
Abstract
Objectives
Genitourinary syndrome of menopause (GSM) is a common condition, yet there is no accessible, objective clinical method with which to make a diagnosis of vaginal changes associated with GSM. We undertook a feasibility study to assess suitability of different objective diagnostic methods and obtained quantitative scores using a new GSM Assessment Tool (NGAT) and vaginal maturation vlue (VMV). These scores were correlated with patient reported symptoms obtained via a questionnaire.
Study Design
VAginal Health – What’s Normal (VAN) Study is a prospective, observational, feasibility study, evaluating NGAT and VMV. Sixty women (12 healthy controls and 48 symptomatic) were recruited and had a baseline assessment. The symptomatic women were offered treatment and had a second assessment 16 weeks later.
Results
Compared with control group, symptomatic women had higher NGAT and VMV scores at baseline. After treatment, in symptomatic women, symptoms improved and NGAT scores reduced, while the median value for VMV was unexpectedly reduced.
Conclusions
This data suggests that clinical assessment and accurate recording of GSM can be supported by an objective scoring system, particularly in primary care and warrants adequately powered future studies to assess the utility of these methods in clinical and research setting.
Keywords
Introduction
Genitourinary syndrome of menopause (GSM) affects many women. Although different terminology is used to describe the condition, GSM acknowledges that tissue quality in the vulva, vagina, bladder and urethra can all be affected by lack of estrogen, occurring most commonly due to the cessation of ovarian estrogen production at the menopause. 1 The vaginal mucosal layer is made up of the epithelium and the lamina propria. The vaginal epithelium is a multi-layered, stratified, non-keratinised squamous epithelium, which continuously regenerates. In adequately estrogenised women, a cell layer sheds from the vaginal epithelium every few hours, with considerable amounts of glycogen in the desquamated cells. Lactobacilli, which predominate in a healthy vagina, produce lactic acid from glycogen, maintaining an acidic environment within the vagina. A reduction in superficial cells, associated with a drop in estrogen levels following the menopause, reduces vaginal glycogen, lactic acid and lactobacilli and the pH rises as a result. In addition, the reduction in superficial cells alters the ratio in relation to intermediate and parabasal cells, influencing the vaginal maturation value (VMV). 2
For some women with GSM, the onset of symptoms occurs several years after the other more commonly recognised symptoms of menopause, and thus, the association of GSM with the menopause is lost. As a result, GSM is an under-reported, under-researched, under-diagnosed and under-treated condition, with women assuming that the symptoms they experience are a normal part of ageing. 3 A clear diagnosis of GSM based on the patient’s history and clinical examination findings is recommended by both the British Menopause Society Consensus statement on Urogenital Atrophy 4 and the North American Menopause Society Position Statement on GSM. 5 An accurate diagnosis is necessary to implement the various available treatment options to manage GSM, such as those recommended by the National Institute for Health and Care Excellence (NICE). 6 However, there is currently no consensus on the best diagnostic method for GSM in a clinical setting. Symptomatic women are managed by clinicians either in primary or secondary care, where a clinical diagnosis is based on symptoms and signs, if examination is performed. The United States Food and Drug Administration (FDA) have recommended that all research studies investigating potential new treatments for GSM, record the most bothersome symptom and they have exacted that women in such studies have a clinical examination, including measurement of the pH of vaginal secretions, likely to be higher than 5 in women with GSM 7 and an evaluation of VMV. Measurement of pH is an easily performed test, not requiring additional laboratory investigations, but is not part of routine practice and has thus far not been evaluated in adequately powered clinical trials.
