
Abstract
Objective
The objective of this study is to investigate the combination effect of anti-muscarinic medication and topical vaginal estrogen in the treatment of overactive bladder (OAB) and female sexual dysfunction in postmenopausal women.
Study design
After IRB approval, 23 female subjects who met the entry criteria were randomized into two groups: (1) fesoterodine (Toviaz®, Pfizer, NY) with topical vaginal estrogen (Premarin®, Pfizer, NY) once daily or (2) fesoterodine once daily alone. If 4 mg fesoterodine was tolerated at 1-week, the dose was increased to 8 mg.
Main outcome measures
Primary endpoints were improvement in OAB symptom severity (Overactive Bladder Questionnaire, OAB-Q SF), improvement in OAB health-related quality of life (HRQL) (OAB-Q SF), and sexual function (Sexual Quality of Life–Female, SQOL-F) after 12 weeks. Secondary endpoint was change in total number of micturitions.
Results
After 12-weeks, the combination group had a significant improvement in OAB symptom severity (p = 0.006), HRQL (p = 0.029), and SQOL-F (0.0003). The fesoterodine alone group also had significant improvement in OAB symptom severity (p < 0.0001), HRQL (p = 0.0002), and SQOL-F (p = 0.02). When compared directly to the fesoterodine alone group, the combination group after 12-weeks had a reduced OAB symptom severity (10 versus 23.3; p = 0.35), higher HRQL (96.9 versus 84.6; p = 0.75), and higher SQOL-F (99 versus 81; p = 0.098). The total number of micturitions over 3 d was significantly reduced in the combination group (45–26, p = 0.03) between baseline and 12-weeks.
Conclusions
The combined effect of fesoterodine and topical vaginal estrogen improved OAB symptoms and sexual function in postmenopausal women.
Keywords
Introduction
The International Continence Society defines overactive bladder (OAB) as urinary urgency, usually accompanied by frequency and nocturia, in the absence of infection or pathology. 1 OAB is associated with lower scores in overall health, quality-of-life, psychological well-being, sexual satisfaction, and work productivity when compared with patient controls.2,3 Prevalence estimates of OAB in women range from 12 to 32%, and increase with advancing age.4–6 OAB is largely underreported; in a population-based survey, only 60% of women with OAB symptoms sought medical treatment, and even fewer (27%) received treatment. 5 Patients with OAB have reported diminished sexual activity and enjoyment of sex 7 and it has also been published that 23% of patients felt that overactive bladder had an impact on their sex life. 8
After failure of conservative methods, anti-muscarinic medications are the first-line treatment for OAB. Anti-muscarinics are safe and well-tolerated therapy that can significantly improve urinary symptoms and quality of life when compared with placebo. 9 Although less utilized as OAB treatment, local estrogen therapy has also shown to significantly relieve urogenital complaints and sexual function.10,11 Previous studies have investigated if the administration of local estrogens in addition to anti-muscarinics could have a synergistic effect in the therapy of overactive bladder (OAB) with conflicting conclusions.12,13 The anti-muscarinic tolterodine alone has been shown to also improve sexual function.14,15
We sought to investigate the combined effect of anti-muscarinic medication and topical vaginal estrogen in the treatment of both overactive bladder and female sexual dysfunction in postmenopausal women.
