
Abstract
This review article considers how social-ecological systems change is transforming human health in the Anthropocene. From hunting and gathering bands through modern globalized societies, human health has been shaped by circular feedbacks between ecological processes, available energy sources, levels of social complexity, and cultural ontologies. As the environmental crises of the early Anthropocene (biodiversity loss, climate change, land use changes) push ecosystems across thresholds into new configurations, we are experiencing an equally profound transition for human health. Drawing on literatures from medical anthropology, sociology, complexity science, and ecological economics, this article argues that promising alternatives for health systems in the Anthropocene are emerging beyond the boundaries of the formal healthcare sector in community-based practices that can take root in a context of ecological limits, economic contraction, and growing networks of reciprocal care.
Keywords
Health in the Anthropocene
The Anthropocene is the geological era of human impact. It marks a profound reorientation of planetary dynamics, a shift toward the human socio-economic sphere as the determining force in processes of biophysical change (Lovelock, 2014; Steffen et al., 2015; Zalasiewicz et al., 2010). The Anthropocene is a time of uncertainty and contingency, of surpassing ecosystem thresholds that have not been crossed for thousands, sometimes millions of years (Lovelock, 2014; Rockström et al., 2009). The catalysts of these biophysical changes, namely human population growth, technological development, skyrocketing affluence (for some), and the associated rise in the material and energetic footprint of human society beginning in the Industrial Revolution and accelerating in 1950, have unleashed dynamics whose effects will be felt for hundreds of generations (Lovelock, 2014; Steffen et al., 2015; Zalasiewicz et al., 2010). On a planetary scale, we are moving out of the stable climactic conditions of the Holocene epoch and walking into a future predicted to be far less conducive to human flourishing (Lovelock, 2014; Rockström et al., 2009). As a result, the converging social-ecological crises we face in the Anthropocene will urge us to rethink long-held assumptions about human health.
The environmental signatures of the Anthropocene are already profoundly affecting health outcomes around the world (McMichael, 2014; Whitmee et al., 2015). The implications of ecological transformation include the exacerbating effect of environmental destruction on malnutrition and food insecurity (Friel, 2010; Whitmee et al., 2015), the impact of rising temperatures on the geographical range and virulence of infectious disease (Alley and Sommerfeld, 2014), and the influence of climate change on anxiety and stress-related mental illnesses (Doherty and Clayton 2011; Hidaka, 2012). The Anthropocene also marks a shift in the interactions between socio-economic inequality, anthropogenic environmental change, and ecologies of disease. This is evident, for instance, in the emergence of illness complexes known as syndemics, interactional diseases involving both chronic and acute conditions whose effects are multiplied by synergistic relationships between pathogens, human biology, and social vulnerability (Singer, 2009). Changes in the dynamics of health and disease in the Anthropocene, particularly the increasing synergism of social and environmental risks, stand to remind us of the relationship between human health and ecology, political economy and social complexity. The future of human health will depend on the extent to which these relationships come to figure prominently in the way we rethink health and restructure health systems.
This article argues that high-overhead, high-technology and high-consumption approaches to health will come under pressure in the Anthropocene as ecological limits to economic growth become more pronounced (see Meadows et al., 2004). The Western biomedical model that is broadly perceived to offer the highest standard of medical care ever available to human beings is predicated on a level of consumption that cannot be maintained in a future of tightening ecological constraints on human action (see Zywert and Quilley, 2017). Although this poses significant challenges for the future of human wellbeing (Horton et al., 2014), it does not preclude the development of new approaches that make use of existing medical knowledge and capacities while significantly reducing the resource throughput of health care systems. As discussed below, the characteristics of social-ecological systems have influenced epidemiological patterns, health care structures, and ontologies of health throughout human history, and new patterns are emerging in response to the unique dynamics of the Anthropocene. By connecting literatures about human health, the Anthropocene, and social-ecological systems change, this article proposes that we have the opportunity to build alternatives in advance of regime-level transformation to make it more likely that they will take root when the system shifts. It concludes by presenting a range of structural and ontological alternatives that hold potential to improve human health amid rising social, economic, and ecological instabilities.
Human health through time
From an anthropological perspective, there is no universal, definitive way to think about health. Ontologies of health and illness are inextricable from the cultural contexts in which they arise, and are shaped by surrounding political economies, social institutions, and ecosystems (Baer et al., 2013; Goodman, 2013; Lock and Nguyen, 2010; McElroy and Townsend, 2014). For the most part, ontologies of health remain unconscious, embodied in approaches to treatment, arrangements of health and care practices, and the daily routines people pursue to ward off disease (Young, 1982 as cited in Lock, 2001). To comprehend the extent to which our understanding of health is contingent upon social-ecological context, it is useful to trace large-scale transformations in epidemiological patterns, health system structures, and ontologies of health from the advent of the human species to the present (see Barrett and Armelagos, 2013; Harper and Armelagos, 2010; Zuckerman, 2014). This also helps us identify possible trajectories for the future of human health given the convergence of economic, demographic and ecological pressures in the Anthropocene. To illustrate dominant patterns, it is necessary to present complexes of epidemiology, social structure, and ontology as ideal types (see Weber as cited in Giddens, 1971). This is not meant to downplay the presence of significant diversity either today or in humanity’s past. Lock (2001, 2002) and Lock and Nguyen (2010) illustrate how the same technological advances and scientific knowledge can translate into diverse health care practices in different cultural settings. However, when bounding the system at the scale of the global social-ecological regime, clear trends emerge that have vital implications for the future of human health.
Figure 1 demonstrates the extent to which human health and approaches to health care are contingent on the characteristics of the social-ecological regime. Synthesizing the evidence presented in sections ‘Epidemiological transitions’, ‘Energy, social complexity, and institutional structures’ and ‘Ontologies of health’, it illustrates how circular feedbacks between the biophysical environment, energy sources, levels of social complexity, and cultural epistemologies and ontologies create distinctive ecologies of disease, influence health care structures, and shape ontologies of health.
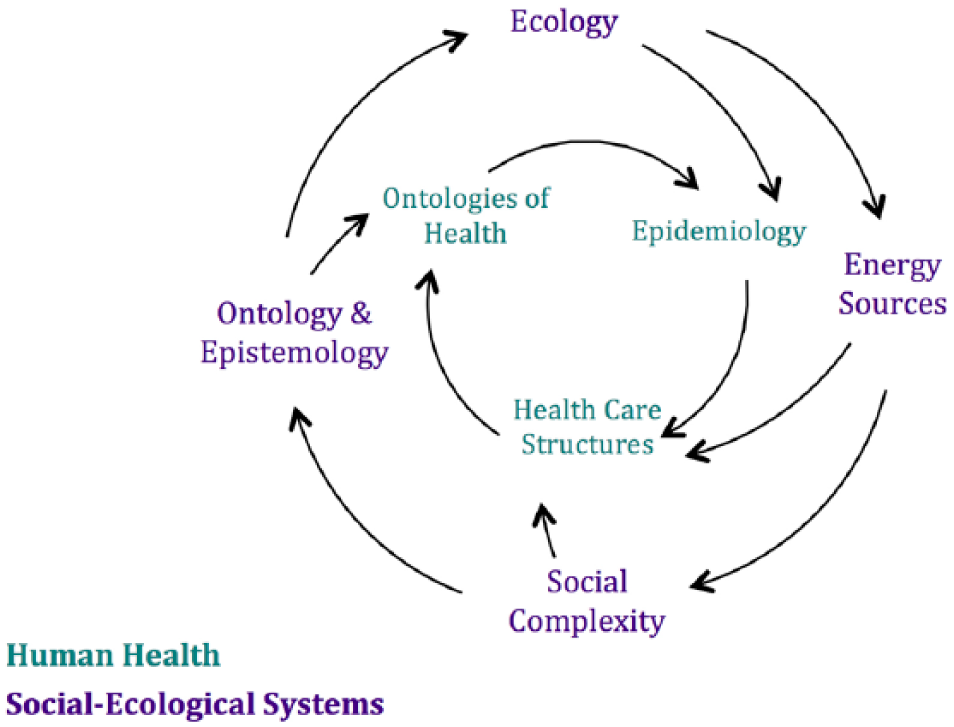
Relationships between ecology, energy social complexity and ontology in social-ecological systems and human health.
