
Abstract
Objectives:
We report on the outcomes following holmium laser enucleation of the prostate (HoLEP) and/or prostate artery embolization (PAE) for patients with catastrophic haematuria secondary to prostatic bleeding.
Patients & Methods:
A retrospective review of all patients receiving HoLEP and/or PAE between April 2023 and 2025 for prostatic bleeding was performed in our tertiary centre. We report on outcomes following intervention.
Results:
Eleven patients were included with prostate volumes > 100cc: seven received HoLEP, three PAE and one received HoLEP after PAE. Median (interquartile range [IQR]) time from admission to procedure was 6 days (4–11) and 11 days (7–13) for HoLEP and PAE, respectively. All patients had successful resolution of haematuria; median time from procedure to resolution was 1 day (1–2) and 1 day (1–1), and median length of stay was 10 days (8–14) and 13 days (8–17), for HoLEP and PAE respectively. Six patients required transfusion during admission, median (IQR) pre-operative Hb drop was 14 g/L (5–21) and successful trial without a catheter was performed on all patients. One patient developed a hospital-acquired pneumonia; another required an urgent HoLEP following PAE for ongoing haematuria on day 8.
Conclusions:
Within our unit, urgent HoLEP and PAE are complementary management options for patients with intractable bleeding from significantly enlarged prostates. Timely intervention prior to the procedure is vital in the safe management of such patients.
Introduction
Patients suffering from significant haematuria secondary to significant prostatic enlargement poses clinical challenges. Traditional transurethral resection of the prostate (TURP) provides limited haemostatic control due to operative time constraints in potentially unstable patients while open simple prostatectomy subjects patients to significant intra-operative bleeding and prolonged post-operative recovery in hospital. 1 Holmium laser enucleation of the prostate (HoLEP) and prostate artery embolization (PAE) have been developed to manage benign prostatic enlargement, particularly in extremely large prostates that otherwise would be subject to simple prostatectomy or catheter-based management.2,3 Reports in the use of these techniques in the context of persistent haematuria are limited.4,5 Improved safety and efficacy of HoLEP and PAE compared to TURP have been demonstrated in elective cases with and without anticoagulation.6–8 Predictably, patients receiving anticoagulation demonstrated higher rates of post-HoLEP haemorrhagic complications than those without anticoagulation. 9 The aim of this study was to evaluate the emergency use of HoLEP and PAE for life-threatening haematuria requiring admission from a high-volume tertiary centre.
Patients and methods
Cohort
All patients receiving either HoLEP or PAE were reported into a prospective database. Interventions were considered ‘emergency’ if performed within the same admission for haematuria. Retrospective case review was performed on all patients treated with emergency HoLEP and/or PAE between April 2023 and 2025 and registered locally as an audit of safety outcomes. HoLEP and PAE were performed by experienced clinicians.
Procedural technique
HoLEP was performed under general anaesthesia using a 550-µm holmium laser end-fire fibre connected to the Lumenis PulseTM 120H generator and 26-Ch continuous flow resectoscope. Enucleation technique included trilobar, bilobe and en bloc depending on prostate anatomy and clinician experience. PAE was performed under local anaesthesia, and preoperative computed tomography (CT) angiogram was obtained for planning. Right-sided common femoral access was gained with 5F sheath. Left internal iliac artery was cannulated with a 65-cm 4F c2 catheter and 180-cm 0.035ʺ Terumo wire. Through the c2 catheter, the prostate artery was then accessed with a combination of 2.0 Progreat catheter and 200-cm 0.014ʺ fathom wire. The artery was preloaded with 5 ml of 5% dextrose and then embolised with a 1:6 glubran–lipiodol mix. A Waltman loop was formed in the aorta using the c2 catheter and Terumo wire, and the right internal iliac artery was accessed. The right prostate artery was then accessed in the same manner as the left one and embolised. The arteriotomy sight was then closed using a 5F Mynx device.
Post-treatment care
Continuous bladder irrigation was provided in all patients following intervention and reviewed daily. The absence of urothelial malignancy was confirmed with CT intravenous urogram, ultrasound, and/or cystoscopy. The decision for HoLEP was based on haemodynamic stability, the ability to discontinue anticoagulation therapy where relevant and the need for cystoscopic evacuation of blood clot from the bladder under general anaesthetic.