Materials and methods
This Institutional Review Board approved 12-week trial was conducted in an outpatient setting at a tertiary care facility in a urology practice. This was an unblinded study without placebo. Eligible patients were postmenopausal women with a history of overactive bladder symptoms for at least 3 months, including an average of 8 or more micturitions per 24 h and at least one urgency incontinence episode per 24 h recorded in 3-d bladder diaries at baseline. All participants reported significant OAB symptom bother and reduced quality of life as measured by the Overactive Bladder questionnaire short form (OAB-Q SF). 16 The original 33-item, self-administered OAB-Q contains a symptom bother and HRQL scale. 16 Each item is rated on a six-point response (“not at all” to “a very great deal”) and scored 1–6. We used a validated shorter version (OAB-Q SF) developed by the original authors containing 19 questions (six-items in the symptom bother scale and 13-items in the HRQL scale). 17 In addition, patients also reported the effect of their lower urinary tract symptoms on sexual function by means of sexual quality of life – female (SQOL-F) questionnaire. The SQOL-F questionnaire has been developed to assess the impact of female sexual dysfunction (FSD) on a woman's sexual quality of life. 18 It consists of 18 items and each item is rated on a six-point response (completely agree to completely disagree) and scored from 1 to 6 giving a total score of 18–108 with higher score indicating better female sexual quality of life. 18
Patients with evidence of chronic urologic inflammation, uncontrolled narrow angle glaucoma, recurrent urinary tract infection, and significant stress incontinence were excluded from the study. Patients with a partner with sexual dysfunction, an anatomic disorder of sexual function, a recent major gynaecological surgery, abnormal cervical smear results, history of gynaecological malignancy, and/or uncontrolled hypertension were also excluded. It was calculated that a total sample size to achieve our objectives was at least 21 subjects. With an attrition rate of 10%, 24 subjects per arm were required. However, insufficient numbers of patients were enrolled and the study is presented as a pilot study.
