
Abstract
Background:
Active surveillance (AS) is an established management strategy for patients with low- and favorable intermediate-risk prostate cancer (PCa). Accurately distinguishing indolent from aggressive disease and identifying progression during follow-up remain significant clinical challenges. Artificial intelligence (AI) has appeared as a promising approach to enhance risk stratification and support clinical decision-making. Our aim was to evaluate the role of AI-based decision support systems in patient selection and monitoring during AS for PCa, as well as their potential to guide timely transition to definitive treatment.
Methods:
A scoping review was conducted in accordance with Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines. The review protocol was prospectively registered in PROSPERO (CRD420261358519). Literature searches in PubMed and Scopus were performed, applying filters for English-language studies published within the past 5 years. Of 133 records identified, 24 studies met the inclusion criteria after screening and eligibility assessment.
Results:
Most included studies were retrospective and used machine learning (ML) or deep learning (DL) techniques on clinical, radiological, and histopathological data. AI models demonstrated stronger predictive performance than traditional statistical methods, with reported area under the curve (AUC) values ranging from 0.74 to 0.96. Radiomics-based models derived from magnetic resonance imaging (MRI) facilitated non-invasive characterization of tumor aggressiveness, while DL algorithms applied to biopsy whole-slide images improved grading accuracy and progression prediction. Multimodal models that integrated heterogeneous data sources consistently outperformed single-modality approaches. Finally, longitudinal models including serial prostate-specific antigen (PSA) measurements and imaging data enabled dynamic risk assessment and customized monitoring during AS.
Conclusion:
AI-based models show considerable potential to improve patient selection and predict progression in AS for PCa, potentially reducing overtreatment and unnecessary biopsies. However, current evidence is limited by retrospective study designs, lack of external validation, and variability in AS protocols. Prospective multicenter studies and enhanced model explainability are necessary before routine clinical implementation.
Level of evidence:
Not applicable.
Keywords
Introduction
Prostate cancer (PCa) is one of the most diagnosed malignancies in men worldwide. 1 Its marked clinical heterogeneity makes management challenging. The disease can behave indolently or aggressively, creating an urgent need for strategies that separate patients who need intervention from those who can be safely observed. Active surveillance (AS) has become a leading approach for patients with low-risk and some favorable intermediate-risk PCa. This strategy seeks to balance oncological safety with minimizing overtreatment.
Although AS is widely used, clinicians must accurately identify which patients can be safely monitored and which may require earlier treatment due to the risk of progression. Current protocols rely on several tools: digital rectal examinations (DREs), prostate-specific antigen (PSA) and PSA density (PSAd) measurements, multiparametric magnetic resonance imaging (mpMRI), and serial prostate biopsies. 2 These tools may be essential for monitoring, but each has significant limitations. Repeated prostate biopsies are associated with risks, such as bleeding and infections that could require hospitalization. Magnetic resonance imaging (MRI) scans are costly and may not be widely available. In addition, common clinical measures and imaging may not fully capture the aggressiveness of the malignancy, leading to misclassification or delayed detection of cancer progression.
In this context, artificial intelligence (AI) has rapidly emerged as a promising tool in medical research and clinical practice. Unlike conventional methods, AI, through machine learning (ML), deep learning (DL), and radiomics, has the potential to uncover subtle, complex patterns in clinical and imaging data that might be overlooked by human observers. 3 This unique analytical capability enables more refined risk stratification and supports clinicians by synthesizing multifaceted data sources to inform decision-making. AI-based models may thus uniquely enhance the identification of suitable candidates for AS and the early detection of disease progression.
This scoping review examines whether AI-based decision support systems can improve patient selection and monitoring during AS for PCa. In addition, it discusses their potential to guide timely moves from surveillance to surgery.
Materials and methods
Two independent reviewers (D.D. and N.A.) performed the literature search through the PubMed and Scopus databases. The review protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD420261358519). The search strategy included both Medical Subjects Headings (MeSH) and free-text terms, using the following keywords: “prostatic neoplasms [MeSH],” “prostate cancer,” “prostate carcinoma,” “active surveillance,” “active monitoring,” “artificial intelligence [MeSH],” “machine learning [MeSH],” “deep learning,” “radiomics,” “risk stratification,” and “predictive modeling.” The search was conducted in accordance with Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines. 4 Discrepancies were resolved after consensus with the senior author (T.T.). A total of 133 records were identified. We selected English-written studies published during the last 5 years. Specifically, 63 records were identified in PubMed and 70 in Scopus. Eighteen duplicate records were removed. During the screening process, 89 records were excluded; 53 records were not original articles (reviews, notes, letters, editorials), 20 records were excluded as irrelevant to AI, 13 to AS, and 3 to PCa. A total of 26 reports were assessed for eligibility. After the eligibility assessment and exclusions (two reports were excluded; one was irrelevant to AS and one was published over 5 years ago), 24 studies were included in the review. Figure 1 shows details of the selection process. Due to study heterogeneity and the nonstandardized quality appraisal, a narrative synthesis was performed.
