
Abstract
Objective
The aim of this study was to repeat a previous audit, performed from 2009 to 2013, for the cohort of 2018 to determine how the resistance rates in urinary pathogens in women over 18 years of age have changed. A secondary aim of the study was to use resistance data from a different UK hospital in the same year to compare differences in resistance rates across different geographic locations
Study design
This was a retrospective study of all positive urine cultures grown from female patients attending two different hospitals in the year 2018. Resistance patterns were analysed.
Results
The resistance rate to co-amoxiclav continues to increase with amoxicillin retaining high resistance patterns. There are some significant differences in resistance patterns between the different locations.
Conclusion
Antimicrobial resistance is a significant problem in the UK particularly in antibiotics used to treat UTI. These patterns can vary across different geographical locations and over time; therefore, up-to-date knowledge of local anti-biotic resistance is essential when making an appropriate prescription choice.
Introduction
The inability to treat common infections effectively is at risk of becoming a global health crisis. 1 In 2014, the World Health Organisation published a report highlighting the extent of this problem, and offering solutions. Many national Governments have taken action recently to address the threat of antimicrobial resistance (AMR). As a result of that report, we audited and published our results on the antibiotic susceptibilities of bacteria isolated from adult, female urine samples from a UK Specialist hospital between 2009 and 2013. This audit demonstrated a concerning increase in resistance to ciprofloxacin and co-amoxiclav, two of the broadest-spectrum options for oral treatment of urinary tract infection (UTI). 2 Since that time there has been growing recognition of the global importance of AMR. In 2019, the UK Government published its second five-year national action plan, which defined standards across 15 areas of practice, including strengthening antibiotic stewardship. 3 Concurrently, the English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) published a report that estimated 165 severe infections with AMR were diagnosed per day in 2018 in England and there was a 22% increase in the rate of blood stream infections. 4 Escherichia coli is not only the most commonly implicated organism in UTI but also in bloodstream infections, probably secondary to infection of the urinary tract. 4 There is evidence of increasing AMR in E. coli and mortality rates for patients infected with these resistant bacteria are higher than for non-resistant. 4 In response to these further reports, we re-audited our results and added a second hospital with a different population.
Background
Urinary tract infections (UTI) are the most commonly diagnosed bacterial infections in primary care 5 and are therefore a source of a large number of antibiotic prescriptions. The number of prescriptions along with the mechanism of transfer of resistance in the target organisms contributes to the high prevalence of AMR amongst urinary pathogens. 6 This has been shown in a recent Scottish study which demonstrated a dose-related response between prescription and multi-antibiotic resistance. 7
On-going surveillance of antibiotic resistance and tailoring of the local antibiotic regimen with regular amendments, may help reduce or slow AMR, 8 as well as being important in ensuring that patients receive effective empirical antibiotic treatment. This is especially important given that NICE Guidance recommends that the majority of women with uncomplicated UTI are treated empirically without culture confirmation of their infection. 9
Aim
The aim of this study was to repeat the 2009-–3 audit for the cohort of 2018 to determine how the resistance rates have changed. A secondary aim of the study was to use resistance data from a different UK hospital with a general hospital practice in the same year to compare differences in resistance rates across different geographic locations. Finally, we discuss these results in the context of recently published NICE antimicrobial prescribing guidance.
Methods
This was a retrospective study of all positive urine cultures grown from female patients attending Birmingham Women’s and Children’s NHS Foundation Trust (BWH) for 2018. BWH is an inner city, tertiary specialist hospital in the UK which manages Obstetric and Gynaecological patients. Resistance rates of Enterobacteriaceae were compared to the 2013 study.
Positive urine cultures were also identified from women attending King’s College Hospital (KCH), London. This is also an inner city, tertiary hospital but manages multiple specialties.
