
Abstract
Urogenital atrophy occurs as a result of the effect of estrogen deficiency on the tissue quality in the vulva, vagina, urethra and bladder. It is a common consequence of the menopause, with possibly up to 80% of women experiencing symptoms. Despite a number of different diagnostic methods, there is no validated objective method by which to confirm the diagnosis in clinical practice and research settings. Education, for women and clinicians, is called for to support diagnosis and treatment. However, before this can be of global benefit, development of an accessible and reproducible diagnostic test is required. Current assessment methods include routine history and clinical examination, with the clinician’s opinion based on their subjective observations. A vaginal smear to assess the ratio of superficial to parabasal cells and measurement of the pH of the vaginal secretions is more commonly used in research settings. A number of formulae have been postulated to facilitate the diagnosis including the Vaginal Health Index, the Vulval Health Index, the Genitourinary Syndrome of the Menopause assessment tool, the Genital Health Clinical Evaluation and vaginal biopsy and assessment of the vaginal microbiome. However, none of these potential methods of assessment has been validated. This article focuses on what we do not know about urogenital atrophy including the prevalence, the most appropriate terminology, aetiology, pathogenesis and the most objective and reproducible method of assessment.
Introduction
Urogenital atrophy is a condition affecting urogenital tissue quality as a result of estrogen deficiency. It has been described as a silent epidemic with lack of awareness in both women and clinicians affecting an accurate diagnosis and access to treatment.1–4 The European REVIVE Survey undertaken in 2016, involving participants from four European countries (Italy, Germany, Spain and the UK), concluded that urogenital atrophy is an under-recognised, under-diagnosed and thus under-treated condition and recommended a public awareness campaign with a focus on education. 5 Another survey of women in Latin America, 6 VIVA-LATAM, reached the same conclusions. Lack of awareness influences the number of symptomatic women with an accurate diagnosis who subsequently have access to appropriate treatment. Findings in both studies are compounded by the absence of a simple, accessible and objective diagnostic method, which would inform accurate numbers of affected women and provide a means of assessing response to treatment both in clinical practice and also in clinical trials.6–10 This needs to be developed and validated before raising awareness through education can have any significant impact on the number of women receiving an accurate diagnosis and appropriate treatment. This review paper examines the available evidence relating to diagnostic accuracy of urogenital atrophy and sets the scene to consider what measures need to be taken to improve the utility of current commonly used methods. The information covered is relevant to all clinicians who may encounter women with symptoms related to urogenital atrophy, including gynaecologists, urologists, dermatologists, general practitioners, sexual health clinicians, specialist nurses and practice nurses.
Method
A PubMed (Medline) search was performed using a combination of key words and relevant controlled vocabulary terms related to urogenital atrophy. The keywords used included menopause, vulvovaginal atrophy, genitourinary syndrome, local oestrogen therapy, local estrogen therapy, vaginal oestrogen, vaginal estrogen and CO2 laser therapy. Studies included those investigating urogenital atrophy and treatment for the condition, published from database inception until July 2020.