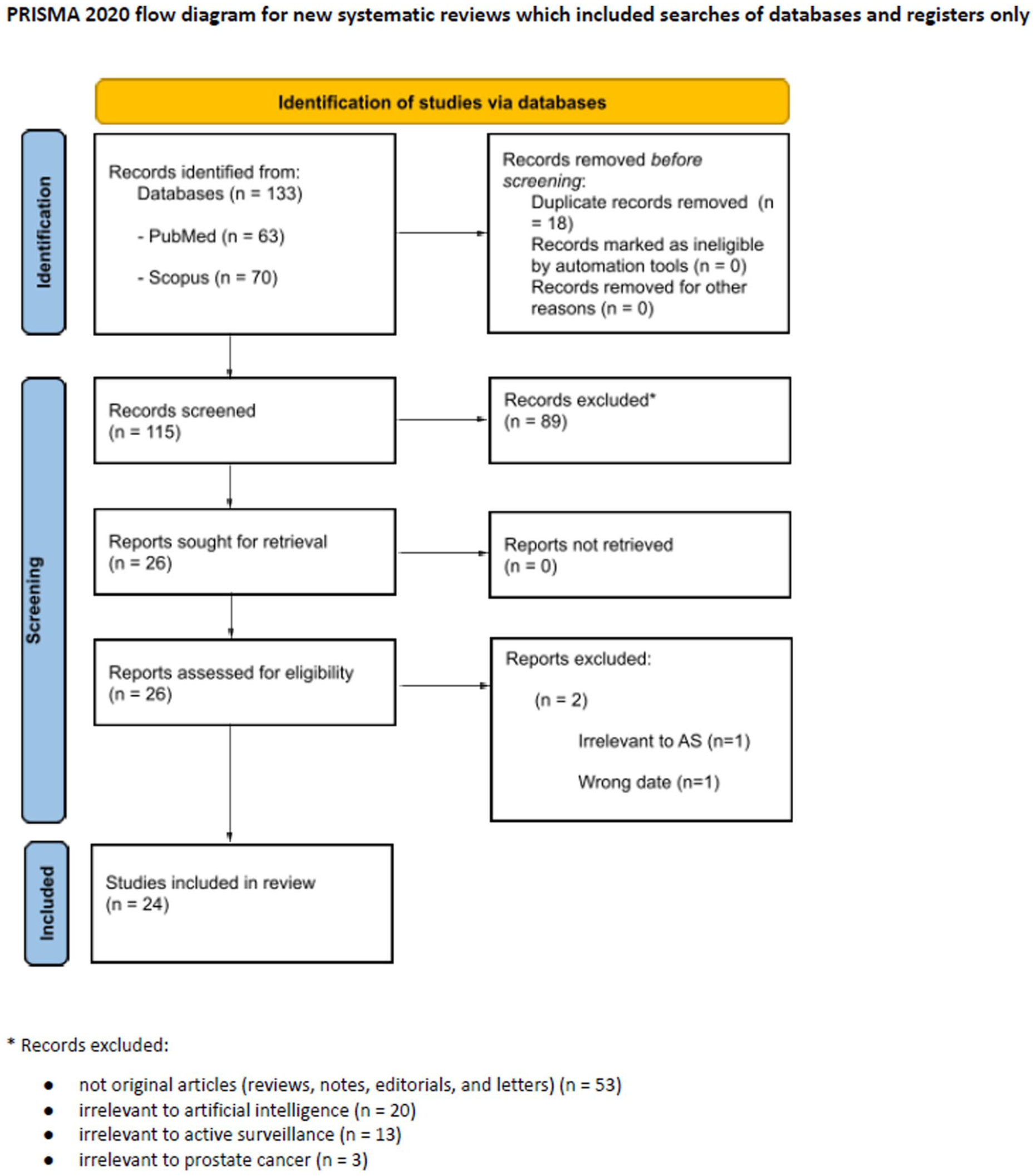
Literature search flowchart according to PRISMA 2020 guideline.
Results
Twenty-four studies met our inclusion criteria. In most studies, AI models were evaluated on retrospective cohorts of patients with PCa managed on AS.5,6,7–12,13,14 Cohort sizes varied from 42 15 to 1422 patients. 16 Predictive models for PCa progression and risk stratification were developed using various ML techniques, most commonly random forests, support vector machines, and decision trees (DTs),6,7,11,13,16–22 as well as DL models, including convolutional and recurrent neural networks.5,9,19,23–27 Long short-term memory8,12,14 and temporal outcome-oriented clustering methods 10 were implemented in prospective longitudinal models for predicting progression. Data sources varied across studies and included clinical variables (PSA measurements, PSAd, DRE results, etc.),6,7,10,12–14,16,17,19,21,22,25 radiological features extracted from bi- and multiparametric MRI scans,7–15,16,18–20,22,24,27,28 and histopathological data.5–7,10,17,21,23,25,26 Model performance was mostly reported using the area under the receiver operating characteristic curve (AUC), sensitivity, and specificity.