Epidemiological transitions
Humans with the capacity for cultural expression evolved approximately 2 million years ago and lived in hunting and gathering bands for more than 99% of our time on the planet (Devore, 1968, cited in Katz, 1982; McElroy and Townsend, 2014). Among hunters and gatherers, malnutrition, starvation, and chronic diseases were rare. Predation accounted for a small number of deaths, and exposure to infectious disease varied by ecological niche. Social mortality (deaths due to infanticide, gerontocide, and interpersonal conflict) were ever-present (Dunn, 1977, cited in Baer et al., 2013). While there is little evidence regarding mental illnesses among historical hunters and gatherers, epidemiological patterns in contemporary foraging groups suggest that stress-related diseases were uncommon (Baer et al., 2013; McElroy and Townsend, 2014).
The transition to agriculture approximately 10,000 years ago began the first epidemiological transition. As people settled in agricultural communities, populations grew and living arrangements became increasingly dense. Fecal contamination and close proximity to domesticated animals allowed infectious diseases to thrive. Nutrition declined as diets became less diverse and more dependent on the harvest of a small number of species. With the development of agricultural states, social differentiation increased and disparities between the health outcomes of upper and lower classes emerged. The incidence and severity of epidemics steadily rose (Armelagos et al., 2005; Barrett et al., 1998).
The second epidemiological transition followed the development of germ theory, improvements in hygiene, and the establishment of public health measures during the industrial revolution (Barrett et al., 1998; Harrison, 2004). Combined with antibiotics, which enabled effective treatment of bacterial infections and expanded surgical capacity, the incidence of infectious disease declined dramatically. Chronic and degenerative diseases induced by longer lifespans, pollution, and other environmental toxins of industrialization became the dominant source of mortality and morbidity (Barrett et al., 1998; Omran, 1971, as cited in Armelagos et al., 2005). These diseases arise out of the gulf between the environments in which the human species evolved and the behavioural patterns of industrialized nations, and include diabetes, cancer, osteoporosis, and heart disease (Hidaka, 2012).
In the mid-20th century, a third epidemiological transition began with the resurgence of infectious disease caused by human manipulation of the environment and the appearance of antibiotic-resistant pathogens and pesticide-resistant disease vectors (Armelagos et al., 2005; Barrett et al., 1998). Highly interconnected and mobile social patterns in globalized societies further promote the rapid spread of disease through geographically distant populations (Armelagos et al., 2005; Homer-Dixon, 2006). Low- and middle-income countries experience a double burden of disease, continuing to deal with a heavy load of infectious disease especially among impoverished peoples, as well as rising chronic and degenerative illnesses (Zuckerman, 2014). The epidemiology of mental illness has also shifted. Anxiety, suicide, and personality disorders have increased (Hidaka, 2012; Patel et al., 2016; World Health Organization (WHO), 2015) and depression can now be classified as a ‘disease of modernity’, one that has reached an epidemic level in affluent nations, particularly among young people (Hidaka, 2012: 206). In low- and middle-income countries, the prevalence of common mental disorders is also growing, and mental illness is associated with living in poverty (Lund et al., 2010; Patel et al., 2016).
Energy, social complexity and institutional structures
Epidemiological trends demonstrate that societal structures impact microbial genetics, human biology, and ecologies of disease (Armelagos et al., 2005; Barrett et al., 1998). Each transition followed changes in human society along three central trajectories: population, complexity, and energy use (McElroy and Townsend, 2014). With the agricultural revolution, humanity moved from a long-standing solar-energy regime to one that also harnessed power from domesticated animals, water, and wind. These new energy sources made it possible to add new layers of complexity to human societies, creating greater social differentiation through an expanded division of labour (McElroy and Townsend, 2014; Tainter, 1988). While hunter-gatherer medicine likely involved community-centric healing and reciprocal care among extended kin groups (see Katz, 1982), the transition to agriculture began a process of medical specialization, establishing practitioner groups including herbalists, midwives, bonesetters, and barber-surgeons (Harrison, 2004).
With the discovery of fossil fuels, social structures became even more differentiated (Heinberg, 2010; Tainter, 1988). In Europe, the Industrial Revolution expanded the division of labour and shifted the political economic center of gravity away from community reciprocity toward markets as the ‘organizing principle’ of society (Polanyi, 1944: 79). Expansion of the market economy facilitated growth in modern scientific and medical capacities (Baer et al., 2013). States developed increasingly sophisticated processes to monitor and control public health, implementing sanitation and vaccination programs that dramatically improved population level health outcomes (Harrison, 2004; Scott, 1998). To counteract the social disturbances caused by the rapid extension of market economies, nations instituted welfare policies to redistribute social goods including education and healthcare (Dale, 2010; Polanyi, 1944; Quilley, 2012).
In the 20th century, accessibility of cheap energy enabled population and material affluence to grow at an unprecedented rate (Heinberg, 2010; Odum, 2007). Modernization spread outward from Europe, characterized by the disembedding of the economy from society (Polanyi, 1944), faith in the ideals of progress and development (Berman, 1982), increased bureaucratic rationalism (Weber as cited in Giddens, 1971), and rising individualization (Bauman, 2012; Beck and Beck-Gernsheim, 2002). Tied to processes of modernization and colonialism, biomedicine became the dominant paradigm structuring the provision of health care services around the world (Baer et al., 2013; Lock and Nguyen, 2010). Biomedical health care, funded both privately and by welfare states, is oriented toward high technology treatments, the use of pharmaceutical drugs, and the delivery of professionalized medical services in organized centers such as hospitals and clinics (Baer et al., 2013; Bednarz and Beavis, 2012). These factors jointly contribute to the high ecological footprint of modern health care through transportation costs for health professionals, patients, and supplies, the use of petrochemicals to manufacture medical equipment and pharmaceuticals, and the massive consumption of energy and disposable materials by medical facilities (Campion et al., 2015; Hess et al., 2011; Thiel et al., 2015).
Ontologies of health
The historical trajectories of human health and health care demonstrate that in addition to epidemiological and institutional changes, increased social complexity and new energy sources are coupled with changes in cultural ontologies of health (Baer et al., 2013). Social relations in pre-modern societies are generally collectivist and community-centric, defined by lifelong relationships within extended kinship networks and bonds of mutual obligation rooted in custom and religion (Greenfield, 2009; Tönnies and Price Loomis, 1887). In pre-modern communities, collective interests supersede individual needs (Polanyi, 1944) and members are united through strong meaning frameworks (Becker, 1973; also see Giddens, 1984). Ontologies of health and illness in pre-modern societies reflect their collectivist social structure (Greenfield, 2009). Theories of disease causation emphasize discordant social relations and healing is a communal process in which ritual plays a central role (Katz, 1982; Levi-Strauss, 1963, as cited in Schepper-Hughes and Lock, 1987; Turner, 1977). For example, among the Kalahari Kung, sickness is a latent presence in everyone that can only be prevented through ceremonial dances aimed at rebalancing relationships between individuals, society, and the environment (Katz, 1982). Pre-modern ontologies of health are more holistic, with reality perceived in terms of ‘harmonious wholes’, microcosms and macrocosms, and ‘complementary dualities’ rather than binary oppositions (Schepper-Hughes and Lock, 1987: 12). Among the Qollahuaya-Andean in Bolivia, for instance, the human body and their homeland of Mount Kaata are perceived as homologous. Illness is conceptualized in terms of environmental destruction, as rockslides and earthquakes, and is treated in communal ceremonies that return integrity to the mountain (Bastien 1978, 1985, as cited in Schepper-Hughes and Lock, 1987).
