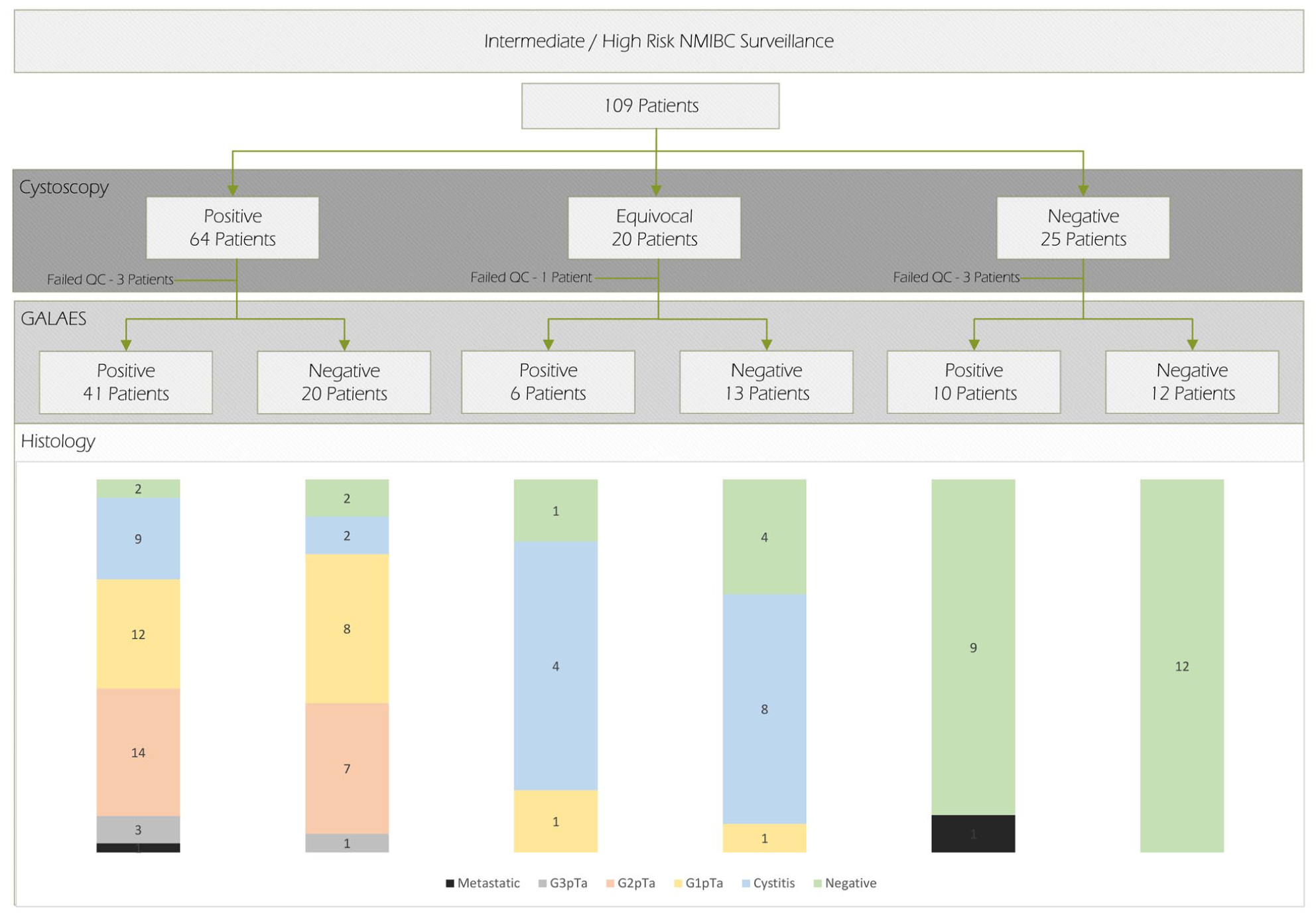
Patients and Methods: Patients undergoing NMIBC surveillance in a TULA clinic were prospectively evaluated between February-November 2025. Eligible patients had a confirmed diagnosis of intermediate/high-risk NMIBC. Cohorts included endoscopic surveillance alone or in combination with intravesical therapy. GALEAS urine samples were collected on the day of surveillance cystoscopy, prior to the procedure. Concordance between biomarker, cystoscopic and histopathological findings were evaluated.
Results: 109 patients (mean age 78.6 years; male-to-female ratio 2.75:1) were reviewed, 7 samples failed to meet Quality control and were excluded. Comparative assessment of cystoscopy, histology, and biomarker results identified 47 confirmed recurrences. GALEAS detected 32 of these, yielding a positive predictive value of 78.9%, sensitivity of 75%, and specificity of 71.4%. GALEAS-detected recurrences included 40.6% low-grade, 43.7% intermediate-grade, 9.3% high-grade, and 6.2% metastatic disease. Positive GALEAS results in patients with metastatic disease, and no visible lesions are likely to indicate circulating molecular disease activity limiting its usefulness in surveillance.
Conclusion: The GALEAS urinary biomarker demonstrates high levels of diagnostic accuracy in the outpatient surveillance of NMIBC. Further work to optimise GALEAS collection, improve histopathological sampling/reporting errors and assess long-term following in false positive patients would help to develop risk-adapted surveillance pathways.
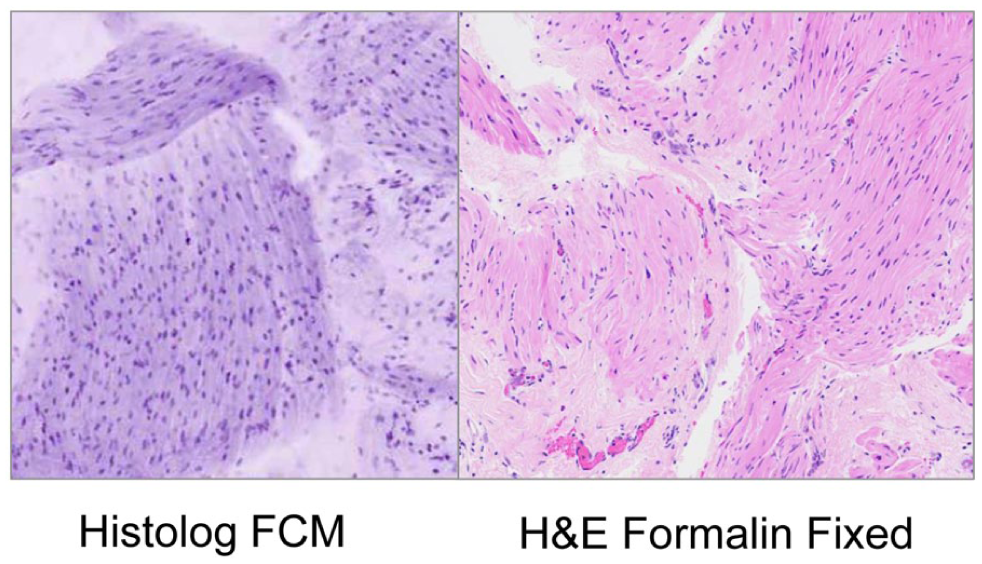
P3-3 Immediate detrusor muscle status at time of primary transurethral resection of bladder tumour: a prospective, paired, cohort feasibility study using fluorescence confocal microscopy (IB1-LaserComplete)
Mr Martin Connor1, Dr Archana Gopalakrishnan1, Prof Rakesh Heer2, Ms Eva Bolton2, Mr David Hrouda2, Dr Anna Silvanto3, Dr Andrew Smith2, Prof Mona El-Bahrawy1, Mr Mathias Winkler1, IB1-LaserComplete Trial Investigators1
1Imperial College London, London, United Kingdom, 2Imperial College Healthcare NHS Trust, London, United Kingdom, 3University College London Hospitals NHS Foundation Trust, London, United Kingdom
Introduction: Patients without detrusor muscle (DM) present at first TURBT risk poorer oncological outcomes and re-resection. 30-60% have no DM present. Ex vivo fluorescence confocal microscopy (FCM) produces high-resolution digital images of fresh tissue offering the opportunity for immediate detrusor status intra-operatively.
Patients and Methods: In this prospective, blinded, paired cohort feasibility study (IB1-LaserComplete; ISRCTN16114765) all patients undergoing primary TURBT for suspected NMIBC were enrolled between Sept/2025-Sept/2026. DM status on intraoperative FCM of tumour base, using the Histolog® scanner, was reported by a blinded uropathologist and a urologist. This was compared to formalin-fixed histopathology reference standard. The primary outcome was feasibility, defined as sufficient FCM image for DM interpretation. Secondary outcomes included diagnostic performance of FCM for DM status on a per-patient level, and inter-observer agreement of uropathologist and urologist reporting FCM using percentage agreement and Cohen’s kappa index.
Results: 30 patients were recruited; DM was absent in 13% (4/30) specimens. FCM was sufficient for interpretation of DM status in all patients (100%; 30/30). For DM status, the sensitivity, specificity, PPV, NPV were 42% (95% CI 26-61), 100% (95% CI 51-100), 100% (95% CI 74-100), and 21% (95% CI 9-43). Inter-observer agreement of FCM DM status between uropathologist and urologist was high (83%) (κ=0.72; [95%CI 0.47–0.97]). Median time for FCM DM status was 5.39 minutes (IQR 4.95-5.39).
Conclusion: FCM has a high specificity for intraoperative detection of DM during primary TURBT. This technology is rapid, can be accurately reported by bedside urologists and may guide surgical decision-making for immediate re-resection.
P3-4 Impact of prior pelvic radiotherapy on Perioperative Safety and Functional Outcomes of Robot-assisted Cystectomy and Intracorporeal Ileal Conduit Diversion: A Propensity-score Matched Analysis
Mr Youssef Ibrahim1, Miss Yasmin Abughanem, Miss Elsie Mensah, Dr Mohammed Gad, Prof Shamim Khan, Mr Ramesh Thurairaja
1Guys Hospital, London, United Kingdom
Objective: To evaluate peri-operative safety, short- and long-term functional outcomes of robot-assisted cystectomy with intracorporeal ileal conduit diversion (RAC+ICIC) in patients previously exposed to pelvic radiotherapy exposed (RE) patients, compared to radiotherapy-naïve (RN) controls.
Patients and Methods: All RE patients undergoing RAC+ICIC between 2014 and 2024 were identified from a prospectively maintained database. RN controls were selected from the same cohort and matched 1:2 by propensity scores including age, sex, BMI, Charlson Comorbidity Index, and previous abdominal surgery. Operative metrics, early (<90days) and late (⩾90days) complications (Clavien–Dindo) were compared. Multivariable regression modeling identified predictors of complications.
Results: From 770 cystectomies, 45 RE patients were matched to 90 RN controls. Median operative time was 360 vs 330minutes (p=0.2603), with comparable intra-operative complication rates. Median length of stay (9vs 8days, p=0.4820) and 30-day readmission (17.8%vs 12.7%, p=0.3820) were not significantly different. Early complications occurred more frequently in RE (48.9% vs 25.6%; p=0.0067). Over median follow-up of 24.5months (IQR 12.4–62.8), late complications were higher in RE (31.1% vs 14.4%; p=0.0225). Within RE cohort, benign cystectomy for radiation toxicity carried the highest late complication risk. At multivariable analysis, RE was the only independent predictor of higher rate of early (OR: 4.23; 95%CI 1.82-9.79) or late (OR: 2.83; 95%CI 1.09-7.32) postoperative complications.
Conclusions: Robot-assisted intracorporeal urinary diversion following prior pelvic irradiation is a safe and feasible, despite the technical complexity and elevated risk profile. Patient receiving cystectomy for radiation-induced toxicity are particularly at higher risk of late-complications.
P3-5 Cystoscopic RADA16 (PuraStat®) as an Adjunct and Salvage Therapy for Refractory Radiation
Cystitis: Expanded Prospective Outcomes
Mr Mohamed Gad1, Mr John O’Kelly, Mr Youssef Ibrahim, Miss Elsie Mensah, Prof Muhammad Shamim Khan, Miss Yasmin Abu Ghanem, Mr Ramesh Thurairaja
1Guys’ Hospital, LONDON, United Kingdom
Introduction and Objectives: Haematuria secondary to radiation cystitis is a challenging late complication of pelvic radiotherapy, frequently resulting in hospital admissions, transfusion dependence, and escalation to invasive salvage procedures. RADA16 (PuraStat®) is a self-assembling peptide haemostatic agent with proven efficacy in radiation proctitis; its role in radiation cystitis is evolving. We report expanded prospective outcomes of cystoscopic RADA16 application for refractory radiation-induced haematuria.
Methods: Patients with refractory haematuria due to radiation cystitis, unresponsive to standard endoscopic and intravesical treatments, were prospectively treated with cystoscopic RADA16 between February 2024 and November 2025. Outcomes included haematuria response, need for re-intervention, transfusion requirement, salvage surgery, and complications.
Results: Thirty-five patients underwent 42 RADA16 applications. Median age was 75 years (range 54–91), with a median interval of 6 years from pelvic radiotherapy (range 1.5–17). All patients had undergone prior intervention for haematuria.
At 6 weeks, 29/35 patients (83%) demonstrated significant haematuria reduction, including 71% with complete macroscopic resolution. Six patients (17%) had no sustained response. Three-month follow-up was available for 24 patients, of whom 19/24 (79%) maintained haematuria control. Re-intervention was required in 10/35 patients (29%), including six repeat RADA16 applications and four adjunctive endoscopic procedures. Complications included Grade I urinary retention (n=2) and Grade II transfusion (n=3), with no Clavien–Dindo ⩾III complications attributable to RADA16.
Conclusion: Cystoscopic RADA16 is a safe and effective adjunctive or salvage therapy for refractory radiation cystitis, offering a bladder-preserving option that may reduce bleeding burden and delay invasive surgery.
P3-6 Frailty predicts all-cause mortality in patients with bladder cancer and outperforms WHO performance status
Miss Charlotte Simms, Mr Angus Hall, Mr Mohantha Dooldeniya
1Pinderfields Hospital, Wakefield, United Kingdom
Introduction: Bladder cancer commonly affects older patients with comorbidities, making treatment decisions challenging. While WHO performance status guides management, it may not reflect physiological vulnerability. This study evaluated the association between frailty, WHO performance status, and mortality in bladder cancer patients.
Patients and Methods: This retrospective study included bladder cancer patients undergoing transurethral resection of bladder tumours (TURBT) at a tertiary centre. Frailty was assessed using the Clinical Frailty Scale (CFS): fit (CFS 1–3), moderately frail (CFS 4–5), or severely frail (CFS 6–7). All-cause mortality was analyzed using Kaplan–Meier methods and Cox regression. Early mortality (death within 4 months of diagnosis) was analysed using logistic regression.
Results: Of 169 patients, 38 (22.5%) died during follow-up. Early mortality occurred in 4/115 (3.5%) fit, 1/32 (3.1%) moderately frail, and 7/22 (31.8%) severely frail patients. One-year mortality increased with frailty: 7/115 (6.1%), 4/32 (12.5%), and 12/22 (54.5%) patients respectively. In multivariable analysis, severe frailty independently predicted increased mortality compared to fit patients (HR 7.16, 95% CI 2.52–20.38, p<0.001), while WHO performance status did not. Severe frailty strongly predicted early mortality after adjusting for age and WHO status (OR 24.40, p=0.007).
Conclusions: Frailty predicts mortality in bladder cancer patients better than WHO performance status. For severely frail patients, TURBT may not meaningfully alter prognosis beyond diagnosis or symptom control. Benefits should be weighed against procedural risks, supporting goal-directed decision-making and consideration of palliative approaches.
P3-7 The Impact of Socioeconomic Status in Influencing Stage at Presentation and Overall Survival in Bladder Cancer: A West of Scotland Experience
Mr Jamie Leask1, Mr Ibrahim Ibrahim1, Mr Blair Wilson1, Ms Jane Hendry1, Mr Abdullah Zreik1
1Queen Elizabeth University Hospital, Glasgow, United Kingdom
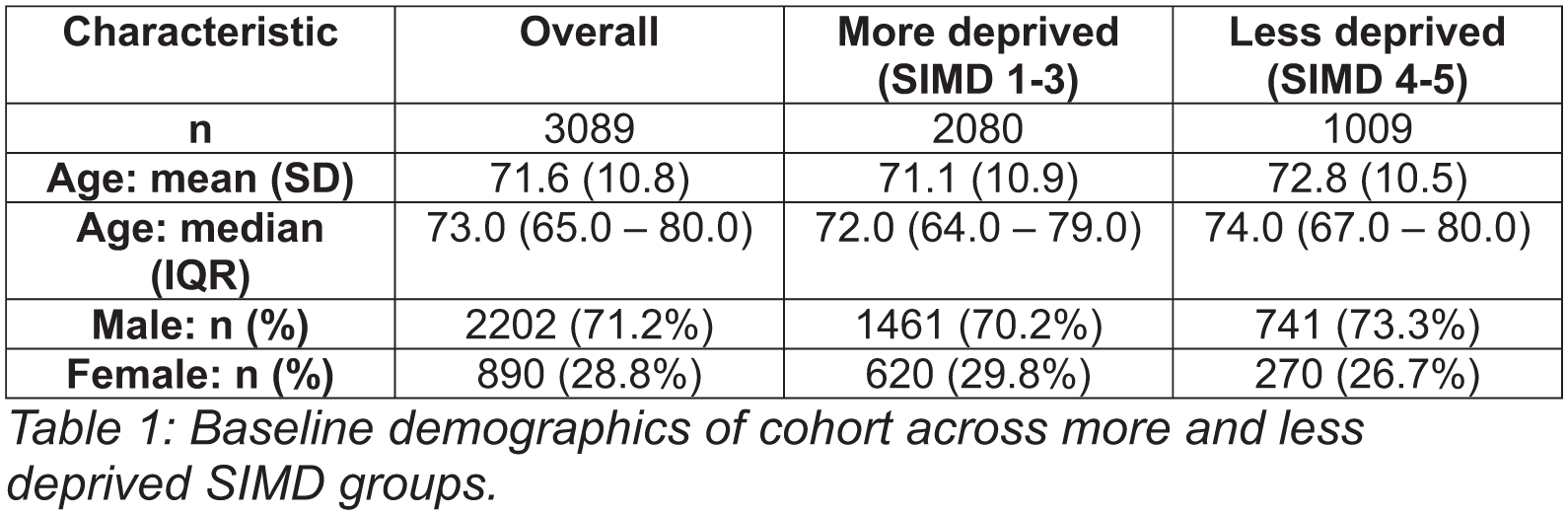
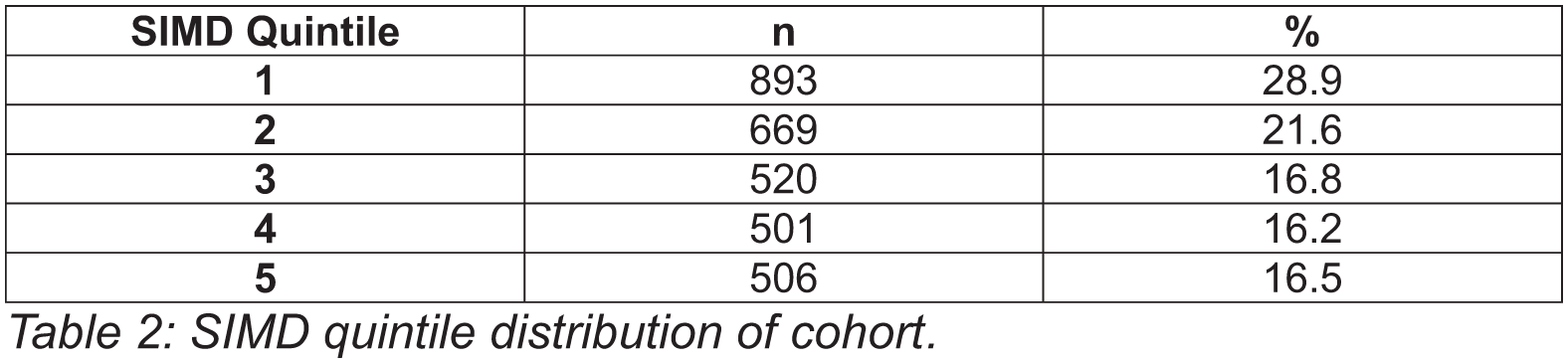
Introduction: Bladder cancer is responsible for significant decrements in health-related quality of life and economic burden. Despite this, large scale studies on the relationship between socioeconomic differentials and bladder cancer outcomes are lacking. We conducted a retrospective cohort analysis to determine whether deprivation had any impact on the stage at presentation or overall survival (OS) in bladder cancer patients.
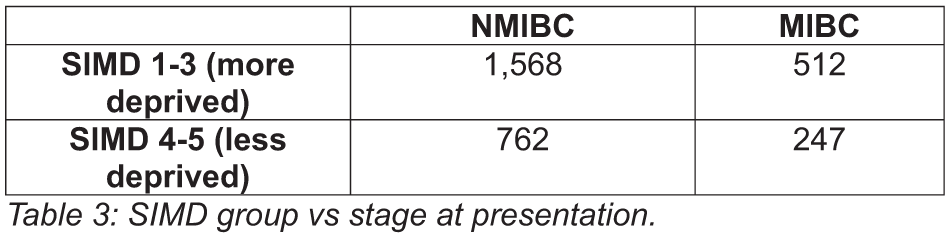
Materials and Methods: Information was collated on every patient diagnosed with bladder cancer in West of Scotland over a 5-year period (n=3,089). The Scottish Index of Multiple Deprivation quintiles were used as a surrogate for socioeconomic status. Multivariable logistic regression and Cox models were applied to evaluate the impact of social deprivation on both the stage at presentation and OS.
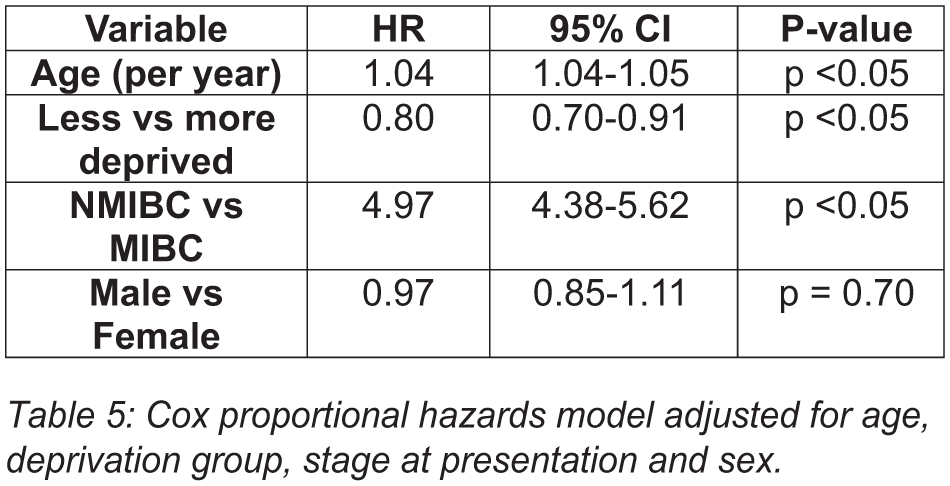
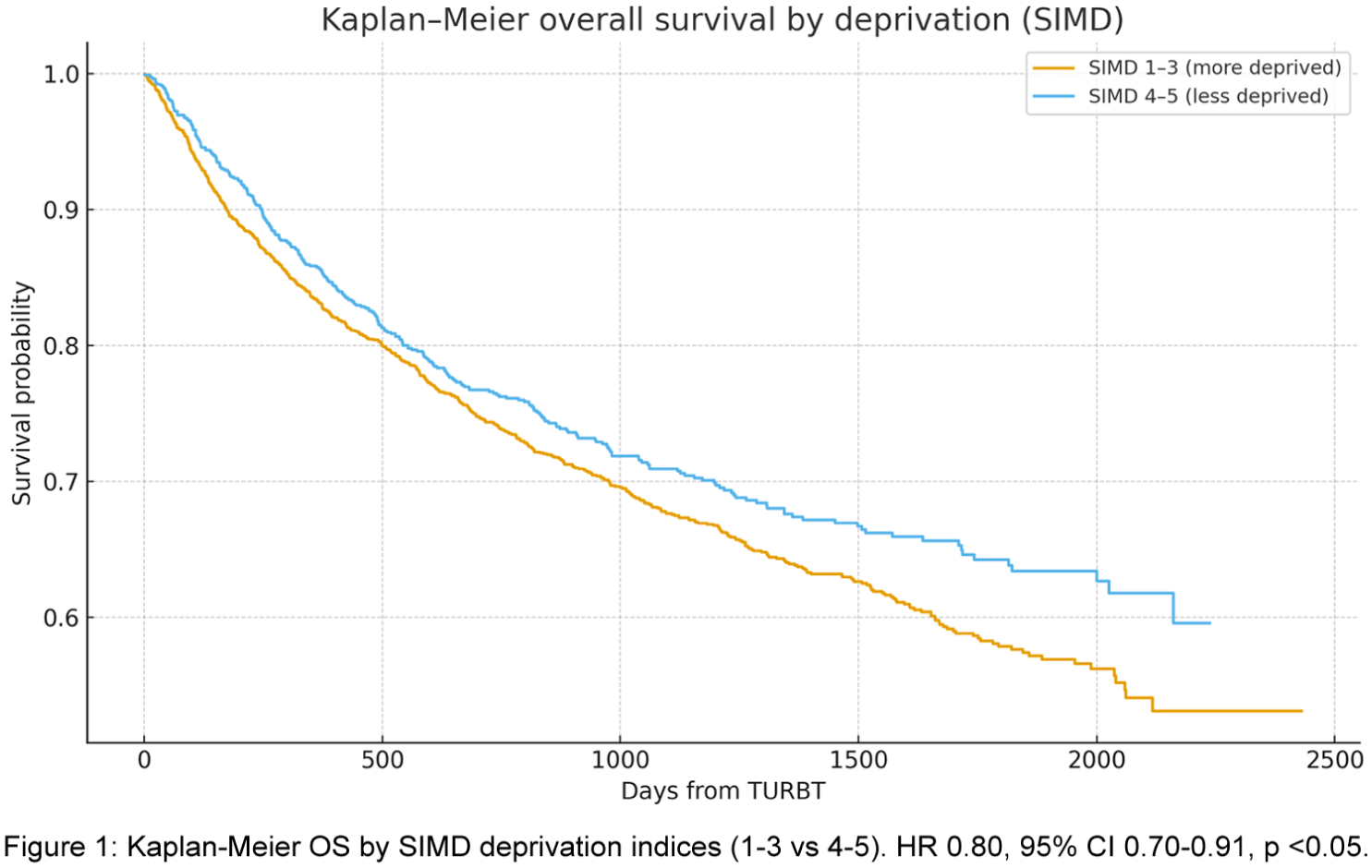
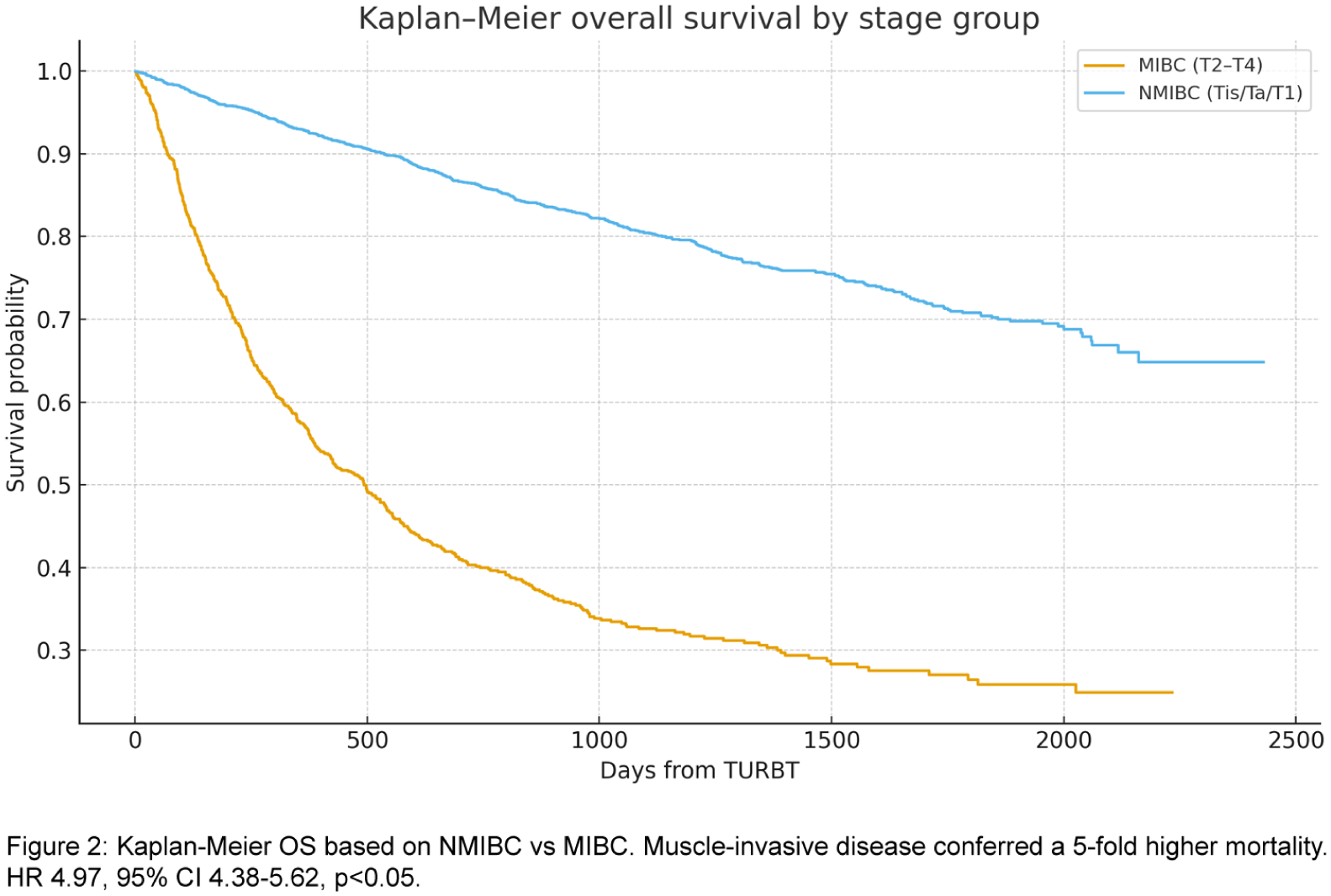
Results: In the multivariate Cox model, the less deprived had a lower hazard of death (HR 0.80, 95% CI 0.70-0.91, p <0.05), with significantly worse OS in the more deprived group (~25% higher hazard). More females presented with MIBC. The proportion presenting with MIBC was 24.6% in the more deprived group and 24.4% in the less deprived group (p=0.94). Thus, deprivation was not associated with increased odds of MIBC at diagnosis.
Conclusions: Lower socioeconomic status was seen to negatively affect OS in bladder cancer within this cohort. Females were found to present with more advanced disease. These findings complement previous studies. However, to the best of our knowledge this is the first study which demonstrates that socioeconomic status in patients with bladder cancer does not influence stage at presentation.

P3-8 Beyond the guidelines: A real-world assessment of NMIBC surveillance in NHS Scotland and potential cost-effectiveness of the Epicheck biomarker
Dr Jasmin Hart Brooke1,3, Dr Delphine Chabut2, Mr Simon Verdonck2, Professor Paramananthan Mariappan1,4
1Edinburgh Bladder Cancer Surgery (EBCS), The University of Edinburgh, Western General Hospital, Edinburgh, United Kingdom, 2Menarini Diagnostics GmbH, Basel, Switzerland, 3Edinburgh Medical School, The University of Edinburgh, Edinburgh, United Kingdom, 4The University of Edinburgh, Edinburgh, United Kingdom
Introduction: Despite guideline recommendations, adherence to NMIBC surveillance regimes is often challenging due to patient-related factors and NHS constraints. We quantify the deviation from guideline-recommended surveillance in the Scottish NHS, and evaluate the potential for a urinary biomarker to improve adherence and cost-effectiveness.
Material & Methods: Prospectively maintained data of 2,284 consecuitve NMIBC patients from Scotland’s QPI programme with 5-year follow up [DOI: 10.1016/j.euo.2024.01.012] was analysed. Number of surveillance cystoscopies was compared against the number expected under EAU guidelines. Patient drop-out rates and contributing factors were quantified. Using a health economic model, two scenarios were compared over a 10-year time horizon:
(a) “Scottish Real-World Evidence (RWE)” arm;
(b) “Biomarker” arm, assuming that using a non-invasive test could improve adherence by halving the non-clinical patient drop-out rate.
The model evaluated progression to MIBC, quality-adjusted life years (QALYs), total costs, and the incremental cost-effectiveness ratio (ICER).
Results: In total, 11,203 cystoscopies were performed over 5 years, 52% less than the 23,485 expected under EAU guidelines. 550 patients discontinued surveillance. The biomarker arm resulted in 33% fewer progressions to MIBC (68 vs. 96) and a net gain in population health (15,312 vs. 15,214 QALYs), compared to the RWE arm. The 10-year cost was higher in the biomarker arm (£49.73M vs. £48.69M), due to more patients undergoing surveillance. This yielded an ICER of £10,612 per QALY, indicating the strategy as being cost-effective.
Conclusions: The non-invasive nature of a urinary biomarker can improve patient adherence to surveillance, while being cost-effective and improving long-term clinical outcomes.
P3-9 Moving the dial on haematuria investigation – a multicentre real-world evaluation of the Haematuria Cancer Risk Score
Mr Tom Malik1, Mr Jonathan Denfhy1, Dr Hpone Theinka Lin1, Dr Lubna Mohammed1, Miss Kirthana Babureddy2, Miss Amber Pankhurst2, Miss Amina Buba3, Miss Jessica Head4, Ms Sian Dudley5, Professor Jonathan Aning1, et al.
1Bristol Urological Institute, Bristol, United Kingdom, 2Gloucestershire Hospitals NHS Foundation Trust, Cheltenham, United Kingdom, 3Royal United Hospitals NHS Foundation Trust, Bath, United Kingdom, 4Somerset Foundation Trust, Taunton, United Kingdom, 5Great Western Hospitals NHS Foundation Trust, Swindon, United Kingdom
Introduction: NICE NG12 guidance governs urgent referral for suspected bladder cancer (BCa) and haematuria is the predominant referral symptom. Significant over-investigation happens on the present pathway. We evaluated the potential of the recently described Haematuria Cancer Risk Score (HCRS) to improve practice.
Materials & Methods: The HCRS was developed to improve selection of patients for cystoscopy for suspected BCa, using a weighted HCRS cut-off of ⩾82. Data were retrospectively evaluated for all patients referred to five institutions meeting NG12 criteria, January to April 2025. The primary outcome was cancer detection rate.
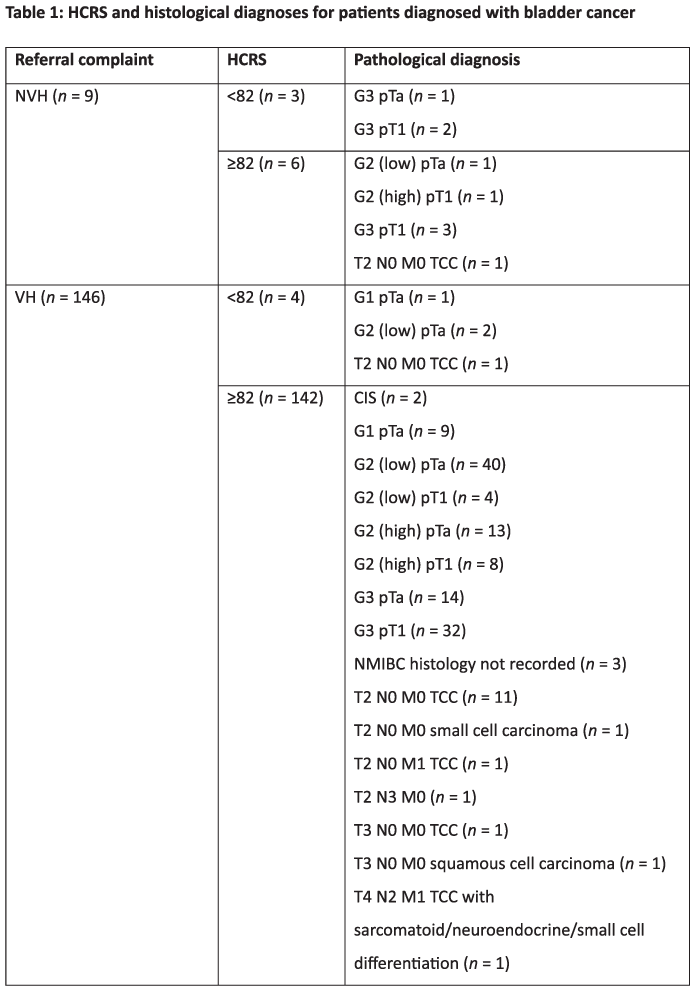
Results: In total 1731/1944(89%) referrals were eligible. Of these 1421/1731(82%) had sufficient information to calculate the HCRS. Overall 1152/1421(81%) scored HCRS ⩾82, of whom 148/1152(13%) had BCa detected. In the 269/1421(19%) with HCRS <82, 7/269(3%) had BCa
Of 349/1421(25%) presenting with non-visible haematuria (NVH), HCRS was ⩾82 in 148/349(42%), of whom 5/148(3%) were diagnosed with NMIBC and 1/148(0.7%) with MIBC. HCRS was <82 in 201/349(58%), of whom 3/201(1%) had NMIBC, no MIBC were missed.
Of 1072/1421(75%) with VH, HCRS was ⩾82 in 1004/1072(94%). Of these 125/1004(12%) had NMIBC and 17/1004(2%) MIBC. Of 68/1072(6%) with HCRS <82, 3/68(4%) had NMIBC and 1/68(1%) MIBC. Table 1 summarises histology by HCRS score.
Conclusions: The HCRS is a simple, effective method to further risk stratify NG12 referrals and significantly reduce over-investigation with flexible cystoscopy. In NVH there was potential for a 60% reduction in flexible cystoscopies. In VH HCRS demonstrates potential for identifying patients who may benefit most from biomarkers in future pathways.
P3-10 Contemporary Practice Patterns in Female Radical Cystectomy: Results of a UK and Ireland Survey
Miss Elizabeth Day2, Mr Francesco Pio Bizzarri1, Ms Rebecca Martin3, Mr Adam Nelson1, Miss Alexandra Colquhoun1, Miss Helena Burden4, Mr Benjamin Ayres5, Mr Vishwanath Hanchanale6, Mr James Douglas7, Professor Jonathan Aning4, Miss Niyati Lobo1
1Cambridge University Hospitals NHS Foundation Trust, Cambridge, United Kingdom, 2NHS Ayrshire and Arran, Scotland, 3Royal Marsden NHS Foundation Trust, London, UK, 4Bristol Urological Institute, Bristol, UK, 5St George’s University Hospitals NHS Foundation Trust, UK, 6Royal Liverpool and Broadgreen University Hospital NHS Trust, UK, 7University Hospital Southampton NHS Foundation Trust, Southampton, UK
Introduction: Female patients undergoing radical cystectomy (RC) face unique challenges, including sexual dysfunction, vaginal morbidity, and surgical menopause. Organ-sparing techniques may reduce these complications, yet practice remains inconsistent and gender-specific pathways are lacking. We evaluated current UK and Ireland practice to identify gaps and opportunities for standardisation.
Patients and Methods: A 36-item online survey explored pre-operative counselling, surgical technique, and post-operative care. It was distributed to all cystectomists in the UK and Ireland.
Results: Sixty-four surgeons (56.1%) from 41 centres (70.7%) responded; 82.8% were male, and 76.6% performed >5 female RCs annually. Robotic surgery predominated (70.3%).
Pre-operatively, 71.9% used gender-specific leaflets, and most discussed sexual dysfunction (98.4%) and vaginal shortening (96.9%), but more rarely prolapse (68.8%) or vaginal discharge (17.2%). Prehabilitation was uncommon (topical oestrogen 4.7%, pelvic floor exercises 20.3%).
Organ-sparing RC was never or rarely performed by 28.1%, mainly due to oncological concerns (72.2%). Among those performing organ-sparing, 19.6% required MRI for patient selection.
Post-operatively, sexual function (57.8%) and prolapse (56.3%) were commonly assessed, but vaginal examination (17.2%) and PROMs (9.4%) were infrequent. Pathways for managing vaginal complications were absent in 64.0%, and access to rehabilitation was limited: 50.0% lacked female-specific sexual therapy, and 45.3% lacked vaginal dilators, with nearly half reporting unstructured provision.
Conclusion: Practice in female RC is highly variable, with gaps in counselling, organ preservation, and follow-up. Gender-specific, evidence-based pathways and training in techniques such as nerve-sparing are urgently needed to standardise care.
ePoster Session 4: Functional Urology & Neuro-Urology Bladder Dysfunction and Reconstruction 1, John Blandy, June 16, 2026, 08:00 - 09:00
P4-1 Clinical Outcomes of Multidisciplinary Care for Recurrent Urinary Tract Infections: Four-Year Data from a Complex UTI Clinic
Miss Hira Bakhtiar Khan1,2, Dr Anandana Bhattia1, Miss Pragnitha Chitteti2,3, Miss Sindhu Sankaran1,2, Jayne Morris-Laverick1, Stephanie Bezemer1, Mr George Hanna1, Mr Ahmed Ghonaimey1, Dr Csaba Marodi1, Miss Mehwash Nadeem1,2
1James Cook University Hospital, Middlesbrough, United Kingdom, 2Teeside Urology Research Alliance (TURA), Middlesbrough, United Kingdom, 3Royal Salford Hospital, Middlesbrough, United Kingdom
Introduction: Recurrent urinary tract infections (rUTIs) are challenging to manage and are associated with significant morbidity, antimicrobial resistance, and healthcare costs. We assessed treatment outcomes in patients with rUTIs managed through a multidisciplinary complex UTI clinic at a single tertiary centre.
Methods: In response to the increasing prevalence of antibiotic resistance and the financial burden of rUTIs, a multidisciplinary complex UTI clinic supported by specialist nurses and microbiologists was established in April 2021. A prospectively maintained database of all patients referred between April 2021 and March 2025 was reviewed. Data collected included demographics, urine culture results and antimicrobial sensitivities, investigations performed, and treatment outcomes.Quality of life (QoL) was assessed pre- and post-treatment, and patient-reported outcomes were measured using the Patient Global Impression of Improvement (PGI-I)scale.Minimum follow-up was six months.
Results: 368 patients were included (meanage 59 ± 19 years; 317 female [86%], 51 male [14%]). Escherichiacoli was the most common causative organism (47%), and 25% of patients had multi-drug-resistant infections. All patients received first- and second-line treatments, resulting in UTI resolution in 70%. The remaining 30% required escalation to intravesical instillation therapy following multidisciplinary team discussion. Post-treatment, QoL scores improved significantly, with approximately 70% of patients reporting good to excellent outcomes. On the PGI-I scale, 80% (n=294) reported good to excellent improvement, with overall treatment success achieved in 88% (n=324) of patients.
Conclusion: A dedicated multidisciplinary complex UTI clinic provides effective management for patients with rUTIs, achieving high rates of symptom resolution, improved QoL, and patient-reported satisfaction, while supporting antimicrobial stewardship.
P4-2 Clinical Outcomes and Differential Organism Response to Intravesical Aminoglycoside Therapy in Adults with Recurrent Urinary Tract Infections
Miss Sindhu Sankaran1,2, Miss Pragnitha Chitteti1,2, Miss Hira Bakhtiar Khan1,2, Dr Csaba Marodi1, Miss Jayne Morris1, Miss Stephanie Bezamer1, Miss Mehwash Nadeem1,2
1James Cook University Hospital, Middlesborough, United Kingdom, 2Teeside Urology research Alliance, Middlesborough, United Kingdom
Introduction: Intravesical aminoglycosides are increasingly used in adults with complex, refractory recurrent urinary tract infections (rUTIs), particularly where antimicrobial resistance (AMR) limits oral treatment options. While overall clinical benefit has been reported, data comparing outcomes by infecting organism remain limited.This study evaluates clinical outcomes and organism-specific response to intravesical aminoglycoside therapy.
Methods: A retrospective analysis was conducted of adult patients treated with intravesical gentamicin or amikacin for complex rUTIs in a dedicated UTI clinic between May 2021 and May 2024. Data collected included demographics, infecting organisms, AMR patterns,UTI frequency, UTI-related hospital admissions, and clinical outcomes before and after treatment. Subgroup analysis compared Escherichia coli and non–E. coli infections.
Results: Fifty-six patients (41 gentamicin,15 amikacin) with mean age of 54 years were included. Non–E. coli infections were associated with higher rates AMR compared with E. coli infections (48% vs 21%). Overall, intravesical aminoglycoside therapy resulted in a substantial reduction in UTI episodes across both treatment groups. In the gentamicin group, 85% of patients experienced a reduction in UTI frequency,with 18% becoming infection-free. In the amikacin group,UTI episodes were reduced by 53%, with 26% becoming infection-free.Among 23 patients with prior UTI-related hospital admissions,87% avoided further inpatient admission following treatment. Of 28 patients with multidrug-resistant infections, 75% demonstrated improved antimicrobial susceptibility.
Conclusion: Intravesical aminoglycoside therapy is associated with meaningful clinical benefit in adults with complex rUTIs, including those with non–E. coli and multidrug-resistant infections.Reductions in UTI frequency and hospital admissions highlight its value as an effective treatment strategy with potential benefits for antimicrobial stewardship and healthcare utilisation.
P4-3 Clinical Effectiveness of a Double-Dose MV140 Regimen in Recurrent Urinary Tract Infections Associated with Neuropathic Bladder
Mr Sagar Kanabar1, Mr Stephen Foley, Mr Bob Yang
1Royal Berkshire Hospital, Reading, United Kingdom
Introduction: Recurrent urinary tract infections (rUTIs) can cause significant morbidity in patients with neuropathic bladder (NB), contributing to antimicrobial resistance and quality of life. MV140 is a sublingual bacterial immunomodulator containing inactivated Escherichia coli, Klebsiella pneumoniae, Enterococcus faecalis, and Proteus vulgaris, with established efficacy in idiopathic rUTIs. However, evidence for its use in NB remains limited. This study prospectively evaluates the effectiveness and safety of double-dose MV140 in patients with NB-associated rUTIs.
Patients and Methods: A prospective review was conducted of 14 patients (3 male, 11 female; mean age 46 years, range 24–72) with NB of mixed aetiologies, including spinal cord injury (n=6), multiple sclerosis (n=1), prior incontinence surgery (n=1), Fowler’s syndrome (n=1), and advanced insulin-dependent diabetes mellitus (n=1). All patients received double-dose MV140 (two sublingual puffs twice daily). Thirteen patients (93%) performed intermittent self-catheterisation. Concomitant intravesical gentamicin (n=3) and iALURIL instillations (n=1) were continued. Mean follow-up was 12 months. The primary outcome was reduction in infection frequency; secondary outcomes included UTI-free status, symptom severity, and microbiological findings.
Results: Before treatment, five patients experienced monthly infections and nine had recurrent infections despite prophylaxis. Post-treatment, 9/14 (64%) remained UTI-free, while 5/14 (36%) experienced breakthrough infections of reduced severity. Median annual infection frequency fell from five to two episodes. Post-treatment cultures were negative in most cases, with two cases of asymptomatic bacteriuria. No adverse events were reported.
Conclusions: Double-dose MV140 was safe and associated with a clinically meaningful reduction in rUTIs in patients with neuropathic bladder, extending existing evidence to this cohort.
P4-4 The Natural History of Continence and Patient Satisfaction after Mesh Removal: a Tertiary-Centre Experience
Mr Ioannis Loufopoulos1, Mr Keith Pace2, Mr Loai Alqahtani2, Mr Kapriniotis Konstantinos2, Miss Helena Gresty2, Mrs Tamsin Greenwell2, Mr Jeremy Ockrim2
1Royal Free Hospital, London, United Kingdom, 2University College London Hospitals, London, United Kingdom
Introduction: To characterise continence outcomes, pain resolution, and patient satisfaction following mid-urethral sling (MUS) removal and salvage interventions.
Materials and Methods: A retrospective analysis of 106 women undergoing MUS removal (2020–2025) at a Complex Mesh Centre was performed. Indications, imaging (MRI/TRUS), complications, post-removal continence, secondary continence procedures, clean intermittent self-catheterisation (CISC), and satisfaction were assessed.
Results: Pain was the primary indication for mesh removal (94%). Recurrent UTIs occurred in 39%, pelvic organ prolapse in 27%, bladder/urethral extrusion in 27%, and vaginal exposure in 29%. Persistent urinary incontinence was recognised in 78.5%. MRI reliably identified retropubic TVT arms but was poor for obturator visualisation, while TRUS detected urethral or bladder involvement in 92%. Partial mesh removal was performed in 57% and total removal in 43%. Median length of hospital stay was 4 days, with predominantly Clavien–Dindo I–II complications.
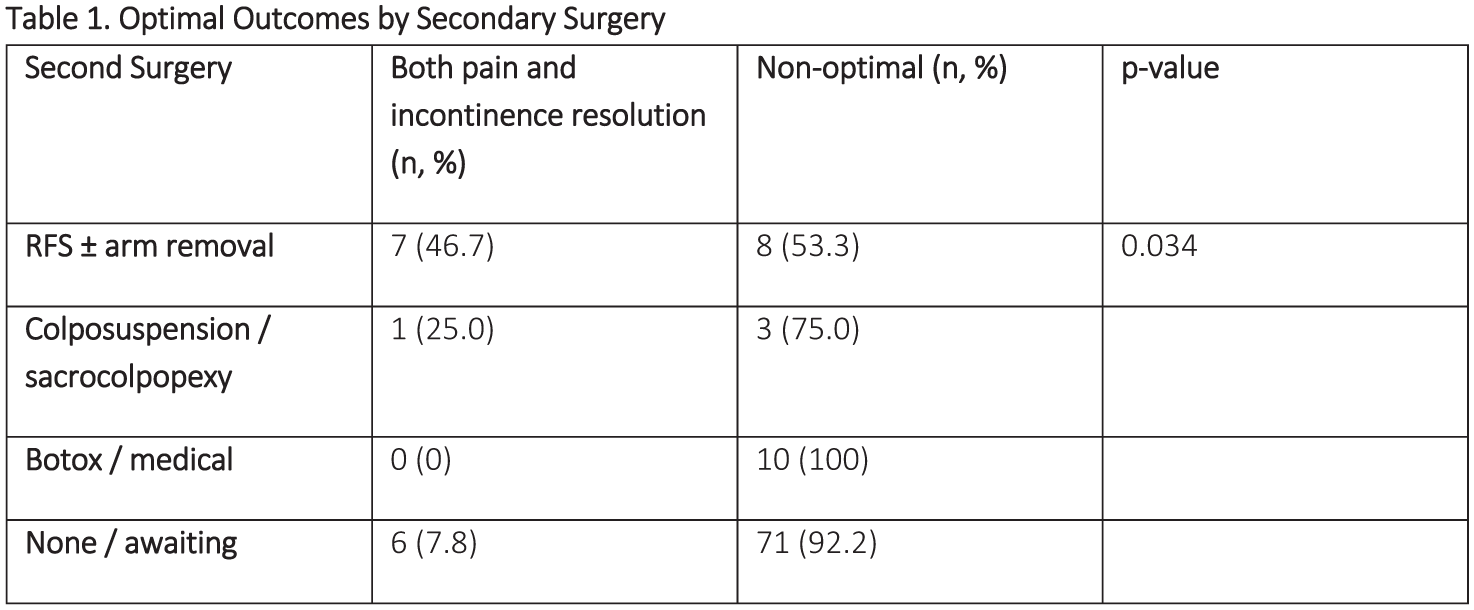
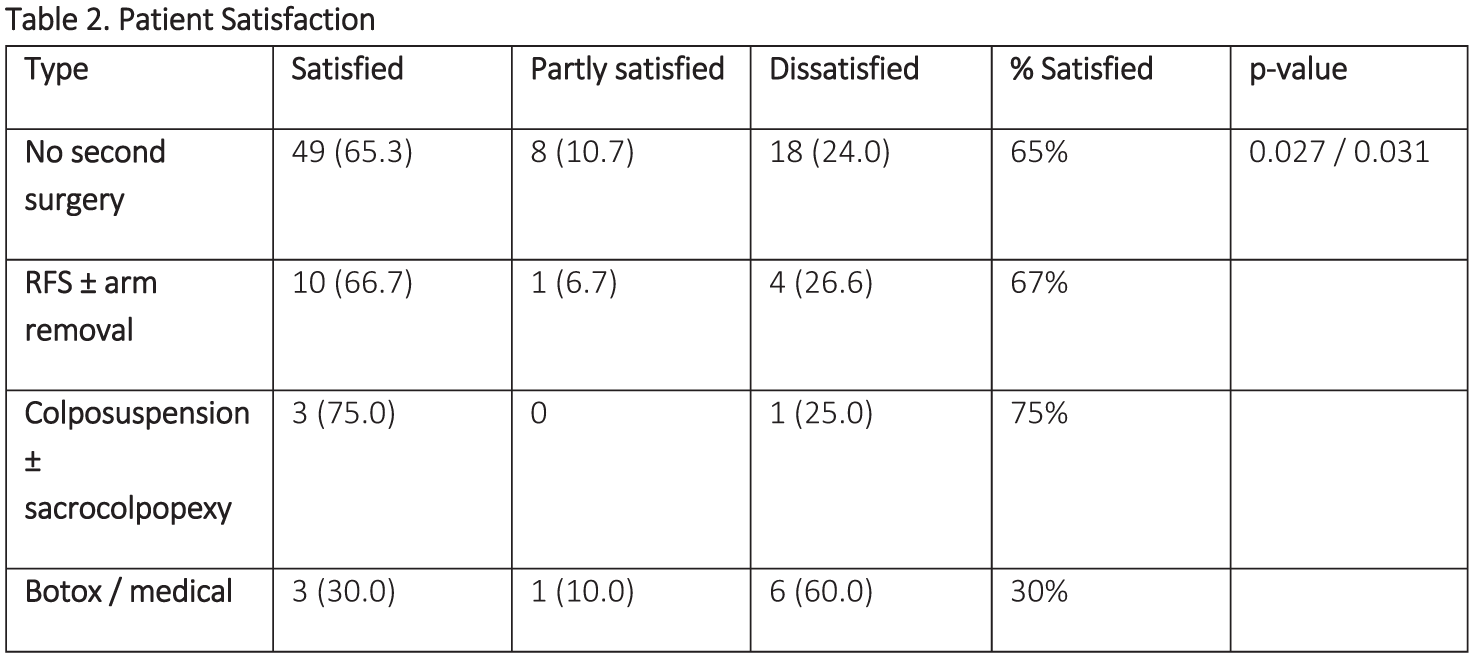
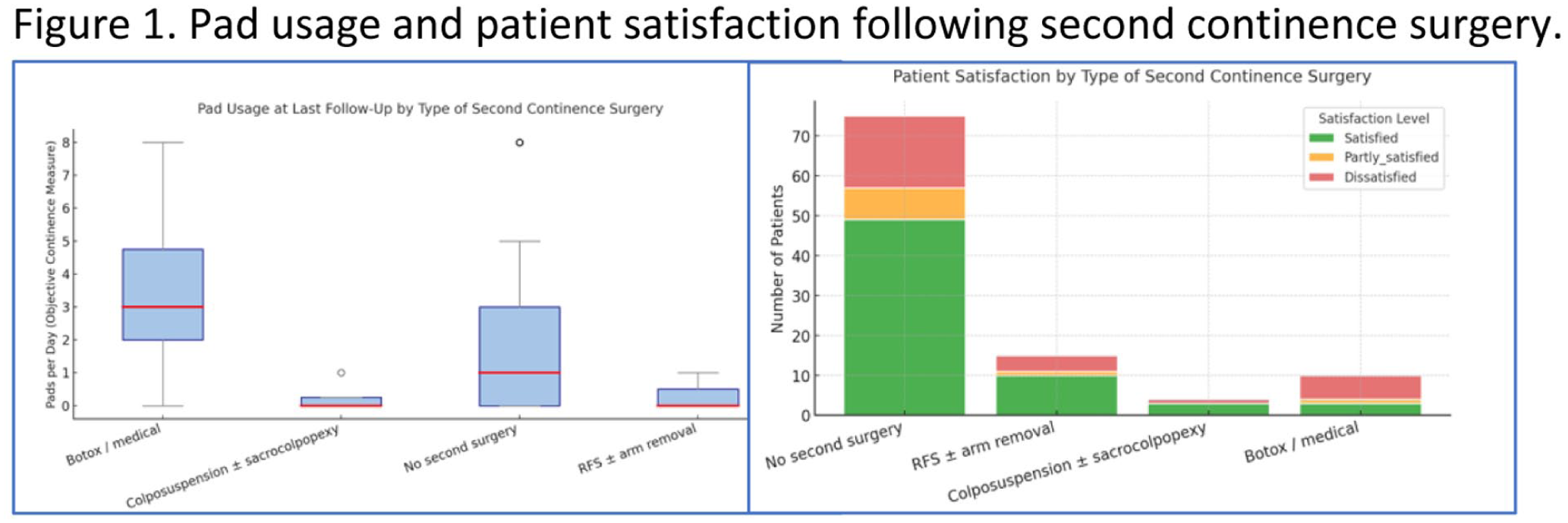
At follow-up, 79.2% reported urinary incontinence. Video-urodynamics showed intrinsic sphincter deficiency (44%), rotational incontinence (29%), and simple hypermobility (27%). ISD predominated after TVT removal, while hypermobility was more common after TVTO (p=0.02). Twenty-five patients (28.7%) underwent secondary continence surgery, most commonly rectus fascial sling or colposuspension, achieving lower pad use than conservative management (p<0.05). Complete pain resolution occurred in 45%. 13% achieved both pain and incontinence resolution, predominantly following RFS (47%) (p=0.034). Satisfaction was greater after colposuspension (75%) and RFS (66.7%), compared to Botox (30%)(p<0.05).
Conclusions: MUS removal improves pain in half of patients but leaves most incontinent. Salvage continence surgery improves dryness and satisfaction, with a risk of voiding dysfunction.
P4-5 Long-term pilot assessment of Alluzience botulinum toxin A in patients with Botox-refractory detrusor overactivity
Mr John Piedad1, Mr Steve Foley2, Mr Bob Yang2
1Hereford County Hospital/Royal Berkshire Hospital, Hereford/Reading, United Kingdom, 2Royal Berkshire Hospital, Reading, United Kingdom
Intra-detrusor Allergan Botox improves symptoms in pharmacotherapy-refractory detrusor overactivity (DO). However, some patients develop ‘resistance’ to Botox. Alluzience abobotulinumtoxin type A (Galderma SA, Lausanne, Switzerland) may be an alternative. We present long-term follow-up of the first assessment of Alluzience in patients who no longer derive benefit from Botox.
Eighteen patients with DO received intra-detrusor 250 Speywood units of Alluzience from April to December 2024, after gaining ethical approval. The majority were female (83.3%), with a median age of 69 (59-77) years. Baseline pad use and incontinence scores were collected using the International Consultation on Incontinence Questionnaire-Urinary Incontinence Short-Form (ICIQ-SF) and Incontinence Impact Questionnaire Short-Form (IIQ-SF). These were repeated at short term and long-term telephone follow-up, and analysed against baseline scores.
Patients had short-term follow-up at 20 (16-27) days and long-term follow up at 12 (10-13) months. One patient went into urinary retention requiring indwelling and then transient intermittent urinary catheterisation, with no other complications. Pad use decreased from 4.5 (3.0-5.3) to 1.5 (1.0-4.0) and then 3.0 (1.0-4.0) at short and long-term follow-up, respectively (P<.001). Total ICIQ-SF scores improved short-term by 44.7%, and only 26.3% at long-term follow-up compared to baseline (P<.001). Total IIQ-SF scores dropped by 32.3% at short-term, and 16.1% at long-term follow-up (P=.001).
This pilot assessment shows clear early benefit from Alluzience which is maintained for some patients long-term. It is also safe with no unexpected complications. In a patient population refractory to Allergan Botox, and considering more invasive surgical interventions, it provides an alternative option.
P4-6 Long term outcomes of sacral neuromodulation in patients with psychiatric disorders
Mr Stefanos Agiotakis1, Mr Anastasios Natsos1, Ms Saddaf Hina1, Ms Paraskeve Granitsiotis1, Mr James Blackmur1
1Western General Hospital, Edinburgh, United Kingdom
Introduction: Psychiatric disorders are common among patients undergoing sacral neuromodulation (SNS). The existing literature already describes an association between psychiatric comorbidity and overactive bladder. We investigated the impact of formal mental health service involvement on SNS outcomes.
Methods: Retrospective analysis of 72 patients with permanent SNS implants at our tertiary centre. 49 were prescribed psychiatric medications, with a median age of 46 years (17–68) and mean follow up time of 16 months. Patients were stratified according to prior review by mental health services (psychiatry or psychology). Outcomes were analysed by urological indication, including voiding dysfunction (VD) and detrusor overactivity (DO). Treatment success was defined as discharge to patient-initiated follow-up or documented symptomatic improvement.
Results: 49 patients receiving psychiatric medications- 23 were under mental health services and 26 weren’t. Successful outcomes were recorded in 15/23 patients (65.2%) with mental health service involvement and 16/26 patients (61.5%) respectively (p = 0.57). Among VD patients (28), success rates were 7/15 (46.7%) in those with mental health service involvement and 9/13 (69.2%) in those without (p = 0.28). In patients treated for DO (n = 19), success was achieved in 8/8 (100%) where mental health services were involved compared with 6/11 patients (54.5%) without (p = 0.045).
Conclusions: In patients receiving psychiatric medications, overall SNS outcomes were not significantly influenced by mental health service involvement. Subgroup analysis suggests a potential benefit of mental health service input in patients treated for DO as opposed to those with VD. Larger cohorts are required for further research.
P4-7 Long-term outcomes of urethral diverticulectomy in women: A 20-year single-centre review
Miss Amna Butt1, Miss Amna Hashmi, Miss Nuseyba Sheikh
1University College Hospital, London, United Kingdom
Introduction: Female urethral diverticulum is an uncommon but clinically relevant condition. Surgical excision remains the gold standard for treatment; however, postoperative recurrence and incontinence remain potential concerns. This study aimed to evaluate the long-term surgical outcomes of urethral diverticulectomy in women over a 20-year period at a tertiary referral center.
Methods: A retrospective review was conducted of 224 women who underwent urethral diverticulectomy between 2005 and 2024.Demographics, diverticulum characteristics (location and complexity), operative details, and postoperative outcomes were analyzed. Surgical success was defined as the absence of diverticulum recurrence. Additional outcomes included urinary flow rates, bladder capacity, continence status, requirement for secondary interventions, and complication rates.
Results: Among the 224 patients, the mean age was 46.5±12.9 years, with a median symptom duration of 24 months. Most diverticula were mid-urethral (65.9%) and 75% classified as complex. Preoperative Qmax averaged 14.4±12.0 mL/s, and bladder capacity remained stable postoperatively. Median catheterization duration was 4 weeks, and median hospital stay was 3 days. Surgical success was achieved in 95% of cases, with a recurrence rate of 5%. De novo stress and urgency incontinence developed in 29% and 17% of patients, respectively. Seventy-eight patients had preoperative stress urinary incontinence (SUI).At last follow-up, 49% of patients were completely continent, while 51% had persistent incontinence; 9.4% underwent subsequent anti-incontinence procedures.
Conclusions: Urethral diverticulectomy provides excellent long-term surgical and functional outcomes,with high success rates and durable symptom relief. However, postoperative incontinence remains a significant issue for a subset of patients, highlighting the importance of thorough preoperative counseling and individualized follow-up strategies.
P4-8 Outcomes of Daycase Artificial Urinary Sphincter Placement in Men: A Tertiary Centre Experience
Ms Nikita Bhatt1, Eva Browne2, Victoria Lavin2, Jonathan Barclay2, Christopher Harding2, Arjun Nambiar2
1St Vincent’s University Hospital, Dublin, Ireland, 2Newcastle Hospitals NHS Foundation Trust, Newcastle, United Kingdom
Introduction: Traditionally,patients are admitted postoperatively after Artificial urinary sphincter (AUS) implantation for intravenous antibiotics and catheter management, followed by discharge the next day. Since 2021, our centre has adopted a day-case AUS insertion protocol. This study evaluates the safety and efficacy of this approach.
Materials & Methods: We conducted an audit of male bulbar AUS insertions performed in a tertiary centre over three years (2022–2025). Procedures were performed by three surgeons, with a plan to discharge patients the same day.
Results: A total of 98 men underwent AUS insertion, with 88% discharged on the day of surgery. Forty-seven (48%) of these patients received postoperative oral antibiotics. The median age was 72 years (IQR: 67–77), with radical prostatectomy being the most common etiology of UI (63%). At a median follow-up of 23 weeks (IQR: 15–35) in the cohort discharged on the day of surgery, early readmissions occurred in 2 patients (2%):one for urinary retention and one for sepsis. The commonest reason for patients to stay overnight was anaesthetic or medical issue, followed by social reasons. Demographics were similar between the day of surgery discharge group and those that stayed overnight. Two patients in the cohort that stayed overnight were readmitted within the first 6 weeks (12.5%), one for orchitis and the other for device infection.
Conclusions: We demonstrate the safety and efficacy of same day discharge with AUS insertion. Wider adoption of this model could benefit resource-limited healthcare systems like the NHS. Multicentre studies are warranted to validate these findings.
P4-10 Robotic Reconstructive Urologic Surgery: Multicenter outcomes of IURES Robotic Urology Special Interest Group
Dr Ahmet Furkan Sarikaya1, Dr Mustafa Kıraç2, Dr Fevzi BEDİR3, Dr Orçun ÇELİK4, Dr Giray ERGİN2, Dr Bahri GÖK5, Dr Serdar AYDIN6, Dr Ahmet GÜRBÜZ7, Dr Tayfun OKTAR7, Dr Kanan VALİYEV8, Dr Arif ÖZKAN9, Dr İbrahim Can AYKANAT10, Dr Tomislav Kuliš11, Dr Serdar MADENDERE12, Dr Barış ESEN7, Dr Emre HURİ8, Dr Mevlana Derya BALBAY12, Dr Abdullah Erdem CANDA13
1Viransehir State Hospital, Sanliurfa, Türkiye, 2Yüksek İhtisas University, Koru Ankara Hospital, Ankara , Türkiye, 3Erzurum Regional Training and Research Hospital, Department of Urology, Erzurum, Türkiye, Erzurum, Türkiye, 4Bazekol Çiğli Hospital, Department of Urology, İzmir, Türkiye , İzmir, Türkiye, 5Lokman Hekim University, Department of Urology, Ankara, Türkiye, 6Koç University, Faculty of Medicine, Department of Obstetrics and Gynecology, İstanbul, Türkiye, 7Koç University, Faculty of Medicine, Department of Urology, İstanbul, Türkiye, 8Hacettepe University, Faculty of Medicine, Department of Urology, Ankara, Türkiye, 9Medicana Zincirlikuyu Hospital, İstanbul, Türkiye, 10Balıkesir University, Faculty of Medicine, Department of Urology, Balıkesir, Türkiye, 11Department of Urology, University Hospital Center Zagreb , Zagreb , Croatia, 12VKV American Hospital, Department of Urology , İstanbul, Türkiye, 13Koç University, Faculty of Medicine, Department of Urology, İstanbul, Türkiye & Director RMK AIMES Training Center, Istanbul, Türkiye
Introduction: Robotic surgery has increasingly been adopted for complex reconstructive urologic procedures; however, multicenter data on its safety and feasibility remain limited. We report the initial outcomes of the International Urologic Research Society (IURES) Robotic Reconstructive Urology Special Interest Group(SIG), combining experiences from multiple centers and surgeons.
Methods: We retrospectively analyzed 66 patients who underwent robotic reconstructive urologic surgery across five centers performed by nine surgeons. Procedures included pyeloplasty, ureteroureterostomy, ureteroneocystostomy (UNC), augmentation ileocystoplasty,Y-V plasty,vesicovaginal fistula repair, UNC with psoas hitch, sacrocolpopexy, transvesical bladder neck stricture repair with lingual mucosa, and selected robotic reconstructive procedures. Demographics, operative time, estimated blood loss, length of hospital stay, and complications (Clavien–Dindo classification) were evaluated.
Results: Median patient age was 42 years (range 6–76). Pyeloplasty was the most common procedure(n=35), performed for intrinsic obstruction or crossing vessels. Additional procedures included ureteroureterostomy(n=6), ureteroileal stricture repair following RARC with intracorporeal neobladder(n=4) & ileal loop(n=2), UNC for iatrogenic injury or stricture(n=5), augmentation ileocystoplasty(n=3), vesicovaginal fistula repair(n=3), Y-V plasty(n=2), transvesical bladder neck stricture repair(n=2), and several single-case reconstructive procedures. Operative time ranged from 28 to 297 minutes. Estimated blood loss was minimal in most cases (10–200 mL). Median hospital stay ranged from 2 to 5 days. No intraoperative conversions occurred, and no major complication (Clavien ⩾III) was observed.
Conclusion: This first multicenter experience of the IURES Robotic Reconstructive Urology SIG demonstrates that robotic reconstructive surgery across a wide range of procedures is safe and feasible, with low morbidity and short hospital stays. These findings provide a basis for future prospective studies and procedural standardization.
ePoster Session 5: Andrology 1, John Anderson, June 16, 2026, 08:00 - 09:00
P5-1 Patient-Reported Satisfaction Following Primary and Revision Inflatable Penile Prosthesis (IPP) Surgery: A Multicentre Analysis Using a Validated Instrument
Mr Abdullah Al-Mitwalli1, Dr H Bernie3, Dr E Abou Chawareb2, Dr M Hammad2, Mr A Di Giovanni1, Mr M Shah1, Dr L Amorim3, Dr T Pereira3, Dr Lai Lillian4, Ms N.B Liso5, Dr A Wan1, Dr M Gosalia1, Dr A Liaw4, Dr C Nelson5, Dr J.M Flores5, Mr W.G Lee1, Ms P Sangster1, Dr F Yafi2, Prof J.P Mulhall5, Prof David Ralph1
1University College London Hospitals, London, United Kingdom, 2University of California, Irvine, United States of America, 3Indiana University, United States of America, 4Wayne State University, United States of America, 5Memorial Sloan Kettering Cancer Center, United States of America
Background: Surgeon-reported outcomes following IPP consistently report satisfaction rates approaching 98%; however, validated patient-reported outcomes provide more accurate assessment of real-world experience. The Satisfaction Survey for Inflatable Penile Implant (SSIPI) is the only validated English-language instrument assessing outcomes across four domains. This study evaluates SSIPI following primary and revision IPP.
Methods: Men from multiple referral centres who underwent primary or revision IPP surgery and completed SSIPI ⩾6 months postoperatively were included. SSIPI: 16 questions across 4 domains including, satisfaction (S, 4Q/score range 4-20), pain (P, 2Q/2-10), appearance (A, 5Q/6-30) and function (F, 4Q/4–20), each composed of questions scored on 1–5-point Likert scale (maximum score 80), where higher scores indicate more favourable outcomes. We selected an endpoint of scoring ⩾4 (most of the time) define overall high satisfaction (high satisfaction, low pain, high comfort with appearance, excellent function).
Results: To date, 332 primary IPP and 66 revision patients completed SSIPI. Mean total SSIPI scores were 64 (SD 14) for primary IPP and 56 (SD 18) for revision IPP. Overall high satisfaction was reported by 74% of primary and 61% of revision patients. Across domains, P consistently scored highest, while A scored lowest in both cohorts. Among revision patients, satisfaction declined with increasing number of revisions, and those revised for mechanical failure reported higher satisfaction than those revised for infection.
Conclusion: Using a validated instrument, satisfaction following both primary and revision IPP surgery is lower than previously reported. These findings highlight the importance of standardized, validated outcome measures in accurately characterizing IPP patient satisfaction.
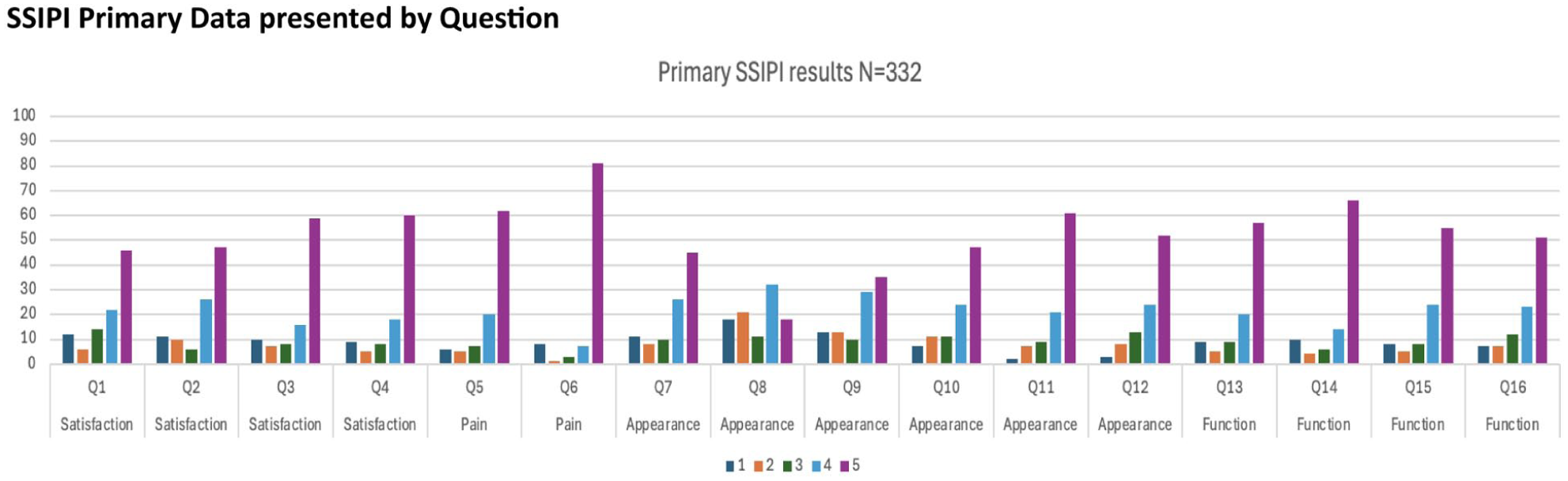
P5-2 Plaque Incision and Grafting for Peyronie’s Disease: 15-year experience and functional outcomes from a high-volume andrology centre
Dr Shiv Sarna1, Mr Karl Pang3, Prof David Ralph2, Prof Asif Muneer2, Mr Hussain Alnajjar2
1Norfolk And Norwich University Hospital, Norwich, United Kingdom, 2University College London Hospital, London, United Kingdom, 3Chelsea and Westminster Hospital, London, United Kingdom
Introduction: Plaque incision and grafting (PIG) is a well-established treatment for severe or complex Peyronie’s disease and preserved erectile function. While PIG can correct challenging curvatures and minimise further penile shortening, it carries risks including erectile dysfunction (ED). We evaluated long-term outcomes, patient satisfaction and complication rates following PIG for Peyronie’s disease at a single high-volume centre.
Patients and Methods: This retrospective single-centre cohort study evaluated 325 patients undergoing the procedure between 2009 and 2024 at a high-volume centre.
Results: Median pre-operative curvature was 80° (IQR 60-90°) and 46.8% (152/325) had complex deformities (wasting 36.6%, hourglass 10.2%). 90.2% (293/325) completed follow-up (median 9.8 months) and were included in outcome analysis. Overall satisfaction was 87.0% (255/293), with 90.1% (264/293) resuming penetrative intercourse. Perceived length reduction occurred in 29.4% (86/293) and hypoaesthesia in 15.4% (45/293). Patients were stratified by baseline erectile status: 72.4% (212/293) had normal pre-operative erectile function and 27.6% (81/293) had pre-existing erectile dysfunction (ED). New-onset ED occurred in 22.2% (47/212) of previously potent men. Among men with pre-existing ED, 37.0% (30/81) improved and 13.6% (11/81) worsened. Multivariable regression showed cardiovascular comorbidities were significantly associated with post-operative ED, whereas graft size and complex deformity did not. Re-operation was required in 8.5% (25/293).