AI for selection of patients eligible for active surveillance
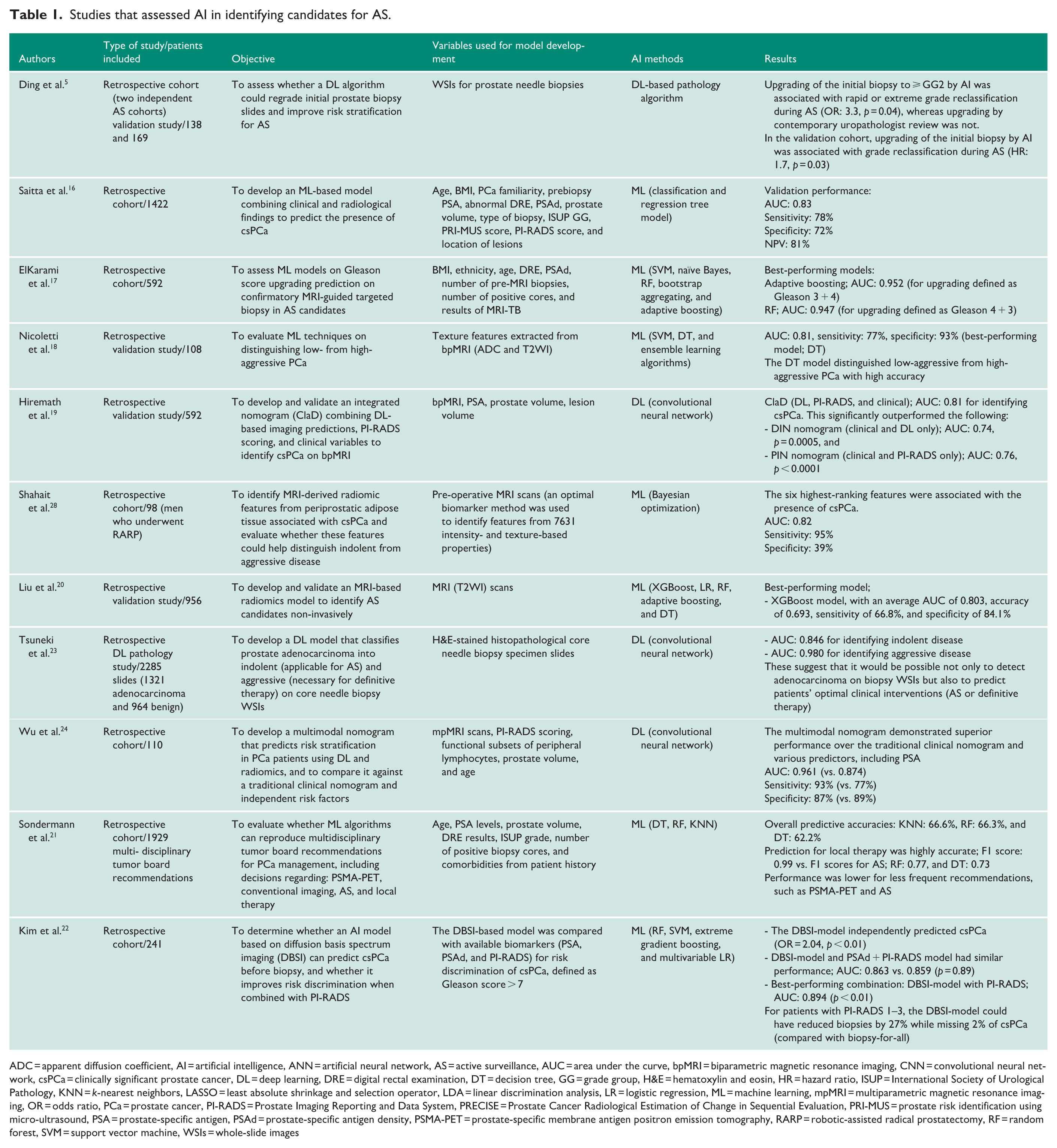
The first major domain, presented in Table 1, included studies that assessed the role of AI in improving risk stratification and identifying patients who could be managed on AS. These studies aimed to distinguish patients with indolent disease from those harboring clinically significant or more aggressive PCa.
Studies that assessed AI in identifying candidates for AS.