Modernization processes are associated with a shift from Gemeinschaft (community-centric) to Gesellschaft modes of social organization ordered by the market economy, the state, and the rational transactions of autonomous individuals (Greenfield, 2009; Quilley, 2012; Tönnies & Price Loomis, 1887). Modern ontologies of health and illness, shaped by Western philosophical and scientific traditions, likewise feature naturalistic theories of disease causation, a mechanistic view of the human body, and an individualistic approach to curing (Foucault, 1994; Harrison, 2004; Lock and Nguyen, 2010). During the enlightenment, this ontology of health took root in a Western scientific approach to medicine that, advanced by rising state power and technological developments, influenced conceptualizations of human health and illness around the world (Baer et al., 2013; Harrison, 2004). Modern understandings of the human body were highly influenced by the Cartesian separation of body and mind (Schepper-Hughes and Lock, 1987). Physics became the dominant metaphor for natural processes, contributing to a reductionist, materialist approach to a mechanical universe populated by objective, individual actors (Ophuls, 2011; Sutherland, 2015). Clinical medicine rose to prominence, no longer viewing illness as a property of diseased people or miasmic environments, but as isolatable entities that can be eradicated using pharmaceutical and surgical interventions directed at individual bodies (Foucault, 1994; Harrison, 2004; Shepper-Hughes and Lock, 1987). Health came to exist in a dualistic relationship with disease, conceptualized as a state of normalcy or the absence of pathology (McElroy and Townsend, 2014). For human bodies, ‘normal’ was defined based on statistical data about population health, with disease increasingly perceived to affect bodies in the same way regardless of cultural or environmental locality, contributing to the rise of a strictly biological approach to medical intervention (Lock and Nguyen, 2010).
When the process of modernization began in Europe, it was associated with the utopian ideal of wiping away archaic social structures and replacing them with a rationally designed society that could meet all human needs (Bauman, 2012; Berman, 1982). In medicine, this ontology combined with new technological and pharmaceutical advances to make unlimited medical intervention a moral imperative (Bauman, 1998; Zola, 1975). Germ theory acted as a model for all disease, including mental illnesses and social problems (Harrison, 2004). As the vast social design projects of the 20th century were found to cause extreme human suffering, however, the utopian vision of the first phase of modernity fell away, replaced by the revolutionary impulse itself (Bauman 2012; Berman, 1982; Scott, 1998). The drive to constant change and reflexivity pervaded all realms of life, and medical knowledge became subject to continual revision through processes of increasingly specialized scientific inquiry and practice (Bauman, 2012). The medicalization of social issues ramped up, with pharmaceutical companies stepping in to pathologize and treat aspects of normal human variation perceived as deviant (Bauman, 1991, 2012; Foucault, 1994; Schepper-Hughes and Lock, 1987; Zola, 1975). In this context, the very concept of health was subsumed by ‘fitness’, a value that embodies the modern ideal of progress in its quest to optimize physical performance and appearance by shopping for the latest tools and techniques (Bauman, 1998; Beck and Beck-Gernsheim, 2002).
Modern ontologies of health are also profoundly shaped by rising levels of individualization (Beck and Beck-Gernsheim, 2002). Elias proposes that processes of sociogenesis (the development of society) mirror processes of psychogenesis (the development of the mental states of individuals within societies) (Elias, 1978). By establishing an increasingly complex and specialized division of labour, industrialization and capitalism shift social relations in an individualistic direction (Berman, 1982; Marx as cited in Giddens, 1971; Polanyi, 1944). For medicine, individualization transfers the locus of responsibility for health and care from the sphere of social relations onto the individual, with illness perceived as a consequence of poor choices (Bauman, 1991, 2012; Beck and Beck-Gernsheim, 2002; Maynard, 2006). The goal of modern medicine becomes preserving individual life at all costs, heroically extending the lifespan over all other considerations including quality of life and social wellbeing (Gawande, 2014). Individualization is further reinforced by the development of the discipline of psychology, which in applying scientific principles to inner life, reduces the ‘soul’ to the ‘self’ (Becker, 1973: 191).
Figure 2 offers an illustration of how human health and health care have changed over time alongside changes in the broader social-ecological regime. It tracks high-level transitions in energy availability, social organization, political economy, disease ecology, medical technologies, health practitioners and etiologies of disease from the time of hunters and gathers to the emergence of a Western biomedical approach to health.
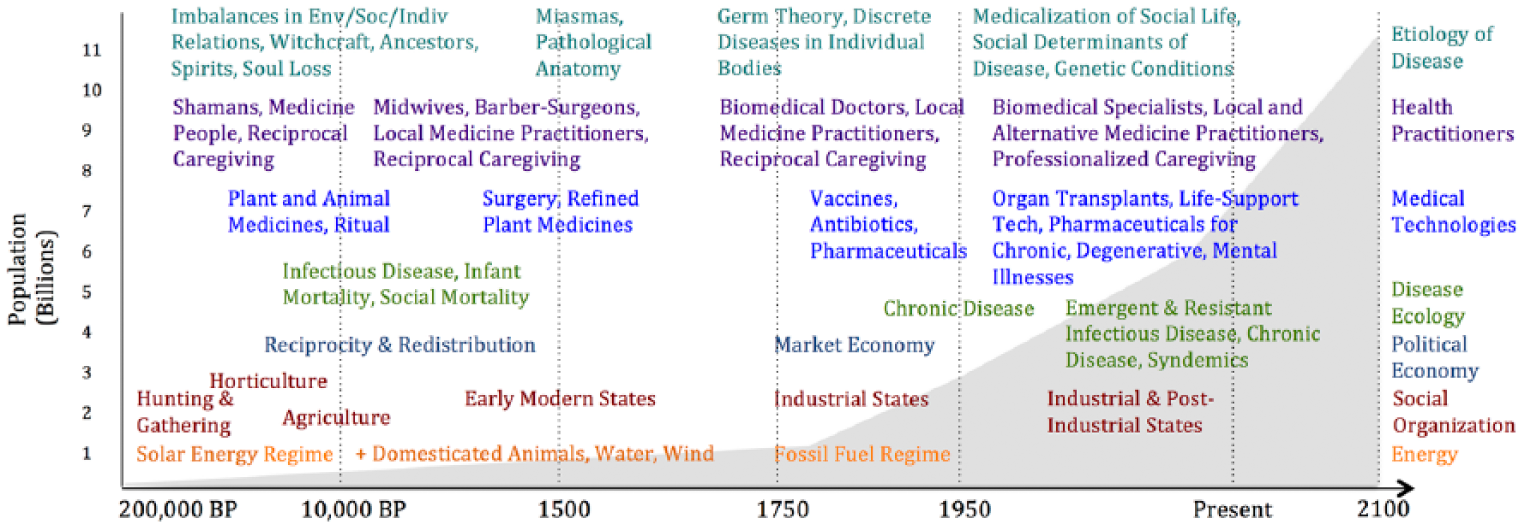
Changes in social-ecological systems, human health, and health care.