COMMA, the Core Outcomes in Menopause global initiative, 8 have developed a core outcome set (COS), for genitourinary symptoms associated with menopause. This includes an assessment of the following criteria: pain with sex, vulvovaginal dryness, vulvovaginal discomfort or irritation, discomfort or pain when urinating, change in the most bothersome symptom, distress, bother or interference in association with genitourinary symptoms and satisfaction with treatment and side effects of treatment. The COMMA group’s recommendations lacked consensus in relation to any of the following examination criteria: genital appearance as assessed by a clinician, vaginal elasticity measured by stretching, vaginal pH (acidity), VMV or endometrial histology. These recommendations represent significant progress, but a diagnosis of GSM is best confirmed by examination, to rule out other potential causes of vulvovaginal symptoms, as recommended by the European Vulvovaginal Epidemiological Survey (EVES). 9 A critical analysis of methods for assessing GSM in clinical trials published in 2019 concluded that VMV was the most effective method, followed by vaginal pH. 10 However, a literature review, published recently, which explored diagnostic methods, concluded that there is a lack of consensus regarding the best method, with which to make a diagnosis of GSM. The authors highlighted the need for a validated, cost-effective and accessible clinical diagnostic method to be developed for future use and that this should be available to primary as well as secondary care clinicians. 11 Authors of another paper focussing on deficiencies in studies investigating dehydroepiandrosterone (DHEA) for vaginal use 12 raised concerns that a vaginal smear to calculate the ratio of superficial, to intermediate and parabasal cells, is not a procedure undertaken as part of routine clinical care. Innovation of an alternative assessment tool to VMV which is readily available, reliable and reproducible, to diagnose GSM, could potentially impact on research outcomes in addition to improving day-to-day clinical diagnosis and management of GSM. Currently, any diagnosis of GSM is assumed, as there is no diagnostic test that is incorporated into day-to-day clinical practice.
Considering the information presented above, a feasibility study, VAN, VAginal Health – What’s Normal? was designed to consider the most appropriate methods, in terms of patient acceptability, accuracy and reproducibility with which to assess vaginal health and potentially diagnose and monitor GSM.
Methods
VAN was a UK-based, small, single centre prospective, observational, feasibility study (IRAS no.: 288402, ethical approval LREC: 21/WA/0026) designed to consider concordance of different methods of assessment of vaginal health, compared with the current standard, a clinical assessment, based on symptoms and signs. Use of a vaginal speculum modified by a bespoke insert, providing a new GSM Assessment Tool (NGAT) and vaginal maturation value (VMV) were two of the clinical methods employed in this study, and the results are detailed in this paper. A questionnaire, DIVA 13 (Day-to-Day Impact of Vaginal Ageing), was used to determine the impact of symptoms on day-to-day function, including sexual function, in all participants and the results of this arm of the VAN study have already been published. 14 This previously tested PROM, with a focus on genitourinary symptoms was the questionnaire chosen for the VAN study for the following reasons. It was recognised by the COMMA consortium 15 as a suitable measure to assess the impact of genitourinary symptoms on normal life. It was also used in the MsFLASH Vaginal Health Trial, 16 which identified that women with a history of depression and less frequent sexual activity, experienced a greater impact of genitourinary symptoms on quality of life. The DIVA questionnaire supported collection of information from participants, in relation to four domains: activities of daily living, emotional well-being, sexual functioning, self-concept and body image, with the emphasis on the impact of symptoms, and ability to function. Use of it for the VAN study also fulfilled a recommendation by the original authors of this PROM, to compare the questionnaire with other diagnostic methods, to ensure that DIVA achieved the goal it was designed for, to accurately diagnose and monitor women with GSM. A PROM should have high-quality evidence to support content validity and internal consistency. For the VAN study, this translates as a meaningful score for the outcome, genitourinary symptom impact, over a recall period of 4 weeks across the four domains described above.
The DIVA symptom scores are used in this paper as a point of reference to correlate with NGAT and VMV scores.
The overall study design aimed to provide information on the most acceptable, objective and reproducible methods to assess vaginal health and if GSM likely, support the diagnosis and monitor response to any treatment.
Sixty patients were recruited in total over a period of 4 months (12 women without symptoms (control group) and 48 symptomatic women, eligible for some form of GSM treatment as recommended by the COS developed by the COMMA group). Symptomatic women were provided with individualised treatment following discussion with the lead clinician. The study was not designed to assess the suitability or outcomes associated with individual treatments and previous treatment was not a contraindication to recruitment. Recruitment took place in various different gynaecology outpatient clinics in Liverpool Women’s Hospital (LWH), in the United Kingdom. Written informed consent was obtained from all women who were recruited to participate in the study prior to any intervention. Following consent, participants completed the DIVA questionnaire, before undergoing a clinical examination, which included NGAT and assessment of VMV.