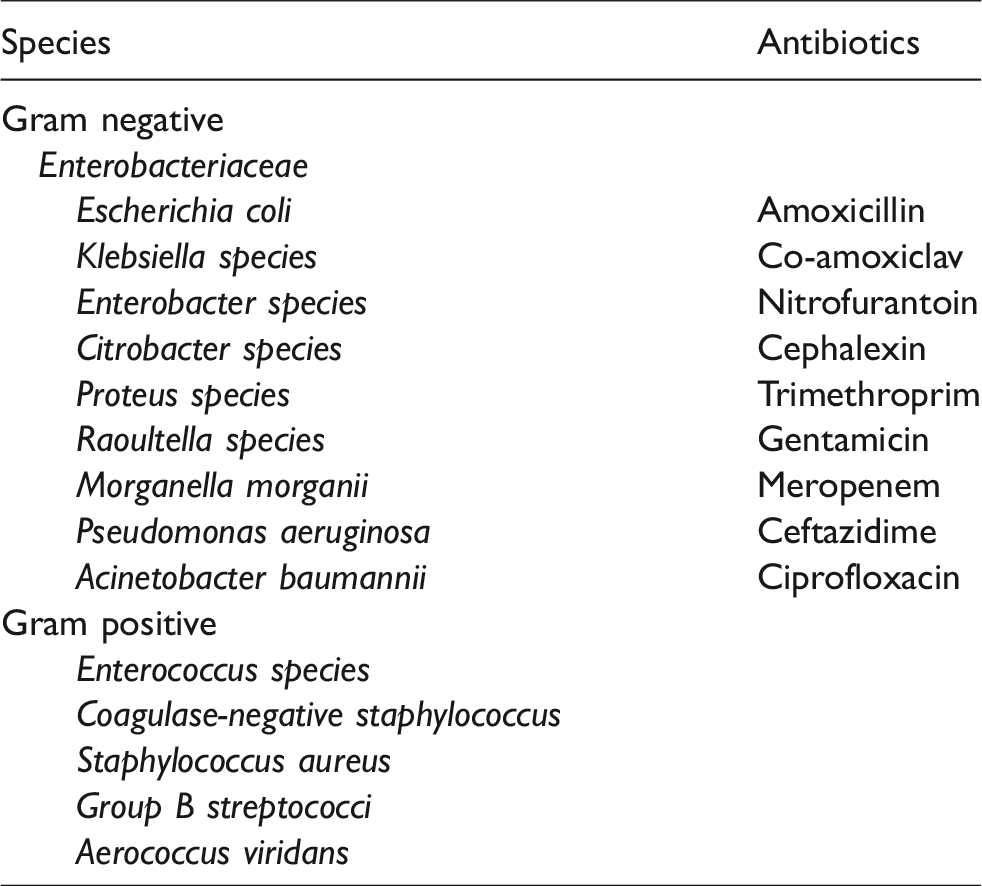
Pre-defined species were identified (see Table1) and antibiotic resistance analysed.
The data were compared at BWH from the 2013 audit and also with the 2018 data from KCH and Chi squared was used to look for significant differences.
Classification of urinary tract infection
UTI refers to the presence of bacteria in the urinary tract, either in the kidneys (pyelonephritis), bladder (cystitis), or urine (bacteriuria). UTIs can either be uncomplicated or complicated. Uncomplicated refers to a UTI where there has been no recent antibiotic treatment, no recent instrumentation, and no functional anatomical abnormality of the genitourinary tract. If any of the above is present in the setting of a UTI, they are referred to as complicated UTIs. 9
Current diagnostic criteria are defined by positive urine culture which is the growth of a single organism ≥104 colony-forming units (CFU), mixed growth ≥105 with one predominant organism, e.g. E. coli or Staphylococcus saprophyticus ≥103. 10 Organisms grown are often similar to gut or vaginal bacteria. 11 However, this has been challenged as artificial and based on flawed research originally by Kass 12 and it is possible that the diagnosis of UTI needs to be re-examined.
Results
From the year 2018, there were 855 samples with a positive culture obtained from BWH compared to 8425 at KCH. The range of species grown at the two different hospitals was not significantly different and is illustrated in Figure 1. The most commonly grown species at both hospitals was E. coli followed by Klebsiella sp.