Implications for the Anthropocene
Modern health care is highly complex, technologically advanced, and resource and energy intensive (Bednarz and Beavis, 2012; Odum, 2007). It is integrated into and dependent upon the capitalist economy, with market forces determining medical research priorities, trends in professional specialization, and the ongoing medicalization of social problems (Alley and Sommerfeld, 2014; Bauman, 2012; Janes et al., 2006; Missoni, 2015; Twenge and Campbell, 2010). Biomedical health care is upheld by modern ontologies that individualize illness and position curing individual bodies and extending the lifespan as the primary goals of medicine (Beck and Beck-Gernsheim, 2002; Gawande, 2014; Janes et al., 2006). These ontologies and structures are premised on a high degree of social complexity maintained through large and continually expanding throughputs of materials and energy (Odum, 2007; Quilley, 2013; Tainter, 2014). In the Anthropocene, fault lines are appearing in the ecological, social, and ontological bedrock of modern medicine. As has happened in the past, the way we think about health and the way we structure health care will need to adapt to the conditions of an alternative social-ecological regime as the system transforms.
For over 40 years, modern societies have been pushing up against ecological limits (Meadows et al., 2004). Environmental scientists have identified nine planetary boundaries, three of which (climate change, biodiversity loss, and the nitrogen cycle) have already been crossed (Rockström et al., 2009). Crossing ecological thresholds can result in nonlinear changes, causing systems to flip into novel patterns of behavior that are not as conducive to human wellbeing as the stable Holocene states in which our species evolved (Lovelock, 2014; Rockström et al., 2009). Ecological footprint assessments estimate that on a global scale, we are overshooting available material resources by 20% (Meadows et al., 2004). Rapid consumption of fossil fuels, accelerating exponentially since 1950 (Steffen et al., 2015), has depleted stocks of our highest-quality energy source (Greer, 2009; Heinberg, 2010; Kallis et al., 2014; Raffle, 2010). We have also passed the peak of many of the world’s material resources, including minerals and metals that we use to build renewable energy and communication technologies (Kershner, 2014). As the planet’s stocks of fossil fuels become depleted, society’s energy return on investment decreases as it costs more energy to make energy (Odum, 2007; Tainter, 1988).
Without fossil fuels, social institutions could not be structured as they are today (Homer-Dixon, 2006; Hopkins, 2008; Odum, 2007). Existing institutions are dependent on economic growth, which has underpinned the social compact for 200 years (Daly, 2005; Jackson, 2009; Meadows et al., 2004). For instance, the welfare state is funded by fiscal transfers that are generated through economic growth (Bailey, 2015). However, despite the connection between growth and wellbeing in modernity, economic growth and environmental sustainability are incompatible (Homer-Dixon, 2006; Kallis et al., 2014; Quilley, 2017). There is no evidence that improvements in efficiency lead to absolute reductions in material and energy use at a global scale. In contrast, enhanced efficiency can actually accelerate consumption through a vicious feedback loop known as the Jevons Paradox (Jackson, 2009; Kallis et al., 2014). Furthermore, resource and energy limits mean that material standards of living cannot infinitely increase in affluent countries, especially if anything resembling a socially just global distribution of material resources is to be achieved (Flipo and Schneider, 2014; Jackson, 2009; Ophuls, 2011).
The convergence of resource constraints and declining energy return on investment, multiplied by the risks associated with crossing ecological thresholds, makes modern societies increasingly vulnerable to rapid losses of social complexity (Beddoe et al., 2009; Greer, 2009; Homer-Dixon, 2006; Kallis et al., 2012; Tainter, 1988, 2014). This could occur as a widespread social collapse with devastating consequences for human civilization such as the fall of the Roman Empire or the collapse of the Lowland Mayan civilization (Tainter, 1988). In these two scenarios, collapse proceeded largely in response to the diminishing returns of increased social complexity (Tainter, 1988, 2014). When societies encounter problems, the easiest solution is often to add a new layer of complexity that builds on existing social structures. Once the new layer is established, it becomes normalized and society subsequently requires even more energy to sustain itself. For the Romans and the Maya, the need to sustain greater social complexity prompted them to accelerate production, ultimately depreciating their available resources until it was no longer possible to meet material and energetic demands (Tainter, 1988, 2014). When societies reach a point of diminishing returns on existing levels of social complexity and energy return on investment, they become vulnerable to rapid losses of social complexity which can be experienced as a loss of governance capacity, territory, and population, a reduction in long-distance communication and trade, and a reversion to simpler technologies and social arrangements (Tainter, 1988). Alternatively, losses of social complexity could proceed as a series of smaller breakdowns that present opportunities for catagenesis or ‘creative renewal’ following a crisis (Homer-Dixon, 2006: 268). The strongest alternative to collapse is planned descent, in which energy and material limits are anticipated before they become unavoidable and are incorporated into policy and practice at state and local levels (D’Alisa et al., 2014; Hopkins, 2008; Jackson, 2009). This requires planned restructuring of social institutions, political economic arrangements, and relationships between people and the environment (Beddoe et al., 2009; Westley et al., 2011).
In the same way that modern ontologies and social structures are premised on high material and energy throughput, low material and energy throughput will anchor a different type of society in a different social-ecological regime (de Molina Navarro and Toledo, 2014; Quilley, 2013, 2017). As Tainter (2014) describes, losses of social complexity are often followed by a period of relocalization in which the needs of a community must be met locally in the absence of networks for trading or bureaucratically redistributing resources. Using the human past as a model, we can anticipate that a low-energy modernity would involve low levels of material consumption, the reemergence of reciprocity and redistribution as primary economic systems and means of securing social welfare, and relocalization of production and consumption activities (Hopkins, 2008; Kish et al., 2016). This would in all likelihood lead to the retrenching of we-identities based in place over cosmopolitan individualism, and a return to Gemeinschaft modes of living (Elias, 2001; Greenfield, 2009; Quilley, 2017).
Social-ecological systems change
Human health and health systems, defined by the WHO to encompass all existing health care services, service providers, information networks, medical equipment and technologies, and financing and governance systems (WHO, 2007), are shaped by the characteristics of the social-ecological systems within which they develop (McMichael, 2014). Given this, theories of social-ecological systems change drawn from ecology, complexity science, and sustainability studies are useful for thinking about the future of human health.
Social-ecological systems transform as a result of intersecting pressures at the levels of sociotechnical landscapes, regimes, and niche innovations (Westley et al., 2011, 2014; Wiseman et al., 2013). Transitions from one social-ecological system to another are co-evolutionary processes that alter social institutions, formal and informal governance systems, cultural values and behaviour patterns, and daily practices and skills (deMolina et al., 2014; Westley et al., 2011; Wiseman et al., 2013). The course of human history has been defined by global-scale social-ecological systems transitions including the agricultural, industrial, and global communications revolutions (Holling et al., 2002a; Homer-Dixon, 2006). As discussed above (see Figure 2), these changes at the social-ecological scale affect human health and approaches to healing both by changing ecologies of disease as well as by enabling the development of distinct medical technologies, health practitioners, and ontologies of health and illness.
With the transition to industrial modernity, rising populations and enhanced human capacity to manipulate nature have caused the Earth’s ecological and socio-economic systems to be increasingly coupled (Steffen et al., 2015; Zalasiewicz et al., 2010). The greater the level of interconnectedness in a system, the more vulnerable it becomes to cascading change (Gallopín, 2002; Homer-Dixon, 2006). As a result, in the existing social-ecological regime, crises at the level of planetary biophysical processes (climate change, biodiversity loss, environmental destruction) rapidly translate into economic and social crises including recession, reemerging infectious disease, rising energy costs, and mass migration. Current challenges could therefore be early warning shocks of a coming regime change, one that is likely to rival the agricultural or industrial revolutions in its depth and scope (Homer-Dixon, 2006).
