
Abstract
Objective:
To propose a surveillance approach for upper tract urothelial carcinoma (UTUC) recurrence in high-risk and very high-risk non-muscle invasive bladder cancer (HR NMIBC) patients.
Method:
Retrospective analysis in 2024 of 317 patients diagnosed with HR NMIBC in our centre between 2008 and 2018, including histology, CT urogram (CTU) frequency, radiation dose, UTUC recurrence, outcome, and risk factors for UTUC recurrence.
Results:
A total of 283 patients were included for analysis. Incidence of UTUC recurrence 5.7% (n = 16/283), with 3.5% (n = 10/283) undergoing nephroureterectomy. Mean time from initial diagnosis to UTUC recurrence is 5.2 years. At 5- and 10-year follow-up, UTUC incidence was 3.5% and 2.1%, respectively. No patients diagnosed with UTUC recurrence beyond 10 years. Patients underwent mean 2.2 surveillance CTU every 1.9 years, with 17.7 mSv mean radiation dose per scan. No significant increased risk of UTUC recurrence associated with carcinoma in situ (CIS) at diagnosis (χ2 = 0.006, p value = 0.94). Risk of UTUC recurrence significantly increased in patients with recurrent HR NMIBC (27%) versus those without (4%) (relative risk = 7.12, χ2 = 20.9, p value < 0.00001).
Conclusion:
Consider surgical fitness and HR NMIBC recurrence status when determining duration of surveillance for patients. We propose biennial CTU in patients fit for nephroureterectomy, continuing up to 10 years if recurrent HR NMIBC, or up to 5 years if recurrence-free.
Level of evidence:
2b – Retrospective cohort study
Introduction
The European Association of Urology (EAU) and the National Institute for Clinical Excellence (NICE) recommend the risk stratification of patients diagnosed with non-muscle invasive bladder cancer into low, intermediate, high, and very high-risk disease, in order to follow-up patients according to an appropriate protocol that reflects the risk of disease recurrence and progression associated with each risk category.1,2
The incidence of upper tract urothelial carcinoma (UTUC) recurrence in high and very high-risk non-muscle invasive bladder cancer (HR NMIBC) is 2.6–5.8%.3–5 Previous studies describe possible risk factors for UTUC recurrence, including carcinoma in situ (CIS) and multiple and recurrent HR NMIBC; 10-year UTUC recurrence rates are quoted as ranging from 2.8% for those with CIS 6 to 25% in patients with multiple and recurrent HR NMIBC. 7
Both the EAU and NICE guidelines for follow-up of NMIBC patients recommend bladder surveillance with flexible cystoscopy for HR NMIBC patients. However, NICE offers no published guidance on upper tract imaging follow-up, and EAU guidelines suggest an annual CT urogram (CTU) up to 5 years, followed by a biennial CTU up to 10 years; however, this is a weak recommendation. 1 At our centre, we perform biennial CTU surveillance for all patients diagnosed with HR NMIBC, or earlier if bladder recurrence is detected, if the patient is deemed fit for surgical management.
The objective of this study is to evaluate the incidence of UTUC recurrence during long-term follow-up of patients with HR NMIBC, to evaluate the radiation exposure of each surveillance CTU, and to identify risk factors for UTUC recurrence, in order to propose an appropriate upper tract surveillance approach which balances the risk of UTUC recurrence with the cumulative risk of radiation exposure.
Methods
This study is a retrospective cohort analysis. Patients diagnosed with HR NMIBC at our tertiary referral centre between 2008 and 2018 were added to a database by the bladder cancer team at time of diagnosis. Data on primary histology and patient demographics, including gender, age, and hospital number, were recorded. HR NMIBC was classified as any high-risk or very high-risk NMIBC – any G3 tumour, T1 tumour, or CIS on histological analysis – with diagnosis and risk stratification ratified by the bladder cancer multidisciplinary team (MDT).