Definition of urogenital atrophy
There is a diversity of definitions for urogenital atrophy with the common theme being that this condition is a frequent manifestation of estrogen decline. This is most commonly due to the menopause and is associated with specific symptoms, the most common of which are vaginal dryness, itching, irritation and dyspareunia.7–23 Urogenital atrophy also impacts on the tissue quality in the bladder and urethra, but in affected women, the changes are more easily observed and quantified in the vulva and vagina. 24
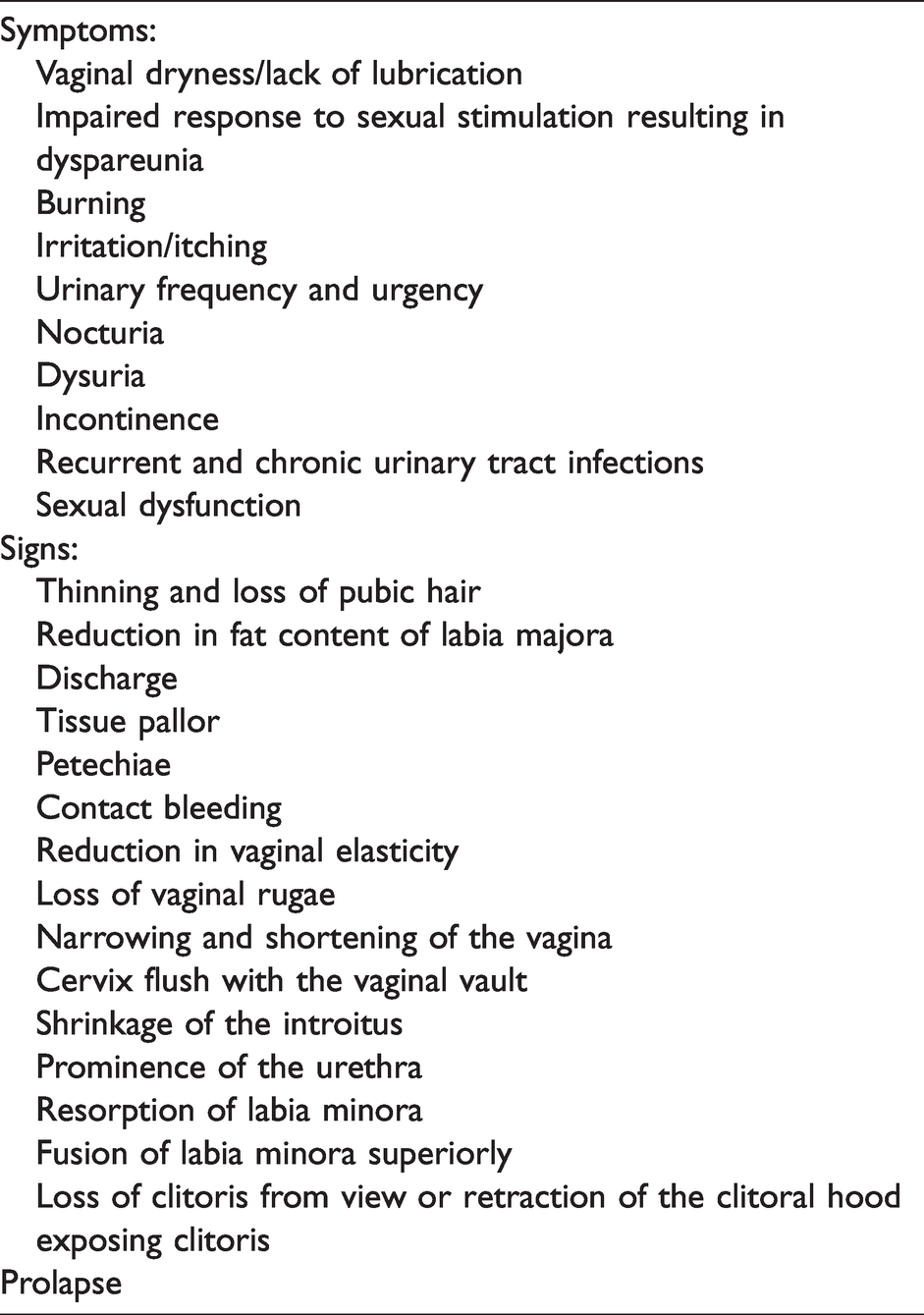
Symptoms and signs associated with urogenital atrophy
In women with urogenital atrophy, there is an alteration in the appearance and function of the vulva, vagina, bladder and urethra. Whilst not a life-threatening condition, urogenital atrophy can have a devastating effect on women and their partners as highlighted by the CLOSER survey, which examined the adverse emotional and physical impact of this condition on postmenopausal women and the repercussions for sexual relationships.25,26 A comprehensive list of potential symptoms and signs are included in Table 1.
Symptoms and signs associated with urogenital atrophy.
Unknown factor 1: Prevalence of urogenital atrophy
Many women accept symptoms of urogenital atrophy as a normal part of aging and as a result do not seek medical help. 25 Lack of a validated method of assessment affects any attempt to correlate urogenital symptoms with clinical findings. 8 The exact number of affected women is thus unknown, with speculative estimates ranging from 10–84% of menopausal women.3,4,24–55 Improving diagnostic accuracy has the potential to improve precision in relation to prevalence rates and to support a more accurate estimate of the burden of the disease.