The characteristics of complex adaptive systems help to explain the dynamics of social-ecological systems change. Complex adaptive systems such as ecosystems, human beings, and economies are controlled by circular feedback processes that generate distinctive patterns of behaviour (Bateson, 1987; Meadows, 2008). They are self-organizing, or capable of solving problems by adding layers of complexity over time to adapt to external and internal conditions (Meadows, 2008; Tainter, 1988). Complex adaptive systems also exist in dynamic equilibrium, a state in which change is an essential component of long-term stability (Lovelock, 2014; Meadows, 2008; Walker and Salt, 2006). In social-ecological systems, stability dynamics depend on resilience (the ability to adapt to disturbance while maintaining the same basic structure and function) and transformability (the ability to develop new systemic structures when ecological, economic, and/or social pressures make the existing system untenable) (Walker et al., 2004).
Dynamic equilibrium at the scale of social-ecological systems can be conceptualized through the state-space metaphor of a ball within a basin (Homer-Dixon, 2006; Walker and Salt, 2012; Westley et al., 2011). In the same way that a ball rolls to the bottom of a basin, a complex system seeks a steady state. External conditions in the system cause the shape of the basin and the position of the ball within it to continually shift. Complex adaptive systems have multiple potential steady states or ‘basin[s] of attraction’ (Walker and Salt, 2012: 6). Their position in relation to these potential states is controlled by a number of key variables that, when pushed past a threshold, cause the system to tip into a new equilibrium, a new basin that imposes an alternate identity, structure, and function on the system (Beddoe et al., 2009; Homer-Dixon, 2006; Walker and Salt, 2012; Westley et al., 2011).
Social-ecological systems change is also governed by the dynamics of the adaptive cycle (Holling and Gunderson, 2002; Walker and Salt, 2006; Westley et al., 2011). The adaptive cycle describes the periodic movement of complex systems through phases of ‘exploitation’, ‘conservation’, ‘release’, and ‘reorganization’, stages characterized by shifting levels of potential, connectedness, efficiency, rigidity, vulnerability, and innovation (Holling and Gunderson, 2002: 35). Adaptive cycles occur at every scale from individual organisms to communities and ecosystems (Walker and Salt, 2012; Westley et al., 2011). From the perspective of the adaptive cycle, regime change occurs in the ‘release’ phase and involves a period of ‘creative destruction’ during which the structures and institutions of the dominant regime collapse, freeing up resources to be put to new uses in an emerging systemic order (Holling and Gunderson, 2002: 45). This model presents change as an ingrained, unavoidable dynamic of complex social-ecological systems, one that generates opportunities for innovation, creativity, and renewal (Holling and Gunderson, 2002; Homer-Dixon, 2006; Westley et al., 2011). Adaptive cycles are linked at different scales, creating highly complex social-ecological feedback systems known as panarchies that can precipitate cascading change that flows from one scale to another (Holling and Gunderson, 2002; Walker et al., 2004).
Theories of systems transformation present regime-level change as ecological and anthropological constants. If change is inevitable, bolstering the current system of modern medicine, dependent as it is on the dynamics of industrial capitalism, is not the most effective way to secure long-term human health on a global scale. Vulnerabilities and crises such as rising inequality, economic instability, and climate change are pushing the current social-ecological regime toward thresholds that could precipitate a significant collapse in the coming decades (Homer-Dixon, 2006; Tainter, 2014). Converging challenges including aging demographics, slowed economic growth, and spiraling costs of health care services threaten the viability of the welfare state, while the need to adapt to and mitigate environmental damages, to innovate new sources of energy, and to invent new social and economic systems create further tension (Tainter, 2014). Figure 3 uses the adaptive cycle to illustrate how vulnerabilities accumulating at the level of social-ecological systems translate into vulnerabilities at the level of health systems and human health outcomes, with a growing potential for release or ‘creative destruction’ to cascade through the entire panarchy. The same vulnerabilities that are affecting the social-ecological regime, namely declining energy return on investment, limits to growth, inequality, and ecological crises, are also evident at the level of health systems. Health systems experience these pressures as financial constraints due to declining resource and energy availability, dependence on fossil fuels for technologies, supplies, and transportation, and increasing strain on governance systems like the welfare state (Bailey, 2015; Hess et al., 2011; Raffle, 2010; Tainter, 2014). At the level of human health, tension in the social-ecological regime is experienced as emerging illnesses caused by climate change and other ecological disruptions, increasing commodification of care in capitalist modernity, and loss of access to assistance due to shrinking networks of reciprocal caregiving among extended families and communities.
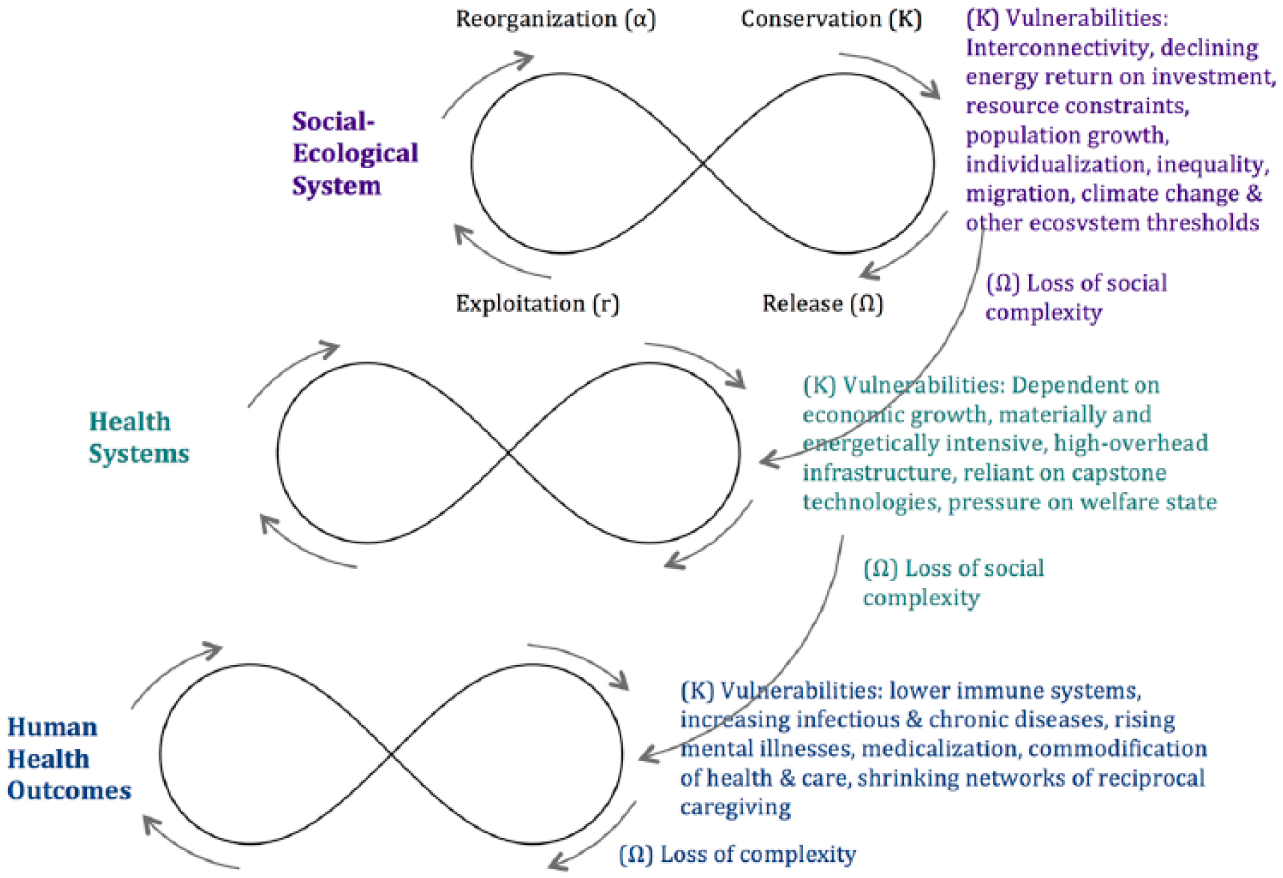
Health panarchy with vulnerabilities cascading from social-ecological systems through health systems to human outcomes.