ADC = apparent diffusion coefficient, AI = artificial intelligence, ANN = artificial neural network, AS = active surveillance, AUC = area under the curve, bpMRI = biparametric magnetic resonance imaging, CNN = convolutional neural network, csPCa = clinically significant prostate cancer, DL = deep learning, DRE = digital rectal examination, DT = decision tree, GG = grade group, H&E = hematoxylin and eosin, HR = hazard ratio, ISUP = International Society of Urological Pathology, KNN = k-nearest neighbors, LASSO = least absolute shrinkage and selection operator, LDA = linear discrimination analysis, LR = logistic regression, ML = machine learning, mpMRI = multiparametric magnetic resonance imaging, OR = odds ratio, PCa = prostate cancer, PI-RADS = Prostate Imaging Reporting and Data System, PRECISE = Prostate Cancer Radiological Estimation of Change in Sequential Evaluation, PRI-MUS = prostate risk identification using micro-ultrasound, PSA = prostate-specific antigen, PSAd = prostate-specific antigen density, PSMA-PET = prostate-specific membrane antigen positron emission tomography, RARP = robotic-assisted radical prostatectomy, RF = random forest, SVM = support vector machine, WSIs = whole-slide images
Several studies focused on baseline reclassification using clinical variables and biopsy-derived information. In patients undergoing confirmatory MRI-targeted biopsy, ElKarami et al. 17 showed that ML models could accurately predict upgrading, with models achieving AUC values up to 0.952. Similarly, a DL pathology model applied to initial biopsy slides in two independent AS cohorts improved baseline risk stratification by identifying patients initially classified as GG 1 who were more likely to undergo rapid or extreme grade reclassification. 5 Tsuneki et al. 23 also demonstrated that DL applied to whole-slide images (WSIs) could distinguish indolent from aggressive prostate adenocarcinoma with high discriminative performance (AUC values of 0.864 for indolent and 0.980 for aggressive disease). Regarding clinical decision support systems and recommendations, Sondermann et al. evaluated ML algorithms on reproducing multidisciplinary tumor board recommendations for PCa management (including AS) using clinicopathological variables. However, the model showed moderate performance in reproducing AS recommendations compared with its performance in predictions regarding local therapy or conventional imaging. 21
Several of the included studies have tested radiomics models derived from prostate MRI scans. Radiomics analysis enables the extraction of multi-dimensional quantitative imaging features that can reflect tumor heterogeneity and biological aggressiveness. Multiple studies have developed ML models using radiomic features derived from biparametric or multiparametric MRI sequences, such as T2-weighted imaging and apparent diffusion coefficient maps.18,20,22,28 These radiomics-based approaches have demonstrated promising diagnostic performance in distinguishing indolent from aggressive PCa, thereby supporting non-invasive identification of patients suitable for AS. For example, Nicoletti et al. 18 showed that texture-based radiomic features extracted from bpMRI were used to train classifiers that accurately distinguished low-aggressive from high-aggressive disease, achieving 77% sensitivity and 93% specificity with a DT model. Shahait et al. 28 explored radiomic features extracted from periprostatic adipose tissue, demonstrating that non-tumoral biomarkers may also help discriminate csPCa. In another study, Liu et al. 20 developed a radiomics model using various ML techniques to identify AS candidates, with the best-performing model achieving an average AUC of 0.803, showing potential for non-invasive identification.
Multimodal AI models combining imaging and clinical variables also showed encouraging results and tended to outperform traditional risk stratification tools. Hiremath et al. 19 developed a nomogram that combined DL-based imaging predictions, PI-RADS scoring, and clinical parameters, demonstrating superior performance compared with models based on fewer modalities. Wu et al. 24 similarly reported stronger performance (AUC: 0.961) of a multimodal nomogram incorporating mpMRI, peripheral lymphocyte subsets, and clinical variables compared with a traditional clinical nomogram (AUC: 0.874) for risk classification. Saitta et al. 16 integrated micro-ultrasound features with other clinical, pathological, and imaging data to develop an ML-based model for predicting csPCa. Overall, the proposed models showed statistically significant improvements in predictive performance, achieving AUC values ranging from 0.81 to 0.96.16,19,24 Kim et al. 22 showed that combining a diffusion basis spectrum imaging model with the PI-RADS score accurately detected csPCa (AUC: 0.894), with the potential to reduce biopsies by up to 27% in patients with a PI-RADS score of 1–3, while missing 2% of csPCa. These findings underscore the importance of integrating clinical, radiological, and pathological features into predictive models, as this approach achieves higher accuracy and could pave the way for more robust risk stratification tools.
Taken together, these studies suggest that baseline assessment using AI algorithms may improve selection for AS by enhancing non-invasive identification of patients with low- or favorable intermediate-risk disease.
