
Abstract
Objectives:
Urologists are noting a surge in patients they see who are concurrently taking weight-loss injections, due to exponential rises in prescriptions of glucagon-like peptide-1 receptor agonists (GLP-1RAs) for medical and aesthetic purposes. This study aims to summarise current evidence around GLP-1RAs by categorising their unintended benefits and side effects across common urological conditions that may have important ramifications within the field of urology.
Materials and methods:
Comprehensive literature review using PubMed®, MEDLINE® and Google™ Scholar for relevant scientific articles published in English. Manual bibliography search and “related article” functions were employed to supplement original searches.
Results:
Current knowledge of the collateral impact of GLP-1RA on common urological conditions, such as erectile dysfunction (ED), UTIs, urolithiasis, urological malignancies and hypogonadism is conflicting and predominantly based on weak levels of evidence. Pubmed® identifies 79 relevant studies relating GLP-1RA to the chosen common urological conditions. There are no randomised controlled trials (RCTs) dedicated to GLP-1RA whose primary outcome pertains directly to urological symptoms and/or sequelae.
Conclusion:
GLP-1RA may exert clinically relevant effects across multiple urological domains; however, current evidence is insufficient to draw definitive conclusions. Long-term safety data are lacking. Urologists should remain vigilant while prospective, urology-focused RCTs are urgently needed.
Levels of evidence:
Not applicable.
Keywords
Introduction
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are a medication class originally developed to treat type 2 diabetes. 1 GLP-1 receptor activation results in numerous physiological changes, including slowed gastric emptying, improved glucose homeostasis and stimulation of satiety, such that certain GLP-1RAs were approved to treat obesity. 1
Tirzepatide (Mounjaro®) and semaglutide (Wegovy®), for example, were recently authorised by the medicines and healthcare products regulatory agency (MHRA) for such use in the United Kingdom in 2023 and 2026, respectively.2,3
This recent UK market access rapidly led to a surge in use of weight-loss drugs – both for medical and aesthetic purposes – with an estimated 1.6 million people having used a weight-loss injection in 2024 in the United Kingdom. 4 Their use is predicted to rise dramatically worldwide during the forthcoming decade. 4
Urologists, like most other UK specialists, have inevitably and anecdotally noted a significant rise in the proportion of patients they are seeing in daily practice who concurrently happen to be using GLP-1 agonists.
Current knowledge of the unintended impact of GLP-1RA on common urological conditions, such as ED, UTIs, urolithiasis, urological malignancies and hypogonadism is often conflicting and predominantly based on anecdotal evidence rather than dedicated high-powered studies. Indeed, there are no randomised controlled trials (RCTs) dedicated solely to GLP-1RA whose primary outcome pertains directly to urological symptoms and/or sequelae.
Furthermore, the long-term risks (including cancer of any type) of GLP-1RA used over many years or decades remain unknown. 5
This study, therefore, aims via a comprehensive literature review to evaluate and summarise current available evidence around the use of GLP-1RA from a broad-based urological perspective, aiming to categorise their unintended benefits and side effects across common urological conditions that may have important ramifications on current and future practice of urologists.
To the author’s knowledge, this is the first such comprehensive and structured article in the literature.
Materials and methods
The method of the study was a comprehensive literature review performed by all the authors. PubMed, MEDLINE® and Google™ Scholar were searched for relevant scientific articles published to date in English. Manual bibliography search of the identified publications and “related article” functions were employed to supplement the original search.
No specified time frame for publication was set. No specific exclusion criteria were applied.
Keywords for the literature search included “GLP-1 agonist and -erectile dysfunction,” “urinary tract infections,” “kidney stones,” “prostate cancer,” “renal cancer,” “bladder cancer” and “hypogonadism”
These were also used in combination with the Boolean operators: AND OR.
Artificial intelligence was not used in any part of the study or manuscript production.
Results and discussion
Erectile dysfunction
Obesity is a well-established risk factor for developing ED in men. Lifestyle modification resulting in a decrease in patient’s body mass index (BMI) is favourable in improving their erectile function. 6 It would, therefore, be logical to hypothesise that the weight loss associated with the prescription of GLP-1RA would translate into improved erectile function in those with ED.
Current evidence, however, features contrasting results in this regard. This may partly be attributable to an incomplete understanding of the mechanisms by which GLP-1RA influences sexual function.