Approaches aimed at managing these problems will not be enough to avoid collapse or to secure a long-term future in which human societies can flourish (Homer-Dixon, 2006; Lorek, 2014). Change at the regime level is needed to escape the negative trajectories of the current system, including feedback loops that maintain our dependence on economic growth and destroy the environment, and meaning frameworks that are oriented toward individual material consumption and erode social practices of reciprocal care (D’Alisa et al., 2014; Homer-Dixon, 2006; Westley et al., 2011). However, we continue to face a void of large-scale solutions to large-scale problems. Most proposed solutions work within systems whose dynamics perpetuate the same problems they attempt to solve (Berry, as cited in Lockyer and Veteto, 2013). They are therefore prone to generating unintended consequences at higher scales through feedback processes that involve long time delays and geographically distant effects (Holling et al., 2002b; Meadows, 2008; Rogers, 1983; also see Giddens, 1984). Management approaches also leave out a vast amount of anthropological evidence about the underlying motivations of human behavior. Rooted in modern assumptions about autonomous individuals as agents of social change, managerial solutions focus on material incentives, education, and rational decision-making while neglecting non-rational drivers of behaviour and the influence of cultural ontologies and meaning frameworks on patterns of collective action (Dickinson, 2009; Quilley, 2017).
To develop more promising strategies for addressing the problems currently surfacing at the level of the social-ecological regime, it is useful to return to the state-space metaphor of basins of attraction. When systems transition from one social-ecological regime to another, they seek a new steady state (Walker and Salt, 2012). As such, solutions to systemic problems can be found in alternatives that deepen new basins of attraction before the system shifts (Homer-Dixon, 2006; Jackson, 2009; Westley et al., 2011). Within the dominant regime, alternatives develop in niches, spaces of experimentation that are protected from regime-level pressures where groups can implement social, cultural, and economic innovations. These niche alternatives or ‘shadow networks’ of solutions may remain relatively insignificant so long as the dynamics of the existing system prevail, but can quickly gather momentum as the system transitions into a new equilibrium (Westley et al., 2011: 771).
Building alternatives in advance can help to avoid catastrophic collapse by enabling catagenesis, a period of creative flourishing that follows systemic breakdown (Homer-Dixon, 2006). Generating social momentum around promising alternatives before a crisis occurs improves the chances that humane alternatives will take root after a period of creative destruction (Homer-Dixon, 2006; Jackson, 2009). Identifying ‘possible new trajectories’ for systems before they cross thresholds therefore increases the chances of constructive transformations (Walker and Salt, 2012: 21), while building energy around diverse and numerous adaptive solutions further strengthens the resilience of possible alternatives (Greer, 2009; Westley, 2013).
Building alternatives
This section outlines emerging structures, practices and ontologies that can contribute to deepening an alternative basin of attraction for health in the next social-ecological regime. As discussed above, the expansion of biomedicine has accompanied modernization processes around the world (Baer et al., 2013), leading to the establishment of a high-overhead, materially and energetically intensive health care system that will not survive the transition to a social-ecological system defined by ecological constraints (see Odum, 2007; Zywert and Quilley, 2017). To adapt to this transition, we must develop structural and ontological alternatives for human health that reflect the logic of an ecologically viable society.
Conventional approaches to sustainability and health tend to reinforce underlying biomedical assumptions while subscribing to a Promethean discourse that emphasizes efficiency, cost-effectiveness, and technological innovation (see Dryzek, 2013). Strategies such as reducing the waste and emissions of health care services are essentially management approaches that take the resources and systemic feedbacks of the existing regime for granted. As a result, the most promising alternatives for human health are often found outside the boundaries of formal health systems, in social movements that reinvigorate networks of community reciprocity, policies that reduce the reliance of health and care activities on economic growth, and institutions that can provide effective care in contexts of resource scarcity. Alternatives can also be found in medicines that take into account the social and ecological dimensions of the healing encounter and that experiment with community-centric, context-dependent, and systemic approaches to health. The sections that follow introduce a set of structural and ontological alternatives that could anchor an alternative basin of attraction for health in a novel social-ecological system. Linking these diverse alternatives together by emphasizing points of connection such as the development of reciprocal care networks, low material and energy consumption, and the rejection of individualism in favour of systems perspectives, can help us understand not only how to build resilience within the current regime, but also how to begin hollowing out a new basin of attraction in preparation for social-ecological transformation.
Structural and institutional alternatives
The degrowth movement offers one of the most comprehensive policy visions for an alternative economic system that can remain within ecological limits while increasing social wellbeing (see D’Alisa et al., 2014; Martínez-Allier et al., 2010; Missoni, 2015). Health is a prominent structural element in this paradigm, which sees uncontrolled economic growth as the culprit of ecological crises that cause declining health outcomes over the long-term. Degrowth economies could be centered on labour-intensive health and care activities that provide opportunities for meaningful employment (Kallis et al., 2014; Missoni, 2015). Emphasizing economic relocalization, degrowth policies also focus on reducing the most environmentally and socially corrosive aspects of modern medicine, including medical consumerism and profit-driven international pharmaceutical chains. In their place, health in a degrowth economy would be sustained through public health interventions, preventative health activities, and local production of essential medicines (Missoni, 2015). To address declining employment opportunities, degrowth policies also advocate for a shortened work week, providing opportunities to reinvigorate informal networks of intergenerational care for children, the elderly, and other vulnerable people in extended families and cohousing structures (Kallis et al., 2014; Missoni, 2015).
Transition Initiatives, a community-led social movement that began in Totnes, UK, work toward many of the same goals, emphasizing energy descent and relocalization of health services in response to concerns about peak oil and climate change (Hopkins, 2008; Richardson et al., 2012). Transition Towns are developing health system models that feature local health centers, preventative programs, integration of biomedical and complementary treatment options, and a range of public health activities. They partner with local schools to educate children about healthy living, providing nutrition courses that encompass topics ranging from agriculture to cooking, simultaneously addressing ecological, social, and personal health. The transition movement’s vision of relocalized health care also involves cultivating medicinal plants and manufacturing small batches of pharmaceuticals on a local scale (Hopkins, 2008). In this vision, more meaningful work, a rise in physical activity, and more satisfying daily lives would lower stress and anxiety compared with current levels despite a reduction in material affluence (Hopkins, 2008; Richardson et al., 2012).