Unknown factor 2: Most appropriate terminology for the condition
Lack of consensus and frequent changes to terminology have further added to lack of clarity in the diagnosis and management of this condition. In 2014, the International Society for the Study of Women’s Sexual Health and the North American Menopause Society jointly published recommendations in relation to descriptive terminology for urogenital atrophy. 56 The consensus was to use the term Genitourinary Syndrome of Menopause (GSM) in preference to Vulvovaginal Atrophy (VVA), but the British Menopause Society in their consensus statement published in June 2018, refer to changes in urogenital tissue quality due to estrogen deficiency as Urogenital Atrophy. 24 The desire to change the terminology, moving away from terms such as senile vaginitis in addition to VVA is related to negative connotations associated with the word ‘senile’ and the possible suggestion of inflammation/infection associated with the word ‘vaginitis’. VVA fails to include the impact of estrogen deficiency, on the bladder and urethra in addition to the vulva and vagina. GSM may not be the term preferred by affected women, since many would not consider that they have a ‘syndrome’. Considering all of these issues, we chose Urogenital Atrophy as the definitive terminology for this paper. 24
Unknown factor 3: The aetiology of urogenital atrophy
Urogenital atrophy is most commonly a consequence of the menopause, due to the impact of estrogen deficiency and also lower levels of circulating androgens on tissue homeostasis, maintenance and regeneration. 57 Other causes include breast feeding as high levels of prolactin antagonise the production of estrogen, 58 use of depot medroxyprogesterone acetate for contraception, 59 Gonadotrophin releasing hormone analogues (GnRH) analogues which inhibit the hypothalamo–pituitary–ovarian axis, diabetes due to peripheral neuropathy and microvascular disease 60 and side effects of cancer treatments associated with ovarian suppression or failure, particularly breast cancer treatments.61–66 It is not clear why some post-menopausal women are affected, and others are not, irrespective of use of systemic Hormone replacement therapy (HRT). Continuing sexual activity may prevent progression of tissue changes, ‘the use it or lose it’ theory. 27
Unknown factor 4: Pathogenesis of urogenital atrophy
Estrogen is responsible for the normal healthy pink colour and normal secretions of the vaginal mucosa and preserves epithelial thickness and the vaginal rugae. Estrogen deficiency, in addition to affecting mucosal epithelial tissue quality (the epithelium becomes thin, pale and is more easily damaged 67 ), results in hyalinisation and fusion of the collagen fibres in the dermal layer, reducing tissue elasticity in association with fragmentation of the elastin fibres. This can result in bleeding and pain, most notably in association with sexual activity. 1 Not all women with low levels of estrogen have symptoms and/or signs of urogenital atrophy and this is an area for further research as there may be factors beyond estrogen deficiency that contribute to the condition.
Diagnosis of urogenital atrophy
The majority of peri and postmenopausal women are likely to be affected by some degree of urogenital atrophy. Currently, the diagnosis is based on a clinical assessment which includes the history of symptoms and a physical examination. Although a combination of objective and subjective assessments to support the diagnosis has been recommended, 67 no consensus has been reached regarding the best method with which to objectively diagnose urogenital atrophy. 68 Such a method should minimise inter- and intra-observer discrepancy, 6 support diagnosis and inform and monitor the most appropriate treatment. This is of particular value to researchers conducting clinical trials to assess novel treatments.
Diagnostic precision and the right treatment have the ability to reduce any negative effect on sexual function and quality of life.27,69
Unknown factor 5: What is the best method to assess urogenital atrophy?