Outcomes
The primary outcome was time to resolution of haematuria. Baseline demographics, course of events during admission including blood results and adverse events following treatment were evaluated and described. Baseline demographics included age at the time of admission, method of prostate cancer evaluation, admitting hospital status (local or external), prostate volume according to imaging and anticoagulation status.
Secondary outcomes included (1) change in serum haemoglobin use, (2) requirements of red cell transfusion before and after the procedure, (3) time to procedure, (4) catheter dwell time, (5) length of admission and (6) status at last case note review (30 September 2025). Descriptive statistics are reported as appropriate. This retrospective review was conducted in accordance with the Declaration of Helsinki.
Results
Demographics
Eleven patients were included in the study, 7 (64%) patients received HoLEP (patients 2–8), 3 (27%) received PAE (patients 9–11) and another received PAE followed by HoLEP as a planned staged procedure (patient 1). Patient demographics are reported in Table 1, post-treatment outcomes are reported in Table 2. One patient receiving emergency HoLEP had a PAE 5 years prior for lower-urinary-tract symptoms (patient 5), and another received a PAE with temporary resolution of haematuria on an admission 31 days prior to re-admission for further bleeding (patient 6). Figure 1 demonstrates the imaging associated with patient 9, who underwent a PAE following multiple admissions for prostatic bleeding. Only one patient received PAE for haematuria following a diagnosis of prostate cancer (patient 11); the other 10 patients were evaluated for prostate cancer using serum Prostate Specific Antigen (PSA) and/or PSA density (using magnetic resonance imaging [MRI] or CT prostate sizing).
Pre-treatment demographics.
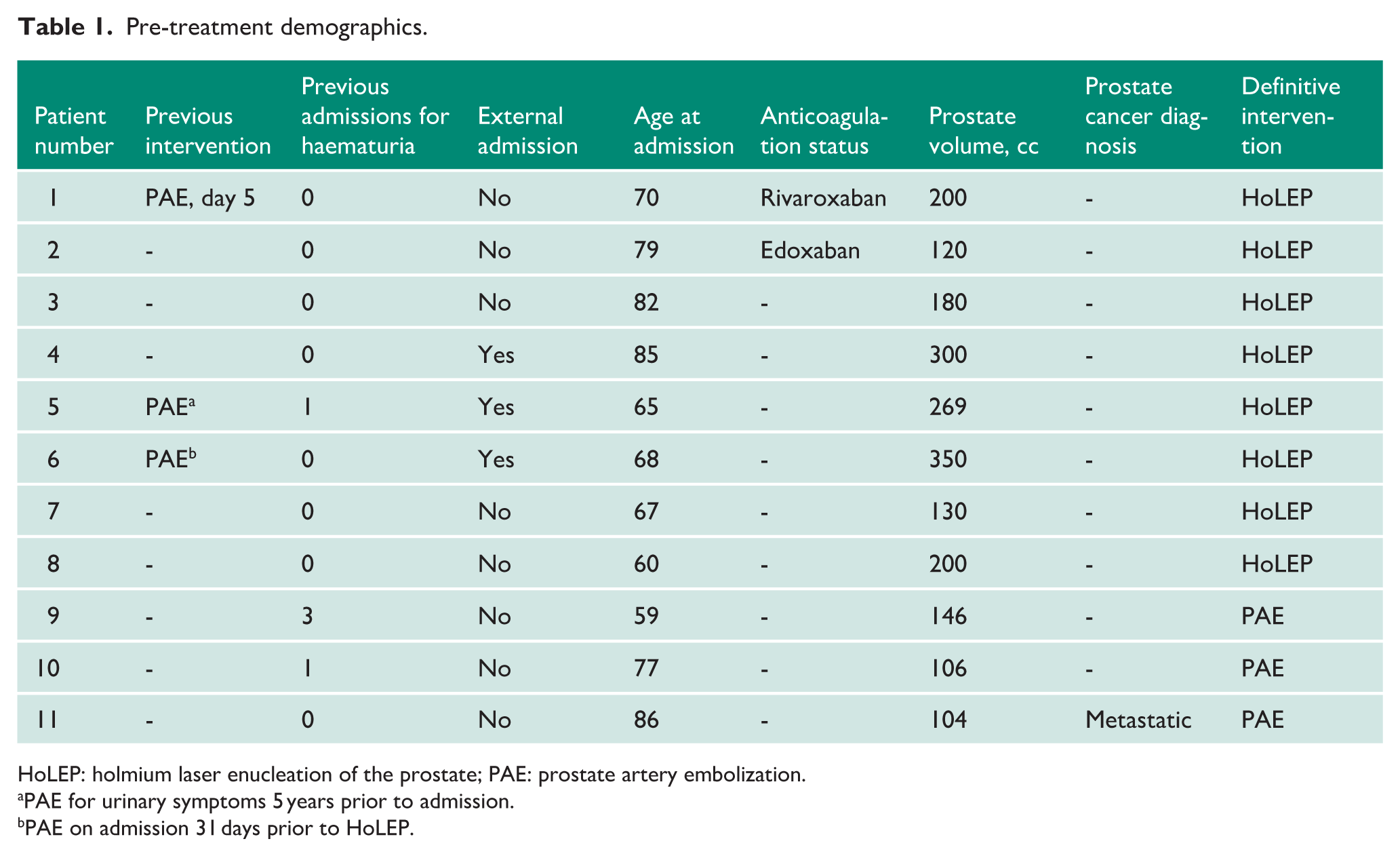
HoLEP: holmium laser enucleation of the prostate; PAE: prostate artery embolization.