The PubMed® database identifies 25 studies under the search “GLP1-RA and erectile dysfunction.”
Able et al. 7 compared a cohort of 3094 obese non-diabetic men aged 18–50 years receiving semaglutide, with an equal number cohort of obese non-diabetic men who never received the drug, finding the cohort receiving semaglutide was significantly more likely to develop ED and/or be prescribed PDE5 inhibitors.
Langroudi et al. 8 analysed the Food and Drug Administration Adverse Event Reporting System (FAERS) database on reports of male sexual dysfunctions associated with the prescription of GLP-1RA. Numerous reports of male sexual dysfunction were identified, with a greater frequency of events compared with general adverse events. Further analysis, however, suggested the association was weak and potentially lacked clinical significance.
Conversely, other studies found therapeutic benefit of GLP-1RA on ED, particularly in diabetics.
Giagulli et al. 9 conducted a retrospective study evaluating whether adding liraglutide to lifestyle changes, metformin and testosterone replacement could improve erectile function in hypogonadal diabetic obese men with ED. The study found that the addition of liraglutide resulted in a significant increase in international index of erectile function (IIEF) score. 9
Similarly, in a sub-analysis by Bajaj et al. 10 as part of a placebo-controlled RCT of the effect of dulaglutide on cardiovascular outcomes, participating men were asked to complete IIEF-scores at baseline and as follow-up. This study showed that men receiving dulaglutide had smaller decreases in erectile function over time, compared with placebo.
More research is required to fully determine the relationship between ED and GLP-1RA. Currently, a comprehensive summary of the literature does not clearly determine whether GLP-1RAs are beneficial/detrimental to treating ED.
Urinary tract infections
UTIs are not listed as recognised side effects of GLP-1RA, although anecdotal evidence features reports of patients experiencing UTIs or similar lower urinary tract symptoms (LUTS) while taking such medications. Recognised side effects of GLP-1RA, however, include nausea, vomiting and diarrhoea, 11 which if severe can lead to dehydration, thus hypothetically predisposing the development of UTI in affected patients.
Conversely, the anti-inflammatory properties and improved diabetic control associated with GLP-1RA are also well-established in clinical practice, which should thus confer protection against infections. 12
Hence, the full relationship of GLP-1RA and risk of UTI remains unclear, and current evidence features contrasting results.
PubMed® database identifies seven studies under the search “GLP1-RA and urinary tract infections.”
Chan et al. 13 conducted a retrospective study comparing a cohort of diabetic adults managed initially via semaglutide with a control cohort who were prescribed other medications (e.g. insulin and metformin), with the primary outcome being incidence of common infections. The study found 23%–49% relative reductions in common infections in adults with type 2 diabetes taking semaglutide, including a reduced UTI incidence.
Likewise, Hammad et al. 14 reported lower incidences of UTI in patients taking GLP-1RAs in their retrospective cohort study comparing non-diabetic patients undergoing overactive bladder (OAB) treatment with onabotulinum toxin-A with GLP1-agonist versus receiving onabotulinum toxin-A alone.
These findings, however, were not supported in the meta-analysis of 136 RCTs by Han et al., 12 who despite identifying that GLP-1RA was associated with a significant reduction in certain serious infections, such as respiratory and musculoskeletal, no benefit was observed in the reduction of UTIs.
In contrast, Hsiao et al. 15 reported a higher risk of catheter-associated UTIs in diabetic patients with chronic kidney disease associated with GLP-1RA use, compared with patients in the same group taking SGLT2 inhibitors (e.g. dapagliflozin).
Similarly, Frías et al. 11 in their double-blind, placebo-controlled trial randomising diabetic adults on metformin to receive additional once-weekly exenatide versus placebo found UTI was the most common adverse event reported, albeit comparable between the two groups.
More research is, therefore, required to fully determine the relationship between UTI and GLP-1RA. Currently, a comprehensive summary of the literature does not clearly determine whether GLP-1RAs are beneficial/detrimental to preventing UTIs.
Urolithiasis
It is well-established that obesity, as part of the wider “metabolic syndrome,” is a risk factor for urolithiasis. 16 However, it also holds true that rapid weight loss, for example, in patients undergoing bariatric surgery, can increase the risk of urolithiasis. 17
There is thus conflicting evidence in the literature around the association of urolithiasis with GLP-1RA use.