AI for PCa progression prediction and exiting active surveillance
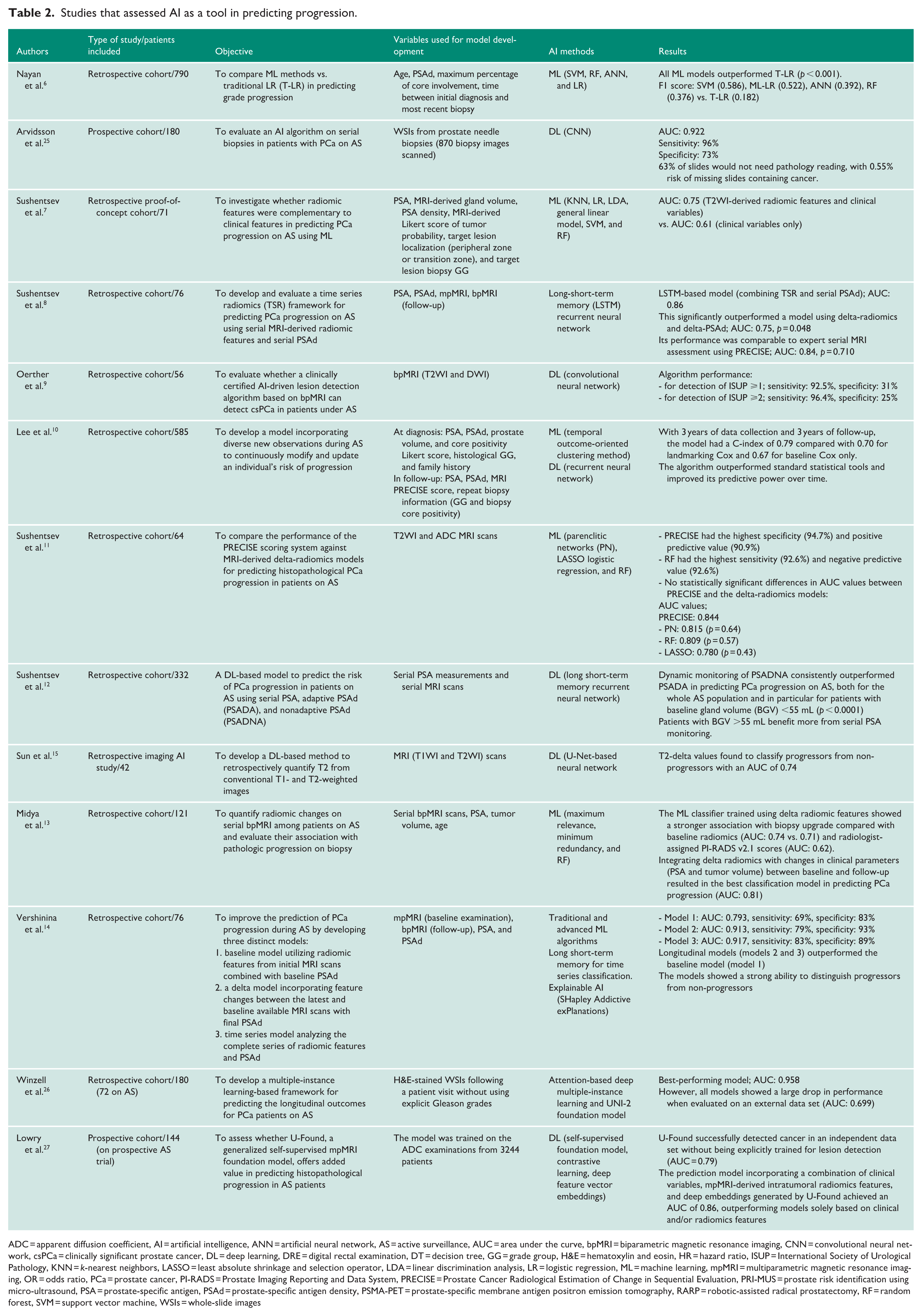
AI approaches have been increasingly investigated to predict disease progression in patients undergoing AS for PCa, with the aim of identifying patients at higher risk of pathological upgrading or clinical progression who may require definitive treatment rather than continued surveillance. The second major domain of our review, presented in Table 2, comprised studies that assessed AI as a tool for predicting disease progression in AS.
Studies that assessed AI as a tool in predicting progression.
ADC = apparent diffusion coefficient, AI = artificial intelligence, ANN = artificial neural network, AS = active surveillance, AUC = area under the curve, bpMRI = biparametric magnetic resonance imaging, CNN = convolutional neural network, csPCa = clinically significant prostate cancer, DL = deep learning, DRE = digital rectal examination, DT = decision tree, GG = grade group, H&E = hematoxylin and eosin, HR = hazard ratio, ISUP = International Society of Urological Pathology, KNN = k-nearest neighbors, LASSO = least absolute shrinkage and selection operator, LDA = linear discrimination analysis, LR = logistic regression, ML = machine learning, mpMRI = multiparametric magnetic resonance imaging, OR = odds ratio, PCa = prostate cancer, PI-RADS = Prostate Imaging Reporting and Data System, PRECISE = Prostate Cancer Radiological Estimation of Change in Sequential Evaluation, PRI-MUS = prostate risk identification using micro-ultrasound, PSA = prostate-specific antigen, PSAd = prostate-specific antigen density, PSMA-PET = prostate-specific membrane antigen positron emission tomography, RARP = robotic-assisted radical prostatectomy, RF = random forest, SVM = support vector machine, WSIs = whole-slide images
ML models based on clinical variables have demonstrated superior performance compared with traditional statistical methods. A retrospective study involving 790 patients undergoing AS showed that several ML classifiers (achieving F1 scores ranging from 0.392 to 0.586) significantly outperformed traditional logistic regression (F1 score: 0.186, p < 0.001) in predicting grade progression. 6 Likewise, Sushentsev et al. 7 demonstrated that adding MRI-derived radiomic features to standard clinical parameters improved baseline prediction of progression (AUC improved from 0.61 to 0.75).