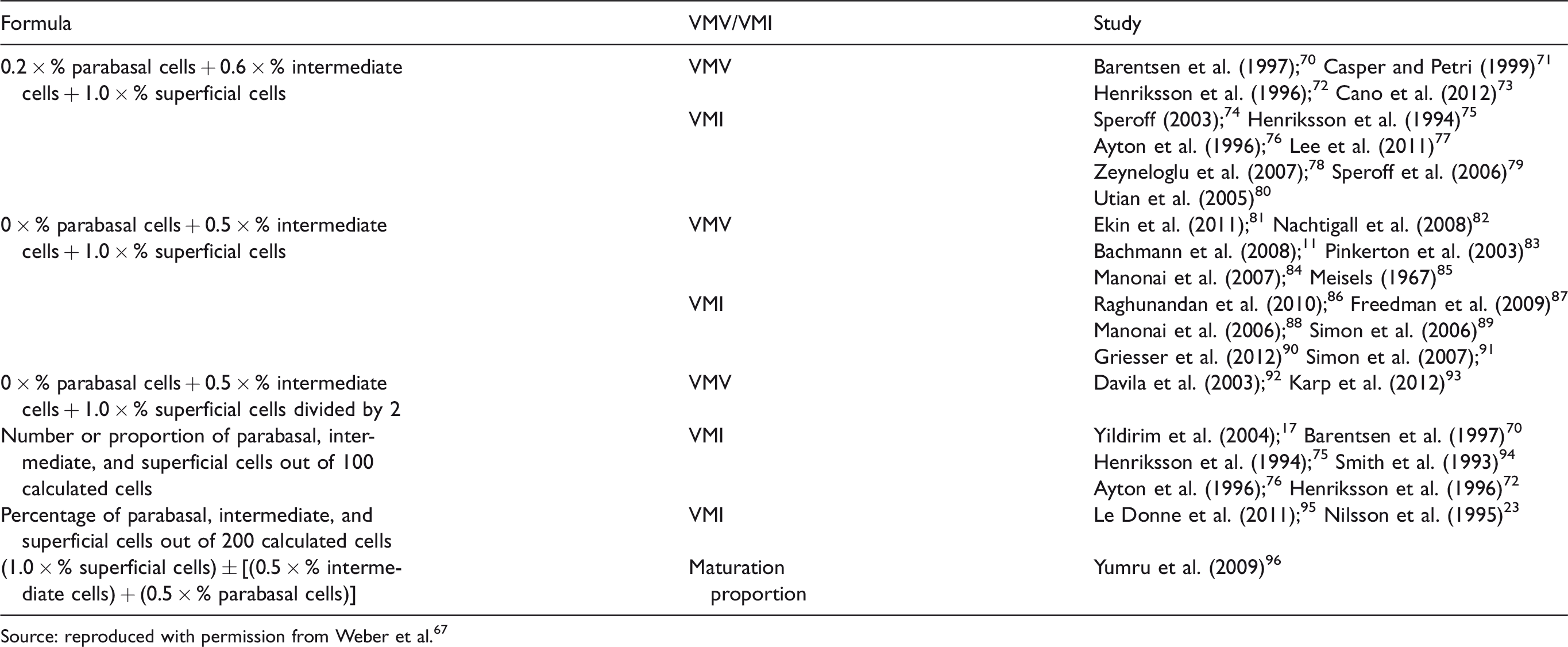
Currently available methods to assess urogenital atrophy
Vaginal Maturation Value (VMV)/Vaginal Maturation Index (VMI) From: assessment of vaginal atrophy: a review. Source: reproduced with permission from Weber et al.