PAE for urinary symptoms 5 years prior to admission.
PAE on admission 31 days prior to HoLEP.
Clinical outcomes.
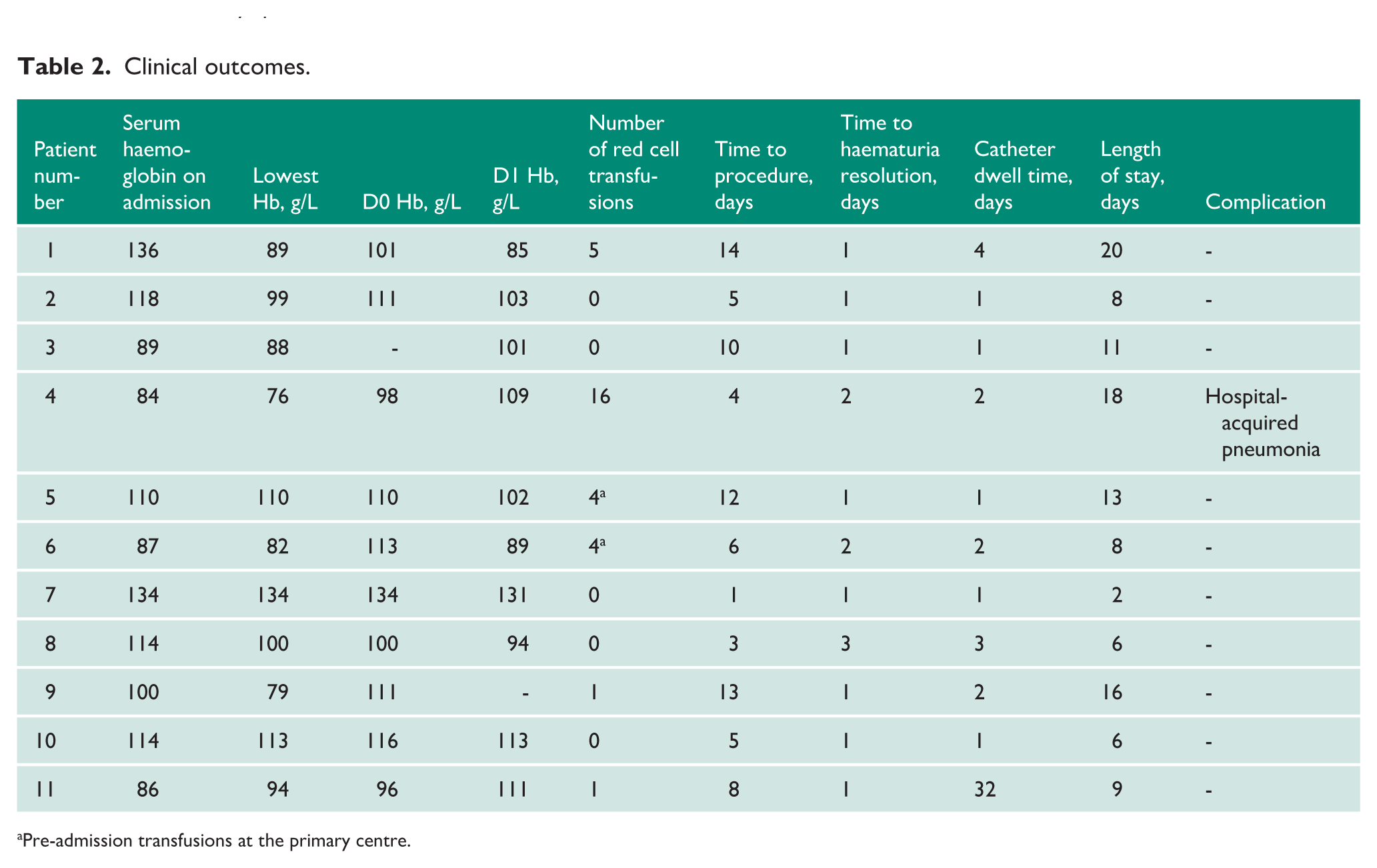
Pre-admission transfusions at the primary centre.