Informed consent was obtained and 23 female subjects who met the eligibility criteria were randomized (computer generated) into one of the two study groups: administration of fesoterodine (Toviaz®, Pfizer, NY, USA) 4 mg once daily with topical vaginal estrogen (Premarin®, Pfizer, NY, USA) or fesoterodine 4 mg once daily (Figure 1). The fesoterodine was taken within 4 h of bedtime, and the topical vaginal estrogen was applied at bedtime. If at the 1-week visit, the 4 mg fesoterodine dose was tolerated, there was a titration to the 8 mg fesoterodine dose. Subjects in both groups remained on the 8 mg fesoterodine dose for the remaining 11 weeks of the study. If subjects were unable to tolerate the 4 mg dose, they exited from the study. The topical vaginal estrogen dose was 0.5 mg (0.3 mg conjugated) per day for 21 d on and 7 d off for treating postmenopausal symptoms. These are the FDA approved dosing regimens.
Study flowchart.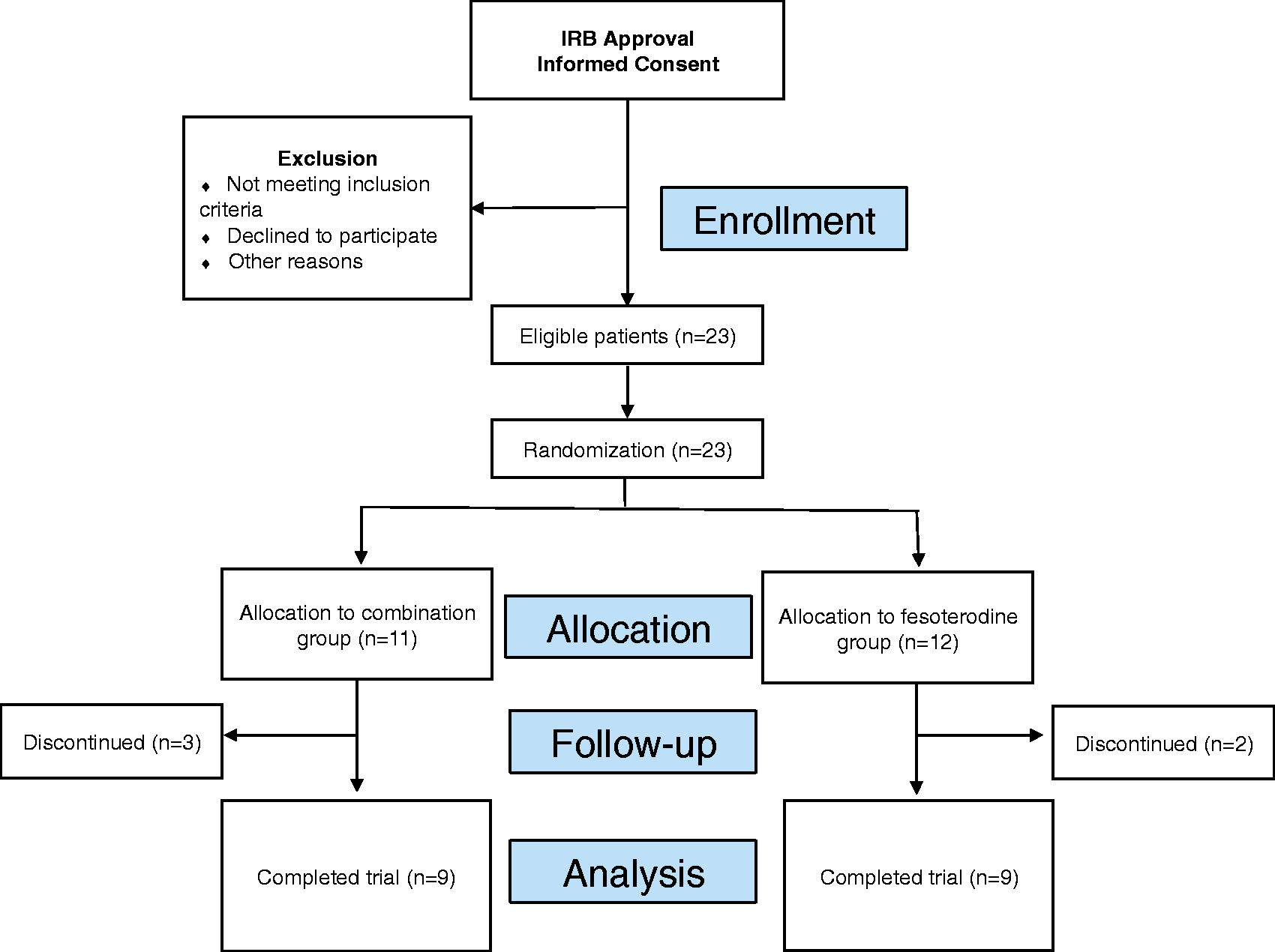
The primary endpoints included improvement in OAB symptom severity (measured by the OAB-Q SF), improvement in OAB health-related quality of life (HRQL) (measured by OAB-Q) and sexual function (measured by the Sexual Quality of Life – Female questionnaire, the SQOL-F) after 12 weeks. Secondary endpoint was changes in the total number of micturitions over 3 consecutive days. Clinic visits took place at baseline: 1, 4, and 12 weeks. Subjects completed 3-d bladder diaries prior to clinic visits at weeks 4 and 12. Diary completion included recording the time of each micturition or UUI episode during three consecutive days. At baseline and week 12, subjects completed the OAB-Q SF to assess symptom bother and the impact of OAB on HRQL and SQOL-F questionnaire. Groups were compared statistically using a non-parametric Mann–Whitney tests and a p value of <0.05 was deemed significant. All analyses were performed using Prism Version 6 (GraphPad Software Inc., CA).
Results
Postmenopausal women were randomized to either a combination of fesoterodine with topical vaginal estrogen or fesoterodine alone. Overall, 11 women were randomized to the combination therapy of fesoterodine with topical vaginal estrogen and 12 women were randomized to the fesoterodine alone group. The median patient age was 55.4 years (range: 40.7–66.6). During the 12-week trial, 22% (n = 5) of women discontinued their medications and were not included in further analysis due to adverse side effects from medication. Adverse effects included dry mouth (n = 3) and constipation (n = 2). There were nine patients remaining in each group at week 12.