67
Review of existing assessment methods
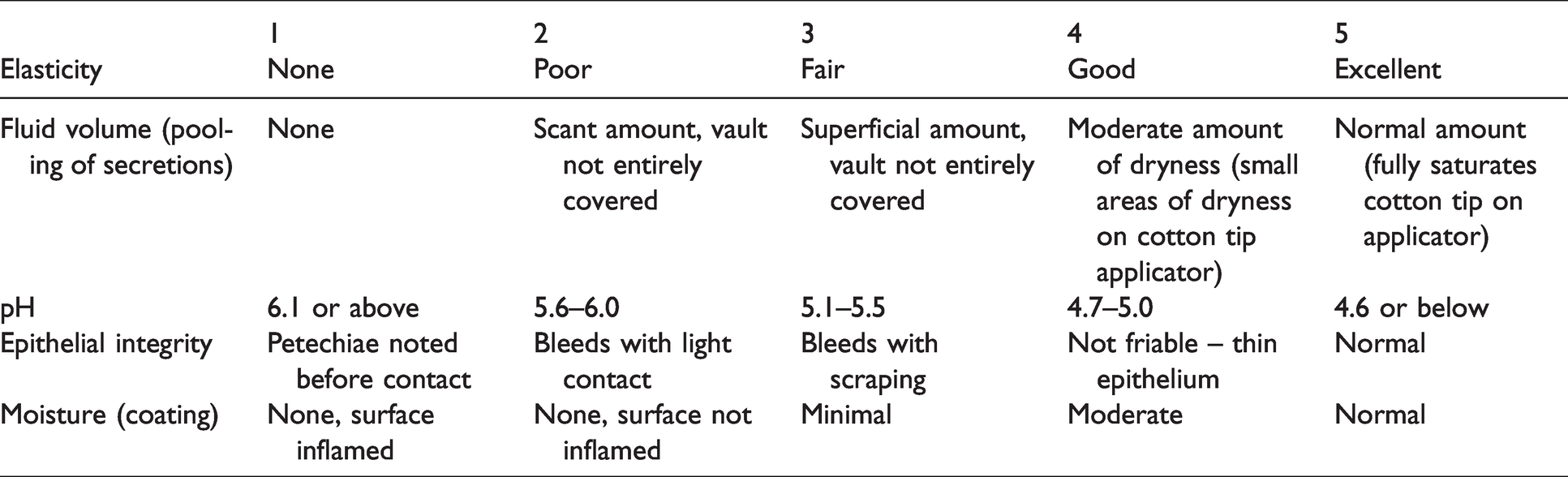
The Vaginal Health Index
This dates back to the early 1990s and was developed by Bachmann. 98 The table below describes how Vaginal Health Index (VHI) is calculated, the lower the score, the less healthy the vagina. Scores range between 5 and 25 with a score of < 15 being indicative of urogenital atrophy (Table 3). The main limitations of this system are that it only assesses the vagina, not the vulva and urinary tract and lacks objectivity. There is no clearly defined method by which to quantify vaginal elasticity, fluid volume, epithelial integrity and moisture.
The Vaginal Health Index (VHI).
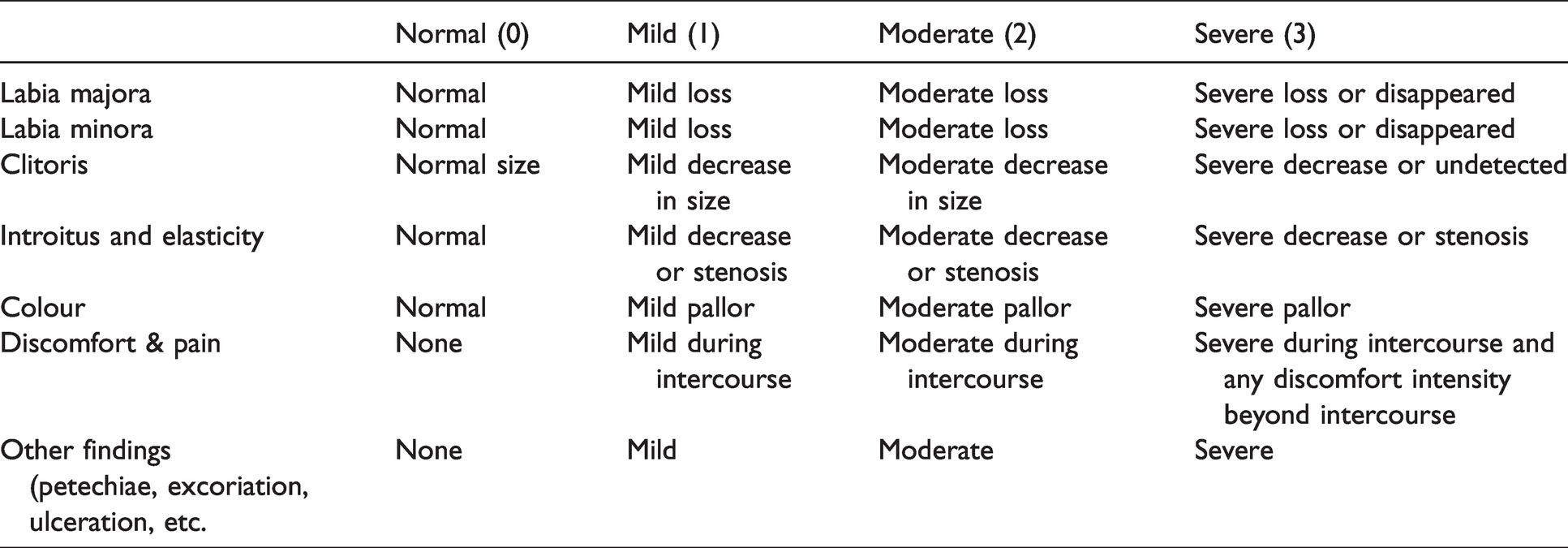
The Vulval Health Index
This tool addresses elements lacking in the VHI, including the appearance of the labia majora, minora, clitoris and introitus, 99 but it is yet to be validated and has similar limitations to the VHI, with lack of objectivity. A score is calculated by adding together individual scores with higher scores indicating more severe vulvar atrophy (Vulval Health Index > 8 or a score of 3 in any category confirms urogenital atrophy) 100 (Table 4).