Conclusions: These findings suggest functional decline following PIG is often driven by systemic health rather than surgical technique. Integrating cardiovascular risk assessment into counselling is essential, as baseline vascular health significantly influences long-term recovery. Management at a high-volume centre remains key to optimising functional outcomes.
P5-3 Penile implants in prolonged ischemic priapism- malleable vs inflatable penile prosthesis insertion
Mr Abdullah Al-Mitwalli1, Mr C Kats-Summercorn2, Dr J Banerjee1, Mr M Shah1, Mr W.G. Lee1, Ms P Sangster1, Prof D Ralph1
1UCLH, London, United Kingdom, 2Whittington Hospital, London, United Kingdom
Introduction: Refractory ischemic priapism often leads to definitive erectile dysfunction necessitating need for penile prosthesis. Early penile prosthesis insertion is recommended to reduce complications and improve patient satisfaction. There is limited literature assessing malleable (MPP) vs inflatable penile prosthesis (IPP) as the initial implant.
Methods: Patients undergoing penile prosthesis surgery for refractory ischaemic priapism were retrospectively identified at a tertiary referral center from 1999-2025. Early implantation was defined <4 weeks weeks of priapism onset, delayed as >4. Data collected: demographics, priapism treatment, timing of surgery along with intraoperative details and complications.
Results: Data collected on 128/165 patients with mean age was 51.4 years (SD 14). First implant was MPP in 80 patients and IPP in 48. Among those receiving an initial MPP, 32 patients (40%) subsequently underwent exchange to IPP. Overall complications occurred in 10 (7.8%), including perforation (n=2), mechanical failure (n=1), infection (n=3), erosion (n=2), haematoma (n=2). 5 patients complained of sequalae of floppy glans n=2 and pain (n=3). There was no significant difference in complication rates between malleable and inflatable penile prostheses (Fisher’s exact test, p = 0.55). Table 1.
Conclusion: MPP are more commonly used as the initial implant in prolonged ischaemic priapism, although approximately one-third of patients subsequently undergo conversion to IPP. Early penile prosthesis implantation should be considered preferably giving patients the choice between a malleable vs inflatable type.
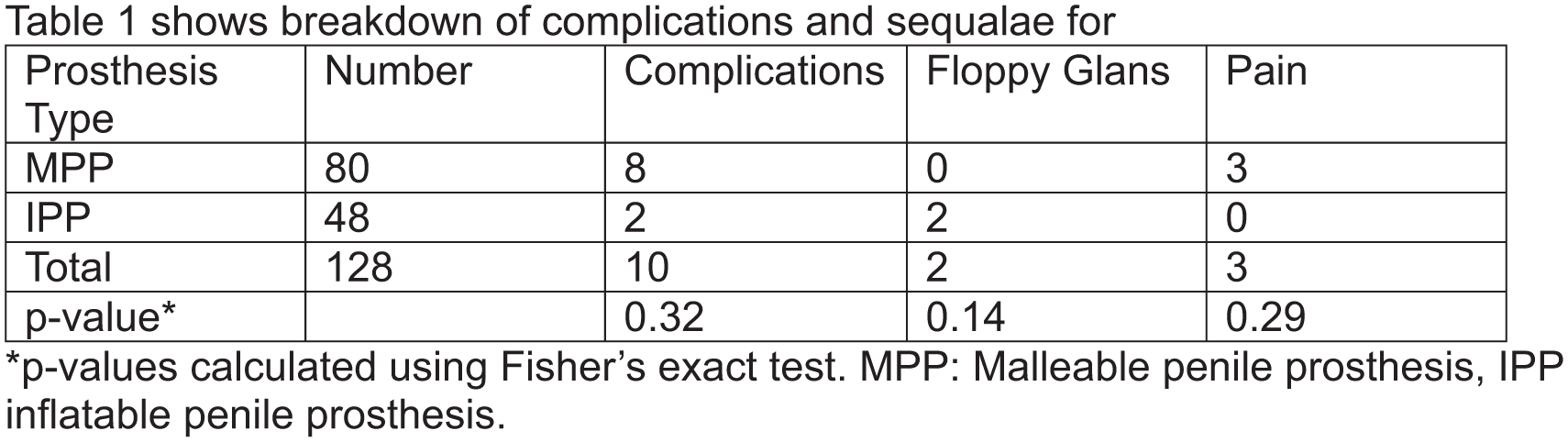
P5-4 The Impact of Body Mass Index on Survival After Penile Cancer Surgery
Dr Cesare Saitta1, Mr Mahmood Ziada1, Mr Adnan Ahmad1, Mr Paul Hadway1, Mr Raj Nigam1, Mr Varun Sahdev1, Mr Hussain Alnajjar1, Prof Asif Muneer1
1Male Genital Cancer Centre, Department of Andrology, University College London Hospitals, London, United Kingdom
Introduction: We investigated the impact of body mass index (BMI) on survival outcomes in patients undergoing surgery for primary penile cancer.
Materials and Methods: Patients undergoing surgery for primary penile cancer were identified from a single-centre institutional database. Obesity was defined according to World Health Organization criteria. Outcomes of interest were all-cause mortality (ACM) and cancer-specific mortality (CSM). Multivariable Cox regression models were used to identify predictors of outcomes, and 5-year survival estimates were assessed using Kaplan–Meier analysis.
Results: A total of 712 patients were included, with a median follow-up of 93 months (IQR 70–143). Of these, 130 (18.7%) were obese (BMI >30 kg/m²), 470 (66.0%) overweight (BMI 25-29.9kg/m²), 104 (14.6%) normal weight (BMI 18.5-24.9 kg/m²), and 8 (1.1%) underweight (BMI <18.5 kg/m²). On multivariable analysis for ACM, lymphovascular invasion (LVI; HR 1.67, p=0.07), increasing age (HR 1.01, p=0.011), pT3–4 vs. pT1–2 disease (HR 1.48, p=0.026), and pN3 vs. pN0–2 status (HR 3.37, p<0.001) were associated with increased mortality risk. Conversely, obesity (HR 0.35, p=0.019) and overweight status (HR 0.18, p<0.001) were associated with reduced ACM. For CSM, LVI (HR 2.12, p=0.02), advanced pT stage (HR 1.96, p=0.002), and pN3 disease (HR 5.17, p<0.001) were adverse predictors, while overweight status remained protective (HR 0.25, p=0.026). Five-year overall survival was 81.5% vs. 64.0% for obese vs. non-obese patients, and 5-year cancer-specific survival was 87.4% vs. 74.8% (both p<0.001).
Conclusion: Obesity was paradoxically associated with improved survival following penile cancer surgery, potentially reflecting a protective effect of greater metabolic reserve.
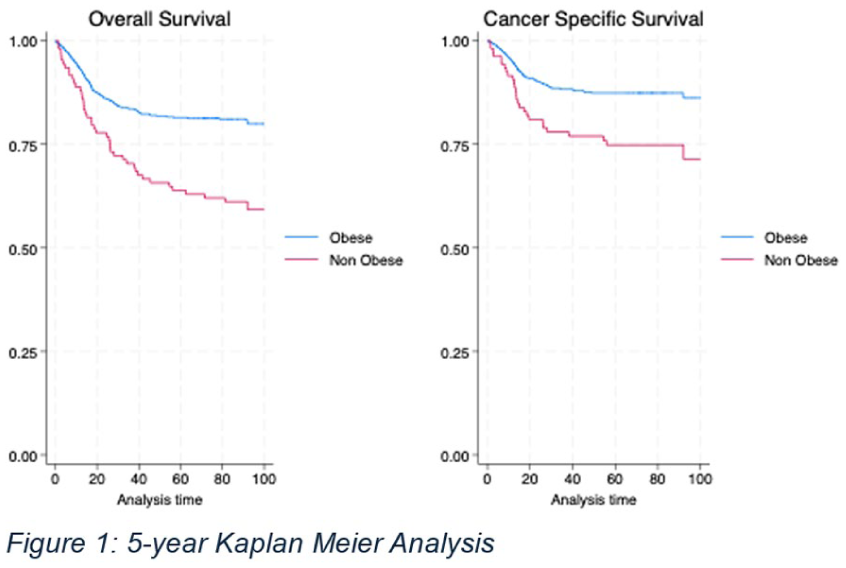
P5-5 A long learning curve demonstrates the complexity of gender-affirming inflatable penile prosthesis insertion
Mr Andrea Gobbo1, Mr Angelo di Giovanni1, Prof David John Ralph1, Mr Andrew Nim Christopher1, Mr Wai Gin Lee1
1New Victoria Hospital, London, United Kingdom
Introduction: Inflatable penile prosthesis (IPP) insertion in transgender and gender diverse (TGD) individuals is challenging even for high-volume implanters. The learning curve (LC) for this procedure has never been described. The aim was to construct outcome-based LCs for primary gender-affirming IPP insertion.
Material and Methods: 694 patients underwent gender-affirming IPP insertion at a single tertiary centre between 2001 and 2024. The case number was used as a proxy for surgical experience. The analysed outcomes included: revision surgery for any cause, revision for dissatisfaction with the device, and explant for infection. A risk-adjusted cumulative sum (RA-CUSUM) analysis was performed for each outcome to visually represent the learning trajectory and to identify the peak proficiency point (PPP- defined as the case number by which procedural competence was achieved).
Results: Adjusted probabilities for all outcomes showed a progressive risk reduction as experience improved. The adjusted probability for revision surgery decreased from 65% to 33%. Similarly, revision for dissatisfaction decreased from 32% to 15% and explant for infection from 24% to 4%.
RA-CUSUM analysis identified the PPP at case 311 for the risk of revision surgery, 261 for revision due to dissatisfaction, and 264 for infection. The RA-CUSUM plots demonstrated a steep learning period up to case 200, a transition between cases 250 and 300, with subsequent plateau indicating procedural proficiency.
Conclusion: This is the first study to define and describe outcome-based LCs for IPP insertion in TGD individuals. Outcomes depend on surgeon experience, with a high case number required to reach the PPP.
P5-6 Does Orchidopexy for Testicular Torsion Affect Long-Term Fertility Parameters in Males: A Systematic Review
Mr Muhammad Shariq Rahemtoola1,2, Miss Avula Aishwarya Rao2, Mr Hassaan Aziz2, Mr Peter Grice2, Mr Mohamed Mubarak2, Miss Theodora Stasinou2, Professor Ian Pearce2, Professor Vaibhav Modgil2
1Royal Bolton Hospital, Greater Manchester, United Kingdom, 2Manchester Andrology Research Collaborative, Manchester, England
Introduction: Testicular torsion (TT), a urological emergency, primarily affects adolescents and young adults. Prompt surgical intervention is crucial, as delays beyond six hours increase the risk of atrophy and necrosis, potentially affecting fertility. This review evaluates fertility outcomes in patients who underwent orchidopexy following torsion.
Patients (or Materials) and Methods: A systematic review was conducted in line with PRISMA guidelines and registered on PROSPERO. A literature search was performed between June-October 2025 across Scopus, PubMed, Web of Science. Studies included males with previous TT who underwent orchidopexy. Case reports, case-series, cohort, and case-control studies and RCTs were included. Extracted variables included demographics, follow-up duration, pregnancy outcomes, semen parameters, hormonal profiles, and anti-sperm antibodies.
Results: 17 studies involving 324 patients reported fertility and hormonal outcomes after detorsion with orchidopexy. Fertility was assessed through semen parameters and pregnancy outcomes. Pregnancy rates were consistently high at 90.2–91.3%, with a mean time to conception of 7.8 ± 1.6 months. One study found a paternity rate of 91%. Six studies presented semen analyses (mean sperm counts 97.2±112.1 × 10⁶, motility of 58.6±7.7%, and morphology 13.9±12.2%). Hormonal profiles were generally within expected ranges, including FSH, LH, testosterone, and inhibin B. Anti-sperm antibodies averaged 23.6 ± 3.6%. Mean follow-up was 4.2 years, without longitudinal fertility reporting.
Conclusion: Fertility appears largely preserved after surgical detorsion with orchidopexy.
However, small sample sizes, heterogeneity, and limited long-term data highlight the need for larger, standardised studies.
P5-7 Utility of preoperative imaging in penile fracture management
Dr Bianca Chua1, Dr Mohammad Shah1, Dr Suraj Pinni1, Dr Mohannad Nasser1, Dr Angelo di Giovanni1, Dr Abdullah Al-Mitwalli1, Dr David Ralph1, Dr Conrad Von Stempel1, Dr Wai Gin Lee1
1University College London Hospital, London, United Kingdom
Introduction: Penile fractures (PF) represent a rare yet significant urological emergency typically addressed by immediate surgical exploration. However, this traditional approach can result in negative explorations and extended surgical incisions. This study examines the utility of preoperative imaging in guiding surgical strategy, with a focus on minimising the need for degloving incisions.
Method: 220 patients with clinically suspected PF were analyzed over a 10-year period, with 194 undergoing surgical exploration.
Results: Preoperative imaging (ultrasound or MRI) occured in 95.4% of cases, while 4.6% did not receive any imaging prior to surgery. 62 patients had their fracture sites marked based on radiological findings, and 67.7% demonstrated accurate marking correlated with intraoperative results. Of the patient explored,100 patients had a penoscrotal or longitudinal incision; 12 had a circumferential degloving incision; 5 had a perineal incision; The rest were undocumented.
Conclusions: The penoscrotal incision approach provided adequate exposure while reducing trauma compared to traditional degloving incisions, which, despite allowing broader anatomical access, can compromise local nerve and vascular structures, posing risks to post-operative sexual function and prolonging recovery. The findings underscore the necessity of correlating imaging results with surgical approaches to diminish the reliance on degloving techniques in PF management. Preoperative imaging is recommended to avoid unnecessary surgery and to enhance the recovery of sexual function in patients following PF repair. Limitations in the adoption of this approach may arise from the availability of and expertise among Uroradiologists, warranting further research and implementation strategies to optimise patient outcomes.
P5-8 Off-label tamoxifen plus phosphodiesterase type 5 inhibitor improves outcomes in acute Peyronie’s disease
Mr Charles Katz-summercorn, Mr Abdullah Al-Mitwalli, Mr Mohammad Shah, Mr M Megson, Ms R. Fratangelo, Mr P. Shergill, Mr R. Shahzad, Mr A. Di Giovanni, Mr J. Zhang, Mr James Banerjee, Mr W.G. Lee, Professor D.J. Ralph, Professor S. Cellek
1Whittington Hospital, London, United Kingdom
Introduction: Peyronie’s disease (PD) is a fibrotic disorder of the penile tunica albuginea, commonly presenting with pain, penile curvature and erectile dysfunction. Non-surgical treatment options in the acute phase remain limited. Our previous preclinical studies suggest synergistic antifibrotic effects from combining phosphodiesterase type 5 inhibitors (PDE5i) with selective oestrogen receptor modulators.
Patient & Methods: Men presenting with acute PD were treated with tamoxifen (20 mg twice daily) in combination with a daily PDE5i (sildenafil 50 mg or tadalafil 5 mg). Penile curvature and pain scores were assessed at baseline and after three months. Outcomes were compared with a standard care cohort receiving observation or vitamin E. The treatment group comprised 133 men (mean disease duration 7.1 months), while the comparator group included 26 men (mean duration 7.8 months).
Results: Patients receiving combination therapy demonstrated a significant reduction in penile curvature at three months. No improvement in curvature was observed in the standard care group. Pain scores improved in both cohorts, with a greater reduction seen in patients treated with tamoxifen and PDE5i.
Conclusions: Combined tamoxifen and PDE5i therapy may stabilise or reverse disease progression in acute Peyronie’s disease, improving both curvature and pain outcomes. This represents the first clinical evidence supporting this combination as a potential non-surgical treatment strategy.
P5-9 Mapping the Tumour Immune Microenvironment in Metastatic Penile Cancer
Mr Fowz Azhar1,2,3, Mrs Claire Hart1, Dr Mick Brown1, Dr Diego Sanchez-Martinez4,5, Dr Pedro Oliveira5, Mr Arie Parnham2, Professor Vijay K Sangar2, Professor Noel W Clarke1,2,3, Mr Ashwin Sachdeva1,2
1Genito Urinary Cancer Research Group, The University of Manchester, Manchester, United Kingdom, 2Department of Surgery, The Christie NHS Foundation Trust, Manchester, United Kingdom, 3Department of Urology, Salford Royal NHS Foundation Trust, Manchester, United Kingdom, 4Cancer Research UK Manchester Institute, Manchester, United Kingdom, 5Department of Pathology, The Christie NHS Foundation Trust, Manchester, United Kingdom
Penile carcinoma (PeCa) is a rare but aggressive malignancy, with five-year overall survival falling from 95% in node-negative disease to 35% with advanced nodal involvement. Although immune checkpoint inhibitors (ICIs) show activity in a subset of patients, responses remain inconsistent. Improved characterisation of the tumour immune microenvironment (TME) across disease stages is required to inform rational immunotherapeutic strategies.
Whole formalin-fixed paraffin-embedded sections from primary tumours (PTs) and matched lymph nodes (LNs) were analysed using multiplex immunofluorescence across three optimised panels on the Ventana Discovery ULTRA platform. Each panel combined a single immune checkpoint (PD-L1, CTLA-4, or LAG-3) with lineage-specific immune markers. Multispectral images were acquired using the Vectra 3 system, with single-cell spatial analysis performed in HALO. Statistical analyses were conducted in R (v4.2.1).
Fifty-two matched cases were analysed: N0 (n=21), N1/N2 (n=11), and N3 (n=20). In PTs, LAG-3 expression was significantly higher in node-positive disease than in N0 tumours (8.5% vs 4.2%, p<0.001), while PD-L1 and CTLA-4 expression did not differ by nodal status. Within LNs, LAG-3 expression was markedly increased in metastatic compared with non-metastatic nodes (72% vs 28%). PD-L1 and CTLA-4 expression were enriched in LNs relative to matched PTs. Co-expression analysis demonstrated predominant PD-L1/CTLA-4 overlap in inguinal LNs and PD-L1/LAG-3 overlap in pelvic LNs. Spatial profiling identified enrichment of exhausted T-cell phenotypes and pro-tumourigenic M2 macrophages in node-positive PTs and corresponding LNs.
Advanced PSCC demonstrates a LAG-3-dominant, immunosuppressed TME with compartment-specific immune checkpoint patterns. These findings support spatially informed and combinatorial immunotherapeutic strategies in metastatic PeCa.
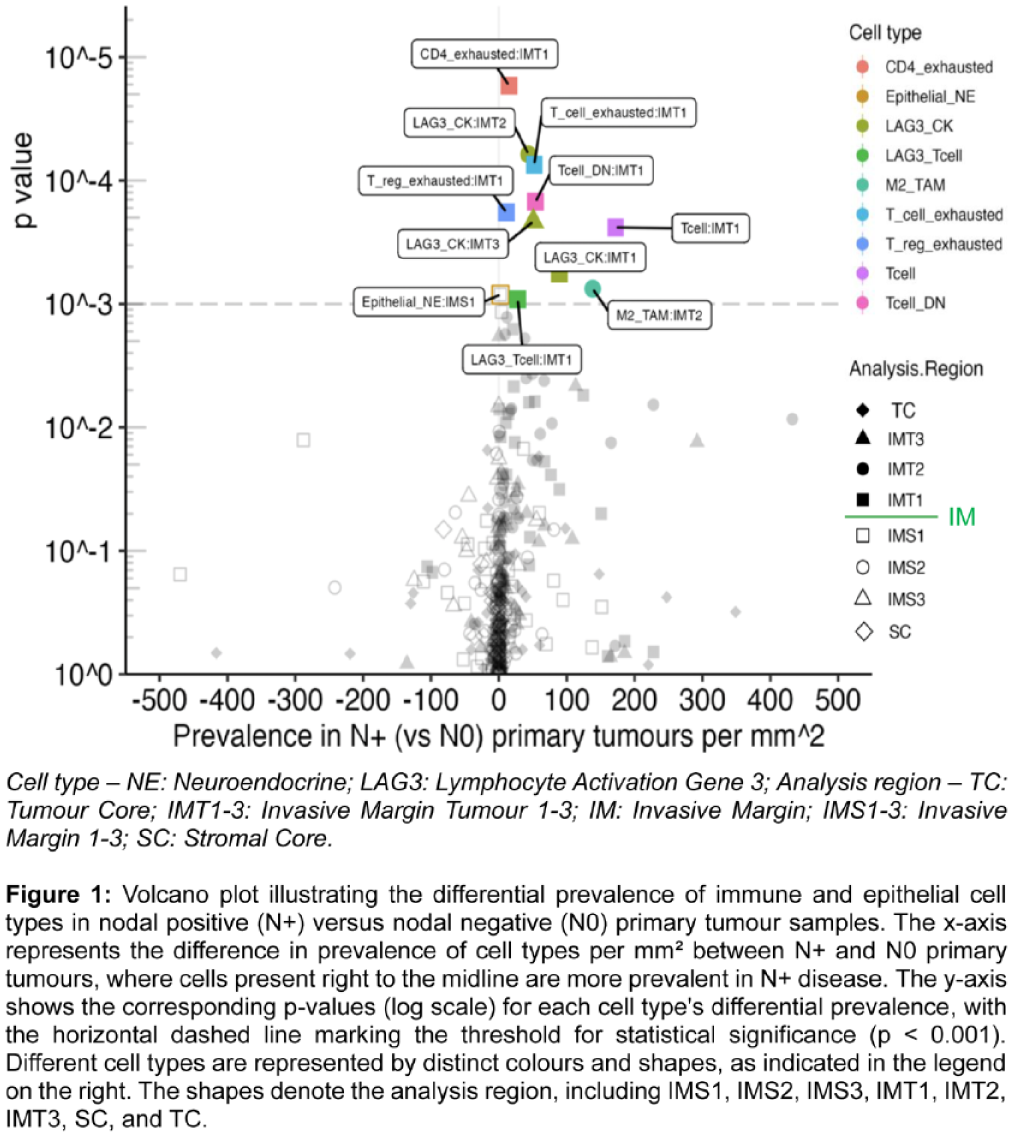
P5-10 Patient satisfaction and outcomes following the insertion of a penile prosthesis in men aged ⩾ 75
Mr Jamie Lindsay1, Professor David Ralph1, Professor Asif Muneer1, Mr Hussain Alnajjar1
1Department of Andrology, University College London Hospitals NHS Foundation Trust, United Kingdom
Objective: To evaluate outcomes and satisfaction following penile prosthesis (PP) implantation in men aged ⩾75 years.
Methods: Patients who underwent PP surgery between January 2020 and January 2025 and were aged ⩾75 years. All patients were assessed postoperatively, with satisfaction recorded at a minimum of six months. A total of 48 patients met the inclusion criteria.
Results: A total of 48 patients underwent penile prosthesis (PP) surgery, comprising 30 primary insertions and 18 revision procedures. The mean age was 77 years, with a mean follow-up of 36 months. 33 (69%) received an inflatable three-piece PP and 15 (31%) a malleable PP.
The aetiology of erectile dysfunction included metabolic syndrome (40%), post-prostatectomy (27%), diabetes (20%), Peyronie’s disease (7%), priapism (3%), and post-TURP (3%). Median ASA grade was 3. Median length of stay was 2 nights.
There was one readmission (2%) within 30 days due to infection, resulting in prosthesis removal (Clavien-Dindo 3b). There were no other readmissions within 30 or 90 days.
Three patients (6%) required subsequent revision surgery for autoinflation, faulty pump and a perceived lack of rigidity of a malleable PP. Overall satisfaction was high at 93% (43/46). Two patients (4%) reported dissatisfaction due to perceived lack of rigidity.
Three deaths (6%) were recorded, all occurring more than 36 months post-PP surgery.
Conclusion: This represents one of the few contemporary UK series evaluating PP outcomes in elderly men. Penile prosthesis implantation in men aged ⩾75 years demonstrated excellent satisfaction and functional outcomes with low complication and revision rates.
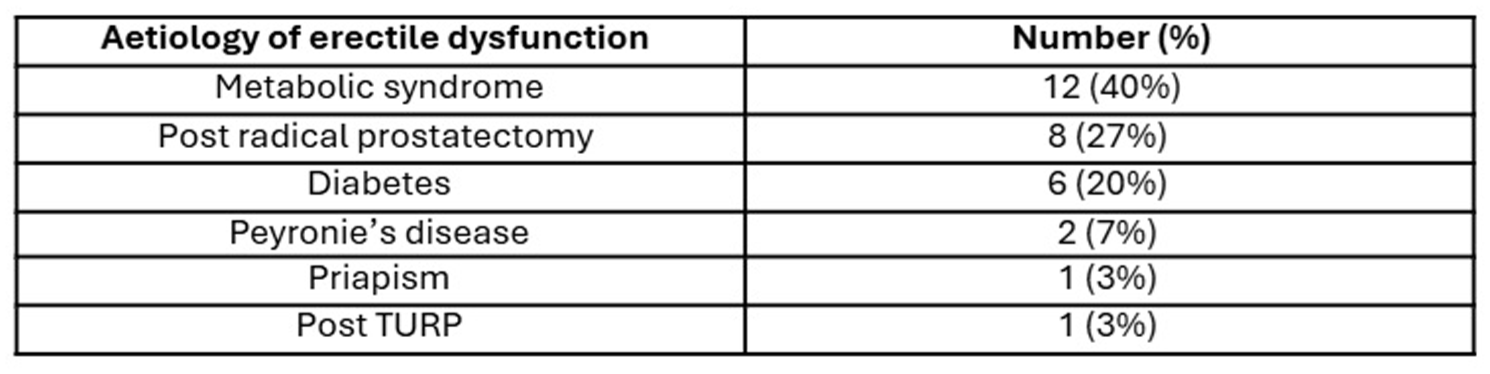
ePoster Session 6: General - Sustainability, Inclusivity, Wellbeing and Healthy Work Environment, Paddy O’Reilly, June 16, 2026, 08:00 - 09:00
P6-1 Clean pulp versus sterile plastic for mid-stream urine collection: a paired equivalence study comparing the microbiological performance of a novel low carbon collection device with the standard of care
Dr Joseph John1, Mr Nick Burns-Cox1
1Somerset Ft, Taunton, United Kingdom
Introduction: Urine collection for testing is an important high-volume urological activity, but which incurs substantial plastic waste. We describe a clinical non-inferiority study and carbon footprint assessment comparing a novel clean pulp urine collection device – the PiP (Pee-In-Pot) – with the standard of care (SOC).
Methods: This prospective, single-centre paired comparison study compared microscopy results for 1353 urine samples, of which 808 paired samples underwent culture. Urine was either decanted directly from a sterile plastic bowl into a boric acid tube (SOC), or via the PiP. The primary outcome was the proportion of positive urine culture results and secondary outcomes were microscopy counts and heavy mixed growth cultures.
Results: Overall, urine cultures were positive in 9.3% (75/808) and 10.0% (81/808) of PiP and control cases respectively. Matching between PiP and control arms for reportable positive culture results was 98.5% (796/808), with a Cohen’s Kappa test coefficient (κ) of 0.9149 (almost perfect agreement). There were no significant differences on subanalysis for specific organisms. For microscopy, there was agreement in meeting culture thresholds for 1308 of 1353 paired samples with a difference in culturing rates of 0.00517 (95% C.I. -0.0045-0.015, i.e. high level of agreement). The estimated base case carbon footprint of PiP testing was 95g CO2e compared to 270g CO2e for SOC testing.
Conclusions: This study found the PiP to be non-inferior for routine urine microscopy and culture testing and to have a lower carbon footprint compared with SOC urine testing.
P6-2 Quantifying carbon and energy savings between prostate MRI protocols
Mr Chengxuan Li1, Mr Nikhil Mayor1, Dr Jasmin Cooper1, Professor Hashim Ahmed, Professor Andrea Rockall1, Dr Onesmus Mwabonje1
1Imperial College London, London, United Kingdom
Introduction: Environmental sustainability across MRI protocols has yet to be established. We aimed to assess the carbon and energy savings of biparametric (bp) compared to multiparametric (mp) MRI.
Methods: We performed a life cycle assessment to quantify the carbon footprint and energy demand of prostate MRI, capturing the full diagnostic process for a single MRI examination, including scanner electricity use, HVAC cooling, consumables, gadolinium contrast, and data storage. Departmental data on scan duration and file size were used, with published emission factors applied for electricity and materials. We compared bpMRI and mpMRI protocols at both varying field strengths.
Results: At 3T, an mpMRI generated 5.9 kg CO₂-eq and required 205 MJ per scan. BpMRI on the same scanner reduced emissions to 4.9 kg CO₂-eq and 173 MJ (-17% carbon, -16% energy). with further reductions at 1.5T, where bpMRI emitted 4.4 kg CO₂-eq and 164 MJ per scan (-25% CO₂-eq, -20% energy versus 3T mpMRI). Implementing scanner power-saving or overnight shutdown policies lowered electricity consumption by 20-30%. PACS data storage was a major contributor: increasing file size from 1.2 GB (typical of bpMRI) to 1.8 GB (mpMRI) increased emissions by 18% per examination.
Conclusions: BpMRI lowers the environmental impact of PCa diagnostics by shortening scan time, avoiding gadolinium use, and producing smaller image files, directly reducing both energy consumption and carbon emissions. Switching from 3T mpMRI to 1.5T bpMRI reduces carbon emissions by approximately one quarter, which is equivalent to the electricity used by an average UK household over five days.
P6-3 Live, Semi-Live, or As-Live Surgery? A Global EAU Endourology and ESU Survey of Surgeons’ Perspectives as Operators, Audience Members, and Hypothetical Patients
Ms Amelia Pietropaolo, BB Martinez, Arman Tsaturyan, Vineet Gauhar, c Bouma - Houwert, Olivier Traxer, Ioannis Kartalas Goumas, E Liatsikos, Eugenio Ventimiglia, BK Somani
1University Hospital Southampton Nhs Foundation Trust, Southampton, United Kingdom
Introduction: Live surgery has long been a cornerstone of surgical education but remains controversial due to concerns over patient safety, ethical justification, and surgeon performance. Semi-live and as-live formats have emerged as potential alternatives. This international survey, conducted under the auspices of the Endourology Sections of YAU and EAU and the European School of Urology (ESU), aimed to capture surgeons’ contemporary views on live surgical broadcasting from three perspectives: operator, audience member, and hypothetical patient.
Methods: A 36-item online questionnaire was distributed to urological surgeons worldwide. The survey comprised three domains: (1) surgeon as operator, (2) surgeon as audience member, and (3) surgeon as hypothetical patient.
Results: A total of 250 surgeons responded, of whom 40% had performed live surgery, 13% semi-live, and 7% as-live demonstrations, while 40% had no such experience. Nearly two-thirds (64.4%) preferred pre-recorded as-live demonstrations over live procedures. If live-surgery guidelines are not followed, there seems to a perception that live surgery might lead to higher risk of complications, potentially compromising patient safety. Most (68%) felt that live demonstrations best reflected real-world scenarios. Semi-live (54%) and as-live (53%) formats were most preferred educationally, ranking higher in overall value than live surgery.
Conclusions: This international survey highlights that while live surgery remains valued for its educational realism, there is growing preference towards semi-live and as-live formats. Undeniably semi-live and as-live formats seem to be growing in momentum. These findings support a balanced approach with all types of surgery having their audiences and preferences.
P6-4 Promoting Inclusivity and Wellbeing in Training: A Survey of Maternity Leave Experiences Among East of England Urology Trainees
Miss Dhanashree Moghe1, M Carey, R Hilbert
1Broomfield Hospital, Mid And South Essex Nhs Foundation Trust, Chelmsford, United Kingdom
Introduction: Urology training is a demanding programme that often overlaps with peak childbearing years. In the East of England deanery, female urology trainees now outnumber their male counterparts (53% vs. 47%). This survey explored the impact of pregnancy and childbirth on urology training, and how these findings informed the development of a regional maternity leave guidance handbook.
Materials and Methods: An anonymised electronic survey was distributed to all female trainees (ST3–ST7) in the east of England deanery between June and September 2025. The questionnaire captured demographics, maternity leave patterns, perceived support, impact on training progression, and family planning decisions.
Results: Most trainees took 9–12 months of maternity leave, with several reporting extensions to training. Trainees highlighted challenges such as demanding on-calls, yearly rotations causing long commutes, and childcare difficulties. Over half (55.6%) reported delaying family initiation due to training pressures, and most indicated concerns of training progression influenced their intended family size. Although overall programme support was rated positively, trainees highlighted inconsistent guidance and limited structural flexibility within rotational training posts.
Conclusions: This survey highlights significant inclusivity and wellbeing challenges faced by female urology trainees who are undertaking or considering maternity leave. The findings emphasise the need for clear, deanery-wide guidance to foster a healthier working environment. These results directly informed the development of a regional maternity leave guidance handbook. It is hoped that these findings will support and encourage the development of comparable guidance across other UK deaneries.
P6-5 Outcomes from a weekly Video Bladder Cancer Scheduling Meeting (BCSM): improved decision making and resource utilisation
Mr James Brittain1, Mr Rustam Karanjia1, Mr Sarosh Janardanan1, Mr Sachin Agrawal1
1Ashford and St. Peter’s Hospitals NHS Foundation Trust, Chertsey, United Kingdom
Introduction: GIRFT recommend outpatient based Local Anaesthetic Transurethral Laser Ablation (TULA) and daycase Transurethral Resection of Bladder Tumour (TURBT) for diagnosing bladder cancer. Decision making is often complex due to an increasingly co-morbid population and inconclusive cystoscopic findings. We report the impact on decision making and resource utilisation of a weekly Bladder Cancer Scheduling meeting (BCSM).
Methods: A 45-minute meeting was conducted weekly for patients booked for TULA or TURBT between June-November 2025. The meeting involved two consultant urologists, a trainee, specialist nurses and the hospital bookings team. Information reviewed included patient history, co-morbidity and cystoscopic video footage. Diagnostic impressions and proposed treatments were ratified or adjusted. Suspected muscle-invasive cases were fast-tracked for TURBT. Videos of indeterminate lesions were reviewed.
Results: 58 cases were reviewed. Median age was 77 [range 52-101]. 31(53%) had previously diagnosed bladder cancer and 18(35%) had prior intravesical chemotherapies or radiotherapy. These cases included 7(12%) patients with solid tumours, 19(33%) papillary and 19(33%) indeterminate lesions. For solid tumours, median time from cystoscopy to TURBT was 13 days [range 6-33] and histology turnaround was 7 days [range 4-14]. Of 19 indeterminate lesions, 8/19(42%) were cancelled or downgraded to repeat cystoscopy with no missed cases of bladder cancer. In total, 22(38%) patients had either booking or management changes made.
Conclusion: A weekly BCSM improved decision making in 38% of cases, reduced unnecessary investigations without compromising oncological outcomes and ensured an efficient pathway for suspected muscle-invasive disease. A standardised proforma has been developed and we recommend its implementation nationally.
P6-6 Patient awareness and attitudes toward the kidney stone Multi-Disciplinary Meeting (MDT): Identifying opportunities for better communication and engagement
Mr John Bose1, Ms Amelia Pietropaolo, Prof Bhaskar Somani
1University Of Southampton, Southampton, United Kingdom
Background: Kidney stone disease (KSD) places a significant burden on healthcare systems, highlighting the need to optimise treatment pathways. Kidney Stone Multidisciplinary Team (MDT) enables collaborative, personalised care through input from multiple specialities. Despite its widespread use, little is known about patients’ awareness or perceptions of the MDT process. This study aimed to evaluate understanding and attitudes toward Kidney Stone MDT and to compare views between individuals with and without a history of KSD.
Methods: An 18-item online questionnaire (multiple-choice and open-ended) was distributed via QR codes to patients attending a urology centre. University ethics approval was obtained (ERGO number: 103105). The survey assessed baseline awareness, perceived benefits, communication preferences, and suggestions for improvement. Responses were analysed descriptively using Microsoft Excel.
Results: A total of 151 responses were collected, 51 (33%) from patients with KSD. Baseline awareness of the MDT was low in both groups (29% KSD vs 34% non-KSD). 54% felt that all KSD patients should be discussed at MDT, and 84% expressed a desire for their own case to be reviewed. 77% believed MDT involvement improves care and represents efficient use of resources (79%). There were no significant differences in perceptions between patient groups.
Conclusion: Patient perceptions of Kidney Stone MDT were consistently positive, with strong support for its role in improving care and resource management. However, low awareness highlights the need for improved patient education. Future work should explore how MDT discussions are communicated to patients and how patient preferences can be better incorporated into shared decision-making.
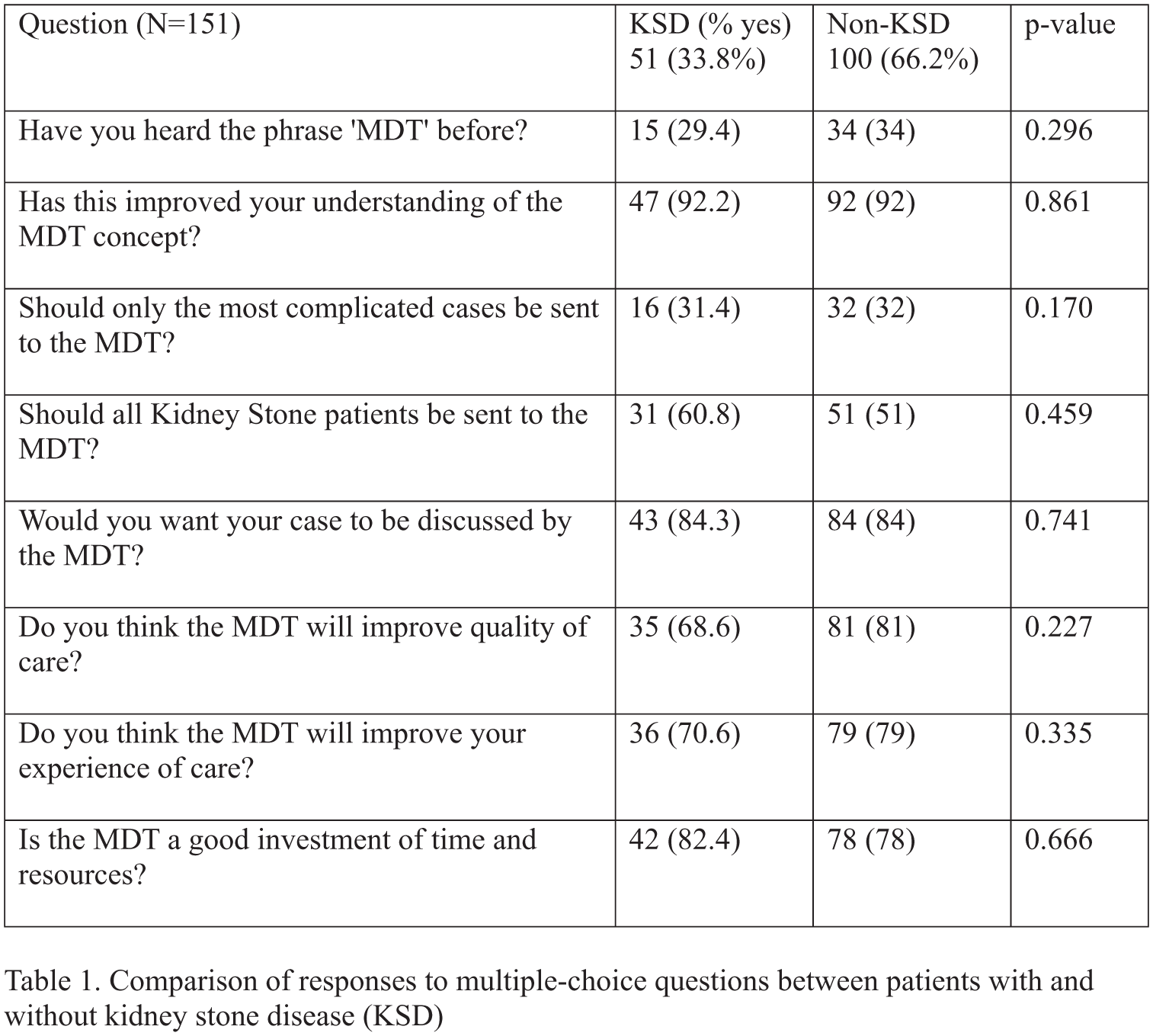
P6-7 High Intensity Clinics
Miss Cara Vincenti1, Dr Karina Laing1, Dr Simon McIntyre1
1Raigmore Hospital, Inverness, United Kingdom
Introduction: Approximately 600 patients were waiting to be seen in our service. To support recovery and meet the national target of having no patients wait more than 52 weeks by March 2026, we secured planned-care funding to trial High Intensity Clinics. The key aims were to reduce waiting times, improve patient experience and enhance clinic efficiency and flow
Patients: We selected penoscrotal conditions as they were common and typically did not require on-the-day investigations such as flow studies or ultrasound. We also developed a standardised proforma to support consistent documentation and decision-making.
Methods: We adopted an A&E-style workflow: three patients were brought in at the same time and the three clinicians saw the next patient when available. To support safe and efficient care, we used pre-assessment questionnaires, standardised consent and BAUS information leaflets. The proforma was uploaded to our online system for accessibility and continuity, and relevant documentation was shared with GPs.
Results: Across the trust, waiting numbers reduced to ~200, supported by this initiative and other running clinic. 137 patients were reviewed in these clinics with outcomes seen in Figure 1. There were 7 DNAs, and 10 slots were left intentionally vacant to accommodate patients who had been booked inappropriately so we did not need to reschedule them.
Conclusions: The High Intensity Clinic model significantly reduced long waits in NHS Highland, helped standardise documentation, and improved patient flow. High intensity clinics can effectively reduce wait times with the aid of a proforma which can improve efficiency and documentation.
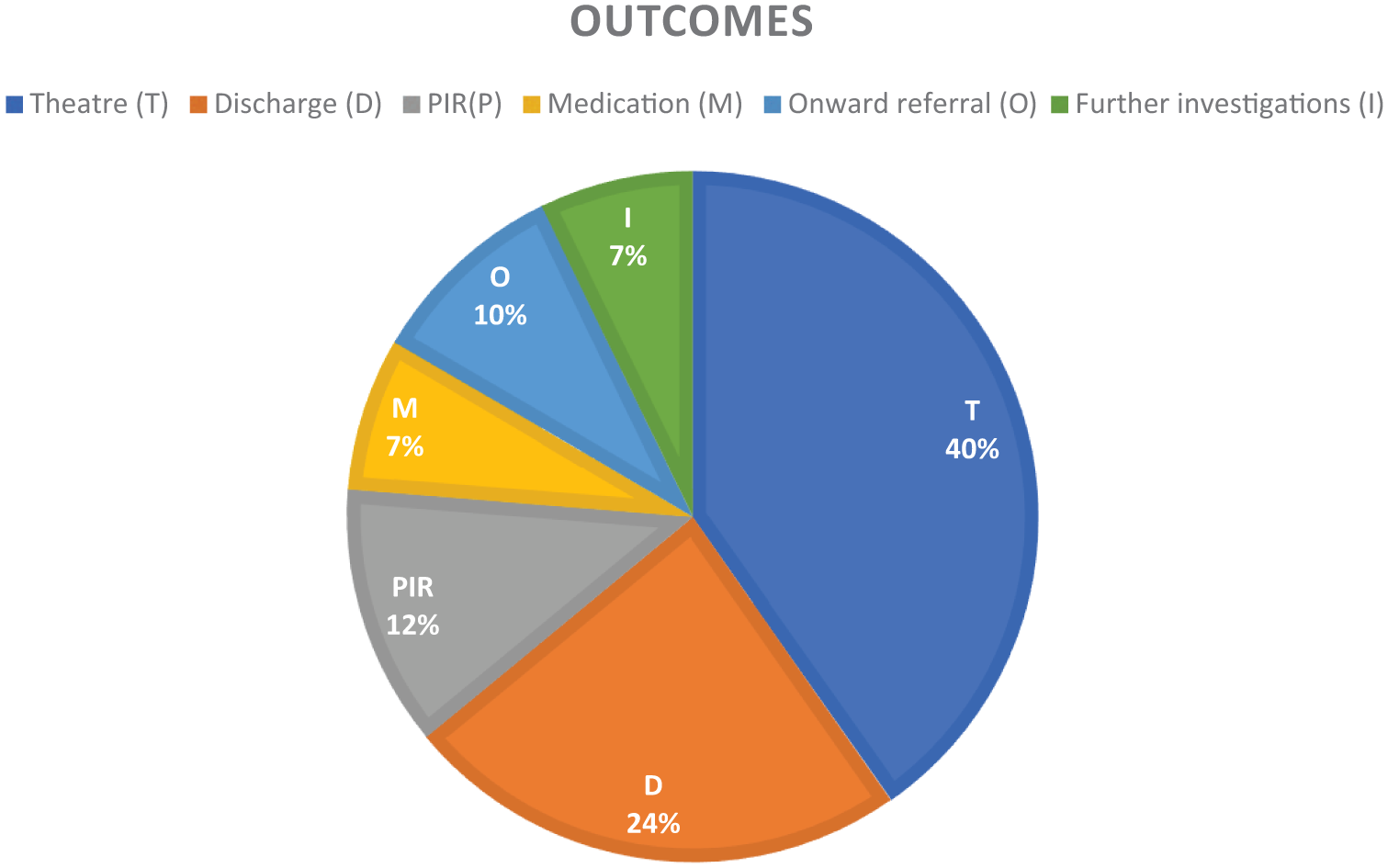
P6-8 Evaluation of the urology specialty training recruitment process, applicant experience, and perceived stress: A national survey
Ms Meghan Coyle1, Ms Kelly Ong, Ms Bushra Abdelqader
1Epsom Hospital, Epsom, United Kingdom
Introduction: Competition for urology specialty training has increased markedly, with competition ratios rising from 2.16:1 in 2016 to 4.64:1 in 2025. Recruitment is coordinated nationally via Oriel, with portfolio scores determining interview shortlisting. In 2025, 34.4% of applicants were invited to interview. Repeated application cycles and increasing uncertainty may contribute to significant psychological stress. This study evaluated applicant experience, recruitment outcomes, and perceived stress among urology applicants.
Materials and Methods: A cross-sectional survey incorporating a 22-item questionnaire including the validated Perceived Stress Scale (PSS-10) was distributed nationally to urology trainees, trust-grade registrars, and senior house officers. Descriptive analyses were performed for recruitment outcomes, applicant experience, and total and item-level PSS scores.
Results: 108 responses were analysed. Overall, 71.9% of respondents secured a training post, 55.6% of all respondents completed multiple application cycles. Portfolio validation issues were common, with 55.6% of respondents appealing point deductions and 31.5% losing points for evidence previously accepted. Thirty-nine respondents reported significant challenges during the application, while only 16 received adequate institutional support.
The mean PSS score was 21.3 (SD 3.0; range 13–32), indicating moderate perceived stress, with 71.3% reporting moderate to severe stress. Highest scoring items reflected feeling nervous/stressed, reduced control over important aspects of life, and feeling overwhelmed, alongside reduced confidence in coping with daily demands.
Conclusions: Urology ST3 applicants experience moderate to severe stress within increasingly competitive and uncertain recruitment processes. Inconsistencies in portfolio scoring and limited support further exacerbate this burden, highlighting the need for transparent recruitment practices and targeted wellbeing interventions.
P6-9 Are We ‘Clicking’ with Informed Consent? A Sharp Look at E-Consent Compliance. Report of audit
Dr Rosa Mancuso
1
1Kingston and Richmond NHS Foundation Trust, London, United Kingdom
Introduction: Consent forms are not merely formalities but vital tools for patient decision-making, requiring time, patience, and clear explanation. In the digital era, are consent processes being rushed, or do they uphold fairness, transparency, and honesty? This audit evaluates whether the electronic consent (e-consent) system implemented in our trust in 2023 meets national standards outlined in the Surgical Good Practice guide (Royal College of Surgeons, 2025).
Materials & Methods: We retrospectively reviewed 30 consent forms for urology procedures from January to July 2024. Ten standards from the SGP national guideline were assessed, focusing on clarity, accuracy, completeness, and documentation of patient engagement.
Results: Clear diagnosis was documented in 66% of cases. Correct procedures were indicated in 96%, but no cases adhered to the mandatory two-week reflection period; all forms were signed on the procedure morning. Patient wishes, goals, and expectations were not recorded in any case. Risk and benefit documentation was thorough in 96% of consents. Only 3% documented patient capacity, and none recorded the patient’s decision process. All forms were signed, with 93% completed electronically.
Conclusions: The e-consent system ensures signature compliance and supports digital adoption, but significant gaps exist in critical areas, including diagnosis clarity, patient deliberation, and preferences. Targeted staff training and allocation of adequate time for consent discussions are recommended. While electronic systems are beneficial, they must balance efficiency with comprehensive, patient-centered informed consent to maintain fairness, transparency, and inclusivity.
P6-10 Model Hospital Data - Is It Reflecting the True Outcome for Our NHS Patients?
Dr Olivia Gemmill1, Dr Suraiya Van den Bos1, Mr Debhias Sarkar1
1Dorset County Hospital, Dorchester, United Kingdom
NHS trusts are increasingly assessed and benchmarked using Model Hospital data, which informs evaluations of productivity and quality. For transurethral resection of bladder tumour (TURBT), the national Getting It Right First Time (GIRFT) standard day-case rate is 44.0%. Model Hospital reports our trust’s day-case TURBT rate as substantially below this benchmark. This audit aimed to establish the true local day-case TURBT rate and compare outcome-based data with Model Hospital reporting.
A retrospective audit of all TURBT procedures performed between 1st October 2024 and 30th June 2025 was completed. Electronic clinical records were reviewed to confirm day-case status and TURBT completion. Local audit outcomes were then compared against Model Hospital statistics.
N= 76 eligible patients. Model Hospital report a day-case TURBT rate of 32.4% (national benchmark 44.0%, peer median 41.5%) In contrast, local outcomes demonstrated a day-case TURBT rate of 50.0% (95% CI 38.7-61.3%), representing a statistically significant difference between day-case rates over the set time period.
Our data shows a discrepancy - we are still exploring why. Possibilities include coding errors, management intent, and data filtering processes. Other NHS trusts should interpret Model Hospital data with caution and audit their own local outcomes to ensure accurate performance reporting, and for the scope of further improvement.
ePoster Session 7: History of Urology, Olympia, June 16, 2026, 08:00 - 09:00
P7-1 The Untold Influence of Marie Antoinette, Queen of France, and Her Sister Maria Carolina, Queen of Naples and Sicily, in the Birth and Rise of Urology as a Medical Specialty
Dr Rosa Mancuso
1Kingston and Richmond NHS Foundation Trust, London, United Kingdom
Introduction: The reigns of Marie Antoinette and her sister Maria Carolina coincided with a period of political upheaval and intellectual transformation that reshaped surgery.This abstract examines how political environments, royal patronage, and personal networks influenced the early development of urology.
Materials and methods: A review of historical medical treatises, Italian and French biographies, and literature was conducted.
Results: In France, the fertility difficulties of Marie Antoinette complicated by the phimosis of Louis XVI, drew public attention to reproductive and urinary health, contributing to early discourse in andrology and urology. The French Revolution catalyzed radical reforms, abolishing the Collegia Medica and establishing hospital-based training.Within this revolutionary context, Jean Civiale, pupil of Souberbielle, played a pivotal role by founding the first department of urological surgery at the Hôpital Necker in Paris. His innovations in lithotripsy, suprapubic lithotomy, and catheter use laid the foundations of modern urogenital surgery.
In contrast, the development of urology in Naples occurred within a more politically controlled and loyalist framework. Deeply affected by her sister fate after the Revolution, Maria Carolina sought to preserve political stability while promoting scientific advancement. Her patronage enabled Michele Troja, connected to the royal court through marriage, to emerge as first Professor of Urology at the Incurabili Hospital in Naples. Troja’s work on flexible catheters and ethical post-operative protocols formalized urology as a distinct academic and clinical specialty.
Conclusions: The intertwined lives of the royal sisters and their contrasting political responses to revolution significantly shaped the birth and institutionalisation of urology in Europe.
P7-2 100 years on: Mapping the past, present and future directions of TURP
Dr Shathar Mahmood1, Ms Helen Stephens1, Mr Michael George2,3, Prof Ian Pearce1,3, Ms Theodora Stasinou1,3
1Manchester University NHS Foundation Trust, Manchester, United Kingdom, 2Stockport NHS Foundation Trust, Stockport, United Kingdom, 3Manchester Andrology Research Collaborative, Manchester, United Kingdom
In 1926, the surgical landscape of urology changed irreversibly with the introduction of the Stern resectoscope – a step that laid the foundation for what would become one of the most effective procedures in urological history: transurethral resection of the prostate (TURP). Today, TURP remains a cornerstone in the surgical management of benign prostatic enlargement. This historical review maps the major milestones in its technical and clinical evolution.
Materials/Methods: A systematic search of electronic databases including original research, historical articles, and literature reviews.
Results: Stern’s original tungsten wire loop resectoscope was refined in the early 1930s by Davis to include a dual-current switch enabling cutting and coagulation, and by McCarthy through improvements in optics and loop control. The identification of the verumontanum as a critical intraoperative landmark further advanced anatomical precision. Doyle and Feggetter reported early clinical success with TURP in patients deemed unsuitable for prostatectomy. Subsequent innovations included Nesbit’s pistol-grip handle, Creevy’s introduction of glycine irrigation, and the Hopkins rod-lens endoscope, with the latter revolutionising image quality. From the 1970s, video-assisted surgery, fibre-optics, and continuous irrigation systems shaped the modern technique. Monopolar TURP became widely adopted in the 1980s, followed by bipolar systems in the early 2000s, improving safety and reducing the risk of TUR-syndrome. The parallel rise of medical therapies shifted TURP’s role towards refractory or catheter-dependent cases.
Conclusion: As TURP approaches its centenary, its ubiquitous worldwide use attests not only to its therapeutic efficacy but also reflects its rich history and remarkable capacity for adaptation and innovation.
P7-3 From “Whispered Symptoms” to Prime-Time Television: British Media Narratives of Prostate Disease and Urinary Incontinence (1950–2025)
Miss Pragnitha Chitteti1, Miss Mehwash Nadeem
1Salford Royal Hospital NHS Foundation Trust, Salford, United Kingdom, 2South Tees Hospitals NHS Foundation Trust, Middlesbrough, United Kingdom
Introduction: Public attitudes to lower urinary tract symptoms (LUTS), benign prostatic hyperplasia (BPH), prostate cancer and urinary incontinence are shaped by cultural constructions of masculinity, stigma, and bodily control. As urology advanced technically, through endoscopy, PSA-era diagnosis, MRI-based pathways and modern functional urology, media language evolved in parallel. This historical review examines how British media representations of prostate disease and incontinence changed and considers its implications for symptom recognition and help-seeking.
Materials and Methods: A structured review was conducted across national newspaper archives, advertising, and NHS/ charity campaigns from 1950- 2025. Primary sources were identified using terms including “prostate”, “prostate enlargement”, “LUTS”, “TURP”, “PSA”, “MRI”, “biopsy”, “incontinence”, “overactive bladder”, “pelvic floor”, and “pads/leaks”. Content was analysed for technical terminology, depiction of interventions/pathways, and stigma framing.
Results: Three phases were observed.
1950–1985: prostate symptoms commonly described as “prostate trouble” or “waterworks”, with euphemistic framing of retention, nocturia and frequency as private decline; incontinence rarely discussed beyond institutional care.
1986–2005: increased procedural visibility (“prostate operation”, TURP-era narratives), and continence product advertising normalised leakage via humour; PSA appeared in mainstream reporting, often simplifying screening versus diagnostic testing and underrepresenting harms/false positives.
2006–2025: campaigns increasingly used anatomically direct and clinically aligned terms (BPH/LUTS; “PSA blood test”, “MRI scan”, “targeted biopsy”), alongside wider functional urology representation, and signposting to rapid-access pathways (Figure 1).
Conclusion: British media progressively shifted from euphemism to urology-specific language reflecting contemporary practice. This evolution informs modern patient communication, expectation management and future public education strategies in LUTS/BPH, prostate cancer and incontinence.
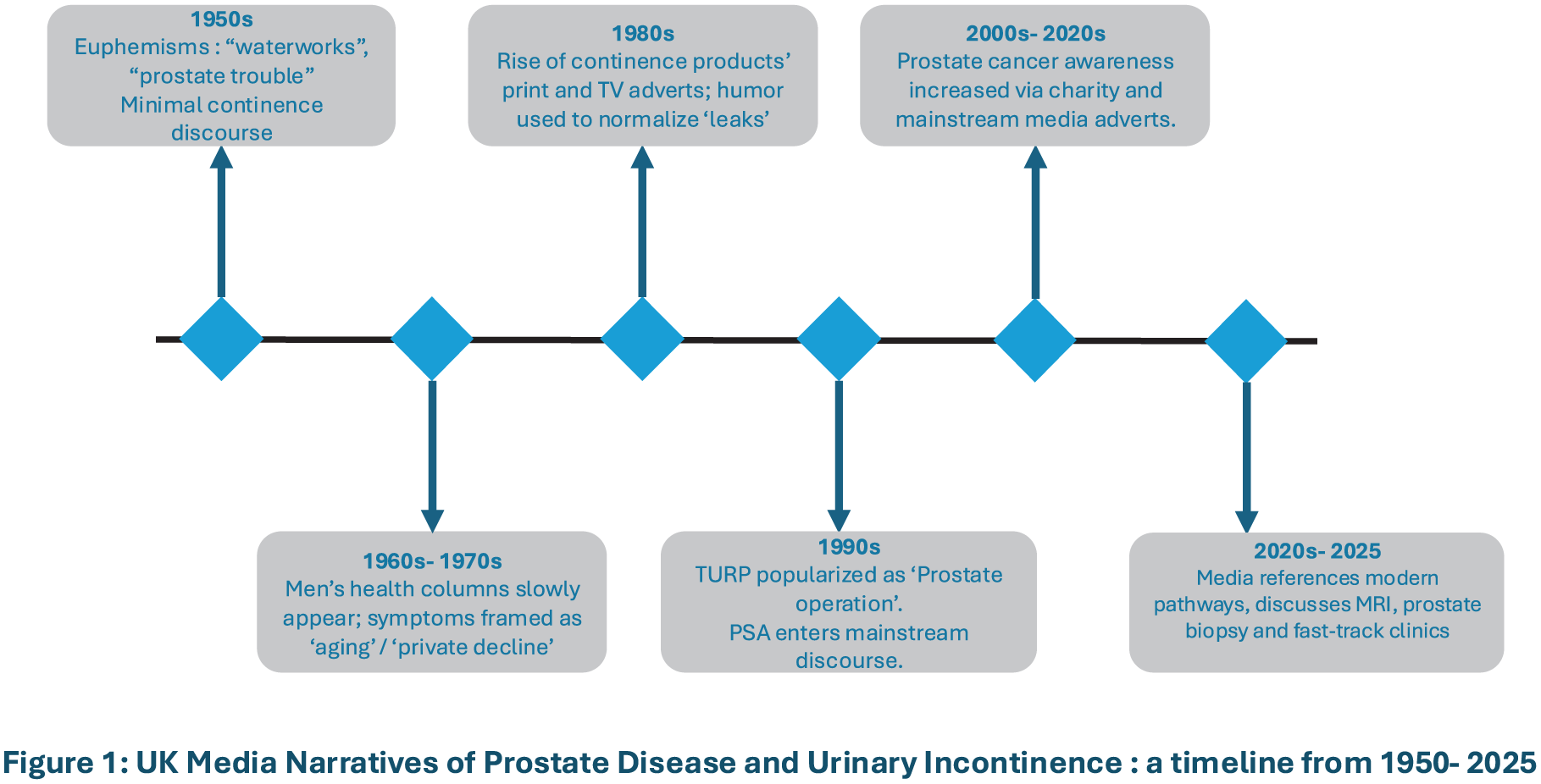
P7-4 Albucasis and The Kitāb al-Taṣrīf: The legacy of a pioneer from the Golden Age of Islamic medicine
Mr Aadam Masood1, Dr Kevin George2, Mr Damiete Harry2, Mr Junaid Masood2
1University of Newcastle, School of Medicine, Newcastle, United Kingdom, 2Barking, Havering & Redbridge University Hospitals NHS Trust, Romford, United Kingdom
Abu Al-Qasim Khalaf Ibn al-Abbas al-Zahrawi al-Ansari, known as Albucasis in the Western world, was an Arab physician, surgeon and chemist. Considered one of the greatest surgeons of the Middle Ages and the “father of surgery” he was born in 936AD in Al-Zahra, close to modern-day Cordoba, capital of Islamic Spain known as Al-Andalus. He held the esteemed position of court physician to Caliph Al-Hakam II.
Published in 1000 AD, his greatest legacy, the 30-chapter “Kitāb al-Taṣrīf”, took over 50 years to complete, including work on surgery, medicine, dentistry, childbirth and pathology. Translated into Latin in the 12th century, it remained the primary source on surgery in Europe for the next 500 years. He depicted over 200 surgical instruments, most of which he invented. Fourteen chapters were dedicated to urology. He founded lithotripsy, describing bladder stone extraction using innovative surgical instruments such as the “michaab” to crush and remove them. He classified the types of stones, their presentation and medical treatment. He advocated the need for surgery in impacted urethral stones and two-stage procedures for complex stones. He meticulously described circumcision using designated scissors, surgery for meatal stricture, and the use of oil-lubricated, smooth silver catheters for managing urinary retention. A passionate educator, he recognised the importance of a good doctor-patient relationship and social equality over nearly 5 decades of practice.
Albucasis’s pioneering work, especially in stone removal, laid a platform for the development of modern urology. Through rigorous documentation and illustration, he bequeathed an invaluable legacy to future generations.
P7-5 From Scalpel to Screen: The First Documented Urological Motion Picture
Mr Rizwan Iqbal1, Ms Kay McGillivray1
1University Hospital Monklands, Glasgow, United Kingdom
Introduction: Wirt Dakin (1883–1975) was past president of the American Urological Association (AUA) and its dedicated historian. Born in Michigan, he completed his medical education at the University of Southern California Medical School. He is widely recognised as the urologist responsible for producing the first documented urology motion picture.
Materials and Methods: A literature review was conducted focusing on Wirt Dakin and the origins of the first urological motion picture.
Results: In 1916, a Hollywood film producer became Mr Dakin’s patient and encouraged Mr Dakin to document a surgical procedure on film. Mr Dakin eagerly embraced this opportunity and selected a young patient scheduled for an open prostatectomy. Due to inadequate lighting conditions within the operating theatre, the procedure was filmed on the rooftop of Los Angeles County Hospital.
Two cameramen were employed; however, one fainted during filming, while the other was found vomiting at the side of the building. Despite these challenges, the actual operation proceeded without complication and the patient survived. The resulting 22-minute film was presented at the 1917 AUA meeting. The film is currently housed at the William P. Didusch Museum in Baltimore where approximately one-third of its original footage has since been restored.
In addition to this remarkable achievement, Mr Dakin authored Urological Oddities, a publication describing unusual foreign bodies encountered within the genitourinary system.
Conclusion: Wirt Dakin is remembered for his leadership within the AUA and his historical contributions to the specialty, as well as for pioneering the first documented urology procedure on film.
P7-6 Arthur T. Cantwell and the Birth of Anatomical Reconstruction in Epispadias Surgery
Dr Dhineshkumar P1, Dr Nitin Kekre1
1Naruvi Hospitals, Vellore, India
Introduction: For much of the nineteenth century, epispadias was viewed as a superficial congenital deformity. Urinary incontinence was considered unavoidable, and surgical treatment was largely cosmetic. There was little understanding of the underlying anatomy of the urethra and corpora. In 1895, Arthur T. Cantwell introduced a new concept that changed how epispadias was understood and treated.
Materials and Methods: A historical review of early surgical literature on epispadias was performed. Cantwell’s original description and subsequent historical publications were analysed.
Results: Before Cantwell, most surgeons believed that continence could not be restored in epispadias. Cantwell was the first to describe epispadias as a problem of anatomical malalignment rather than isolated urethral deficiency. He recognised the dorsal position of the urethra and separation of the corpora as key abnormalities. His operation involved mobilisation and ventral repositioning of the urethra with partial corporal realignment. Although continence outcomes were limited, Cantwell introduced the crucial idea that restoring normal anatomy was essential for functional improvement. This concept influenced later developments, including bladder neck reconstruction and staged epispadias–exstrophy repair.
Conclusion: Arthur T. Cantwell represents a pivotal figure in the history of epispadias surgery. His contribution marked the transition from cosmetic repair to anatomical reconstruction. While continence was not immediately achieved, Cantwell’s ideas laid the foundation for modern continence-focused surgery. His work remains a landmark in reconstructive urology and continues to influence epispadias management today.
P7-7 Tubularised Bladder Flap for Distal Ureteric Reconstruction: Was it really Boari’s Flap?
Miss Amy Hodder1, Miss Isobel Radford2, Mr Iain Wharton1
1University Hospital of Coventry & Warwickshire, Coventry, United Kingdom, 2University of Bristol Medical School, Bristol, United Kingdom
Although Achille Boari (1863-1937) described a tubularised bladder flap in 1894, it was not until 1936 that it became eponymous to him. Nelse Ockerblad (1881-1954), urologist at University of Kansas, operated upon a patient with a ureterovaginal fistula. Her distal ureter was ischaemic and recalling a reference to Boari in Spies, Johnson & Wilson’s work on avoiding ureteric anastomotic strictures (1933) Ockerblad performed a tubularised bladder flap with ureteric anastomosis which he credited to him (Boari-Ockerblad flap).
Boari, urologist in Ferrara Italy, extensively studied ureteric injury. In canine studies he unsuccessfully replaced ureter with carotid artery, trachea and glass tubing. In 1894 he reconstructed a severed distal canine ureter by isolating a bladder flap 5cmx2cm. This was tubularised and anastomosed to proximal ureter. In 1900, Boari summarised his work in “Chirurgia dell’ureter”.
However, one year prior to Boari’s reconstruction Weller VanHook(1862-1918), surgeon at Northwestern Medical School Chicago, published “The Surgery of the Ureters. . ..” (JAMA,1893). This paper significantly advanced ureteric surgery by addressing injuries from operative procedures. VanHook described cutaneous ureterostomy, refinement of uretero-ureterostomy and the creation of a tubularised bladder flap to replace distal ureter. Performed on cadavers, VanHook made two longitudinal bladder incisions, 1.5cm apart. Extended caudally, they were united and the created flap everted, tubularised and anastomosed to proximal ureter.
Ockerblad was unaware of the earlier publication of this practically identical flap even though it was by a fellow american just 500miles from Kansas. Ironically, the flap nomenclature also evolved to be purely “Boari” and Ockerblad’s contribution to this invaluable “rescue” procedure became vastly diminished.
P7-8 Votes for Women!
Ms Oluwabukola Olaitan1, Miss Harriet Poppy Hannaford Goddard2, Mr Jonathan Charles Goddard1
1University Hospitals of Leicester NHS Trust, Leicester, United Kingdom, 2Loughborough College, Loughborough, United Kingdom
Introduction: Charles Mansell-Moullin (1851–1913) was a distinguished British surgeon whose career spanned clinical innovation, medical education, and social advocacy. Educated at Oxford and Bart’s, then Vienna, Strasbourg and Paris on a Radcliffe Travelling Fellowship, he was houseman, assistant chloroformist, surgical registrar and then consultant at the London Hospital until his retirement in 1909.
Methods: Modern and contemporary sources were searched.
Results: He was particularly interested in surgery of the genito-urinary system and was an early pioneer in abdominal surgery. He gave the 1892 Hunterian lecture on The Operative Treatment of Enlarged Prostate, the following book traversed 4 editions. Regarded as a “fine teacher”, he examined at Oxford, Cambridge and Glasgow.
Mansell-Moullin was an avid supporter of women’s suffrage; his wife was a well-known Suffragist. As a doctor he drew attention to the mistreatment of Suffragettes, in particular on the impact of force-feeding on hunger strikes. At the 1913 Epsom Derby, the suffragette Emily Wilding Davison tried to grab the reins of King George V’s horse and fractured her skull. Mansell-Moullin performed emergency surgery on her at the local Cottage Hospital in an attempt to save her; alas she died.
Conclusions: Charles Mansell-Moullin was a pioneer of early British urology and prostatic surgery and should be celebrated for that. But also, and unusually for his era, he was an ardent supporter of women’s suffrage. He co-founded the Men’s League for Women’s Suffrage and publicly condemned the medical consequences of suffragette mistreatment, in particular force-feeding.
P7-9 Claude François Lallemand and the Controversies of Sexual Health Medicine in the 19th Century
Dr Ayaz Khan1, Mr Michael George2, Professor Vaibhav Modgil3, Professor Ian Pearce3, Miss Theodora Stasinou3
1Department of Urology, Royal Bolton Hospital, Bolton NHS Foundation Trust, Bolton, United Kingdom, 2Department of Urology, Stepping Hill Hospital, Stockport NHS Foundation Trust, Stockport, United Kingdom, 3Department of Urology, Manchester Royal Infirmary, Manchester University NHS Foundation Trust, Manchester, United Kingdom
Introduction: Claude François Lallemand (1790-1854) was a French surgeon and professor regarded as a pioneering figure in early urology and sexology. In Des pertes séminales involontaires (1836-1842), he described spermatorrhoea as a serious disorder with physical, psychological, and moral consequences. He identified masturbation as a principal cause of ill health and viewed the foreskin as a source of harmful stimulation, promoting disease. These beliefs informed his preventative medical practices and shaped surgical interventions. This historical review examines Lallemand’s contributions, contextualised within 19th-century medical practice and social norms.
Materials and Methods: Primary texts by Lallemand, contemporary translations, 19th-century surgical literature, and modern historical analyses were reviewed to assess his influence on clinical practice.
Results: Lallemand advocated invasive treatments for spermatorrhoea, including urethral cauterisation and circumcision. Following English translation, his views influenced Victorian medical practice, notably shaping William Acton’s promotion of circumcision to prevent perceived sexual excess. His work exemplifies the medicalisation of morality, reframing behaviours such as masturbation as pathological conditions requiring surgical intervention. Central to his theories was the belief that foreskin anatomy promoted masturbation and subsequent ill health, an assertion not supported by modern evidence. Nonetheless, his work contributed to the integration of circumcision into medical practice beyond religious or cultural indications.
Conclusions: Lallemand remains a significant figure in urological history. Although his practices are not supported today, his work reflects early preventative medicine and highlights the importance of separating moral judgement from evidence-based clinical care.
P7-10 From Undesirable to Undeniable: The History of Methenamine
Mr Saurabh Verma1, Mr Chandran Tanabalan1
1Northampton General Hospital NHS Trust, Northampton, United Kingdom
Methenamine hippurate, introduced in 1895 as a urinary antiseptic, became a conerstone for preventing recurrent urinary tract infections (rUTIs) in the pre-antibiotic era. This review explores its historical trajectory - the rise, decline and resurgence in contemporary urological practice.
A narrative historical review was undertaken using journal articles, early 20th-century reports and contemporary literature addressing methenamine use, antibiotic development and antimicrobial resistance (AMR). Trends in clinical indications, prescribing patterns and mechanistic understandings were examined across pre- and post-antibiotic eras.
In the early 20th century, methenamine was widely adopted for UTI prophylaxis due to its broad, resistance-independent antimicrobial activity. The discovery of penicillin in 1928 and subsequent antibiotic classes led to a rapid decline in methenamine, as antibiotics offered faster symptomatic resolution and broader therapeutic scope. Decades of widespread antibiotic use for rUTIs have contributed to rising antimicrobial resistance (AMR), prompting renewed evaluation of non-antibiotic strategies. Recent trials have demonstrated methenamine to be non-inferior to continuous antibiotic prophylaxis for preventing rUTIs in selected populations, with no associated emergence of bacterial resistance.
Methenamine hippurate represents a rare example of a historical treatment regaining clinical relevance in the AMR era. Its resurgence reflects a paradigm shift towards sustainable infection management and antibiotic stewardship. Understanding its historical evolution provides valuable insight for urologists seeking effective non-antibiotic strategies for rUTI prevention, with the fundamental philosophy of prevention being better than a cure.
ePoster Session 8: TUF - BAUS Best of the Regions, Olympia, June 16, 2026, 10:45 - 11:45
P8-1 Outcomes Following Mesh Excision from a Tertiary Referral Centre
Ms Oluwabukola Olaitan1, Mr Jaskarn Rai1, Ms Pravisha Ravindra1
1University Hospitals Of Leicester Nhs Trust, Leicester, United Kingdom
Introduction: Synthetic mesh was widely adopted from the 1990s for stress urinary incontinence (SUI) and pelvic organ prolapse (POP). Increasing recognition of complications—including chronic pelvic pain, mesh erosion, and recurrent urinary tract infections (UTIs)—has led to reduced use and the development of specialist mesh removal centres. This study evaluates outcomes following mesh excision in a tertiary referral centre.
Methods: A retrospective review identified patients undergoing mesh excision between August 2021 and September 2025 under the urology team at University Hospitals of Leicester. Electronic medical records and clinic correspondence were analysed for presenting symptoms, investigations, surgical management, and postoperative outcomes.
Results: Thirty-one patients underwent mesh removal. Presenting symptoms were overlapping and included pain (n=14), recurrent UTIs (n=11), storage LUTS (n=10), and incontinence (n=15). Mesh removal was performed for erosion in 24 patients and for pain in 7. Procedures included total tape excision (n=5), vaginal/urethral excision with Martius graft (n=13), laser ablation (n=12), and partial arm removal (n=2). Two patients required repeat intervention.
All patients with pain reported symptomatic improvement, though patient-reported outcome measure (PROM) completion was limited. Postoperatively, 21/31 patients developed recurrent SUI. Six patients were diagnosed with POP (four identified at presentation). Postoperative complications included one labial haematoma and one urethral leak requiring further surgery.
Conclusion: In this cohort mesh excision improved pain but was associated with a high incidence of recurrent SUI. Comprehensive preoperative counselling regarding expected outcomes is therefore essential. Routine use of validated PROMs and standardised pain scoring systems would enhance future evaluations.