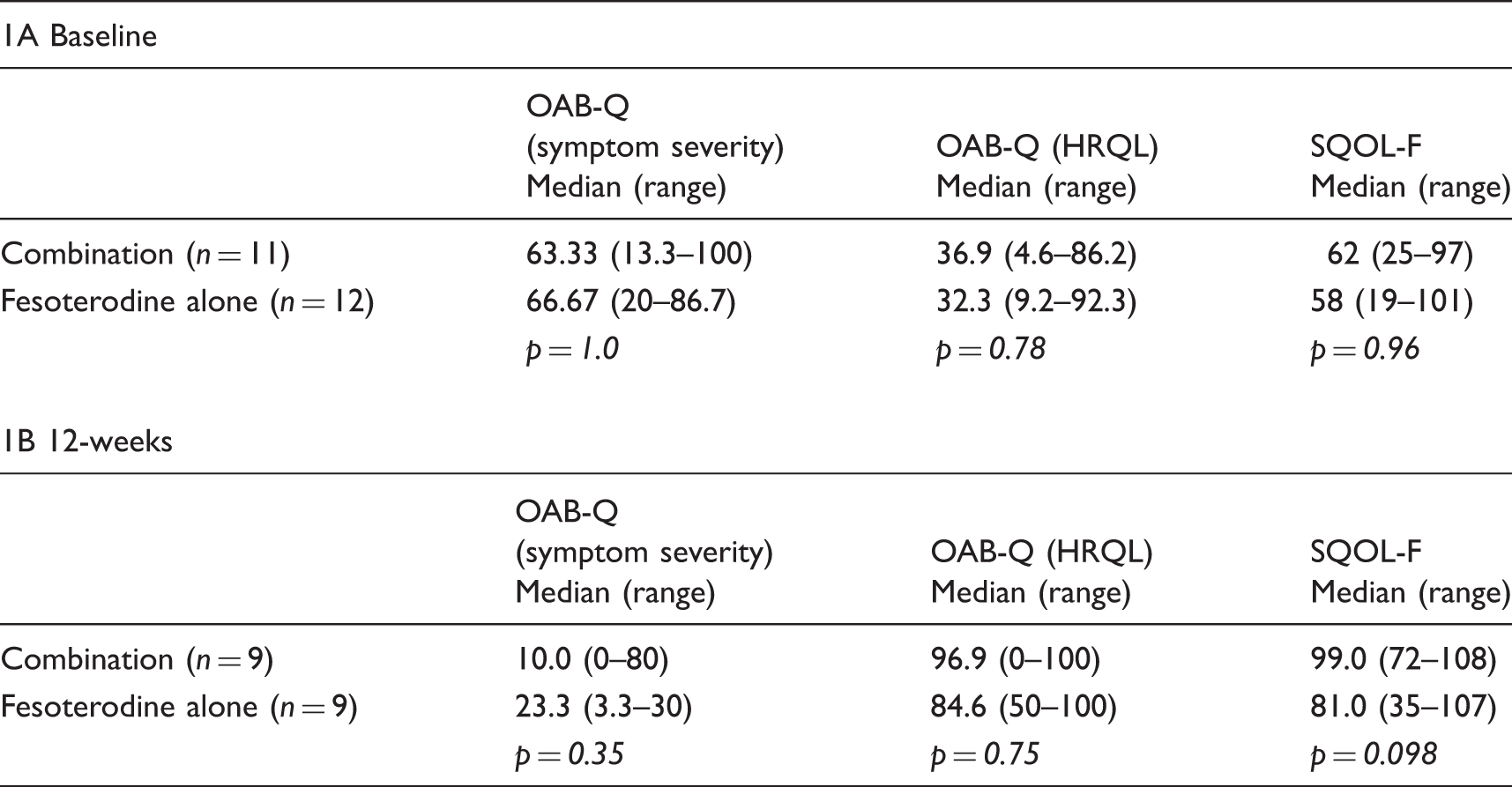
Comparisons of symptoms at baseline (1A) and at 12 weeks (1B).
Changes in scores (median) between baseline and 12 weeks.