The Vulval Health Index.
Genitourinary syndrome of menopause assessment tool.
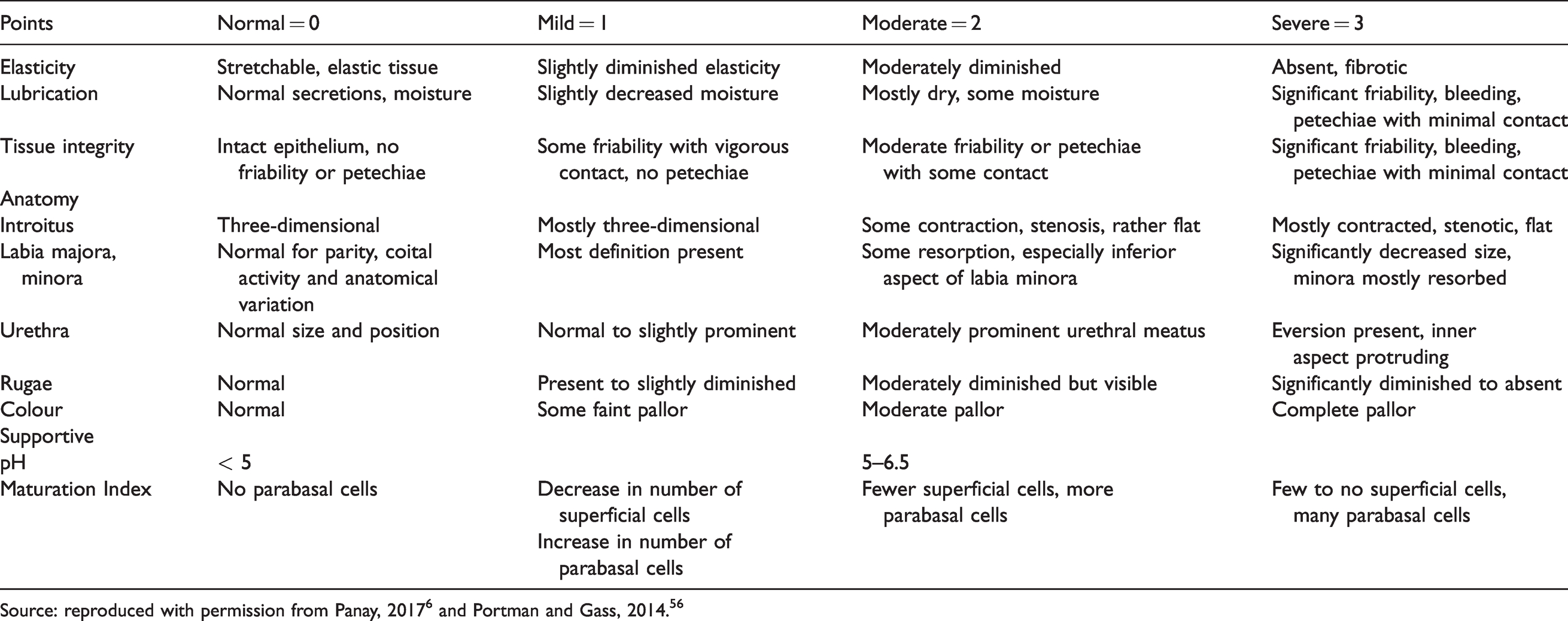
Source: reproduced with permission from Panay, 20176 and Portman and Gass, 2014. 56
The GSM assessment tool (Table 5)
This was developed by the International Society for the Study of Women’s Sexual Health and the North American Menopause Society, but scientific validation is required before it can be incorporated into routine clinical practice.