The PubMed® database identifies five studies under the search “GLP1-RA and kidney stones.”
A retrospective study by Xie et al., 18 which used a US database of more than a million diabetic patients to evaluate the risks of GLP-1RA compared with other commonly used hypoglycaemic agents, reported an increased risk of urolithiasis in patients taking GLP-1RA.
Another meta-analysis of 20 RCTs by Liu et al. 19 involving 15,905 patients, which aimed to evaluate the relationship between tirzepatide and adverse cardio-renal events, however, did not identify an increased risk of urolithiasis in patients receiving GLP-1RA.
A similar lack of association was reported by Soogoor et al. 20 in their retrospective review of the TriNetX network. This study compared adults aged 18–60 years receiving semaglutide for weight management versus a matched control never receiving the drug, finding no increased risk of urolithasis in the treatment group.
Feghali et al. 21 evaluated 24-hour urine chemistry alterations in patients with urolithiasis during weight loss with GLP-1RA, noting limited reductions in urinary oxalate concentration in treated patients whose lithogenicity was not found to be increased.
A retrospective study of patients with a kidney stone also taking GLP-1RA found that those on semaglutide had a significantly lower risk of stone growth and intervention, compared with those on liraglutide or dulaglutide. 22 The pathophysiology behind this association was not elucidated, but the authors highlighted a potential role of semaglutide in the management of high-risk stone formers.
Currently, a comprehensive summary of the literature does not clearly determine whether GLP-1RAs are beneficial/detrimental to preventing stone formation and/or growth.
Urological malignancies
Numerous studies investigating GLP-1RA have highlighted their potential to interfere with the proliferation of several cancer types.23,24 GLP-1RA also plays a key role in modulating cellular apoptosis, which thus may have implications in carcinogenesis. 1
The long-term oncological safety of decades of GLP-1RA use, however, remains unknown.
Preliminary meta-analyses of the general oncological risks of GLP-1RA have not shown a definite increase in risk for any type of malignancy; however, all the studies included had follow-up periods below 10 years. 5
Correspondingly, there is a paucity of strong evidence addressing the association of GLP-1RA with urological malignancies.
PubMed® database searches identify 10 studies under “GLP1-RA and prostate cancer,” 24 studies under “GLP1-RA and renal cancer,” and 3 studies under “GLP1-RA and bladder cancer.”
The relationship between GLP-1RA and prostate cancer has been explored in preliminary studies. 25 GLP-1 receptor activation was initially linked to suppression of cellular androgen activity, which theoretically would mimic hormone therapy for prostate cancer; however, studies subsequently demonstrated no discernible alteration in androgen receptor expression within prostate cells during GLP-1RA therapy. 25
Sharma et al., 26 in a meta-analysis of five studies, reported a statistically significant 28% reduction in prostate cancer risk associated with GLP-1RA use versus placebo or other antidiabetic drugs. The authors recognised the inherent limitations of observational studies, which formed the majority of their data, and recommended that further research be undertaken.
Retrospective review of health-record databases of diabetic patients by Wang and Kim 27 compared the cancer risk of metformin versus GLP-1RA users. This also showed that GLP-1RA use reduced the risk of prostate cancer. Another retrospective review by Levy et al. 28 of obese patients via the TriNetX database also found GLP-1RA use reduced the risk of prostate cancer compared with untreated patients.
No meta-analysis or large-scale retrospective cohort review has reported an increased risk of prostate cancer in patients treated with GLP-1RA.
Fewer studies have focused on the association between GLP-1RA and risk of urothelial and/or upper tract malignancies.
Network meta-analysis by An et al. 29 of studies featuring diabetic patients being compared with different classes of antidiabetic drugs versus placebo or another antidiabetic drug found a significant reduction in bladder and renal cancers in GLP-1RA users versus placebo.
These findings, however, were not reported in Silverii et al.’s 5 meta-analysis, where no difference in bladder cancer incidence was found in GLP-1RA users versus other comparator arms. Another meta-analysis of RCTs involving patients receiving tirzepatide versus placebo or any active comparator in the control arm also did not note a risk reduction in bladder and/or renal cancer. 30
Currently, a comprehensive summary of the literature does not clearly determine whether GLP-1RA increases or decreases the risk of urological malignancy – although no clear link has been found.