Following identification of the dataset, data was transferred to a Microsoft Excel spreadsheet for further retrospective data collection and analysis. Data collection occurred between January and August 2024 using the trust’s electronic patient record and radiology systems. The following data was collected: age at diagnosis; WHO performance status; cross-checking of primary histological diagnosis; dates, number, and frequency of initial and surveillance CTUs; presence of UTUC recurrence on CTU; radiation dose of each CTU; length of follow-up; incidence of recurrence and/or progression to muscle invasive bladder cancer (MIBC); and survival data. Statistical analysis was performed using the functions within Microsoft Excel.
Results
A total of 317 patients were diagnosed with HR NMIBC between 2008 and 2018, of which 34 were excluded from analysis: 11 patients had been incorrectly diagnosed with HR NMIBC, 9 patients were unsuitable for CTU due to renal dysfunction or poor performance status, 9 patients were found to have UTUC as a primary diagnosis, and 5 were lost to follow-up.
Demographics
A total of 283 patients were included for analysis, of which 81% (n = 229/283) were male, with a mean age at diagnosis of 72 years (SD = 10.4 years). Eighty-five percent of the cohort had a recorded WHO performance status of 0, 1, or 2 (n = 240/283).
Histology
The distribution of histological subtypes is shown in Figure 1. The commonest histological subtype was G3T1 ± CIS (53%, n = 149/283), followed by G3Ta ± CIS (35%, n = 99/283). CIS was present (either G3Ta + CIS, G3T1 + CIS, or CIS alone) at diagnosis in 34% of the cohort (n = 95/283).
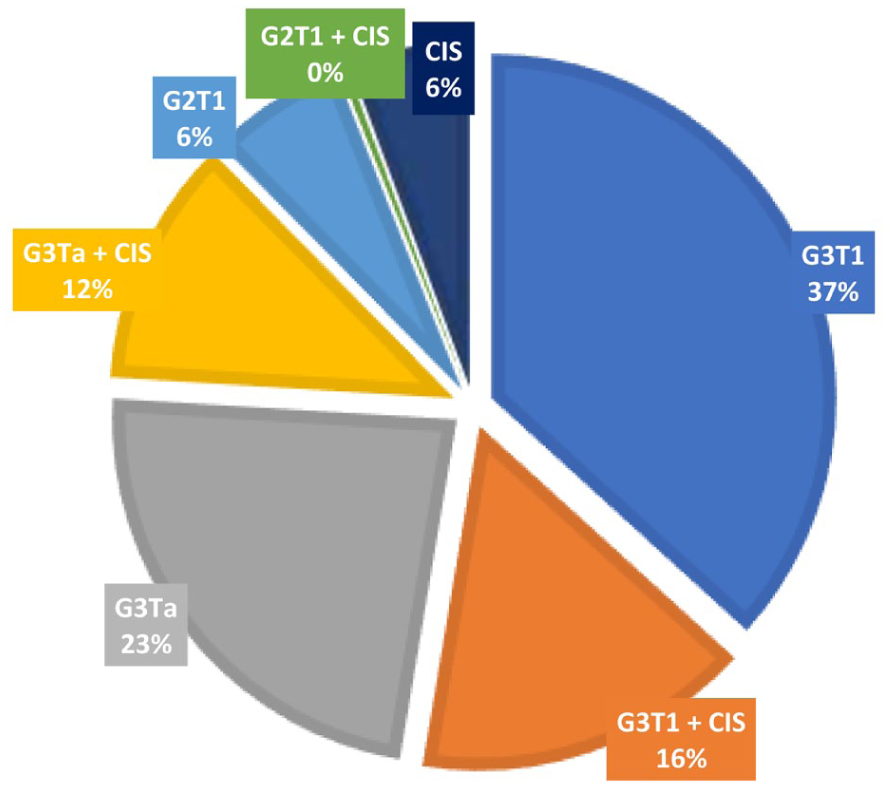
Graph showing the distribution of histological subtypes for patients diagnosed with HR NMIBC.
Follow-up and CTU surveillance
The mean and median follow-up time was 7.2 years from diagnosis (SD = 2.7 years), and 11% (n = 32/283) were followed up for ⩾ 10 years. A total of 629 CTUs were performed across the cohort, with patients undergoing an average of 2.2 surveillance CTUs, with a mean interval time between scans of 1.9 years (SD = 0.26 years).