The clinical examination incorporated an assessment of urogenital tissue quality and architectural features, supported by use of a small clear plastic vaginal speculum, chosen specifically for its dimensions, considering some participants might have GSM. The small speculum beak length from the tip to the front of the handle is 80 mm and the beak width is 21.1 mm. The speculum was modified by a bespoke insert supporting a numerical value for tissue colour and elasticity (Figure 1). Early prototype of the speculum used for NGAT scoring system.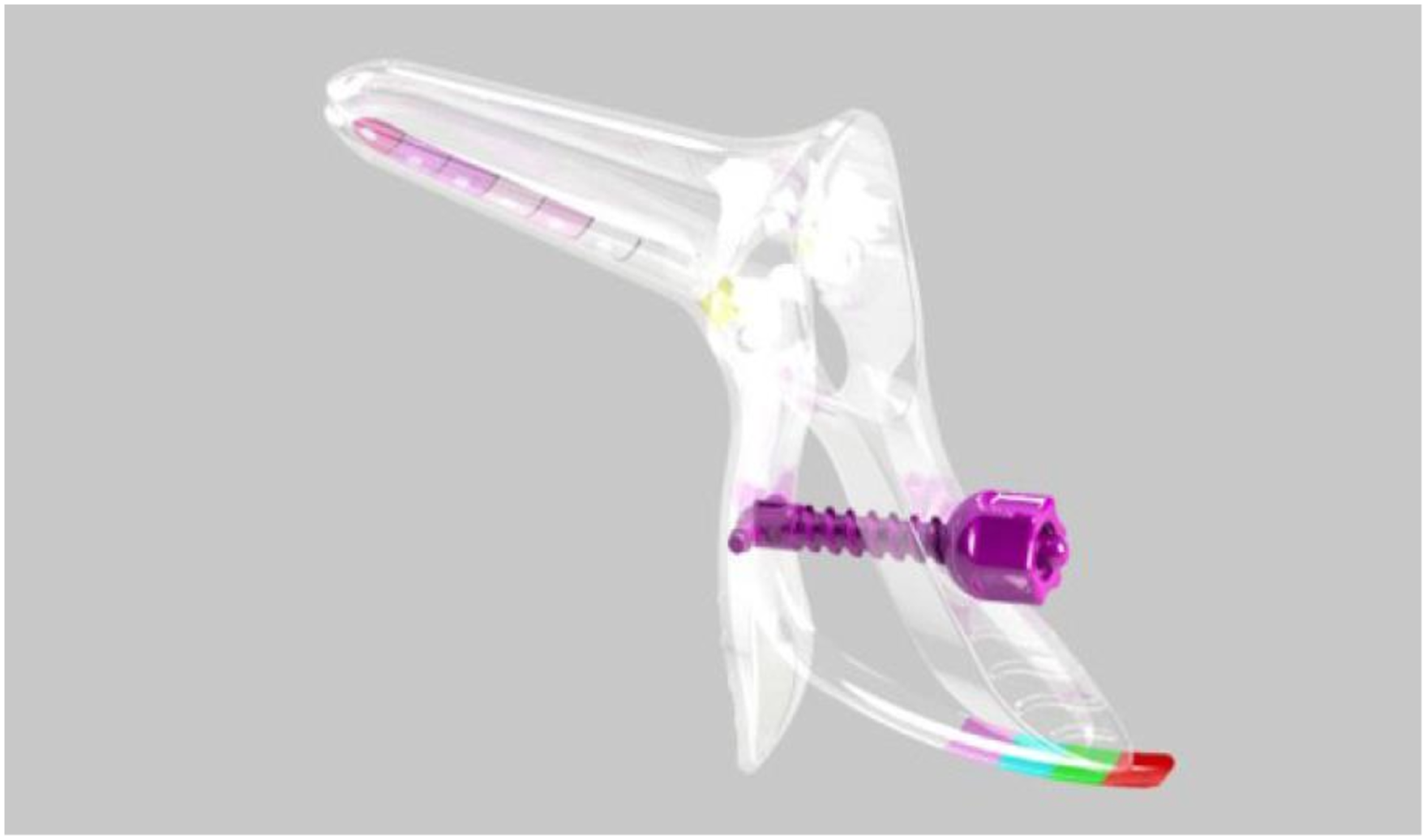
In addition, the pH of vaginal secretions was recorded, as well as other anatomical features. The scoring system is described in more detail below. A vaginal smear was taken, from the lateral mid-vaginal walls, to assess VMV.