Hypogonadism
Testosterone replacement therapy (TRT) is the standard intervention to treat symptomatic male hypogonadism. TRT, however, is associated with increased risks of prostate cancer, cardiovascular complications and thromboembolism. 31 Alternatives to TRT, therefore, have been explored to regulate testosterone.
Simply losing weight will increase testosterone levels in obese men by reducing their body fat, which converts testosterone into oestrogen. GLP-1RA, therefore, is appealing in the management of hypogonadism not only due to the weight loss associated with their use but also via their potential to directly affect testosterone levels. Evidence suggests that GLP-1 receptors are present in the testes, 32 raising questions about the potential implications of these drugs on male fertility.
The PubMed® database identifies five studies under the search “GLP1-RA and hypogonadism.”
Meta-analysis by Orra et al., 33 incorporating four studies of adult men with hypogonadism and/or obesity and/or diabetes, revealed that GLP-1RA use versus placebo, or versus other diabetic medication, was associated with a significant increase in bioavailable testosterone – but no change in free testosterone or SHBG.
Similarly, Raheem et al.’s 34 systematic review, which included seven studies involving adult men, reported GLP-1RA therapy was associated with significant increases in total testosterone concentrations, compared with TRT, placebo or metformin.
A small randomised control study by La Vignera et al. 35 randomised 83 obese men with hypogonadism to tirzepatide versus no treatment versus transdermal TRT. In their short follow-up study of 2 months, they reported a statistically significant increase in total testosterone in the tirzepatide group, who also benefitted from statistically significant reductions in body weight and waist circumference. The authors proposed that the increase in testosterone was most likely due to tirzepatide’s ability to enhance insulin sensitivity and reduce visceral fat, both of which are known to affect testosterone production.
Despite potentially promising results of GLP-1RA therapeutic role in the management of low testosterone, caution must be exercised as the direct effects of these drugs on sperm function and overall male fertility remain largely unexplored in clinical studies. For example, Fontoura et al. 36 published a case report regarding the adverse effect of liraglutide on sperm quality, which was restored after 5 months of discontinuation of the medication.
Currently, a comprehensive summary of the literature does not clearly determine whether GLP-1RAs are beneficial/detrimental in the management of hypogonadism. Evidence, however, is strong that weight loss and exercise have a favourable impact on the management of hypogonadism.
To date, no prospective RCT has been conducted comparing GLP-1RA versus placebo, with the primary outcome determined as effect on serum testosterone or quality of semen parameters.
Overall, in the literature review, there is a noteworthy preponderance of retrospective and database-based studies. Most studies focus on non-urological primary outcomes, and so there is a recognised risk of confounding.
Furthermore, the urological benefits noted from GLP-1RA, which undoubtedly have potential promise, could arguably result from the achieved weight loss as opposed to being specific to the drug itself. Nonetheless, collateral benefits are still clinically important.
A summary of all the studies and outcomes discussed in the ED, UTIs, urolithiasis, urological malignancies and hypogonadism sections is included in Table 1.
Summary of studies of GLP-1RA with urological relevance and their outcomes.