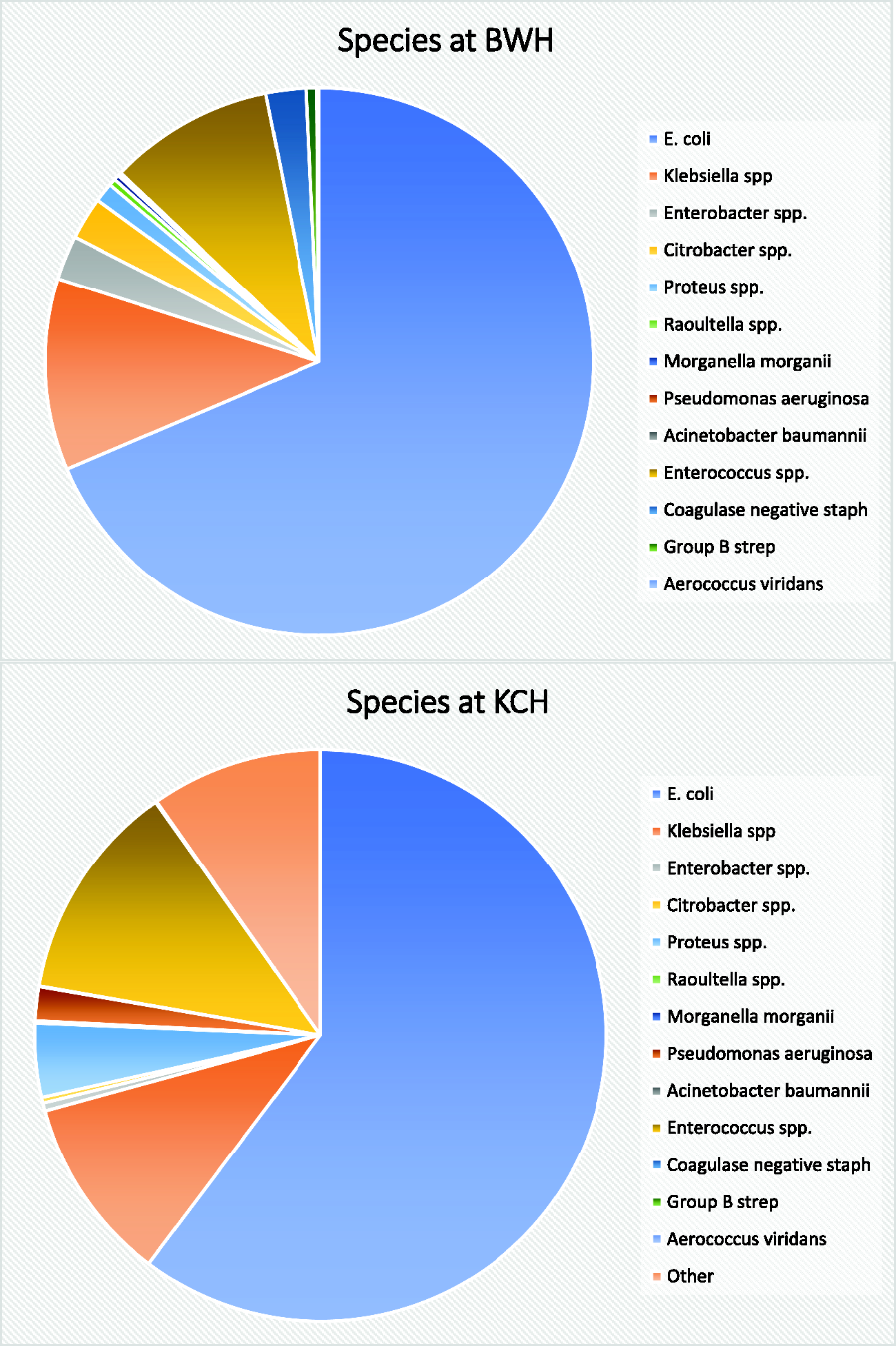
Different species grown in urine culture at BWH and KCH.
We analysed specimens growing Enterobacteriaceae listed in Table 1 and found a very high rate of resistance to amoxicillin (58% at BWH and 60% at KCH). Lowest rates of resistance were to meropenem with no samples being resistant at BWH and only one from KCH.
Different species and antibiotics studied.
When the differences in resistance patterns for Enterobacteriaceae were compared between BWH and KCH, the only significant difference was for co-amoxiclav, with a resistance rate of 36% at BWH compared to only 12% at KCH (p < 0.01). All other species had statistically similar resistance across the two sites, see Figure 2.