Ecovillages offer a similar structural alternative. Looking to the anthropological record for insight, they intentionally design ways of living to create healthy environments for people and the land (Lockyer and Veteto, 2013). Often founded on the permaculture ideals of care for the Earth and care for people, they build local prevention and healing capacities and try to function as much as possible outside the dominant health care system (Da Silva, 2009; Lockyer and Veteto, 2013). For instance, Earthaven ecovillage teaches self-healthcare skills and provides residents with biomedical and alternative health services performed by doctors, midwives, and herbalists who live on site (Da Silva, 2009). The long-standing ecovillage The Farm in Tennessee built a local health system that includes a laboratory, medical dispensary, infirmary, ambulance, midwives, neonatal ICU, and training for barefoot doctors (Lockyer and Veteto, 2013). Ecovillages and Transition Initiatives embody general principles with potential to make health systems more equitable, less dependent on nonrenewable resources, and more capable of addressing complex challenges. These include offering context-dependent services to local populations, enabling community participation in caring for the sick and vulnerable, emphasizing prevention, reducing costly treatments that deliver only marginal benefits, and making connections with related sectors such as education and housing (Farmer, 1999; Raffle, 2010).
Traditional medicines also present structural alternatives for health in a future defined by ecological constraints. During the second half of the 20th century, indigenous medicines were sanctioned by states throughout Asia as an alternative to expensive technological medicine in times of resource scarcity (Baer et al., 2013; Janes 1995; Janes and Hilliard 2008; Rogers, 1983). The People’s Republic of China trained close to 2 million barefoot doctors from poor backgrounds to administer basic Chinese and biomedical treatments in rural areas including suturing, setting bones, delivering babies, and diagnosing common diseases (Rogers, 1983). Traditional Tibetan medicine became a central component of Tibet’s expanding primary health care system in the 1980s, with traditional doctors offering inexpensive, locally available remedies (Janes, 1995). During Mongolia’s economic transition in the 1990s, health outcomes declined as the economy collapsed, and doctors turned to alternative medicines to better serve their patients (Janes and Hilliard, 2008). Although most health systems around the world include the provision of biomedical health services, practitioners of traditional medicines continue to serve 90% of rural communities (Bastien, 1992, cited in Baer et al., 2013). Traditional medicines offer structural alternatives that can function in environments of economic contraction and declining resources while incorporating greater attention to the social and ecological bases of health and illness. However, they are only viable alternatives to the extent that they remain tied to cultural meaning systems rooted in place. These contextual elements are in danger of being lost when traditional medicines are incorporated into state bureaucratic systems, which impose conformation to biomedical regimes of practice, training, and epistemology (Janes, 1995).
Ontological alternatives
To support human health in the Anthropocene, emergent structures and institutions must be grounded in ontologies that reconnect bio-psycho-spiritual aspects of personal health to the social-ecological context. The significance of ontology is evident in the durability of the family care system in Geel, Belgium. Sustained for over 700 years, families in Geel foster people with serious mental illnesses, living and working with them as contributing members of the family and community (Goldstein and Godemont, 2003; Jay, 2014). The practice is upheld by religious and cultural traditions, with families often making lifetime or multi-generational commitments to care for a stranger in what becomes a mutually beneficial relationship. Now overseen by the state, with biomedical treatments available at a community hospital, most care continues to occur in the everyday contexts of family and workplace. People with mental illnesses are known locally as ‘boarders’ rather than ‘patients’, and families are often unaware of the medical diagnoses of those they have taken into their homes (Jay, 2014: n.p.). Integration into community life is seen as a primary factor in successful health outcomes, contrasting with cold institutional approaches to mental illness (Tuntiya, 2006). Family care in Geel offers a model for addressing a complex health issue while rejecting medicalization, reducing the resource and energy throughput of medical services, and increasing community networks of reciprocal care (Goldstein and Godemont, 2003; Jay, 2014; Tuntiya, 2006).
Ontologies of health affect not only how we think about wellbeing and disease, but also how we attribute meaning to lifecycle milestones including birth, adolescence, elderhood, and death. As most medical interventions occur close to death (Gawande, 2014), alternative ontologies that reconceptualize death as a social-ecological process hold potential to reduce the energetic and material throughput of modern medicine. Reframing death also offers ways to strengthen cultural systems of symbolic immortality, reducing widespread psychological distress stemming from the breakdown of accessible immortality projects in modern societies (see Becker, 1973; Solomon et al., 2015).
In pre-modern societies death was rarely associated with finality, but instead represented a temporary separation from social life that ended with inauguration as an ancestor or rebirth in the next generation (Lock, 2002; Schepper-Hughes and Lock, 1987). Death signified a rite of passage, the end of one life and the beginning of another (Eliade, 1987). Modernity displaced death from the circularity of the social world, replacing it with a linear life that terminates in biological death (Bauman, 1998; Lock, 2002). Through processes of modernization, death was transformed into a scientific, biological event to be overseen by medical experts (Lock, 2002). From a biomedical perspective, death is often treated as a failure of medical expertise and technology (Foucault, 1980, as cited in Lock, 2002). The medicalization of death therefore separates it from social contexts that satisfy the human desire for meaning and continuity (Becker, 1973).
Becker (1973) argues that cultural meaning frameworks arise to address the human fear of death by creating avenues for symbolic transcendence such as an afterlife or the enduring effect of one’s actions in the world. In pre-modern societies, symbolic immortality could be attained through the daily activities of raising children and performing ascribed roles within extended family groups, whereas in modern societies it centers on the acquisition of material possessions and is inaccessible to the vast majority of people (Becker, 1973; Dickinson, 2009; Solomon et al., 2015) Resisting the medicalization of death through practices such as the hospice movement (Gawande, 2014; Lock, 2002) and developing green immortality projects that turn environmentally sustainable behaviours into sources of cultural heroism (Dickinson, 2009; Quilley, 2017) therefore offer promising ontological alternatives for health in the Anthropocene.
Alternative ontologies of health may also seek to reincorporate ritual in healing. Ritual figured prominently in indigenous and traditional medicines, giving meaning to events in the life course, redressing social conflict, and building community solidarity through collective experiences of liminality and communitas (Durkheim, as cited in Giddens, 1971; Katz, 1982; Turner, 1977, 2012). Although modern sensibilities initially rejected ritual as a holdover from a traditional world that limited individual autonomy and imposed arbitrary constraints that denied the inner self, interest in ritual is steadily increasing in the 21st century (Seligman et al., 2008). The move away from ritual in the early phase of modernity could also relate to rising levels of material affluence in the Global North. In traditional cultures, rituals were rarely needed when a resource was readily available (people standing before a river do not dance for rain), but become more prevalent during times of resource scarcity (Solomon et al., 2015). Similarly, the economic and material constraints of the Anthropocene could see a resurgence of ritual as a means of understanding and acting in the world to improve the health of humans in their social and environmental contexts. Seen as a mode of interaction, ritual creates a ‘shared subjunctive’ that increases social cohesion and makes it possible for people to act within the world they collectively create (Seligman et al., 2008: 7). ‘Sincerity’, the alternative to ritual action, emphasizes the importance of authenticity, the true self, and the objective world (Seligman et al., 2008: 7). By privileging inner states, it makes intent more important than action and is thus a poor ground for morality, as the sincerity of one’s own or another’s motivations can always be questioned. In contrast, the ritual mode emphasizes action over intent, making proper behaviour more important than belief and laying a stronger foundation for the development of collective interests (Seligman et al., 2008). In this way, ritual provides a means for combating individualism (see Durkheim, as cited in Giddens, 1971).