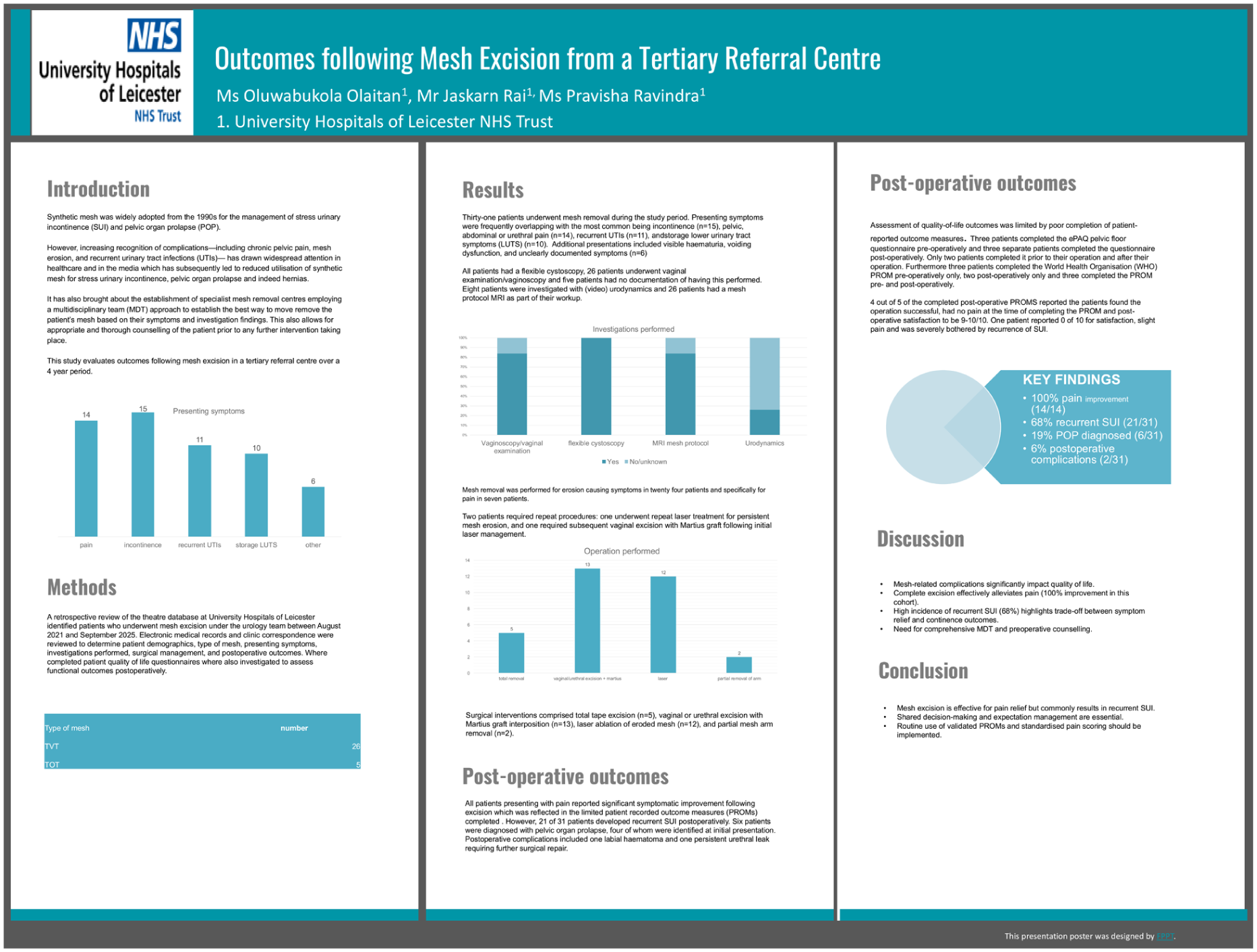
P8-2 Robotic RPLND and Resection of Non-Genitourinary Retroperitoneal Tumours: Exploring Feasibility and Common Surgical Ground in a Specialised Centre
Miss Parthvi Vanalia1, Dr Alberto Costa Silva, Mr Jeremy Oates, Mr Aziz Gulamhusein
1Christie’s Nhs Foundation Trust, Manchester, United Kingdom
Introduction: Urologists are highly familiar with the retroperitoneum through both open and robotic assisted (RA) approaches, raising the question of whether this expertise can be effectively translated to non-genitourinary retroperitoneal tumour surgery.
Aim: To evaluate the feasibility and perioperative outcomes of robotic-assisted resection of selected non-genitourinary retroperitoneal tumours (RA-RTR) performed by urologists with established experience in robotic retroperitoneal lymph node dissection (RA-RPLND), within a specialised centre.
Methods: A retrospective analysis was conducted of all patients undergoing RA-RPLND for testicular cancer and RA-RTR for non-genitourinary tumours between January 2022 and May 2025. Procedures for renal, adrenal and upper tract urothelial malignancies were excluded. All operations were performed using a four-port da Vinci Xi® platform.
Results: Forty-five patients were included: 27 RA-RPLND and 18 RA-RTR. RA-RTR patients were older (median 50 vs. 36 years, p = 0.024). Preoperative tumour size was larger in RA-RTR (56 mm vs. 20 mm, p < 0.001), although specimen dimensions were similar. Operative time was longer for RA-RPLND (143 vs. 90 minutes, p = 0.045). Estimated blood loss (40 vs. 20 mL, p = 0.077) and length of stay (1 vs. 2 days, p = 0.272) were comparable. No conversions or transfusions occurred. Complication rates did not differ (14.8% vs. 5.6%, p = 0.333) and all cases achieved negative margins.
Conclusion: Comparable perioperative outcomes between RA-RTR and RA-RPLND indicate that these surgeries can be performed in specialised centres by urologists experienced in complex retroperitoneal surgery.
P8-3 Penile Fracture Repair: Long-Term Erectile Function, Urinary Symptoms, and Penile Deformity
Mr Abdullah Al-Mitwalli1, Mr M Shah2, Ms B Chua2, Mr M Nasser2, Ms P Sangster2, Mr W.G Lee2, Professor Ralph David2
1South Wales, Cardiff, United Kingdom, 2UCLH, London, UK
Introduction: Penile fracture (PF) is a urological emergency characterised by rupture of the tunica albuginea of the corpora cavernosa, with concomitant urethral injury in up to 15% of cases. Prompt surgical repair is essential to restore anatomical and functional integrity; however, long-term outcomes remain incompletely defined. This study evaluates long-term sexual and urinary function following PF repair, with and without urethral injury, using validated patient-reported outcome measures.
Methods: All patients undergoing PF repair at a tertiary referral centre were contacted and invited to complete the International Index of Erectile Function–Erectile Function Domain (IIEF-EFD) and the International Prostate Symptom Score (IPSS), alongside additional questions on penile curvature. This study was conducted as a registered audit.
Results: A total of 108 men responded (mean age 41±12 years). Imaging was utilised in 96% of cases, predominantly ultrasound. Bilateral corporal injury occurred in 20%, and urethral injury in 27%, all of which were repaired primarily. Mean IIEF-6 and IPSS scores were 25.3±6.5 and 2.9±4.6, respectively. There were no significant differences in erectile function (p=0.49) or urinary symptoms (p=0.29) between patients with and without urethral injury. PDE5 inhibitor use was reported in 15.7% of patients, with no intergroup difference. Penile curvature was reported in 31.5%, typically mild, with one patient requiring corrective surgery. No patients required urethral intervention during follow-up.
Conclusion: Timely surgical repair of PF, including cases with urethral injury, preserves erectile function and is not associated with increased risk of urethral stricture. Penile curvature is relatively common but usually mild.

P8-4 Innovating BPH care: Regional Aquablation launch for large prostates
Ms Vaishnavi Chakravarthy1, Ms Lesley-Ann McCullough1, Mr Ajay Pahuja1, Mr Kenneth Hiew1
1Ulster Hospital, South Eastern Health and Social Care Trust, Dundonald, United Kingdom
Introduction: Access to surgical treatment for large prostates (>80cc) is often limited by operative time and morbidity. We report the outcomes of the first regional Aquablation service in our Urology area network, established to provide equitable access across four Trusts and tackle long-term waiting lists.
Methods: A regional hub was created to centralise referrals. Prospective data was collected on the first 73 patients. The service prioritized regional equity, treating patients from four different Trusts. We evaluated the “learning curve” efficiency and the feasibility of a high-throughput model (5–6 cases/list).
Results: 73 patients were treated (Trust 1: 36; Trust 2: 31; Trust 3: 4; Trust 4: 2). Mean prostate size was 106cc (43–300cc). Pre-operatively, 61.6% (45/73) were catheter-dependent (35 LTC, 10 CISC) and 24.6% had high-pressure chronic retention.
Median wait time was 3 months, but notably addressed backlogs as well. Post-operatively, 94.5% were catheter-free. Median IPSS improved from 21 to 7, and QoL improved from 5 to 2. Despite large volumes, efficiency was high: 34% of cases were completed in <60 minutes. Mean theatre time for the largest glands (>140cc) was 90 minutes. Complications were low: with infections in 5.4% (n=3), take back to theatre 1.37% (n=1), with a 5.4% 30-day readmission rate (n=3) for washout.
Conclusion: This regional model demonstrates that Aquablation can efficiently clear long-term surgical backlogs for large prostates. By operating as a cross-Trust hub, we achieved high-throughput results and excellent functional outcomes, providing a blueprint for future regional urology area networks.
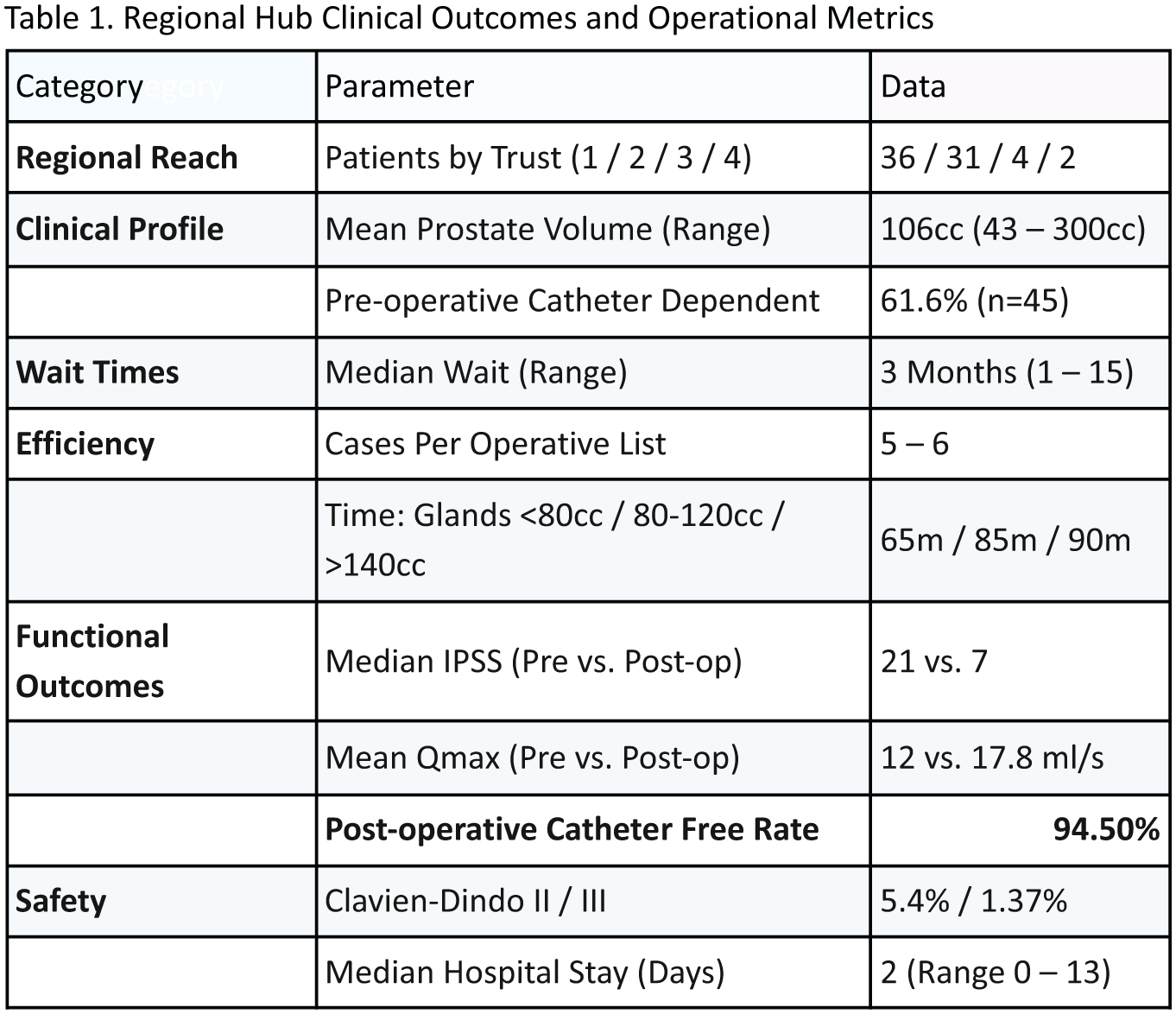
P8-5 A UK national survey; NICE vs EAU guidelines’ adoption, consistency and usability in low/intermediate risk NMIBC groups
Mr Youssef Ibrahim1, Mr Luis Ribiero, Mr John O’Kelly, Dr Mohammed Gad, Mr Adham Ahmed, Prof Shamim Khan, Mr Ramesh Thurairaja, Mr Raj Nair, Ms Elsie Mensah, Ms Yasmin Abughanem
1Guys Hospital, London, United Kingdom
Objectives: To evaluate current patterns of guideline adoption for low-and intermediate-risk non–muscle-invasive bladder cancer (NMIBC) in the UK and to assess clinicians’ ability to apply their chosen guideline consistently to real-world clinical scenarios.
Methods: UK-wide, cross-sectional survey was distributed to clinicians involved in NMIBC management. Respondents reported unit-level and personal guideline adoption (NICE vs EAU) and completed three case-based scenarios derived from real NMIBC cases with discordant risk stratification between guidelines. Cases were randomly selected from a local database using a computer-generated random number function in Microsoft Excel. Concordance between respondents’ decisions and their stated guideline was assessed for risk stratification and surveillance duration. Categorical variables were compared using χ² or Fisher’s exact tests.
Results: Total of 174 eligible responses were analysed. Units most commonly recommended NICE guidelines (38%), whereas individual clinicians most frequently reported following EAU guidelines (39%). NICE-followers demonstrated significantly higher concordance with guideline-recommended surveillance duration than EAU-followers (78.9% vs 49.2%, p<0.001). Deviations among NICE-followers predominantly reflected longer surveillance, while EAU-followers frequently adopted shorter-than-recommended follow-up (p<0.001). Consistent guideline-based risk stratification across case scenarios was achieved in 77.1% of NICE-followers compared with 34.1% of EAU-followers (p<0.001). Acceptable recurrence risk at discharge did not differ between guideline groups (p=0.278).
Conclusions: Substantial variation exists in NMIBC guideline adoption and real-world application in the UK. NICE guidance was associated with greater consistency and usability compared with EAU guidance for low- and intermediate-risk disease. These findings highlight the need for clearer, unified recommendations to promote equitable care and rational use of surveillance resources.
P8-6 Diagnostic approach and post-operative outcomes for patients with upper tract urothelial carcinoma undergoing radical nephrouretectomy at Sheffield Teaching Hospitals
Miss Samantha Conroy1, Dr Amy Stuart1, Dr Leah Mangham1, Mr Altaf Mangera1, Mr David Yates1, Miss Beverley Wilkinson1, Mr Marcus Cumberbatch1, Mr Neil Oakley1, Mr Christopher Hillary1
1Sheffield Teaching Hospitals, Sheffield, United Kingdom
Introduction: Upper tract urothelial carcinoma(UTUC) is an aggressive cancer, requiring timely and accurate diagnosis and management. Radical nephroureterectomy(RNU) is the surgical standard of care, but no consensus exists on optimal pre-operative diagnostic approaches. Here, we review diagnostic pathways and post-operative outcomes for RNU patients, at our institution.
Patients and Methods: At Sheffield Teaching Hospitals, we retrospectively reviewed case notes for consecutive patients undergoing RNU between 2018-2024(n=173). Exclusion criteria included: benign indication(n=6), non-UTUC pathology at RNU(malignant=10 and benign=7), concurrent cystectomy(n=27), previous positive margin(n=1), and bilateral UTUC(n=2). Primary outcomes included: time from imaging to RNU; use of pre-operative ureteroscopy(URS); time from imaging to RNU in URS and non-URS cohorts; post-operative Mitomycin-C(MMC) instillations; adjuvant chemotherapy referrals; and oncological outcomes.
Results: In total, 120 patients were included. The median(IQR) age was 73(68-77)years and 79(65.8%) were male. Prior or synchronous bladder cancer diagnosis was identified in 29(24.2%) patients. Median(IQR) follow-up was 19(10-38) months. Median(IQR) time from imaging to RNU was 120(77-173) days. A total of 51(42.5%) patients underwent pre-operative URS, leading to significant delays from imaging to RNU(158(120-193) vs 91(60-144) days, URS v non-URS, Mann Whitney-U, p<0.0001); there was no significant difference in oncological outcomes. Only 10.8%(10/93) of eligible patients received peri-operative MMC. Of the patients with pT2 UTUC, 52.8%(28/53) were referred for adjuvant chemotherapy.
Conclusion: In this retrospective, single-centre study, pre-operative URS significantly delayed time from imaging to RNU, but did not impact on oncological outcomes. Potential benefits/harm of URS within the UTUC diagnostic pathway requires further evaluation, and a standardised pathway agreed.
P8-7 Smart BPH Tool
Mr Mohammed El Bahnasawi1, Mr Toby Page1
1Freeman Hospital, Newcastle Upon Tyne, United Kingdom
Aims: This study aimed to design and implement a smart digital BPH decision aid tool to support shared decision-making, aligning patient priorities with the most suitable BPH treatment options.
Methods: A web-based tool was created with feedback from patients and BPH clinicians. Users asked to prioritise five outcomes—recovery time, sexual function, time to catheter-free status, durability of procedure and flow improvement—using a Likert scale (1–5). Responses were analysed by computer algorithms to recommend the closest matching surgical intervention, with alternative options also presented. At the end of consultations, both patients and clinicians provided feedback on satisfaction and usability of the tool.
Results: Clinician feedback has been positive across the board on the useability and the potential of this digital tool. It addresses a gap in BPH counselling not fulfilled by paper decision aids. Early patient feedback demonstrated better understanding of their surgical options, greater engagement during consultations, and improved knowledge retention. Feedback was highly positive, with suggestions to expand the platform to include outcome recording, auditing, and long-term data collection. Further plans to publicise tool through BAUS website.
Conclusion: The smart BPH decision aid tool enhanced patient-centred decision-making by aligning treatment choices with individual priorities. It improved satisfaction and confidence for both patients and clinicians with potential to streamlining consultations. With further development, the tool is capable to evolve into a comprehensive electronic BPH diary, supporting long-term monitoring and outcomes research. Further piloting across multiple sites is planned for validation and Quality improvement.

P8-8 The Burden of ketamine on the NHS. An ever growing K hole
Mr Joel Corkill1
1Royal Bournemouth Hospital, Bournemouth, United Kingdom
Introduction: Increasing numbers of patients are presenting to Urology secondary to complications from taking ketamine. Long term abstinence is a challenge meaning management can take up vast amounts of NHS resources. We aimed to add to the evidence base of this by providing a snapshot of patients seen in our centre.
Methods: Retrospective analysis was performed of clinics from the last three years for patients referred with ketamine bladder. Furthermore any patient presenting to the acute take in 2025 with symptoms secondary to ketamine (not previously seen in clinic) were also included.
Results: 26 patients were identified of which 20 were male and 6 female.
Treatments provided included: medication, intravesical instillations, cystoscopy and hydrodistension and/or botox and complex surgical. (Of these, 4 patients underwent a cystectomy and neobladder while 1 a cystoplasty).
46% of the patients had an impairment in GFR while 58% had evidence of hydronephrosis.
There were 64 emergency admissions in the population contributing to a total of 226 days in hospital. The mean days spent in hospital as an emergency admission per patient was 9.
Assessing costs of treatment using data from NHS England the total cost of nights in hospital for this population was £89,270 while the cost of treatment was £88,549.
Conclusion: Ketamine bladder is placing a large burden on hospital resources through repeated admissions and costs of treatments. Further research into outcome and abstinence measures are required, especially following surgical intervention to assess whether this is the optimal way to approach these patients.
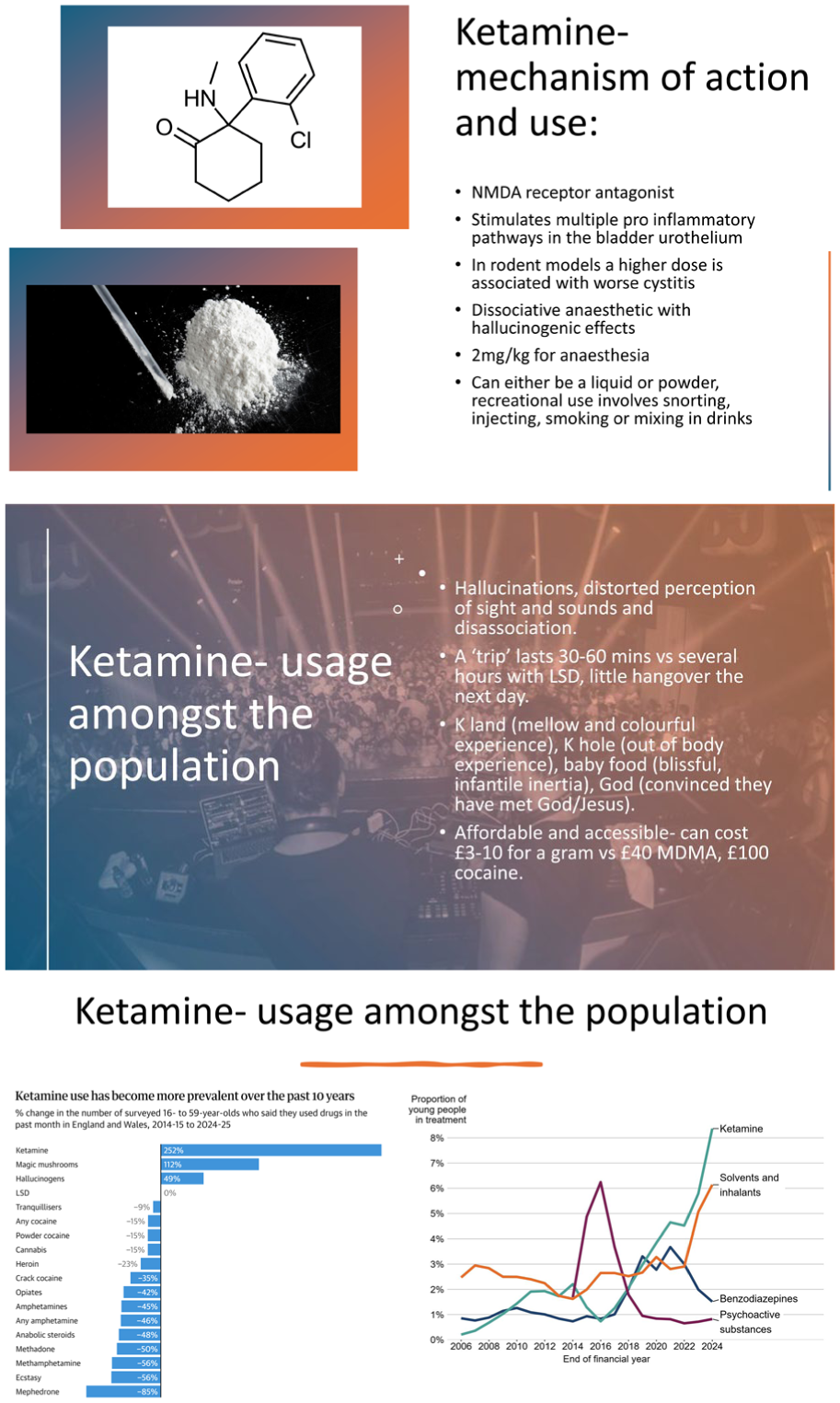

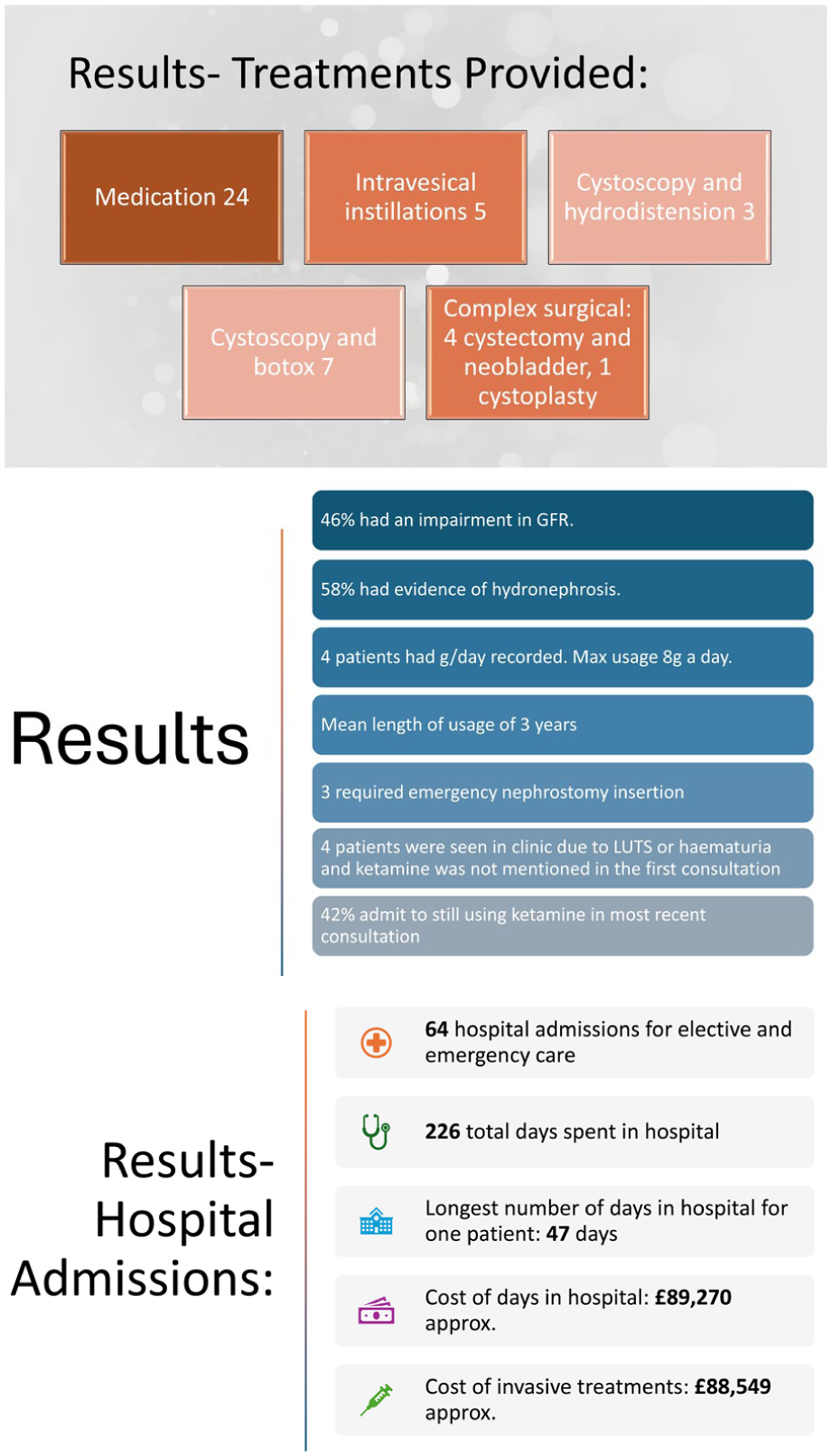

P8-9 Characterisation of the Mechanical Properties of Human Ureter and their implications in Ureteral Stricture Disease
Ms Sorcha O’meara1,2,3, Dr. Eoghan Cunnane6, Prof. Fergal J. O’Brien5, Prof. Niall F. Davis3,4
1St. Vincent’s University Hospital, Dublin, Ireland, 2Strategic Academic Recruitment Programme (StAR), Royal College of Surgeons of Ireland , Ireland , 3Dept. of Urology, Blackrock Health, Ireland, 4Dept. of Surgery, Royal College of Surgeons of Ireland , Ireland, 5Tissue Engineering Research Group, Royal College of Surgeons of Ireland, Ireland , 6Dept. of Engineering , University of Limerick, Ireland
Introduction: Management of ureteral stricture disease (USD) depends on the extent and site of stricturing, with buccal mucosa the gold standard autologous graft. We aim to characterise the mechanical properties of human ureter and buccal mucosa for the management of USD, including the design of tissue engineered alternatives.
Methods: Human ureter was collected from human adults at the time of radical nephrectomy (REC22/20). Tissue was subjected to uniaxial mechanical strength testing to evaluate tensile strength (UTS), elastic modulus (EM) and suture retention force (SRF). Mechanical testing was performed in porcine buccal mucosa and ureter. Finally, a tissue engineered ureteric graft alternative was developed and underwent mechanical and biocompatibility testing.
Results: Human ureter is anisotropic with testing in the longitudinal direction demonstrating a greater UTS (652.9±940.1kPa vs 562.5±857.5 kPa, p=0.08) and EM (3316.8±5189.1kPa vs 1869.5±3056.9, p=0.27) compared to circumferential direction. Porcine buccal mucosa is isotropic, and demonstrates significant variation in UTS and EM when compared to porcine ureter. A novel ureter tissue alternative demonstrated comparable mechanical properties to human ureter, with the ability to support cell activity.
Discussion: This work contributes to the understanding of the mechanical properties of human ureter and the factors that may contribute to USD. Our results provide a benchmark for the development of tissue-engineered alternatives for human ureter.
P8-10 Comparative performance of the CamPROBE double freehand LA transperineal biopsy device versus in line guides for detection of significant prostate cancer
Ms Hannah Thorman2, Mr Saiful Miah1, Mr Syed Shah1, Professor Vincent Gnanapragasam1, Mr Adham Ahmed2
1Cambridge University Hospitals, Cambridge, United Kingdom, 2West Suffolk Hospital, Bury St Edmunds, United Kingdom
Introduction: The CamPROBE double freehand device offers a versatile alternative to current devices for local anaesthetic transperineal (LATP) prostate biopsies. Here we present a 2-centre audit of its performance for LATP biopsies.
Methods: The outcomes of 3 surgeons who adopted the CamPROBE device in 2 units were compared to a retrospective series of biopsies using the Precision Point (PP) device from June-December 2024. Primary outcomes were first biopsy significant cancer detection rates (⩾GG2 or ⩾CPG2) and biopsy target positivity.
Results: Data from 105 PP and 107 CamPROBE procedures were compared of which 96/105 (91.4%) and 87/107 (79.3%) were first biopsies respectively. All were done with cognitive image guidance including sectoral +/- target sampling. There were no significant cohort differences in pre-biopsy age, PSA, T stage or PIRAD 4-5 lesions. Significant cancer (⩾GG2) yields from first biopsies was 56/96 (58.3%) with the PP device and 59/87 (67.8%) using CamPROBE (p=0.18). Target biopsy positive rates were 52/83 (62.6%) with PP and 52/70 (74.2%) using CamPROBE (p=0.12). Overall detection of ⩾CPG2 disease was 61/96 (63.5%) with PP device and 60/87 (68.9%) using CamPROBE (p=0.43). Similar results were found when active surveillance re-biopsies were included. Per device costs were £47 for CamPROBE versus £200 for PP. Median LA use was 16 mls for CamPROBE.
Conclusion: This data demonstrates the real-world efficacy of the CamPROBE device for LATP biopsies, offering comparable cancer detection and target positive rates to in-line devices, with reduced costs and LA usage.
P8-11 Time is Testicle: A retrospective look at regional urological service scrotal exploration rates
Dr Rebecca Watson1
1University Hospital Ayr, Ayr, United Kingdom
Introduction: Testicular torsion, as a urological emergency is recommended to be surgically explored within 4-8 hours of onset of symptoms. This represents a multitude of challenges including theatre and surgical availability. However, regardless of these, patient presentation following onset of symptoms can often dictate the clinical course. Delayed torsion symptom presentation resulting in orchidectomy has been found to be associated with reduced socioeconomic status and health literacy. This retrospective study looked to analyse scrotal explorations conducted between October 2022 - 2025 in NHS Ayrshire and Arran hospitals for possible torsions, and their outcomes.
Method: Data was collected from OPERA in both sites, using Scrotum/Scrotal as keywords for coding between October 2022 and October 2025 inclusive. 83 cases were identified, and records screened as per inclusion/exclusion criteria. Only scrotal explorations to rule out torsions were included, and 27 patients identified and their deprivation demographics collected.
Results: From 27 patients identified with a mean age of 19.1, 15 (56%) of these were identified as true torsions. 5 of these patients had salvageable testes and underwent bilateral orchidopexy, with 10 undergoing orchidectomy due to unsalvageable testes. For all patients explored, the average time from onset of symptoms to initial presentation was 24 hours. Within the true torsion group the average presentation time was 28 hours after onset of symptoms. Those in the higher decile of income presented exclusively within 8 hours.
Conclusion: Delayed presentation rates of testicular pain appear to correlate with a higher rate of deprivation within NHS Ayrshire and Arran.
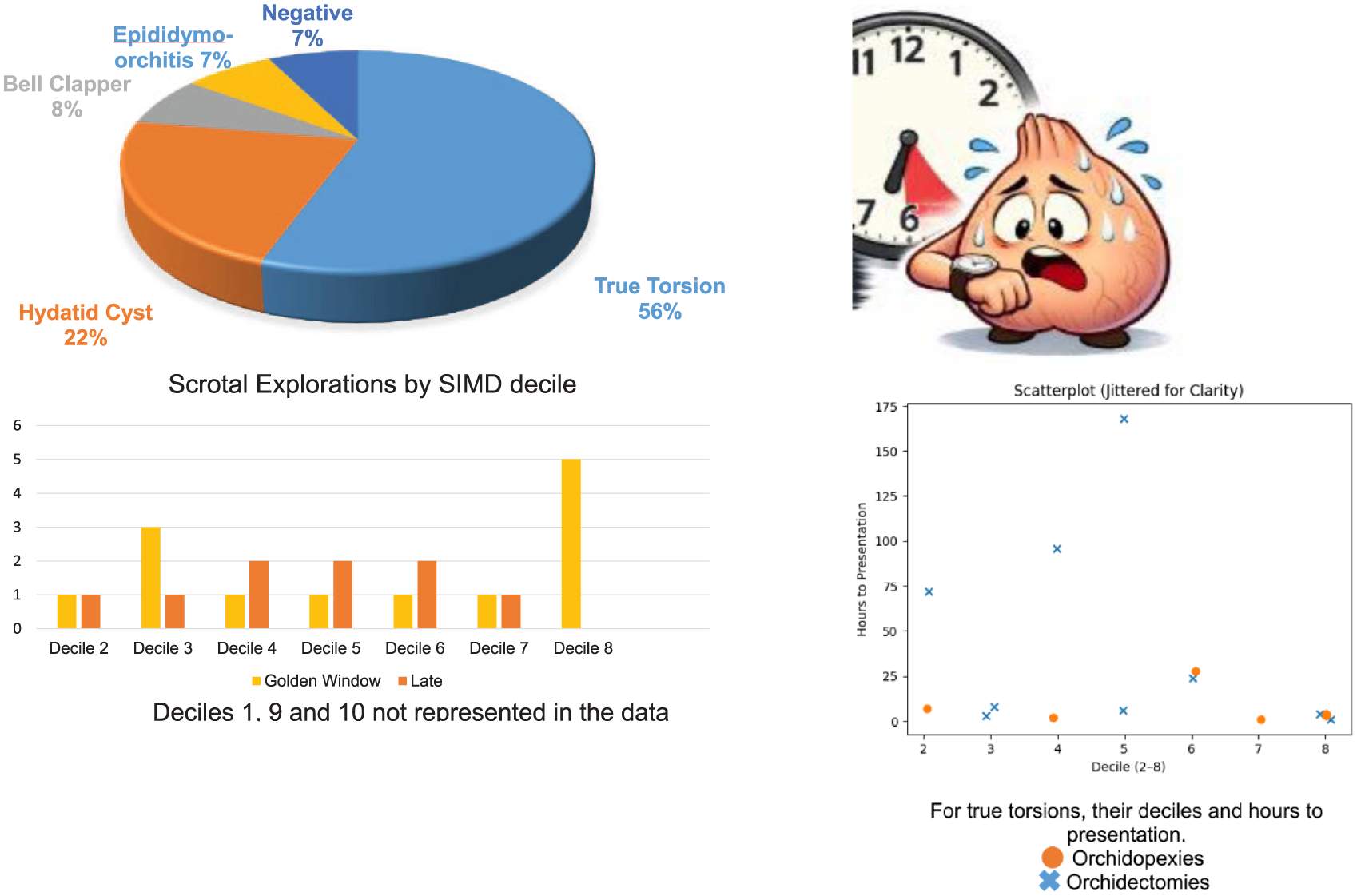
P8-12 EORTC Risk-Matched Long-Term Outcomes of Outpatient Transurethral Laser Ablation for NMIBC
Mr Kohei Yamada1, Dr Nicole Lim1, Mr Zelig Ho1, Dr Faria Antara1, Dr Vaishnavi Bose1, Dr Salman Anwar1, Miss Hira Sayed1, Mr Sachin Agrawal1
1St. Peters Hospital, Chertsey, United Kingdom
Objectives: To evaluate long-term recurrence, progression, and survival outcomes of NMIBC managed with outpatient TULA, benchmarked against EORTC risk-matched predictions.
Patients and Methods: A retrospective cohort study was conducted of patients undergoing outpatient TULA for NMIBC at a single centre between January 2017 and December 2024. Patients were stratified into EORTC recurrence and progression risk groups at index TULA. Primary outcomes were recurrence-free survival (RFS) and progression-free survival (PFS); secondary outcomes included overall survival (OS), cancer-specific survival (CSS), and predictors of recurrence and progression.
Results: A total of 388 patients (mean age 75.7 years; mean Charlson Comorbidity Index 6.6) underwent 1,021 TULA procedures over a mean follow-up of 36.3 months. Overall 1- and 5-year RFS were 69.9% and 41.3%. Five-year PFS was 94.2%; observed progression rates in the high- and very high-risk groups were substantially below EORTC estimates. Five-year OS and CSS were 63.5% (95% CI 57.5–70.2%) and 93.1% (95% CI 89.7–96.7%) respectively. Of 104 deaths (26.8%), only 16 (4.1%) were attributable to bladder cancer. On multivariable analysis, EORTC recurrence risk group was an independent predictor of RFS and EORTC progression risk group independently predicted PFS; age, sex, and comorbidity were not independently associated with either outcome.
Conclusion: TULA provides durable oncological control for NMIBC, with recurrence and progression outcomes broadly consistent with EORTC standards. Bladder cancer-specific mortality was low and largely confined to patients managed with palliative intent, supporting TULA as a safe management strategy for elderly and comorbid patients across a broad risk spectrum.
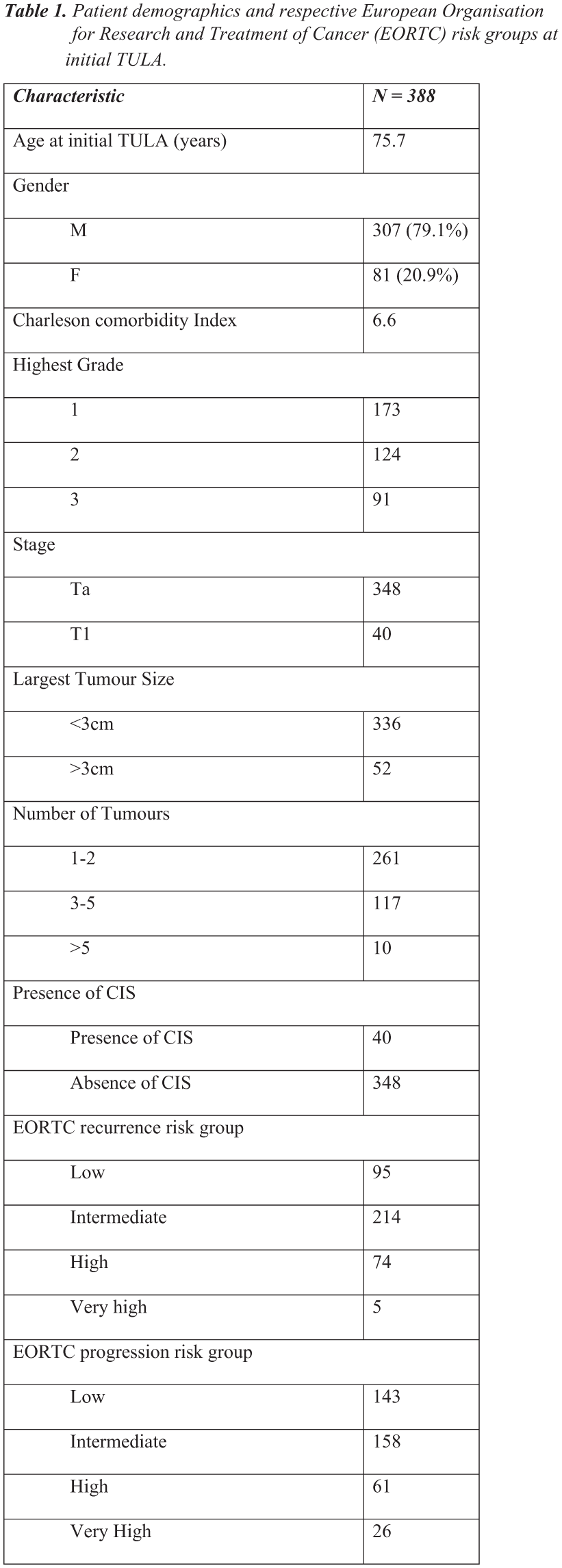
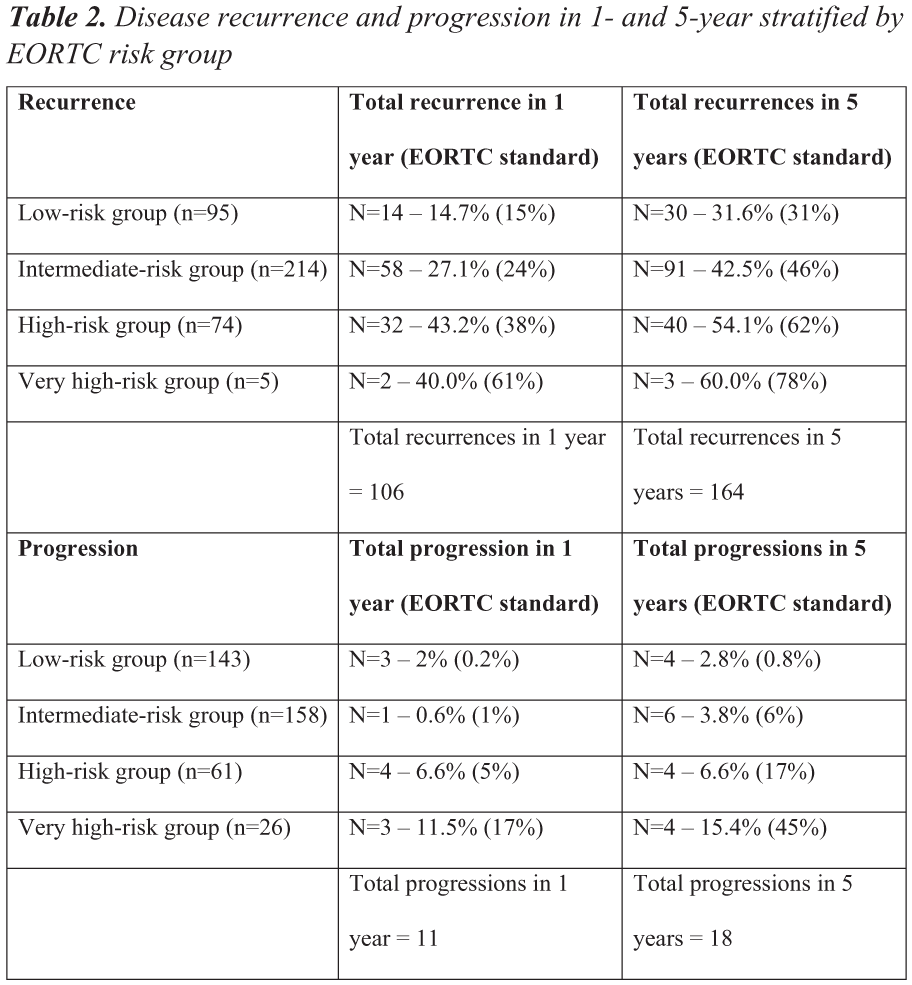
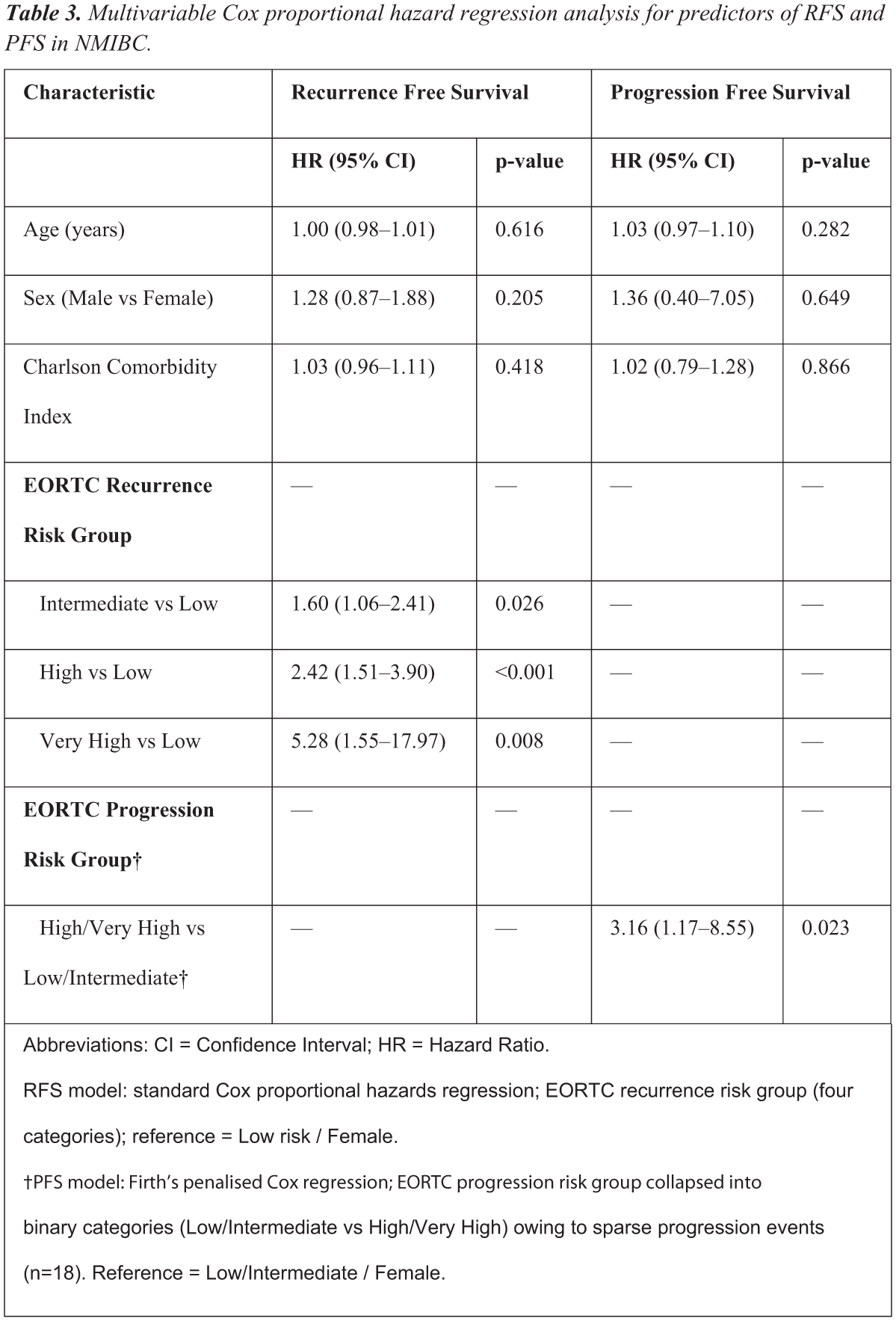
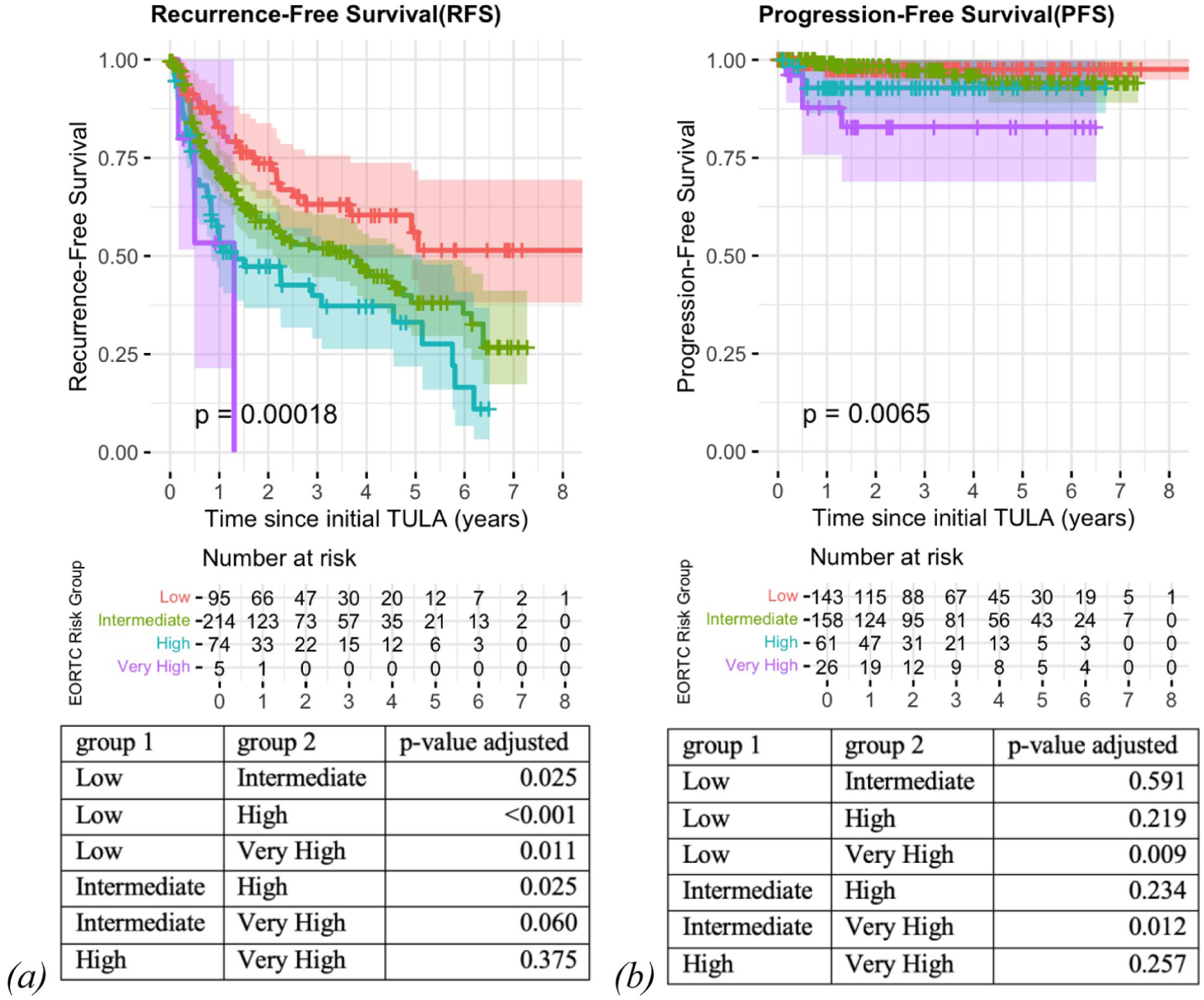
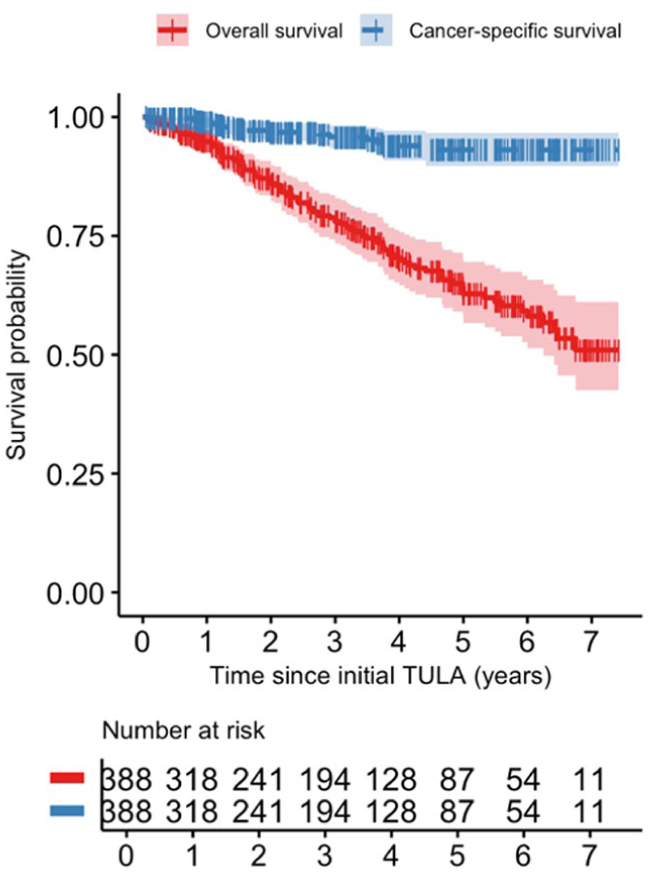
P8-13 Surgical Outcomes and Risk Factors in Clean Scrotal Operations: A Retrospective Cohort Study
Mr Ko Ko Zayar Toe1, Miss Rachel Ball1, Dr Arif Baluch1, Mr Abhilash Cheriyan1
1Aberdeen Royal Infirmary, Aberdeen, United Kingdom
Introduction: Clean scrotal surgery is generally regarded as low risk, yet reported postoperative morbidity varies and contemporary real‑world UK data are limited. We evaluated outcomes following clean scrotal surgery and explored associations with metabolic comorbidity and peri‑operative antibiotic prophylaxis.
Materials and Methods: Retrospective cohort study at Aberdeen Royal Infirmary(Apr 2024–Jun 2025). Included benign clean scrotal operations (hydrocele repair, epididymal cyst excision and orchidopexy). Excluded contaminated emergency cases and procedures requiring inguinal access. Data were extracted from anaesthetic and peri‑operative electronic records. Primary outcome was postoperative complication requiring additional attendance. Variables included age, BMI(BMI⩾30), diabetes mellitus(DM) and prophylactic antibiotic use.
Results: Ninety‑five patients were included (n=95). Overall complication rate was 13/95(13.7%). Haematoma was most frequent(6.3%), with other complications including infection/abscess(~3%) and recurrence(~2%). Prophylactic antibiotics were administered in 35/95(36.8%). Complications occurred early (median 11 days, IQR 6–24; timing available for 12/13). BMI was recorded in 85/95; complications were higher with BMI⩾30(10/35 [28.6%]) than BMI<30(3/50 [6.0%]), OR 6.27. Complications were higher in DM (3/7 [42.9%]) than non‑DM (10/88 [11.4%]), OR 5.85. Antibiotics were associated with lower complication risk (2/35 [5.7%] vs 11/60 [18.3%]), ARR 12.6%, NNT≈8; benefit appeared greatest in obese and diabetic subgroups (small numbers).
Conclusion: Clean scrotal surgery is not uniformly low risk. Obesity and diabetes are associated with increased morbidity, and selective antibiotic prophylaxis may reduce complications in higher‑risk patients. Limitations include single‑centre retrospective design, potential confounding by indication, and small event numbers. Next steps are multi‑centre prospective data collection and a closed‑loop evaluation of a risk‑stratified prophylaxis pathway.
P8-14 How Do I Feel About Starting Urology Registrar Training? A Study of Anticipatory Emotions and Self-Efficacy
Ms Eleftheria Xilas
1, Ms Lilli Cooper2, Mr Shekhar Biyani3, Ms Kelly Ong1
1Whipps Cross Hospital, Barts Health, London, United Kingdom, 2Department of Surgery and Cancer Imperial College London, London, United Kingdom, 33, St James’s University Hospital, Leeds, United Kingdom
Introduction: Transitioning into a registrar role is a milestone in postgraduate training, associated with excitement and anxiety. Understanding these anticipations can help tailor support for trainees. The primary-aim is to explore the relationship between self-efficacy and anticipatory emotions among new registrars. The secondary-aim was to categorise their anticipated challenges, fears, and motivations.
Methods: A total of 50 responses were collected from incoming urology-ST3 registrars at the urology bootcamp. The survey included self-efficacy scale and open-text questions exploring emotions. Emotional responses were mapped using a PANAS-derived valence scale. Qualitative responses were thematically categorised into clinical, logistical/workload, and social/personal domains. Correlation between mean emotional valence and self-efficacy was calculated using Pearson’s r, and subgroup-analysis by gender was performed.
Results: The PANAS map demonstrated a predominance of positive-affect, with pockets of emotions reflecting apprehension. A weak positive correlation was observed between self-efficacy and emotional valence (r = 0.236). Mean self-efficacy was similar between males (2.86 ± 0.25) and females (2.77 ± 0.28), though males reported marginally higher mean valence (+0.20 vs –0.08). The most reported challenges were logistical/workload pressures (40%), followed by clinical demands (38%) and social/personal factors (22%). Negative anticipations were primarily logistical (39%), whereas positive anticipations were largely social/developmental (40%).
Conclusion: Registrars exhibit a positive emotional profile underpinned by self-efficacy, with minimal gender variation. While self-efficacy appears to support more positive emotional anticipation, external pressures particularly workload/system-related challenges remain the predominant concern. Supporting trainees through structured mentorship, workload management, and role-transition programmes may enhance self-efficacy and promote a positive emotional adjustment.
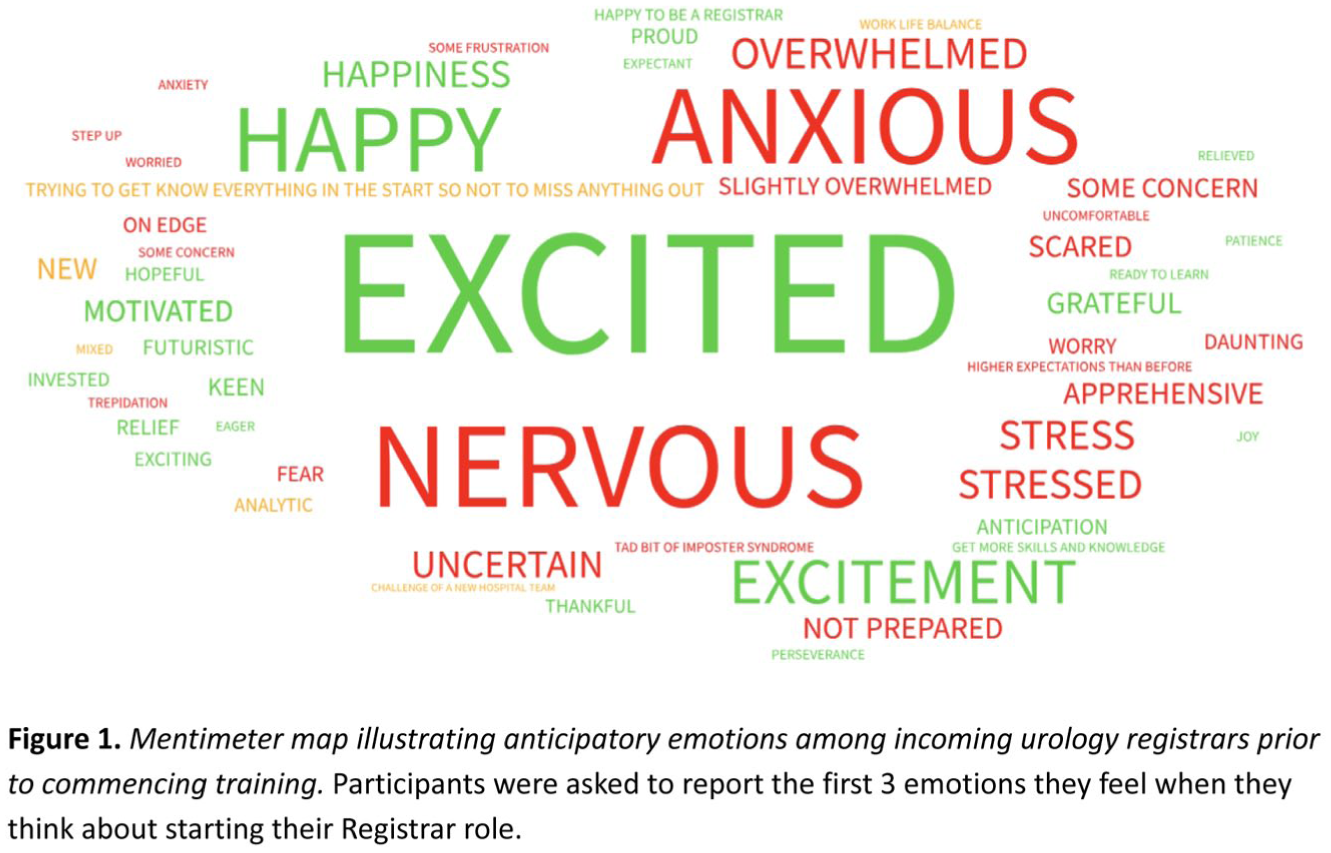
P8-15 The efficacy of follow up of small distal ureteric stones
Dr Vysh Sathish
1
1Torbay Hospital, Leicester, United Kingdom
Introduction: Routine follow-up imaging for conservatively managed ureteric stones varies, with limited national guidance regarding optimal surveillance strategies. Our institution routinely performs follow-up CTKUB for all conservatively managed ureteric stones regardless of size or location. This study evaluated whether CT follow-up is necessary.
Methods: A single-centre retrospective review was performed of patients attending a virtual stone clinic between December 2022 and January 2024 following emergency admission with a CT-confirmed ureteric stone. Stones were categorised by size (<4 mm vs >4 mm) and location (distal/VUJ,MU,PU). Binary logistic regression was used to identify predictors of spontaneous stone passage.
Results: A total of 148 patients were included (mean-age 50 years). Stones <4 mm demonstrated significantly higher spontaneous passage rates compared with stones >4 mm (89% vs 57%, p<0.05). Distal ureteric stones <4 mm had the highest passage rate (88%). Stone size and location were significant predictors of spontaneous passage. Stones <4 mm were associated with increased likelihood of passage (p=0.02), while distal and mid-ureteric stones were more likely to pass spontaneously than proximal stones (OR 2.30, p=0.03; OR 2.31, p=0.049 respectively). No complications occurred in patients who passed stones spontaneously. Few patients underwent negative ureteroscopy despite persistent stones reported on follow-up CTKUB.
Conclusion: Small distal ureteric stones demonstrated high rates of spontaneous passage with low complication rates. Routine CTKUB follow-up for all conservatively managed ureteric stones may expose selected patients to unnecessary radiation and healthcare costs. Patient-initiated follow-up or ultrasound surveillance may represent safe alternatives in asymptomatic patients with small distal ureteric stones.
ePoster Session 9: General - Management, Governance, Education and Quality Improvement 2, Paddy O’Reilly, June 16, 2026, 13:15 - 14:15
P9-1 Design, implementation, and evaluation of a curriculum to teach emergency simulation in Urology: a 9-year experience of a national simulation course
Miss Iona Fernandes1, Mr Mark Rochester, Miss Ruth Doherty, Mr Snehal Patel, Mr Stephen Payne, Mr Mamoun Hamid Elmamoun, Mr Vishwanath Hanchanale, Mr Chandra Shekhar Biyani, Mr Karan Wadhwa
1St James’s University Hospital, Leeds, United Kingdom
Introduction: Simulation-based education is increasingly recognised as a core component of surgical training, particularly for emergency management and development of non-technical skills (NTS). This study evaluates the design, evolution, and educational impact of the emergency simulation training session over a 9-year period.
Materials and Methods: The session delivers high-fidelity emergency urology scenarios using a SimMan® 3G mannequin, trained actors, and structured faculty-led debriefing. Scenarios were designed to reflect common on-call urological emergencies and to challenge decision-making, communication, leadership, and situational awareness. Trainees were introduced to cognitive workload assessment and NOTSS (Non-Technical Skills for Surgeons) domains. Post-course feedback from delegates and faculty between 2015 and 2024 was analysed using Likert-scale responses and free-text comments.
Results: Over nine years, 387 trainees participated in the session. Feedback demonstrated high satisfaction across multiple domains (Figure), including critical thinking (75–90%), clinical understanding (70–90%), and non-technical skills (75–90%). Participants reported significant improvements in communication, decision-making, and teamwork. Longitudinal data showed an increase in positive feedback and perceived educational value, with nearly 90% of participants indicating they would recommend the course to peers .
Conclusion: This is the largest and longest-running dedicated emergency urology simulation training session in the UK. Sustained positive feedback over nine years demonstrates that immersive emergency simulation effectively develops non-technical skills and supports the transition to resident-level practice. The session highlights the value of embedding structured simulation within national urology training curricula to enhance trainee preparedness and patient safety.
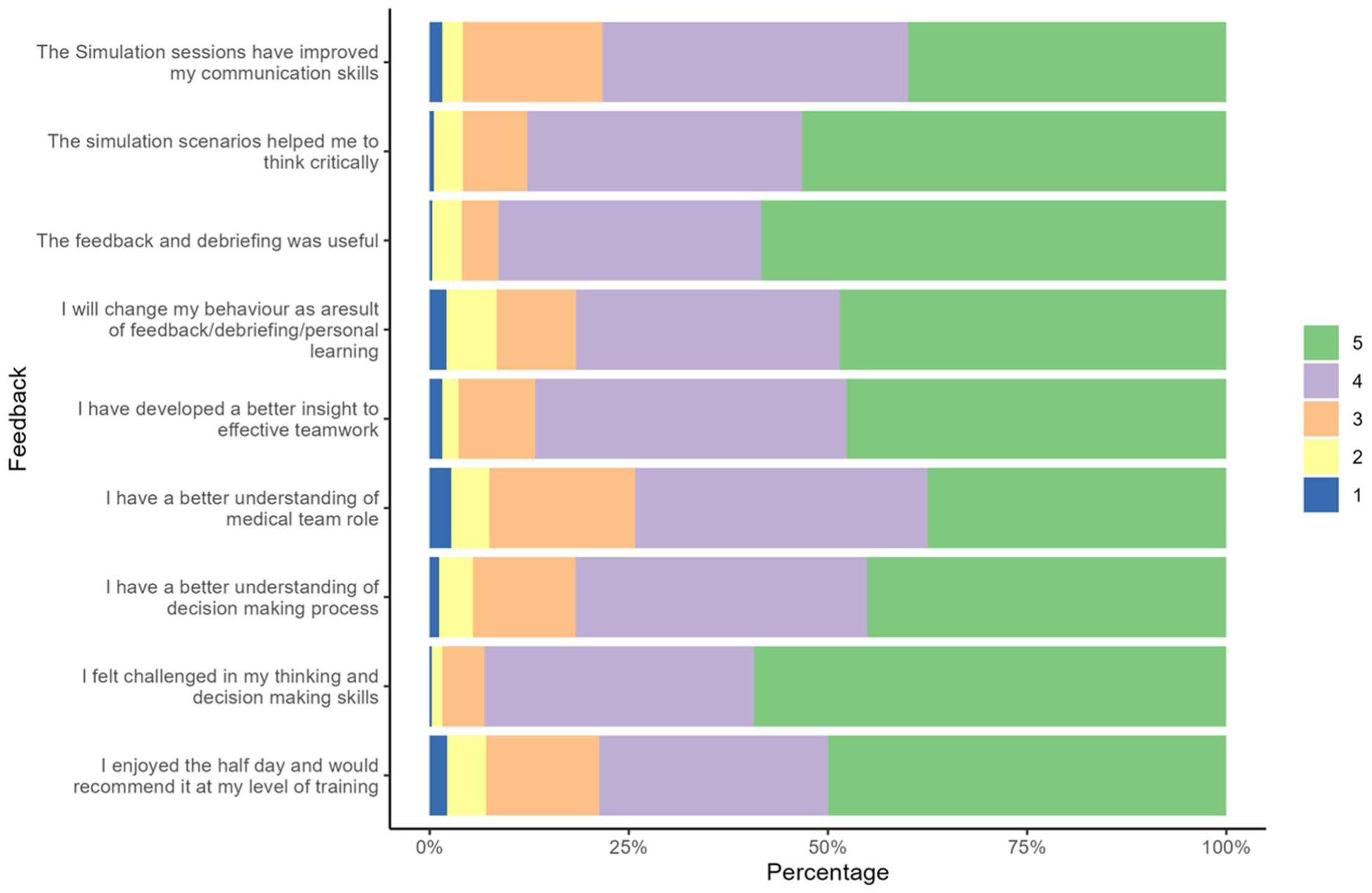
P9-2 Implementation of a Virtual Stone Clinic (VSC) to Improve the Management of Ureteric Calculi
Mr William Fowler, Mr Kenneth Mackenzie, Mr Ameet Patel
1South Tyneside and Sunderland NHS Foundation Trust, NEWCASTLE UPON TYNE, United Kingdom
Introduction: Traditional pathways for managing ureteric stones are hampered by excessive inpatient reviews and inconsistent waiting times. Increasing referral volumes necessitate novel, streamlined solutions. As most patients require conservative management, we evaluated a Virtual Stone Clinic (VSC) to ensure access to prompt imaging and telephone review, while simultaneously offering definitive treatment to patients requiring intervention.
Patients and Method: A retrospective audit established baseline performance (Cohort A), repeated following VSC implementation (Cohort B). The VSC enabled imaging and referral review to facilitate triage and appropriate repeat imaging requests; telephone reviews subsequently informed patients of results. Identification of those likely to fail conservative management allowed for fast-track to definitive treatment. Primary endpoints were time to repeat imaging and clinical review.
Results: In baseline audit (Cohort A, n=50), mean time to clinical review was 90 days and imaging was 98 days. Following VSC implementation (Cohort B, n=34):
Average time to repeat imaging decreased to 28 days (71.4% reduction).
Average time to clinical review decreased to 30 days (66.7% reduction).
Clinical outcomes: 56% (n=19) were successfully discharged virtually; 35% (n=12) were listed for intervention (6 ESWL, 6 Ureteroscopy); one required further imaging (CTU), and one DNA’d.
No adverse events or complaints were recorded.
For those fast-tracked, mean time to ESWL was 12.8 days.
Conclusion: VSC implementation led to significant reductions in diagnostic and review times. Decoupling decision-making from physical attendance achieved a more responsive service. This model allows rapid identification of patients failing conservative management, ensuring they reach definitive treatment faster than traditional pathways.
P9-3 Between Care and Consent: Medico-Legal and Ethical Challenges of Early Genital Surgery in Patients with Disorders of Sex Development – A Scoping Review
Dr Muhammad Asykar Palinrungi1, Profesor Hamzah Halim1
1Universitas Hasanuddin, Makassar, Indonesia
Introduction: Early genital surgery for Disorders of Sex Development (DSD) presents a profound clinical dilemma, balancing functional benefits against ethical concerns regarding autonomy and consent. Lacking a patient’s decision-making capacity, urologists typically rely on parental consent, which exposes clinicians to ethical uncertainty and significant medico-legal risk. This scoping review analyzes existing ethical and legal frameworks governing early surgery to identify their implications for clinical decision-making and professional liability in urological practice.
Materials and Methods: A scoping review was conducted using international medical and legal literature concerning genital surgery in minors with DSD. Relevant publications were identified via PubMed, Scopus, and legal databases. Studies were analyzed thematically, focusing on informed consent, parental decision-making authority, surgeon responsibility, and evolving human rights standards regarding bodily integrity and patient autonomy.
Results: Six international studies met the inclusion criteria. The literature demonstrates that parental consent frequently substitutes for fully informed, patient-centered decision-making, allowing irreversible interventions at an early age. While emerging human rights frameworks recommend deferring non-urgent surgery until patients can meaningfully participate in consent, clinical uncertainty and parental anxiety continue to drive early intervention. From a medico-legal perspective, the absence of unified guidelines leaves surgeons vulnerable to legal challenges as societal and legal norms evolve.
Conclusions: Early DSD surgery highlights a persistent tension between clinical care and consent, placing urologists at the intersection of ethical responsibility and legal risk. A shift toward rights-based, patient-centered frameworks is necessary to protect autonomy and provide legal clarity. Consistent guidance is essential for ethically sound urological practice.
P9-4 Improving Efficiency in TURP: Introduction of a Day-Case TURP Pathway Reduces Length of Stay Without Increasing Readmission
Miss Tirion Smith1, Mr Marc Williams
1Musgrove Park Hospital, Taunton, United Kingdom
Introduction: Transurethral resection of the prostate (TURP) has traditionally been managed as an inpatient procedure, contributing to bed pressures and variation in length of stay. GIRFT (Getting It Right First Time) guidance supports the use of day-case pathways for suitable TURP patients. This study evaluated the impact of the introducing a day-case TURP pathway on several outcomes including length of stay, discharge rates, and readmissions.
Patients and Methods: A retrospective review was performed comparing TURP patients prior to pathway implementation (July 2024-March 2025) with those treated following the pathway’s introduction (April-October 2025). Assessed outcomes included same-day discharge, length of stay, trial without catheter (TWOC) success, 30- day reattendance, and patient characteristics. Reasons for overnight admission and reattendance were also analysed.
Results: 37 patients were included pre-pathway and 60 post-pathway. Same- day discharge rates increased from 11% to 45%. Mean length of stay reduced from 1.27 to 0.65 nights. 30-day reattendance decreased from 30% to 12%, with a reduction in the severity of complications. TWOC success improved post-pathway from 65% to 83%. The number of TURPs undertaken increased from an average of 4 to 9 per month. Patient characteristics such as frailty, pre-operative catheterisation and anticoagulation were comparable between cohorts. The majority of overnight admissions post-pathway were routine rather than clinically indicated.
Conclusions: Implementation of a structed day-case TURP pathway significantly reduced average length of stay and increased same-day discharge without increasing 30-day reattendance. These findings support the safe adoption of day-case TURP to reduce elective bed pressures.
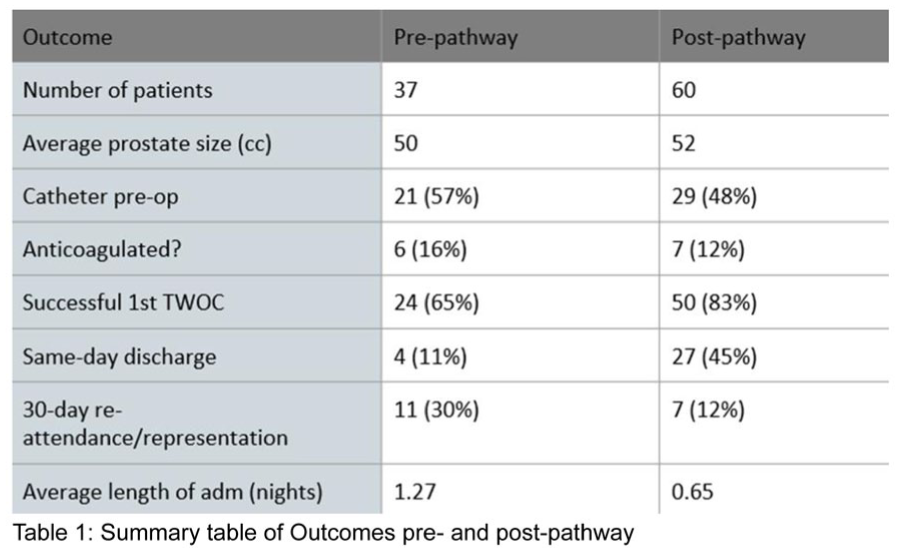
P9-5 Improvement in Radical Prostatectomy Surgical Outcomes: A 10-Year Analysis of Complications
Dr Declan Cahill2, Ms Mia Tazi1, Dr Duncan Self2, Dr Andri Orrason2, Dr Netty Kinsella2
1King’s College London/ Rmh, London, United Kingdom, 2Royal Marsden Hospital, London,
Introduction: Surgical complications remain a major determinant of healthcare burden and patient experience. In radical prostatectomy (RARP), complication rates reflect both surgical performance and system efficiency. This study aimed to describe the incidence, pattern, and evolution of postoperative complications following RARP over a 10-year period.
Methods: A prospectively maintained database of 1,978 radical prostatectomies performed between 2015 and 2024 was reviewed. Postoperative complications were recorded, categorised, and analysed annually to evaluate trends. Complications were further classified as idiosyncratic, representing unpredictable or non-preventable events, or recurrent, reflecting issues potentially mitigated through process refinement.
Results: The overall complication rate was 18%, with annual incidence decreasing from 40% in 2015 to 5% in 2024, demonstrating a sustained improvement in perioperative outcomes.
Approximately 5% of complications were idiosyncratic, often prompting procedural refinements that enhanced overall patient safety. A further 13% were recurrent, amenable to targeted process interventions to prevent recurrence. The most frequent complications are outlined in Table 1 and contribute 68% of all complications encountered.
The progressive reduction in complication rates was attributed to systematic outcome auditing, increasing surgical caseload improving technical consistency, and accessible postoperative communication enabling early recognition and management of emerging issues. Enhanced complication awareness also strengthened patient selection, perioperative management, and the validity of informed consent discussions.