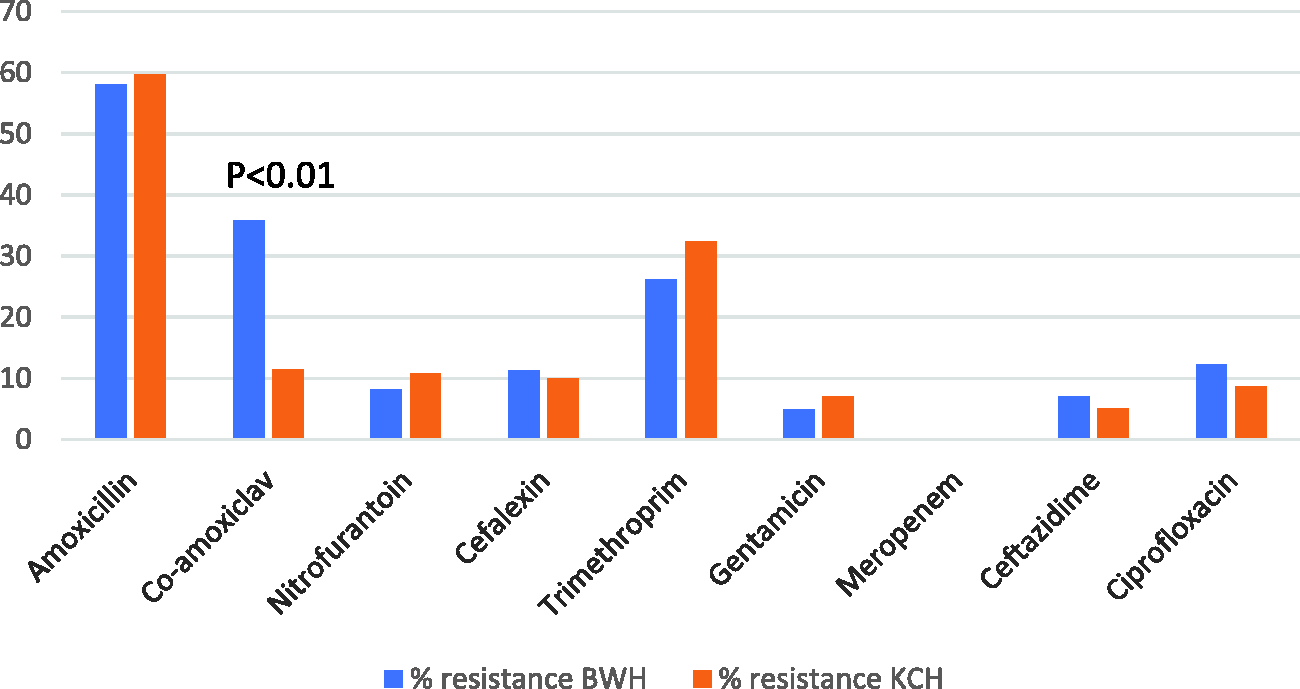
Resistance of Enterobacteriales in BWH and KCH.
Table 2 summarises the rates of antibiotic resistance categorised by species of Enterobacteriaceae. Across both sites, there were high resistances to amoxicillin.
Comparison of resistance between BWH and KCH by species and antibiotic.
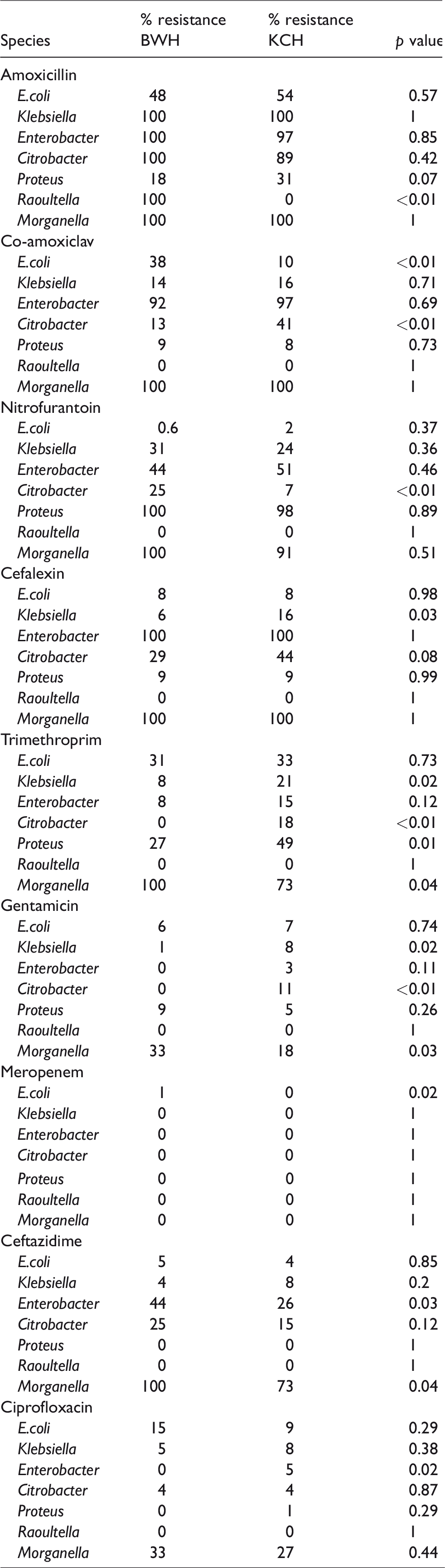
While trimethoprim did not have significantly different resistance rates across the two sites or Enterobacteriaceae as a whole, when broken down for distinct species, differences emerged. Klebsiella sp. were significantly more likely to be resistant to trimethoprim at KCH compared to BWH (21% vs. 8%, p = 0.02) as were Citrobacter (18% vs. 0%, p < 0.01) and Proteus (49% vs. 27%, p = 0.01). The trend with trimethoprim was reversed for Morganella (73% at KCH vs. 100% at BWH, p = 0.04).