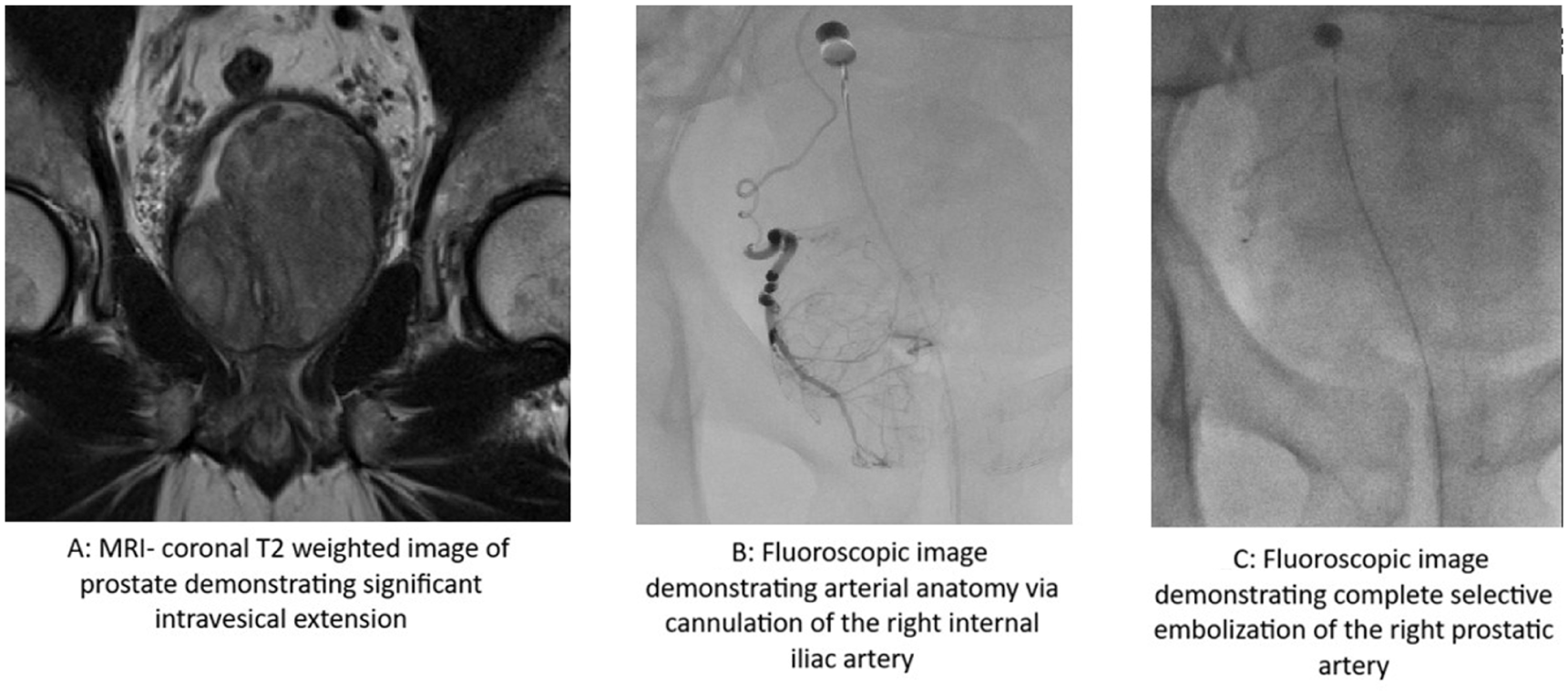
Images of patient 9 receiving PAE for prostatic bleeding.