Conclusion: Complications following radical prostatectomy can be substantially reduced through continuous process improvement. Key drivers include consistent outcome measurement, recognition of recurrent issues, procedural refinement, and experience accumulation. Sustained improvement is achievable when complications are measured, understood, and addressed systematically.
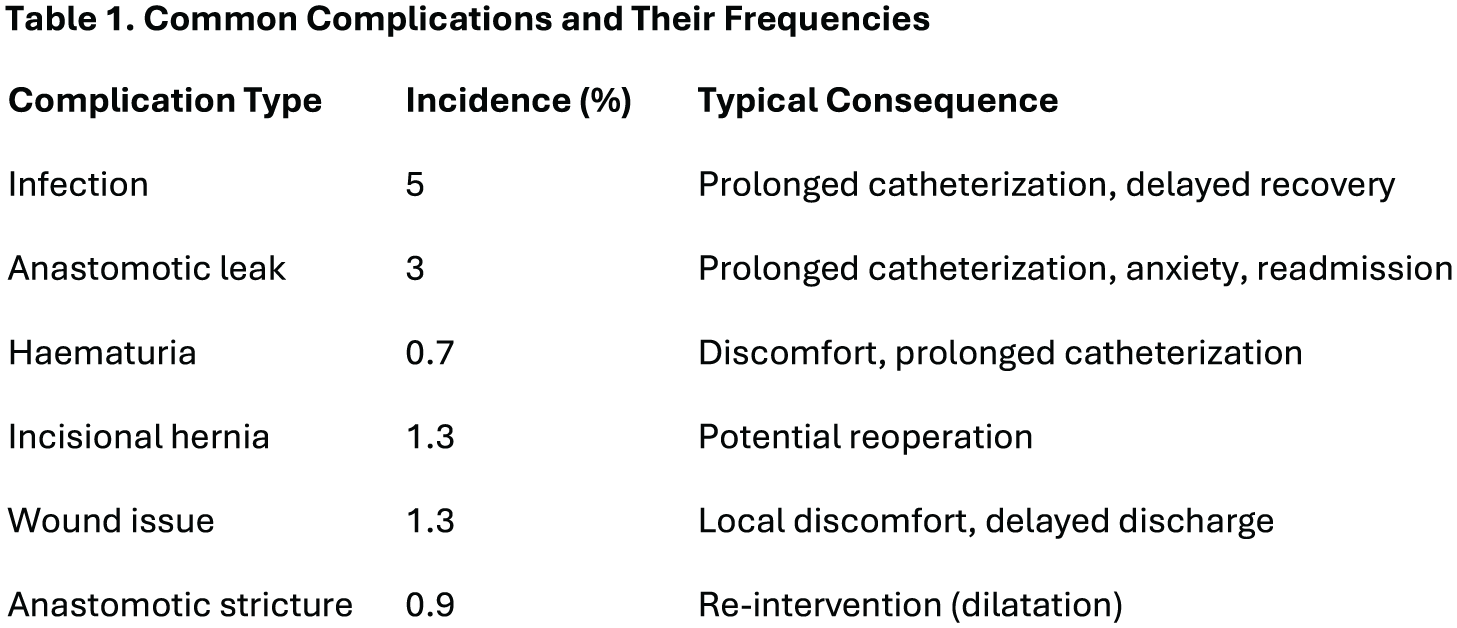
P9-6 A clinical pathway incorporating the TWIST score and ultrasound for low risk cases safely decreased the negative exploration rate and time to theatre in testicular torsion
Mr Samuel Folkard1, Miss Amy Wombwell2, Mr George Tyler2, Mr Ed Hart2, Mr Chim Chipeta2, Mr Max Kemp3, Miss Samaher Al Binali2, Mr Ian Rudd2, Mr Ali Henderson2
1Princess Royal University Hospital, Orpington, United Kingdom, 2Maidstone & Tunbridge Wells NHS Trust, Maidstone, United Kingdom, 3Kent & Medway Medical School, Canterbury, United Kingdom
Introduction: Due to concerns regarding missed torsions and a high negative exploration rate, we put in place this protocol incorporating the TWIST clinical scoring system and ultrasound for the low to intermediate risk cases of acute scrotal pain.
Patients: Audit data was collected prior to the protocol being put in place in December 2021 (n=144), with patients being identified from theatre coding and A&E coding detailing patients attending with acute scrotal pain. We collected three years of data following the change (n=178) to compare the two groups. Continuous variables were analysed by t-test and the negative exploration rates by Chi squared test. Operative details were identified by operation note review.
Results: Prior to the protocol there were 144 explorations (8 per month), and after there were 178 explorations (6.5 per month). The time to theatre decreased by mean 100 minutes from 5 hours 4 minutes to 3 hours 25 minutes after protocol implementation (P=0.01, CI 23.8 to 174.4). The negative exploration rate decreased from 78% to 71% and is on a downward trend (P=0.15, CI –2.5% to +16.5%). In the protocol group, two torsions were identified as potentially preventable with non-traumatic presentation of testicular pain through the governance process, both with a delay in line with national guidance.
Conclusions: A scrotal pain pathway incorporating ultrasound and the TWIST clinical score decreased the number of explorations completed, the negative exploration rate, and also the time to theatre. There were no preventable ‘missed torsions’ as a result of following the pathway.
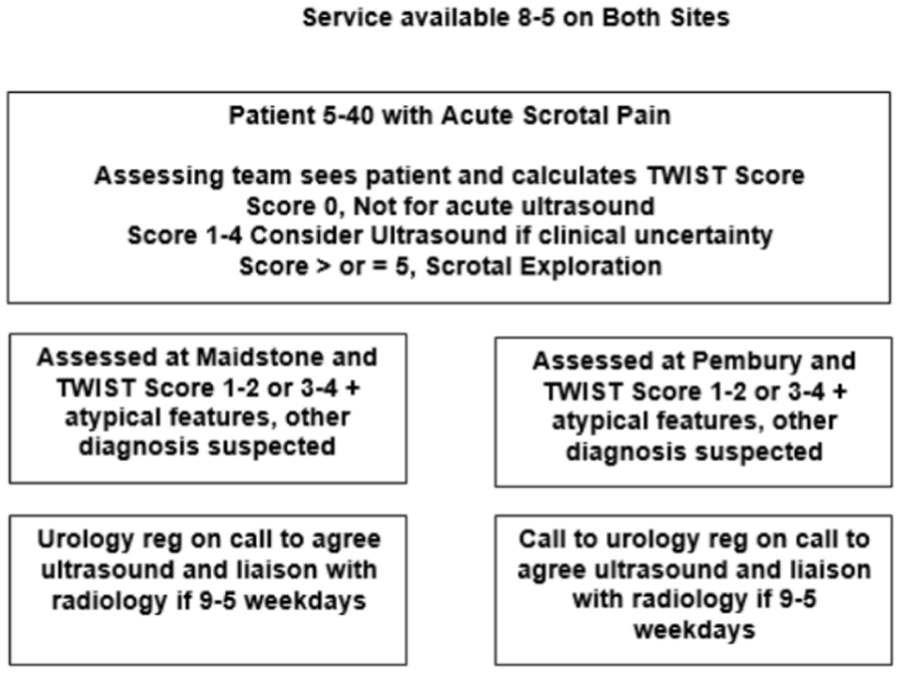
P9-7 Sustainability of Antibiotic Stewardship Interventions in Emergency Urology: Results from a Three-Cycle Audit
Miss Hira Bakhtiar Khan1,2, Dr Ahsan Iftikhar, Miss Pragnitha Chitteti2,3, Miss Mehwash Nadeem1,2
1James Cook University Hospital, Middlesbrough, United Kingdom, 2Teeside Urology Research Alliance (TURA), Middlesbrough, United Kingdom, 3Royal Salford Hospital, Manchester, United Kingdom
Background: Antimicrobial stewardship (AMS) is essential in emergency urology, where diagnostic uncertainty, time-sensitive clinical decisions, and high patient turnover can compromise adherence. This study aimed to evaluate AMS practices through a multi-cycle clinical audit and assess sustainability over time.
Methods: A three-cycle clinical audit was conducted in a single urology unit. All patients admitted through the emergency with suspected or confirmed infection and treated with systemic antibiotics were included. Cycle 1 (January–March 2022) served as the baseline. Following a poster-based AMS checklist as an intervention, Cycle 2 (January–March 2023) re-audited these practices. Cycle 3 (October–December 2024) evaluated the long-term sustainability. Data collected included microbiological sampling prior to antibiotic initiation, choice and duration of antibiotic, and modification following microbiology results. Clinical practices were assessed against the National Institute for Health and Care Excellence (NICE) guidelines and local Trust antimicrobial prescribing policies.
Results: A total of 263 patients were included across the three cycles. While practices initially improved post-intervention, these were not sustained. In Cycle 3, 38.1% of patients received antibiotics without prior microbiological sampling. Empirical prescribing showed considerable variation and often deviated from local guidance. Escherichia coli was the most frequently isolated organism in urine, blood, and pus cultures. Antibiotic therapy was modified in 22% of cases, primarily following microbiology results or during intravenous-to-oral step-down.
Conclusions: Targeted antibiotic stewardship interventions led to short-term improvements but did not sustain compliance. These findings highlight the need for ongoing education, system-based stewardship support, and regular re-auditing to uphold effective antimicrobial stewardship in high-turnover settings.
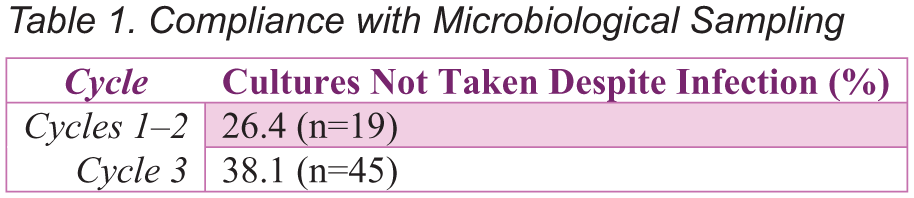
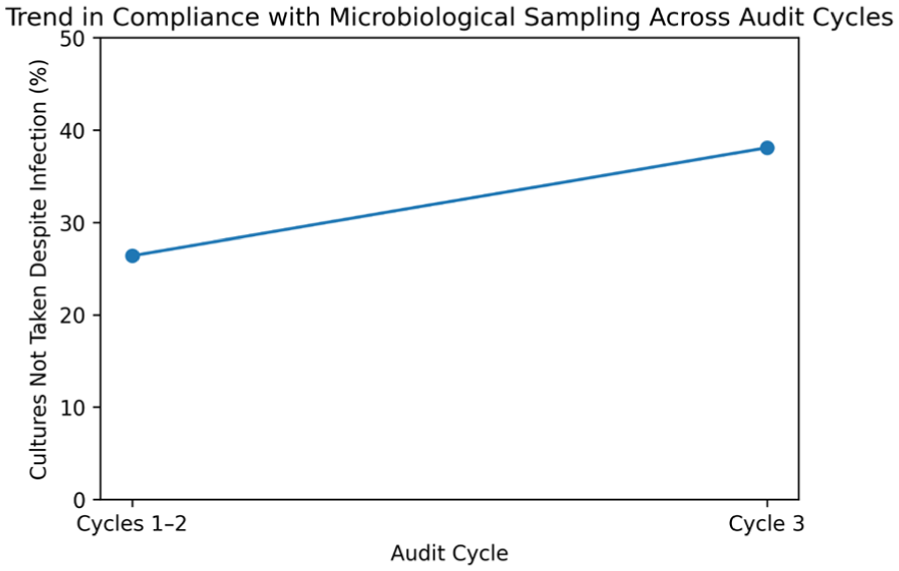
P9-8 A five-year retrospective review of patients investigated for non-visible haematuria, does cystoscopy confer any long-term benefit?
Mr Guy Grain1, Ms Elizabeth Bright1
1Royal Cornwall Hospital, Truro, United Kingdom
Introduction: There is currently no UK guidance regarding the role of cystoscopy in patients with non-visible haematuria (NVH) who do not meet two-week-wait criteria, despite NVH being prevalent in the unselected UK population and evidence that bladder cancer (BC) detection is low in this population. We sought to determine the incidence of BC in this population at both the time of referral and five-year follow-up, to determine if NVH was a prodrome for short or long-term BC diagnosis.
Patients and Methods: Retrospective case note review of all patients referred with NVH between May-October 2018, regarding the outcome of investigations for NVH and presence of a cancer diagnosis, at both initial referral and any subsequent re-referral for NVH in the succeeding five years.
Results: 286 patients (male (n=99), female (n=187); 21-93 years, mean age 66 years) received a cystoscopy for investigation of NVH between May-October 2018. Three patients (1%) were diagnosed with BC. In the follow-up period, 15 patients were referred for repeat cystoscopy for either NVH (n=7) or visible haematuria (n=8), of which one patient in the visible haematuria cohort was diagnosed with BC. A further patient was re-referred with an upper tract urothelial malignancy on imaging.
Conclusion: Our data suggests a low incidence of BC in unselected patients with NVH and no evidence that NVH represented a prodrome for future development of urological cancer. Consideration should be given to limiting NVH referrals only to those meeting the two-week-wait criteria.
P9-9 Readmission Following Urological Surgery in 2025: Identifying Opportunities for Quality Improvement
Mr Saeid Haghdani1, Dr Ghofran Al-Arbi1, Dr Aarthi Krishnan, Mr Ehab Abusada, Mr Khaled Hosny
1East Lancashire Hospitals NHS Trust, Blackburn, United Kingdom
Introduction: Hospital readmission following urological procedures represents an important quality of care and governance metric. This audit aimed to assess the rate, causes, and severity of readmission following urological surgery during 2025 and to identify service improvement strategies to reduce avoidable reattendance.
Patients and Methods: A retrospective review was conducted of 2,450 urological surgeries performed from January to December 2025. Readmission was defined as either a one-day review (attending the Emergency Department or Surgical Ambulatory Care but not admitted) or an inpatient readmission within 30 days of surgery. Data were collected on procedure type, reason for reattendance, and Clavien–Dindo grade of complication.
Results: A total of 211 patients (8.6%) were reviewed postoperatively. Of these, 158 (6.4%) were managed as one-day reviews, most commonly following circumcision (n=26), scrotal surgery (n=27), and TURBT (n=16). The leading reasons were wound problems (26%), pain (22%), and haematuria (15%). They were Clavien–Dindo grade I–II, requiring no further inpatient care. Additionally, 53 patients (2.2%) required inpatient readmission. The most frequent reasons were haematuria (17%), infection (15%), and wound complications (15%), with 75% graded as Clavien–Dindo I–II and 25% as grade III.
Conclusions: While the overall inpatient readmission rate remains low (2.2%), the significant number of outpatients’ reattendances (6.4%) reflects an opportunity for improvement. Many issues, mainly minor wound care or pain management, could be addressed through structured SOP’s for example telephone follow-up reviews, hot clinics, and enhanced discharge education. Implementing these governance measures could reduce unnecessary reattendance, improve patient satisfaction, and enhance continuity of postoperative care.
P9-10 Urolink and Global Urology: A ten-year review of UK urological participation
Mr Mayur Gami1, Mr Mike NG2, Mr Stephen Payne3, MS Suzie Venn4, Mr Chandra Shekhar Biyani5, Ms Danielle Whiting6, Mr Nicholas Campain7
1Southend Hospital and Cambridge Global Health Fellow, Southend/Cambridge, UK, 2North Bristol NHS trust, 3Manchester University NHS Foundation Trust, Manchester, UK, 4Worthing Hospital, , UK, 5St James’s University Hospital, Leeds, UK, 6Frimley Park Hospital, , UK, 7Royal Devon and Exeter Hospital, , UK
Introduction: Profound global inequities in urological care persist, driven by severe workforce shortages in low- and lower-middle-income countries despite evolving models of sustainable partnership. This study summarises current UK urologists’ engagement with global urology and compares attitudes with 2016 data to inform Urolink’s future strategic direction.
Methods: A 2025 cross-sectional survey, adapted from one carried out in 2016, collected demographic data, global surgery experience, suggested Urolink priorities, and barriers to global health work on a 5-point Likert scale, with further suggestions as free text. Quantitative data were analysed descriptively, and subjective data responses, thematically.
Results: One hundred urologists responded. 38% had previously undertaken urological work in low- and lower-middle-income countries (LMIC), consistent with the 2016 survey. Activity, mentoring, and in-country training were rated the most important Urolink functions at means of 4.5/5 and ~4.5/5, respectively. Advocacy, regional training hubs, equipment support, and reciprocal training opportunities scored means of ⩾4.0/5. Barriers included lack of time, insufficient professional leave, family commitments, and financial constraints. 90% of respondents believed professional leave was important for humanitarian work. 89% of respondents viewed Urolink as important to BAUS’s international profile. 79% expressed interest in remote engagement.
Conclusion: UK urologists show sustained commitment to global health and have clear preferences for partnership-based, educational, and sustainable models. The findings support expanding long-term institutional links, structured remote training and mentorship, and advocating formal professional leave to facilitate global health activities. Respondents also endorsed reciprocal training opportunities for LMIC and UK trainees, providing a focused framework for Urolink’s future strategy.
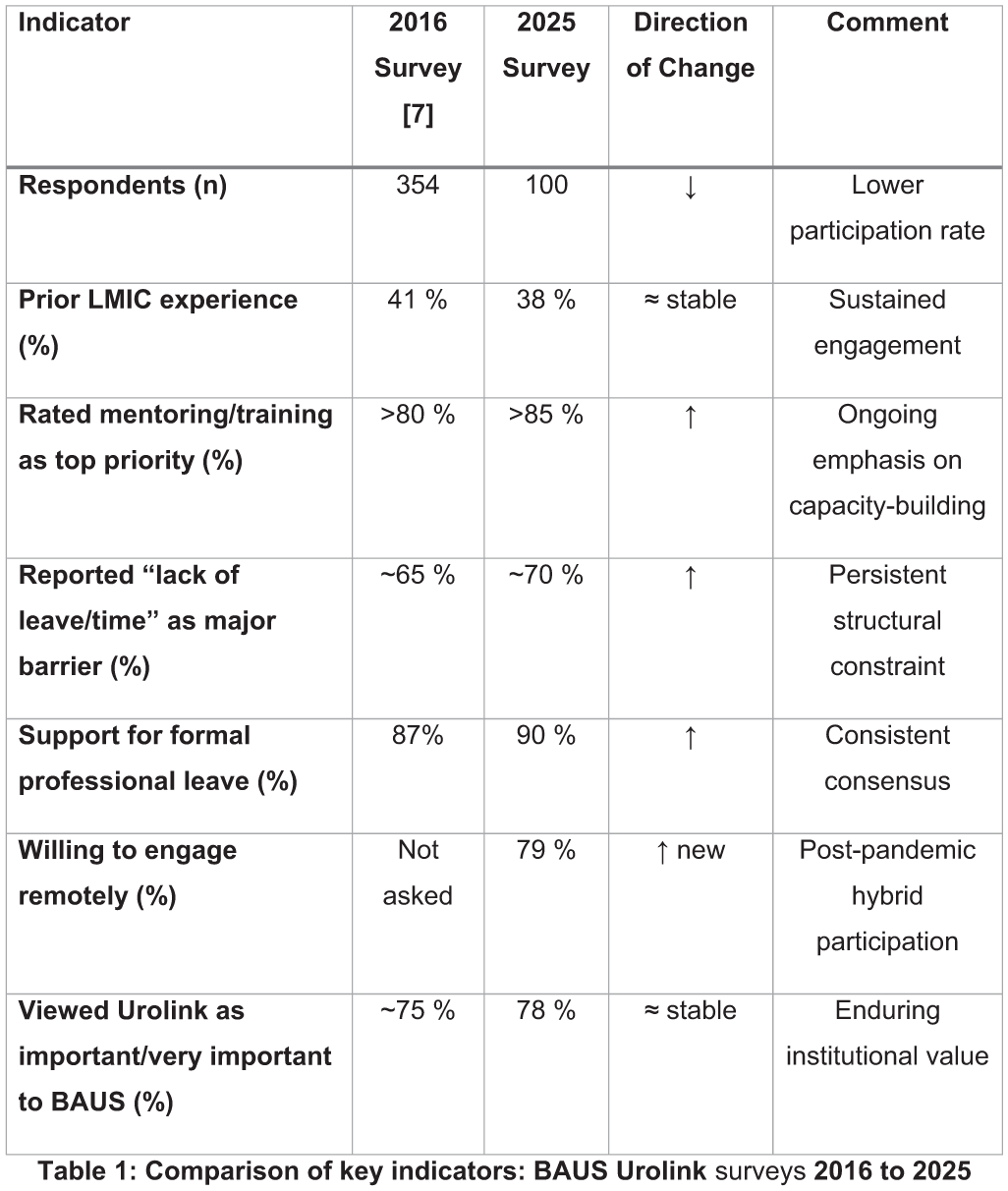
ePoster Session 10: Stones, Imaging and Upper Tract Disorders 1, John Anderson, June 16, 2026, 14:15 - 15:15
P10-1 Nephrostomy in malignant ureteric obstruction: Balancing benefit and burden in a palliative setting - a high volume single centre study
Mr Ahmed Badr1, Mr William Thompson1, Dr Noor Al-Bassam1, Dr Mikias Lemma1, Dr Matthew McClafferty1, Dr Jade Morgan1, Dr Tze Chan1, Mr Suresh Venugopal
1Liverpool University Hospital NHS Foundation Trust, Liverpool, United Kingdom
ePoster Session 10: Stones, Imaging and Upper Tract Disorders 1, John Anderson, June 16, 2026, 14:15 - 15:15
Introduction: Malignant ureteric obstruction frequently presents acutely and often necessitates decompression with nephrostomy insertion. However, nephrostomies are associated with significant morbidity and adversely affect quality of life, particularly in the palliative setting. As clinical needs differ between treatment-naïve patients and those who have exhausted oncological options, we reviewed nephrostomy insertions for malignant ureteric obstruction at our centre to evaluate outcomes in patients managed palliatively.
Methods: A retrospective review was conducted of all patients undergoing nephrostomy insertion for MUO between 2019 and 2021. Data collected included treatment stage when initially inserted,survival outcomes,type of malignancy, and subsequent interventions.Outcomes were analysed with particular focus on patients receiving their first nephrostomy in a palliative context.
Results: A total of 411 patients underwent nephrostomy insertion for MUO with prostate,bladder and gynecological malignancies leading the etiology. Of these, 173 patients had their first nephrostomy inserted at a palliative stage. Within this group,158 patients (91.3%) died within one year,with 142 (82.1%) dying within three months of insertion. Overall,282 (68.6%) patients died during this period. Seventy patients (17.03%) underwent nephrostomy removal with successful conversion to ureteric stenting. We noted 113 patients (27.49%) required more than one nephrostomy exchange prior to death or study completion. Only 16 patients (3.89%) became nephrostomy-free following further oncological treatment, none of which were palliative on presentation.
Conclusion: Patients chosen for Nephrostomy insertion for MUO, particularly in the palliative setting shoudl be carefully selected especially those woth compelling social circumstances, as default insertion could compose more of a burden than benefit.
P10-2 A United Kingdom Delphi consensus for the management of Malignant Upper Urinary Tract Obstruction
Professor Jonathan Aning1, Mr James Blackmur2, Mr Alexander Laird2, Dr Sophy Gretton3, Professor Tristan Barrett4, Dr Nadeem Shaida4, Professor Amit Bahl5, Mr Subu Subramonian6, Mr Rob Calvert7, Dr Anne Fee1, et al.,
1Bristol Urological Institute, North Bristol NHS Trust, Bristol, United Kingdom, 2Department of Urology, Western General Hospital, Edinburgh, United Kingdom, 3Department of Palliative Medicine, University Hospitals Bristol and Weston NHS Foundation Trust, Bristol, United Kingdom, 4Department of Radiology, Cambridge University Hospitals NHS Foundation Trust, Cambridge, United Kingdom, 5Bristol Haematology and Oncology Centre, University Hospitals Bristol and Weston NHS Foundation Trust, Bristol, United Kingdom, 6Department of Urology, Queen Elizabeth Hospital, University Hospitals Birmingham NHS Foundation Trust, Birmingham, United Kingdom, 7Department of Urology, Royal Liverpool University Hospital, Liverpool University Hospitals NHS Foundation Trust, Liverpool, United Kingdom
Introduction: Malignant upper urinary tract obstruction (MUUTO) is caused by advanced cancer. MUUTO patients when referred to hospital for treatment to relieve the obstruction present an important management dilemma. Consensus on key principles of management are currently lacking. This study aimed to establish a multidisciplinary expert consensus within the United Kingdom using a modified Delphi methodology.
Materials and Methods: A 131- item survey was developed through systematic review, expert opinion, and deconstruction of the MUUTO care pathway. A multidisciplinary panel comprising urologists, radiologists, oncologists, palliative medicine, general practitioners and cancer nurse specialists participated in iterative Delphi rounds via online questionnaires. Consensus was predefined as ⩾75% agreement, a median score >4, and an interquartile range <1. A public panel reviewed the results. Ethical approval was granted by the Health Research Authority (HRA) and Health and Care Research Wales (HCRW) (ref: 25/PR/0825).
Results: One hundred and twenty-seven clinicians participated in Round 1, and ninety-six in Round 2. Following a final face-to-face meeting, over 90 statements achieved consensus regarding the clinical management of MUUTO. Consensus was achieved on: standards for advanced elective discussions with patients; criteria for referral; appropriate emergency versus elective referral to secondary care; information for patients, carers and clinicians; MUUTO decompression techniques; management strategies, and aftercare. Key areas requiring further research were identified, particularly regarding antegrade stenting and bilateral renal decompression.
Conclusions: This modified Delphi study establishes practical consensus-based recommendations to guide the clinical management of MUUTO and highlights priorities for future research.
P10-3 COMPARE SAFETY AND EFFICACY OF MULTIPLE-TRACT VS SINGLE-TRACT PERCUTANEOUS NEPHROLITHOTOMY: A SINGLE-CENTRE EXPERIENCE
Dr Kamran Bhatti
1
1Hmc, Alkhor, Qatar
Background: Percutaneous nephrolithotomy (PCNL) is established as the standard minimally invasive approach for the management of large and complex renal calculi. The choice between single-tract and multiple-tract access remains debated, with concerns about safety, efficacy, and complication rates.
Objective: To compare the safety and efficacy of multiple-tract versus single-tract PCNL in patients with complex renal calculi at a single tertiary care center.
Methods: A retrospective analysis was conducted of 500 adult patients who underwent PCNL between January 2014 and December 2022. Patients were divided into single-tract (n=400) and multiple-tract (n=100) groups. Baseline characteristics, operative parameters, complications, and follow-up outcomes were compared. Statistical analysis was performed using t-test and chi-square tests, with p 2 cm (65% vs 30%, ) Patients in the multiple-tract group had significantly larger mean stone size (28.5 ± 10.2 mm vs 19.8 ± 7.5 mm, p2 cm (65% vs 30%, Postoperative complications, including fever (11% vs 5%, p=0.04) and Clavien–Dindo ⩾III events (6% vs 2%, p=0.03), were more frequent with multiple tracts. Hospital stay was longer (5.4 vs 3.8 days, )
Conclusion: Multiple-tract PCNL is associated with increased operative time, blood loss, complications, and hospital stay, though it remains an effective strategy for achieving acceptable stone clearance in complex cases. Careful patient selection and surgical planning are essential to optimize outcomes.
P10-4 Ascorbic acid supplementation effectiveness in reducing Double-J ureteric stent encrustations. A multicenter perspective
Mr Tamer Ewida1, DR Adel Elatreisy, DR Hamada Youssof
1Blackpool Teaching Hospital, Blackpool, United Kingdom
Introduction: Double-J stent encrustation is a common complication that can impede stent removal. Urinary pH and indwelling time are key contributors, and oral ascorbic acid has been proposed as a urine acidifier that might mitigate encrustation risk. This study aimed to assess whether daily ascorbic acid supplementation reduces the incidence of DJ stent encrustations.
Patient and Methods: A multi centre, non concurrent cohort study was conducted at three centres including adults undergoing endourological stone procedures with DJ stent insertion between July 2017 and January 2024. Group I comprised 359 patients prescribed oral ascorbic acid 500 mg three times daily from discharge until stent removal, while Group II included 483 patients who did not receive supplementation. Demographics, stent indwelling time, encrustation graded by the KUB system, and stent related adverse events were compared, and logistic regression was used.
Results: A total of 842 patients were included, and 172 (20.4%) developed DJ stent encrustations with a mean total KUB score of 6.2 ± 2.91. only 9 patients (2.5%) in Group I versus 163 (33.7%) in Group II (p < 0.001), while urinary tract infection was more frequent without ascorbic acid (57.8% vs 30%; p = 0.02). Multivariate analysis, lack of ascorbic acid intake, male gender, and longer stent were significant independent predictors of encrustation (p < 0.05).
Conclusion: Ascorbic acid supplementation is associated with a marked reduction in the DJ stents encrustations and fewer infective complications. Absence of ascorbic acid therapy, male gender, and prolonged stent should be considered key risk factors.
P10-5 Outcomes of the Endourological Management of Encrusted Ureteric Stents
Ms Maryam Rasheed1, Ms Stephanie D’Costa, Dr Muhammad Muneeb, Mr Damiete Harry, Mr Andrew Ballaro, Mr Junaid Masood
1Barking, Havering and Redbridge University NHS Trust, Ilford, United Kingdom
Introduction: Encrustation is a serious complication in patients whose ureteric stents are “delayed” or “forgotten”. Long waiting lists, limited theatre capacity and COVID pandemic delays have increased the incidence of encrusted stents. We present our experience in the often complex endourological management of encrusted stents.
Methods: A retrospective review of patients with encrusted ureteral stents at our unit between January 2022 and December 2024 was conducted. Data was collected on patient demographics, indications for and stent dwell times, extent and location of encrustation, procedures performed, and outcomes.
Results: 69 patients (34 male, 35 female), mean age 60.5 years (28-91) were included. The median stent dwell time was 297 days (457−191.5). 73.9% had a stent inserted for urolithiasis. 26.1% were stented for malignant or benign obstruction. 62% needed a combination of rigid and flexible uretero-renoscopy to remove the stent. 65% of patients needed cystolitholapaxy. One patient underwent a PCNL followed by endoscopic combined intra-renal surgery (ECIRS). 6 patients required 2 procedures to remove the stent.
92% of patients had complete stone clearance. 6 patients had residual fragments (4 managed conservatively, 2 needed relook surgery). The mean hospital stay was 1.2 days (1-8). Four patients needed HDU care post-operatively. Three patients had post-operative urosepsis.
Discussion: The removal of encrusted ureteric stents can be challenging, often requiring complex endo-urological approaches with associated morbidity. A structured stepwise approach can achieve high clearance rates. Strategies minimising stent insertion, patient education and robust stent monitoring systems can reduce the incidence of stent encrustation and associated complications.
P10-6 Quantification of Urinary Stent Calcification in an Ex-Vivo Biomimetic Model: Role for New Materials
Dr Feras Al Jaafari1,2, Dr Ellie Tang3, Dr Jennifer Kervadec3, Dr Emmanuel Letavernier3, Dr Michel Daudon4
1NHS Fife University Health Board, Kirkcaldy, United Kingdom, 2School of Medicine, University of St Andrews, St Andrews, United Kingdom, 3INSERM UMR1155, Common and rare kidney diseases, Hôpital Tenon, 75020 Paris, France, 4Sorbonne Université, Service des Explorations Fonctionnelles Multidisciplinaires, AP-HP, Hôpital Tenon, 75020 Paris, France,
Introduction: Ureteral stent encrustation remains a clinical challenge. Silicone stents have shown lower encrustation rates than polyurethane-based ones. Recently, new stents with modified surface properties were introduced, aiming to reduce encrustation. This study compares the encrustation of stent materials using a dynamic in-vitro urinary model.
Methods: Four stents—hydrocoated silicone (Imajin®hydro, Coloplast), Inlay Optima™ (Bard), Percuflex™ and Tria™ (Boston Scientific)—were incubated for 7 days in non-sterile human urine. They were then placed in a glass kidney-ureter-bladder model with circulating artificial urine at 37°C for another 7 days. This experiment was repeated eight times. Encrustation was semi-quantitatively assessed by two independent observers using a validated scale. Calcium deposits were quantified after acid extraction.
Results: Encrustation varied by stent region. Overall, Imajin®hydro (IH) and Inlay Optima™ (IO) showed significantly less encrustation than Percuflex™ (P) and Tria™ (T). IH performed best in stent holes, while IO outperformed P and T in stent loops. Both IH and IO showed reduced encrustation on the stent body. Despite standardized conditions, inter-experiment variability affected calcium quantification. Median calcium burden was highest in P stents. Only silicone stents showed significantly lower calcium levels when compared to P. Deposits included brushite, calcium oxalate monohydrate and apatite, mixed with biofilm proteins.
Conclusion: In line with previous findings, our biomimetic model confirms that silicone stents exhibit lower encrustation potential than other materials. Semi-quantitative scoring and/or calcium quantification showed significantly reduced calcification in silicone stents compared to Tria™ and Percuflex™, supporting their continued use in clinical practice.
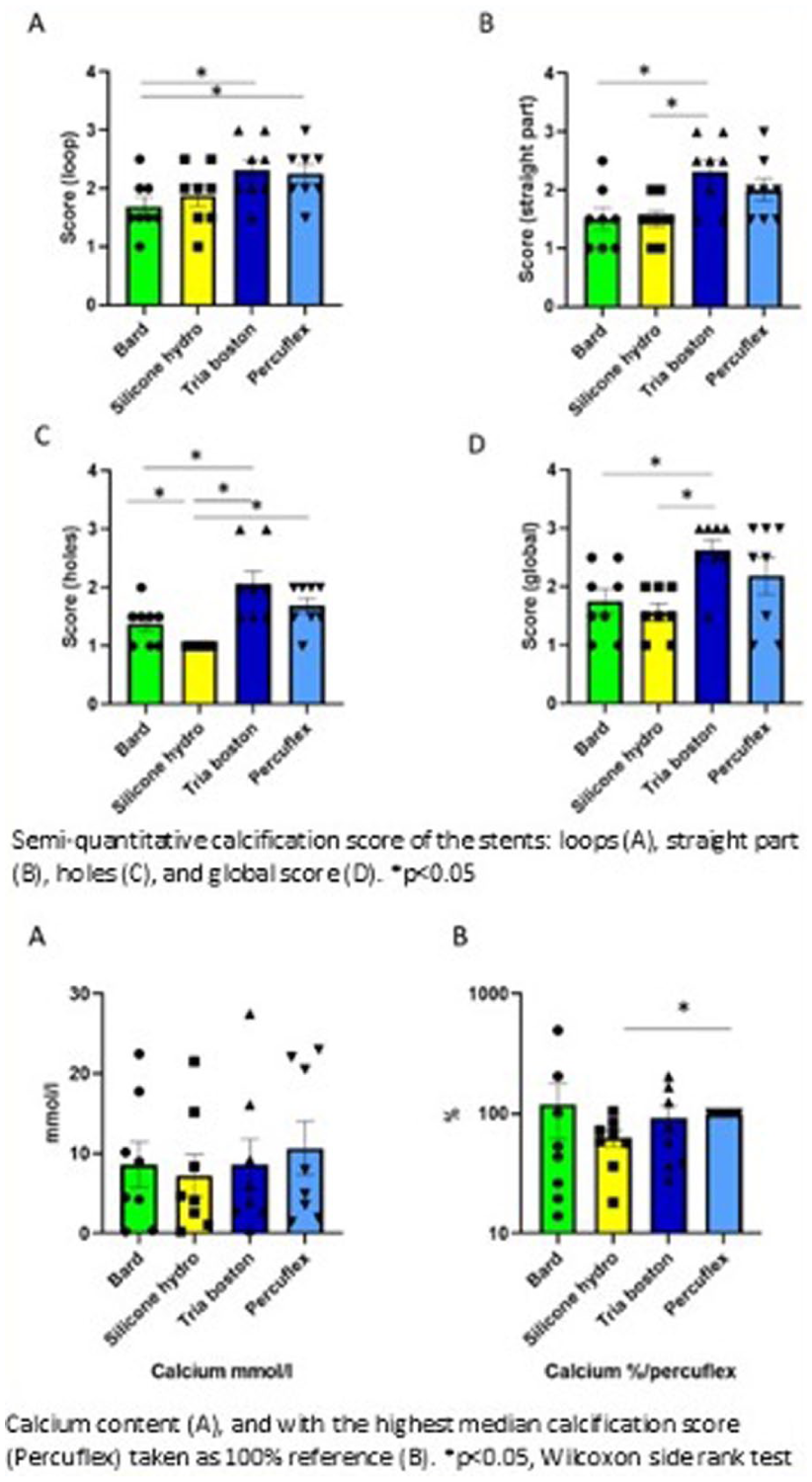
P10-7 Sent dwell time and a pragmatic tiered framework for NEWS2-defined post-ureteroscopy urosepsis after emergency ureteric stenting: a prospective cohort study
Mr Omar Ramadan1, Mr Yazeed Moahmmed1, Mr Pejman Kheirandish1, Ms Jemma Hale1, Mr Rajeshwar Krishnan1, Mr Issam Ahmed1
1East Kent Hospitals University NHS Foundation Trust, Canterbury, United Kingdom
Background: Emergency ureteric stenting is commonly used to temporise obstructing urolithiasis, but delay to definitive ureteroscopy (URS) may increase infectious complications.
Objective: To evaluate the association between stent dwell time and NEWS2-defined post-URS urosepsis, and to propose a pragmatic tiered prioritisation framework based on observed risk gradients.
Methods: Prospective cohort of adults undergoing elective URS following emergency ureteric stenting for obstructing urolithiasis. Post-URS urosepsis was defined as suspected infection with clinical deterioration within 48 hours meeting a NEWS2 sepsis trigger (NEWS2 ⩾5 or any single-parameter score of 3). Multivariable logistic regression assessed independent associations across patient, stone and operative factors. Risk gradients were summarised by (i) number of independently associated factors and (ii) dwell-time bands; these informed a pragmatic tiering framework (not a validated prediction score).
Results: Among 256 patients, 49 (19%) developed urosepsis and 2/49 (4%) required intensive care. Independent associations included ASA ⩾III (adjusted odds ratio [aOR] 5.6, 95% CI 2.6–8.3), proximal/renal stones (aOR 3.0, 95% CI 1.2–4.3), higher stone density (aOR 2.8, 95% CI 1.4–6.7), preoperative leucocytosis (WCC >11,000/mm³; aOR 1.5, 95% CI 1.0–2.5), longer operative time (aOR 6.75, 95% CI 4.30–10.34) and longer stent dwell time (aOR 9.4, 95% CI 5.45–12.6). Odds increased stepwise with ⩾4 risk factors (OR 10) and with dwell time ⩾8 weeks (OR 5–7) .
Conclusions: In emergency-stented patients undergoing URS, prolonged dwell time and cumulative adverse factors are strongly associated with NEWS2-defined post-operative urosepsis. A pragmatic tiered framework may support prioritisation those with multiple adverse factors), pending external validation
P10-8 Infectious complications post ureteroscopy: Incidence and risk factors: Results over a 12-year period
Dr Shriya Fernandes1, Mr Nico Christian Grossmann, Miss Florencia Maria Frascheri, Mohammed Boulmani, Erin Chaussee, Nazanin Tabesh, Ms Amelia Pietropaolo, Professor Bhaskar Somani
1University Hospital Southampton, Southampton, United Kingdom
Background: Infectious complications after ureteroscopy (URS) ranging from postoperative urinary tract infection (UTI) to sepsis, may lead to critical care admission, particularly in high-risk patients. We evaluated the incidence and univariable predictors of postoperative infectious complications.
Methods: A retrospective single-centre URS cohort from a UK hospital (2012–2024) was analysed (n=1,259). The primary outcome was any postoperative infectious complication (composite); secondary outcomes included postoperative UTI/fever, sepsis, and intensive care unit (ICU) admission for sepsis. Demographics, comorbidities, renal function, stone factors, and peri‑operative variables were compared using univariable analyses;significance was set at p < 0.05.
Results: Postoperative complication occurred in 125/1,259 (9.9%), including any infectious complication in 69 (5.5%), UTI/fever in 66 (5.2%), post-operative sepsis in 32 (2.5%), and ICU admission in 7 (0.6%). Infection was more common in patients aged >75 years (11.4% vs 4.0%, p<0.001, Table 1) and in females (7.4% vs 4.3%, p=0.029). Significant comorbidity associations included chronic obstructive pulmonary disease (19.0% vs 4.9%, p=0.001), multiple sclerosis (50.0% vs 4.9%, p<0.001), ischaemic heart disease/heart failure (11.9% vs 4.9%, p=0.020), prior
TIA/CVD (13.3% vs 5%, p=0.013), and CKD (14.1% vs 4.8%, p=0.002). Lower pre‑ and postoperative eGFR categories were associated with higher infection rates (both p<0.001). Procedural factors associated with infection included longer operative time (p=0.006), postoperative stent use (p=0.018), and non‑day‑case admission (p<0.001).
Conclusions: Complications after URS (10%) are not uncommon; infectious complications
disproportionately affect fragile patients. These findings highlight the need for careful pre-operative risk stratification and tailored procedural planning, to improve safety and reduce post-operative URS-related complications.
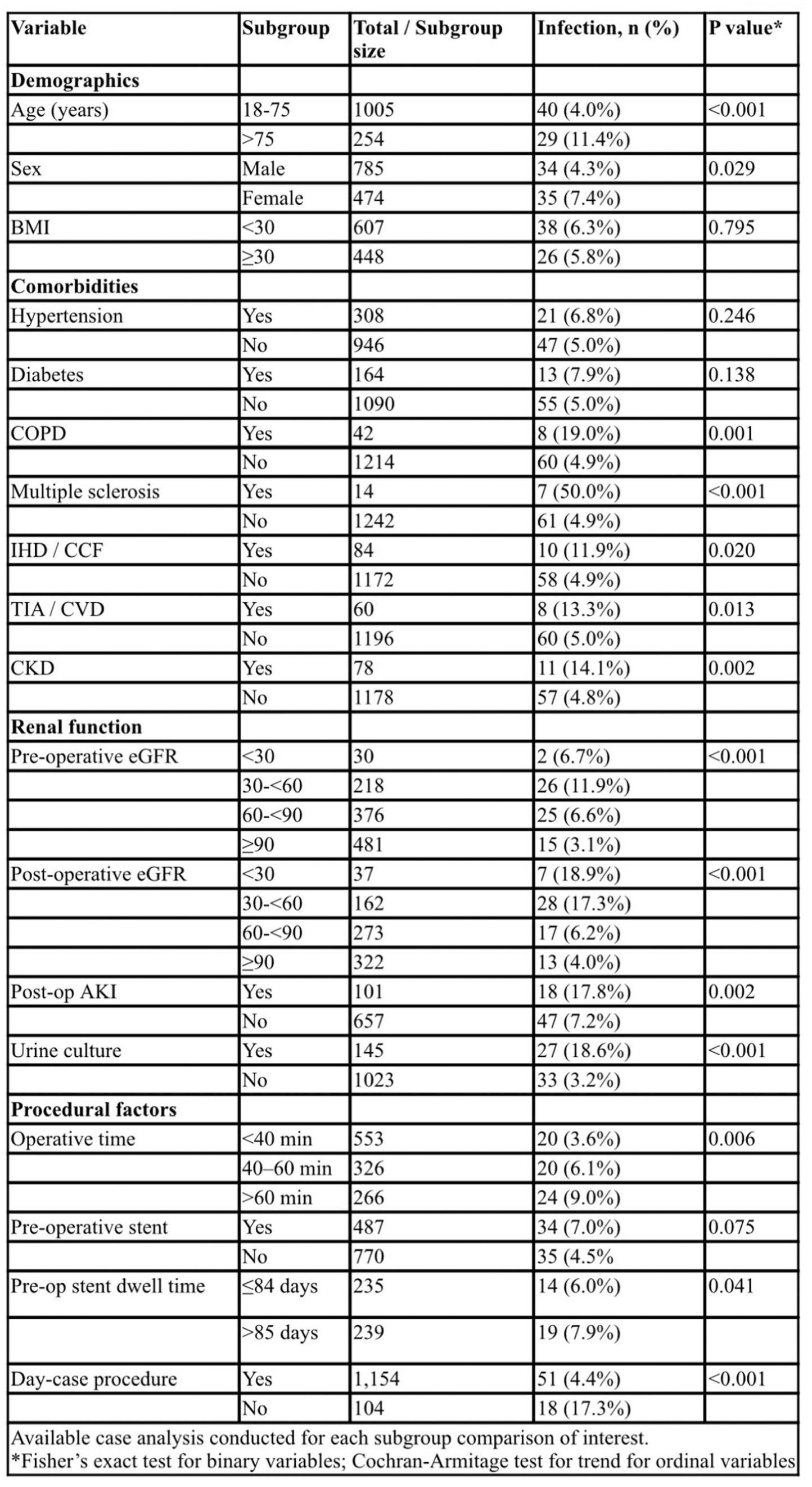
P10-9 Pilot Clinical Study on Real-time Intrarenal Pressure (IRP) Monitoring and Automated Irrigation Suction System with Flexible Ureteroscope and IRP-monitoring Flexible and Navigable Suction Ureteral Access Sheath (FANS) with iMimer system
Professor Steffi Kar Kei Yuen1, Professor Vineet Gauhar2, Professor Bhaskar Somani3, Professor Chi Fai Ng1
1Chinese University of Hong Kong, Hong Kong, Hong Kong, 2Ng Teng Fong General Hospital, Singapore, Singapore, 3University Hospital Southampton, NHS Trust, Southampton, U.K.
Introduction: Elevated intrarenal pressure (IRP) during flexible ureterorenoscopy (fURS) is a known risk factor for post-operative infectious complications and renal damage. While suction-assisted devices like FANS can lower IRP, manual regulation of irrigation and suction is imprecise and operator-dependent. We present the initial clinical experience of IRP-monitoring FANS with iMimer™ system for real-time IRP monitoring and automated control.
Materials and Methods: This prospective pilot study (Oct 2024-Mar 2025) involved 20 patients undergoing fURS for renal stones, utilising a pressure-sensing channel within 10/12Fr IRP monitoring FANS connected to the iMimer™ console. An intelligent algorithm autoregulates irrigation and suction to maintain IRP below a set safe threshold (30 mmHg), with data displayed live.
Results: The system was successfully deployed in all cases with no device-related adverse events. Automated regulation maintained IRP below 30 mmHg for 96.5% of operative time, and it never exceeded 40 mmHg. Surgeons reported significantly fewer manual adjustments and optimal kidney distension >90% of the time. There were no septic or major complications.
Conclusion: This study demonstrates that real-time IRP monitoring with intelligent autoregulation using the iMimer™ FANS system is both feasible and safe. The technology effectively minimizes hazardous IRP elevations during fURS, potentially reducing the risk of pyelovenous backflow and sepsis. This automated approach represents a significant step towards standardizing a critical safety parameter in endourology and may facilitate more complex procedures with a superior safety profile, relieving surgeon mental burden on intraoperative devices control.
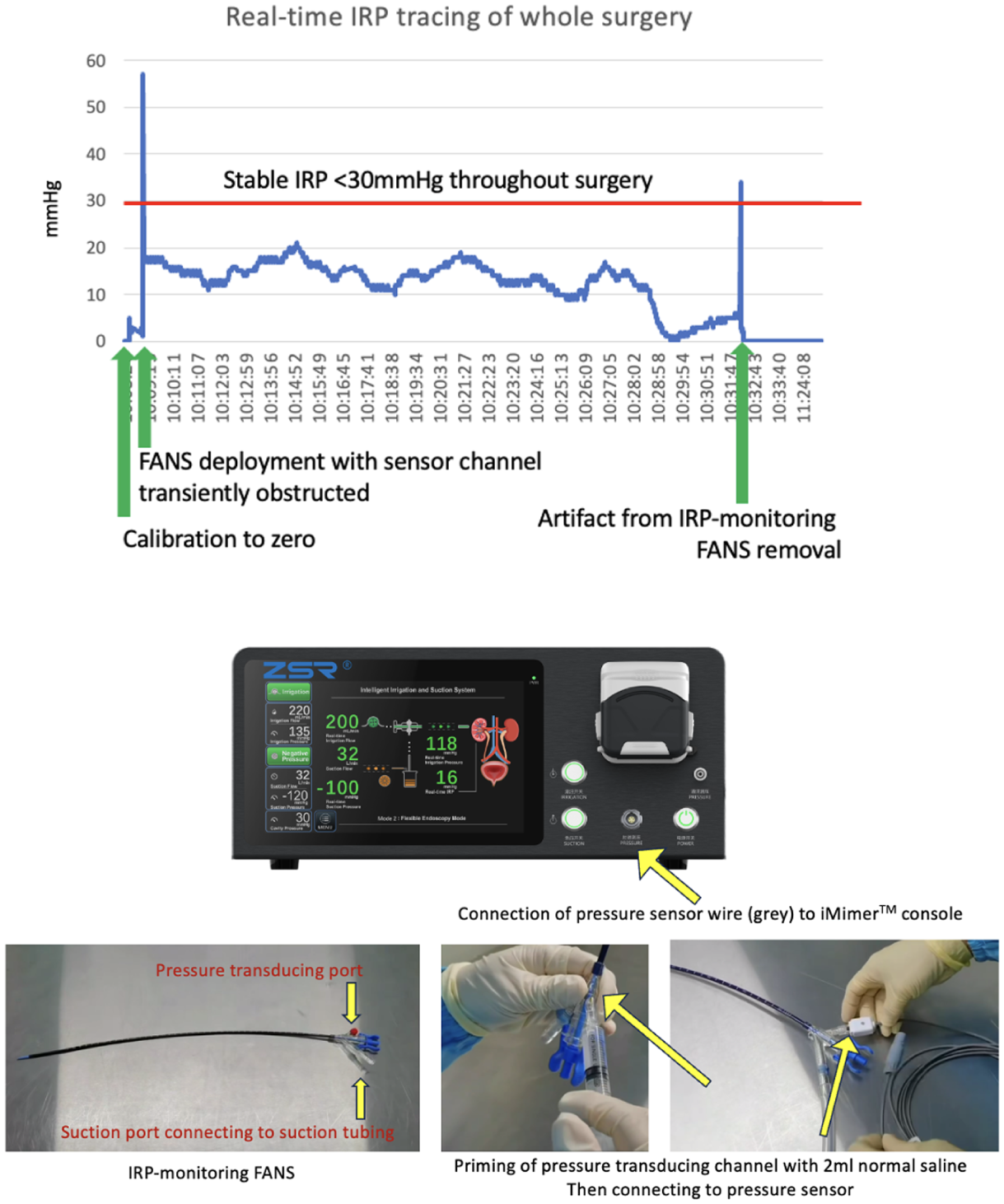
P10-10 Performance of flexible suction aided management of upper tract urolithiasis: A systematic review and meta-analysis of randomised controlled trials
Mr Syed Mustafa Shah1, Ms Zaara Nabi1, Mr Ghulam Nabi1, Mr Jose Antonio Campos Sañudo2, Mr Saddam ALDemour3, Mr Mohammed H Khan4
1Faculty of Medicine, Univeristy of Dundee, Dundee, United Kingdom, 2Department of Urology, Dr Sulaiman Alhabib Medical Group, Riyadh, Saudi Arabia, 3Department of Urology, The Univeristy of Jordan, Amman, Jordan, 4Department of Urology, Tawam Hospital, Al Ain, United Arab Emirates
Introduction: Suction use during management of upper tract urolithiasis has increased recently, however its clinical performance and cost benefit analysis remain under-defined. We performed a systematic review with meta-analysis to evaluate the efficacy of Flexible and Navigable Suction Sheath (FANs) technology.
Patients and Methods: Embase, PubMed, Scopus and Cochrane databases were searched (September 2025 to December 2025) for RCTs comparing FANs with conventional treatments (Ureteral Access sheaths (UAS) or mini- PCNL) for the management of upper tract urolithiasis. Outcomes included stone-free rate (SFR), operative time, re-intervention, complications, quality of life (QoL) and health economics.
Results: Seven RCTs (1,592 participants) were identified. Compared to traditional UAS, FANs demonstrated a significantly higher SFR (RR:1.21; 95% CI: 1.07-1.38: p<0.003) and significantly lower re-intervention rate (RR:0.29; 95% CI: 0.16-0.52; p<0.0001). FANs significantly reduced overall complications (RR:0.36; 95% CI: 0.22-0.59; p<0.0001) and infection risk (RR: 0.28; 95% CI: 0.15-0.52; p<0.0001) versus UAS, with no significant difference in operative time (p=0.94).
Compared to mini-PCNL, FANs showed no significant difference in SFR (p=0.23) or infection rates (p=0.91). However, FANs had significantly longer operative times (MD: 22.24 min; p=0.002). Reintervention and serious complication rates showed a lower trend in the FANs group. Quality of life and health economics data were sparse but favoured FANs.
Conclusions: FANs significantly improve SFR, reduces reintervention, overall complication and infection rates compared to traditional non suction sheaths. FANs preformance is comparable to mini PCNL except for a longer operative time. These findings suggest FANs are a superior alternative to traditional non suction sheaths.
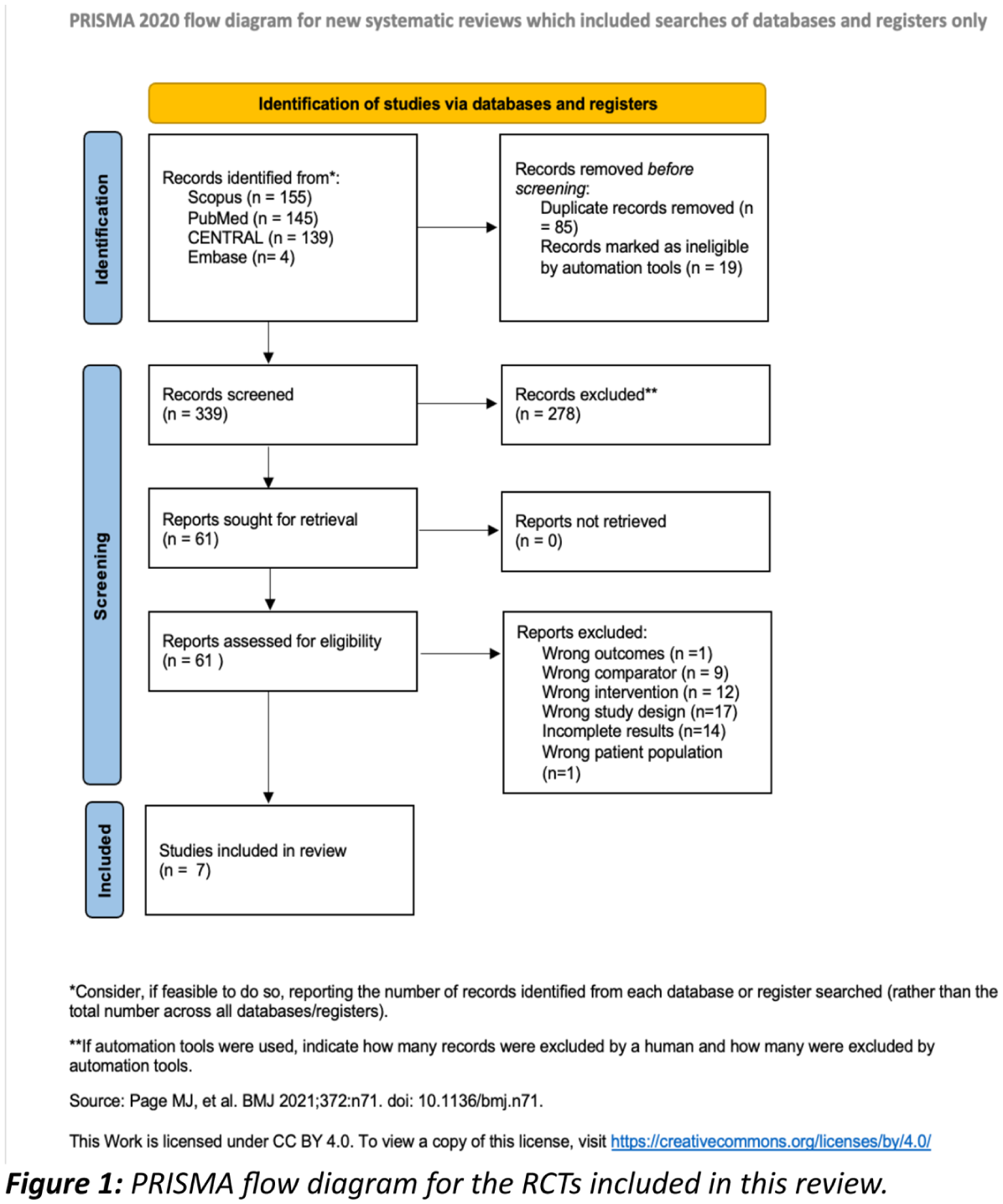
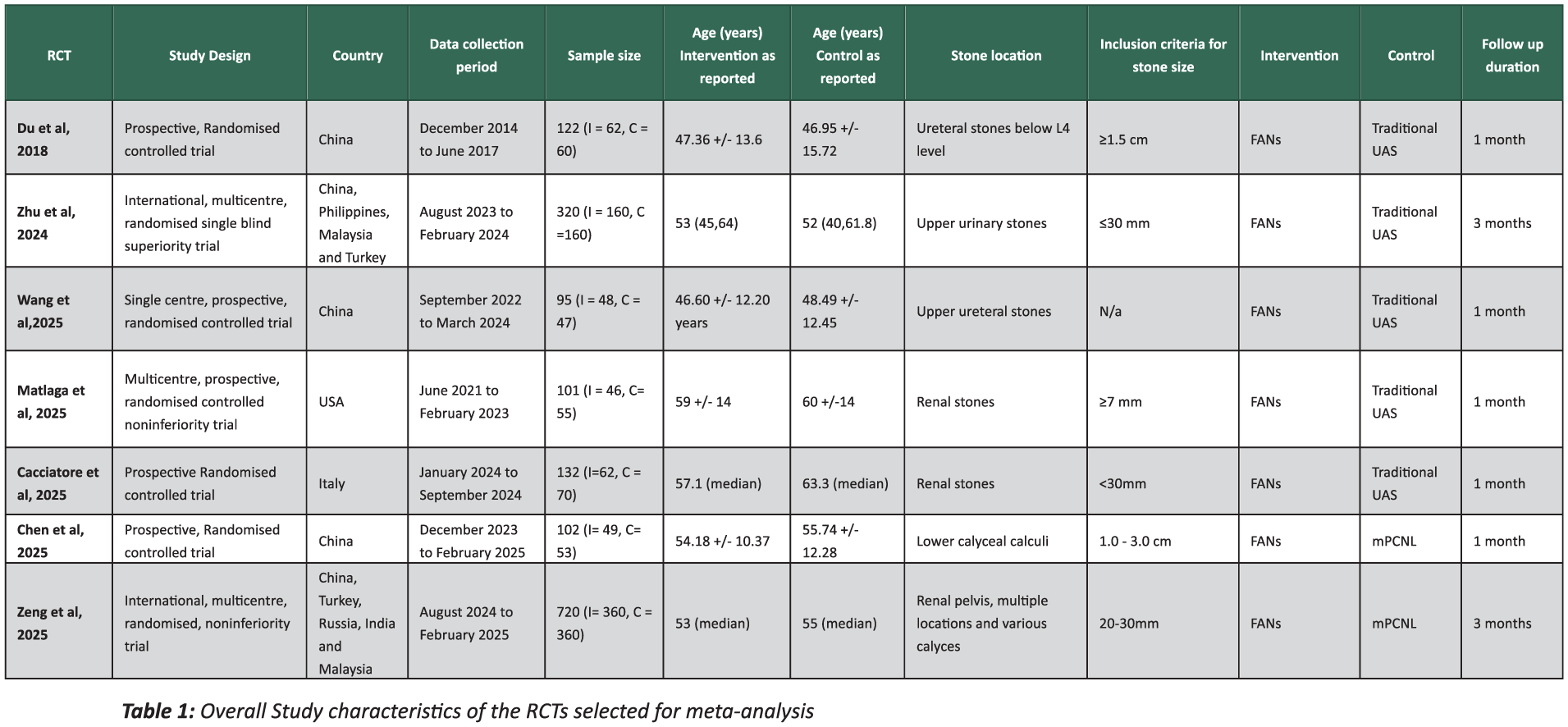
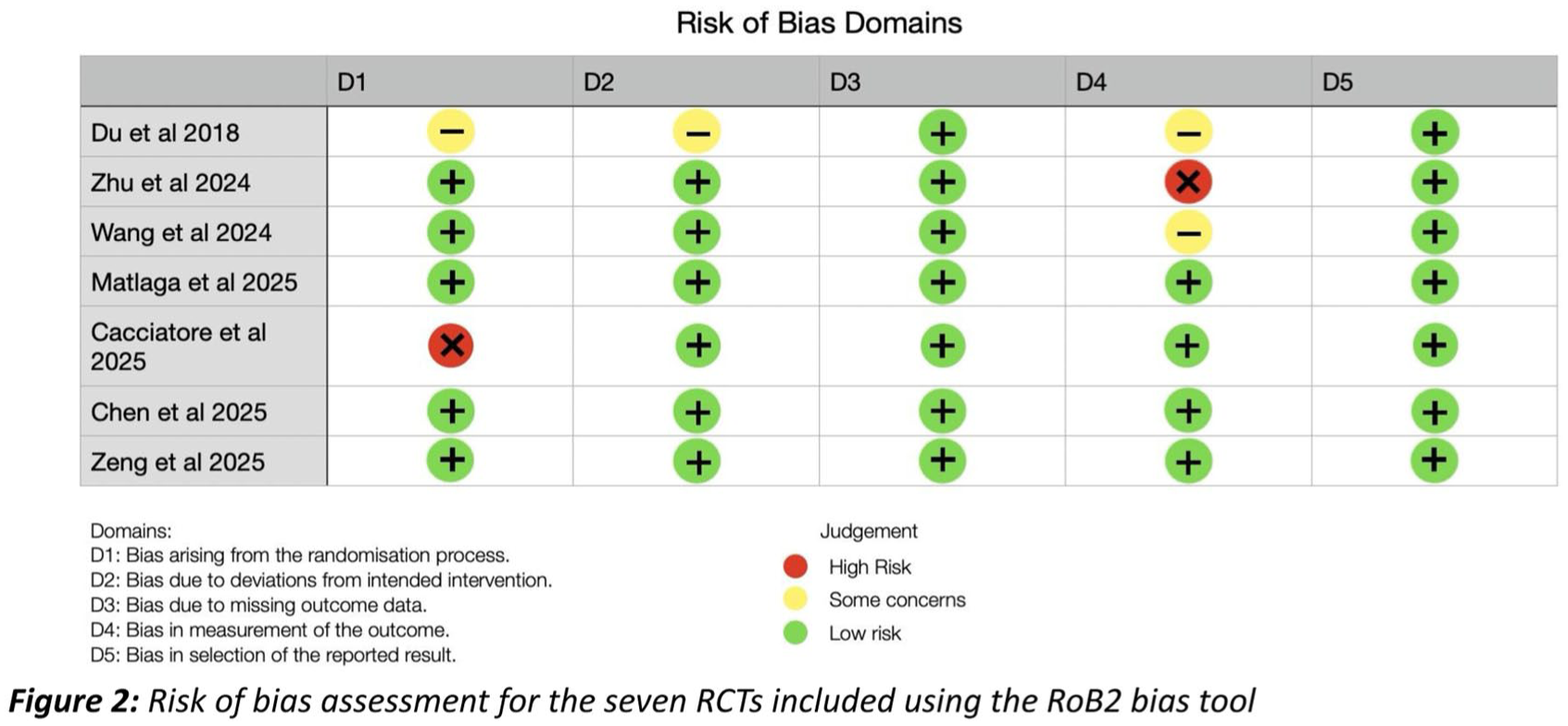
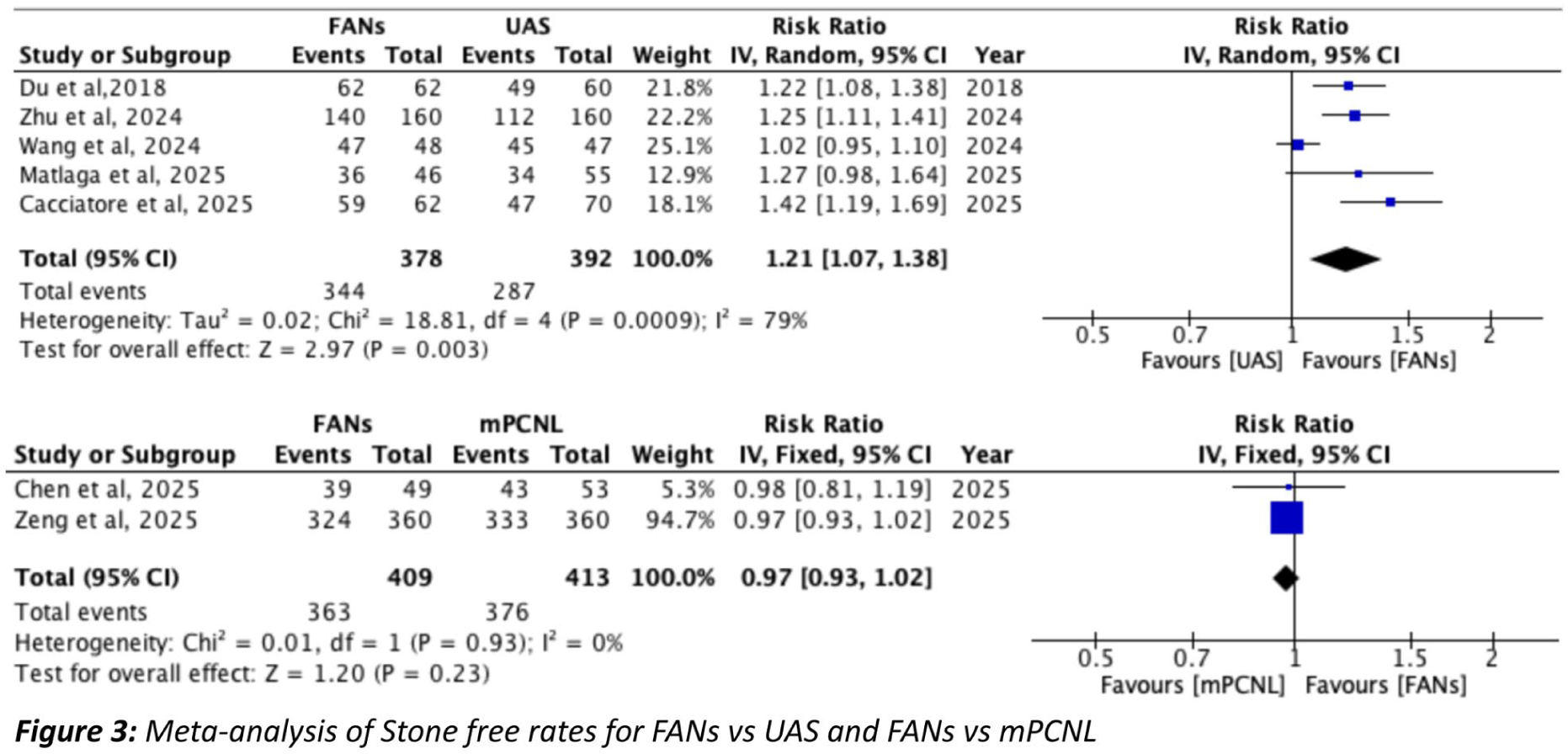
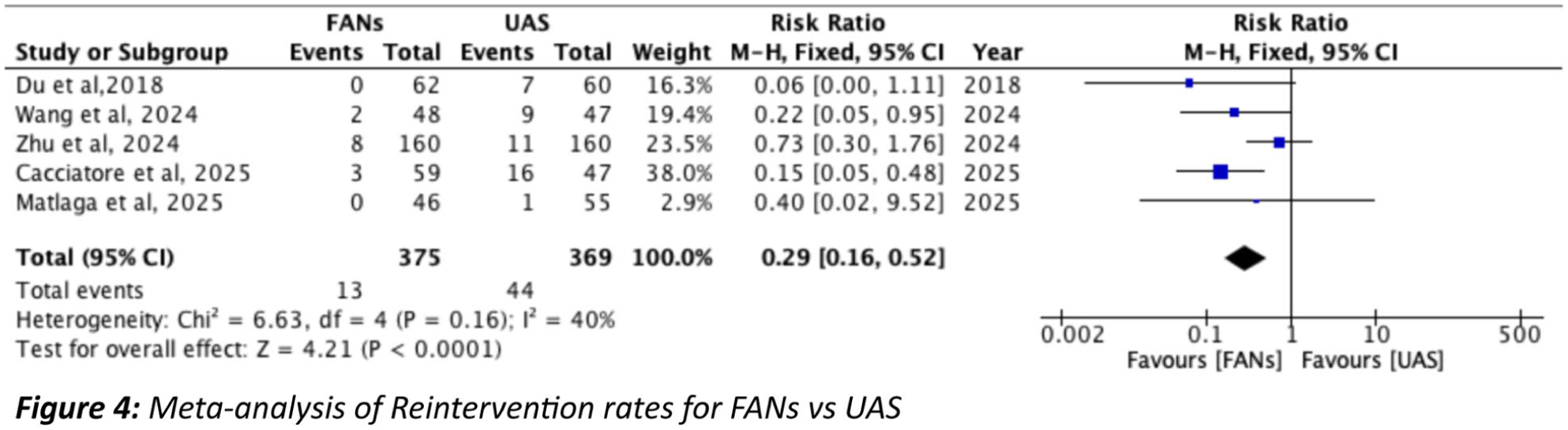
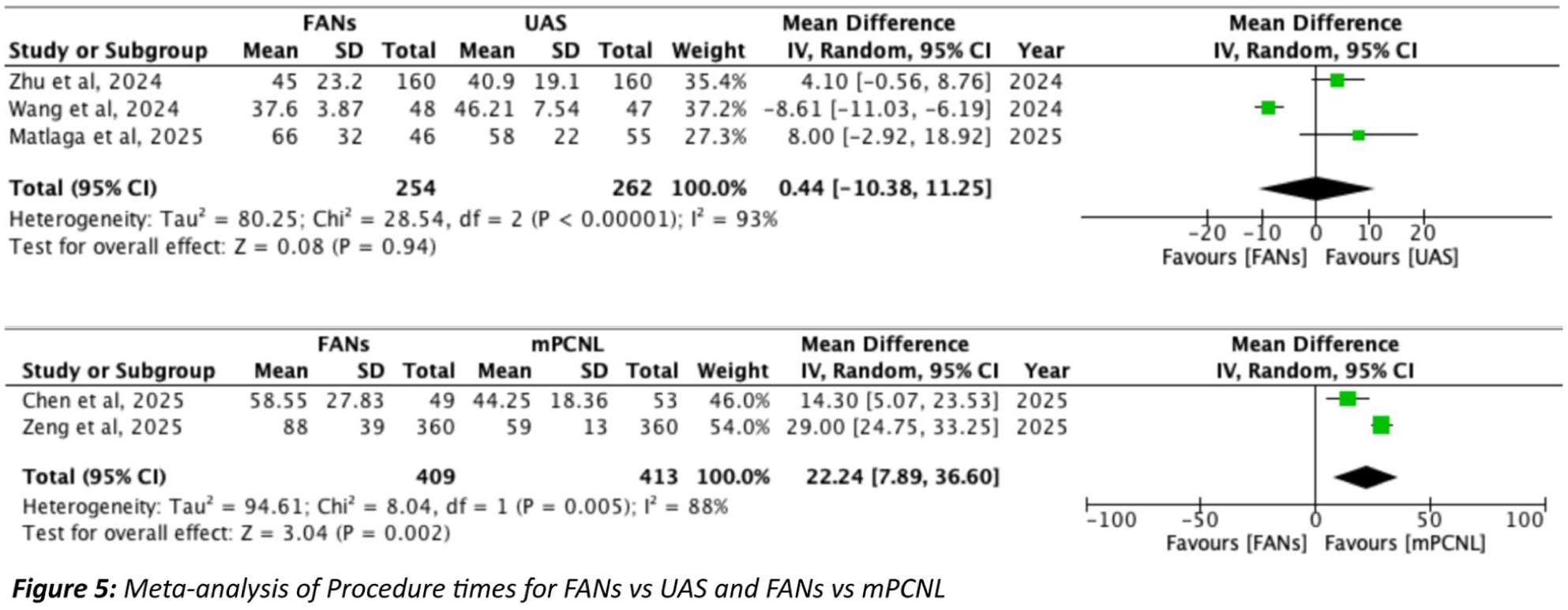
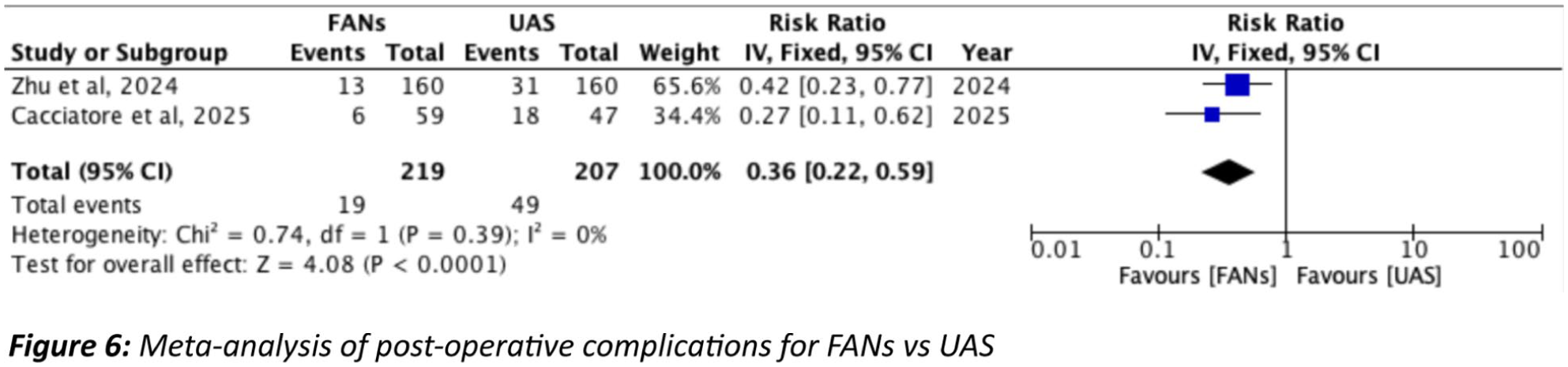
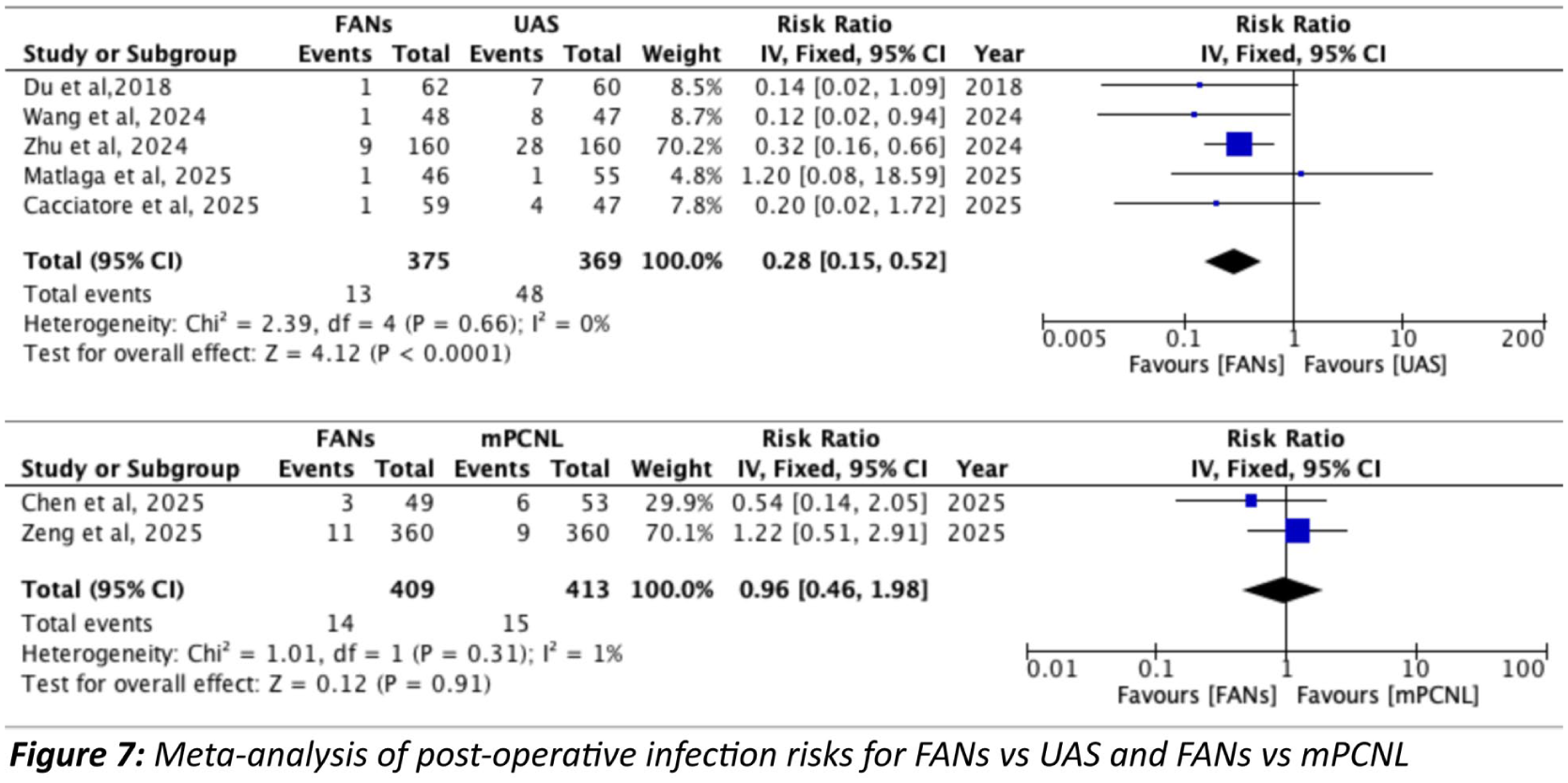


ePoster Session 11: Andrology 2, Paddy O’Reilly, June 16, 2026, 14:15 - 15:15
P11-1 Predictive Value of Flexible Cystoscopy for Late Stricture Recurrence Following Primary Bulbar Urethroplasty
Mr Efstathios PAPAEFSTATHIOU1, Mr Paul Anderson1
1Russells hall Hospital DGFT, UK, 53 Market St Kingswinford, United Kingdom
Introduction: Bulbar augmentation urethroplasty is the standard treatment for long bulbar urethral strictures, yet the prognostic value of early postoperative cystoscopic findings for late recurrence remains unclear.