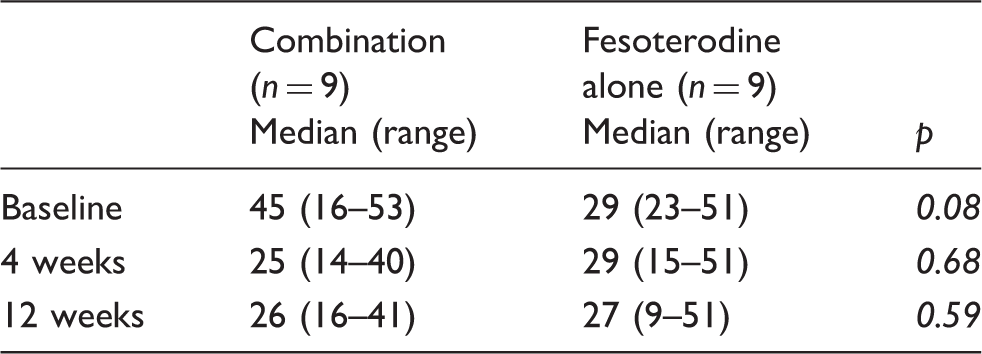
Comparison of micturitions over 3 consecutive days.
Discussion
In our study, we found that the combination of anti-muscarinic medication and topical vaginal estrogen therapy was effective in the treatment of OAB and related sexual dysfunction. At baseline, both groups had similar OAB symptom severity, health quality of life (HRQL), and sexual function scores (SQOL-F). Both groups individually had an improvement in scores at 12 weeks with increased with reduced OAB symptom severity and improved HRQL and SQOL-F scores. While there was no significant difference between combination and fesoterodine alone groups at 12 weeks, the combination treatment recorded a greater reduction in OAB symptom scores, and higher HRQL and SQOL-F scores. When we compared each group individually at baseline and 12 weeks, there were significant improvements noted. The number of micturitions over 3 consecutive days significantly reduced in the combination group between baseline and 12 weeks.
A 2008 study by Serati et al. concluded there to be no synergistic effect of anti-muscarinics and local estrogens in improving the symptoms of OAB. 12 In a non-randomized approach, 129 women were prescribed tolterodine alone (4 mg once daily) and 100 women were prescribed both tolterodine and oestriol cream (once daily) for 12 weeks. Both treatment groups had similar efficacy rates in terms of cured (62.8% versus 62%, p = 1), improved (17.8% versus 20%, p = 0.73), and non-responders (19.4% versus 18%, p = 0.86). All non-responders were found to have higher rates of urodynamically detrusor overactivity following provocative manoeuvres (p < 0.001) and coital urinary incontinence at orgasm (p = 0.01). These conclusions are limited by the lack of a randomized design of the study and utilization of an asymmetric three-item scale for treatment efficacy, which may not have shown a benefit. The study also was not powered to show less than a 12% difference.
In contrast, Tseng et al. found a positive synergistic effect with anti-muscarinic medication and estrogen combination therapy. 13 In 2009, 80 postmenopausal women with OAB were randomized into 12-week treatments of either tolterodine alone (2 mg twice daily) or tolterodine and vaginal estrogen (twice weekly). They concluded that after 12 weeks the tolterodine and estrogen combination significantly improved mean voiding frequency (5.8 versus 6.4, p = 0.001) and voided volume (141.9 versus 134.5, p = 0.007), but no significant difference was seen in urgency, nocturia, or urge incontinence. Quality of life was defined by the urogenital distress inventory (UDI-6) and the incontinence impact questionnaire (IIQ-7). After 12 weeks, the tolterodine/estrogen group recorded a significantly lower score for subjective perception of bladder problems than the tolterodine alone group (p < 0.001 for both questionnaires). The positive synergistic effect with anti-muscarinic medication and estrogen combination therapy seen by Tseng et al. 13 may be explained by including women with symptoms of OAB as opposed to the lack of a synergistic effect seen by Serati et al. 12 who included only women with urodynamic proven detrusor overactivity. The trends we observed in our cohort were similar to that of Tseng et al. where the total number of micturitions, symptom severity, and quality of life significantly improved to a greater extent for the combinations patients than the tolterodine alone.