Lowry et al. assessed a generalized self-supervised mpMRI foundation model to predict progression in 144 patients in a prospective AS trial. The predictive model achieved an AUC of 0.86 when combined with clinical variables and intratumoral radiomics, outperforming models that relied solely on clinical and/or radiomics features (AUC values ranging from 0.71 to 0.82). 27
Studies using serial MRI and delta-radiomics have also been used to predict disease progression in patients already enrolled in AS programs. These models aim to detect subtle imaging characteristics associated with biologically aggressive disease and to identify patients at higher risk of progression while on AS. DL-based methods, including long short-term recurrent neural networks, were implemented in four studies8,9,14,15 to retrospectively detect progression in patients under AS. Sun et al. 15 introduced a DL approach to quantify changes in T2 signal intensity between serial MRI scans, achieving an AUC of 0.74 for distinguishing progressors from non-progressors. MRI-derived delta-radiomics, based on ML techniques, demonstrated performance comparable to that of the PRECISE scoring system, although PRECISE showed the highest specificity of 94.7% and positive predictive value (90.9%). 11 In another study, Sushentsev et al. 8 developed a time series radiomics model integrating serial MRI features and serial PSAd measurements (AUC: 0.86), which outperformed conventional delta-radiomics (AUC: 0.75) and performed comparably to expert PRECISE scoring assessment (AUC: 0.84). Similarly, Midya et al. 13 showed that delta-radiomics from serial MRI scans in conjunction with changes in clinical parameters (PSA levels and tumor volume) can improve progression risk prediction, as AUC improved from 0.62 and 0.72, for radiologist-assigned PI-RADS scoring and baseline radiomics, respectively, to 0.74 for the ML-based delta-radiomics model. In this context, Vershinina et al. 14 also demonstrated improvements from a baseline radiomics model (AUC: 0.793) to delta radiomics (AUC: 0.913) and time series models (AUC: 0.917), with the longitudinal models achieving a greater ability to distinguish progressors from non-progressors than the baseline model. In addition, convolutional neural network–based lesion detection algorithms applied to bpMRI demonstrated high sensitivity (92.5% for International Society of Urological Pathology (ISUP) 1 detection and 96.4% for ISUP 2) for detecting clinically significant disease progression during AS, although specificity remained relatively low (31.5% for ISUP 1 detection and 25% for ISUP 2). 9
A long short-term recurrent neural network was also used to evaluate serial PSAd in predicting disease progression risk in AS patients. 12 Specifically, Sushentsev et al. found that nonadaptive PSAd outperformed adaptive PSAd and serial PSA for progression prediction, particularly in men with prostate glands below 55 mL.
Lee et al. evaluated a DL-based individualized model incorporating new clinical, radiological, and histopathological findings in AS. The model outperformed standard statistical tools (C-index of 0.79, compared to 0.70 for landmarking Cox and 0.67 for baseline Cox) and improved its predictive power over time. 10 Longitudinal models operate on real-time data, enabling a more personalized approach during follow-up and supporting decision-making about whether to remain on AS or switch to radical treatment.
AI models applied to histopathological whole-slide images (WSIs) have shown particularly high predictive performance. Arvidsson et al. 25 developed a convolutional neural network model applied to biopsy slide images from a prospective cohort of AS patients, achieving an AUC of 0.922, with 96% sensitivity and 73% specificity for identifying patients likely to fail AS, thus reducing by almost two-thirds the number of slides requiring pathologist review, while maintaining a 0.55% risk of missing slides containing cancer. Winzell et al. used WSIs (without explicit Gleason scores) and multiple-instance learning to predict longitudinal outcomes, achieving an AUC of 0.958 with the best-performing model. However, all models showed a large drop in performance (AUC: 0.699) when evaluated on an external data set. 26
Overall, these studies suggest that AI models may enhance decision-making during AS through improved ability to predict disease progression and longitudinal monitoring. Notably, across the studies, models incorporating longitudinal or multimodal data consistently outperformed those based on single baseline measurements.