Materials and methods: A retrospective analysis of 174 patients who underwent primary bulbar urethroplasty in a single centre was performed. Patients with stricture recurrence within the first two years or prior urethral reconstruction were excluded. All patients underwent flexible cystoscopy at two and five years postoperatively. The mean patient age was 59.2 ± 14.4 years. Failure was defined as need for intervention, urethral narrowing<16Fr or symptoms recurrence at five years. Variables analysed included age, total graft length, graft orientation (dorsal, ventral, or double-faced), stricture aetiology, and ISD. Univariate and multivariable analysis was performed.
Results: At a median follow-up of 25 months, 10 patients (5.7%) demonstrated urethral narrowing to 16 Fr. Over a median follow-up of 62 months, recurrence occurred in 20.0% of patients with early narrowing compared with 2.4% of those without narrowing (p = 0.003). Increased graft length was significantly associated with recurrence, whereas age, stricture aetiology, ischaemic spongiosum disease, and graft orientation were not. In multivariable analysis graft length and early urethral narrowing independently predicted five-year recurrence. Each additional centimetre of graft length increased recurrence risk by approximately 76%, while early narrowing conferred an elevenfold increased risk of subsequent failure.
Conclusions: A urethral calibre >16 Fr at 2-year cystoscopy is strongly predictive of durable long-term success, while longer grafts and early narrowing identify patients who may benefit from closer surveillance.
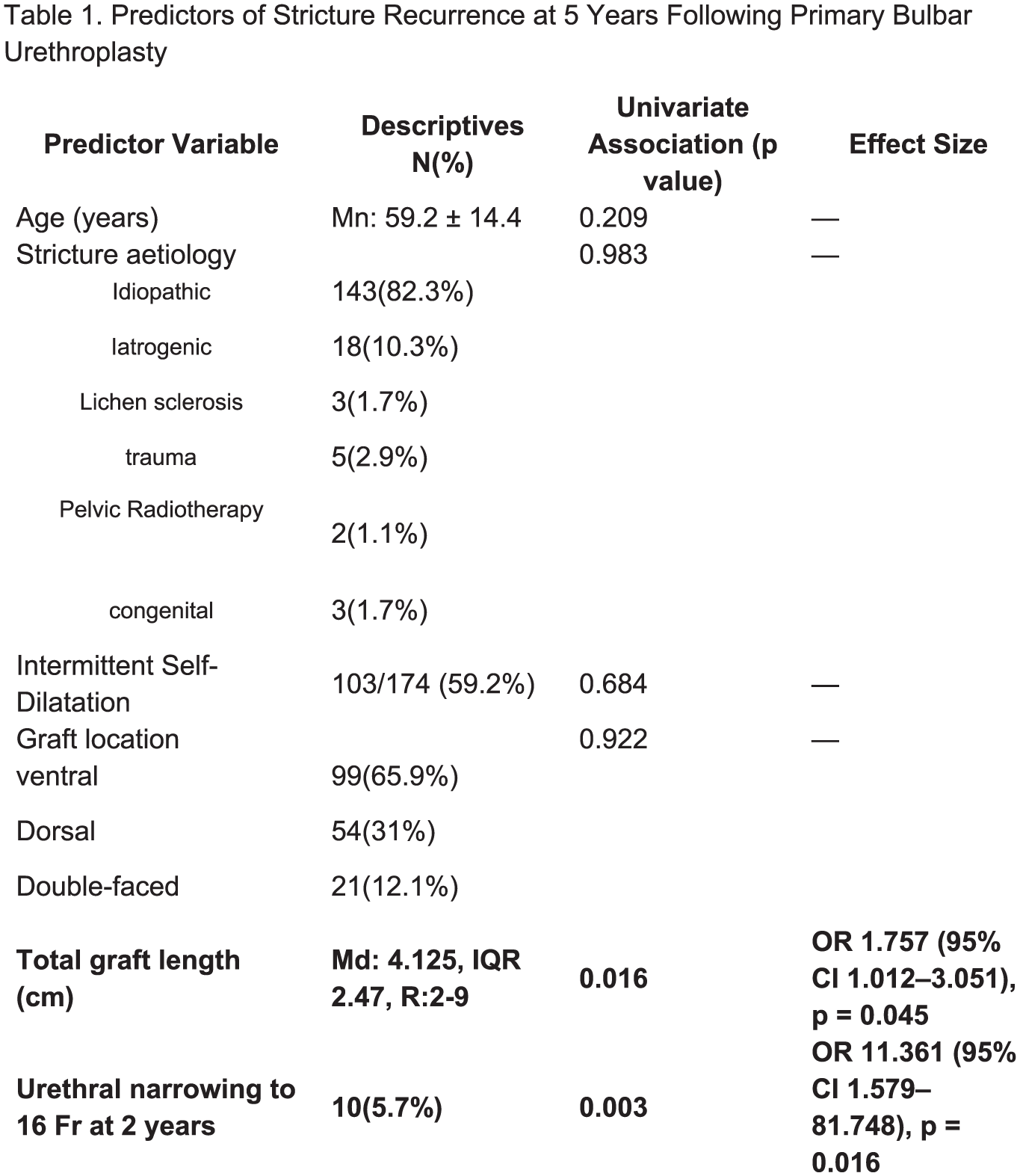
P11-2 When Surgery Isn’t an Option: Outcomes in Node-Positive Penile Squamous Cell Carcinoma (pSCC) Patients Unfit for Radical Inguinal Lymph Node Dissection (RILND)
Miss Catherine McCollum1, Miss Victoria Hyett4, Mr Cameron Boyle2, Miss Rebecca Huey2, Mr Ross Vint2, Mr Allan Johnston2, Mr Michael Fraser2, Mr David Hendry3, Mr Jonathan Salmond3, Mr Matthew Rewhorn2
1Forth Valley Royal Hospital, Falkirk, United Kingdom, 2Glasgow Royal Infirmary, Glasgow, United Kingdom, 3Queen Elizabeth University Hospital, Glasgow , United Kingdom, 4University Hospital Monklands, Lanarkshire, United Kingdom
Introduction: RILND is the standard of care for node-positive pSCC but carries substantial morbidity, with many unfit for surgery. We evaluated outcomes in node positive pSCC managed non-surgically.
Patients (or Materials) and Methods: Retrospective cohort study of 287 adults with new pSCC from 2017 to 2024, across four regional referral centres, was performed. Nodal status was determined pathologically on Sentinel lymph node biopsy, or radiologically with core node sampling. Demographics, treatment modalities, and survival outcomes were analysed.
Results: 85 patients (29.6%) presented with nodal disease (N1=31, N2=13, N3=41). Mean age was 65.6 (range 31–92), and 41.2% had palpable nodes. 12 patients with distant metastases were excluded. Median follow-up was 19.5 months.
56.5% underwent RILND; 18.8% received neoadjuvant systemic anti-cancer therapy (SACT) and 20.8% adjuvant radiotherapy. The remaining 43.5% were unfit for RILND and were managed with SACT plus radiotherapy (10.8%), radiotherapy alone (56.8%), SACT alone (10.8%), or supportive care (21.6%).
Kaplan–Meier analysis demonstrates superior survival with surgical management. Among non-surgical patients, SACT plus radiotherapy achieved the best outcomes, followed by radiotherapy alone, while supportive care yielded the poorest survival.
Recurrence rates were similar in surgical (31.7%) and non-surgical (30%) cohorts, although recurrence in non-surgical patients is likely underestimated, as 72.2% died from primary disease.
Conclusions: A substantial proportion of patients (43.5%) are unfit for RILND. Although SACT combined with radiotherapy appears to offer the best survival in this group, outcomes remain poor. Further research is required to optimize systemic therapies and improve prognosis for patients unsuitable for surgical nodal management.
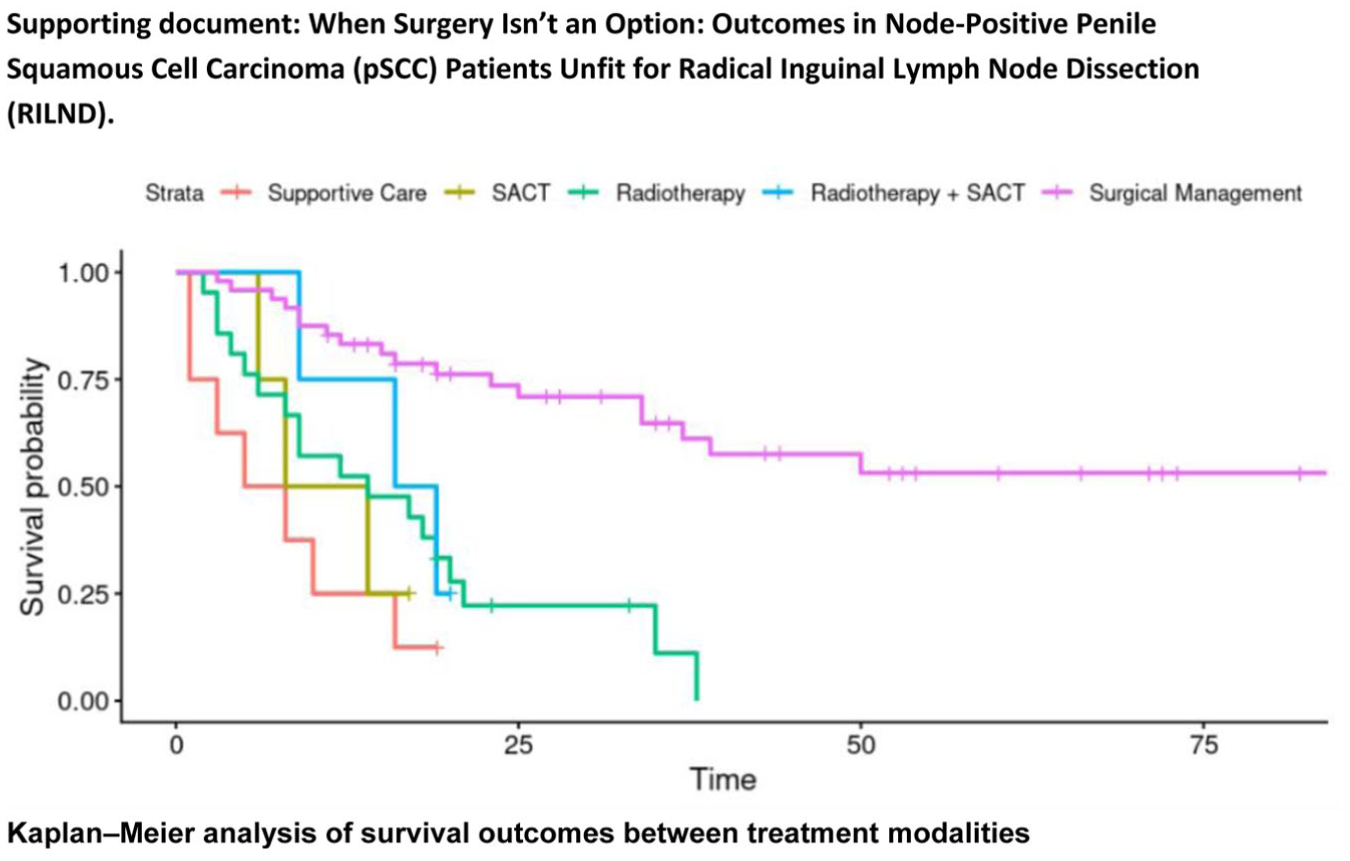
P11-3 High Body Mass Index Does Not Limit Semen Quality Improvement After Varicocele Repair
Mr Albert Wong1, Ms Isabel Dighero1, Ms Anam Salim2, Professor David Ralph1, Dr Miles Walkden1, Ms Philippa Sangster1
1University College London Hospital, London, United Kingdom, 2University College London, London, United Kingdom
Introduction: In the face of an abnormal sperm count, varicocele treatment can improve sperm parameters. However, when this is recognised in men who are obese, is the effect of varicocele treatment as effective? We set out to investigate whether a higher BMI influences the efficacy of varicocele treatment in improving semen parameters and negates the need for treatment.
Patients and methods: A retrospective study was carried out on consecutive varicocele embolisation (VE) and microsurgical varicocelectomy (MSV) from 2017-2025 at a single institution. Men who had repeat semen analysis 3 months after treatment and recorded BMI were included. BMI was analysed both as a linear and categorical variable (healthy weight, overweight and obese)
Results: Seventy-seven patients were included and the median BMI was 25.4. Thirty-one patients had BMI <25, 22 were overweight (25–30) and 31 were obese (>30). Median age was 36 and median pre-treatment testosterone was 15.7.
The median increase of total motile sperm count (TMSC) was 27.0 million/ejaculate (p = 0.025). A linear regression of ΔTMSC on BMI showed a negative but non-significant association between BMI and improvement in TMSC (p = 0.916). When stratified by BMI ⩽30 and >30, the association remained non-significant. The Kruskal–Wallis test comparing ΔTMSC across BMI categories (healthy, overweight, obese) also showed no significant difference (p = 0.857). There was no significant difference in ΔTMSC with and without hypogonadism.
Conclusion: In this single-institutional cohort, improvement in semen parameters after VE or MSV was not impacted by a BMI. Patients with BMI >30 also benefited.
P11-4 Lymph Node Ratio as an Independent Prognostic Factor for Overall Survival in Penile Cancer
Dr Cesare Saitta1, Mr Mahmoud Ziada1, Mr Adnan Ahmad1, Mr Paul Hadway1, Mr Raj Nigam1, Mr Varun Sahdev1, Mr Hussain Alnajjar1, Prof Asif Muneer1
1Male Genital Cancer Centre, Department of Andrology, University College London Hospitals, London, United Kingdom
Introduction: Identification of regional metastatic disease after lymph node dissection (LND) in penile cancer may improve prognostic stratification. We evaluated the prognostic value of lymph node ratio (LNR; positive nodes/total nodes removed) for overall survival (OS) and explored the association between extent of dissection and number of positive nodes.
Methods: From a single-centre institutional database, we identified patients undergoing radical inguinal and/or pelvic LND for penile cancer. Primary outcome was all-cause mortality (ACM). Multivariable Cox regression assessed predictors of ACM. The number of positive nodes was modelled against the total number of bilateral nodes removed and clinicopathological covariates using linear regression. A multivariable logistic regression model estimated adjusted marginal probabilities of death across increasing LNR values.
Results: Overall, 556 patients were analysed (median follow-up 99 months; IQR 71–146). On multivariable Cox analysis, higher LNR (HR 2.61; p=0.023), lymphovascular invasion (LVI; HR 2.55; p<0.001) and extranodal extension (ENE; HR 4.61; p<0.001) were independently associated with increased ACM. In linear regression, the total number of nodes removed correlated with the number of positive nodes (β 0.125 per node; p<0.001), and LVI remained associated with nodal positivity (β 0.571; p=0.042). In logistic regression, ENE (OR 5.72; p<0.001) and LVI (OR 2.97; p<0.001) were associated with higher mortality at 5 years. Marginal predictions showed a dose–response relationship, with adjusted mortality increasing from 13% at LNR=0 to 27% at LNR=1.
Conclusions: LNR is an independent prognostic factor and demonstrates a consistent dose–response association with adjusted mortality.
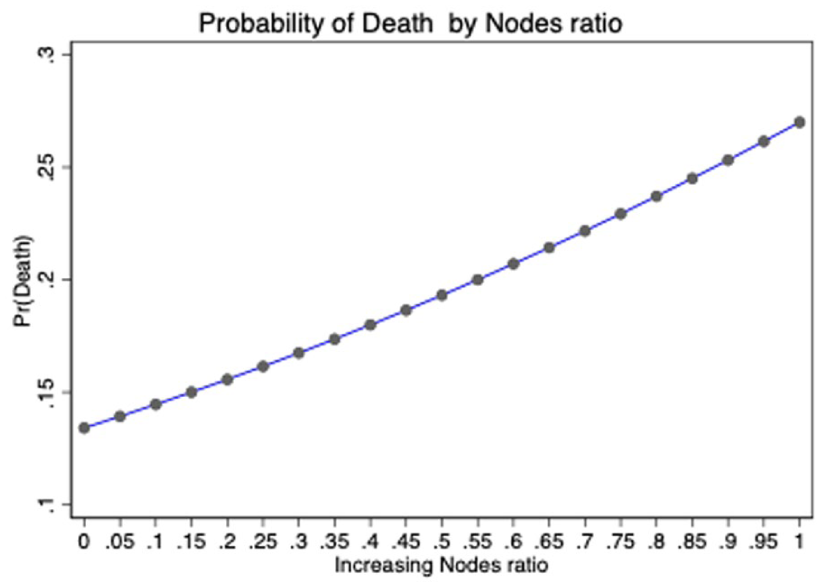
P11-5 Human papillomavirus Status as a Prognostic Marker in Penile Cancer
Miss Catherine McCollum1, Miss Victoria Hyett4, Mr Cameron Boyle2, Miss Rebecca Huey2, Mr Ross Vint2, Mr Allan Johnston2, Mr Michael Fraser2, Mr David Hendry3, Mr Jonathan Salmond3, Mr Matthew Rewhorn2
1Forth Valley Royal Hospital, Falkirk, United Kingdom, 2Glasgow Royal Infirmary, Glasgow, United Kingdom, 3Queen Elizabeth University Hospital, Glasgow, United Kingdom, 4University Hospital Monklands, Lanarkshire, United Kingdom
Introduction: Human Papillomavirus (HPV) is a recognised risk factor for penile cancer, however prognostic significance of HPV status varies across literature. In this study we evaluated the staging and prognostic implications of HPV-associated and HPV-independent squamous cell carcinoma of the penis (pSCC).
Patients (or Materials) and Methods: A retrospective cohort study was conducted, including all adults with newly diagnosed pSCC between 2017 and 2024, across four regional referral centres. HPV status was determined using p16 immunohistochemistry. Demographic, pathological, treatment, and survival data were analysed.
Results: 125 patients with HPV status assessed were identified. HPV status breakdown was: 77 positive (62%), 44 negative (35%), and 4 inconclusive (3%). Median follow-up was 20.5 months. Patients with HPV-independent disease presented with higher Tumour stage (p = 0.03), although nodal and metastatic burden did not differ significantly (p = 0.90 and p = 0.41, respectively). More extensive surgical intervention was required in HPV-independent cases, with 63.4% undergoing partial or total penectomy compared with 35.6% of HPV-associated cases. Kaplan-Meier curve shows overall survival between the two groups with HPV-associated disease demonstrating superior overall survival (p=0.02)
Recurrence rates were similar, with a rate of 18.6% in HPV-associated cases and 25.6% in HPV-independent cases.
Conclusions: HPV status is an important prognostic marker in patients with pSCC. HPV-associated disease presented with lower Tumour stage, required less extensive surgical resection, and demonstrated superior overall survival compared with HPV-independent disease. These findings highlight the importance of routine HPV status testing in pSCC to improve risk stratification and guide treatment planning.
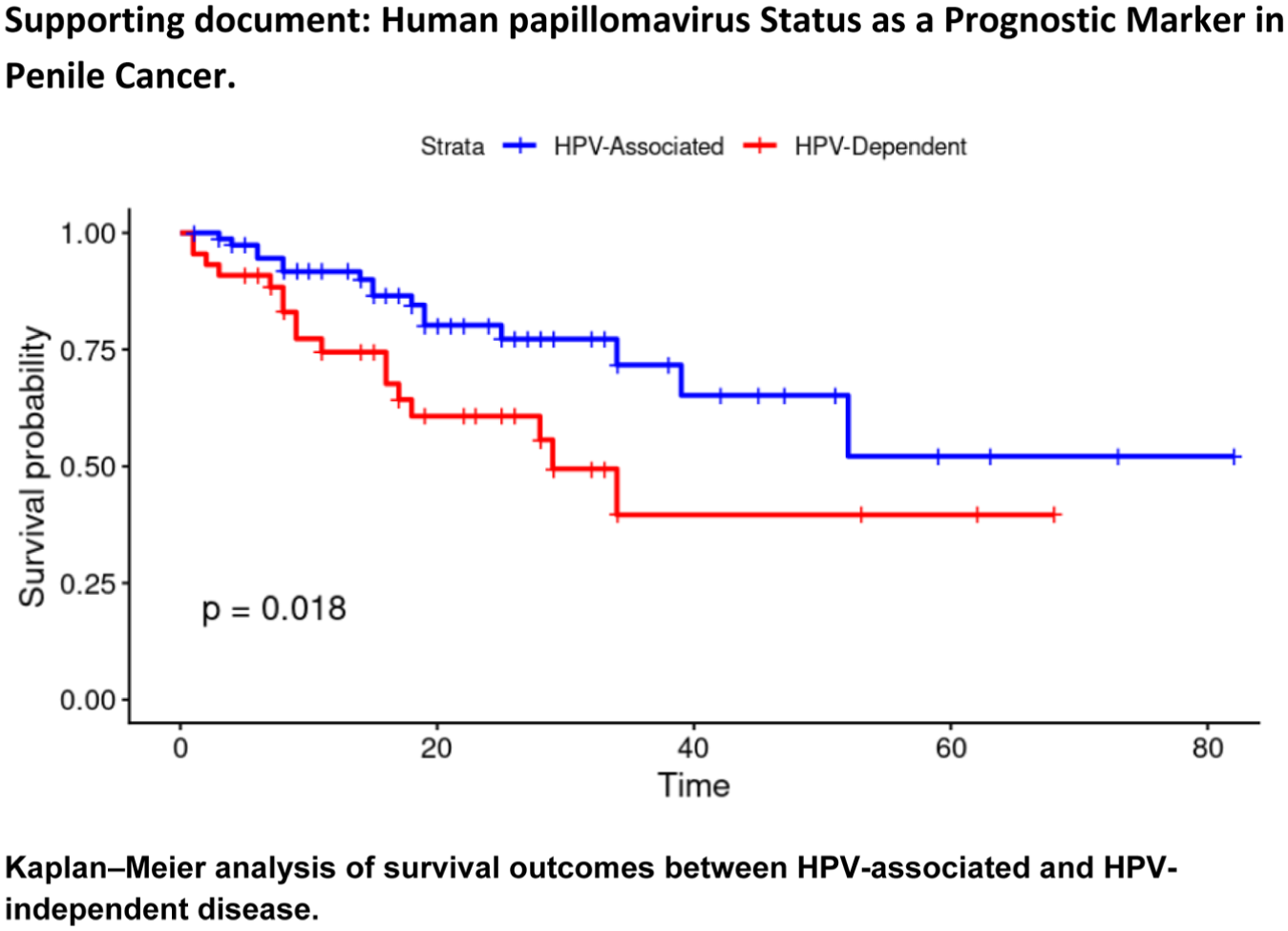
P11-6 Preoperative sexual dysfunction in south asian men undergoing radical prostatectomy: An overlooked contributor topostoperative erectile outcomes
Dr Mukkani Velan1, Dr Vilvapathy karthikeyan1, Dr Kuldeep Sardana1, Dr Madhav Tiwari1, Dr Narasimhan Ragavan1, Dr Sandeep Bafna1
1Apollo Hospitals, Chennai, India
Introduction: Erectile dysfunction (ED) is a common complication after radical prostatectomy (RP), with reported rates varying widely. However, baseline sexual dysfunction in South Asian men is poorly documented due to cultural taboos and limited use of validated tools. Applying Western potency outcomes without accounting for pre-existing dysfunction may overestimate surgical morbidity. This study aimed to objectively assess baseline erectile function in Indian men undergoing RP using the Sexual Health Inventory for Men (SHIM) and Erectile Hardness Score (EHS), and to analyse associations.
Materials & Methods: This prospective observational study included 70 men planned for RP for localised or locally advanced prostate cancer were included after ethics approval and informed consent . Preoperative evaluation included SHIM, EHS, stretched penile length (SPL), sexual activity in the past six months, partner interest, and willingness for postoperative rehabilitation. Statistical analysis was performed using SPSS v25; p < 0.05 was considered significant.
Results: Mean age was 64.6 ± 8.2 years; 48.6% had hypertension and 44.3% diabetes. Mean SHIM was 17.4 ± 4.0, EHS 2.7 ± 0.8, and SPL 11.4 ± 1.6 cm. Overall, 80% had some degree of ED, and only 28.6% achieved EHS ⩾ 3. Sexual inactivity (62.9%), partner disinterest (58.5%), and willingness for rehabilitation (5.7%) were low. Age negatively correlated with SHIM and EHS, while SHIM correlated positively with SPL.
Conclusions: Most South Indian men undergoing RP have significant pre-existing sexual dysfunction and low rehabilitation readiness. Routine preoperative SHIM and EHS assessment is essential for realistic counselling and postoperative expectation setting.
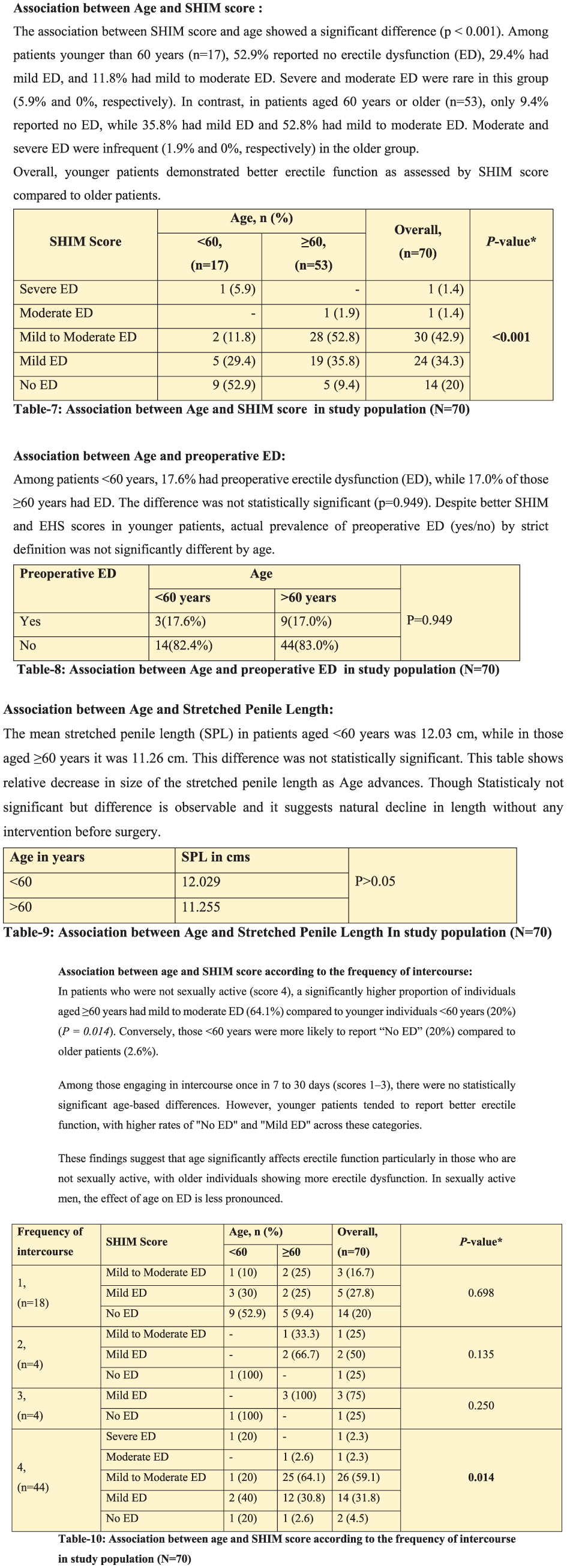
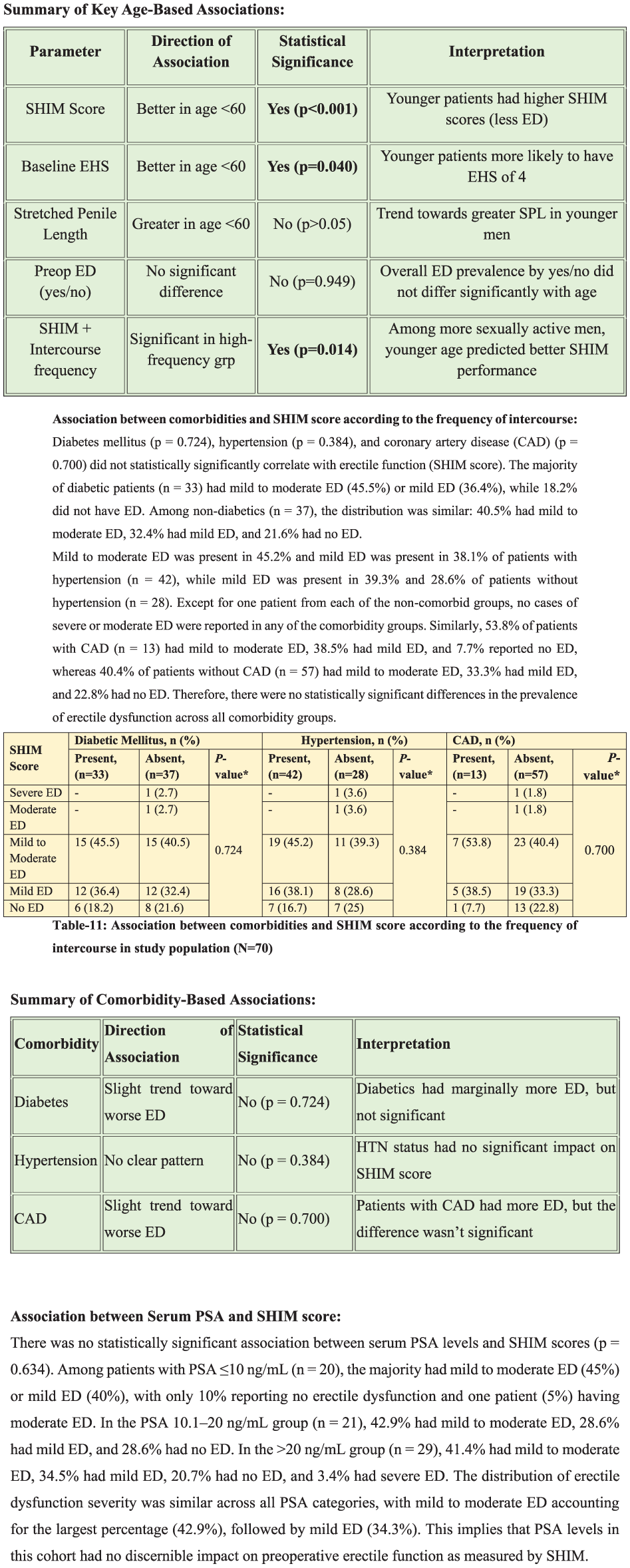
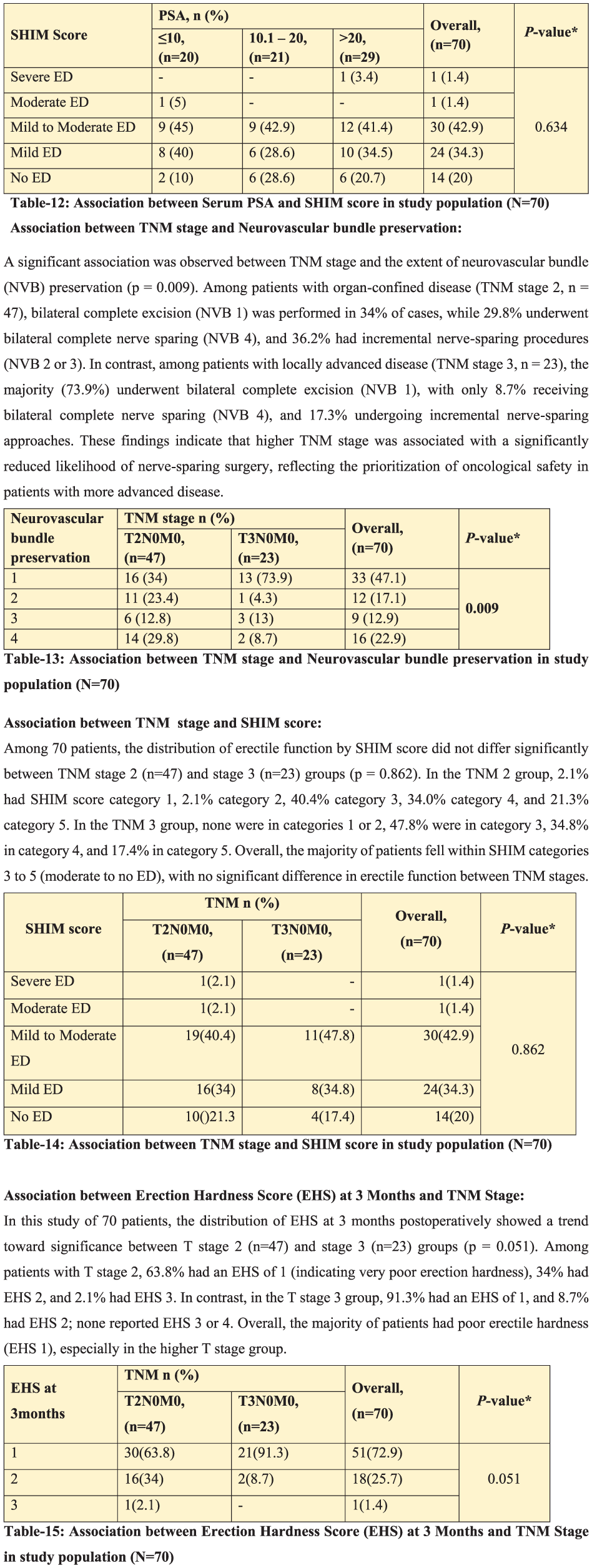
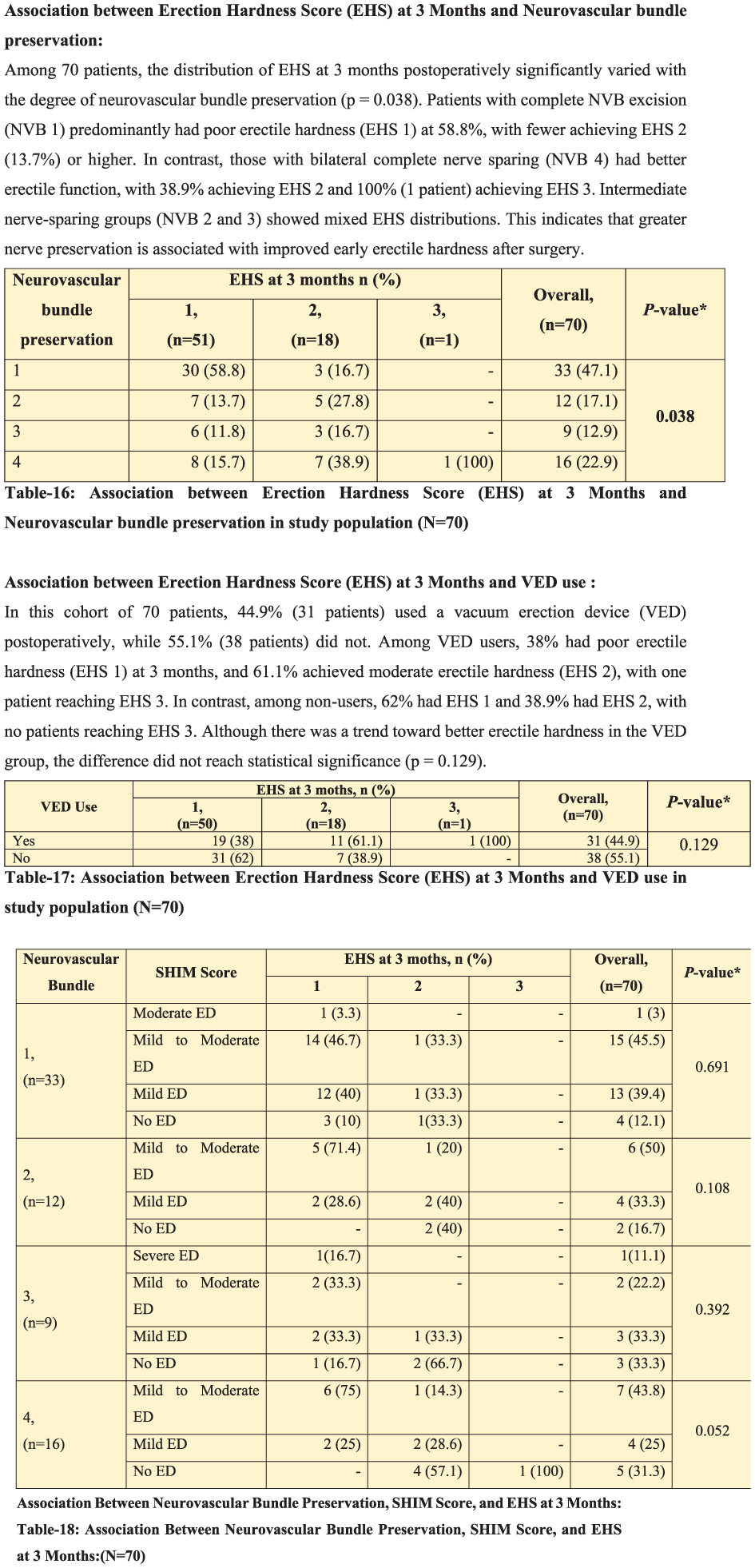
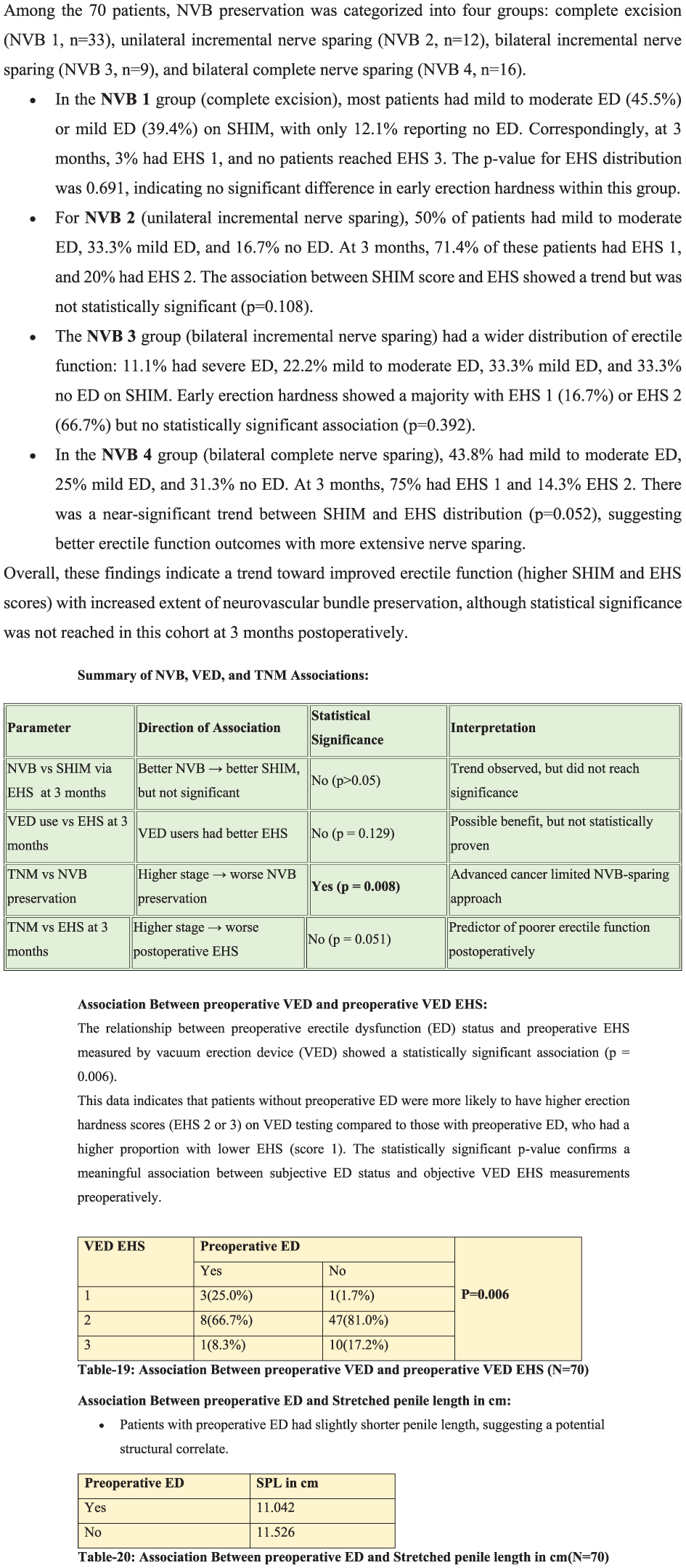
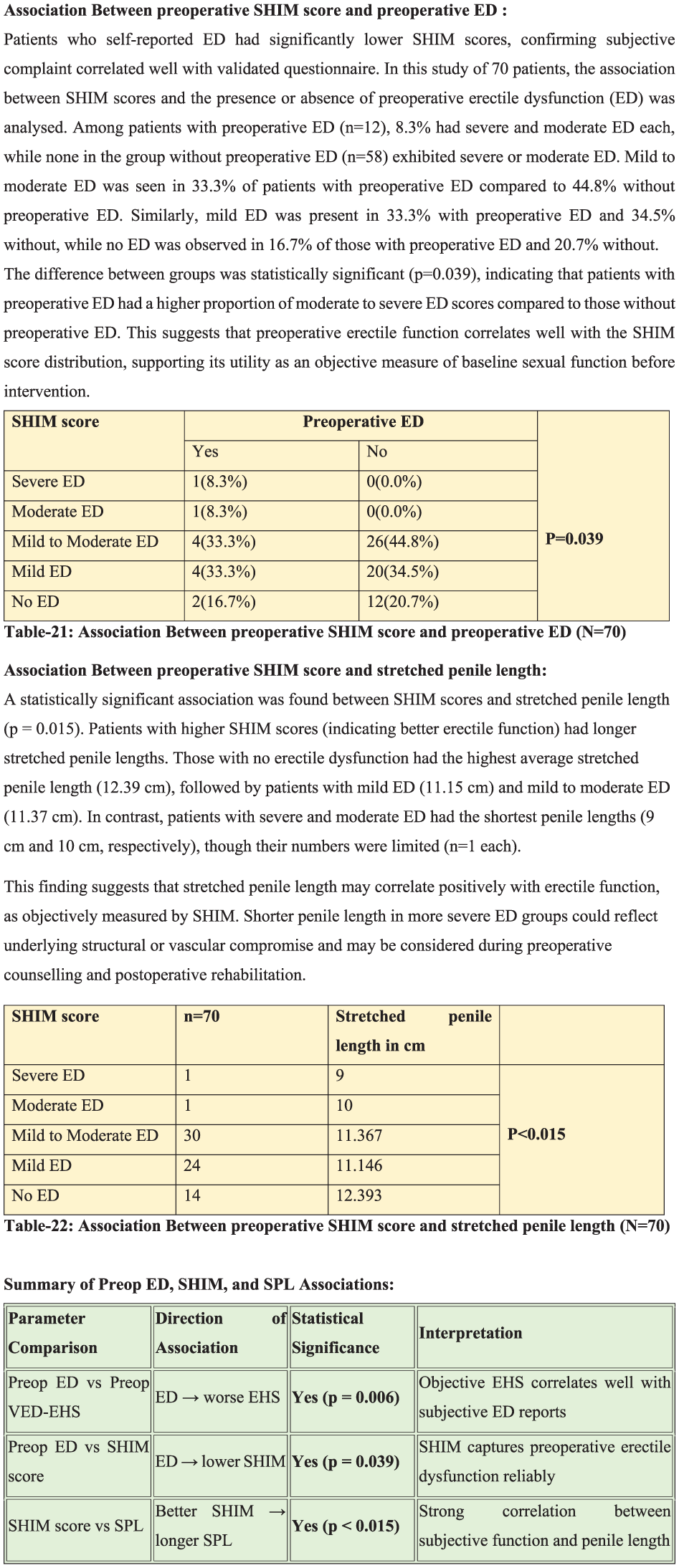
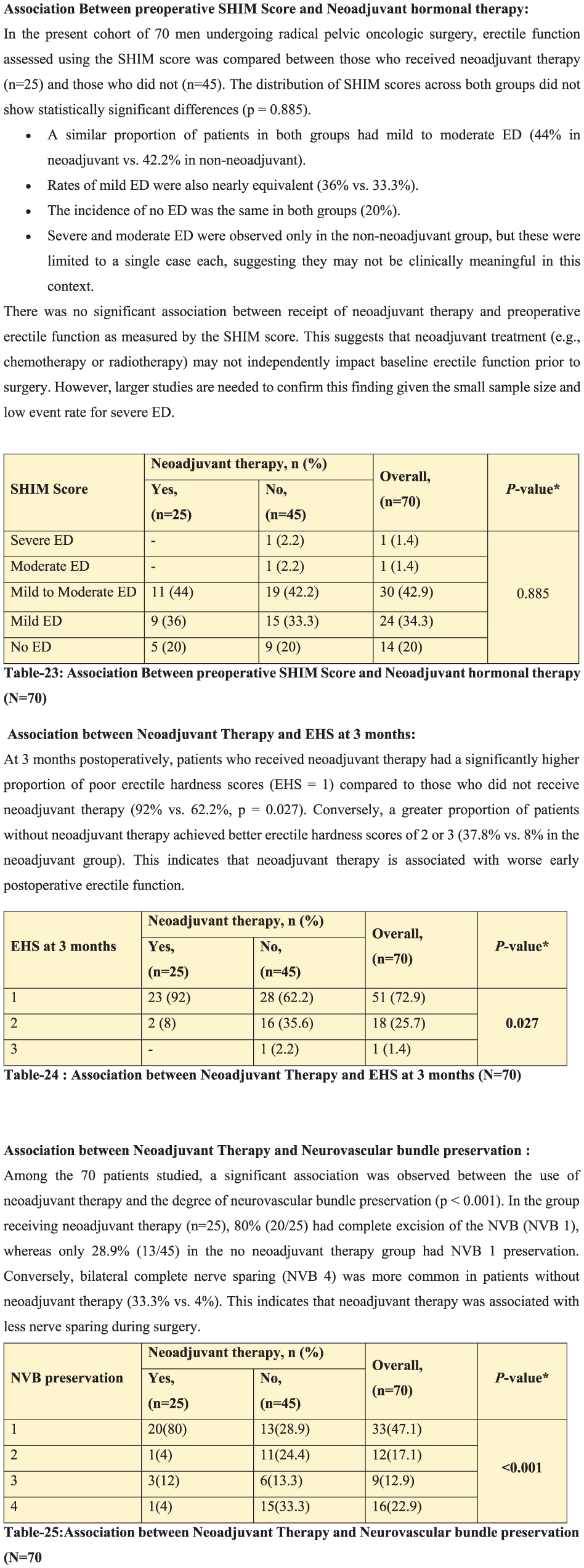
P11-7 Comparative Outcomes of T Shunt and Penoscrotal Decompression in Ischaemic Priapism
Mr Abdullah Al-Mitwalli1, Ms C Pozo1, Mr R Aldarrab1,2, Mr A Gobbo1, Mr J Lindsay1, Mr A Wong1, Dr A Wan1, Dr M Gosalia1, Mr M Shah1, Ms P Sangster1, Mr W.G Lee1, Prof David Ralph1
1Uclh, London, United Kingdom, 2King AbdulAziz Medical City, Riyadh, Saudi Arabia
Introduction: T shunts (TS) and penoscrotal decompression (PSD) remain established surgical options for corporal drainage in cases of ischaemic priapism. Despite timely intervention, a substantial proportion of patients progress to erectile dysfunction, ultimately requiring penile prosthesis implantation. To date, there are no comparative studies evaluating TS versus PSD.
Patients: Retrospective cohort study of patients with ischaemic priapism requiring surgical intervention after failed conservative management (aspiration + phenylephrine) (2013-2025), comparing TS and PSD. Data collected included successful detumescence, postoperative pain, corporal histology and imaging, erectile dysfunction, and penile prosthesis implantation.
Results: To date, 26 patients underwent PSD. Mean age was 40.5 years (SD 12.5), with 85% undergoing bilateral PSD and the remainder unilateral. The mean duration of ischaemia prior to PSD was 53.7 hours (SD 34.4). Initial successful detumescence was achieved in 96% of patients, and corporal biopsies were obtained in 81%. Recurrent priapism occurred in 8 (31%). Thirteen patients (50%) had penile prosthesis.
To date, 45 patients underwent TS. Mean age was 41.7 years (SD 12.0), with a mean ischaemic duration of 87.2 hours (SD 74.7) prior to intervention. Initial successful detumescence was achieved in 38% of patients. Corporal biopsies were obtained during TS in 98% of cases. Ultimately, 33 (73%) required prosthesis.
Conclusion: Both TS and PSD are surgical options for ischaemic priapism. PSD was associated with higher detumescence rates and fewer subsequent penile prosthesis implantations than TS, although this is likely influenced by longer ischaemic duration in TS. Larger, propensity-matched studies are required to better compare outcomes.
P11-8 Long term sexual and urinary outcomes following penile fracture repair
Mr Charles Katz-summercorn1, Mr Abdullah Al-Mitwalli, Mr Mohammad Shah, Mr M Nasser, Mr B. Chua, Mr S. Pinni, Mr James Banerjee, Miss P. Sangster, Mr W.G. Lee, Professor D. Ralph
1Whittington Hospital, London, United Kingdom
Introduction: Penile fracture (PF) is a urological emergency resulting from rupture of the tunica albuginea of the corpora cavernosa that may occur with concomitant urethral injury occurring in up to 15% of cases. Early surgical repair is essential to restore anatomical and functional integrity. This study assesses long-term functional outcomes, including erectile function, penile deformity, plaque formation, and urethral complications.
Materials and Methods: All patients who underwent PF repair at a tertiary referral centre were contacted to complete validated questionnaires (IIEF-EFD and IPSS). Additional questions assessed penile curvature.
Results: 108 men responded. The mean age at PF was 41 years. 20% cases had bilateral corporal injury whilst remaining 80% had unilateral corporal fracture. A urethral injury was identified and repaired in 29 (27%) of cases. The mean IIEF-6 and IPSS scores for all patients were 25.3 (6.5) and 2.9 (4.6), respectively. There was no statistically significant difference in IIEF-6 and IPSS scores between patients with or without urethral injury. PDE5i usage was reported in 17 patients overall (15.7%), with no significant difference between groups (p=0.07). Penile curvature was reported in 34 patients (31.5%), of whom the majority described minimal curvature. No patients required urethral surgery during follow-up. The flowrates and urethrograms are pending for those with urethral injuries.
Conclusions: Timely surgical repair of penile fractures preserves erectile function and does not increase the risk of urethral stricture disease. Around one-third of patients report some degree of penile curvature following repair, though most cases are mild.
P11-9 Premature Ejaculation in the United Kingdom: A Nationwide Survey exploring Insights into Contemporary Urology Practices
Dr Imaad Amanulla1, Mr Mohamed Mubarak1, Professor Vaibhav Modgil1, Miss Theodora Stasinou1, Professor Ian Pearce1
1Manchester Andrology Research Collaborative (MARC), Manchester, United Kingdom
Background: Premature ejaculation (PE), a common male sexual dysfunction has established diagnostic and management pathways proposed by international expert bodies. However, real-world practice varies. This study presents the first nationwide assessment of UK urologists’ perceptions and management of PE, focusing on alignment with consensus recommendations.
Patients and Methods: A cross-sectional study was conducted, using anonymised electronic questionnaires distributed to UK urology clinicians following BAUS 2025. Data collected included clinician demographics, clinical exposure to PE, diagnostic criteria used, and treatment strategies. Descriptive statistics were applied.
Results: Sixty-six responses were analysed. Half of respondents were general urologists, and clinical exposure to PE was limited; 37.9% reported no PE cases in the preceding three months. Diagnostic approaches varied; patient-reported concern was most used (49.2%), followed by International Society for Sexual Medicine (33.8%) and American Urological Association/Sexual Medicine Society of North America (12.3%) definitions. Objective assessment of intravaginal ejaculatory latency time was inconsistent; 10.9% used formal timing strategies.
Dapoxetine was the commonest prescribed therapy (71.2%), followed by topical anaesthetics (56.1%) and phosphodiesterase-5 inhibitors (34.8%). 33.6% of respondents reported at least one patient requesting invasive treatment; however, invasive procedures were rarely considered, with 96.9% reporting no referral. Barriers included insufficient evidence, and no guideline endorsement; 98.5% of respondents felt current guidelines do not reflect real world challenges in managing PE.
Conclusion: UK urologists demonstrate substantial variability in PE diagnosis and management, with heterogeneous alignment to consensus-based frameworks. These findings highlight implementation gaps and underscore the need for clearer national guidance given the prevalence of PE.
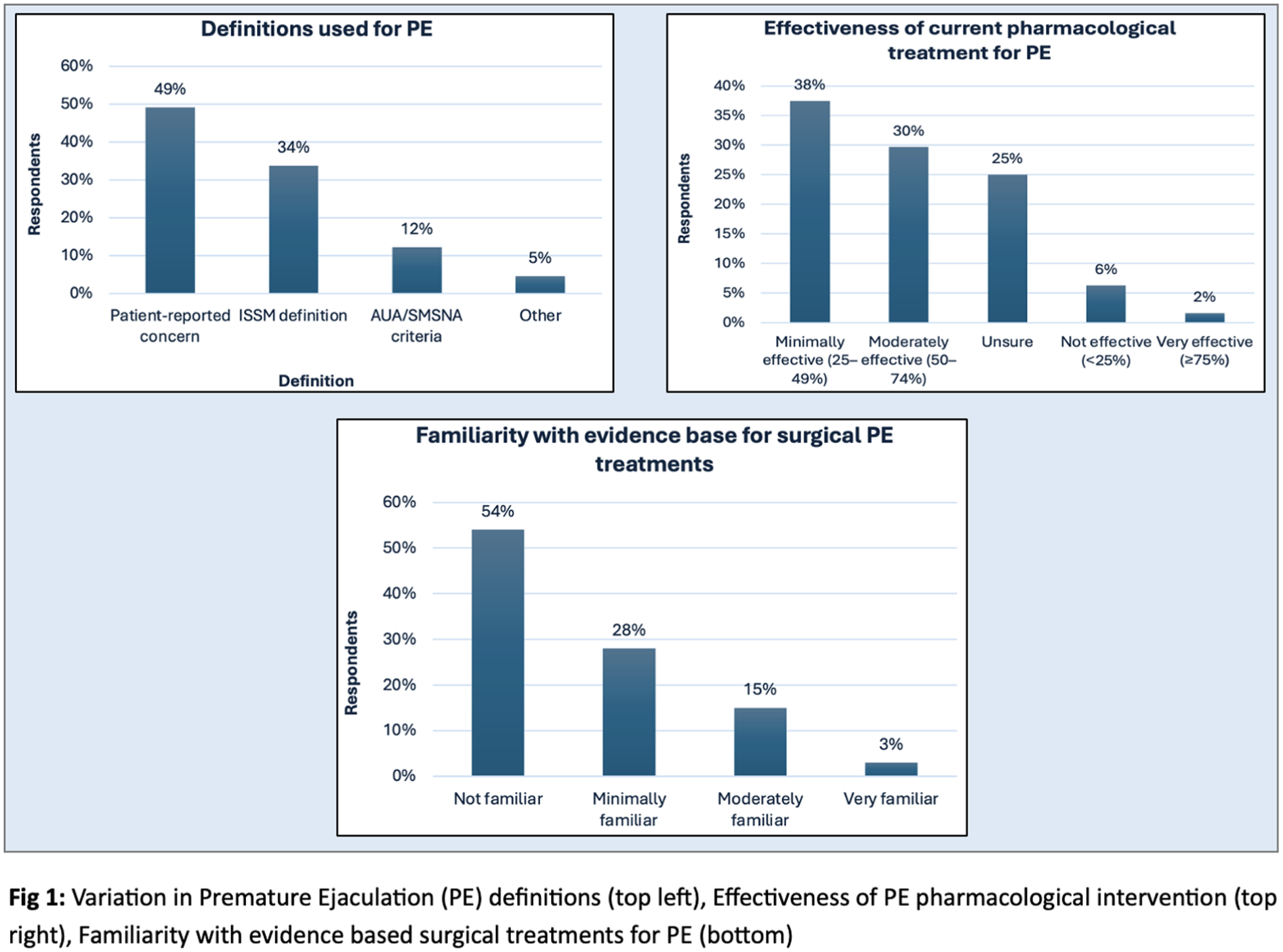
P11-10 Rising incidence of penile squamous cell carcinoma (PSCC) and p16 distribution trends: A retrospective single-centre analysis from 2013 to 2023
Joecelyn Kirani Tan2, Dr Xu Xuan Lim1, Dr Nathanael T Tuffa2, Rosalind Walsh2, Mr Kenneth Paterson1, Dr Diego Sanchez2, Dr Pedro Oliveira1, Mr Ashwin Sachdeva1, Mr Arie Parnham1, Prof Vijay Sangar1
1Christie Hospital, Manchester, United Kingdom, 2University of Manchester, Manchester, United Kingdom
Introduction and objectives: Although PSCC is rare, recent observations suggest a gradual increase in its incidence. The 2016 WHO classification introduced HPV-associated and HPV-independent PSCC, with p16 immunohistochemistry (IHC) serving as a surrogate marker for HPV involvement. Understanding the temporal and clinicopathological trends of these subtypes may provide insight into evolving disease epidemiology and biology.
Methods: 800 patients diagnosed with PSCC between 2013 and 2023 were analysed. All cases were reviewed for p16 IHC status and clinicopathological features. Annual case counts were assessed using Poisson regression to evaluate changes in incidence over time, expressed as the compound percentage annual (CPA) change. Comparative analyses were performed for p16+ and p16- tumours, including age, grade, stage, and follow-up outcomes.
Results: The mean age at diagnosis was 66 ± 13 years (range: 25-97). Annual diagnoses increased from 43 in 2013 to a peak of 95 in 2019 (120% rise), followed by a modest decrease to 76 in 2023. The overall CPA indicated a significant 5.6% increase in PSCC diagnoses per year (95% CI: 3.31-7.98; p = 1.24 × 10-6). There was a higher annual increase among p16-negative cases (8.27%) compared to p16-positive cases (5.48%), though not statistically significant (p = 0.261)
Conclusions: We observed a significant year-on-year increase in penile carcinoma diagnoses, with parallel rises across both HPV-associated and HPV-independent subtypes. These findings highlight an evolving disease landscape that warrants further investigation into contributing epidemiological and environmental factors, as well as implications for screening and prevention strategies.
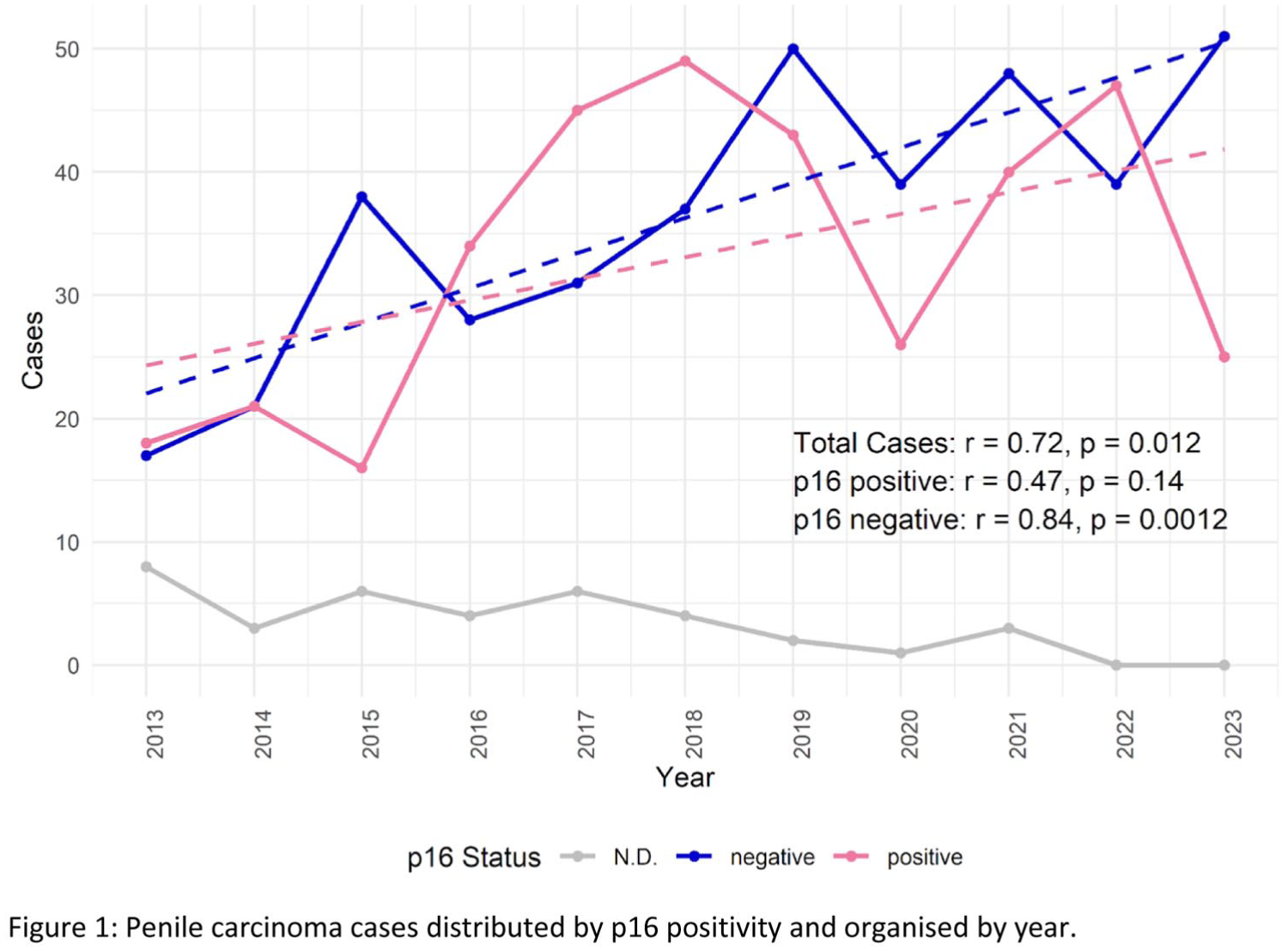
ePoster Session 12: Functional Urology & Neuro-Urology Bladder Dysfunction and Reconstruction 2, Paddy O’Reilly, June 16, 2025, 15:45 - 16:45
P12-1 Safety and Efficacy of Sacral Neuromodulation During Pregnancy: A 15-Year Review from a Single High-Volume UK Centre
Ms Julie Jenks1, Mr Chase Peng Yun Ng1, Dr Vishnu Shadananan1, Ms Rachel Barratt1, Mr Richard Nobrega1, Mr Anthony Noah1, Ms Helena Gresty1, Mr Jeremy Ockrim1, Ms Tamsin Greenwell1, Ms Mahreen Pakzad1
1University College London Hospital, London, United Kingdom
Introduction: Sacral neuromodulation (SNM) is an established therapy for refractory overactive bladder (OAB) and non-obstructive urinary retention (NOUR). In the current literature there are no reports of harm to mother or foetus from active SNM during pregnancy. However, manufacturers advise deactivation during pregnancy. This may lead to recurrence of lower urinary tract symptoms and reduced quality of life.
Methods: A retrospective review was conducted of female patients with SNM implants who became pregnant between 2010 and 2025 at a single U.K centre. Data collected included demographics, indication for implant, device status during pregnancy, mode of delivery, foetal abnormalities, impedance values post-partum, and device-related complications.
Results: Twelve women underwent 13 pregnancies (Table 1). Indications were NOUR (n=8) and OAB (n=4). Four patients maintained active stimulation throughout pregnancy, against medical advice while eight deactivated their device. Delivery was via caesarean section (n=6) or vaginal birth (n=6); one patient delivered twins. No foetal abnormalities were reported. Post-partum impedance was normal in eight patients; one patient developed abnormal impedances, and three were not assessed. Two devices were explanted due to loss of efficacy, unrelated to pregnancy.
Conclusion: SNM appears safe for mother and foetus during pregnancy, irrespective of device status. No adverse obstetric, foetal or neonatal outcomes were observed. Larger multicentre studies are required to validate these findings and inform consensus on whether SNM can remain active during pregnancy. We propose pooling data from all U.K. SNM Centres via the UK SNS Working group.
P12-2 Long-Term Outcomes of Permanent Sacral Neuromodulation in Patients with Functional Neurological Disorder
Mr Stefanos Agiotakis1, Mr Anastasios Natsos1, Dr Aung Thant1, Ms Paraskeve Granitsiotis1, Mr James Blackmur1
1Western General Hospital, Edinburgh, United Kingdom
Introduction: Functional Neurological Disorder (FND) is increasingly recognized as a contributor to voiding dysfunction (VD). To date, outcomes of sacral neuromodulation (SNS) for VD in patients with FND have not been studied. We performed a retrospective analysis of our tertiary centre’s experience to evaluate long-term outcomes.
Methods: We retrospectively reviewed all patients with neurologist-diagnosed FND who underwent permanent SNS implantation at our centre between 2020 and 2025. Primary outcomes were defined as reduction or cessation of clean intermittent self-catheterisation (CISC) for VD, or symptomatic improvement for detrusor overactivity (DO). Secondary outcomes included pain, device complications, revisions, explantations and presence of psychiatric comorbidities.
Results: 72 patients with permanent SNS were followed for ⩾1 year. 10 patients with FND were identified. All were female, with a mean age of 39.2 years, and had normal MRI imaging. Nine patients had VD and one had DO. Overall, 3/10 patients (30%) achieved a successful outcome. Among the seven unsuccessful cases (70%), two underwent explantation due to bladder pain, one required suprapubic catheterisation and three had no change in CISC requirements. One patient had reduced CISC frequency but developed pain and overactive bladder symptoms. Additional psychiatric comorbidities were present in 7/10 patients.
Conclusion: SNS in patients with FND demonstrates a lower success rate (30%) compared with reported outcomes in the general patient population with VD. High rates of pain, revision, and treatment failure underscore the need for careful patient selection and comprehensive counselling through multidisciplinary management.
P12-3 A Structured Management Protocol to Sustain Sacral Neuromodulation (SNM) for Lower Urinary Tract Dysfunction: 8-Year Outcomes
Mr Chase Peng Yun Ng1, Ms Julie Jenks1, Miss Maryam Imran2, Miss Amelia Snook2, Dr Vishnu Shadananan3, Dr Tawa Audu3, Ms Helena Gresty1, Ms Tamsin Greenwell1, Mr Jeremy Ockrim1, Ms Mahreen Pakzad1, Mr et al .1, Mr et al .1, Mr et al .1, Ms et al .1
1Functional, Reconstructive and Adolescent Urology, University College London Hospital, London, United Kingdom, 2University College London Medical School, United Kingdom, 3Department of Urology, University College London Hospital, United Kingdom
SNM is an established therapy for refractory overactive bladder (OAB) and non-obstructive urinary retention (NOUR). However, its maintenance can be limited by adverse events (AEs) which are under-reported. We report the long-term outcomes of SNM following a structured management protocol.
This is a prospective, single-centre cohort study of OAB/NOUR patients who received permanent SNM (Medtronic and Axonics) after a successful tined-lead trial between 2013 and 2022. AEs included return of symptoms and complications (battery site pain, lower limb pain and infection). Management protocol included reprogramming (basic, advanced, and salvage) and operations (battery-site steroid injection; battery re-siting and explantation). Primary outcome was therapeutic success (⩾50% clinical improvement); secondary outcomes were AE and reoperation rates. Kaplan–Meier survival and multivariable Cox regression analyses were performed with missing data imputed.
Of 579 patients trialled, 400(69%) received permanent SNM (OAB, n=208; NOUR, n=192). The median follow-up was 6.3(IQR:3.7-8.4) years. The 8-year therapeutic success was 52.3% (95%CI:46.5–68.8%), with 165(41%) devices explanted at median of 8.4(IQR:7.5-10.2) years. The 8-year AE and reoperation cumulative incidences were 82.5% and 57.0% respectively. Male gender negatively predicts AE (HR0.68, 95%CI:0.49,0.94, p=0.018), whereas age, maximal urethral closure pressure, detrusor overactivity, bladder capacity, post-void residual did not predict therapeutic success or AE. Success rates were 44%, 33%, and 21% for basic, advanced, and salvage reprogramming; 71% for battery re-siting, and 58% for battery-site steroid injection.
Eight years following implant, over half of the patients maintained SNM benefit; 4 in 5 experienced ⩾1 AE; and 1 in 2 required reoperation. A structured management protocol improves SNM long-term effectiveness.
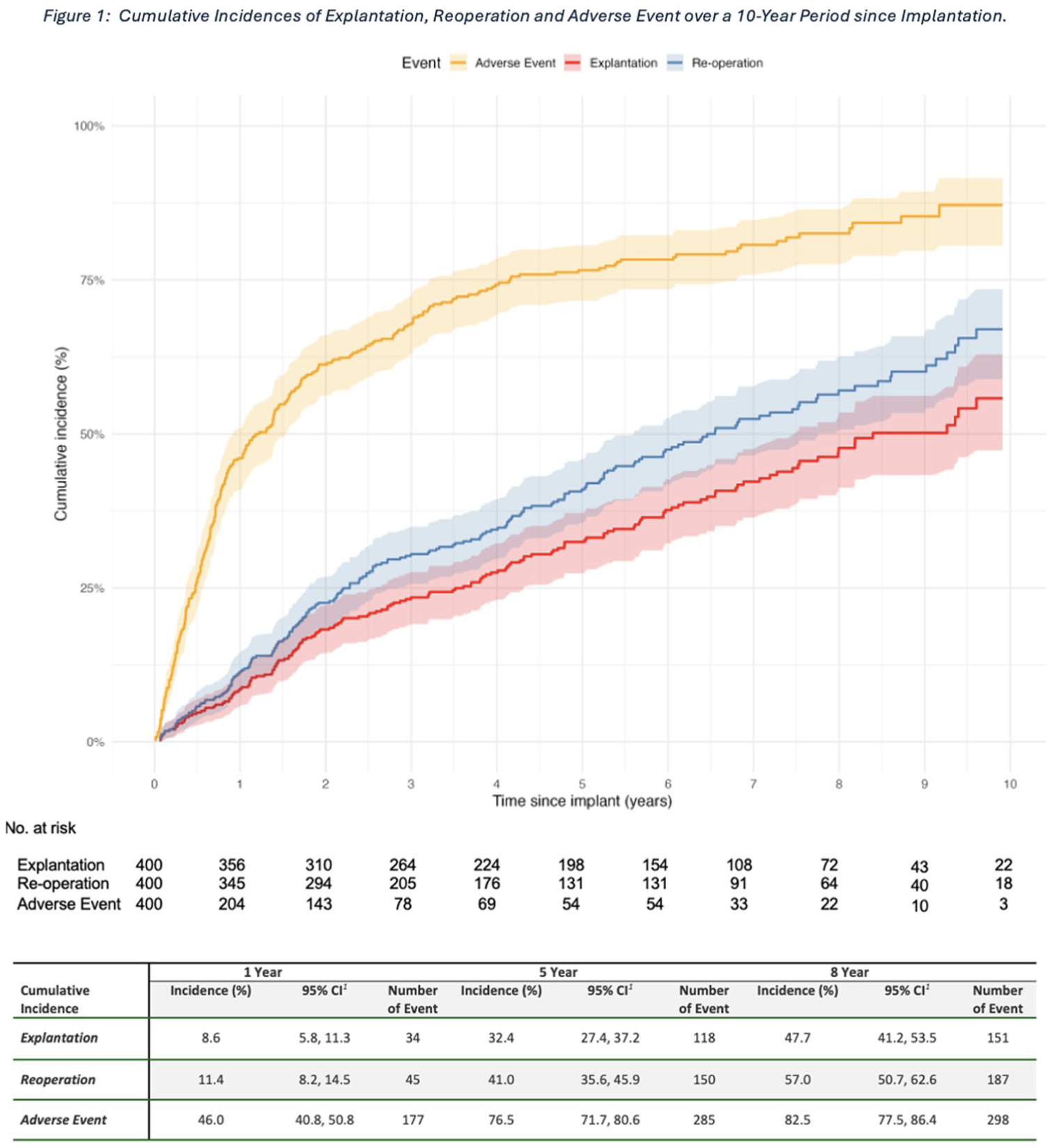
P12-4 Robotic assisted ureteral reimplantation: a series from a single centre
Miss Eva Browne1, Dr Michael Rafeh1, Ms Nikita Bhatt1, Mr Arjun Nambiar1
1Freeman Hospital, Newcastle-upon-tyne, United Kingdom
Introduction: Ureteric reimplantation is a procedure aimed at restoring function of the urinary tract following stricturing or injury of the ureter. This has been traditionally been done as an open procedure but recent advancements in minimally invasive surgery means that robotic-assisted surgery offers several technical advantages.
Methods: We analysed a prospectively maintained database of patients undergoing robotic assisted ureteral reimplantation between March 2022 and October 2025. Data recorded included type of procedure, indication for surgery, pre and post operative renal function, major complication rate and length of stay were recorded.
Results: A total of 26 cases were performed. 8 involved creation of a Boari flap, 12 just required a psoas hitch, 3 were direct ureteric reimplants and 3 buccal patch ureteroplasties were performed. Information regarding pre and post operative renal function was available for 18 patients (69.2%) demonstrating preservation or improvement of renal function in 15 (83.3%). Of 3 patients with ongoing deterioration in function, none required re-stenting or further intervention for obstruction. Of the 8 remaining patients, 6 had preserved split function on post operative imaging and 2 are awaiting follow up. No patients had a major complication (CD >3). Mean length of stay was 3.8 days (median 3).