Embolisation was considered complete in 4/6 (66%) patients (patients 1, 6, 9 and 11). No patients required catheterisation for urinary retention prior to emergency admission. Only two patients were anticoagulated prior to admission with either rivaroxaban or edoxaban; one received PAE followed by HoLEP and one received HoLEP (patients 1 and 2, respectively). The former had a background of left ventricular thrombus, hence complete discontinuation of the anticoagulation therapy (rivaroxaban) was a high-risk step. He was transitioned to treatment-dose low-molecular-weight heparin (LMWH), with discontinuation on the day of PAE and recommencing treatment the following day. He underwent HoLEP while anticoagulated with LMWH. Three patients were transferred from peripheral hospitals for ongoing management of haematuria (patients 4–6), and three had at least one prior admission for haematuria (patients 5, 9 and 10).
Median (interquartile range [IQR]) age of patients receiving HoLEP and PAE was 69 (66–81) and 73 (67–79), respectively. All patients had prostate volumes greater than 100cc based on MRI or cross-sectional imaging, and patients undergoing HoLEP had considerably large prostates. Median (IQR) prostate volumes were 200cc (168–277) pre-HoLEP and 126cc (106–160) pre-PAE. Median (IQR) grammes enucleated via HoLEP was 117 g (98–195).
Primary outcome
All definitive interventions demonstrated resolution of haematuria; median (IQR) time to reported resolution was 1 (1–2) and 1 (1–1) day following HoLEP and PAE, respectively.
Secondary outcomes
Six patients required red blood cell transfusion with appropriate blood product adjuncts prior to the intervention to maintain appropriate serum haemoglobin levels and coagulation profiles. Considerable drops in serum haemoglobin during admission were noted. Patients receiving HoLEP noted median (IQR) haemoglobin of 112 g/L (89–122) on admission, the lowest level was 94 g/L (87–103) pre-operatively and 110 g/L (93–105) on the day of HoLEP. Haemoglobin level on day 1 after HoLEP was 102 g/L (93–105). Patients receiving PAE were admitted with median (IQR) haemoglobin levels of 107 g/L (97–120), and the lowest level was 87 g/L (77–99) and 104 g/L (95–112) on the day of PAE. Two patients undergoing PAE only required one red blood cell transfusion; the patient that underwent PAE and HoLEP required three units around the time of PAE and a further two prior to HoLEP. On day 1 following PAE, the median (IQR) haemoglobin level was 111 g/L (102–112). No patients required transfusion of red blood cells after the definitive intervention.
Patients underwent HoLEP within 6 (IQR 4–11) days of admission, while patients underwent PAE 11 days (7–13) following admission. No adverse events specific to HoLEP or PAE were reported. One patient, while arranging for social support following discharge, developed a hospital-acquired pneumonia following HoLEP, 4 days after resolution of haematuria (patient 4). Median time from catheter removal was 1 day (1–2) and 2 days (2–17) after HoLEP and PAE, respectively. One patient failed to void the day following PAE but passed the trial without catheter following discharge (patient 11). Subsequently, the median (IQR) time from intervention to discharge and total length of stay was 3 (1–3) and 1 (1–2) days and 10 (8–14) and 13 (8–17) days following HoLEP and PAE, respectively. As reported previously, one patient was readmitted for haematuria following PAE and received HoLEP with complete resolution of symptoms. All patients were alive, had no further hospital admissions for haematuria following definitive treatment and were urethral catheter-free at the last case note review.
Discussion
This is the first evaluation of the use of HoLEP and/or PAE in the same unit in the context of significant prostatic bleeding. Patients reported in this study were noted to have significant haematuria, resulting in a decline in serum haemoglobin levels, with half the patients requiring red cell transfusions. HoLEP was the standard treatment of choice, and the three patients receiving upfront PAE were considered high anaesthetic risk for prolonged surgery. Both procedures were safe and provided early resolution of haematuria. Only one patient received PAE and required re-admission for haematuria, subsequently receiving HoLEP to good effect.