As E. coli is the most common pathogenic organism in UTI, the rates of resistance over time have been compared in Figure 3. Data from a previous study 9 were used to identify changes in resistance patterns over time. There has been a significant increase in resistance to co-amoxiclav at BWH with a doubling from 2013 to 2018 (19% to 38%). Nitrofurantoin resistance remains low both at BWH and KCH (0.6% and 2%).
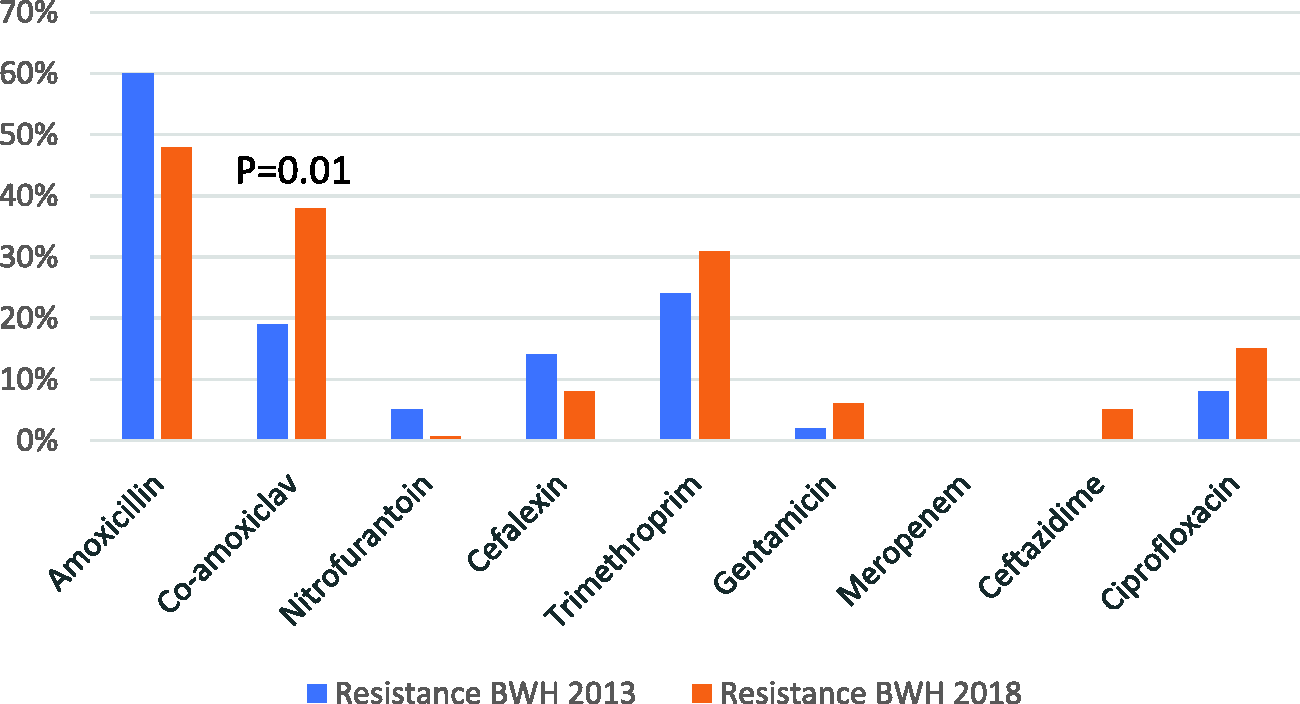
Differences in E. coli resistance between 2013 and 2018.
Treatment of uncomplicated UTI’s
Antibiotic therapy
In October 2018 NICE published guidance on antimicrobial prescribing for lower urinary tract infection. This guidance recommends the use of nitrofurantoin as the first-line treatment option in the management of uncomplicated UTI’s. 9 Nitrofurantoin is an antibiotic with bacteriostatic and bactericidal properties, which disrupts both cellular respiration and the synthesis of nucleic acids. This NICE recommendation is supported by evidence which shows that nitrofurantoin lacked a dose–response relationship with resistance, unlike other antibiotics. 13 It suggests increasing antimicrobial stewardship through education about delayed prescribing, increased prescriptions of nitrofurantoin by 5-fold in contrast to other antibiotics. Despite these benefits, since nitrofurantoin has low tissue penetrance, it can only be used for uncomplicated urinary tract infections 2 a fact which is frequently overlooked by those responsible for prescribing. Another drawback is that Proteus and other Proteaceae are intrinsically resistant to nitrofurantoin.