Discussion
ML is a discipline within AI that focuses on developing algorithms capable of representing patterns in data. Unlike classical programming, where algorithms are explicitly coded using predefined features, ML utilizes subsets of data to generate algorithms that can employ novel or distinct combinations of features and weights, often extending beyond those established by first principles. 29 The subset of ML techniques that use deep neural networks (DNNs) is called DL. 30
AS is a management strategy that involves closely monitoring a patient’s condition without giving immediate treatment, intervening only if the disease shows signs of progression. 31 AS has been established as an acceptable management strategy for patients with low- and favorable intermediate-risk PCa. However, balancing oncological safety against the risk of overtreatment remains a challenge in urology, particularly for appropriate patient selection.1,32 A proportion of patients initially labeled as low-risk may hide more aggressive disease that becomes apparent during follow-up. Current clinical tools included in AS protocols (PSA, mpMRI, and systematic biopsies) offer valuable information but are not always able to distinguish sufficiently indolent PCa from clinically significant PCa. In this context, AI offers the opportunity to integrate large volumes of heterogeneous clinical data to detect and identify complex patterns that are not always discernible through conventional methods. 33
In this work, we summarized the current literature on the role of AI in decision support for patients with PCa managed under AS. The results suggest that AI-based models may contribute to two critical aspects of AS management: identifying appropriate candidates for AS and predicting disease progression that requires radical treatment. Throughout the studies, ML and DL techniques were applied to a wide range of data sources, including clinical variables, imaging-derived features, and histopathological information. Overall, the results highlighted AI’s potential to improve risk stratification and personalize surveillance strategies in PCa.
When selecting patients eligible for AS, risk stratification is based on PSA levels, biopsy findings, and clinical staging, but these traditional tools may not fully capture tumor heterogeneity. Several studies in this review described ML models that integrated clinical variables, MRI-derived radiomics, biopsy-related data, or combinations thereof, improving the detection of csPCa.5,16–24,28 In particular, imaging-based models that utilized data from bi- or multiparametric MRI scans18–20,22,24,28 had been proposed as a non-invasive diagnostic tool to stratify patients into distinct risk categories for PCa, thereby helping to avoid unnecessary biopsies and identify patients who might be candidates for AS.
Regarding disease progression prediction during AS, several studies have proposed AI-based models that assessed progression likelihood using clinical, imaging, and pathological data.6–15,25–27 Identifying patients at higher risk of progression is essential for determining when to discontinue AS to pursue definitive treatment. Notably, DL algorithms showed promising results when longitudinal data were incorporated, enabling the use of real-time data and the individualization of follow-up strategies.
Another significant aspect is the development of multimodal ML-based models that incorporate data from clinical parameters, imaging-derived features, and histopathological findings. Multimodal models significantly outperformed traditional statistical models and ML models that used only clinical or radiological information. These results suggest that the complex biological behavior of PCa is more accurately reflected when all available data are incorporated during predictive model development. As illustrated in Figure 2, by combining heterogeneous data sources and incorporating temporal changes, ML models could offer dynamic and personalized risk stratification during AS.
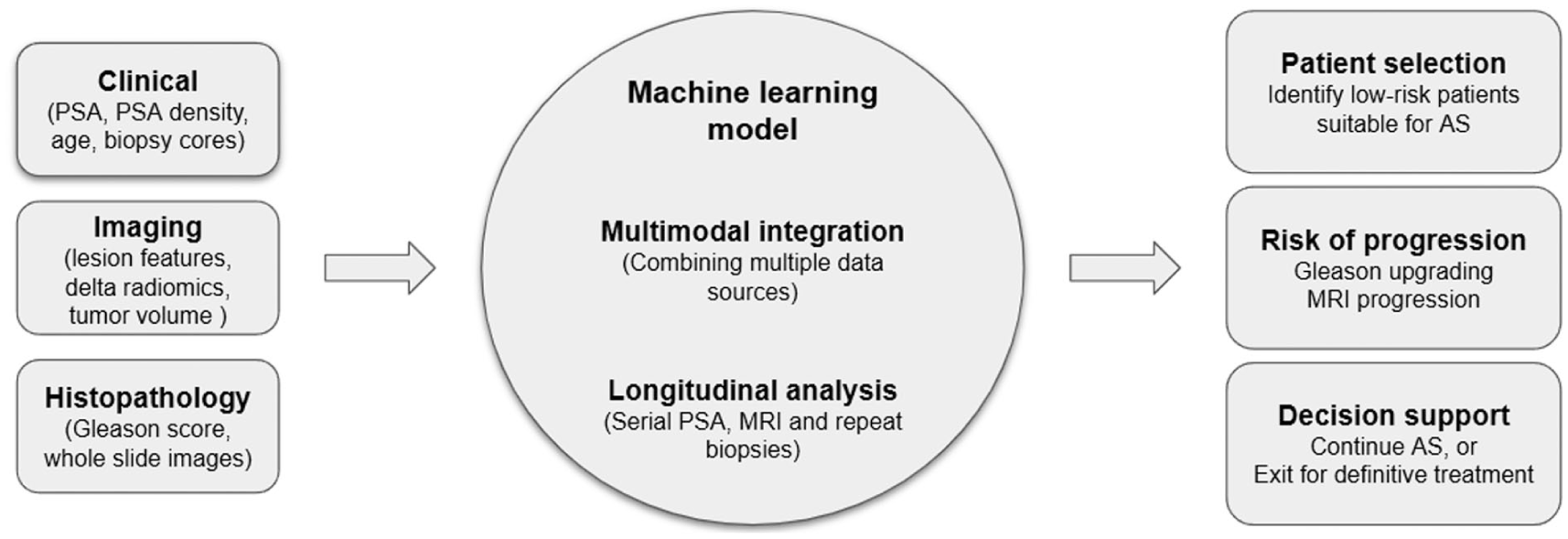
Integration of multimodal and longitudinal data in artificial intelligence models for active surveillance decision support. Multimodal and longitudinal data allow for more dynamic and personalized risk stratification during AS.