Our study utilized a more recently developed anti-muscarinic, fesoterodine, which has been proven effective particularly in patients who may have had a suboptimal response to initial therapy. 19 Fesoterodine is well tolerated in women and has proven more effective than tolterodine. 20 A 2009 trial randomized 1548 women to placebo, fesoterodine 4 or 8 mg, or tolterodine-extended release (ER) 4 mg for 12 weeks. The fesoterodine 8 mg was significantly more effective in improving OAB symptoms and exhibited a dose–response relationship. In 2011, a large multicenter randomized trial similarly found fesoterodine 8 mg superior to tolterodine ER 4 mg in as early as 3 weeks. 21 In patients unsuccessfully treated with tolterodine, 4 mg of fesoterodine was found to be efficient within only a week of treatment. 22
We also noted that both groups had an improvement in sexual function, which was assessed by means of a validated questionnaire SQOL-F. The combination group had a significant increase in SQOL-F scores after 12 weeks of treatment (56–99.0, p = 0.008), as did the fesoterodine alone group (51–81, p = 0.02). When both groups were compared at 12 weeks the combination group had higher scores of 99 compared with 81 in the fesoterodine alone group (p = 0.098). Zahariou et al. 23 previously reported that females with OAB reported higher rates sexual dysfunction compared with a healthy population. The assessment of sexual function in females with OAB has also been recommended by Coyne et al. 7 in the EpiLUTS study. Tolterodine has been shown previously to improve sexual function by Hajebrahimi et al. in a cohort of 30 female patients who were assessed using the Arizona Sexual Experience Scale after 3 months of treatment with the drug. 14 Rogers et al. 15 also showed improvement in SQOL-F scores following treatment with tolterodine. While our comparison between combination and fesoterodine alone groups at 12 weeks for sexual function did not achieve significance, we did note an increase SQOL-F score with combination treatment.
The use of topical vaginal estrogen has been linked to improvement of urinary complaints, 10 and was shown in this study to reduce micturations, decrease OAB severity, and improve HRQL and SQOL-F scores. Previous animal studies have demonstrated that estrogens reduce the frequency and amplitude of detrusor contractions and hence promote relaxation of the detrusor muscle.24,25 Vaginal estrogen is also utilized in the treatment of vaginal atrophy, a prevalent disorder resulting in dryness, burning, and dyspareunia. Topical vaginal estrogen can significantly improve vaginal atrophy symptoms and overall sexual function. 26 Topical estrogen has been shown to improve sexual function in postmenopausal women. Raghunandan et al. 11 studied the effects of local estrogen with or without testosterone on sexual health in postmenopausal women. They concluded that after 12 weeks of treatment local estrogen alone or with an androgen is highly effective in improving sexual function. Our study demonstrates that a positive effect is also found with the newer anti-muscarinic, fesoterodine.
Limitations of our study arise from the unblinded nature of the trial and the absence of a placebo. The study was underpowered and is presented as a pilot study. In addition, patient drop out was not insignificant (22%). Poor adherence to anti-muscarinic therapy is common, and is frequent due to adverse side effects 27 and is standard among OAB studies.28,29 In our study, comparisons between the groups’ results produced large differences, although the differences were not consistently statistically significantly. A larger multi-centre trial could overcome this limitation.
Conclusion
The combination of fesoterodine and topical vaginal estrogen can effectively relieve the symptoms of overactive bladder and improve sexual function. This treatment may be preferential for patients who were previously unsuccessfully treated for OAB with tolterodine and/or vaginal estrogen. Further studies with larger defined subgroups and randomization are needed.
Footnotes
Acknowledgements
Statistical analysis support provided by the Research Design and Biostatistics Core of the Weill Cornell Medical College Clinical and Translational Services Center, under the direction of Dr. Paul Christos.
Authors’ Contributions
Bilal Chughtai: Project development, data collection/management, data analysis, manuscript writing/editing James C.: Data analysis, manuscript writing/editing Jessica Buck: Manuscript writing/editing Tirsit Asfaw: Project development, Data collection/management Richard Lee: Project development, Data collection/management Alexis E. Te: Project development, Data collection/management Steven A. Kaplan: Project development, Data collection/management
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical standards
This study has been approved by the Weill Cornell Medical College Institutional Review Board and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Funding
Funded by an investigator-initiated research grant provided by Pfizer, Inc. As the clinical fellow in voiding dysfunction at Weill Cornell Medical College, Dr J Forde is supported by ‘The Frederick J. and Theresa Dow Wallace Fund of the New York Community Trust’