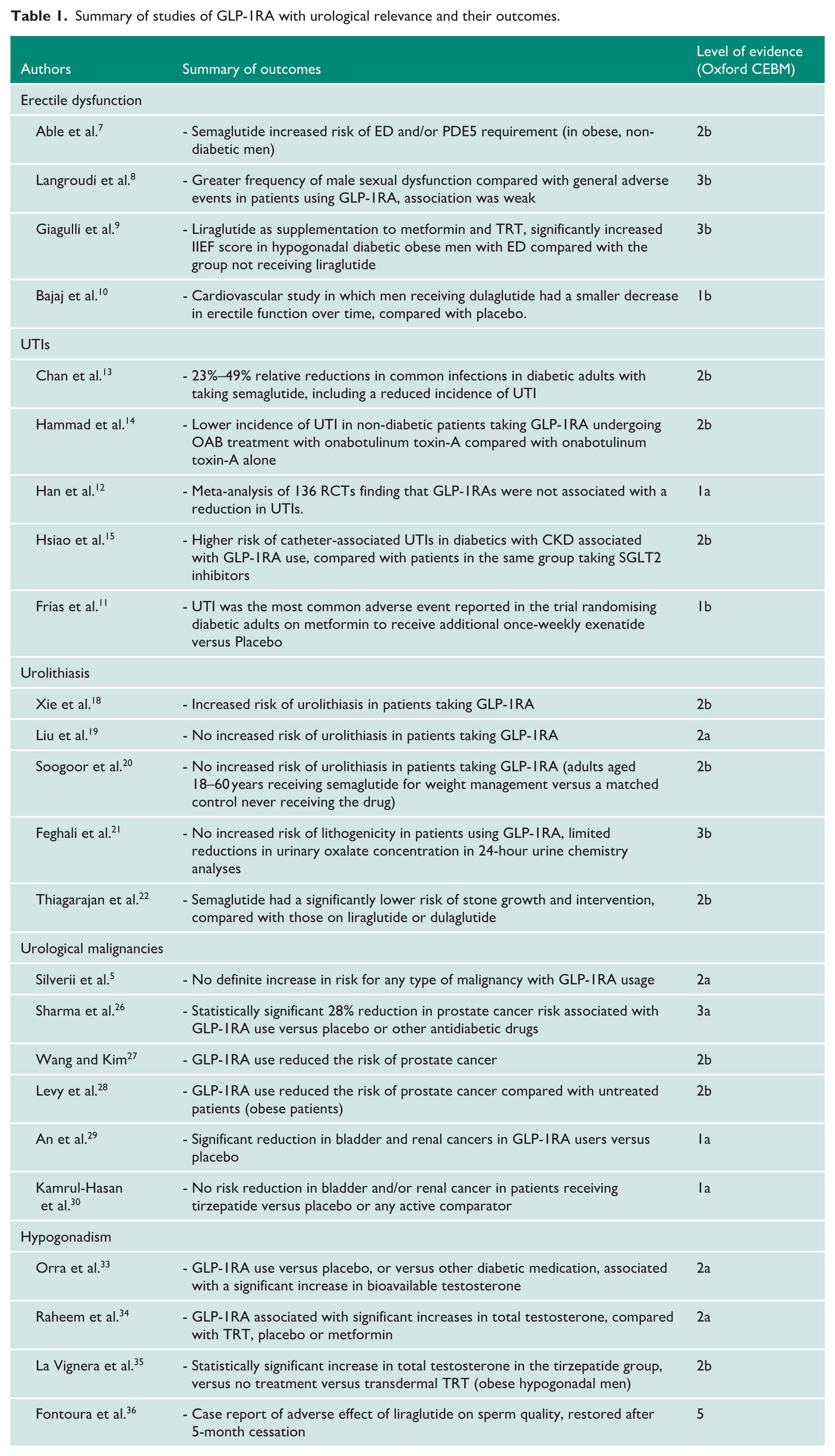
To date, no prospective RCT has been conducted regarding GLP-1RA with the primary outcome determined as evaluating any of ED, UTIs, urolithiasis, urological malignancies or hypogonadism as primary end-points.
Conclusion
The use of GLP-1RA is surging worldwide and thus becoming increasingly prevalent in the urologist’s daily practice.
There are potentially far-reaching urological benefits and side effects of GLP-1RA, with sequelae reported in common urological conditions such as ED, UTIs, urolithiasis, urological malignancies and hypogonadism.
Current evidence is predominantly based on retrospective studies, anecdotal reports, and small-scale studies with short follow-up timeframes. More research is required as these sequelae have not yet to date been evaluated by targeted high-powered clinical studies or RCTs – and currently, the long-term risks of these medications remain largely unknown.
Urologists should be aware of the implications of GLP-1RA in their clinical practice and remain vigilant regarding any urological benefits or drawbacks they observe in their patients who are concomitantly using GLP-1RA.
Footnotes
Acknowledgements
The authors would like to thank Flavia Donati for her assistance, guidance and support throughout this project.
Ethical considerations
None required.
Consent to participate
Patient consent was not applicable/required for the purposes of this study.
Contributorship
A.U. and J.D.B. researched literature and conceived the study. A.A. and L.M. were involved in manuscript production, referencing and fact-checking. A.U. and J.D.B. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Guarantor
J.D.B.