These findings are not without their limitations. The vast majority of the included studies were based on retrospective data, often tested on single-center cohorts. Most of the proposed models lacked external validation before being applied in clinical practice. In addition, the lack of standardized AS protocols and the heterogeneity in definitions inevitably introduce bias and raise questions about ML performance across institutions. Furthermore, the rationale behind AI algorithms is usually difficult to understand, making these models “black boxes” for clinicians and thus limiting their trust. 34 Finally, regulatory and ethical considerations regarding algorithmic transparency and legal responsibility pose notable barriers to the adoption of these tools. 35 Hence, it is too early to draw definitive conclusions about the ability of AI-based predictive tools to support decision-making for AS patients.
Future research should focus on prospective multicenter studies to test and validate the efficacy of such models in real-time clinical settings, thereby enabling safer, more reliable results before incorporating them into daily urological practice.
Conclusion
AI shows significant potential to improve decision-making in AS for PCa. Across the reviewed studies, ML and DL models consistently outperformed traditional approaches, particularly when integrating multimodal data, including clinical, radiological, and histopathological features. These models demonstrated strong predictive performance for both patient selection and progression risk, supporting more accurate risk stratification and potentially reducing unnecessary biopsies and overtreatment.
AI-driven approaches, including radiomics and longitudinal modeling, further enable non-invasive and dynamic monitoring strategies tailored to individual patients. However, current evidence is predominantly based on retrospective, single-center studies with limited external validation. Issues related to model interpretability, heterogeneity in AS protocols, and regulatory considerations remain important barriers to clinical implementation.
Prospective multicenter validation and improved transparency are essential before AI-based tools can be routinely integrated into AS management.
Supplemental Material
sj-docx-1-uro-10.1177_20514158261458173 – Supplemental material for Artificial intelligence for active surveillance decision support in patients with prostate cancer: A scoping review
Supplemental material, sj-docx-1-uro-10.1177_20514158261458173 for Artificial intelligence for active surveillance decision support in patients with prostate cancer: A scoping review by Nikos E. Anthousis, Bhavan P. Rai, Charalampos Mamoulakis, Theodoros Tokas and Dimitrios Damigos in Journal of Clinical Urology
Supplemental Material
sj-docx-2-uro-10.1177_20514158261458173 – Supplemental material for Artificial intelligence for active surveillance decision support in patients with prostate cancer: A scoping review
Supplemental material, sj-docx-2-uro-10.1177_20514158261458173 for Artificial intelligence for active surveillance decision support in patients with prostate cancer: A scoping review by Nikos E. Anthousis, Bhavan P. Rai, Charalampos Mamoulakis, Theodoros Tokas and Dimitrios Damigos in Journal of Clinical Urology
Supplemental Material
sj-png-3-uro-10.1177_20514158261458173 – Supplemental material for Artificial intelligence for active surveillance decision support in patients with prostate cancer: A scoping review
Supplemental material, sj-png-3-uro-10.1177_20514158261458173 for Artificial intelligence for active surveillance decision support in patients with prostate cancer: A scoping review by Nikos E. Anthousis, Bhavan P. Rai, Charalampos Mamoulakis, Theodoros Tokas and Dimitrios Damigos in Journal of Clinical Urology
Supplemental Material
sj-pptx-4-uro-10.1177_20514158261458173 – Supplemental material for Artificial intelligence for active surveillance decision support in patients with prostate cancer: A scoping review
Supplemental material, sj-pptx-4-uro-10.1177_20514158261458173 for Artificial intelligence for active surveillance decision support in patients with prostate cancer: A scoping review by Nikos E. Anthousis, Bhavan P. Rai, Charalampos Mamoulakis, Theodoros Tokas and Dimitrios Damigos in Journal of Clinical Urology
Footnotes
Acknowledgements
None.
Ethical considerations
Ethical approval was not required for this study, as it is a literature review based exclusively on previously published data.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
N.A. contributed to drafting the manuscript. B.R. contributed as a co-author and reviewed the manuscript. C.M. contributed to critical authorship and editing of the manuscript. T.T. contributed to the conceptualization of the study, critical authorship, and editing of the manuscript. D.D. contributed to drafting the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data supporting the findings of this study are available within the article and its supplemental materials.
Informed consent
Informed consent was not applicable, as no human participants were directly involved in the study.
Guarantor
T.T.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.