Conclusion: Our series demonstrates that robotic-assisted ureteric reimplantation is associated with a short median length of stay and low complication rate. In addition to this we have demonstrated high rates of preservation of renal function post intervention with no reinterventions so far.
P12-5 Characterising Ketamine Cystitis: A Service Evaluation of Presentation and Management in a Tertiary Centre
Dr Chiu Ho Quentin Mak1, Miss Yathavi Charavanamuttu2, Miss Emily-Jane Eldred2, Dr Nicola Kalk3, Mr Nicholas Raison1
1Department of Urology, King’s College Hospital NHS Foundation Trust, London, United Kingdom, 2GKT School of Medical Education, King’s College London, London, United Kingdom, 3Addictions Care Team, King’s College Hospital NHS Foundation Trust, London, United Kingdom
Introduction: Ketamine cystitis (KC) is increasingly recognised as a complication of chronic ketamine use. Our understanding of this patient cohort is substandard. We sought to characterise this cohort in our institution and evaluate their relationship with our in-house addiction service.
Patients And Methods: 34 KC patients were identified using CogStack AI in our EPR between 2000 and 2023. The AI tool searched free text to identify documents that mention “ketamine cystitis” or its synonyms. Demographic, treatment and mental health data were obtained for further analysis.
Results: The mean age of our patient cohort at initial diagnosis was 29.6 years (95% CI, 26.7 – 32.4). 24/34 (73.5%) of the patient cohort was male. Advanced disease was prevalent: hydronephrosis (7/25), ureteral stricture (5/25), dilated calyces (5/25). Cystectomy was required in 3/31 patients.
21 patients were known to addiction services. Mental health data were obtained for 17 patients. 6/34 patients were under our in-house addictions service for ketamine use. Polysubstance use was rife (14/17), namely cocaine (8/17) and alcohol (8/17). Concomitant psychiatric comorbidity (13/17) was common, ranging from depression (3/17) to anorexia (2/17). Good engagement was noted in 9/15 patients, and 6/11 managed abstinence. No patients were referred to addiction by urology.
Conclusions: Our patient cohort is young at the time of initial diagnosis. Additionally, they have significant psychiatric co-morbidities and polysubstance use. Finally, our service is seeing them at a late stage of disease. Efforts must be made to develop improved pathways for the earlier identification and treatment of these patients.
P12-6 Transient benefit of intravesical gentamicin instillation for recurrent urinary tract infections in a complex urological cohort
Afia Saiyed1, Aamna Raza1, Samyek Dewan1, Mary Vicencio1, Anthony Kupelian1, Sarah Logan1, Anthony Noah1, Mahreen Pakzad1, Gabriele Pollara1, Dr Rohma Ghani1
1University College London Hospitals, London, United Kingdom
Recurrent urinary tract infections (rUTIs) in complex urological populations impair quality of life and strain healthcare resources. Intravesical gentamicin instillation (IGI) delivers high local antimicrobial concentrations with minimal systemic exposure and is easily administered in patients with catheter-assisted bladder drainage. We evaluated its effectiveness in reducing UTI frequency and healthcare utilisation.
We conducted an observational study of patients with gentamicin-susceptible Gram-negative bacteria rUTIs. IGI was administered as 80 mg daily for 2 weeks, followed by alternate-day dosing for 10 weeks and twice-weekly dosing for 12 weeks. Clinical outcomes were collected for the 6 months before IGI, during, and 6 months after cessation. Repeated-measures comparisons were performed using Wilcoxon signed-rank tests.
Twenty patients received IGI between April 2024 and May 2025. Median age was 46 years (65% female). 40% had a non-native bladder. Bladder drainage was via clean intermittent self-catheterisation (35%), indwelling urethral or suprapubic catheter (25%), or reconstructed channels (40%) (Mitrofanoff or ilea conduit). During IGI, median UTI episodes, antibiotic courses, and hospital admissions decreased by 92%, 83%, and 100%, respectively, compared with the preceding 6 months (p<0.001 for all) and consistent across bladder anatomy and drainage methods. After IGI cessation, UTI frequency increased significantly (p<0.001), with no difference between pre- and post-treatment periods (p=0.40).
IGI markedly reduced UTIs, antibiotic use, and hospital admissions during treatment across diverse urological subgroups. Benefits did not persist after stopping therapy, indicating only a transient prophylactic effect. IGI is effective while in use, but optimal duration, maintenance strategies, and long‑term safety require further study.
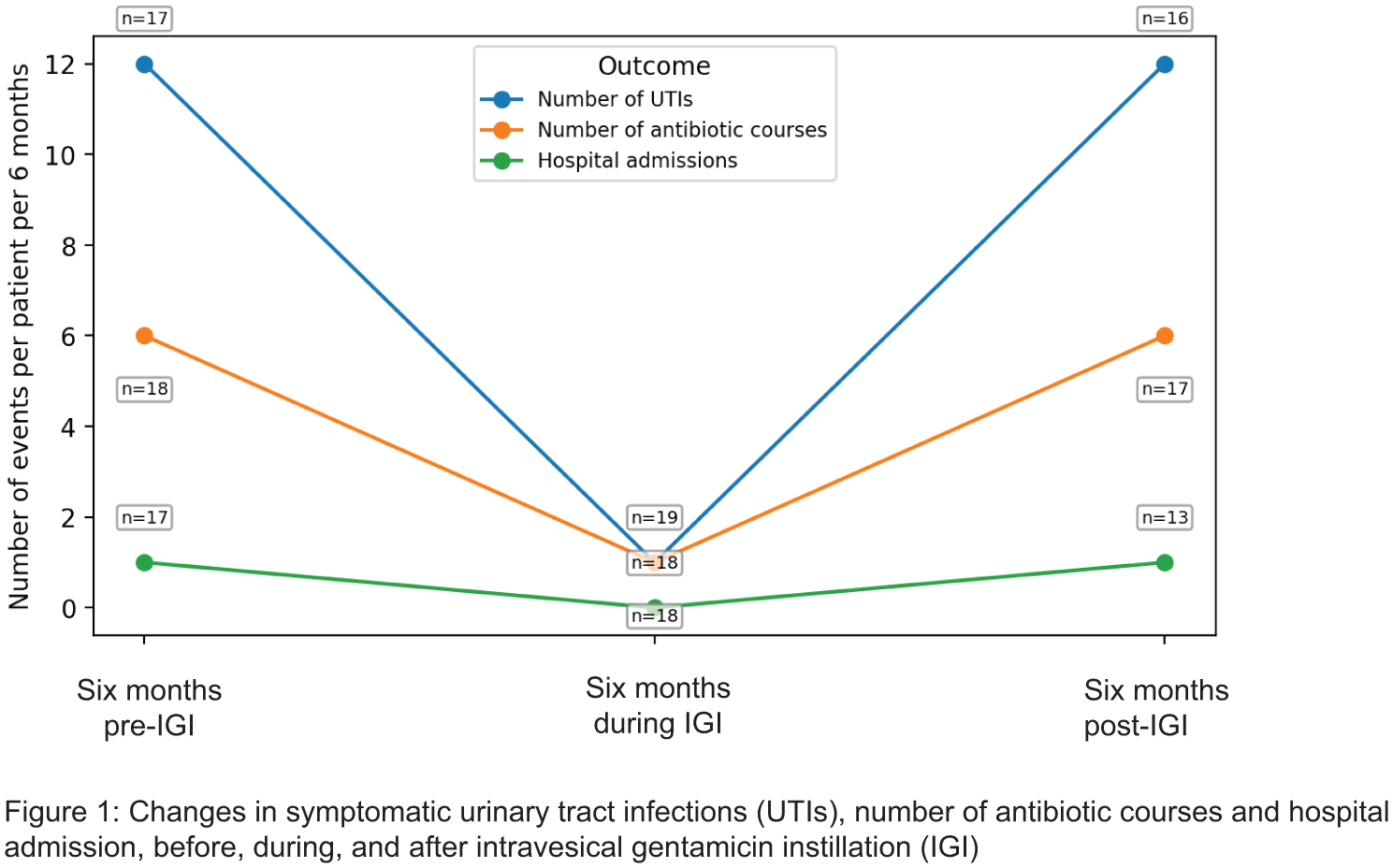
P12-7 ARTIFICIAL URINARY SPHINCTER OUTCOMES IN MEN WITH SPINAL CORD INJURY: REVISITING BULBAR PLACEMENT IN NEUROGENIC STRESS INCONTINENCE
Dr Ioannis Tsikopoulos1, Dr Mohamed Helal1, Mr Prashant Patel1, Mr Frank Lee1, CNS Sharon Gill1, Prof Sarah Knight1, CNS Claire Riley1, Mr Richard Nobrega1
1Royal National Orthopaedic Hospital, Edware, United Kingdom
Introduction: Artificial urinary sphincter (AUS) implantation is the gold standard for male stress urinary incontinence (SUI). In spinal cord injury (SCI) patients, current guidelines favour bladder-neck placement to minimise post-operative complications. However, data comparing bulbar versus bladder-neck placement remain limited. This study reports outcomes of predominantly bulbar AUS placement in men with SCI compared to non-neurogenic cases.
Patients and Methods: We retrospectively reviewed 39 men undergoing AUS implantation between 2015 and 2025 at a single centre. Fifteen (38%) had SCI-related SUI; 24 (62%) had non-neurogenic etiologies. Cuffs were placed in the bulbar urethra (n = 37) or bladder neck (n = 2). Follow-up included continence status (total: 0 pads/day; social: ⩽1 pad/day), ICIQ-UI SF, and EQ-5D-5L scores. Limitations included retrospective design and small cohort size.
Results: Median follow-up was 20 months (range 6–48). Overall, 47% achieved total and 77% social continence. In the SCI subgroup, 53% achieved total and 80% social continence—comparable to non-neurogenic outcomes (p = 0.71). ICIQ-UI SF scores improved from 15.8 to 7.0 in SCI and 16.1 to 6.9 in non-SCI patients (p = 0.62). EQ-VAS improved from 61 to 79 in SCI, and 60 to 81 in non-SCI (p = 0.58). Erosion rates were low in both groups (6.7% vs 4.2%, p = 0.78). No autonomic dysreflexia was reported.
Conclusions: Bulbar AUS implantation in SCI patients yields continence and safety outcomes comparable to non-neurogenic cohorts and published bladder-neck series. It may offer a safe, effective, and less invasive alternative in select cases. Prospective studies are needed.
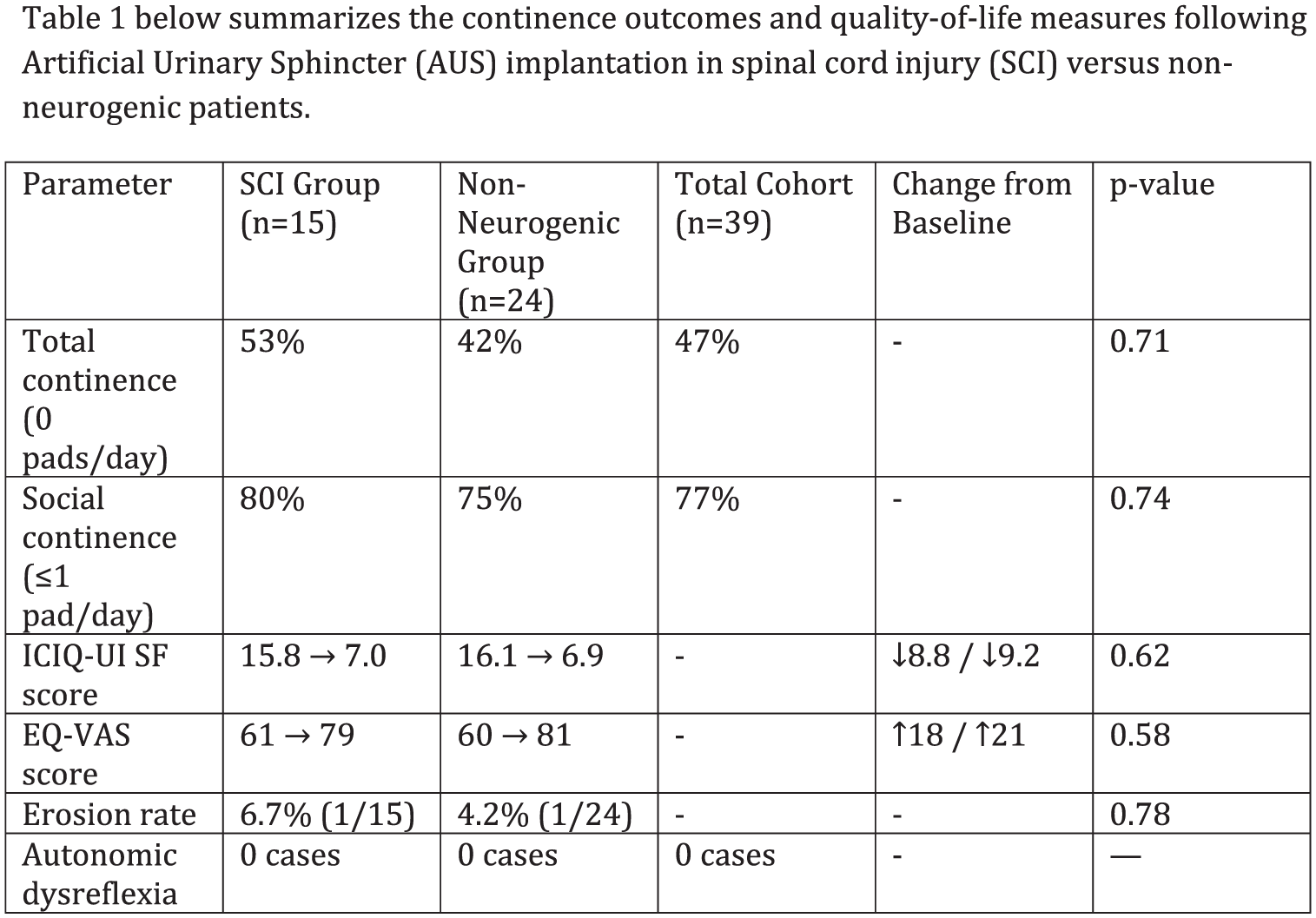
P12-8 Long-term outcomes of augmentation cystoplasty for refractory neurogenic bladder in spinal cord injury patients: a 30-year single-centre experience
Dr Ioannis Tsikopoulos1, Dr Mohamed Helal1, Prof Sarah Knight1, Mr Prashant Patel1, Mr Julian Shah1, Mr Rizwan Hamid1, Mr Richard Nobrega1
1Royal National Orthopaedic Hospital, Edware, United Kingdom
Introduction: Augmentation cystoplasty (AC) remains a key option for spinal cord injury (SCI) patients with refractory neurogenic lower urinary tract dysfunction (NLUTD) when conservative and minimally invasive treatments fail. We evaluated long-term functional and urodynamic outcomes following AC, complication rates over extended follow-up, and outcomes in a subgroup receiving post-operative intradetrusor botulinum toxin (BoNT).
Patients and Methods: A retrospective review was conducted on SCI patients undergoing AC between 1988–2018 at a single centre. Data collected included demographics, urodynamics (maximum cystometric capacity [MCC], maximum detrusor pressure [MDP]), continence outcomes, vesico-ureteric reflux (VUR), urinary tract infections (UTIs), antimuscarinic use, and complications. A subgroup analysis evaluated patients receiving post-operative BoNT. Paired statistical analyses were performed (p<0.05 significant). Ethics approval was obtained.
Results: Seventy patients (median age 55; 47M, 23F) were followed for a mean of 19 years. MCC increased significantly (156 mL → 491 mL, p<0.0001); MDP decreased (72 → 19 cmH₂O, p<0.0001). Continence was achieved in 67%; 24% had infrequent leakage, and 9% used daily pads. Recurrent UTIs (23→17) and antimuscarinic use were reduced (44→20), and VUR improved (9→2). Long-term complications included urolithiasis (10%), malignancy (4%; all >10 years post-AC), and bladder perforation (1.5%). In the BoNT subgroup (n≈18), MDP was reduced significantly (p=0.009), and MCC improved.
Conclusions: AC provides sustained urodynamic and continence benefits in SCI patients with refractory NLUTD. BoNT offers additional value in select patients. Long-term surveillance is vital due to potential delayed complications.
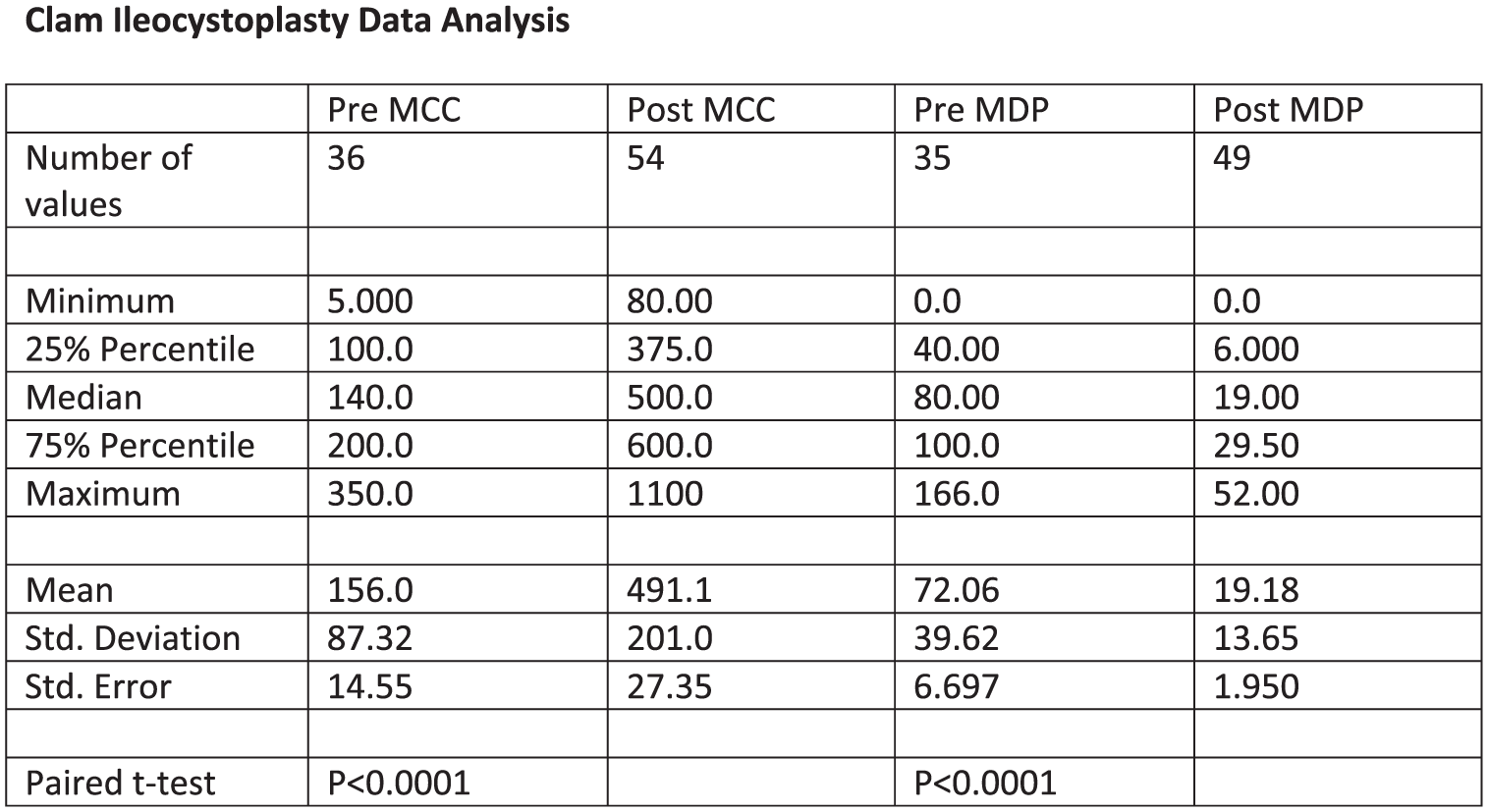
P12-9 Back to the future: A year of urology at a Spinal Injuries Centre
Mrs Kathryn Bandeira De Mello1,2, Mr Wilson To1,2, Mr Wail Ahmed1,2, Miss Katie Eyre1,2
1Buckinghamshire Healthcare NHS Trust, , United Kingdom, 2National Spinal Injuries Centre, Stoke Mandeville, United Kingdom
Introduction: Our centre is one of the largest spinal injuries units in the UK, supporting a growing cohort of patients who now experience near-normal life expectancy. Urologists are essential to their long-term care. We report our experiences in our first year providing dedicated urology services to the Spinal Injuries Centre.
Patients and methods: In November 2024, 248 patients were waiting for video urodynamics, 28 for inpatient urology review, and the wait for urological surgery was nine months. 33% of theatre capacity was occupied by local anaesthetic botulinum toxin injections.
We reviewed the urodynamics waiting list, prioritising the longest waiters and removing patients if appropriate. We re-established urodynamics, reducing the waiting list by 35% in nine months. We introduced an outpatient botulinum toxin clinic, releasing theatre capacity and improving surgical waiting times. The addition of a thulium laser expanded the range of endourological surgery deliverable within the unit.
Results: A dedicated spinal urologist has enabled timely inpatient assessment. We have managed a wide spectrum of complex and often historic urological conditions, including urethral stents, Brindley stimulators, urethro-cutaneous fistulas, high pressure neuropathic bladders, stress urinary incontinence, and challenging bladder and renal stone disease. The introduction of artificial urinary sphincters, ileal conduit formation and bladder augmentation will further improve urological care.
Conclusions: Establishing additional dedicated spinal urology services, targeted waiting list management, and expanded procedural capability has significantly improved urological care for spinal-injured patients. Continued service development will further enhance timely, specialist urological management for this growing and diverse population.
P12-10 Long-Term Urological and Sexual Outcomes After Spinal Cord Injury: A sequential review of medico-legal cases
Professor Julian Shah1, Ms Jasmine Shah, Dr Diana Bell
1King Edward VII Hospital, London, United Kingdom
Introduction: Spinal cord injury (SCI) is associated with long-term lower urinary tract and sexual dysfunction, impacting on quality of life. While acute bladder management is well described, long-term outcomes and variation in follow-up practice across the UK remain poorly characterised. Medico-legal reporting on spinal cord injured patients benefits from access to all the case records and thus is a unique opportunity to study these patients in detail.
Patients: An anonymised cohort of 101 patients with traumatic SCI taken from a medico-legal practice was reviewed to evaluate bladder management strategies, urological morbidity, and documentation of sexual function. This particularly applied to variations in practice around the UK.
Results: The mean age was 36.6 years (range 1–81 - 72 males and 27 females). Road traffic collisions, particularly motorcycle accidents, were the most common mechanism of injury, and thoracic injuries predominated. At discharge, bladder management comprised of intermittent self-catheterisation (35%), suprapubic catheterisation (15%), indwelling urethral catheter (12%), and spontaneous voiding (17%). Younger patients and those with thoracic injuries were more likely to use intermittent catheterisation. Older patients and those with cervical injuries more commonly required indwelling or suprapubic catheters. During follow-up, approximately 50% of patients reported persistent urinary complications, most frequently urinary tract infection (25%), incontinence, or catheter-related problems. Sexual function was poorly documented, with most records noting “not mentioned”. Regional variation was observed in urological management strategies and quality of documentation.
Conclusion: These findings highlight the need for standardised long-term follow-up pathways and improved documentation to optimise neuro-urological care after SCI.
ePoster Session 13: General Urology (BPH/Male LUTS / Emergency / Trauma), Olympia, June 16, 2026, 15:45 - 16:45
P13-1 The WASHOUT study: early proactive intervention in emergency haematuria reduces length of stay, mortality and readmissions
Ms Nikita Bhatt1, Kevin Byrnes, Simona Ippoliti, Raghav Varma, Bing Jie Chow, Quentin Mak, Nikki Kerdegari, Aqua Asif, Arjun Nathan, Alexander Ng, Yazan Qaoud, Luke Lavallee, Anna Ireland, Joanne Cresswell, Amrut Phonde, Kumar Madhavan, Piyush Bhargav Sarmah, Molly Nichols, James Green, Ahmed Ahmayda, Graeme MacLennan, Kevin Gallagher, Sinan Khadhouri, Veeru Kasivisvanathan
1St Vincent’s University Hospital, Dublin, Ireland
Introduction & Objectives: There are no evidence-based guidelines for the management of emergency haematuria, resulting in substantial variation in clinical practice. The WASHOUT study aimed to characterise variation in the management of emergency haematuria and to evaluate the association between management variation and patient outcomes.
Materials & Methods: WASHOUT was a prospective, international, multi-centre cohort study conducted using the British Urology Researchers in Surgical Training (BURST) collaborative model, with patient and public involvement. The primary outcome was length of hospital stay (LoS). Secondary outcomes included 90-day mortality and hospital readmission following the index admission. Outcomes were analysed using multivariable statistical models adjusted for relevant covariates.
Results: Over 8,500 patients from 382 centres were included over a 12-month period. Increasing delay between admission and definitive management was significantly associated with longer LoS and higher risks of readmission and death (OR 1.02, p<0.001). Patients with more than two days between admission and completion of management experienced an adjusted mean increase in LoS of 5.6 days, a 2.5% higher probability of death within 90 days, and a 3.1% higher probability of readmission.
Conclusions: WASHOUT is the first study to evaluate factors influencing outcomes in patients presenting with emergency haematuria. Based on our findings, we propose patients with emergency haematuria should have emergent imaging on admission and intervention within 2 days of admission if the haematuria has not settled by conservative measures. There is an urgent need for evidence-based guidelines to standardise and expedite the investigation and management of emergency haematuria.
P13-2 The WASHOUT study: workup and management of patients with emergency haematuria across the world
Ms Nikita Bhatt1, Kevin Byrnes, Simona Ippoliti, Raghav Varma, Bing Jie Chow, Quentin Mak, Nikki Kerdegari, Aqua Asif, Arjun Nathan, Alexander Ng, Yazan Qaoud, Luke Lavallee, Anna Ireland, Joanne Cresswell, Amrut Phonde, Kumar Madhavan, Piyush Bhargav Sarmah, Molly Nichols, James Green, Ahmed Ahmayda, Graeme MacLennan, Kevin Gallagher, Sinan Khadhouri, Veeru Kasivisvanathan
1St Vincent’s University Hospital, Dublin, Ireland
Introduction & Objectives: Emergency haematuria accounts for approximately 15% of urological emergency admissions, or 4 in 1,000 emergency hospital presentations. This is a prospective international study aimed to describe contemporary management practices and clinical outcomes in patients presenting with emergency haematuria.
Materials & Methods: This international, multicentre, prospective observational study was conducted using the British Urology Researchers in Surgical Training collaborative model. Primary outcomes included length of hospital stay (LoS), mortality, and 90-day readmission rates.
Results: Data were collected for 8,500 patients across 382 centres internationally over a one-year period. Median LoS was four days (IQR 2–8), with a 90-day mortality rate of 9.2% and a 90-day readmission rate of 31%. On admission, 5% of patients were haemodynamically unstable and 11% required high-dependency care. Ward-based management was successful in 35% of cases, 47%) did not undergo imaging during admission, and only 35% received an intervention.
Overall, 25% of patients had malignancy as the underlying cause (12.5% pre-existing and 12.5% newly diagnosed), with a further 5% diagnosed during follow-up. Urothelial carcinoma accounted for 20% of malignancies identified during admission and 4% during follow-up. Median time to diagnosis was one day during admission compared with 21 days following discharge.
Conclusions: Emergency haematuria has high rates of morbidity, readmission, and underlying malignancy. Ward-based management is frequently unsuccessful, with patients often discharged without imaging or intervention, leading to delayed diagnoses. These findings support structured early diagnostic pathways, timely inpatient management, and suggest that discharge without a definitive diagnosis be avoided.
P13-3 Reducing Unnecessary Outpatient Appointments: Virtual LUTS Triage Using IPSS/QOL Stratification in a High-Volume NHS Service
Mr DON WIJAYASURIYA1, Dr Esther Thomas, Mr Adam Cox
1Royal Gwent Hospital, Newport, United Kingdom
Patients and Methods: A retrospective audit of 347 consecutively referred men to a high-volume virtual LUTS service (2019–2020) was undertaken. Data extracted included age, DNA/non-compliance, symptom severity, IPSS, QOL, medications, virtual triage outcome, Final outcome, investigations (flow/Qmax, PVR, UDS), surgery, re-referral, and distance from hospital. IPSS was categorised as mild (0–7), moderate (8–19) or severe (⩾20). Patients with completed key fields in columns D–X were defined as fully assessed.
Results: Mean age was 66.4 years (range 21–94); 97.1% were compliant. Symptom severity was mild in 17.6%, moderate 44.1% and severe 29.7%; IPSS was recorded in 79.5% (mean 16.7; 13.4% mild, 51.1% moderate, 35.5% severe). From virtual triage, 27.1% were discharged, 45.8% referred to F2F, and 23.1% entered remote monitoring. Overall, 51.3% were ultimately discharged, 10.1% managed medically, 5.5% underwent surgery, and 24.8% required further investigation/follow-up. Flow was performed in 50.1%, UDS in 4.6%; 16.4% had surgery (HOLEP 14, TURP 8, BNI 1, others via endoscopic pathways). Re-referral for LUTS occurred in 14.1%. Distance was recorded in 325 patients (mean 12.9 miles); 167 patients discharged/remote‑monitored without surgery accounted for an estimated 4,317.6 avoided return‑trip miles.
Conclusions: Virtual LUTS triage using IPSS/QOL stratification safely discharges or remotely manages around half of referrals while focusing F2F review, investigations and surgery on higher-risk patients. This model reduces unnecessary outpatient appointments and substantially cuts patient travel, supporting both service efficiency and environmental sustainability.
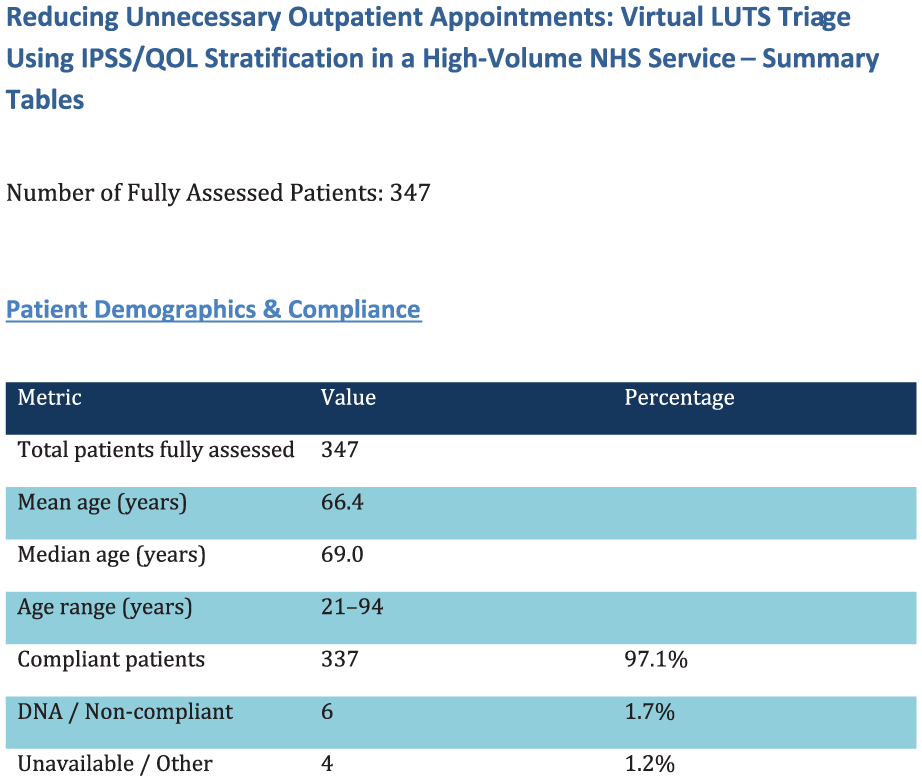
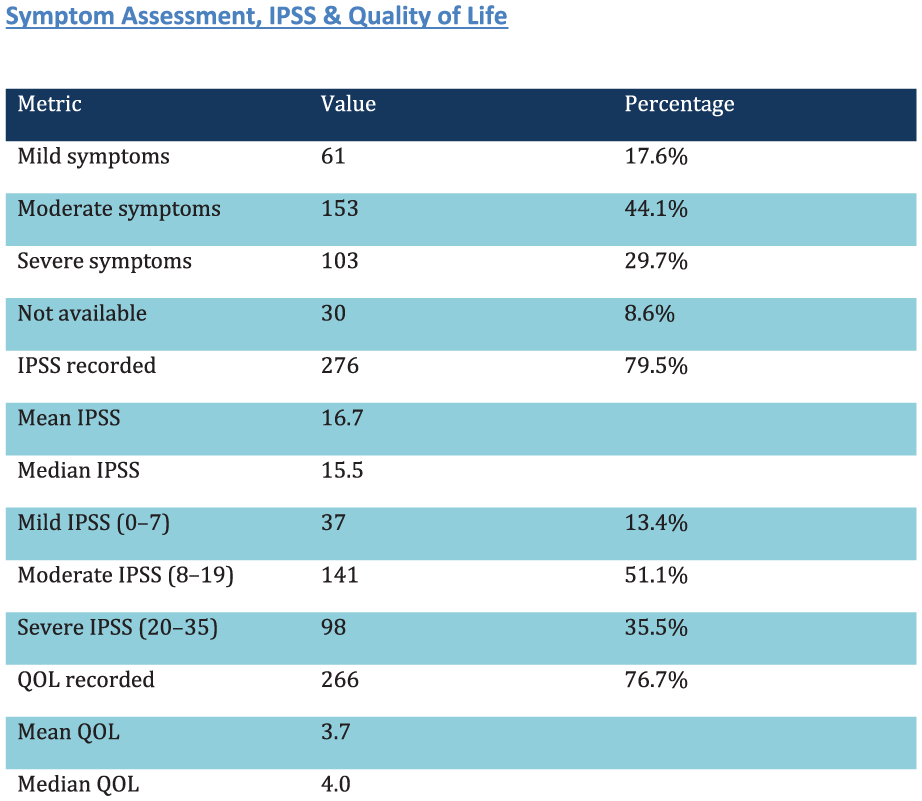
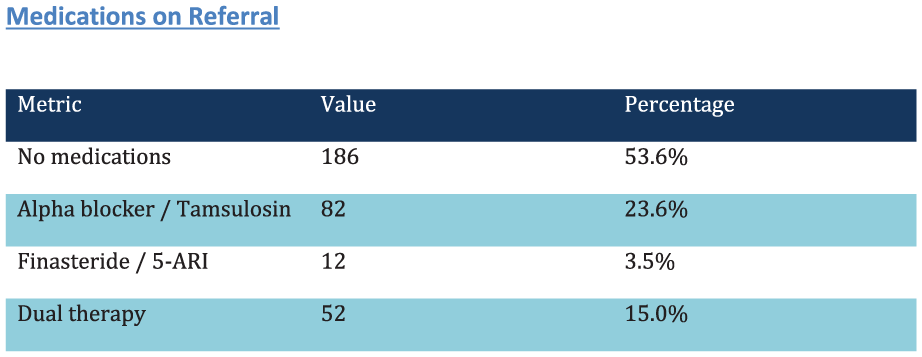
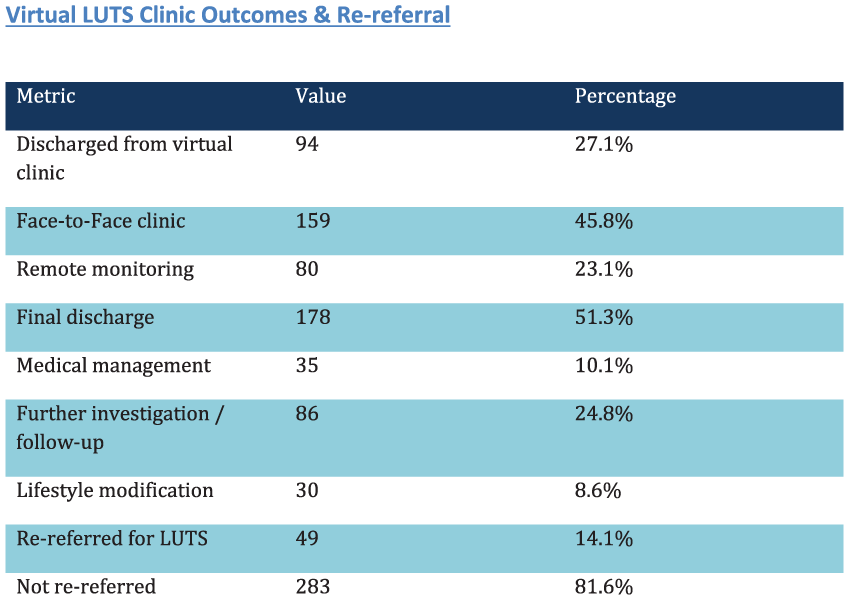
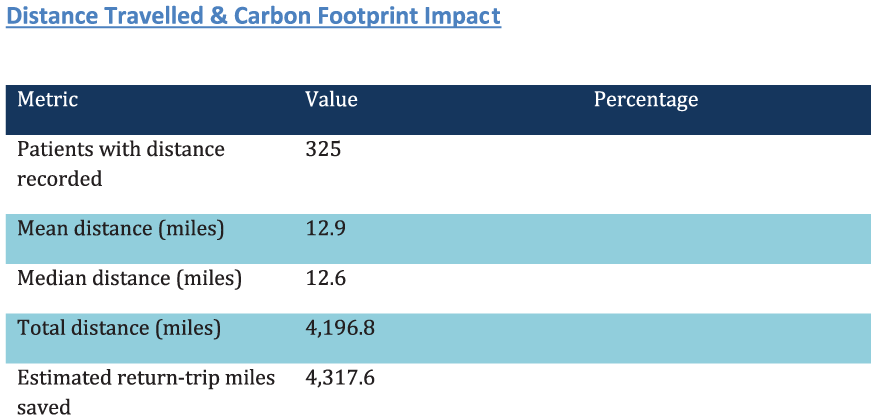
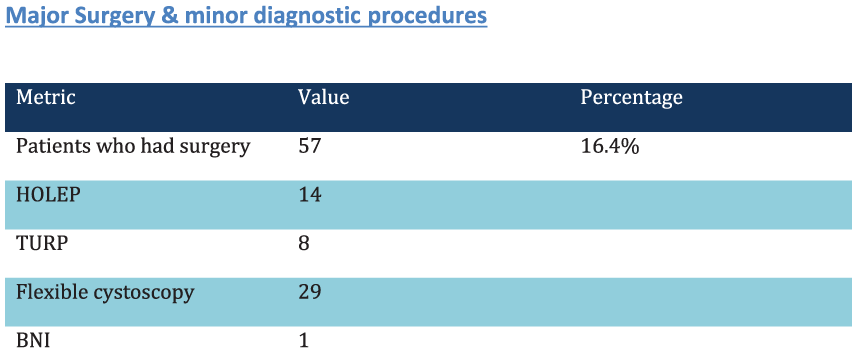
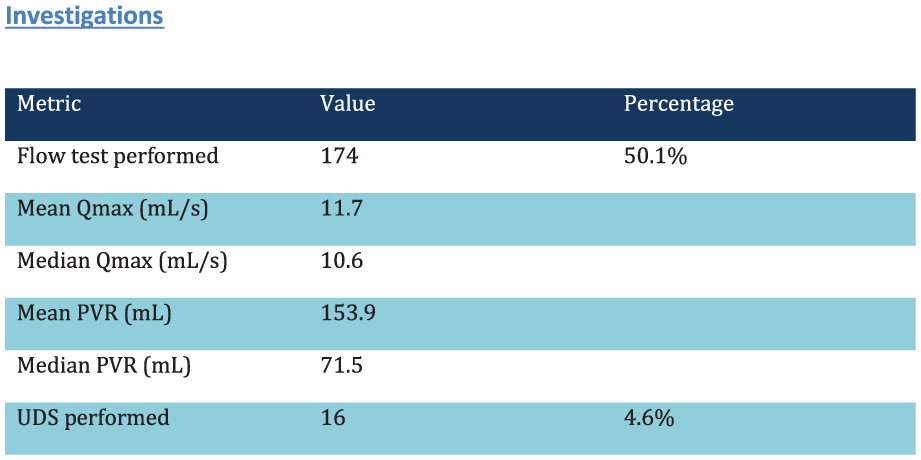
P13-4 Robotic Aquablation for treatment of bladder outlet obstruction, can it democratise theatre time compared to Holmium enucleation?
Miss Deepika Reddy1, Hanna Maroof1, Elsie Mensah1, Oussama El Hage1, Sachin Malde1, Jonathan Noel1, Rick Popert1, Benjamin Challacombe1
1Guy’s and St Thomas’ Hospital, London, United Kingdom
Introduction: Currently a plethora of options exist in the treatment of bladder outlet obstruction caused by benign prostatic hyperplasia. Considerable pressures on waiting lists for benign procedures and to optimise theatre efficiency exist, thus predictability of operating time is vital. We report upon operating times of aquablation and HoLEP cases in a high- volume tertiary teaching centre during a time-period encompassing the learning curve for aquablation for all clinicians, and 4 clinicians new to performing HoLEP and two expert surgeons.
Methods: All operating times of patients receiving HoLEP between Jan 2020-December 2024 or aquablation between July 2022- December 2024. Prostate volumes were prospectively reported using standard of care imaging.
Primary outcome was to determine if operating time, defined as time from scope insertion to completion of procedure, for each modality differed according to prostate volume. Secondary outcome was operating time per prostate volume (up to 150cc) for each modality.
Results: 462 patients received HoLEP, 190 received aquablation, overall median (IQR) prostate volume was 80 (64-110) and 110cc (81-150) respectively (p<0.001), and overall operative time was 56 (47-68) and 103 mins (77-136). Operative time per prostate volume and modality is reported in table 1. After accounting for prostate size, aquablation was significantly quicker than HoLEP. Statistically significant increases in operative time with prostate volume for both treatment modalities were observed.
Conclusions: We report real-world evidence demonstrating that aquablation, compared to HoLEP, has the potential to democratise operating time despite prostate volume and clinician experience.
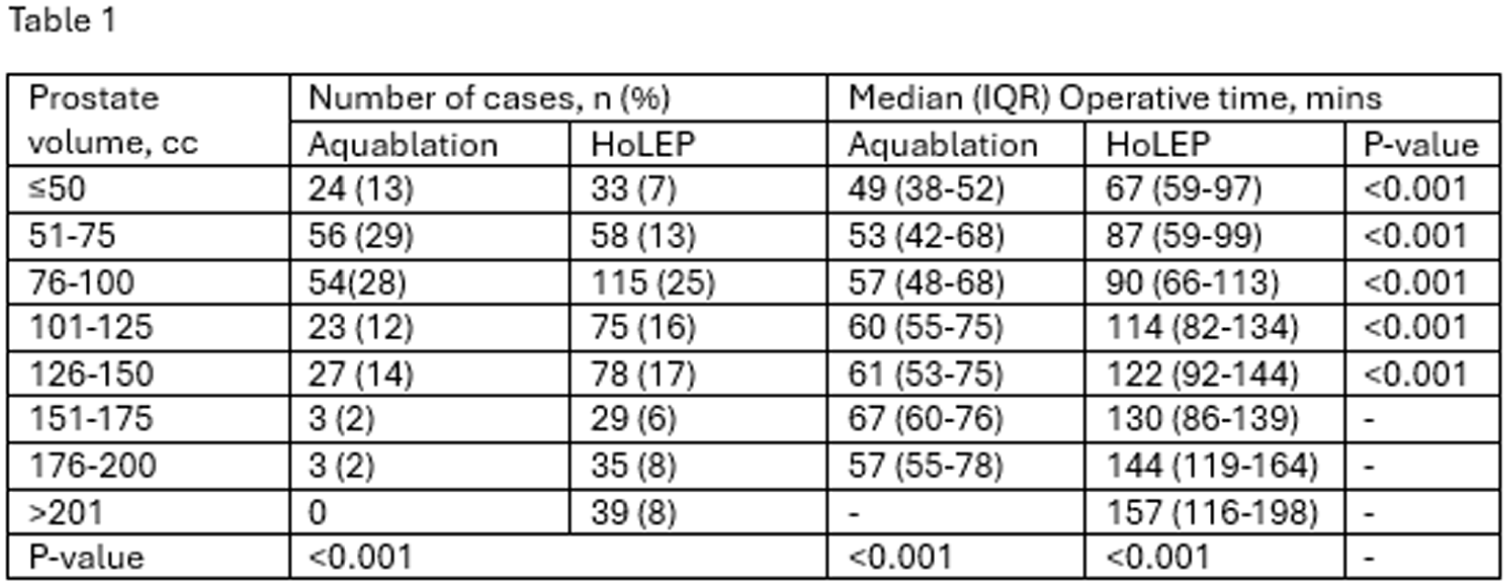
P13-5 PuraStat (RADA16) for radiation cystitis–related severe haematuria: 3-month control and reduced healthcare utilisation in a live register
Mr Petre Cristian Ilie2, Miss Anne Carrie1, Mr Radu Croitoru2, Mr Dimitar Ormanov2, Prof Lee Smith3
1Norfolk And Norwich University Hospital, Norwich, United Kingdom, 2The Queen Elizabeth Hospital, King’s Lynn, United Kingdom, 3Anglia Ruskin University, Centre for Health Performance and Wellbeing, Cambridge, United Kingdom
Introduction: Persistent severe haematuria following pelvic radiotherapy is challenging to manage and commonly drives repeated hospital and urgent care attendances. We evaluated endoscopic PuraStat (RADA16) for symptom control and its impact on subsequent healthcare utilisation, highlighting outcomes by cancer status.
Patients and Methods: A live register was established under REC approval (London – Dulwich Research Ethics Committee; 23/LO/0998; REC opinion 23 Jan 2024; IRAS 336909). Ten patients with persistent severe haematuria secondary to radiation cystitis were included. Mean age was 82.3 years (range 76–89); 90% were male and 10% female. PuraStat (RADA16) 3–6 mL was administered endoscopically per session (mean 1.40 sessions). Pre- vs post-treatment healthcare utilisation (hospital visits, days in hospital, and A&E/GP visits) was compared using the Wilcoxon signed-rank test.
Results: No complications were observed. Following treatment there was a significant reduction in healthcare utilisation: hospital visits decreased by 97% (p=0.007), days in hospital decreased by 98% (p=0.018), and A&E/GP visits decreased by 97% (p=0.018). In patients with no active cancer, haematuria was fully controlled at three months and no further healthcare contacts were required (hospital visits, A&E attendances or GP consultations). Only one patient—treated palliatively for bladder cancer—required admission two months post-treatment.
Conclusions: In this live register, PuraStat (RADA16) was associated with marked reductions in healthcare utilisation and, in patients without active malignancy, complete 3-month control with cessation of subsequent unplanned healthcare contacts. Larger prospective evaluation is warranted.
P13-6 Evaluating the Utility of the TWIST Score in Acute Testicular Pain: Audit of a single centre experience
Mr Khaled Ghanem1, Dr Asma Jamil1, Mr Yasir Khan1, Ms Quratulain Akbar1, Mr Junaid Masood1
1Barking, Havering and Redbridge NHS Trust, Ilford, London, United Kingdom
Testicular torsion is a urological emergency characterised by twisting of the spermatic cord, compromising testicular blood flow. The peak incidence is between 13 and 15 years, affecting approximately 1 in 4,000 males under 25 years. In older patients, diagnosis may be overlooked in favour of more common differentials. Delayed recognition risks irreversible ischaemia and testicular loss. Clinical scoring systems such as the Testicular Workup for Ischaemia and Suspected Torsion (TWIST) score aim to aid risk stratification; however, their application in real-world settings remains uncertain.
A retrospective audit was conducted of all patients presenting with testicular pain to our Trust between February 2024 and February 2025. Demographics, clinical features, TWIST score, ultrasound utilisation, operative findings, and outcomes were analysed.
A total of 380 cases were reviewed. Twenty-seven torsions were identified, including one involving an undescended testis. TWIST stratified 28 high-risk, 66 intermediate-risk, and 286 low-risk patients. Sixty-two explorations were performed, yielding 27 torsions. While most torsions occurred in high- and intermediate-risk groups, two torsions were identified among explored low-risk patients, following ultrasound scans. Ultrasound missed one torsion in a high-risk patient. Abnormal/horizontal testicular lie, not included in TWIST, was documented in 30 patients, 20 of whom had torsion, compared with seven torsions among 350 with normal lie.
TWIST is effective in identifying low-risk patients but demonstrates limited specificity in intermediate- and high-risk groups. Abnormal lie not included in this scoring system appears to be a strong predictor and may enhance clinical risk assessment. TWIST should complement, not replace, senior clinical judgement.
P13-7 Early comparative outcomes of minimally invasive surgical therapies (UroLift, Rezūm and iTIND): a single-centre experience in the management of benign prostatic enlargement
Dr Abhinav Chaudhary1, Mr Keng Lim Ng1, Mr Neil Barber1
1Frimley Park Hospital, Frimley, United Kingdom
Minimally invasive surgical therapies (MISTs) such as UroLift, Rezūm, and iTIND offer symptom relief for benign prostatic hyperplasia (BPH) with lower morbidity than conventional surgery and quite appealing for sexually active men. This study reports a single-centre experience comparing these procedures regarding functional outcomes, symptom improvement, and safety at 12 months. Data were derived from two single-centre randomised trials: the CLEAR trial (Rezūm vs UroLift) and MT08 (UroLift vs iTIND).
Methods: A retrospective review included 33 men undergoing Urolift (n=13), Rezūm (n=9), and iTIND (n=11) between 2022–2025. All procedures were performed under sedation in an outpatient setting. Pre- and 12-month post-operative parameters analysed were age, TRUS-measured prostate volume, PSA, IPSS, QoL, Qmax, and PVR. Exclusion criteria included elevated PSA, PIRADS 3–4 lesions, prior prostate/bladder neck surgery, urethral strictures, or age <20 years and prostate volume more than 80 mls. Statistical analysis used paired t-test or Wilcoxon signed-rank test with p<0.05.
Results: Urolift: IPSS 22.6→12.3 (45.6%), QoL 4.25→2.2 (−48.2%), Qmax 11.8→14.5 ml/s (22.8%), PVR 140.5→67.1 ml (52.2%)
Rezūm: IPSS 26.6→11.2 (57.8%), QoL 5.1→2.4 (−52.1%), Qmax 10.02→13.3 ml/s (24.8%), PVR 200.7→69.6 ml (65.3%)
iTIND: IPSS 21→9.3 (55.7%), QoL 4.27→2.5 (−41.6%), Qmax 9.1→11.2 ml/s (18.8%), PVR 81.5→40.6 ml (50.2%).
All procedures were completed under sedation; no Clavien–Dindo ⩾ III events, retreatments, or medication restarts occurred.
Conclusion: MIST provided sustained 12-month improvements in LUTS and urinary flow. Rezūm achieved the most balanced improvement across symptom scores and flow metrics. Correct patient selection is an essential criteria for best outcomes from the MIST procedures.
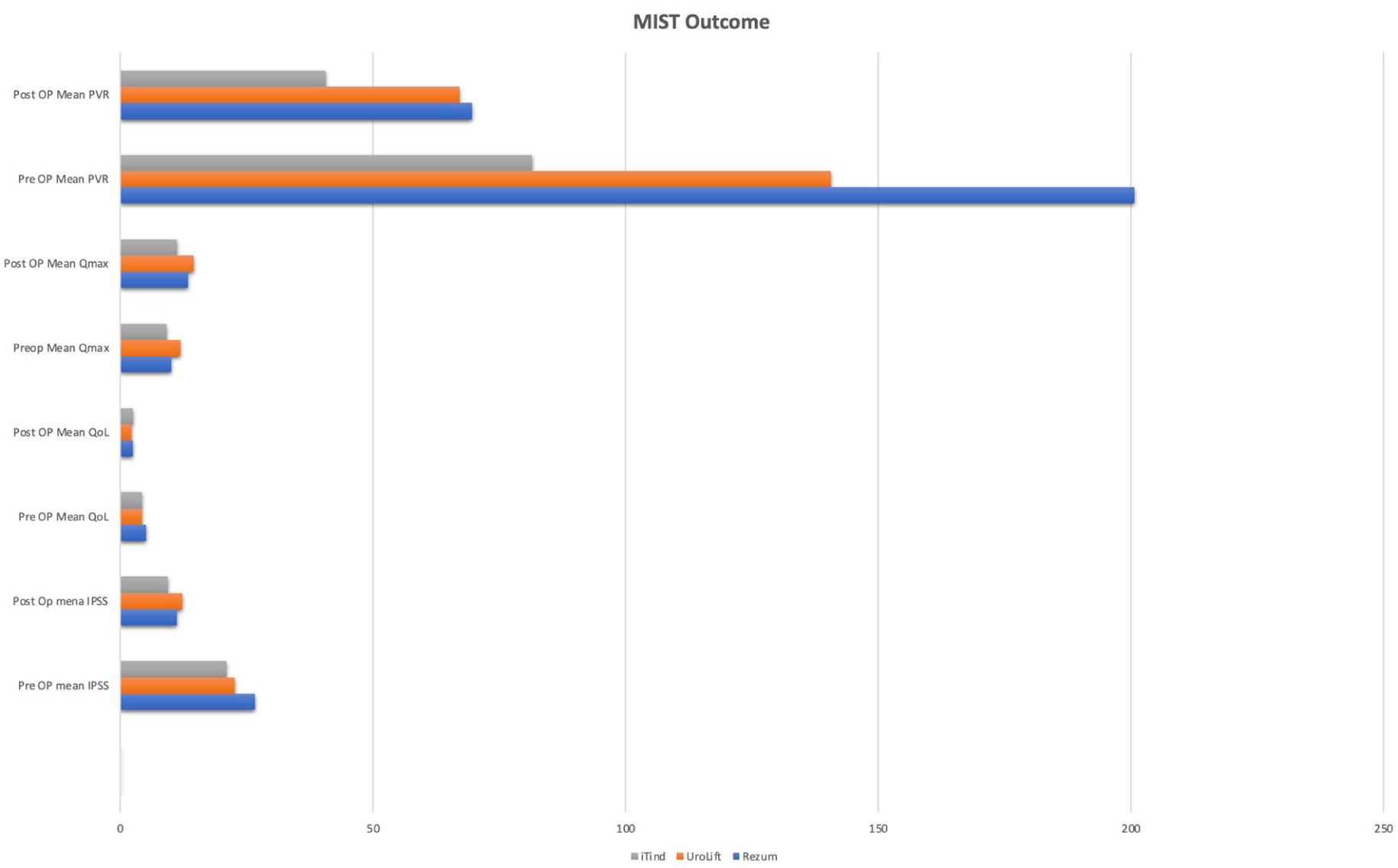
P13-8 CLEAR RCT through 12 Months: Better Early Recovery with UroLift PUL vs Rezum with Comparable Durability
Mr Neil Barber1, Mr. Mark Rochester2, Dr. Brian Mazzarella3, Dr. Christopher Cantrill4, Dr. Bilal Chughtai5, Dr. Arnold Cinman6, Dr. Jeffrey Schiff7, Dr. Claus Roehrborn8
1Frimley Health NHS Foundation Trust/ Cromwell Hospital, Surrey, United Kingdom, 2Norfolk and Norwich University Hospital, Norwich, United Kingdom, 3Urology Austin, Austin, USA, 4Urology San Antonio, San Antonio, USA, 5Plainview Hospital, Syosset, USA, 6Tower Urology, Los Angeles, USA, 7NYU Langone, New York City, USA, 8UT Southwestern, Dallas, USA
Introduction and Objective: CLEAR is the first head-to-head RCT comparing prostatic urethral lift (PUL) with UroLift and water vapor thermal therapy with Rezum. This report focuses on study outcomes through the final endpoint of 12mo.
Methods: CLEAR is a prospective, multinational, 1:1 RCT comparing patient experience, efficacy, and safety in BPH patients treated with PUL or Rezum. The primary endpoint evaluated catheter-independence between postoperative day 3-7. Here, we investigate outcomes through completion of the study (12mo).
Results: 35 Rezum and 38 PUL subjects were included in the 12mo CLEAR RCT analysis. Baseline demographics were similar between groups. 20% of Rezum subjects failed the primary endpoint vs 3% of PUL subjects (p=0.02). At early timepoints, PUL subjects had better improvement in IPSS and QoL; these outcomes were later similar between groups. PUL subjects had better quality of recovery at 3mo (p=0.04), which was then comparable to Rezum at 12mo. More Rezum subjects were catheterized during early follow-up; catheter-related symptoms (i.e., pain, urgency/spasms, bleeding) were more common with Rezum vs. PUL until 2wks. AEs occurred in 51% of Rezum vs 34% of PUL subjects (p=0.2), with macroscopic hematuria presenting at a higher rate in Rezum vs PUL subjects. Surgical intervention rates through 12mo were similar between groups (0.0% Rezum vs 3% PUL, p=1.0).
Conclusion: Early improvements in symptoms and patient-reported experience favored PUL over Rezum. These advantages in the acute recovery period were achieved without compromising 12mo durability, as both groups demonstrated comparable symptom relief and surgical retreatment rates through study end.
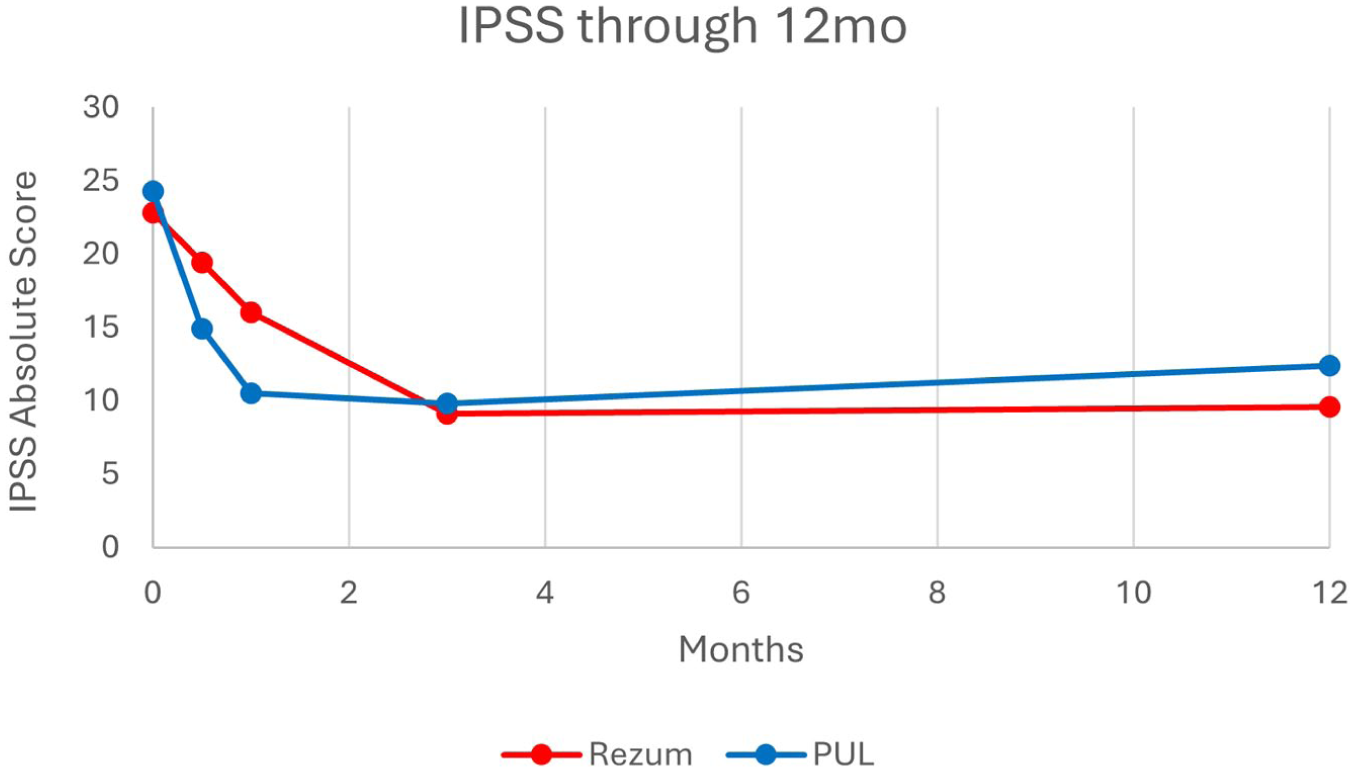
P13-9 True Daycase HoLEP
Miss JESSIE BLACKBURN1, Miss Tiffany Silverside1, Miss Tharani Nitkunan1
1Epsom And St Helier Nhs Trust, London, United Kingdom
Introduction: Getting It Right First Time (GIRFT) guidance states 25% of all bladder outflow obstruction surgery should be performed as a day-case procedure. Trusts achieving this target commonly send patients home on the day with a catheter. Our research has shown that patients wish to be discharged home catheter free. The aim of this project was to discharge patients home on the day of surgery, catheter free, following Holium Laser Enucleation of the Prostate (HoLEP).
Patients and Methods: The project was performed at a single NHS Trust between 01/01/2024 to 09/04/2025. All HoLEPs were performed or supervised by one operating surgeon. Intraoperative factors were recorded in operation notes and postoperative data documented in the patient notes. Data was collected and analysed using Microsoft Excel.
Results: 102 patients underwent a HoLEP in this time period. 67% (68/102) patients underwent Trial Without Catheter (TWOC) on the day of operation. 79% (54/68) of patients TWOC’ed on the day of surgery passed their TWOC. In addition, 56% (30/54) of patients successfully TWOC’ed on the day of surgery were discharged the same day. The overall day-case rate was 33%.
Conclusion: This study has shown that same-day TWOC following HoLEP is feasible. Continued education of patients, nursing and medical teams is required to drive and improve day-case rates.
P13-10 Underuse of Vaginal Oestrogen Therapy in Postmenopausal Women with Recurrent Urinary Tract Infections: A Call for Increased Awareness and Guideline Adherence
Dr Shideh Arameshfard1, Dr Toska Ukaj, Dr Anjali Patel, Dr Neysa Patel, Dr Shannel Darku, Dr Aislinn Pedersen, Ms Izabela Maj, Mr Virgiliu Bodean, Mr Farooq Khan, Mr Anish Pushkaran
1Luton And Dunstable Hospital, Luton, United Kingdom
Introduction & Objectives: Recurrent urinary tract infections (rUTIs) represent significant morbidity and healthcare burden, particularly in postmenopausal women. Oestrogen deficiency contributes to disruption of the vaginal microbiome and impaired urothelial defence mechanisms, increasing susceptibility to infection. Topical vaginal oestrogen therapy restores mucosal integrity. Despite strong recommendations from the EAU and NICE, the adoption of vaginal oestrogen in clinical practice remains suboptimal. This study aimed to evaluate the management of rUTIs in our institution and use of vaginal oestrogen therapy and adherence to guideline-based care.
Materials & Methods: A retrospective review of patients referred for recurrent urinary tract infections (rUTIs) over a two-year period was conducted. Referral letters, clinic documentation, and urine culture results were systematically analysed. Data on diagnostic investigations, antibiotic prescribing patterns, lifestyle counselling, and the prescription of vaginal oestrogen therapy was collected.
Results: Postmenopausal women accounted for 74% (79 patients) of all recurrent urinary tract infection (rUTI) cases. The use of vaginal oestrogen therapy was notably low: 12.7% (10 out of 79 patients) in primary care. In secondary care 26.1% (18 out of 69) of eligible patients were prescribed vaginal oestrogen over multiple clinic visits. In total, 64.6% (51 out of 79) of eligible patients did not receive oestrogen therapy.
Conclusions: Despite strong recommendations from the EAU, vaginal oestrogen remains underutilised in post-menopausal women with recurrent urinary tract infections. Early initiation of this therapy, in both primary and secondary healthcare settings, can significantly reduce disease burden, promote antibiotic stewardship, and decrease associated healthcare costs.
ePoster Session 14: Stones, Imaging and Upper Tract Disorders 2, Catherine Lewis, June 17, 2026, 08:00 - 09:00
P14-1 Multi-centre International Comparison of Conventional versus Laser Cystolithotripsy for the Management of Bladder Stones: 30-day Outcomes from the EAU Endourology Bladder Lithiasis Assessment of Surgical Treatment in real world practice (BLAST) study
Ms Sohani Dassanayake1, Prof Bhaskar Somani1, Dr Clara Cerrato1, Dr Steffi K. K. Yuen2, Dr Angelo Cormio3, Prof Arun Chawla4, Dr Jaisukh Kakathia5, Dr Azizbek Shomarufov6, Dr Ender Cem Bulut7, Dr Tianyu Li8, Dr Zijie Chai9, Dr Wei Zhu9, Dr Deepak Ragoori10, Dr Daniele Castellani11, Ms Amelia Pietropaolo1, Prof Vineet Gauhar12
1University Hospital Southampton NHS Foundation Trust, Southampton, United Kingdom, 2The Chinese University of Hong Kong, , China, 3Policlinico Riuniti di Foggia, University of Foggia, Foggia, Italy, 4Kasturba Medical College, Manipal Academy of Higher Education, Karnataka, India, 5Fortune Urology Clinic, Gujarat, India, 6Republican Specialized Scientific and Practical Medical Center of Urology, Tashkent, Uzbekistan, 7Gazi University, , Turkey, 8The First AffiliatedHospital of Guangxi Medical University, , China, 9The First Affiliated Hospital of Guangzhou Medical University, , China, 10Asian Institute of Nephrology and Urology, , India, 11AziendaOspedaliero-Universitaria Ospedali Riuniti di Ancona , , Italy, 12Ng Teng Fong General Hospital, , Singapore
Introduction: Bladder stones cause significant patient morbidity. Management options include open surgery, extracorporeal shockwave lithotripsy, and endoscopic cystolithotripsy using conventional mechanical or laser technology. Despite increasing use of laser cystolithotripsy, concerns remain regarding complications and stone-free rate (SFR) compared to conventional methods. This study compared outcomes between conventional and laser cystolithotripsy across a large international cohort.
Materials & Methods: An international registry evaluated cystolithotripsy outcomes from 10 centres (2016-2025). Adult and paediatric patients were categorised into conventional cystolithotripsy using shockpulse, trilogy, or lithoclast (Group 1) and laser cystolithotripsy (Group 2). Data included operative details, concomitant procedures, complications, SFR, hospital stay, and 30-day re-intervention. Primary outcome was SFR, defined as no residual fragments. Secondary outcomes were complications, hospital stay, and re-intervention rate.
Results: A total of 374 patients were included (371 adult, mean age 64 ±15.4; 89.2% male; 3 paediatric). Group 1 included 198 patients and Group 2 included 176. Concomitant procedures were more frequent in the Group 2 (44.3% vs 15.2%), while operative time was shorter in Group 1 (48.3 vs 64.1 minutes, p<0.001). No peri-operative complications occurred in Group 1, while minor complications occurred in Group 2. SFR was high and comparable (94.9% in Group 1 vs 96.6% Group 2, p=0.458), with similar re-intervention rates (4.0% vs 2.8%, p=0.583). Mean length of stay was shorter in Group 2 (1.6 vs. 2.8 days, p<0.001).
Conclusion: Laser cystolithotripsy achieved high SFR with shorter hospital stay, despite more concomitant procedures, supporting an effective approach for bladder stone management.
P14-2 Retrospective review of outcomes of pyeloplasty with concomitant pyelolithotomy
Dr Ashwini Kulkarni1, Mr Francis Keeley1, Mr Salah Albuheissi1, Miss Zsuzsanna Zotter1, Mr Anthony Timoney1
1Bristol Urological Institute, Bristol, United Kingdom
Introduction: This study reviews the outcomes of pyeloplasty with concomitant pyelolithotomy at a tertiary referral centre between 2002 and 2025. The objective was to assess outcomes, focusing on stone-free rates.
Methods: Our database of patients with pelvi-ureteric junction (PUJ) obstruction was used to select patients. Of 722 patients with PUJ obstruction, 667 were managed surgically. 97 had stones, and 64 who underwent pyeloplasty and concomitant pyelolithotomy were included. 32 were performed laparoscopically and 32 robotic. 58 were primary and 6 revision procedures.
Results: Of the 64 patients included, 57 (95%) of 60 with adequate follow-up had a successful outcome demonstrated by improved drainage on MAG-3 renogram. Stones were removed in 51 (80%), were not found in 12 (19%), and were left in-situ in 1 patient. Stone-free rate was 76% for solitary stone, 53% for <5 stones and 21% for >5 stones. The overall stone-free rate was 55%. 2 patients had complications ⩾ Clavien-Dindo Grade III and 16 needed further procedures to treat stones. Nephrectomy was done for 2 of 3 patients who did not demonstrate improved drainage.
Conclusion: Pyelolithotomy with pyeloplasty is associated with low morbidity and does not appear to diminish the success of the pyeloplasty. Stone-free rates were inversely related to pre-operative stone burden. Patients with solitary stones had excellent stone-free rates after the primary procedure at 76%. The stone-free rates showed a significant downward trend with increasing stone burden (Figure 1). This highlighted the importance of pre-operative counselling for potential further procedures for stone treatment.
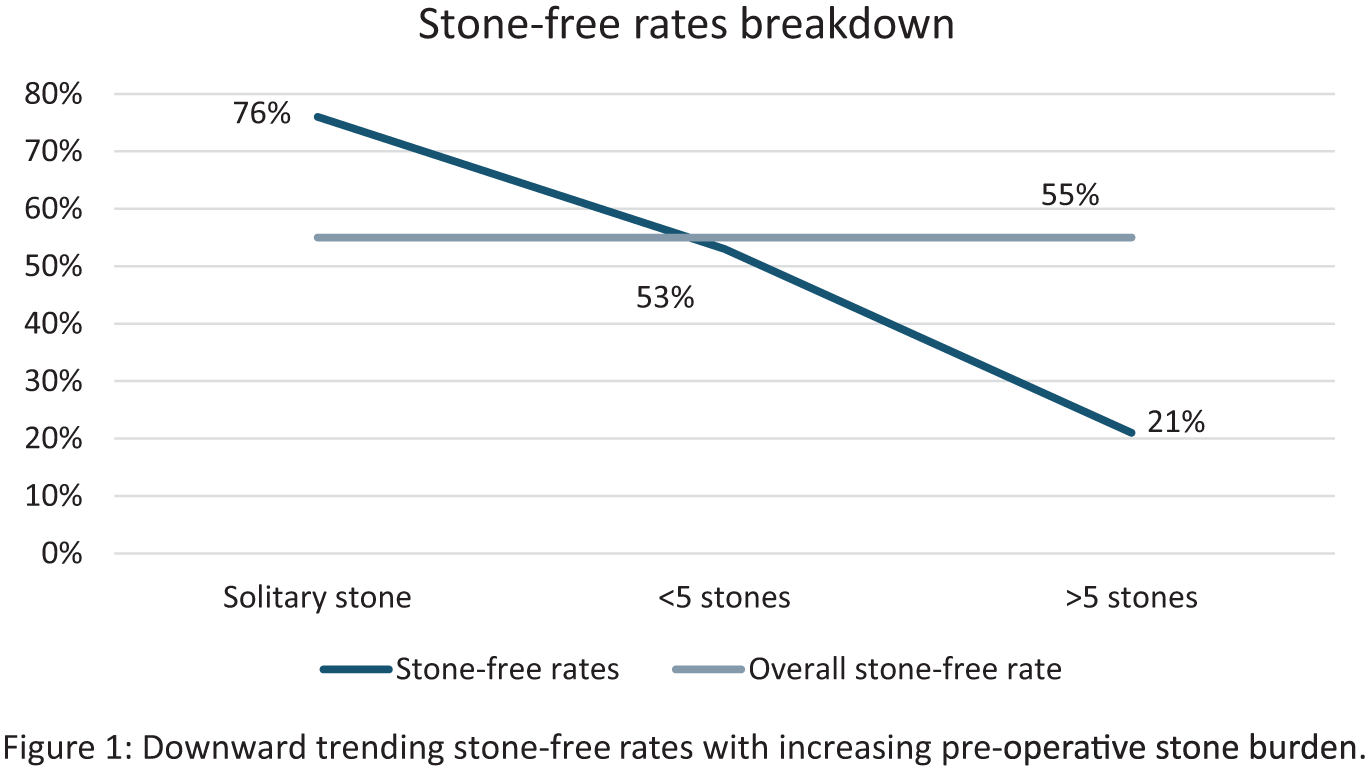
P14-3 Reassessing Antibiotic Prophylaxis in Shockwave Lithotripsy: A Systematic Review and Meta-analysis of Randomized Trials
Dr Saied Mohammed Saied Qasem1, Dr Ahmed Naji Ahmed Hassan, Dr Mustafa Ali Almomani, Dr Mohamad Wasfi Alsawalmeh, Dr Lara Hamzeh Hamzeh, Dr Asmaa Hamdy Abdellatif, Dr Mostafa Eyad Mostafa Mousa
1Faculty of Medicine, Ankara Yıldırım Beyazıt University, Ankara, Turkey, Ankara , Turkey, 2Faculty of Medicine, Sudan University of Science and Technology, Khartoum, Sudan, Khartoum, Sudan , 3Faculty of Pharmacy, Jordan University of Science and Technology, Ar-Ramtha, Jordan, 4Faculty of Pharmacy, Jordan University of Science and Technolog, Ar-Ramtha, Jordan, 5Faculty of Medicine ,Caucasus International University, Tbilisi, Georgia, 6Faculty of Medicine, Qena University, Qena, Egypt, Qena, Egypt, 7Faculty of Medicine, Hashemite University, Alzarka, Jordan
Introduction: The role of antibiotic prophylaxis (AP) in patients undergoing shockwave lithotripsy (SWL) with sterile preoperative urine remains controversial. We performed a systematic review and meta-analysis with trial sequential analysis (TSA) to assess whether AP reduces post-SWL infectious complications.
Patients and Methods: PubMed, CENTRAL, Scopus, ScienceDirect, and Web of Science were searched from inception to December 2025 for randomized controlled trials comparing perioperative AP with placebo or no prophylaxis in adults undergoing SWL with sterile urine. Primary outcomes were symptomatic urinary tract infection (UTI) and asymptomatic bacteriuria (AB). Random-effects meta-analyses, sensitivity analyses excluding high risk-of-bias studies, subgroup analyses by urinary tract instrumentation status, and TSA were performed.
Results: Twelve randomized controlled trials including 3,653 patients were analyzed. AP was associated with a lower risk of symptomatic UTI but did not reach statistical significance (RR 0.50, 95% CI 0.21–1.18; p=0.11; I²=23%). Sensitivity analysis excluding high risk-of-bias studies showed a similar estimate approaching significance (RR 0.51, 95% CI 0.25–1.02; p=0.06). Subgroup analyses showed no significant benefit of AP for UTI or AB among patients with or without urinary tract instrumentation, including those with indwelling stents, suggesting limited benefit even in traditionally high-risk subgroups. TSA demonstrated that evidence for clinical UTI remains underpowered, whereas TSA for AB crossed the futility boundary, indicating further trials are unlikely to demonstrate benefit.
Conclusions: Antibiotic prophylaxis does not significantly reduce infectious complications after SWL in patients with sterile urine. Subgroup and TSA findings support uncertainty for clinical UTI and futility for asymptomatic bacteriuria, reinforcing antimicrobial stewardship.
P14-4 Optimizing Symptom Control After Ureteral Stent Placement: A Systematic Review of Pharmacological Interventions from EAU Endourology
Arianna Pischetola, Dr Yuan Wen Ooi1, Ali Talyshinskii, Professor Bhaskar Somani
1University Hospital Southampton, Southampton, United Kingdom
Introduction: Ureteral stent-related symptoms (SRS) significantly impairs patient quality of life across urinary, pain, and general health domains. This review evaluated the efficacy of pharmacological interventions in alleviating SRS using validated patient-reported outcome measures.