Nitrofurantoin has a rare but significant side-effect of pulmonary toxicity, which occurs in 1% of patients. 14 There are acute and chronic forms of pulmonary reaction to nitrofurantoin. Acute toxicity is a hypersensitivity reaction and usually presents one to two weeks after starting treatment, with an acute onset of fever, dyspnoea, chest pain, cough and rash. Pulmonary oedema may also be present. Symptoms usually resolve within a few days of stopping nitrofurantoin. Chronic pulmonary toxicity due to nitrofurantoin is less common than the acute form. The onset is insidious over months or years and symptoms comprise dyspnoea, dry cough and fatigue. Nitrofurantoin has been shown to produce oxygen-generating compounds and toxic metabolites, which are probably responsible for chronic pulmonary toxicity. The development of chronic interstitial lung disease is related to the total lifetime dose received, and is more common in the elderly in whom declining renal function presumably leads to toxic accumulations. Nitrofurantoin should be stopped at the first signs of pulmonary toxicity and, in most patients, there is a gradual resolution of symptoms over several months. If pulmonary toxicity is not detected and allowed to progress, interstitial lung disease and pulmonary fibrosis can develop, with serious long-term effects. 15 It has been suggested that people suffering serious adverse reactions to nitrofurantoin should carry written warnings about re-exposure.
The other NICE-recommended first-line antibiotic for use in UTI is trimethoprim (with the proviso that there should be a low rate of resistance). Trimethoprim works by disrupting bacterial DNA synthesis. 9 However, resistance to trimethoprim remains rather high and there is evidence that indicates that reducing the prescription of trimethoprim has little impact on the long-term resistance rates in the population, signifying a potential danger with use of this drug. 16
The second-choice antibiotics recommended by NICE are pivmecillinam (a penicillin) or fosfomycin, 8 the latter has the advantage of being a single 3-g oral dose. The use of these drugs in the UK has been constrained by the fact that many laboratories do not test or report susceptibilities to these agents. The European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidance that most laboratories in the UK follow recommends that agar dilution is the reference method for susceptibility testing; with fosfomycin, the situation is made even more complicated by the requirement to include glucose-6-phosphate in the medium.
Pivmecillinam is a prodrug of mecillinam, a synthetic penicillin that is active against Gram-negative bacteria, but not Pseudomonas aeruginosa. Like other beta-lactam antibiotics, mecillinam inhibits bacterial cell wall synthesis, although its mode of action appears to be different to that of other penicillins. Importantly, mecillinam has good beta-lactamase stability, and in vitro is active against at least some extended-spectrum beta-lactamase producing strains of Enterobacteriales. In contrast to increasing levels of resistance against other beta-lactams, the resistance levels to pivmecillinam remain low. 17 However, there is a surprising lack of data on the clinical effectiveness of mecillinam. A recently published cohort study from Norway reported that pivmecillinam given at 400 mg three times daily (rather than the more usual 200 mg) gave comparable clinical and bacteriological cure rates in women with community-acquired E. coli UTIs irrespective of ESBL production. 18 However, the authors of this study did not characterise the types of ESBL. Another approach that appears to improve the activity of mecillinam is to administer it with a beta-lactamase inhibitor, but such combinations are not commercially available.
Fosfomycin is a broad-spectrum bactericidal antibiotic that is effective against Gram-positive and Gram-negative bacteria, including multi drug resistant (MDR) Gram negative bacteria and MRSA. This antibiotic has good tissue penetrance and is excreted unchanged in the urine. 19 Whereas resistance to fosfomycin arises rapidly in vitro, resistance is rarely seen during therapy of UTIs, seemingly because of the low virulence of the resistant organisms and high urinary levels of fosfomycin attainable. Until now, most fosfomycin resistance has been due to mutations, but plasmid-borne resistance, linked to resistance to other drug classes, has also been reported. This presents a significant threat to the future use of fosfomycin, as it becomes increasingly prescribed as therapy for infections with MDR pathogens at sites other than the urinary tract. 20
For use in pregnancy, amoxicillin or cephalexin is recommended. These beta-lactam antibiotics work by inhibiting cross-linkage of the peptidoglycan cell wall of bacteria. NICE Guidance advises that amoxicillin should only be prescribed after susceptibility testing has been performed, 9 and our data confirm that, with high resistance rates. Cephalosporins have a broader range of activity than amoxicillin, which is largely because of better beta-lactamase stability. However, this broad spectrum of activity brings disadvantages such as selection of antibiotic-resistant bacteria including MRSA and ESBL; candidiasis and Clostridioides difficile. In pregnancy, these drawbacks are outweighed by knowledge that cephalexin is safe to use in pregnancy, but in other settings cephalsoporins should be reserved for complex infections that have not responded to first-line treatment.