We propose the below treatment paradigm for patients admitted with intractable prostatic bleeding (Figure 2).
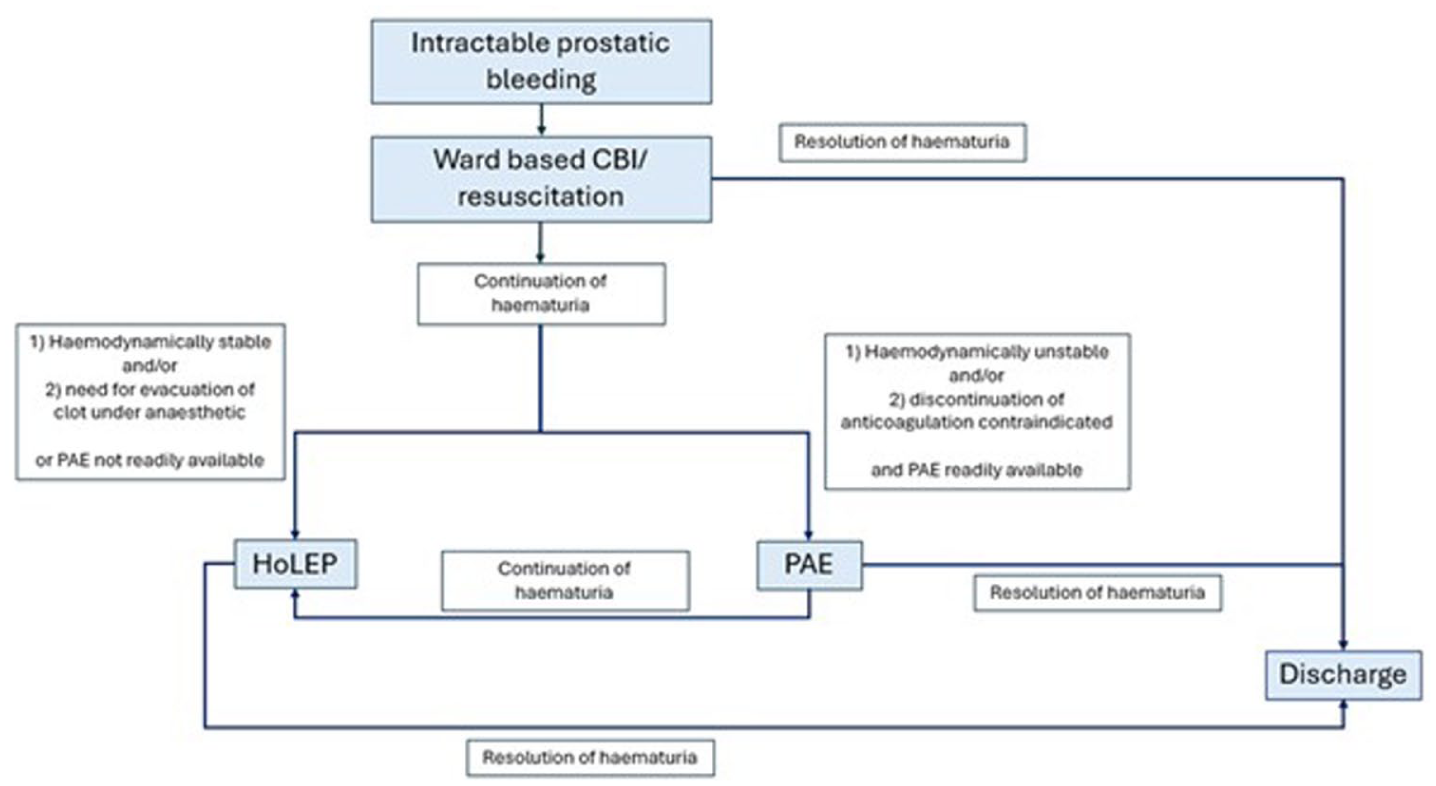
Flow diagram of the proposed treatment algorithm of patients admitted with intractable prostatic bleeding.
Interestingly, contrary to Hines et al., 10 demonstrating persistence of haematuria in 18% of elective patients receiving HoLEP, we report on haematuria resolution within a day of HoLEP in the emergency setting. Our findings compliment that of Elmansy et al., 11 reporting on quick resolution of haematuria with limited morbidity. Resolution of haematuria quicker than typically seen in the elective setting may be due to technical changes, whereby more extensive bipolar and laser diathermy is potentially applied in the emergency setting.