Methods: This review followed PRISMA guidelines and was prospectively registered with PROSPERO (ID: CRD420251163437). PICO: Adult patients (⩾18 years) undergoing ureteral DJ placement (P) receiving pharmacological therapy (I) compared with placebo or alternative regimens (C), assessing improvement in SRS using the Ureteral Stent Symptom Questionnaire (USSQ) (O). The primary outcome was overall and domain-specific improvement in USSQ scores; secondary outcomes compared mono- vs. combination pharmacotherapy. Risk of bias was calculated.
Results: Fifteen randomized controlled trials comprising 2,335 patients were included (mean age 42.4 ± 12.8 years; 63.5% male). Urolithiasis and post-ureteroscopic stenting were the most frequent indications. Five major pharmacological classes were identified: α-blockers, anticholinergics, β3-agonists, GABA agonists, and phosphodiesterase type-5 inhibitors (PDE5i). All pharmacological interventions were superior to placebo, underscoring the benefit of medical management. Combination therapy consistently outperformed monotherapy and placebo across all USSQ domains, while PDE5i-containing regimens enhanced sexual function. The 3 most effective regimens were α-blocker + anticholinergic + PDE5i (USSQ 46.78), anticholinergic + PDE5i (55.19) and α-blocker + anticholinergic (53.49). Risk of bias analysis was low to moderate risk of bias.
Conclusions: Pharmacological therapy significantly improves stent-related symptoms, with combination regimens, particularly including anticholinergics, provide the most comprehensive symptom relief. A multimodal pharmacological approach should be considered to optimize quality of life following ureteral stent placement.
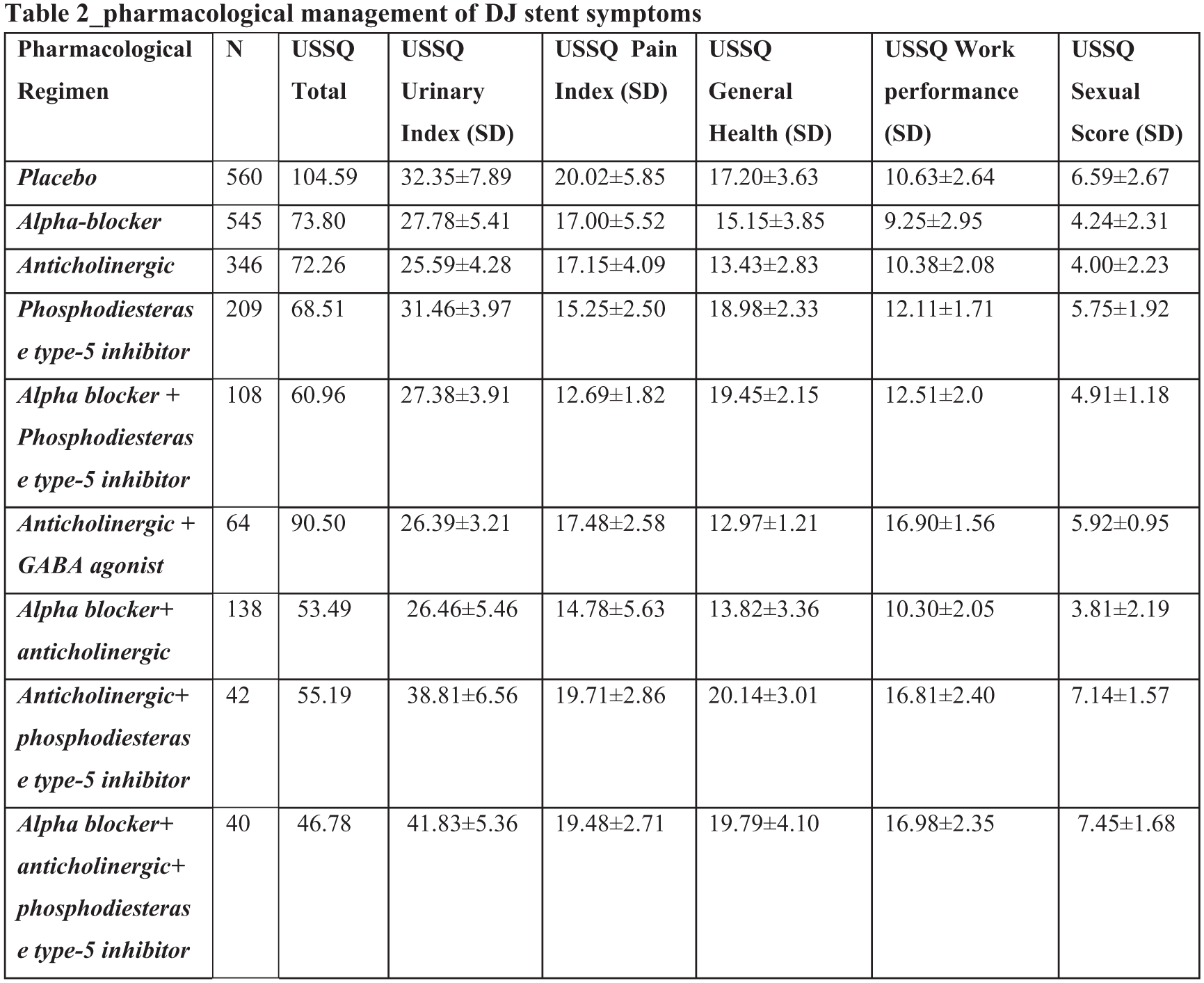
P14-5 Improving Patient Understanding Following Renal Colic Through Targeted Information Leaflets in the Emergency Department
Miss Sai Kalpitha Eragamreddy1, Miss Lap Yan Leung1, Dr Suraya Gafore1, Dr. Gaurika Bharadwaj1, Mr. Hamid Abboudi1, Mr. Tamer El-Husseiny1, Mr. Milad Hanna1, Mr. Ranan Dasgupta1
1Department of Urology, Charing Cross Campus, Imperial College Healthcare NHS Trust, London, United Kingdom
Introduction: Patients discharged from the Emergency Department (ED) with renal colic often report poor understanding of their diagnosis, analgesia, and follow-up pathway, contributing to anxiety and avoidable reattendance. This quality improvement project (QIP) assessed whether a targeted renal stone information leaflet could improve patient understanding and satisfaction following ED discharge.
Methods: A closed-loop QIP was conducted across two tertiary centres over two data-collection cycles. In Cycle 1 (October–December 2024), 95 patients awaiting Renal Colic Virtual Clinic (RCVC) follow-up were contacted using a structured questionnaire assessing baseline understanding of diagnosis, discharge advice, reattendance guidance and the perceived value of written information (32 female, 63 male).
In March 2025, a patient-facing renal stone leaflet was introduced, incorporating visual diagrams, QR codes linking to treatment explanations and dietary advice aligned with British Association of Urological Surgeons (BAUS) guidance. The leaflet was distributed in paper format within ED and made available digitally via Urology department website.
Cycle 2 (April–June 2025) included 162 patients (68 female, 94 male), of whom 134 received the leaflet or accessed the digital version.
Results: Following introduction of the leaflet, patient-reported understanding of diagnosis, treatment and follow-up pathway improved with the majority of patients reporting better understanding compared with baseline.Unplanned ED reattendance prior to RCVC remained low and was predominantly pain-related.
Conclusion: A targeted renal stone information leaflet improved patient understanding and satisfaction following ED discharge for renal colic. This closed-loop QIP supports the use of accessible patient information tools to enhance engagement and support safer emergency urological care pathways.
P14-6 Pulling the string: Patient-reported outcomes following self-removal of ureteric stents using extraction strings
Miss Aswathy Pavithran1, Miss Louise Paramore1, Miss Susan Hall1, Mr Jonathan Lee1, Mr Stephen Miller1, Mr Hari Ratan1, Mr Dhaval Bodiwala1
1Nottingham City Hospital, Nottingham, United Kingdom
Introduction: Ureteric stents are commonly placed following ureteroscopy and usually require removal via flexible cystoscopy. Attaching extraction strings allows patients to remove stents at home, potentially reducing stent dwell time, minimising hospital visits, and lowering healthcare costs whilst potentially improving the patient experience.
Patients and Methods: In January 2025, we introduced ureteric stents with extraction strings for selected patients, supported by a detailed patient information leaflet explaining self-removal and providing contact details for assistance. Over a twelve-month period, patient-reported outcomes were collected prospectively using a questionnaire, accessible via post or a QR code linking to an online survey.
Results: Among patients who responded, self-removal of stent was well accepted, with 86% rating the process as very easy to easy in difficulty. Pain during removal was minimal: 90% reported no or mild pain, 5% moderate pain, and 5% severe pain. Pre-removal anxiety was common, with 15% being terrified. Despite this 90% removed the stent independently and 100% found the instructions clear. Recovery was rapid: over 60% returned to normal activities on the same day. Willingness to use the same method in the future was high (90%). There were four Clavien–Dindo grade I complications, one grade II complication, and one grade IVa complication.
Conclusion: Self-removal of ureteric stents using extraction strings appears safe and acceptable for selected patients. If adopted more widely, this approach could make stent removal simpler for patients, ease pressure on outpatient services, free up cystoscopy appointments for diagnostic purposes, and lead to significant cost savings.
P14-7 Nurse led stone clinic for Urolithiasis: Establishing a guideline-based service using PROM triage
Mr Manash Chakraborty1, Mr Sabin Yadav1, Mrs Alison Wiles1, Miss Hannah Wells1, Professor Hrishi Joshi1
1University Hospital of Wales, Cardiff, United Kingdom
Introduction: Urolithiasis is common and associated with high recurrence, requiring resource-intensive follow-up. Although virtual nurse-led clinics offer a potential alternative, a standardised, patient-centred follow-up pathway is lacking in the UK. This service evaluation describes the implementation of a guideline-based, PROM-driven nurse-led model for urolithiasis follow-up.
Patient and Methods: A specialist nurse-led virtual clinic was developed in line with NICE and EAU guidance. It incorporates pre-clinic PROM-based triage, virtual review with imaging, and pathway-driven management. Patients with recurrent or residual renal stones and those with ureteric stones under expectant management were included following initial consultant review. Outcomes included patient safety, appropriateness of management decisions, and their correlation with PROM scores, radiological findings, and need for consultant input.
Results: Eighty-five patients were reviewed between January and December 2025 (mean age 54.2 years; 75.3% male). 67% were post-treatment follow-ups, while 24.7% were managed for ureteric stones. 77.6% remained under nurse-led follow-up, 15.3% were discharged, 4.7% required consultant review due to rising PROM scores, and 2.3% required active intervention. Clinic outcomes demonstrated good correlation with USIQOL scores and imaging, with ROC analysis showing acceptable discrimination (AUC 0.77 and 0.73). Logistic regression confirmed PROM scores as significant predictors of escalation.
Conclusion: A virtual, PROM-based nurse-led stone follow-up clinic is a safe, patient-centred, and reproducible model of care that aligns with GIRFT and NHS outpatient transformation priorities. It reduces consultant workload, improves patient education and engagement, and is straightforward to implement, with potential for wider adoption. Further multicentre evaluation and patient feedback are planned.
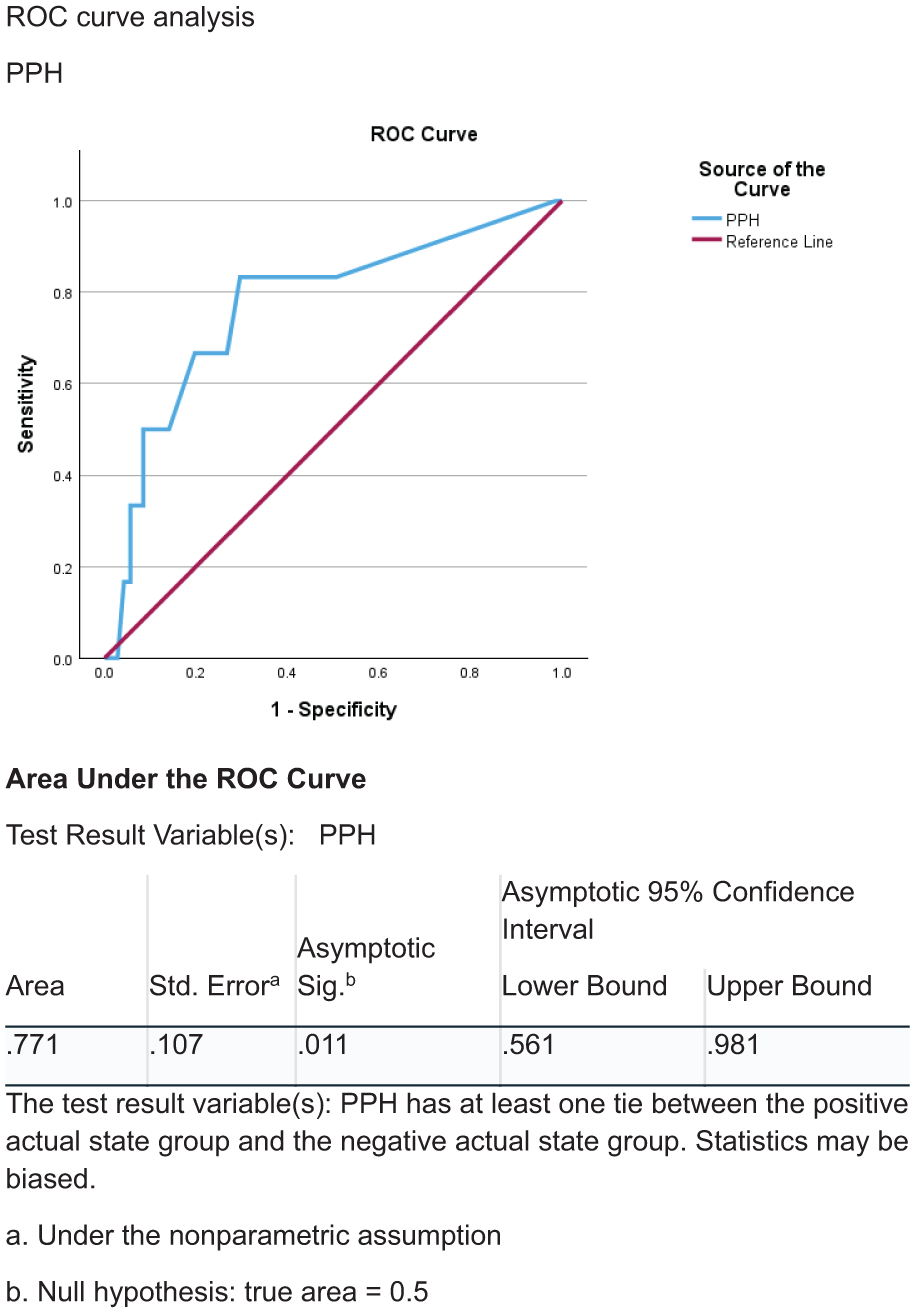
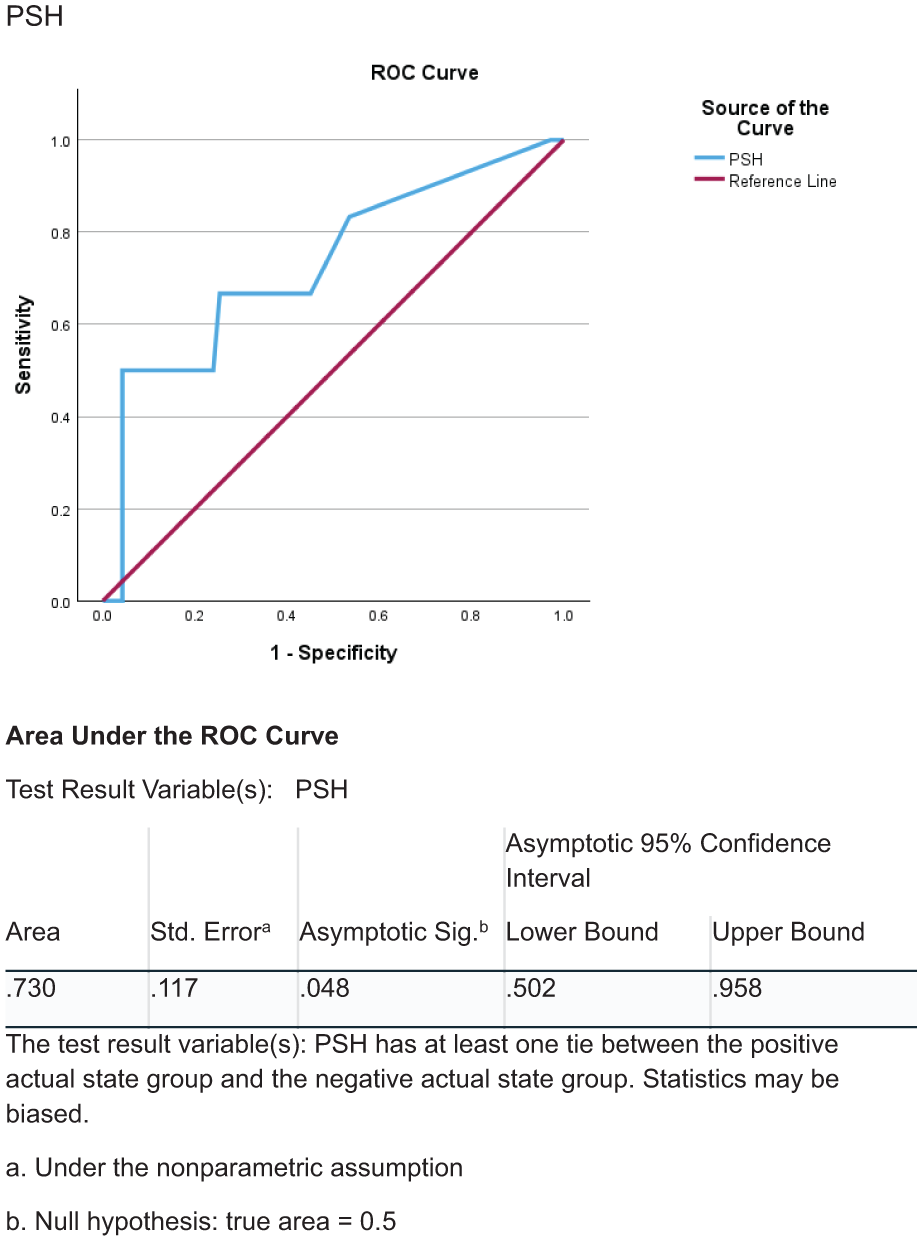
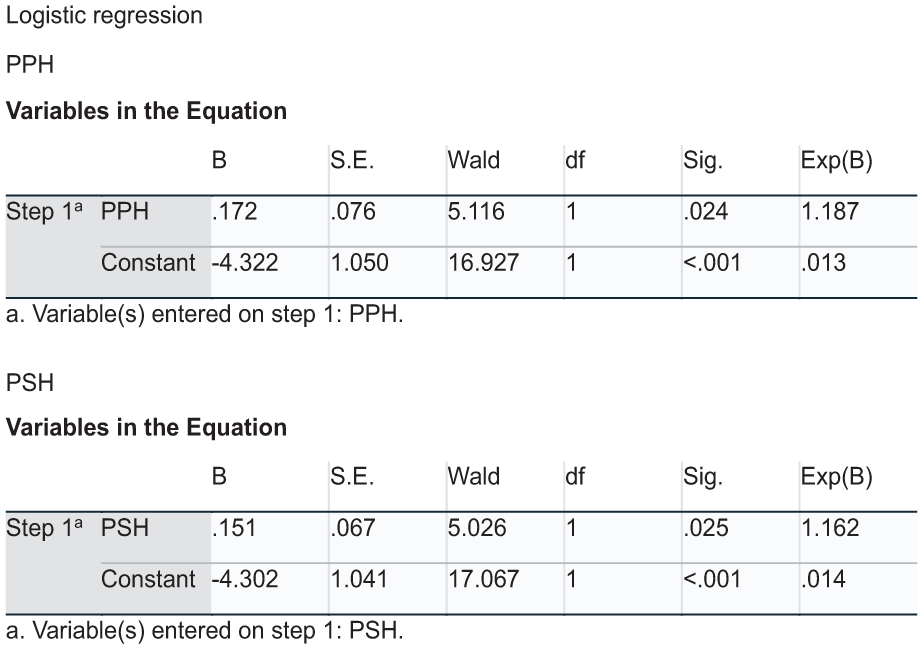
P14-8 Exome-wide association of kidney stone disease in the UK Biobank
Dr Catherine Lovegrove1,2, Professor Michael Holmes3, Professor Dominic Furniss2,4, Professor Sarah Howles
1Glasgow University, Glasgow, United Kingdom, 2University of Oxford, Oxford, United Kingdom, 3University of Bristol, Bristol, United Kingdom, 4Oxford University Hospitals NHS Foundation Trust, Oxford, United Kingdom
Introduction: Kidney stone disease (KSD) has a heritability of ~50%. To date, large-scale genetic association studies in KSD have considered common genetic variants; these account for ~19% of this heritability. To elucidate additional genetic risk factors and identify disease-causing genes we conducted an exome-wide association study (ExWAS).
Materials & Methods: We performed an ExWAS in the UK Biobank considering 11,225 KSD cases and 381,369 controls. We identified KSD cases using ICD9/10, OPCS3/4, primary care, and self-report codes. We studied 5.1 million variants and conducted collapsing analyses of protein-truncating, missense, non-synonymous, and predicted deleterious (Combined Annotation Dependent Depletion (CADD) score ⩾25) variants.
Results: Single variant analyses identified 10 independent variants significantly (P<5x10-8) associated with KSD including missense variants in NBPF3 (Pro281Ser, effect allele frequency (EAF)=0.02, odds ratio (OR)=1.35, 95%-confidence-interval (CI)=1.22-1.49, P=2.95x10-9) and ABCC6 (Arg950Trp, EAF=0.97, OR=1.29, 95%-CI=1.18-1.41, P=1.79x10-8). Non-coding variants were identified at loci with previously reported genome-wide associations, including ALPL, SLC34A1, AMPD3, DGKH, UMOD, CLDN14, and GNAZ.
Collapsing analyses revealed associations of KSD with ALPL, SLC34A1, SLC34A3, and SLC26A2 (Figure A). Effects for ALPL, SLC34A1, and SLC34A3 were driven multiple rare variants whilst SLC26A2 effects were driven by the missense variant Thr574Ile (EAF=0.99 OR=1.28, 95%-CI=1.12-1.45, P=2.25x10−4, predicted benign). SLC26A2 has not previously been associated with KSD and encodes the sulphate transporter which is expressed in the proximal tubule.
Conclusions: This large-scale ExWAS identifies novel associations of KSD with SLC26A2 and affirms the importance of ALPL, SLC34A1, and SLC34A3 in KSD. SLC26A2 may contribute to KSD pathogenesis by altered oxalate metabolism.
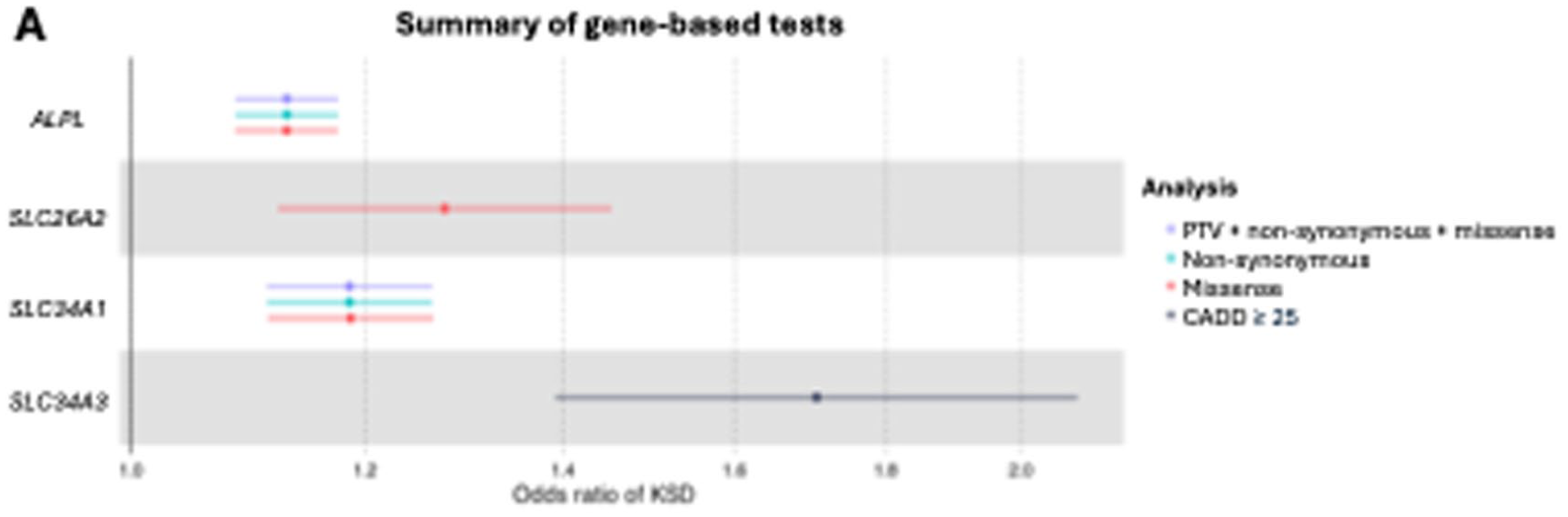
P14-9 Retrograde Intrarenal Surgery Versus Mini-Percutaneous Nephrolithotomy for Treatment of Medium size pediatric renal stones (10-20millimeters). A Randomized controlled trial
Dr Ramy Elbaz1, Dr Mahmoud Lamon, Prof Tamer Helmy, Prof Mahmoud Kenawy, Prof Ahmed Shoma
1Urology and Nephrology Center, Mansoura, Egypt, 2Scunthorpe General Hospital, Scunthorpe, United Kingdom
Objective: To assess the efficacy of mini PCNL versus RIRS in the treatment of medium size pediatric renal stones (1-2 cm).
Methods: In this randomized controlled trial, 114 children younger than 12 years were randomly allocated in 2 groups. The first group underwent mini PCNL 15 Fr and the second group underwent flexible URS. Both groups were compared regarding preoperative demographic characteristics of the patients, stone parameters, intraoperative parameters -including total operative time, fluoroscopy time, lasing time, renal pelvis perforation risk and need for JJ stent fixation- and post operative parameters including fever, hemoglobin drop, pain score, need for secondary procedures, initial stone free rate (SFR) and SFR after 1 month.
Results: Table 1 and 2 showed that both groups were comparable regarding the initial SFR and SFR after 1-month (93% and 89 % for group 1 and group 2, respectively) and the need for secondary procedures. However, the flexible URS group had a statistically significant shorter operative time (61.4 min ± 21 versus 92 min ± 31.3) and fluoroscopy time compared to mini PCNL group (p < 0.001). Regarding the need for postoperative JJ stent fixation, it was significantly higher in RIRS. For postoperative parameters, both groups were comparable regarding post operative fever, pain score, need for blood transfusion and hospital stay.
Conclusion: Both mini PCNL and RIRS are safe and equally effective modalities for treatment of medium size pediatric urolithiasis with comparable SFR.
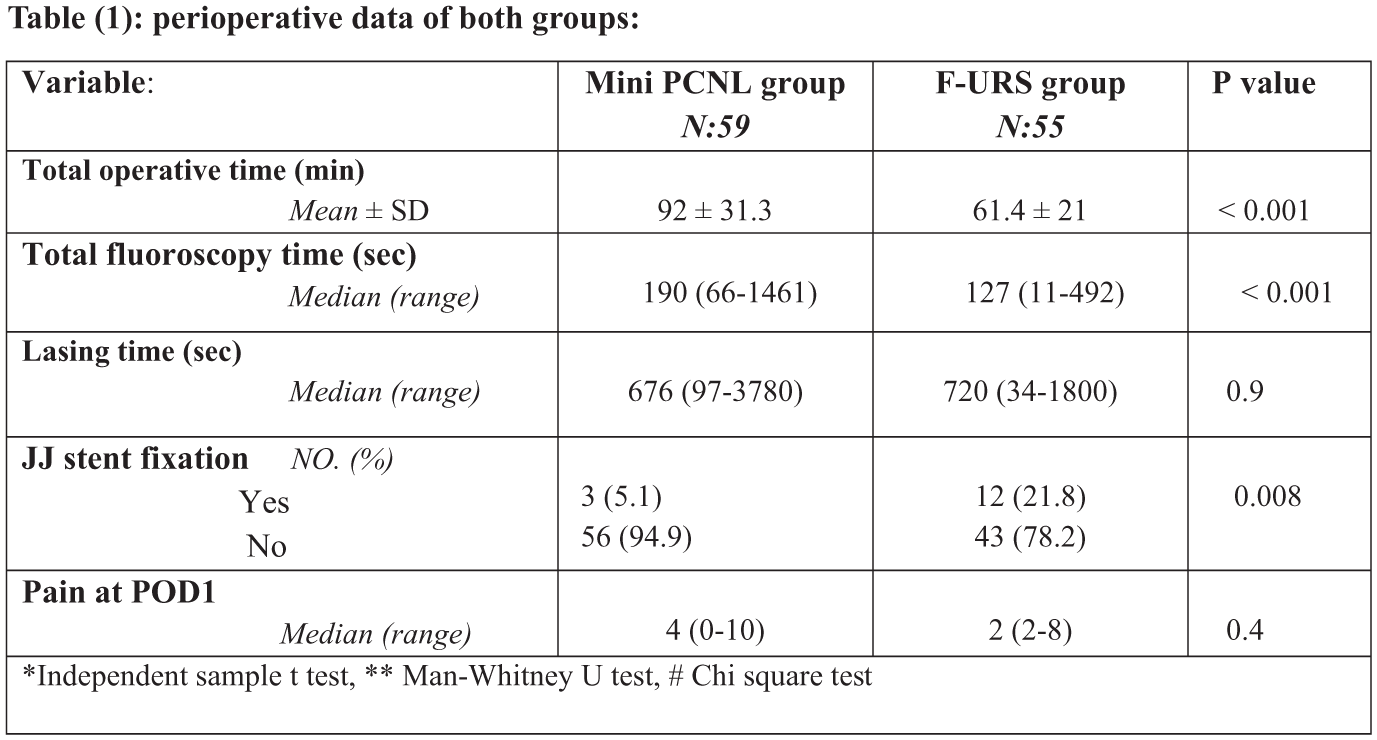
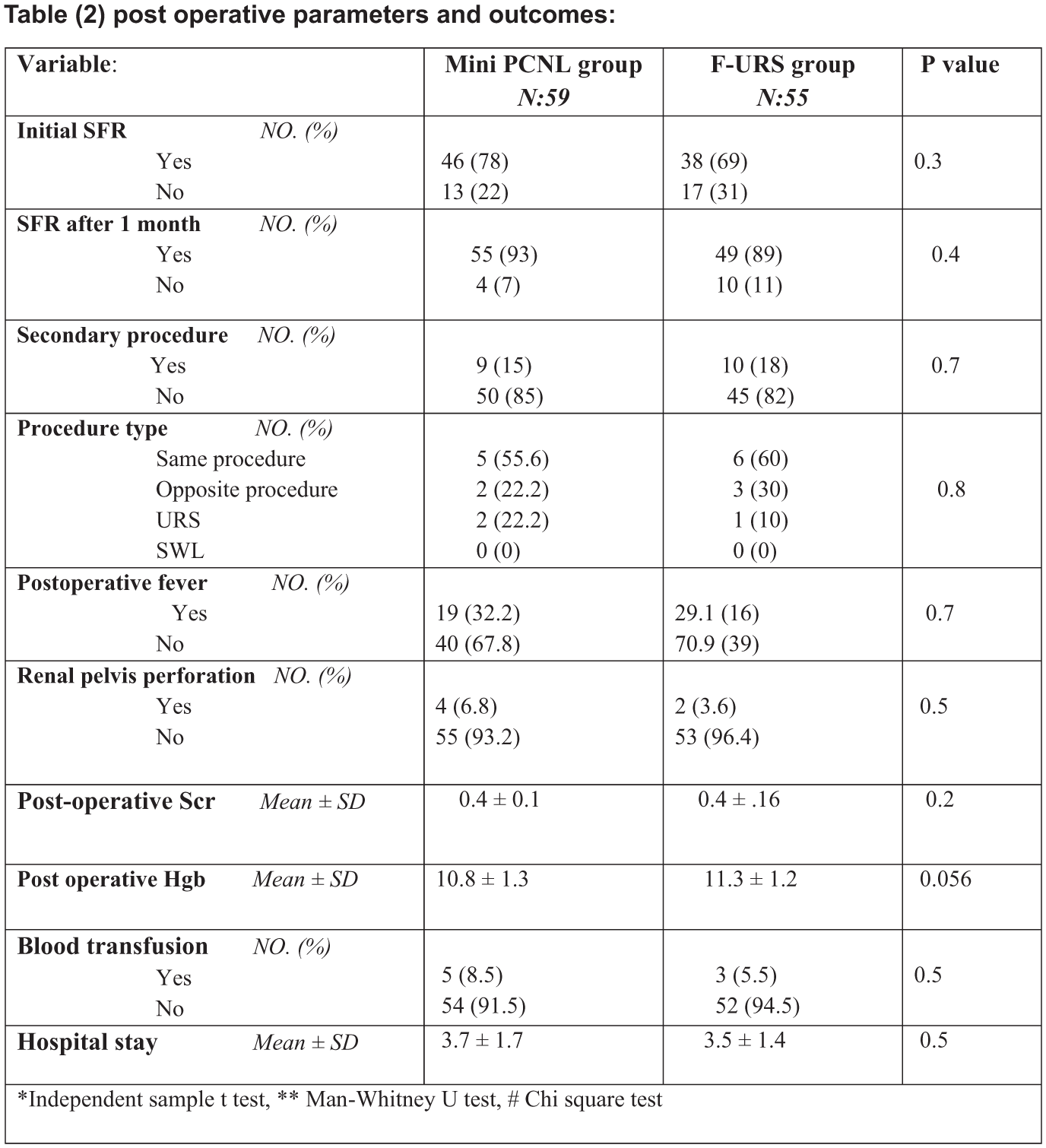
P14-10 An automated stent registry within EPIC electronic patient record
Miss Helen Stephens1, Ms Ann Crump1, Mr Luke Foster1, Prof Ben Grey1, Mr Thomas Brophy1
1Manchester Foundation Trust, Manchester, United Kingdom
Introduction: Ureteric stent tracking is essential to prevent forgotten stents and associated morbidity. Many units rely on manual stent registries, which are time-consuming and prone to human error. With digitalisation of healthcare, electronic patient records (EPRs) offer an opportunity to automate stent tracking using routinely collected data. This study describes the development and validation of an automated stent registry within the EPIC EPR.
Methods: Mandatory implant data recorded at the time of stent insertion within the EPR are used to generate an automated report of all implanted stents. The report extracts patient identifiers, procedure dates, and an expected removal date without additional clinician input. The automated registry was retrospectively cross-checked against the existing manual stent register to assess completeness and accuracy.
Results: The automated EPR-generated report successfully captured all implanted ureteric stents when cross-checked against the manual register. Generation of the automated registry requires no further manual input as implants are scanned into the patients EPR on insertion in theatre, eliminating the need for duplicate data entry. On removal of the stent, explant data is completed, resulting in the patient automatically dropping off the registry, whereas patients remained on the manual registry longer.
Conclusions: Within the EPIC EPR, it is possible to develop an automated, contemporaneous stent registry from live implant data which outperforms a manual register. Automated stent registries have the potential to significantly reduce the risk of forgotten stents and reduces administrative burden on the clinical team.
ePoster Session 15: Prostate Cancer 2, John Blandy, June 17, 2026, 08:00 - 09:00
P15-1 Follow-Up Outcomes After an Initial Negative Prostate Biopsy According to Pre-Biopsy mpMRI Findings: A MULTIPROS Sub-Analysis
Ms Wafa Aloufi1,2, Dr Magdalena Szewczyk-Bieda3, Professor Ghulam Nabi1, Dr Xinyu Zhang1, Dr Yilong Zhang1, Dr Cheng Wei1, Dr Luigi Manfredi1
1University Of Dundee, Dundee, United Kingdom, 2Taif University, Taif, Saudi Arabia, 3Ninewells Hospital, Dundee, United Kingdom
Introduction: Outcomes following a negative prostate biopsy are poorly defined and may vary according to pre-biopsy mpMRI findings. This exploratory analysis evaluated follow-up outcomes in biopsy-naïve men with negative biopsy results, stratified by pre-biopsy mpMRI.
Patients and Methods: This post-hoc exploratory sub-analysis of the prospective MULTIPROS randomised trial included men enrolled between 2015 and 2020 with no csPCa detected at initial biopsy. Two cohorts were analysed: men with negative mpMRI (PI-RADS ⩽2) and negative systematic biopsy (n=99), and men with suspicious mpMRI (PI-RADS ⩾3) but negative biopsy (n=153). Follow-up involved PSA monitoring and clinical assessment, with repeat imaging or biopsy as indicated. The primary outcome was csPCa detection (ISUP ⩾2).
Results: Over a median follow-up of 5 years, csPCa was detected in 4/99 men with negative mpMRI and biopsy, compared with 37/153 men with suspicious mpMRI but negative biopsy. In the MRI-negative cohort, all csPCa diagnoses were preceded by PSA elevation or clinical concern. In the MRI-positive cohort, 28/37 cases were detected within ⩽6 months and 9/37 after >6 months. Of those detected within ⩽6 months, 21/28 (75%) followed initial systematic biopsy alone, while 7/28 (25%) followed combined targeted and systematic biopsy.
Conclusions: Follow-up outcomes after a negative prostate biopsy differed by pre-biopsy mpMRI findings. csPCa was rare after negative mpMRI and biopsy, but some men with suspicious mpMRI and negative biopsy were diagnosed during follow-up, often within 6 months, suggesting missed disease at initial biopsy. Targeted biopsy may reduce the risk of missing clinically significant cancer, pending validation in larger cohorts.
P15-2 Development and Validation of A Novel Risk Model for 10-Year Other-Cause Mortality in Radical Prostatectomy Candidates: Implications for Patient Selection
Dr Davide Farinati1, Dr Francesco Barletta1, Dr Paolo Zaurito1, Dr Alejandro Granados3, Dr Nicholas Raison2,3, Dr Prokar Dasgupta2,3, Dr Giorgio Gandaglia1, Dr Alberto Briganti1
1Unit of Urology/Division of Oncology, URI, IRCCS Ospedale San Raffaele, Milano, Italy, 2Department of Urology, Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom, 3School of Biomedical Engineering & Imaging Sciences, King’s College London, London, United Kingdom
Introduction: Current guidelines recommend radical prostatectomy (RP) for prostate cancer (PCa) patients with a life expectancy ⩾10 years, yet tools to predict other-cause mortality (OCM) based on comorbidities are limited. We developed a novel RP-specific risk score to predict 10-year OCM and improve patient selection.
Patients and Methods: We analyzed 9,445 patients treated with RP between 1985 and 2024 at a single center, excluding those receiving neoadjuvant therapy. Preoperative comorbidities were prospectively collected and the age-adjusted Charlson Comorbidity Index (CCI) calculated. An eXtreme Gradient Boosting (XGBoost) algorithm selected variables associated with OCM. A risk score predicting 10-year OCM was developed in a training cohort (n=6,611) and validated in a testing cohort (n=2,834). Discrimination was assessed using the C-index and compared with CCI; decision curve analysis (DCA) evaluated net benefit.
Results: Median age was 65 years and median PSA was 6.5 ng/ml. Median follow-up for survivors was 68 months, with 335 OCM events. Ten-year OCM-free and cancer-specific mortality–free survival were 93% and 97%, respectively. Key predictors included age, PSA, biopsy ISUP grade, cardiovascular and metabolic conditions, smoking status, BMI, and other comorbidities. The novel score outperformed CCI (C-index 72% vs. 67%) and showed higher net benefit on DCA.
Conclusions: This novel, procedure-specific risk score more accurately predicts 10-year OCM than CCI and may support better selection of RP candidates with sufficient life expectancy.
P15-3 5 year risk of post-prostatectomy radiotherapy in England: a national population level study
Dr Matthew Parry1, Dr Davide Maffei1, Dr Busola Adebusoye1, Dr Arjun Nathan2, Dr John Withington1, Prof Caroline Moore1, Prof Jan van der Meulen2, Dr Alison Tree4, Prof Noel Clarke5
1University College London, London, United Kingdom, 2London School of Hygiene and Tropical Medicine, London, United Kingdom, 3The Royal College of Surgeons of England, London, United Kingdom, 4The Institute of Cancer Research, London, United Kingdom, 5The Christie NHS Foundation Trust, Manchester, United Kingdom
Introduction: There are no contemporary national data in England reporting the use of radiotherapy after radical prostatectomy.
Materials and Methods: English Cancer Registry data and administrative hospital data were used to identify 22,384 men diagnosed with non-metastatic prostate cancer in the English NHS (April 2014 to September 2018) and treated with radical prostatectomy. The national Radiotherapy Data Set (RTDS) was used to identify men who went on to have post-prostatectomy radiotherapy within 5 years. 7,887 men (35%) were excluded due to missing cancer variables (PSA, T stage, Gleason grade group). 5-year risk of post-prostatectomy radiotherapy was stratified according to PSA, T stage and Gleason grade group, where cell sizes of 20 or less were suppressed.
Results: We identified 14,497 men treated with radical prostatectomy with complete cancer variables. The most common cancer profile of PSA <10ng/ml and Gleason grade group 2 had a 5-year radiotherapy risk of 7% for T2 (3,487 men) and 16% for T3a (1,596 men). Radiotherapy risk increased to over 40% according to combinations of at least two higher risk features (PSA >20ng/ml, T3a, Gleason grade group 4), and over 60% for specific cases with very high-risk features (T3b, Gleason grade group 5).
Conclusion: In most cases the use of radiotherapy after radical prostatectomy is expected to be up to 16%. This risk increases with combinations of increasingly higher risk features and most marked at 79% for cases of PSA >20ng/ml, T3b and Gleason grade group 5.
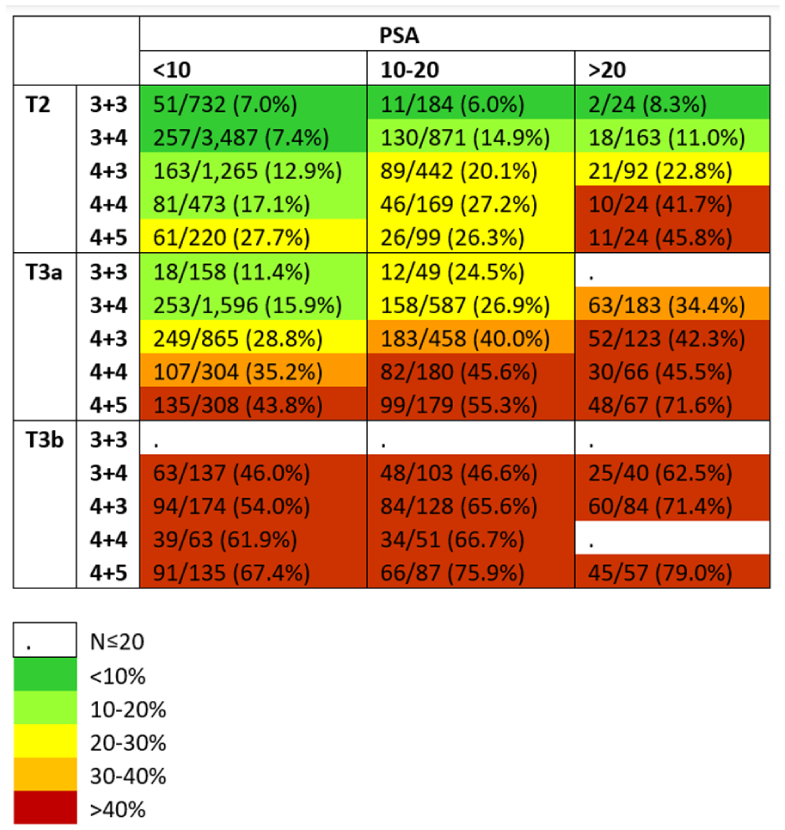
P15-4 Reduced Incidence of Incisional Hernia with Left Paramedian Access During RARP: A UK-Based Analysis
Dr Tom Cahill2, Ms Mia Tazi1, Dr Andri Orrason2, Dr Duncan Self2, Dr Netty Kinsella2, Dr Declan Cahill2
1King’s College London, London, 2Royal Marsden Hospital, London,
Introduction: Radical prostatectomy is the most common major complex urological procedure in the UK (n = 8,760 in 2023; NPCA), predominantly performed robotically (RARP). Extraction port-site incisional hernia (IH) is a recognised complication that may require laparoscopic or open mesh repair, both associated with morbidity. This audit compares two extraction port techniques with respect to IH incidence.
Methods: A retrospective audit was conducted of patients undergoing RARP between 2015 and 2023 by a single surgical team. Two extraction port techniques were compared. Group 1 (2015-2020; n = 917) used a midline supraumbilical incision through the linea alba. Group 2 (2020-2023; n = 744) used a left paramedian incision with transverse anterior rectus sheath incision, muscle splitting, and longitudinal posterior sheath incision, with closure of the anterior sheath only. All other aspects of the RARP technique were identical. Patients were followed for 2 years postoperatively before discharge to primary care. IH was diagnosed clinically and radiologically. Incidence between groups were compared(p < 0.05).
Results: Mean time to IH presentation was 9 months. IH incidence was significantly lower in Group 2 compared with Group 1 (0.3% [2/744] vs 2.4% [22/917]; p < 0.05). No compromise in surgical access or port placement was observed with the left paramedian approach.
Conclusion: Left paramedian extraction site during RARP is associated with a markedly reduced incidence of incisional hernia compared with a midline supraumbilical approach. Applied to UK practice, this represents a substantial reduction in hernia repairs without compromising surgical access or efficiency.
P15-5 Unravelling genomics of prostate cancer using a bioinformatics approach
Mr Omar H Ali1,2, Dr Sergio Llaneza Lago2, Professor Robert D Mills1,2, Professor Colin Cooper2, Professor Daniel Brewer2
1Norfolk & Norwich University Hospital, Norwich, United Kingdom, 2University of East Anglia, Norwich, United Kingdom
Introduction: There is growing interest in the development of non-invasive tests for prostate cancer (PCa) diagnostics. Extracellular vesicles (EVs) contain key genetic markers yielding both diagnostic and prognostic information, and these are extracted from urine. We aimed to examine differences in genomic profiles between different PCa Gleason Grade Groups (GGs) using EVs.
Patients and Methods: Between 2022 and 2024, patients undergoing investigations for prostate cancer at a university hospital were invited to participate in the study. They provided urine samples and each sample was processed using Affymetrix technology to extract EVs and build a global expression profile of genes. Subsequently, patients had a prostate biopsy ascertaining their PCa GGs. Differential gene expression (DGE) analysis was conducted using R.
Results: 351 patients participated in the study. Patients were allocated to PCa GGs as follows: GG1 64, GG2 37, GG3 32, GG4 16, GG5 47, and ‘negative biopsy’ 155. GG3 onwards mark prostate cancer with faster growth rate compared to lower grades, and DGE analysis demonstrated 734 upregulated genes, 399 downregulated genes, and 19,962 genes with no statistically significant differential expression. Amongst the top upregulated genes was S100A8, which codes for calcium-binding protein involved in cell cycle progression and differentiation.
Conclusions: Differentially expressed genes exist between PCa GGs, suggesting important changes in gene regulation as part of the cancer pathogenesis. This DGE analysis demonstrates that a wealth of relevant biomarkers can be extracted from urinary EVs and a bioinformatics-based predictive model is currently being developed through ongoing supervised machine learning work.
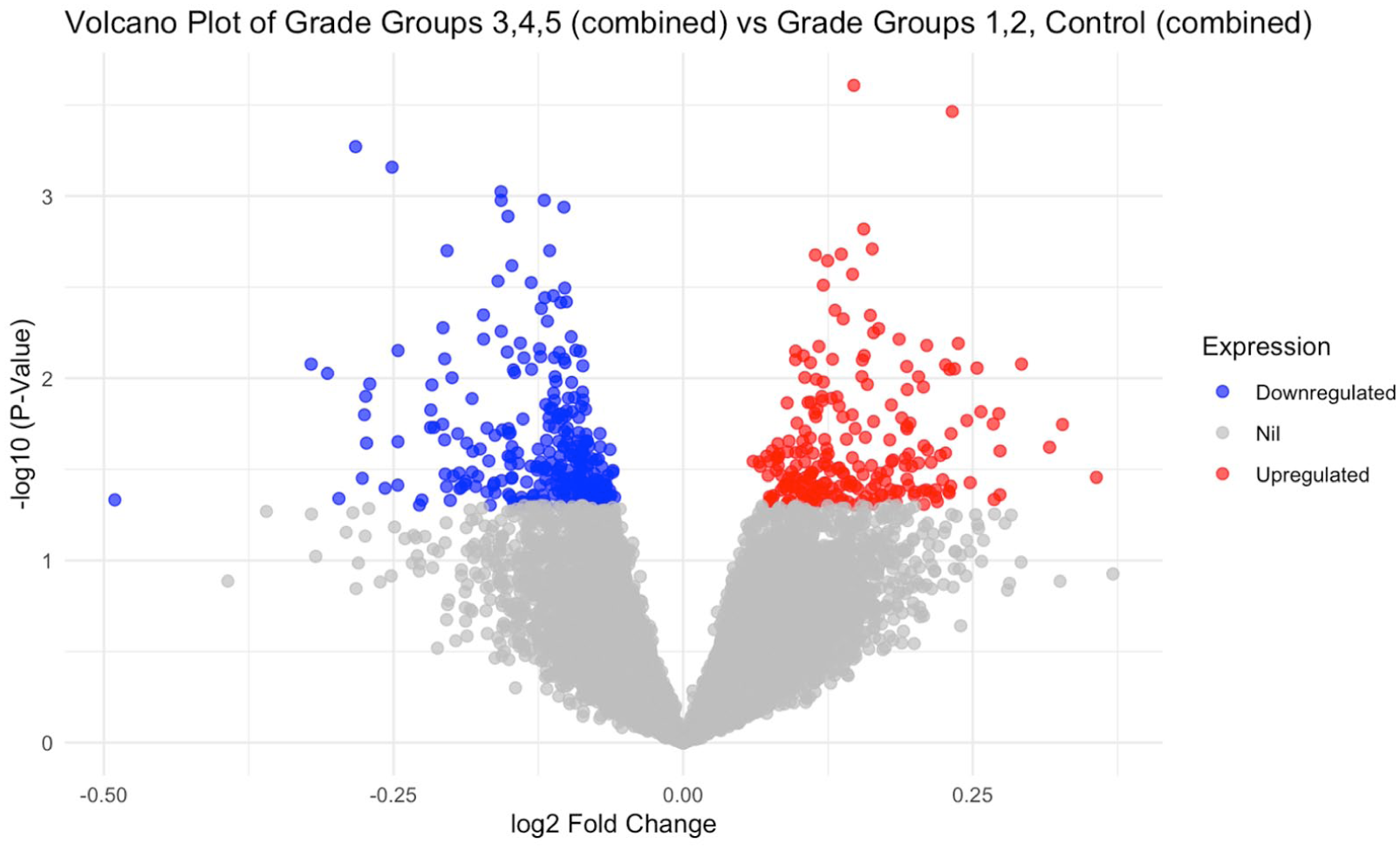
P15-6 Exit Strategy: How Specimen-Extraction Site Influences Incisional Hernias After RARP: a systematic review and network meta-analysis
Dr Jeremy Bolton1, Dr Saad Fahd1, A/Prof Joseph Ischia1, A/Prof Marlon Perera1, Dr Niranjan Sathianathen1
1Austin Hospital, Heidelberg, Australia
Introduction: Incisional hernia at the specimen-extraction site is a clinically important complication after robotic-assisted radical prostatectomy (RARP), and one that can require surgical intervention to repair. The aim of this study was to assess differences in rates of extraction-site incisional hernia between commonly used surgical specimen-extraction techniques (supraumbilical vertical, supraumbilical transverse, lateral port site, and separate Pfannenstiel incision) in patients undergoing RARP.
Methods: We performed a systematic search of multiple databases up to July 2025. We included comparative studies of participants undergoing RARP who had their surgical specimen extracted through different approaches. The primary outcome was the incidence of incisional hernia. We performed a network meta-analysis to compare the risk of incisional hernia between different techniques of specimen extraction.
Results: We included five studies of 4,243 men undergoing RARP. The incidence of incisional hernia at the specimen extraction site was 9.5% (n=402). Using a separate Pfannenstiel incision to extract the specimen resulted in a significant reduction of incisional hernias compared to the supraumbilical vertical incision [RR 0.11, 95%CI 0.03 to 0.27]. The risk of hernias with other methods of specimen extraction (supraumbilical transverse or lateral port site) were not different to that seen with supraumbilical vertical incision (HR 0.98, 0.94).
Conclusions: Prostate specimen extraction via a separate Pfannenstiel incision was associated with a lower risk of extraction-site incisional hernia compared with other approaches. Pfannenstiel extraction should be considered for patients at increased risk of extraction-site hernia (increased prostate weight, prior abdominal surgery, elevated BMI, or rectus diastasis).
P15-7 Propensity Score Matched Analysis: focal therapy compared to robot assisted radical prostatectomy for localized prostate cancer
Miss Deepika Reddy1, Richard Fan2, Masatomo Kaneko3, Pedro Freitas4, Betty Wang5, Piroz Bahar6, Shima Tayebi7, Omar Hayek8, Michael Ayenew1, et al
1Johns Hopkins University, Baltimore, United States of America, 2Stanford University, Stanford, United States of America, 3University of Southern California, LA, United States of America, 4University of Miami, Miami, United States of America, 5Cleveland Clinic, Cleveland, United States of America, 6University of Michigan, Ann Arbor, United States of America, 7University of Chicago, Chicago, United States of America, 8University of Alabama, Birmingham, United States of America, 9Wake Forest Hospital, Winston- Salem, United States of America
Introduction: No randomised control trials have published outcomes comparing radical treatment to focal therapy for patients with localised, intermediate risk prostate cancer yet. We report on oncological outcomes from the largest multi-centre, multi-surgeon-based cohort following focal HIFU, cryotherapy and robot assisted radical prostatectomy (RARP).
Methods: Consecutive patients treated across 7 units with focal therapy, and one unit (16 surgeons) with RARP were included if PSA ⩽20ng/ml, Gleason Score ⩽4+3=7, ⩽T3a disease, up to hemi-ablation was permitted. A 1-1 match based on propensity scores was performed. Primary outcome was failure free survival(avoidance of salvage whole gland/ systemic treatment, metastases or prostate cancer related death). Secondary outcome was treatment failure (avoidance of salvage whole gland/ systemic treatment, metastases or prostate cancer related death, positive surgical margins following RARP and infield recurrence following focal therapy). Kaplan- Meier estimates(95%CI) with log rank analysis determined differences between groups.
Results: 575 and 871 patients following focal therapy and RARP were included. 420 patients were matched in each group. 72 and 79 patients following focal therapy and RARP respectively reported a failure event. 5-year failure free survival was 58% (49-68%) following focal therapy and 84% (80-88%) following RARP, p<0.0001(Figure 1). 112 and 128 patients following focal therapy and RARP respectively reported treatment failure events. 5-year treatment failure free survival was 46% (37-55%) following focal therapy and 72% (68-77%) following RARP p=0.0038.
Conclusions: Clinicians and patients must balance preserved functional against oncological outcomes when considering treatment for localised prostate cancer. Future evaluation of reasons of re-treatment following focal therapy recurrence/residual is required.
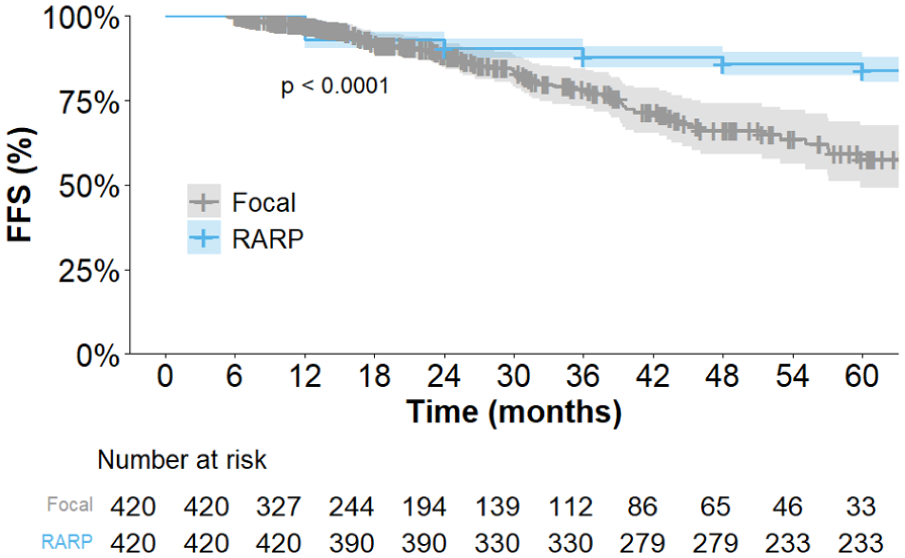
P15-8 The Introduction of Single Port Robotic Radical Prostatectomy in a UK Patient Cohort
Dr Calum Heslop1, Mr Daniel McNicholas1, Mr Tom Thompson1, Mr Ketan Agarwal1, Ms Eloise Dexter1, Mr Robin Weston1, Mr Vishwanath Hanchanale1
1Liverpool University Hospitals, Liverpool, United Kingdom
Introduction: Single-port robot-assisted radical prostatectomy (SP-RARP) represents a recent evolution in minimally invasive prostate cancer surgery. The single-port platform aims to maintain the technical advantages of multi-port robotic systems including three-dimensional visualisation, tremor filtration, and wristed instrumentation, while potentially improving cosmesis and reducing post-operative pain. We report the first UK experience of SP-RARP from a high-volume tertiary referral centre.
Patients and Methods: Prospective data was collected on 54 consecutive patients undergoing SP-RARP over a 15-month period. Peri-operative, oncological, and early functional outcomes were analysed.
Results: Mean age was 61 years, mean BMI 27kg/m², and median ASA 2–3. Mean operative time was 127minutes (range 80–180) with mean estimated blood loss of 127mL (range 20–400). No intra-operative complications occurred. Bilateral nerve sparing was performed in 28 patients, unilateral in 23, and none in 3. Mean first post-operative numerical pain score was 0.9, and median length of stay was 1 day.
At 3 months, 68% were fully continent, with no patients reporting complete incontinence. Erectile function sufficient for intercourse, with phosphodiesterase-5 inhibitors ± vacuum device, was achieved in 72%. Final pathology demonstrated pT2b disease in 3 patients, pT2c in 23, pT3a in 23, pT3b in 1. Positive surgical margin >3mm was observed in one patient.
Conclusions: This represents the first UK case series of SP-RARP. Early outcomes demonstrate the procedure to be feasible and safe, with operative, oncological, and functional results comparable to published international SP-RARP data. Further comparative studies against multi-port RARP are warranted to define relative benefits of the single-port platform.
P15-9 10-year oncological outcomes following focal HIFU and cryotherapy for treatment of localised prostate cancer in the United Kingdom: an analysis of the prospective HEAT and ICE registries
Mr Alexander Light1, Dr Max Peters2, Dr Archana Gopalakrishnan1, Mr Nikhil Mayor1, Mr Samuel Morris1, Ms Emma Cullen1, Professor Hashim U. Ahmed1, Mr Taimur T. Shah1, HEAT Users Group, ICE Users Group
1Imperial Prostate, Imperial College London, London, United Kingdom, 2Radiotherapiegroep, Deventer, The Netherlands
Introduction: Focal HIFU and cryotherapy are increasingly used to treat localised prostate cancer, with previous outcome data reported up to 7 years post-treatment. Here we report 10-year cancer control outcomes.
Patients and Methods: Patients were included who had non-metastatic, previously-untreated prostate cancer and underwent focal HIFU or cryotherapy with ⩾6m follow-up within the HEAT and ICE prospective registries. The focal intervention included up to 2 focal ablative sessions. The primary outcome was cancer-specific mortality. Secondary outcomes were all-cause mortality, metastasis, local retreatment (third ablation or radical treatment), radical treatment, and ADT use. Cumulative incidences were measured 10 years post-treatment using a competing-risks approach.
Results: 3471 patients (HIFU: n=2891; cryotherapy: n=580) were included from 14 UK centres (2004-2024). 48.2%, 22.7%, and 24.8% had EAU intermediate-favourable-, intermediate-unfavourable-, and high-risk disease, respectively. 10-year cumulative cancer-specific mortality and all-cause mortality was 0.1% (95%CI 0-0.5%) and 11.6% (95%CI 8.5-14.6%), respectively (Fig.1). The 10-year cumulative incidence of metastasis was 3.2% (95%CI 2.0-4.8%). The 10-year cumulative incidence of local retreatment and radical treatment was 32.1% (95%CI 28.6-35.6%) and 30.1% (95%CI 26.7-33.5%), respectively, on an intention-to-treat basis. When patients who underwent radical treatment despite having localised intermediate-risk recurrences eligible for redo focal therapy were censored (per protocol analysis), these incidences were 11.1% (95%CI 8.8-13.7%) and 8.9% (95%CI 6.9-11.2%), respectively. The 10-year cumulative incidence of ADT use was 13.6% (95%CI 10.7-16.8%).
Conclusions: In this large multicentre cohort, focal HIFU and cryotherapy had excellent long-term cancer control. Our data support focal therapy as a first-line treatment for non-metastatic clinically-significant cancer.
P15-10 Pre-radiotherapy UroLift for prostate cancer: early outcomes from a multicentre randomised controlled trial
Miss Kathie Wong1, Professor Mieke van Hemelrijck2,3, Mr Jai Seth4, Dr Netty Kinsella5, Mr Toby Page6, Mr Declan Cahill5, Mr Ananda Dhanasekaran7, Mr John Withington8, Dr Vincent Khoo5, Professor Nicholas James5,9, Professor David Nicol5, Mr Simone Giona5, Dr Beth Russell2, Dr Charlotte Moss2, Mr Allayat Ullah7, Mr Masood Moghul5
1North Cumbria Integrated Care Trust / The Royal Marsden Hospital, Carlisle, United Kingdom, 2Kings College London, London, United Kingdom, 3Transforming Cancer Outcomes through Research London United Kingdom, London, United Kingdom, 4St George’s University Hospital NHS Foundation Trust, London, United Kingdom, 5The Royal Marsden NHS Foundation Trust, London, United Kingdom, 6Newcastle Upon Tyne NHS Foundation Trust, Newcastle, United Kingdom, 7Sandwell and West Birmingham NHS Trust, Birmingham, United Kingdom, 8University College London, London, United Kingdom, 9Institute of Cancer Research, London, United Kingdom
Introduction: Lower urinary tract symptoms (LUTS) are common in men undergoing prostate radiotherapy and are often exacerbated by benign prostatic hyperplasia (BPH). Surgical treatment after radiotherapy carries significant morbidity. UroLift® is a minimally invasive alternative to TURP in benign disease and may offer a strategy for pre-emptive LUTS management prior to radiotherapy, with the additional potential benefit of acting as surrogate fiducial markers. We report early operative outcomes from the UroLift arm of the COSTAR trial.
Methods: COSTAR (NCT05840549) is a prospective multicentre randomised controlled trial comparing UroLift with TURP performed before prostate radiotherapy. Eligible men had localised or locally advanced prostate cancer, prostate volume ⩽100 cc, moderate–severe LUTS (IPSS ⩾8), and obstructive flow (Qmax <12 mL/s). This interim analysis reports short-term operative and safety outcomes for patients undergoing UroLift. Procedural details, perioperative events, complications, and early functional outcomes were recorded prospectively.
Results: Fifteen men underwent UroLift prior to radiotherapy. Median age was 75 years, median prostate size 50 cc, and median baseline IPSS 20. A mean of 3.7 implants were placed per patient; 20% required urethral dilation and one-third required temporary post-operative catheterisation. All patients completed planned radiotherapy. No complications above Clavien–Dindo grade II were observed. At six weeks post-procedure, median IPSS improved to 6, quality-of-life score to 2, and Qmax to 11.6 mL/s.
Conclusions: Pre-radiotherapy UroLift appears safe and well tolerated, with early symptomatic improvement and no delay to radiotherapy delivery. Comparative functional and oncological outcomes versus TURP will be reported in future analyses.
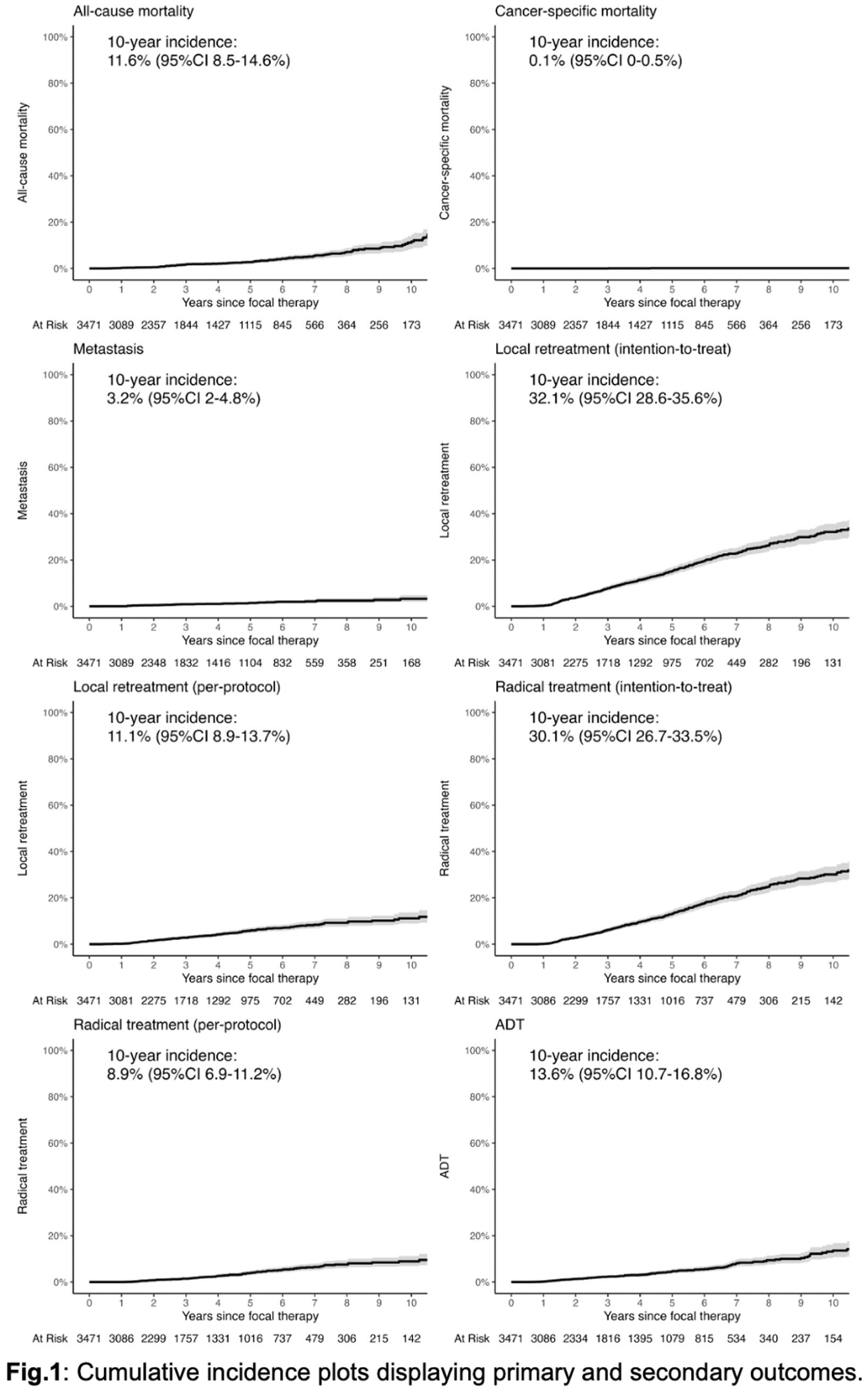
ePoster Session 16: Renal Cancer / Testis Cancer / Sarcoma, John Anderson, June 17, 2026, 08:00 - 09:00
P16-1 When Cancer Isn’t Cancer: Understanding Decision Regret After Partial Nephrectomy for Benign Renal Masses
Ms Sarika Nalagatla1, Dr Maria Yacoub1, Ms Aqua Asif2, Mr Samuel Davis1, Mr Manar Malki1, Mr Muddassar Hussain1, Mr Neil Barber1
1Frimley Renal Cancer Centre, Frimley Park Hospital, Frimley, United Kingdom, 2University College London, Division of Surgery and Interventional Science, London, United Kingdom
Introduction: Percutaneous renal mass biopsy (RMB) can clarify diagnosis for indeterminate small renal masses (SRMs), yet routine use before robotic-assisted laparoscopic partial nephrectomy (RALPN) remains variable. Approximately 30% of excised SRMs (<4cm) are benign. While RALPN preserves renal function and provides oncological control, it carries peri-operative risks. Decision regret is an important patient-reported outcome reflecting dissatisfaction with a healthcare decision. We assessed the prevalence and determinants of decision regret following RALPN for SRMs where final histology was benign and no pre-operative RMB was performed.
Materials and Methods: A mixed-methods study combined retrospective clinical data with prospective patient-reported outcomes. Patients undergoing RALPN for SRMs ⩽4cm (January 2010 - July 2025) without pre-operative RMB and with benign histology were included. A questionnaire incorporating the validated five-item Decision Regret Scale (DRS) was distributed by post, electronically or telephone. Significant regret was defined as DRS ⩾25. Free-text responses underwent thematic analysis.
Results: Of 1,480 RALPNs performed, 158 patients met inclusion criteria; 106 consented and 58 responded. Median age was 66 years and tumour size 30mm. No Clavien-Dindo ⩾III complications occurred. Most participants (79.3%) recalled being counselled the lesion could be benign. RMB was recalled as discussed by 55.2%, while 29.3% reported no discussion. Nearly all respondents (98.3%) felt adequately informed. Mean DRS was 13.6 (95% CI 10-17.1), with 27.6% reporting significant regret (DRS ⩾25).
Conclusions: Decision regret following RALPN for benign pathology was generally low. Higher information quality and explicit RMB discussion were associated with reduced regret, supporting structured shared decision-making and counselling.
P16-2 Impact of Adopting the 2019 Bosniak Classification on the Management of 70 Category IIF Renal Cysts: A retrospective, observational cohort study
Dr Ramy Elbaz1, Dr Shatha Alhilaly, Dr prateek Verma
1Scunthorpe General Hospital, Scunthorpe, United Kingdom
Objective: To assess the impact of the 2019 Bosniak classification (v2019) on the management, malignancy risk, and discharge rate of renal cysts that were previously classified as Bosniak IIF under the old classification.
Methods: 70 patients with Bosniak IIF cysts (old classification) under one-year follow-up were included. Baseline imaging was retrospectively reviewed and reclassified using v2019 criteria. Patient demographics including age and sex, indication for the initial CECT scan, radiological characteristics of the Bosniak IIF cyst(s) at diagnosis (size, location, number of septa, wall thickness, presence of calcification) were documented. Follow-up data including number and type of follow-up imaging studies performed (CECT, Ultrasound, or MRI), interval between the baseline scan and each follow-up study. Outcomes measured were reclassification distribution, evidence of progression/malignancy, discharge rate (downgraded to Bosniak I/II) and number of CT/MRI scans for each patient before reallocation with the new classification.
Results: Upon application of the v2019 criteria, the 70 original Bosniak IIF cysts were reclassified as follows: · Bosniak I/II (Discharge rate, no follow-up): 38 cysts (54.3%) · Bosniak IIF (Continue follow-up): 32 cysts (45.7%). On the next follow up of the 32 Bosniak IIF cyst patients after 6 months, 6 of them showed progression to Bosniak III and one patient progressed to Bosniak IV.
Conclusion: The adoption of the 2019 Bosniak classification led to a significant re-stratification of a cohort of old Bosniak IIF cysts. A significant proportion of patients (near half) could be safely discharged from further follow-up reducing patient anxiety, radiation exposure and healthcare costs.
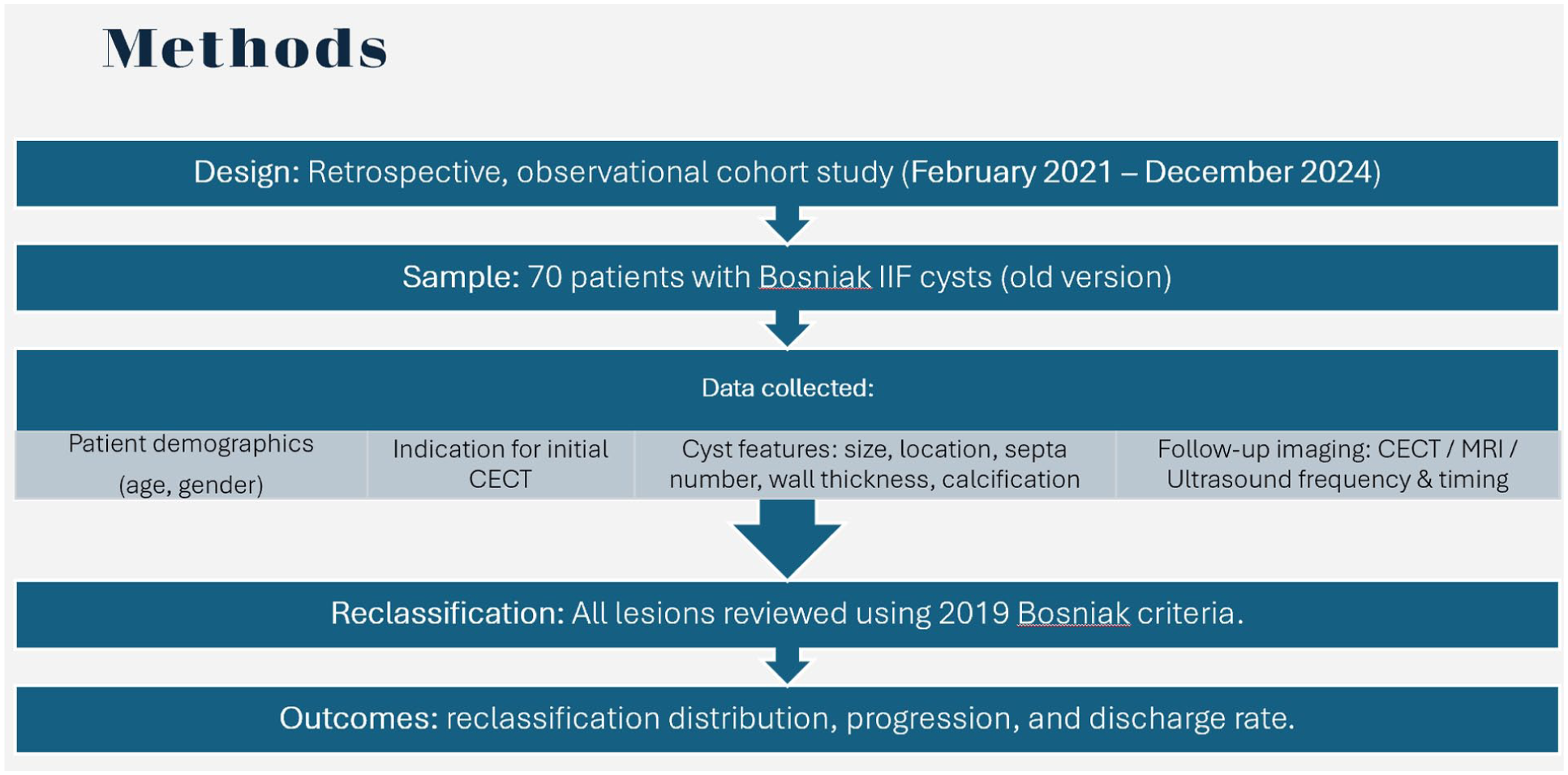
P16-3 Early Outcomes of Single-Port Robotic Renal Surgery: The First UK and European Experience from a High-Volume Centre
Miss Beatrice Ehrnrooth1, Dr Cynthia O’Sullivan2, Mr Sagar Kanabar2, Mr Rajesh Nair2, Professor Benjamin Challacombe2
1Kings College London, London, United Kingdom, 2Guys and St Thomas’ NHS Foundation, London, United Kingdom
Introduction: Single-port robotic platforms represent a recent evolution in minimally invasive renal surgery, with potential advantages in surgical morbidity and recovery. In April 2024, our centre became the first in the UK and Europe to introduce single-port robotic renal surgery. We report early peri-operative outcomes across a range of renal procedures.