CTU radiation
Effective radiation doses were obtained for 76% of CTUs performed (n = 478/629). The mean effective radiation dose per CTU was 17.7 mSv (SD = 10 mSv).
UTUC recurrence
Sixteen patients (5.7%) developed UTUC recurrence: 15 were detected on surveillance CTU, and 1 case was diagnosed intra-operatively during radical cystectomy for recurrent HR NMIBC. Ten patients (3.5%) underwent radical nephroureterectomy. Of the remaining 6 patients, 2 were managed with radiological surveillance and endoscopic ablation of UTUC recurrence, 1 patient died from unrelated causes shortly after diagnosis, and 3 patients were managed by best supportive care: 2 were deemed unfit for surgical management, and 1 was diagnosed with metastatic disease. The mean time from initial diagnosis to UTUC recurrence was 5.2 years (SD = 1.9 years). The incidence of UTUC recurrence was 3.5% at 5 years (n = 10/283) and 2.1% at 10 years (n = 6/283). No patients were diagnosed with UTUC recurrence beyond 10 years of follow-up.
Risk factors for UTUC recurrence
There was no significant increased risk of UTUC recurrence associated with presence of CIS at diagnosis (χ2 = 0.006, p value = 0.94). The risk of UTUC recurrence was significantly increased in patients who developed multiple and recurrent HR NMIBC (27%) versus those who did not (4%) (relative risk = 7.12, χ2 = 20.9, p value < 0.00001).
Incidence of HR NMIBC recurrence/progression to MIBC
Fourteen percent of patients (n = 40/283) developed either recurrent HR NMIBC (8%, n = 22) or progressed to MIBC (6%, n = 18) following intravesical treatment, on average 4.2 years (SD = 2.8 years) following initial HR NMIBC diagnosis. Nine percent (n = 25/283) subsequently received either radical cystectomy or chemoradiotherapy.
Survival
Patient survival from initial HR NMIBC diagnosis is shown in the Kaplan–Meier survival graph in Figure 2. Overall survival at 5 and 10 years is 81% and 56%, respectively.
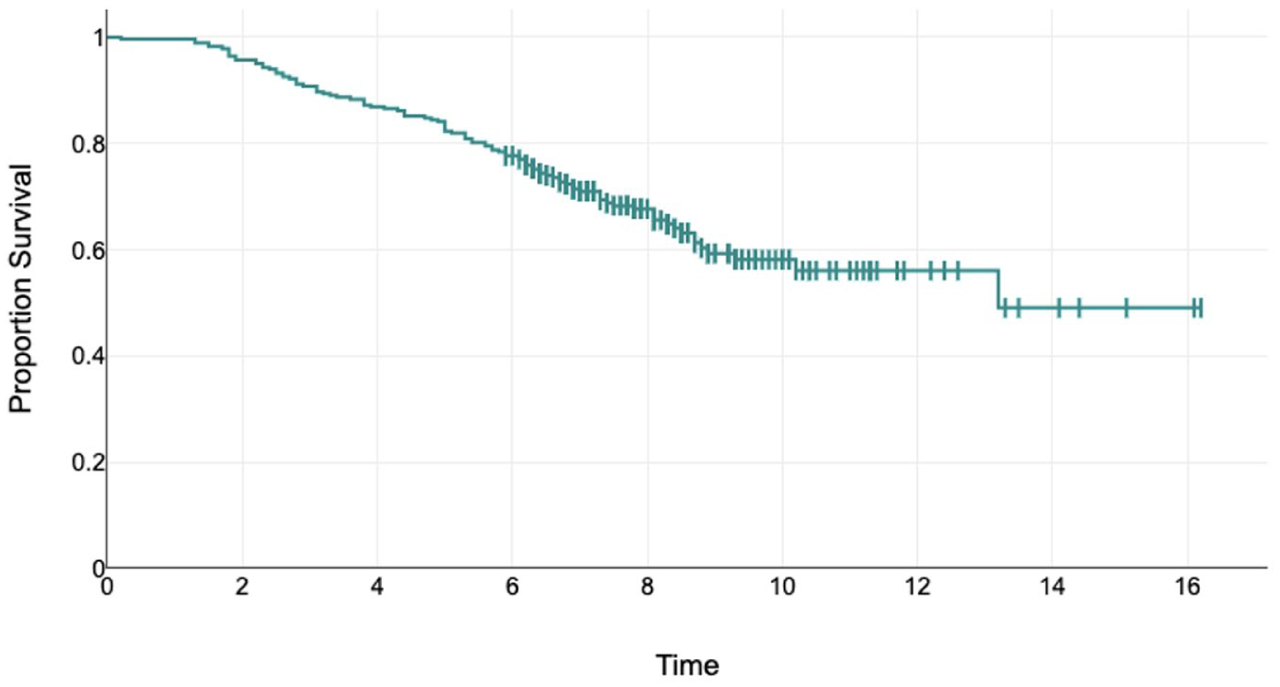
Kaplan–Meier survival analysis showing patient survival from initial HR NMIBC diagnosis, with censoring at last follow-up.