Fluoroquinolones are bactericidal agents which also inhibit DNA synthesis. They are used less widely than other agents due to their adverse effects. They can cause gastro-intestinal upset which may render them unacceptable to patients, but also have more serious side effects such as prolongation of the QT interval, tendinopathy and possibly Clostridium difficile-associated diarrhoea. 21 These agents should be reserved for patients who have penicillin allergies or if first-line treatment fails and where there is clear microbiological proven evidence for their use. In March 2019, the MHRA issued new restrictions and precautions on the use of fluoroquinolones due to very rare reports of disabling and potentially long-lasting or irreversible side effects. These included advice that these drugs should not be used for uncomplicated cystitis unless other antibiotics are inappropriate, to avoid co-administration with corticosteroids, and to prescribe with special caution in people older than 60 years.
Gentamicin is an aminoglycoside antibiotic with bacteriostatic action against a wide range of aerobic bacilli. Due to its high activity even with a large bacterial inoculum, it is used widely for single dose prophylaxis particularly following instrumentation of the bladder. It has serious side-effects of damage to the inner ear and can only be given intra-venously so therapeutic use tends to be limited. 22
Alternatives to antibiotics
It is thought that some behavioural or hygiene practices may be associated with an increased risk of UTI, some of which may be supported by (low quality) evidence and/or anecdote. There are data that suggest that increasing water intake can reduce UTI 23 and that women who regularly use spermicidal agents as well as those on the combined oral contraceptive pill, have an increased risk of UTI. 24 It is known that voiding fewer than three times a day is associated with higher risk of UTI 25 and frequent voiding can be protective. 26 Toileting habits such as the use of feminine/baby wipes can be associated with UTI. 27 A popular non-antibiotic treatment for UTI is cranberry juice/products and some studies showed benefit; however, a Cochrane review demonstrates little benefit from these and concludes that they cannot be recommended for prevention of UTI. 28 D-mannose is a sugar derived from cranberry juice, and a small RCT suggested that it is as effective as nitrofurantoin at preventing UTI. 29 Hence, NICE has suggested that non-pregnant women may find D-mannose useful.
Despite the lack of evidence regarding lifestyle changes, patients are commonly given advice based on sensible principles which may help prevent UTI. This includes avoiding constipation, drinking water, voiding after (not before) intercourse and avoiding vaginal penetration following anal intercourse.
There are other pharmaceutical, non-antibiotic treatments available to women suffering from UTI.
Methenamine Hippurate is a substance that breaks down to ammonia and formaldehyde in acidic urine, making the bladder inhospitable to bacteria. A Cochrane review showed that it is effective at preventing UTI when used as short term prophylaxis. 30
Estrogen has an important role in the urinary tract and it is clear that there is an increase in frequency of UTI in the post-menopausal population. Exogenous estrogens can decrease the vaginal pH and reverse the microbiological changes associated with the menopause. 31 Data from a limited number of studies show that vaginal estrogens can decrease the number of UTIs in post-menopausal women. 32
A recent advance in the treatment of UTI is the development of a vaccine against particular strains of E. coli, Klebsiella, Proteus and Enterococcus faecalis UTI. It is a sub-lingual preparation which works by stimulating a host immune response against these bacteria. A study in the UK has shown a 78% reduction in UTIs in women treated with Uromune vaccine. 33 It is not currently widely used, and further data are required to confirm its effectiveness.
Discussion
In this study, we have revisited our results from urine culture and identified a change in resistance pattern of E. coli from 2013 to 2018 in a single UK Women’s Hospital. We also found differences across two geographical locations. We have shown that across the two sites, E. coli is the most common organism grown in urine cultures, followed by Klebsiella sp.
E. coli has high rates of resistance to amoxicillin which have been consistent over time at BWH as well as almost a third of samples showing resistance to Trimethoprim. Over the time period of five years, the resistance to co-amoxiclav has doubled from 19% to 38%. A previous audit 2 showed an increasing rate of resistance to co-amoxiclav in E. coli at BWH (11% to 19% between 2009 and 2013). Recommendations were made at the time to avoid using co-amoxiclav as a first-line agent for UTI. Unfortunately, the trend has continued despite this suggested antibiotic stewardship.