PAE was performed less often and in our more comorbid patients. Time to haematuria resolution was also 1 day after the procedure and reflects clinical efficacy published in multiple published elective retrospective series.4,5,12 Our unit has previously published upon success rates of haematuria resolution following PAE. 13 Haematuria outside the context of urological cancer and requiring PAE is rare. 14 Other centres have reported on the use of PAE for the management of intractable prostatic bleeding in patients not suitable for prolonged general anaesthetic required for HoLEP, with very little early morbidity associated, aligning with our study. 15 A systematic review by Moramarco et al. 16 report on the safety and efficacy of PAE for prostatic haematuria in patients with a variety of aetiologies and reported demonstrated favourable haemostasis between 67% and 100% of patients, though they additionally note the importance of appropriate selection according to vascular anatomy to provide such reassuring results. The results from this study reinforce the appropriateness of PAE in such a setting.
Similar to Romero-Otero et al., 17 post-HoLEP decline in serum haemoglobin levels did not demonstrate clinical significance, suggesting that HoLEP can resolve haematuria without significant blood loss. Of note, a combined procedure of PAE followed by HoLEP was performed safely in a patient who could not have discontinuation of anticoagulation for significant periods of time. The use of PAE prior to prostatic surgery in anticoagulated patients has been reported by Shin et al., 18 demonstrating lower haemoglobin reduction and shorter length of hospital stay when compared to non-embolised patients. Despite continuation of anticoagulation in our patient, haematuria settled within 1 day of HoLEP, and haemoglobin drop of only 16 g/L was noted.
Like Deuker et al., 19 despite heterogeneity of anticoagulation use in our cohort, our intervention-related complication rates were low. One patient following HoLEP had a prolonged admission due to a case of hospital-acquired pneumonia developed during a period of social admission 3 days after resolution of haematuria. Contrary to previous reports, we observed no haemorrhagic complications specifically associated with the intervention. 9 No long-term sequelae were noted for any patient admitted and treated. Three patients were transferred from external hospitals for definitive management, all of whom were noted to have resolution of haematuria within 2 days of HoLEP.
Only one patient received tranexamic acid within their haematuria management. Assmus et al. 20 did not demonstrate differences in the ability to discharge patients on the same day in the elective setting. A prospective evaluation within the emergency setting is required to determine if the use of tranexamic acid is beneficial.
We acknowledge the limitations of this study. First, our cohort was treated by surgeons with significant experience, and hence may not represent replicable safety results across lesser-experienced clinicians and centres. Second, the small cohort size limits our ability to draw definitive conclusions on the safety of procedures, especially in patients requiring anticoagulative therapies.
This study has numerous strengths. First, we report on a pragmatic approach to the management of intractable prostatic bleeding according to individual appropriateness of intervention. Second, we highlight the importance of a multidisciplinary approach, engaging urological, anaesthetic, haematological, radiological and interventional radiological team members equally. Finally, this study demonstrates that timely intervention within a healthcare network including multiple sites can lead to rapid definitive resolution of significant haematuria with limited associated morbidity.
Conclusions
Patients with large prostates and subsequent significant haematuria pose a clinical dilemma. Haematuria can be catastrophic, and timely definitive intervention is vital. Early transfer to specialist hospitals within healthcare networks can optimise patient outcomes. Both HoLEP and PAE were safe procedures capable of providing resolution of haematuria quickly.
Footnotes
Ethical considerations
All patients were treated with standard of care practice in our unit. The study was performed in accordance with the Declaration of Helsinki.
Consent to participate
Need for informed consent for publication was waived as identifiable data was not used and the study was registered locally as an audit.
Consent for publication
Patient consent for the publication of imaging was provided and stored locally.
Author contributions
All authors participated in the treatment of patients included within the study and in the development and analysis of the manuscript. All authors reviewed and edited the manuscript prior to submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available from the corresponding author upon reasonable request.
Informed consent
Need for informed consent for publication was waived as identifiable data was not used and the study was registered locally as an audit. Retrospective review of case notes was registered locally as an audit of practice, therefore need for informed consent was waived.
Guarantor
DR and BC confirm the accuracy of the data.