Discussion
The observed incidence of UTUC recurrence in our study of 5.7% lies within the top end of the range of previously reported rates (2.6–5.8%).3–5 The majority of UTUC recurrence cases in our study were detected on CTU surveillance (94%), and the single case that was missed on imaging was detected intra-operatively during radical cystectomy for management of recurrent HR NMIBC. CTU is widely accepted in practice as yielding the highest diagnostic accuracy in the detection of UTUC.1,2,8 Symptoms, primarily any history of visible haematuria, may aid clinical decision-making regarding the necessity of additional or early investigations for cancer recurrence. Our data records lacked standardised reporting of visible haematuria, thus symptomatology has not been included within our analysis or follow-up proposal. A similar study by Nishimura et al. 3 reported only 1 out of 19 of patients with UTUC recurrence was diagnosed by the presence of symptoms, with the majority diagnosed on routine CTU surveillance. Nevertheless, we now routinely record the onset of any new symptoms, as this may trigger additional investigation outside of a patient’s established surveillance schedule.
EAU and NICE guidelines recommend lifelong follow-up for HR NMIBC patients.1,2 A pragmatic approach to long-term upper tract surveillance for these patients would consider the risk of UTUC recurrence, the patient’s fitness for intervention if UTUC recurrence is diagnosed, the cumulative radiation risk of CTU, and the financial and resource burden of long-term surveillance within the constraints of the NHS – the latter of which requires detailed economic analysis and is beyond the scope of this study.
The mean effective dose per CTU of 17.7 mSv is approximately equivalent to 6 years of background radiation, with an estimated additional 1 in 2000 lifetime malignancy risk per scan. 9 If upper tract surveillance is not standardised, variations in practice between patients, centres and regions can lead to significant health inequalities from the accumulation of significant and potentially unnecessary radiation exposure through over-investigation, or, conversely, miss potentially treatable disease from under-investigation. Our practice is to perform a CTU for upper tract surveillance every 2 years, or earlier if recurrence is suspected. All patients in our study with UTUC recurrence had potentially treatable disease, except one: in this case, metastatic disease was diagnosed following an interval of 4 years between surveillance scans due to the Covid pandemic. We propose that surveillance CTU every 2 years, in the absence of symptoms, is a reasonable interval for the detection of UTUC recurrence, which aligns approximately with EAU guidance (annual CT for 5 years, then biennial CT up to 10 years). 1
There is a paucity in literature of >10-year follow-up studies for patients with HR NMIBC. Our long-term follow-up data, with a mean follow-up time of 7.2 years, is a key strength of this study. In light of the observation that UTUC recurrence did not occur in any patients beyond 10 years of follow-up, we recommend that upper tract surveillance should continue up to 10 years following initial HR NMIBC diagnosis (if fit for surgical management). This can be further risk-stratified according to HR NMIBC recurrence status; those who develop recurrent, high-volume HR NMIBC are at significantly higher risk of developing UTUC recurrence, thus reasonably should be followed up to 10 years. For those who are recurrence-free, we propose continuing upper tract surveillance up to 5 years following initial diagnosis: only six patients (2.1%) were diagnosed with UTUC recurrence between 5 and 10 years, all of which had developed recurrent HR NMIBC. Interestingly, we did not observe a statistically significant increased risk of UTUC recurrence with the presence of CIS, as has been reported elsewhere. 10 Figure 3 summarises our approach for upper tract surveillance in HR NMIBC patients.