Enterobacteriaceae represent a majority of the cultured organisms at both locations. The resistance patterns are similar to those of E. coli with high rates in amoxicillin and almost zero to meropenem. Whilst amoxicillin is a readily available antibiotic taken orally, meropenem can only be administered parenterally, thus making its use less convenient.
When resistance patterns of Enterobacteriaceae were compared across the two sites, they were similar. The only significantly different finding was for co-amoxiclav which showed a much higher resistance at BWH. This may be due to different prescribing regimens at the different hospitals.
E. coli as the primary causative agent in UTI has been well established. Reported rates are around 60% in England 34 and up to 80% in Europe35–37 this is likely because it is the most prevalent bacteria in the human gastro-intestinal tract. 38 The proximity of the anus to the urinary tract allows passage of the bacteria which can become pathological. Here we have shown that this remains true at BWH and KCH.
Resistance to antibiotics can provide a clinical difficulty in treating UTI. Published data show that E. coli has high resistance rates to amoxicillin in keeping with our findings. 39 E. coli resistance to co-amoxiclav and trimethoprim have been reported as 8% and 23%, respectively, which are both marginally lower than found in this study. 40
A Spanish study between 2003 and 2006 showed an increasing resistance of E. coli to co-amoxiclav over time which fits with the experience at BWH between 2013 and 2018. 41 This was postulated to be due to an increase in community prescription of co-amoxiclav, driving subsequent resistance, whereas in secondary care, prescription rates remained stable. Data from NHS England have shown that the national resistance rate of E. coli to co-amoxiclav has increased from 37% to 43% between 2013 and 2018.
This paper involves a large number of patients across two geographical locations with different demographic and prescribing policies. It adds to national data regarding the incidence of antibiotic resistance in UTIs, how this compares between two different sites, and how resistance changes over time.
Further work that would add to the value of this study would be to obtain prescription data from the same time frame to look at different prescribing patterns and whether these are associated with different resistance patterns. Stratification of samples obtained from primary care and secondary care would enable further comparisons to be made.
Currently, there is a disparity between NICE antibiotic prescribing guidance and the UK Standards for Microbiology Investigations: Investigation of urine, which includes fosfomycin and mecillinam as agents to be considered for supplementary susceptibility testing, and with no recommendation that the results be reported. This situation is likely to remain for the next three years as the NICE guidance was published in October 2018. 9
Conclusion
We again conclude that it essential for all practitioners prescribing antibiotics to have a robust knowledge of local trends for antibiotic resistance and prescribe accordingly. We would recommend this as a key part of antibiotic stewardship alongside consideration of non-antibiotic measures to decrease the incidence of UTI.
A patient presenting at BWH or KCH with a positive urine culture is most likely to grow E. coli. Amoxicillin should not be used to treat UTI as there are universally high resistance patterns.
Rates of resistance to trimethoprim would imply that it is not an effective first-line antibiotic at either BWH or KCH.
Care should be taken with the prescription of co-amoxiclav for UTI (especially at BWH) as there are significant levels of resistance and these appear to be increasing over time. As such, second-line agents such as pivmecillinam and Fosfomycin should be considered.
Nitrofurantoin remains an effective first-line treatment for UTI with low resistance rates in E. coli or across Enterobacteriaceae; however, the clinician should be mindful of the risk of interstitial lung disease when long-term nitrofurantoin is used.
Meropenem and gentamicin should be reserved for drug-resistant bacteria as they have very low resistance patterns across all species.
Supplemental Material
MIN910039 Supplemental Material - Supplemental material for Antibiotic resistance in urinary tract infections: A re-visit after five years and experience over two sites
Supplemental material, MIN910039 Supplemental Material for Antibiotic resistance in urinary tract infections: A re-visit after five years and experience over two sites by Georgina Baines, Adeolu Banjoko, Amalia Brair, Jim Gray, Nergish Desai, Linda Cardozo and Philip Toozs-Hobson in Post Reproductive Health
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LC has been a consultant to Synermed who markets Uromune; PT-H has been a consultant to Synermed who markets Uromune. Other authors state no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Approval for the audit was obtained and document attached.
Guarantor
PT-H.
Contributorship
GB – Data analysis and writing of article.
AB1 – Literature review, writing on manuscript.
AB2 – Literature review, original audit.
JG – Concept design, data collection, reviewing of manuscript.
ND – Data collection, reviewing of manuscript.
LC – Reviewing of manuscript.
PT-H – Concept design, reviewing of manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.