Developments in systems thinking, complexity science, and cybernetics also suggest new pathways for ontologies of health. Systems thinking stresses the interconnections and relationships between elements in a system. Complex adaptive systems are self-organizing and dynamic, displaying emergent properties that are more than the sum of their parts (Meadows, 2008). Patterns of feedback between elements in a complex system are circular and recursive, with overarching resilience rooted in the ability to adapt and maintain basic functions in the face of external or internal pressures (Bateson, 1987; Walker et al., 2004). These characteristics of complex social-ecological systems apply equally well at the scale of human health (Keeney, 1983; Sutherland, 2015; Van Eenwyk, 1997). For instance, fractal dynamics, structures that display self-similarity at different scales, are ubiquitous in nature (tree branches, coastlines) and in human anatomy (the bronchial tree, blood vessels) (Goldberger, 1997; Sutherland, 2015; Van Eenwyk, 1997). Fractals are also evident in physiological processes such as a healthy human heartbeat, which displays an irregular shape like a mountain range when graphed at different scales. Diseased states like a heart attack, in contrast, reflect a loss of complexity and are characterized by periodic rather than fractal dynamics as well as the dominance of a single scale (Goldberger, 1997; Sutherland, 2015; Van Eenwyk, 1997). Similarly, for both social-ecological systems and human health, resilience depends on the presence of diversity and variation. As long-term stability requires adaptation and change, resilience can be compromised by trying to optimize any single variable such as productivity or efficiency (Holling and Gunderson, 2002; Keeney, 1983; Meadows, 2008; Sutherland, 2015; Walker et al., 2004). Attempting to optimize health outcomes for individuals, for example, has led to overuse and misuse of antibiotics, reducing the resilience of the human population as a whole by contributing to the emergence of antibiotic resistant pathogens (Keeney, 1983; Sutherland, 2015).
Ophuls (2011: 43) presents ecology as the necessary ‘guiding metaphor’ for the near future, a paradigm for thinking about and structuring relationships with the natural world in an era when we must respect ecological limits to preserve our own existence. In the same way, systems thinking is a potent metaphor for human health in the Anthropocene. Parallels between social-ecological dynamics at the regime level and at the scale of human health remind us that health is not only biological or psychological, but is an emergent property of social and environmental processes at multiple scales. This perspective mirrors ontologies of health in pre-modern cultures around the world, which positioned social relations and interactions with nature as determining factors in patterns of disease and health (Keeney, 2015; Ophuls, 2011). Systemic ontologies are also becoming more mainstream within the field of global public health, with increasing attention devoted to social determinants of health, the health effects of climate change, and the need to integrate movements for social and ecological justice with concerns about human health outcomes (Buse and Hawkes, 2015; Costello et al., 2009; Kickbusch, 2016; Lang and Rayner, 2012). The One Health movement, for instance, brings together environmental experts, physicians, veterinarians, and health practitioners from diverse fields to address intersecting risks to health across scales from ecosystems to human and animal populations (see Schuftan et al., 2014). Planetary health, a novel theoretical and practical paradigm introduced by Richard Horton and colleagues in 2014 and expanded upon in a Lancet commission report in 2015, also recognizes the profound interconnectedness of the challenges facing human health and environmental integrity in the Anthropocene (Horton et al., 2014; Whitmee et al., 2015). As a field, it acknowledges the extent to which we are ‘mortgaging the health of future generations to realize economic and development gains in the present’ (Whitmee et al., 2015: 1973). In doing so, planetary health draws together a critique of overconsumption with a perception of health that extends the relevant timescale from the life of an individual person to the survival of the human species and the planetary systems that support all life on Earth.
Reclaiming more systemic ontologies could help move our societies toward the broader epistemological changes that will be necessary if we hope to live within ecological limits (see Bateson, 1987; Ophuls, 2011). For instance, highlighting the benefits to human health of mitigating climate change harnesses the momentum of dominant individualistic worldviews (Dickinson, 2009; Twenge and Campbell, 2010; also see WHO, 2015b). At the same time, framing messages about material and resource constraints around the interconnectedness of human and environmental health could help to engage people in behaviours that embody a more systemic epistemology (see Cheng et al., 2011 regarding the effect of message framing on sustainable behaviours). Public communication about the devastating effects of climate change has been shown to raise concern about ecological problems, but to also increase the despair people feel about the likelihood of finding humane solutions (Kaplan, 2000). If communicating about climate change makes people fear death, studies in terror management theory suggest that education and knowledge-sharing can have the opposite of their intended effect, causing people to cling more closely to existing materialistic meaning frameworks, effectively leading them right to the shopping mall and the gas pumps (Dickinson, 2009; Solomon et al., 2015). Emphasizing the interconnectedness of human health and social-ecological resilience could gain more traction, raising concern for nature by making it easier for people to perceive the environment as part of the self (see Schultz, 2000; also see Costello et al., 2009). It could also tap into people’s underlying motivations to demonstrate competence, to be needed by others, and to create a better life for themselves and their families (see Kaplan, 2000).
Figure 4 illustrates emerging structural and ontological alternatives that could help to deepen an alternative basin of attraction for health systems in the Anthropocene. These alternatives have the potential to simultaneously strengthen human health outcomes and ecological integrity in the face of existing pressures on our social-ecological system, as they have been demonstrated to thrive in environments with limited resources by engaging networks of community reciprocity.

Building alternatives in social-ecological systems transformation.
Conclusion
This article presents human health in the context of long-term social-ecological systems change. From hunting and gathering bands through modern globalized societies, the ways humans think about health and structure health care have been grounded in the dynamics of the dominant social-ecological regime. These dynamics are controlled by circular feedbacks between ecological processes, available energy sources, levels of social complexity, and leading ontologies and epistemologies. In turn, these feedbacks shape epidemiological patterns, health care structures, and ontologies of health (see Figure 1).
Today, environmental signatures of the Anthropocene such as climate change and biodiversity loss are pushing ecosystems across thresholds into new configurations (Rockström et al., 2009; Steffen et al., 2015; Zalasiewicz et al., 2010). Vulnerabilities and rigidities are accumulating in the dominant regime, which for over 200 years has been defined by the interactions of capitalist global markets, industrialization, technological manipulation of nature, and a mechanistic, reductionist ontology (see Giddens, 1990; Ophuls, 2011). Among the most significant vulnerabilities is globalized society’s dependence on economic growth to improve material standards of living and secure the social compact, functions that are coupled with rising rates of individualization and the expanding material and energetic footprint of human activities (Beddoe et al., 2009; Polanyi, 1944; Quilley, 2017). Confronted with declining material resources and the environmental imperative to move beyond a fossil fuel-based economy, transition to an alternative social-ecological system appears to be imminent (see Heinberg, 2010; Homer-Dixon, 2006; Meadows et al., 2004; Quilley, 2017; Walker and Salt, 2012).
For human health, the Anthropocene brings increasingly virulent infectious diseases, rising rates of dementia and anxiety disorders, a heightened risk of pandemics, and reduced access to the ecological foundations of life including clean air, water, and nutritious food (McMichael, 2014; Whitmee et al., 2015; WHO, 2015b). The transition to an alternative social-ecological regime could see the collapse of much of what upholds modern medicine, including welfare state benefits, international pharmaceutical and equipment chains, and antibiotic capabilities (Bednarz and Beavis, 2012; Dartnell, 2014; Raffle, 2010). Facing social-ecological regime change, our best hope lies in building alternatives that can hollow out a new basin of attraction for health in an uncertain future. Promising alternatives offer structural and ontological frameworks for a social-ecological regime organized by ecological limits, economic contraction, relocalization, and reemerging networks of reciprocal care. Alternatives that emphasize the systemic relationships between human health outcomes and broader ecological, economic, and social contexts are most likely to generate humane structures for health systems in the Anthropocene.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.