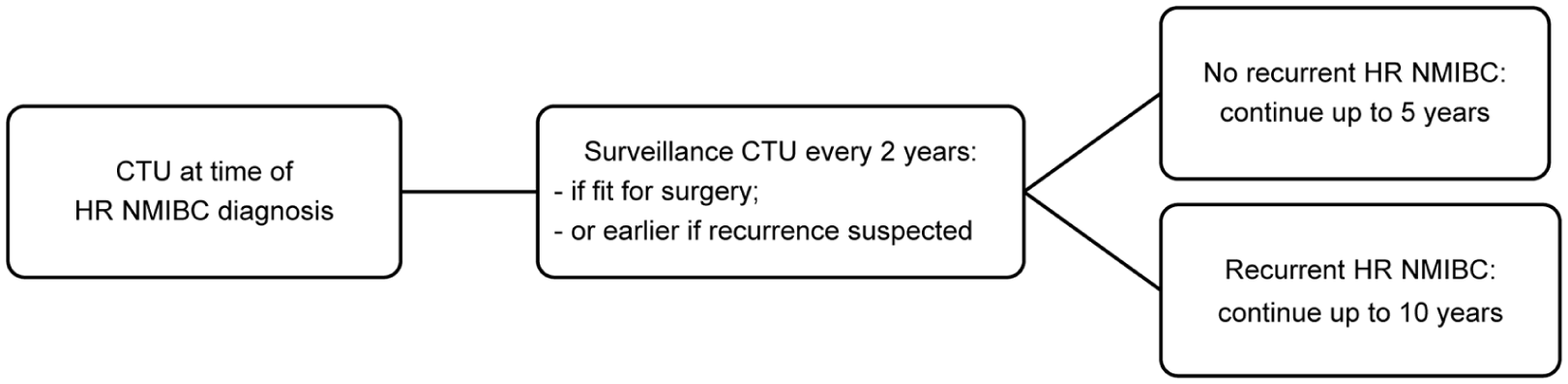
Surveillance approach for detecting UTUC recurrence in patients with HR NMIBC.
The main limitations of this study include its retrospective nature, the relatively small numbers of UTUC recurrence events, changes in record-keeping, and developments in managing NMIBC. There have been several system changes in our centre since 2008, affecting the way data is recorded (i.e. the transition from paper to electronic records, with data recorded across multiple systems), meaning that factors such as symptoms, tumour size and location, and intravesical BCG schedules could not be accurately collected for all patients. In addition, along with advances in managing NMIBC, new guidelines for data recording have been introduced to practice during the follow-up period, for example, quality control indicators for transurethral resection of bladder tumour (TURBT); not only has this improved the quality of data available for collection, but also reduces the risk of recurrence and progression to MIBC at initial TURBT,11,12 thus potentially leading to a lower incidence of UTUC recurrence in these patients. Further prospective studies are therefore needed to identify up-to-date UTUC recurrence rates following these advancements in NMIBC management, as well as to identify and/or validate any new or existing risk factors for UTUC recurrence in order to refine risk stratification tools and shape upper tract surveillance protocols in the future.
Conclusion
UTUC recurrence rate in HR NMIBC patients is 5.7%, which is comparable to existing studies. No new UTUC recurrence was seen beyond 10 years of follow-up. Fitness for surgery and high-risk bladder recurrence status should be considered when determining duration of CTU surveillance for HR NMIBC patients. We propose a surveillance CTU every 2 years in patients fit for nephroureterectomy, continuing up to 10 years in those who develop high-risk bladder recurrence, or up to 5 years if recurrence-free.
Footnotes
Acknowledgements
We would like to thank our colleagues in the Radiology department at Southmead Hospital for their assistance in this research.
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
H.B. and K.W. conceived the study. R.S., J.M. and Y.P.P.L. were involved in data collection and analysis. R.S. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and analysed for this study are available from the corresponding author on request.
Informed consent
Not applicable.
Guarantors
R.S. and H.B.