Patients and Methods: A retrospective review was performed of the first 42 consecutive single-port robotic renal procedures undertaken by two experienced robotic surgeons using the da Vinci single-port platform since April 2024. Procedures included radical nephrectomy(n=6), nephroureterectomy(n=5), partial nephrectomy(RAPN; n=17) and pyeloplasty(n=14). Collected variables included patient demographics, console time, estimated blood loss (EBL), length of stay (LOS), warm ischaemic time for RAPN, and margin status.
Results: Forty-two consecutive procedures were performed across extirpative, nephron-sparing, and reconstructive indications (Table 1). Peri-operative outcomes were consistent across procedure types, with low blood loss and short lengths of stay. Surgical margins were negative in all oncological cases, with one planned positive margin following angiomyolipoma excision. Mean warm ischaemic time for RAPN was acceptable.
Complications were minimal, with no Clavien-Dindo greater>II events. The majority (88%) of procedures were performed using a low anterior extraperitoneal approach.
Conclusions: This initial UK and European experience demonstrates that single-port robotic renal surgery is feasible and efficient, with short hospital length of stay and acceptable early oncological outcomes. The platform appears versatile across a wide spectrum of renal surgery and may facilitate broader minimally invasive surgical applications, with potential to support day-case surgery and patients with prior major abdominal surgery.
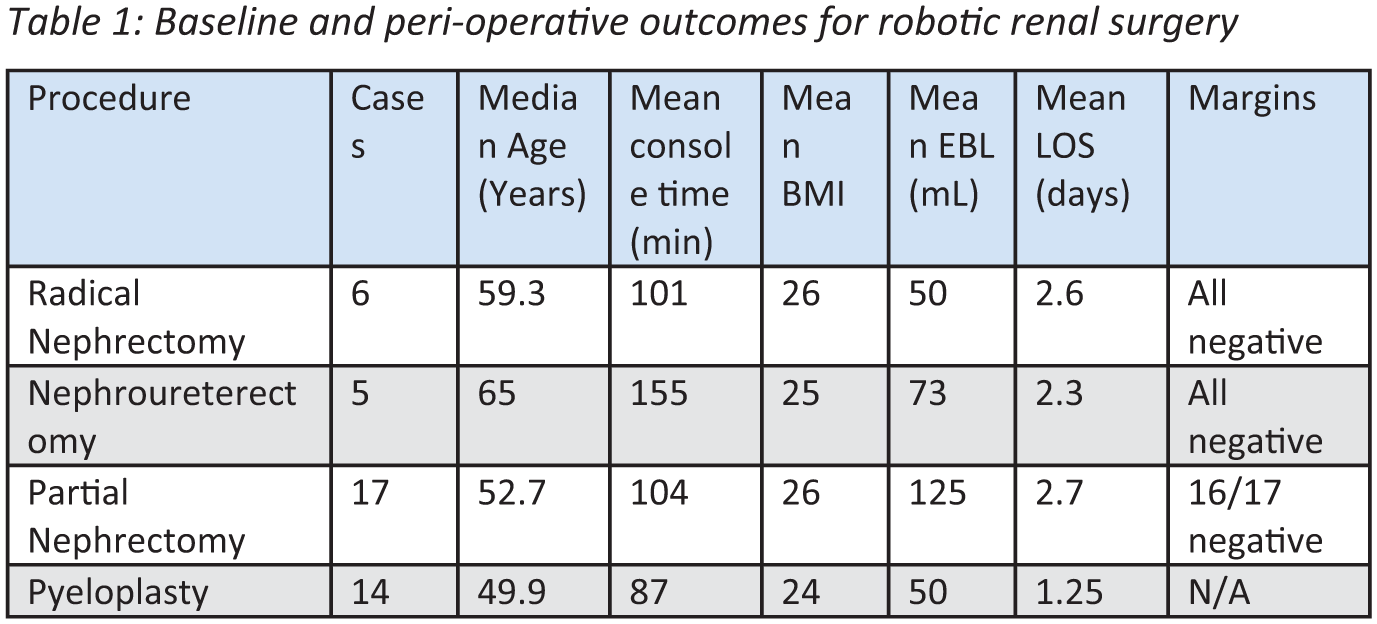
P16-4 Surveillance of Bosniak IIF Renal Cysts in the UK: A Multicentre Mapping Study of Real-World Practice
Miss Amelia Simenacz1, Miss Pinky Kotecha1, Mr Giuseppe Basile1, Mr Eduard Roussel1, Mr Brendan Berry1, Mr Prasad Patki1, Mr Abhishek Reekhaye1, Professor Faiz Mumtaz1, Mr Ravi Barod1, Professor Axel Bex1, Ms Sarika Nalagatla1
1Royal Free Hospital, London, United Kingdom
Introduction: Bosniak IIF renal cysts carry an estimated malignancy risk of 5-10%. There are currently no established UK guidelines defining optimal imaging modality, surveillance intervals, or follow-up duration. Consequently, surveillance remains heterogeneous, with many UK Trusts adopting the 2019 Canadian Urological Association (CUA) recommendations. This study assessed variation in surveillance practice for Bosniak IIF renal cysts across the UK.
Materials and Methods: An online questionnaire was disseminated to consultant renal cancer leads across UK renal cancer centres, purposively sampled to capture clinicians with established specialist involvement in kidney cancer management. Data collected included surveillance imaging modality, frequency and duration of follow-up, use of multidisciplinary team (MDT) discussion, adherence to CUA guidance, and challenges encountered during surveillance.
Results: Responses were obtained from 31/42 trusts. Initial diagnostic imaging was consistent, with all centres using triple-phase CT. However, substantial heterogeneity was observed in surveillance modality, follow-up intervals and overall duration. Initial follow-up most commonly occurred at six months (65%; range 3-12 months), with 71% transitioning to annual imaging thereafter. Patients underwent a mean of three CT scans during follow-up, while CEUS was utilised by only six trusts. Five-year surveillance was reported by 55%. Challenges included inter-observer radiological variability, lack of UK guidance, and uncertainty regarding optimal surveillance strategies.
Conclusions: Variation in practice likely reflects absent national standardisation and may contribute to inconsistent care, increased costs and avoidable radiation exposure. Further research is required to inform UK-specific guidelines and identify higher-risk Bosniak IIF features warranting closer surveillance or earlier intervention in selected patients.
P16-5 Room for Improvement: Hypogonadism and testosterone replacement therapy in testicular cancer survivors
Ms Neve Macdonald1, Mr Raphael Birch1, Ms Alice Cotton2, Dr Ching-Hao Chen2, Prof Tet Yap2
1Kings College London, London, United Kingdom, 2Guy’s and St. Thomas’s NHS Foundation Trust, Department of Urology, London, United Kingdom
Introduction: Despite five-year survival being 95%, testicular cancer survivors (TSCs) often have reduced QoL due to hypogonadism. After bilateral orchidectomy and initiating testosterone replacement therapy (TRT), many remain symptomatic and unilateral cases are frequently unscreened for hypogonadism. This systematic review assesses the role of hypogonadism in TCS and analyses the effect of TRT in improving symptoms and QoL.
Methods: MEDLINE, EMBASE, Global Health and Ovid Journals were searched using PRISMA guidelines for RCTs, observational and case-controlled studies. Patients with hypogonadism and previous orchidectomies due to testicular cancer were included. Patient characteristics, study location, type of surgery and TRT, hypogonadal definitions, assessment tools and outcomes were extracted.
Results: Of 1,676 screened studies, 34 were reviewed for eligibility and 5 (1999-2018) were included, covering 48 bilateral orchidectomy patients and 1366 unilateral orchidectomy patients (25-75). Hypogonadism was prevalent in 19.5% of unilateral orchidectomy patients. Table 1 shows that TRT improved QoL, psychological impact and sexual function in TCSs, whilst observational results were mixed. Mixed results were seen in fatigue and bone mineral density was observed to worsen in hypogonadal patients. No testosterone-related adverse effects were reported.
Conclusions: This suggests TRT should be implemented for TCSs with hypogonadism as, even when unexpected, TRT had positive impacts in TCSs compared to the observational results. More robust studies are needed to rule out survivor bias. Hypogonadism, even in unilateral orchidectomy, is an issue and routine monitoring is needed. There is potential for long-term improvement in symptom burden and QoL in these patients through TRT.
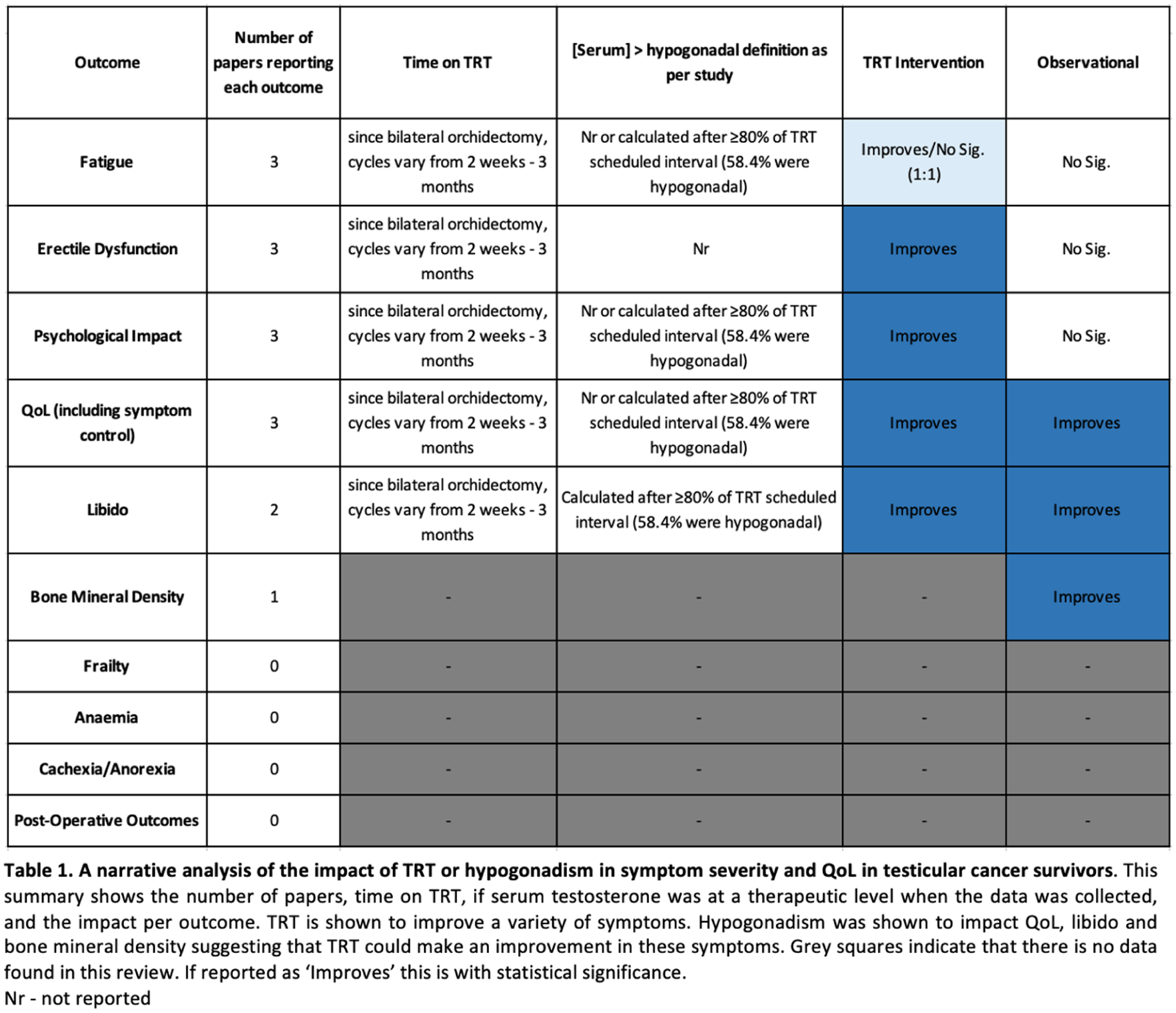
P16-6 Impact of three-dimensional reconstruction on ischemia times and operative times in robot-assisted partial nephrectomy
Dr Kuldeep Sardana1, Dr Deerush Kannan Sakthivel1, Dr Madhav Tiwari1, DR Sandeep Bafna1, Dr Narasimhan Ragavan1
1Apollo Hospitals, CHENNAI, India
Introduction: Partial nephrectomy (PN) is the standard treatment for T1a renal masses, increasingly applied to T1b tumours due to advancements in robotic surgery and imaging. While CT urograms are standard, three-dimensional (3D) reconstruction is gaining traction for complex tumours to enhance preoperative planning. This study compares the impact of 3D reconstruction on operative times and ischemia times during robot-assisted PN.
Methods: A prospective, non-randomized study was conducted on 112 patients who underwent robot-assisted PN between January 2020 and October 2022. Patients were divided into two groups: Group A (n=56) with the aid of 3D reconstruction for complex tumours and Group B (n=56) without 3D reconstruction. Operative times and ischemia times were analysed, along with other outcomes such as margin positivity and postoperative complications.
Results: Despite higher tumour complexity in Group A, mean operative times (190.1 [standard deviation, SD 38.5] min vs. 189.3 [SD 42.6] min) and mean ischemia times (20.4 [SD 5.6] min vs. 20.3 [SD 5.3] min) were comparable between Group A and Group B. Margin positivity and complications were also similar, suggesting that 3D reconstruction aids in efficient surgery even for complex cases.
Conclusions: 3D reconstruction enhances understanding of complex renal tumours, maintaining operative efficiency comparable to less complex cases. Further randomized studies are needed to confirm these findings.
P16-7 Beyond RENAL: Mayo Adhesive Probability (MAP) Score and Operative Complexity in Robotic Partial Nephrectomy (RPN)
Mr Prasenjit Bhowmik1, Mr Shankar Chandrasekharan1
1Heartlands Hospital, University Hospitals Birmingham NHS Foundation Trust, Birmingham, United Kingdom
Introduction: Perinephric fat adhesions can increase the technical difficulty of robotic partial nephrectomy (RPN) for small renal masses. The Mayo Adhesive Probability (MAP) score is a preoperative imaging-based tool used to predict the presence of adherent perinephric fat (APF). This study evaluated whether a high MAP score is associated with longer dissection time and greater estimated blood loss (EBL) during RPN.
Materials and Methods: We conducted a retrospective study of 45 patients who underwent RPN at a tertiary referral centre from January 2025 to December 2025. Preoperative CT scans were used to calculate MAP scores. Patients were stratified into low (MAP 0–2) and high (MAP 3–5) score groups. Primary outcomes included hilar and perinephric dissection time and EBL. Secondary outcomes were operative time, warm ischemia time, and perioperative complications. Statistical comparisons were performed using appropriate univariate analyses.
Results: Preliminary analysis demonstrates that patients with high MAP scores had significantly longer dissection times compared to those with low MAP scores. EBL was also higher in the high MAP group. Overall operative time was increased in patients with higher MAP scores, while warm ischemia time and complication rates were not significantly different between groups.
Conclusion: A high MAP score predicts greater surgical complexity during RPN, with longer dissection times and increased blood loss. Incorporating MAP scoring into preoperative planning enhances risk stratification and operative preparedness by assessing APF not captured by tumour-based scoring systems, while also facilitating more efficient theatre list utilization in the era of rising obesity and widespread RPN adoption.
P16-8 Think Sarcoma! The unusual scrotal lump and the importance of early referral. Retrospective cohort study from a supra-regional tertiary centre
Miss Parthvi Vanalia1, Mr Sami Mustafa, Mr Thomas Lee, Mr Aziz Gulamhusein
1Christie’s Nhs Foundation Trust, Manchester, United Kingdom
Introduction: Soft tissue sarcoma (STS) is a rare and aggressive connective tissue malignancy, representing 1% of adult malignancies. Inguino-scrotal sarcomas comprise 1% of all STS. Management involves radical excision with an emphasis on achieving wide margins due to the high risk of local recurrence. We present a 5-year case series from a large supra-regional sarcoma centre with expertise in retroperitoneal and inguino-scrotal STS.
Patients and Methods: A retrospective review was performed of all patients undergoing hemiscrotectomy for confirmed or suspected inguino-scrotal STS between January 2020 and December 2025. Demographic data, operative details, histology, multidisciplinary involvement, adjuvant therapy, recurrence, and survival outcomes were reviewed.
Results: Twenty patients were included, with a median age of 66.5 years. The mean length of hospital stay was four days. Histopathology demonstrated predominantly well-differentiated or de-differentiated liposarcoma, with one case each of rhabdomyosarcoma and angiofibroma. Three patients required multidisciplinary surgical input at the index operation involving oncoplastic and colorectal teams within the sarcoma MDT. Eight patients had undergone previous incomplete scrotal surgery at referring centres and subsequently required extensive re-resection at our institution. Local recurrence occurred in four patients. One patient developed pulmonary metastases and died from sarcoma-related disease. The remaining three required further surgery with multidisciplinary involvement and had all undergone prior surgery before referral. Two patients received adjuvant therapy.
Conclusion: Management of atypical inguino-scrotal masses should take place at specialist centres. Prior incomplete or non-oncological surgery adversely impacts oncological outcomes, and early referral for specialist assessment is recommended when diagnostic uncertainty exists.
P16-9 Systematic Review of Bacillus Calmette-Guérin Therapy in the Management of Upper Tract Urothelial Carcinoma in Situ
Mr Youssef Garras1, Ms Daniah AlSaadi2, Dr Ned Kinnear3,4, Mr Derek Hennessey1,2
1University College Cork, Cork, Ireland, 2Mercy University Hospital, Cork, Ireland, 3Lyell McEwin Hospital, Adelaide, Australia, 4University of Adelaide, Australia
Upper tract urothelial carcinoma in situ (UT-CIS) is a high-grade non-muscle invasive cancer traditionally managed by radical nephroureterectomy (RNU). Topical Bacillus Calmette–Guérin (BCG) is offered as a kidney-sparing option for UT-CIS, yet contemporary evidence remains heterogeneous. We performed a systematic review to evaluate oncological outcomes focusing on complete response (CR), recurrence, progression, salvage nephroureterectomy (RNU), and renal unit preservation.
A systematic search of PubMed, Embase, Web of Science, the Cochrane Library, and grey literature (2000–2025) was conducted in September 2025. Screening followed PRISMA methodology and PICO-based eligibility criteria. Data extraction and risk of bias assessment (ROBINS-I) were performed. Outcomes were analysed per renal unit and synthesised descriptively due to methodological heterogeneity.
Fourteen studies (297 renal units) met inclusion criteria. CR was reported in 13 studies, with a pooled CR rate of approximately 80%. The pooled recurrence rate was 29%, and progression occurred in 19% of renal units. Salvage RNU was required in 14% of cases. Overall, kidney preservation was achieved in 85% of treated renal units. Variation existed in denominators used for recurrence and progression, and reporting of adverse events was inconsistent across studies.
Topical BCG achieves high CR and kidney preservation rates in selected patients with UT-CIS; however, recurrence and progression remain clinically significant, and approximately one in seven renal units ultimately require RNU. The evidence base is limited by small sample sizes, heterogeneous outcome reporting, and non-randomised study designs. Standardised reporting and prospective studies are needed to better define the role of BCG in upper tract CIS management.
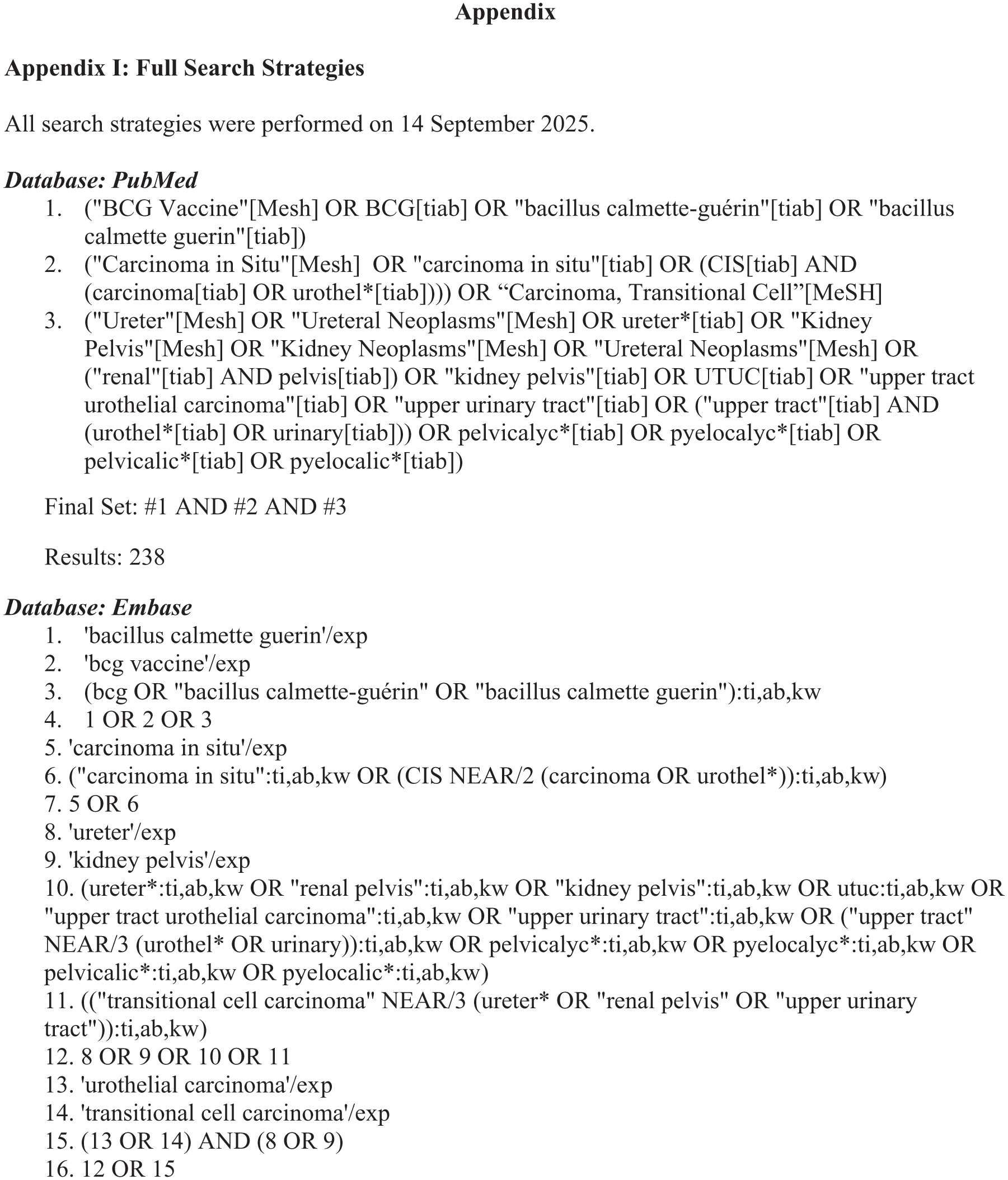
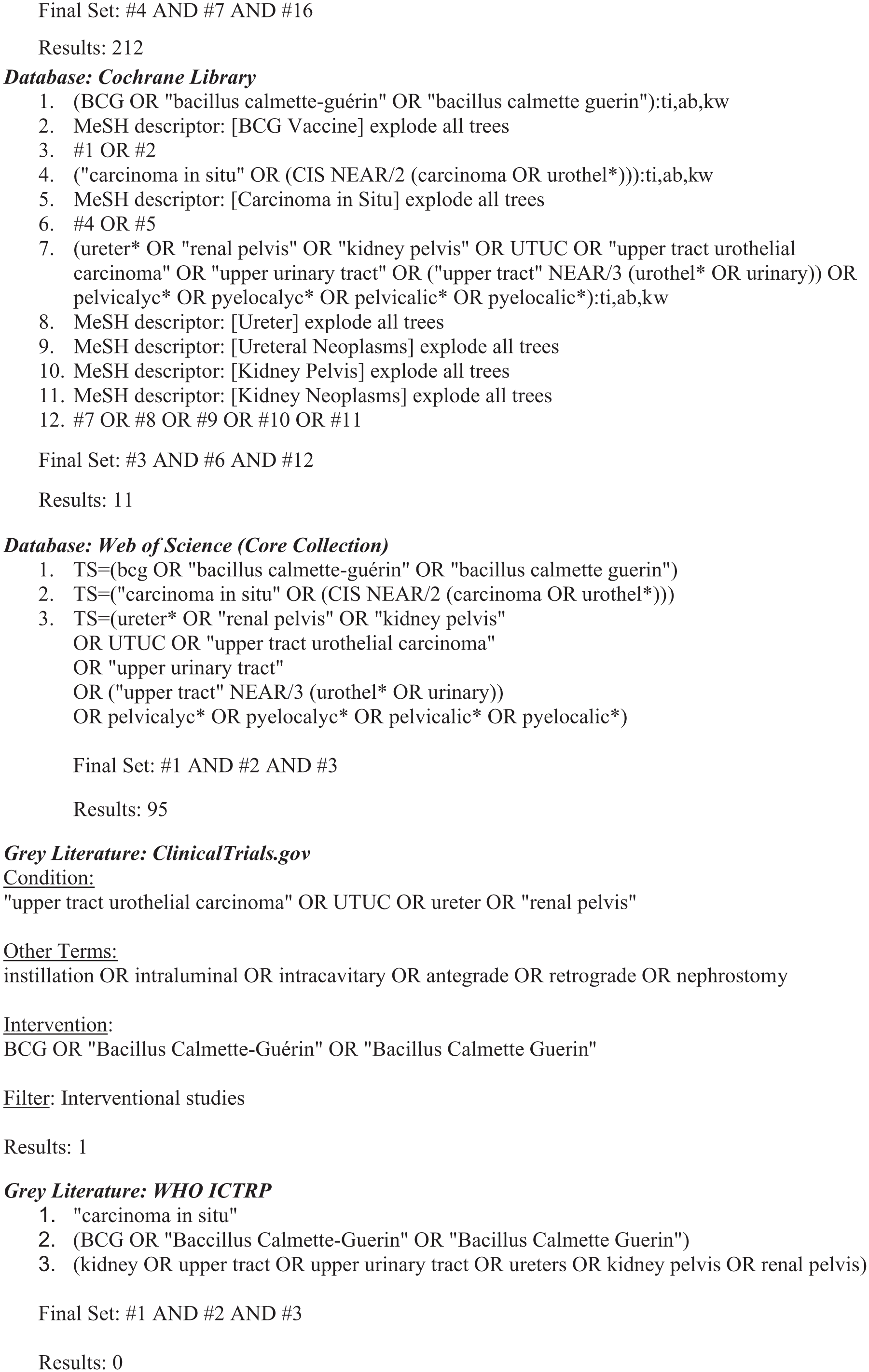
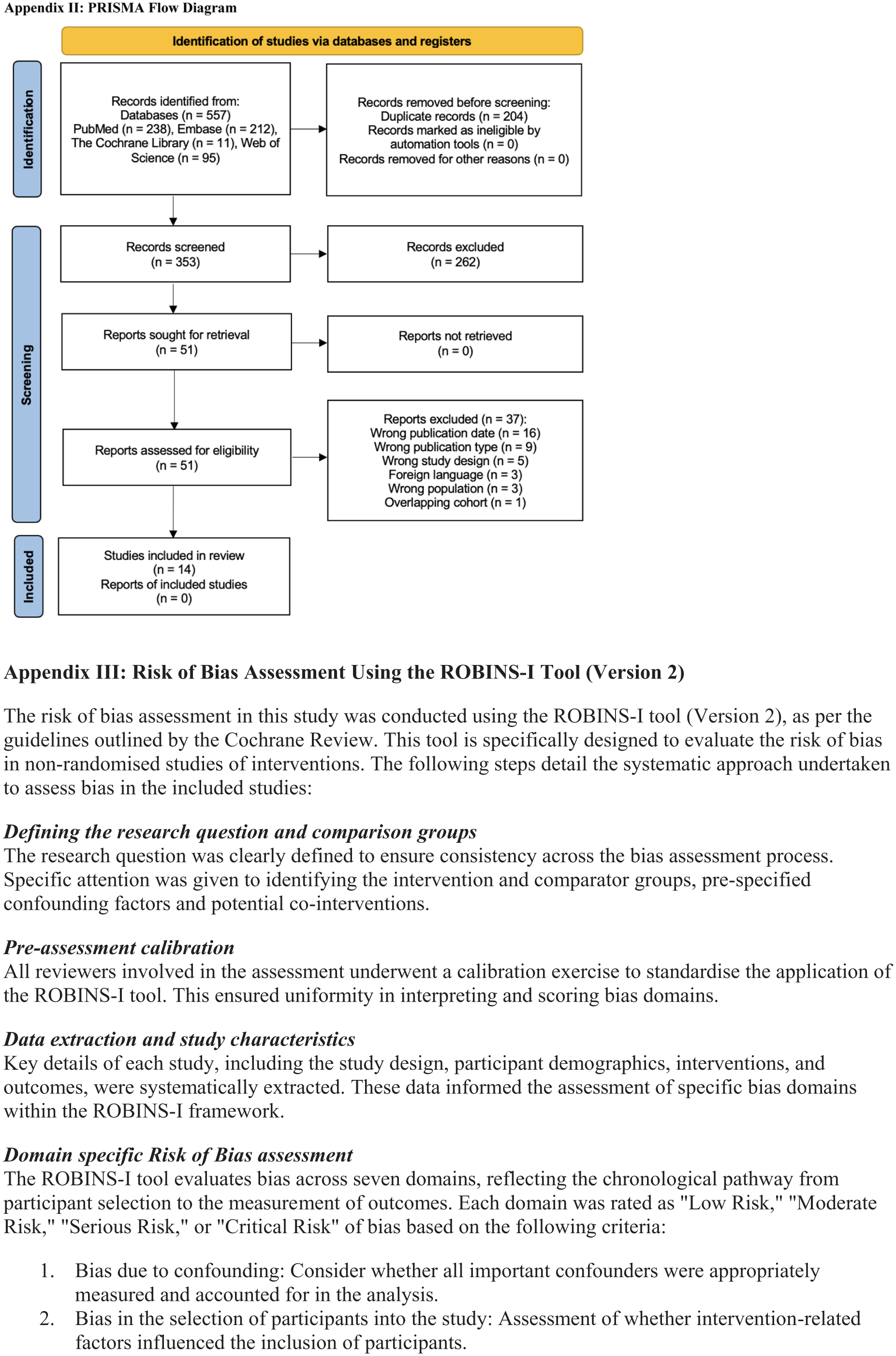
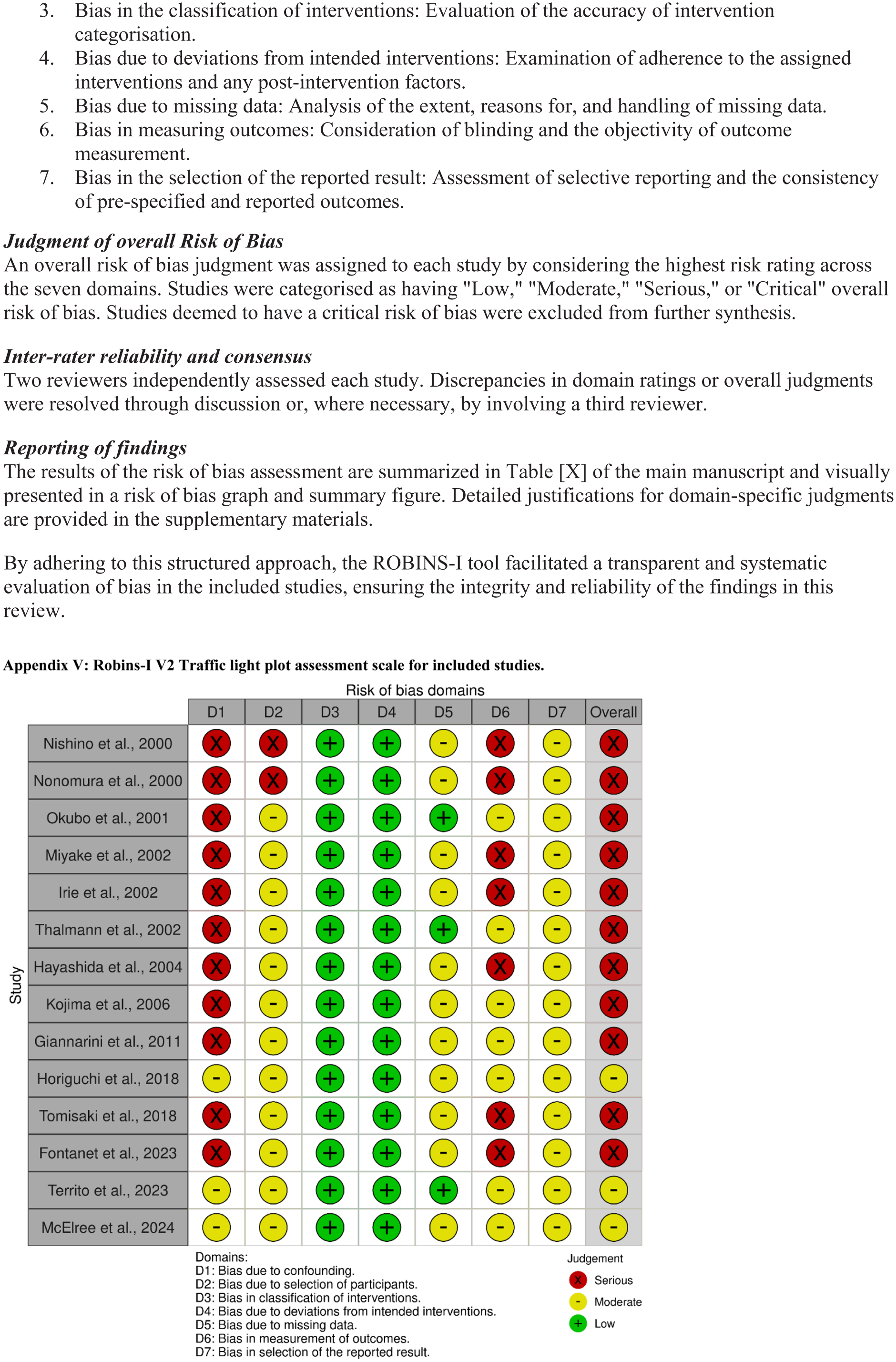
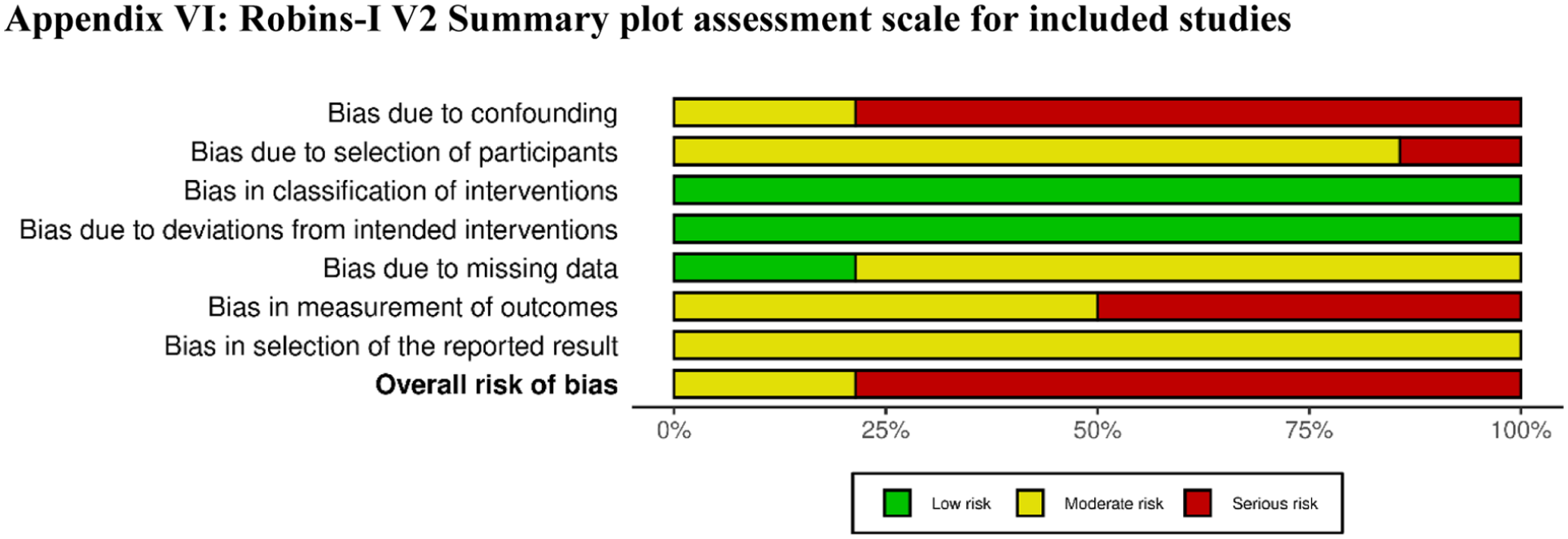
P16-10 Testicular Micro-Kalsi Score (TK Rad Score): A Novel Scoring System for Risk Stratification of Testicular Microlithiasis to Optimise Surveillance in Adults—A Retrospective Single-Centre Analysis
Mr Faiz Shaikh1, Dr Shiney James1, Mr Ma’en Hamawi1, Dr David Maudgil1, Dr Waleed Al-Obaydi1, Mr Harbinder Sharma1, Mr Jas Kalsi1
1Wexham Park Hospital, Slough, United Kingdom
Introduction: Testicular microlithiasis (TML) has no standardised, evidence-based surveillance protocol, leading to variable follow-up and potentially unnecessary imaging. This study proposes a novel risk-stratification scoring system (TK‑RAD) that integrates key clinical and radiological risk factors for testicular cancer to support consistent, tailored surveillance and optimise clinical decision-making.
Materials & Methods: A composite risk score (TK‑RAD) was derived from literature review and expert consensus incorporating clinical and radiological risk factors including testicular atrophy (volume <12 ml), degree of calcification (<5 microliths, 5-10 microliths, >10/’snowstorm’), history of cryptorchidism, infertility, and personal/family history of testicular cancer. The score was applied retrospectively to a cohort of patients with TML to stratify surveillance intensity into low, intermediate and high-risk pathways.
Results: In a cohort of 362 patients with testicular microlithiasis, application of the composite risk score stratified 272 (75.1%) as low risk, 82 (22.7%) as intermediate risk, and 8 (2.2%) as high risk. Based on this stratification, recommended follow-up was regular self-examination for low-risk patients, annual scrotal ultrasound for 3 years for intermediate-risk patients, and annual scrotal ultrasound for 5 years for high-risk patients.
Conclusions: The TK-RAD score offers a structured and evidence-based approach to risk stratification in patients with testicular microlithiasis to guide tailored surveillance. Adoption of this system has the potential to standardise management, reduce unnecessary interventions and optimise early detection in high-risk individuals. Further validation in clinical cohorts is warranted to confirm its predictive utility and impact on patient outcomes.
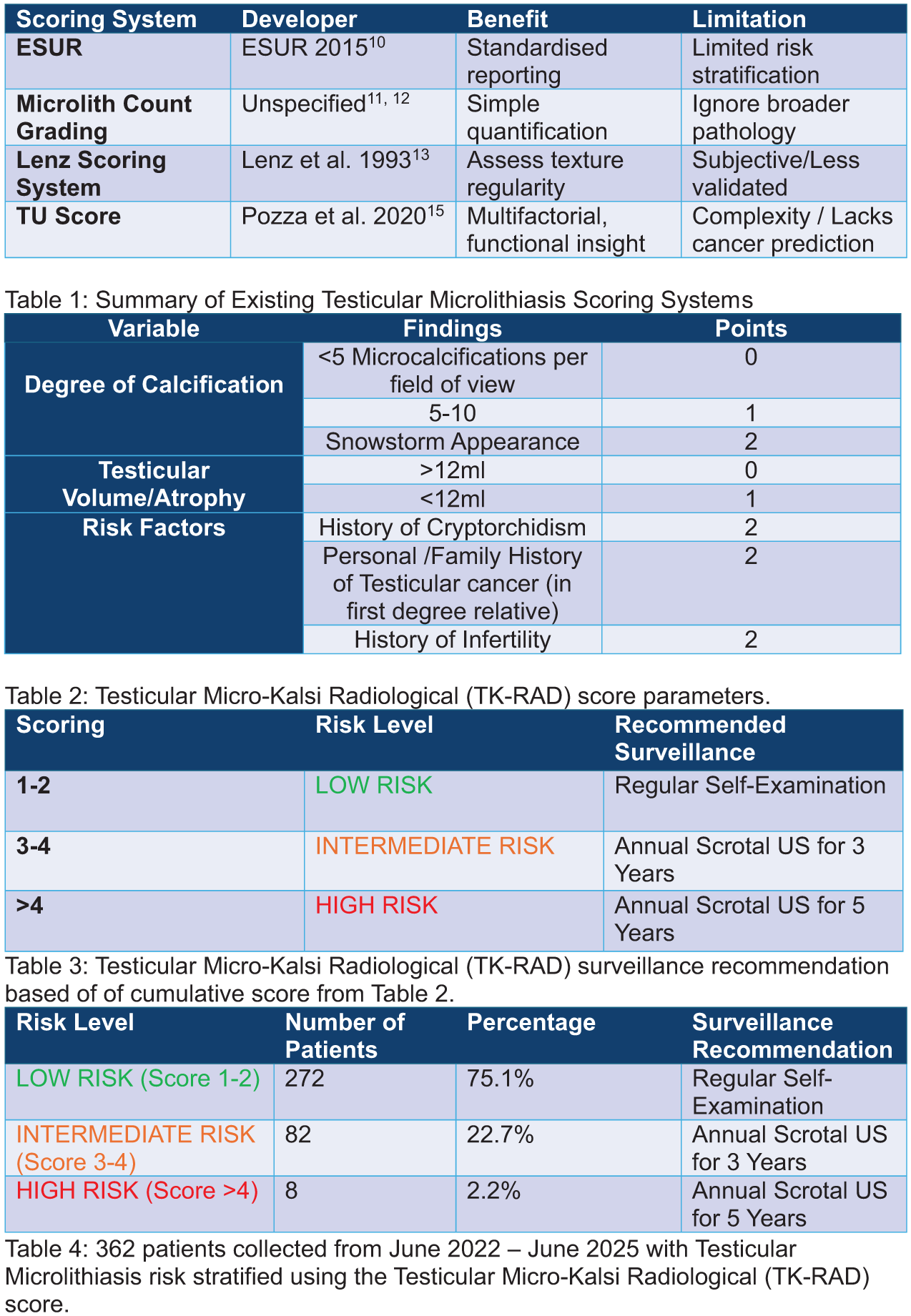
ePoster Session 17: General - Uro-technology, AI & Urology Apps, Paddy O’Reilly, June 17, 2026, 08:00 - 09:00
P17-1 Development and validation of a deep learning tool for automated reading of fluorescence confocal microscopy images in radical prostatectomy
Mr Nikhil Mayor1, Mr Lixiang Fang1, Dr Anna Silvanto2, Dr Aiman Haider2, Dr Ricardo Almeida-Magana2, Professor Greg Shaw2, Professor Hashim Ahmed1, Dr Francesca Fiorentino3, Dr Stamatia Giannarou1, Mr Mathias Winkler1, et al.
1Imperial College London, London, United Kingdom, 2University College London, London, United Kingdom, 3University of Leeds, Leeds, United Kingdom
Introduction: Fluorescence confocal microscopy (FCM) is a more feasible alternative to NeuroSAFE for intraoperative margin assessment in radical prostatectomy (RP). However, FCM images still require pathologist interpretation. We aimed to develop and validate an AI model to distinguish benign from malignant tissue on FCM images in RP.
Methods: FCM images from 153 patients were obtained from the IP8-FLUORESCE study using the Histolog® Scanner. Pathologist-annotated regions containing cancer and benign tissue were used to create a dataset of 275 images (tumour 13%, benign 87%). A modified deep learning architecture was developed using the established ResNet50 convolutional neural network. We applied modified focal loss, balanced data sampling, and classifier head with dropout. The model was trained on 80% of the data and tested on the remaining 20%. External validation was performed using 46 images (23 tumour, 23 benign) from an independent dataset. Gradient-weighted class activation maps (Grad-CAMs) were applied to highlight areas the model identified as suspicious.
Results: On internal testing, our model achieved 87.5% (47.4-99.7) sensitivity, 97.9% (89.2-100.0) specificity (AUC: 0.98; 93.1-100.0) for cancer detection. The model performed well on external validation: 91.3% (73.2-97.6) sensitivity, 73.9% (53.5-87.5) specificity, AUC 0.83 (0.74-91.4). Grad-CAM heatmaps accurately localised malignant glands, highlighting features consistent with pathology assessment.
Conclusion: Our deep learning model demonstrated high accuracy for classifying RP surgical margin status with interpretable visual outputs. This approach has the potential to streamline the use of FCM for intraoperative margin assessment and limit reliance on pathologists. We were limited by the small number of positive cases.
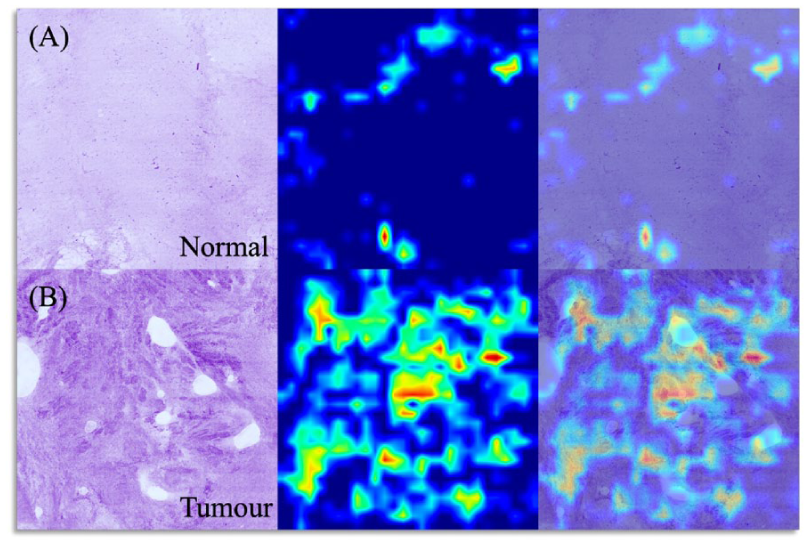
P17-2 Comparative validation of AI-assisted MRI screening pathways in the IP1-PROSTAGRAM study
Mr Nikhil Mayor1, Dr Antony Rix2, Dr Aarti Shah3, Ms Natalia Klimowska-Nassar1, Dr Henry Tam1, Dr Heminder Sokhi4, Mr Mathias Winkler1, Mr David Eldred-Evans1, Professor Anwar Padhani5, Professor Hashim Ahmed1, et al.
1Imperial College London, London, United Kingdom, 2Lucida Medical Ltd, Cambridge, United Kingdom, 3Hampshire Hospitals NHS Foundation Trust, Winchester, United Kingdom, 4Hillingdon Hospitals NHS Foundation Trust, London, United Kingdom, 5Paul Strickland Scanner Centre, Middlesex, United Kingdom
Introduction: AI decision support systems (AI-DSS) could standardise interpretation of screening MRI. We retrospectively validated the Lucida Pi AI-DSS on the IP1-PROSTAGRAM cohort.
Methods: 371 participants were included. Men underwent Prostagram™ MRI, ultrasound and PSA, with systematic biopsy for any positive test and additional targeted biopsy if positive imaging. 159 (42.9%) underwent biopsy, detecting 15 (4.0%) GG ⩾2 & 19 (5.1%) GG1 cancers. Alternative pathways were modelled and compared with the AI-DSS: (P1) MRI for all; (P2) MRI if PSA ⩾1.0; (P3) MRI if PSA ⩾3.0. Outcomes: biopsy recommendation, cancer detection, benign biopsy rate (GG0), and three utility metrics: selectivity (GG ⩾2/GG1), efficiency (GG ⩾2/[GG1+GG0]), and selective biopsy avoidance (GGx [no biopsy]/GG0).
Results: In P1, AI-DSS achieved similar GG ⩾2 yield (11/371, 3.0 %) to PI-RADS ⩾3 (3.5 %) and ⩾4 (3.0 %), with fewer biopsies (9.2% vs 16.7% and 9.7%), GG1 cases (1.1% vs 1.9% and 1.3%), and benign biopsies (5.1% vs 11.3% and 5.4%), improving utility metrics. In P2, AI-DSS maintained GG ⩾2 detection (11/371, 3.0%) relative to PI-RADS ⩾3 (3.0 %) and ⩾4 (2.7%), reducing biopsy rates compared with PI-RADS ⩾3 (8.4% vs 11.1%), with a modest increase compared with PI-RADS ⩾4 (7.0%), and lowest GG1 yield (0.5%). In P3, only 9% of men underwent MRI, yielding 6/371 (1.6%) GG ⩾2 cancers, missing half of all GG ⩾2 cases; here, AI-DSS offered no additional benefit.
Conclusion: On screening data, AI-DSS achieved equivalent or superior detection of significant PCa compared with MRI/PSA pathways whilst reducing biopsy and overdiagnosis.
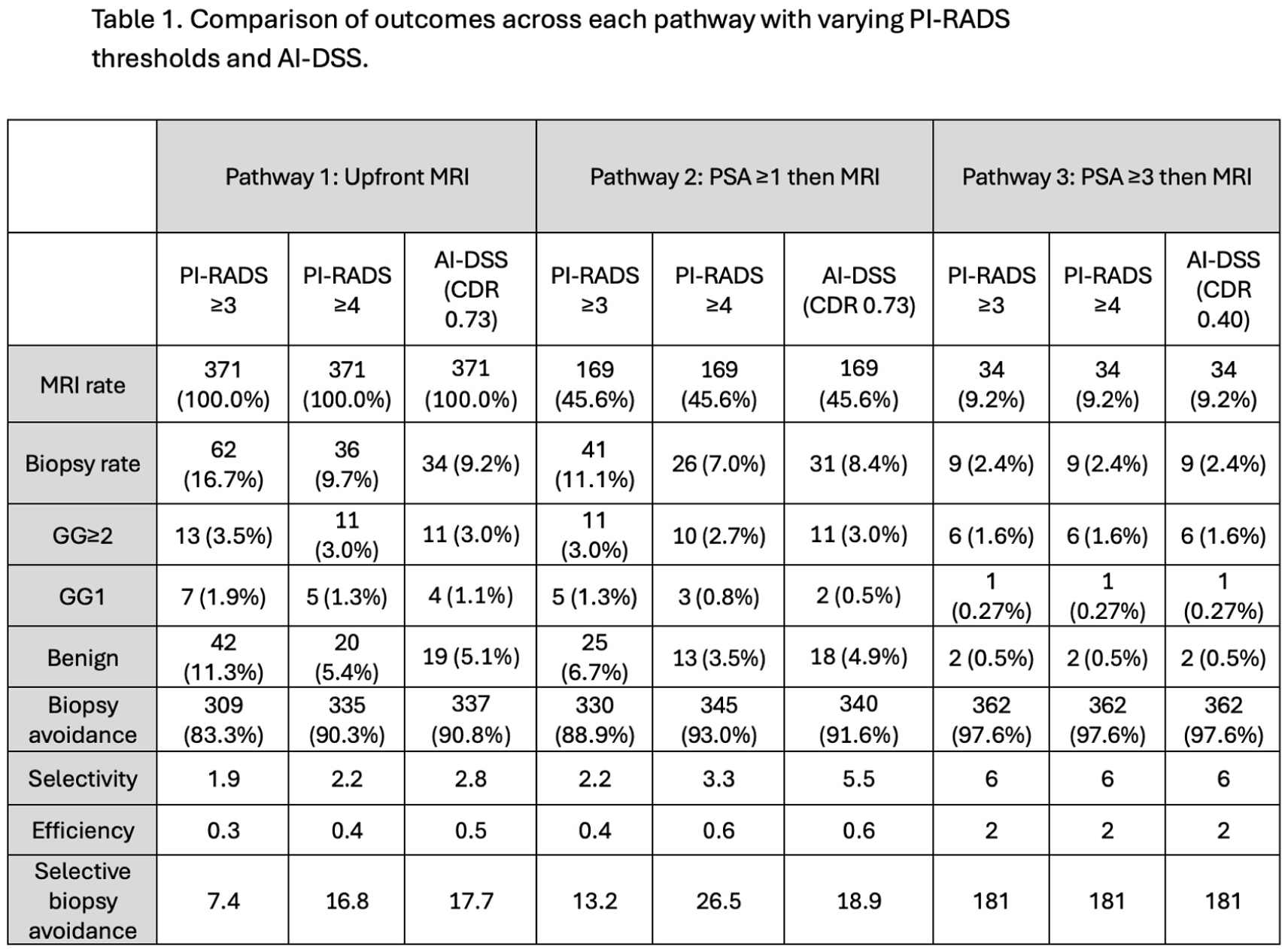
P17-3 Investigating the Use of Virtual Reality to Enhance the Consent Process and Provide Counselling for Patients Undergoing Shock Wave Lithotripsy
Mr Solomon Bracey1, Mr Dara Bamerni1, Ms Phoebe Reynolds1, Ms Loretta Tear1, Ms Tanya Davis1, Dr Maria Frascheri1, Dr Amelia Pietropaolo1, Professor Bhaskar Somani1
1Southampton General Hospital, Southampton, United Kingdom
2Surgassists, Cornwall, UK
Introduction: This research explores the use of VR as a tool to improve the consenting process for Shock Wave Lithotripsy (SWL). We investigated how patients experienced VR and its impact on their understanding, emotions and pain levels.
Patients and Methods: Patients attending clinic for their SWL treatment were prospectively recruited to experience a 3 minute long VR animation. This animation outlined the SWL procedure based on the British and European Urolithiasis guidelines and enabled visualisation of urinary anatomy. Participants then responded to questionnaires, giving insight into their levels of understanding, emotional status and pain.
Results: Two hundred participants fully completed all the questionnaires. VR use significantly improved participants’ understanding and confidence in explaining the SWL procedure, alongside significantly reducing nervousness. Participants reported improvements in all positive emotions and reductions in all negative emotions. VR was rated as significantly more accessible and helpful than current resources, with 76% of participants reporting strong preference for its inclusion in future treatment. These findings were generally consistent across all age groups. Compared with previous SWL research, the mean post procedural pain score (1.86) was lower, suggesting that VR may help to reduce pain.
Conclusions: VR shows great potential to enhance the consenting process for SWL. VR interventions can improve patient understanding, strengthening informed consent. They can also enhance the consenting experience through reducing negative emotions like anxiety while improving positive emotions like satisfaction. Due to, altered emotional status and improved understanding, VR may also have a role in reducing pain.
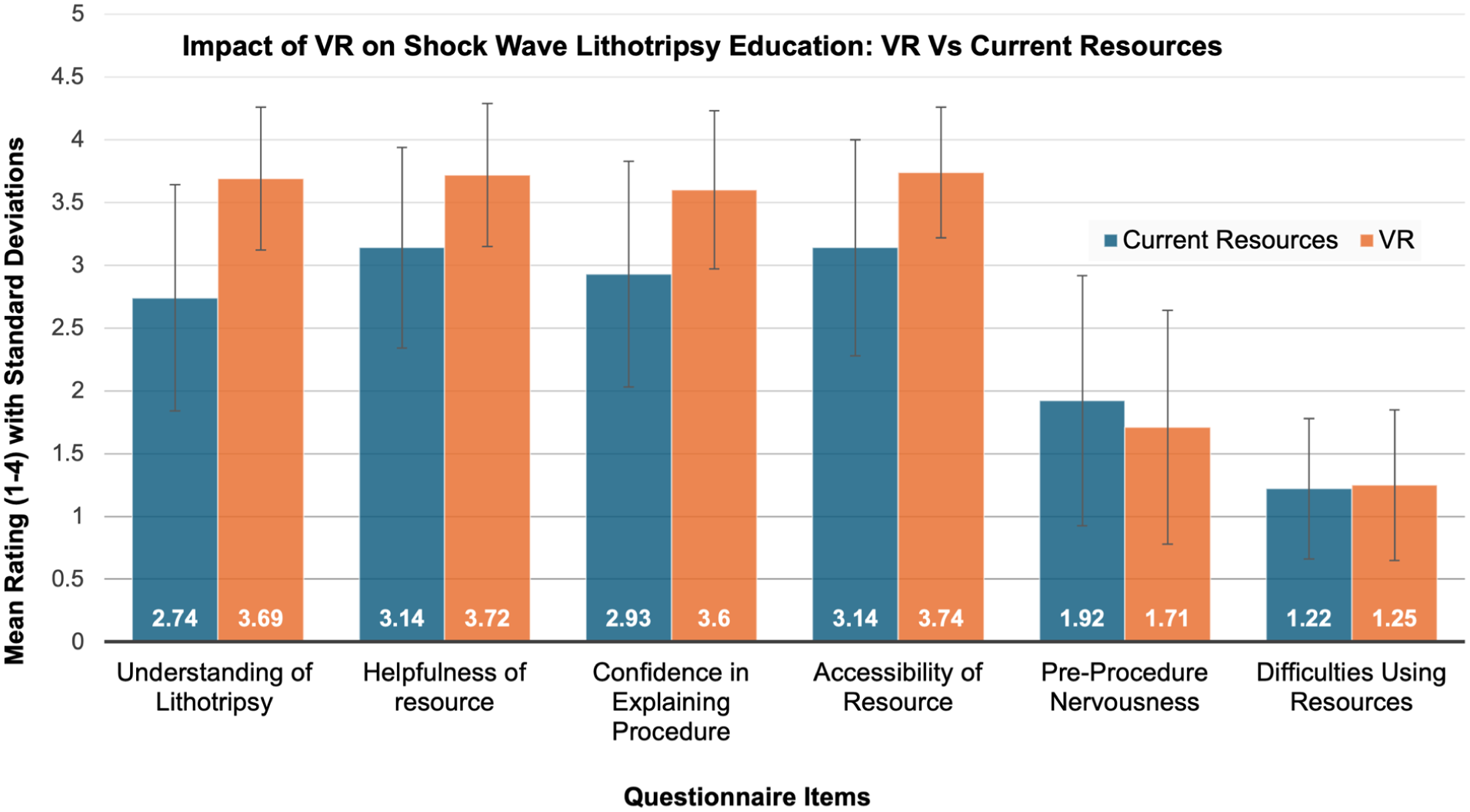
P17-4 Shifting GEARS in the Operating Room: Using Multiple Surgical Robots in Clinical Practice
Dr Noor Haddad1, Mr Mehrshad Sultani Tehrani1, Professor Ben Challacombe1
1Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom
Introduction: As multiple robotic platforms are introduced across centres, concerns persist regarding whether surgeons can safely transition between different systems during routine practice. We collated the evidence for cross-platform skill transfer and propose a structured proficiency framework.
Materials and Methods: We undertook a narrative review of key studies on cross-platform console performance, robotic training curricula and assessment tools, including work validating the Global Evaluative Assessment of Robotic Skills (GEARS) and comparing it with binary, procedure-specific metrics. Concepts from aviation “type-rating” and everyday urological practice using multiple ureteroscopes informed a proposed training pathway.
Results: Simulation studies show early robotic surgeons achieve similar time, safety and efficiency metrics when moving between consoles, supporting cross-platform skill transfer once basic proficiency is reached. A recent scoping review highlights limited but consistent evidence that performance and safety are comparable across systems, with prior robotic experience shortening adaptation. Validated curricula demonstrate that core GEARS domains - depth perception, bimanual dexterity, efficiency, force sensitivity, robotic control and autonomy - can be trained and quantified. Binary, proficiency-based metrics provide more reliable discrimination between proficient and non-proficient trainees than GEARS alone. Synthesising these findings, we outline a stepwise curriculum: generic robotic skills to a GEARS/binary benchmark on one platform, followed by brief platform-specific “type-rating” modules and simple recency requirements on each system.
Conclusions: Available evidence suggests robotic console skills are transferrable between platforms. Embedding GEARS-informed, proficiency-based multi-platform training offers a practical way to address concerns about working across different robots while maintaining patient safety.
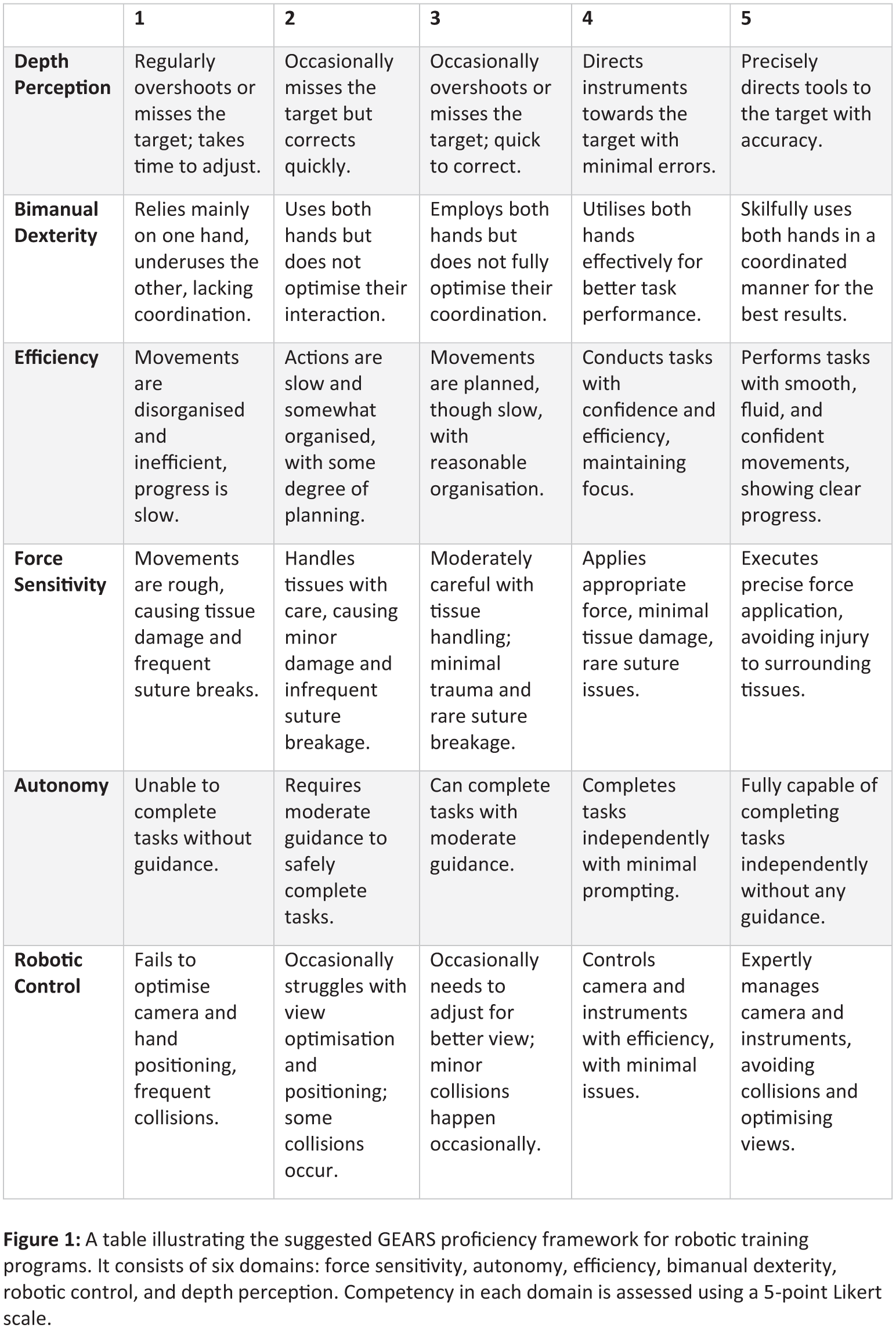
P17-5 Validation and clinical implementation of a Machine Learning model for predicting sepsis risk following ureteroscopy: a web-based decision support tool from EAU Urotechnology
Miss Demetra Fuligni1, Carlotta Nedbal, Vineet Gauhar, Daniele Catellani, Frédéric Panthier, Jeremy Y. C. Teoh, Ben H. Chew, Khi Yung Fong, Nariman Gadzhiev, Bhaskar Somani
1Southampton General Hospital, southampton, United Kingdom
Introduction: Postoperative sepsis remains a significant concern following ureteroscopy (URS). Accurate preoperative risk prediction may enhance perioperative planning and patient safety. This study externally validated multiple machine learning (ML) models for predicting septic risk and stone-free rate after URS, and implemented the validated models into a web-based clinical interface.
Materials: A previously published ML model was trained and internally tested using the multicentre FLEXOR database (6,669 patients). External validation was performed on an independent cohort of 817 patients undergoing URS for urolithiasis. Validation focused on generalization performance, including accuracy, precision, recall, and F1-score. The aim was to identify the most reliable model for predicting postoperative sepsis and related complications.
Results: Development and validation cohorts differed in patient and procedural characteristics, including age (57.2±19.3 vs 49.3±15.6 years), presentation with colic (63.0% vs 71.7%), stone diameter (10.0±6.8 vs 11.7±8.5 mm), use of ureteral access sheath (93.2% vs 35.9%), overall complications (8.0% vs 5.1%), sepsis (1.3% vs 2.8%), and SFR (78.3% vs 93.7%). Among all evaluated algorithms, the Extra Trees Classifier demonstrated the strongest external validation performance for postoperative sepsis (>90% accuracy across all metrics), outperforming other ensemble methods. Additional models showed high predictive ability for outcomes such as reintervention (Random Forest, 88.5%) and ureteral injury (XGBoost, 96.9%). A Python Shiny web application was developed to allow clinicians to input patient data, visualize predicted risks, and examine model explainability via feature importance and confusion matrices.
Conclusions: External validation confirmed that ensemble ML models provide reliable prediction of septic risk after URS.
P17-6 Can AI Hold Its Water? Agreement Between Consultants and an AI Triage Tool – a Pilot Diagnostic Concordance Study
Dr Azeem Kapasi
1
1Salford Royal Foundation Trust, Manchester, United Kingdom
Introduction: Urology consultants dedicate regular sessions to triaging increasing referral volumes. With expanding pre-investigation pathways and specialist clinics, we evaluated whether an AI triage system could replicate consultant decision-making and potentially reduce the clinical burden of manual triage.
Patients and Method: We retrospectively compared triage outcomes from an AI system with decisions made by consultant urologists for 40 anonymised referrals. For each case, we recorded AI-assigned acceptance, urgency (urgent vs routine), clinic allocation, and pre-clinic imaging requirements. Consultants were blinded to AI outputs. Agreement was assessed across three domains: (1) acceptance, (2) clinic allocation, and (3) urgency. Disagreements were reviewed for potential clinical significance.
Results: Consultants accepted 38/40 referrals (95.0%). Agreement between AI and consultants was high for acceptance (95.0%) and urgency (95.0%). Clinic allocation agreement was 85.0%, reflecting the complexity of multi-pathway assignment, with several cases where the AI recommended general urology but consultants selected nurse-led or procedure-specific clinics. Six cases (15%) demonstrated clinic-level disagreement, and two cases (5%) showed discrepancies in acceptance or urgency requiring closer inspection for under-triage risk. No immediate safety concerns, such as missed red-flag cancer referrals, were identified, though case-level review remains essential.
Conclusion: This pilot study shows strong concordance between the AI triage tool and consultant urologists for acceptance, urgency, and agreement for clinic allocation. Discrepancies highlight areas for refinement, particularly within nuanced subspecialty and nurse-led pathways. Larger prospective studies has already begun with integration into real-time triage workflows to determine the system’s potential to ease consultant triage workload before clinical adoption.
P17-7 A purpose-built patient-app platform to improve efficiency and sustainability in a post-MRI prostate cancer virtual clinic
Mr Petre Cristian Ilie2, Miss Anne Carrie1, Mr Mykhaylo Kostyuk2, Mr Radu Croitoru2, Mr Dimitar Ormanov2, Prof Lee Smith3
1Norfolk And Norwich University Hospital, Norwich, United Kingdom, 2The Queen Elizabeth Hospital, King’s Lynn, United Kingdom, 3Anglia Ruskin University, Centre for Health Performance and Wellbeing, Cambridge, United Kingdom
Introduction: A post-MRI prostate cancer Virtual Clinic (VC) can streamline decision-making, but efficiency depends on having structured information available before the consultation. A dedicated Healthium® digital platform with a patient app was implemented to deliver a Healthium Platform Questionnaire (HPQ) prior to VC, capturing symptoms, comorbidity/fitness, key safety information and patient preferences.
Patients and Methods: Two audit cycles assessed pre-clinic HPQ submission and barriers. Cycle 1 included the first 10 VC patients (January 2025; no exclusions). Following review, the pathway was amended by: (1) explaining HPQ importance during triage, (2) pre-VC telephone check of HPQ completion, (3) offering telephone support to complete the HPQ, and (4) updating the HPQ online within the platform. Cycle 2 included the first 50 VC patients (September/October 2025). Data were collected from medical records and transferred to a spreadsheet.
Results: Between 01/01/2025 and 02/10/2025, 198 patients attended the VC pathway. In Cycle 1, 50% had not submitted the HPQ prior to VC; 30% required help completing it; and 20% underestimated its importance (all had access to a computer or smartphone). After interventions, Cycle 2 achieved the 90% pre-VC HPQ completion target. Sustainability estimates per 100 patients were 0.85 tonnes CO₂ saved, 2117.2 travel miles avoided, and 3564 minutes (59.4 hours) of travel time saved.
Conclusions: A purpose-built digital platform with a patient app improved pre-consultation information capture for post-MRI prostate cancer VC appointments, supporting more efficient clinic flow and measurable travel and carbon savings.
P17-8 Efficacy and Safety of the UVapor® System water vapor thermal therapy in Patients with Benign Prostatic Hyperplasia: A Prospective, Multicenter, Single-blind, Randomized Controlled Trial
Dr Yujie Dong1, Dr Yang Yang1, Dr Xu Zhang1, Dr Yu Gao1
1The Third Medical Center of Chinese PLA General Hospital, Beijing, China
Objective: We assessed the efficacy and safety of the UVapor® System water vapor thermal therapy (WVTT) for treating benign prostatic hyperplasia (BPH) by conducting a prospective, multicenter, single-blind, randomized controlled trial.
Patients and Methods: Patients with BPH were randomized to receive either the UVapor® System WVTT or rigid cystoscopy sham surgery. The primary endpoint was the change in International Prostate Symptom Score (IPSS) from baseline at 3 months.
Results: A total of 126 patients were randomly assigned in a 2:1 ratio to either the treatment group (UVapor® System WVTT) or the control group (rigid cystoscopy sham surgery). At 3 months, patients in the treatment group exhibited a mean IPSS improvement of -13.6 ± 0.75 points, significantly greater than that in the control group (least squares [LS] mean difference = -11.7, 95% confidence interval [CI] -14.13 to -9.27). Patients in the treatment group demonstrated significant improvements in lower urinary tract symptoms (LUTS), flow rate, and quality of life (QOL) compared to both baseline and the control group, and were sustained throughout 6 months. Furthermore, no adverse effects on erectile or ejaculatory function were observed with the UVapor® System WVTT. The overall incidence of adverse events (AEs) in the treatment group was comparable to that in the control group, with no participant withdrawal or death resulting from AEs.
Conclusion: The UVapor® System WVTT demonstrates early, effective, and durable relief of LUTS while preserving sexual function, along with favorable safety outcomes. It is an effective and safe minimally invasive treatment for BPH.
P17-9 Patient-Reported Urinary and Sexual Outcomes: Aquablation Versus HoLEP
Dr Shiv Sarna1, Mr Simon McGurk1, Mr Shaun James1, Dr Husam Al Maliki1, Mr Sachinka Ranasinghe1, Mr Johann Boaz1, Mr Mark Rochester1
1Norfolk And Norwich University Hospital, Norwich, United Kingdom
Introduction: Surgical management of benign prostatic hyperplasia (BPH) can negatively affect urinary continence and sexual function, key determinants of post-operative quality of life. We compared patient-reported urinary continence and sexual outcomes following Aquablation and HoLEP in a single-centre cohort.
Patients and Methods: This retrospective single-centre study included men undergoing Aquablation or HoLEP for BPH between January 2023 and June 2025. Patients were contacted by telephone and completed validated post-operative questionnaires assessing urinary incontinence (ICIQ-UI Short Form), erectile function (SHIM), and ejaculatory function (MSHQ-EJD-SF). Baseline demographic and clinical variables were recorded and compared between groups.
Results: A total of 284 procedures were identified (118 Aquablation, 166 HoLEP), with completed questionnaires from 59 Aquablation and 69 HoLEP patients. Median follow-up was 20 months (IQR 10–28). Baseline characteristics, including age, BMI, ASA score, IPSS, and Qmax, were comparable. The mean prostate size for Aquablation and HoLEP was 61cc (±31.5) and 97cc (±70.3) respectively. Aquablation was associated with significantly better urinary continence (mean ICIQ-UI 1.88 vs 3.71, p=0.001) and superior ejaculatory preservation (mean MSHQ-EJD-SF 6.47 vs 3.90, p=0.002). A negative impact on sexual function was reported by 22.0% of Aquablation patients compared with 52.2% following HoLEP (OR 4.00, 95% CI 1.83–8.74, p=0.0005). Erectile function was similar (mean SHIM 12.71 vs 11.52, p=0.350).
Conclusions: Aquablation demonstrates significant advantages over HoLEP in urinary continence and ejaculatory outcomes without compromising erectile function. Our data supports Aquablation as a quality-of-life focused surgical option for appropriately selected men with BPH and should inform shared decision-making.
P17-10 Ejaculatory function preservation and restoration following robotic Aquablation for prostatic bladder outflow obstruction: a large real-world case series
Mr Thomas H Newman1, Dr Diana Shroff1, Dr Sakshi Rajain1, Miss Thomasia Azavedo1, Miss Elsie Mensah1, Mr Jonathan Noël1, Mr Sachin Malde1, Mr Rick Popert1, Miss Clarissa Martyn-Hemphill1
1Guy’s and St Thomas’ Hospital, London, United Kingdom
Introduction: Aquablation for surgical treatment of benign prostatic enlargement (BPE) causing bladder outflow obstruction (BOO) has demonstrated good functional outcomes, even for large glands, with high rates of ejaculatory preservation reported. This study aimed to review real-world outcomes of ejaculatory preservation or restoration post-Aquablation in an unselected cohort.
Patients (or Materials) and Methods: Retrospective data for ejaculatory function were collected from prospectively maintained consecutive case series of patients who underwent Aquablation, in a single UK centre from October 2023 to December 2025. Ejaculatory function was subjectively assessed by men 3-27 months post-operatively, and classified as: antegrade ejaculation, retrograde/low volume ejaculation, anejaculation or not sexually active.
Results: The series included 201 patients with data for ejaculatory function for 172 men (85.6%); mean age 65 years (24-91) and mean prostate volume 72.3cc (21-200). Available functional outcomes demonstrate mean IPSS and PVR improvement (13.6 IPSS decrease, 2.8 QoL increase with 106.2ml PVR reduction).
Of 123 patients (71.5%) who had antegrade ejaculation pre-operatively, 116 were sexually active post-operatively; 91/116 (78.4%) had ejaculation preservation, 11/116 (9.5%) low volume/retrograde ejaculation, and 14/116 (12%) anejaculation. Of the 31 patients who had retrograde (21, 12.2%) or anejaculation (10, 5.8%) pre-operatively, 30 were sexually active post-operatively; 15/30 (50.0%) had ejaculation restoration, 6/30 (20.0%) low volume/retrograde ejaculation, and 9/30 (30.0%) anejaculation.
Conclusion: This series demonstrates that Aquablation, for the treatment of BPE-related BOO, preserves ejaculatory function for most patients, in line with previously published data. It can lead to ejaculatory restoration for men with retrograde/anejaculation pre-operatively.