There are three general categories within this proposed assessment tool for the urogenital tissues:
Elasticity Lubrication Tissue integrity
All of these categories can be scored 0–3 depending on whether the tissues are affected by urogenital atrophy or not, with 0 being normal and 3 the most severely affected.
There is also an anatomical section which includes:
4. Introitus/Prominence of the urethra 5. Vulval anatomy – labia minora, majora 6. Vaginal anatomy – rugae 7. Colour
These categories are also scored 0–3, depending on whether the tissues are affected by urogenital atrophy or not, with 0 being normal and 3 the most severely affected.
Total scores are added together to reach the following degrees of atrophy: < 7 – Mild 7–14 – Moderate >14 – Severe (Maximum score 21)
Summary of limitations of the GSM assessment tool:
The grading for elasticity, lubrication, tissue integrity and the anatomical categories are relatively subjective with limited guidelines on which to base the score (0–3). A more reproducible, objective and validated method of assessment would assist in diagnosing urogenital atrophy, depending on clinical signs. This could be combined with a subjective assessment of symptoms experienced using a validated questionnaire 55 as recommended by Weber and colleagues. 67
Genital Health Clinical Evaluation
A study from India published in 2018 101 assessed symptom score, based on the patient history and a Genital Health Clinical Evaluation (GHCE) score to diagnose urogenital atrophy in women between ages 40 and 75 years. The symptom score was based on the following four symptoms – vaginal dryness, itching, burning and dyspareunia. These were rated as 0 = none, 1 = mild, 2 = moderate and 4 = severe. The GHCE includes a speculum examination and the score is calculated based on the following criteria rated 1–4: vaginal pH, fluid secretion, moisture, vaginal rugosity, mucosal colour and ‘epithelial mucosa’. These scores were compared with the VMI. The study concluded that both symptom score and GHCE score were valid diagnostic alternatives to maturation index. However, despite attempts to make evaluation of urogenital atrophy more objective in this study, assessment remains subjective and provides no improvement on routine basic pelvic examination, including examination of the vulva. No indication is provided as to how to grade the various physical criteria. The GHCE scoring system was used in an earlier study conducted by Raymundo and colleagues in 2004, investigating the impact of topical conjugated equine estrogens on atrophic vaginitis. 102
Vaginal biopsy and other proposed methods of assessment
Although a diagnostic biopsy would support a definitive diagnosis for women with urogenital atrophy, 103 this is not a practical solution and a less invasive method, for use especially in a primary care setting, is required in order to support an accurate diagnosis and treatment. The analysis of the vaginal microbiome was proposed by Lima and colleagues to assess GSM in clinical trials and this may be another potentially more objective method of assessment of urogenital atrophy, which may also provide aetiological and pathological information. 55
Conclusion
A simple, objective, widely available and validated method that is acceptable to women to diagnose urogenital atrophy is essential in clinical practice, as well as in research. Available prevalence rates of this condition are likely to be inaccurate and may not be truly representative of the number of women experiencing symptoms of urogenital atrophy. Lack of a reproducible diagnostic test, suitable for use in all settings including primary care, is one of the most significant limitations affecting assessment of women with urogenital atrophy. Resolving this problem will facilitate realisation of the recommendation of early clinical assessment of symptomatic women and treatment without delay 100 for the benefit of women suffering with urogenital atrophy. Future research should be directed towards developing diagnostic methods for urogenital atrophy which amalgamate patient feedback with an objective clinical assessment of the condition using a validated, composite tool. Once developed, attainment of a general consensus on use of diagnostic criteria is imperative to ensure associated benefits both in clinical care and on-going research.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.