Following routine assessment, by a specialist clinician, based on symptoms and signs, symptomatic women with assumed GSM were provided with individualised treatment plans and followed up at 16 weeks as per routine practice. Assessment with NGAT and VMV was undertaken in addition to routine clinical practice. The treatments provided included vaginal lubricants, moisturisers, vaginal estrogen, DHEA, Ospemifene and CO2 laser. There were 48 symptomatic women, with an assumed diagnosis of GSM, who received treatment. In total, 46 women completed a follow up examination at 16 weeks, as two women were lost to follow up; therefore, 46 treated women were clinically assessed at both time points, (1) before and (2) 16 weeks after the initiation of their treatment, providing 46 paired data sets.
Clinical assessment using the NGAT
NGAT scoring system.
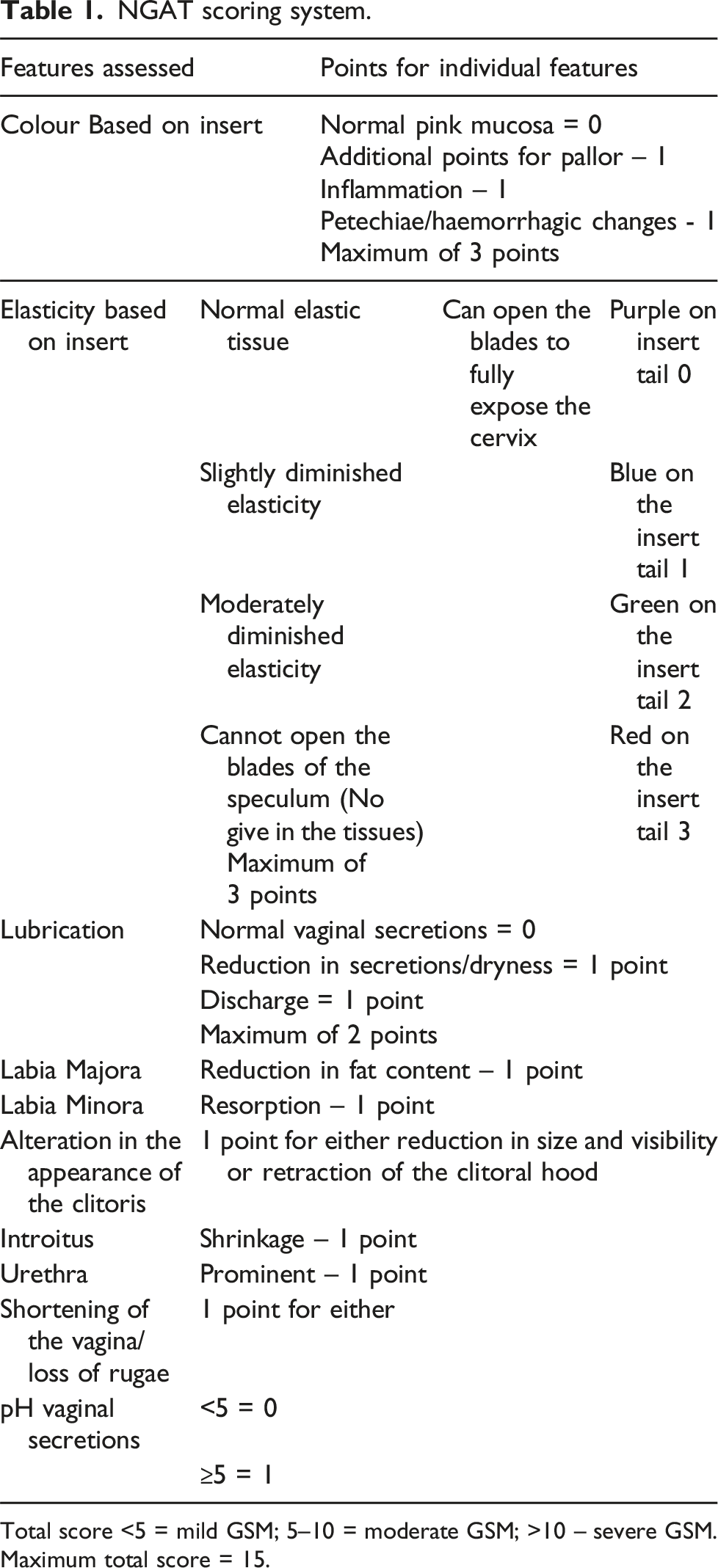
Total score <5 = mild GSM; 5–10 = moderate GSM; >10 – severe GSM. Maximum total score = 15.
Vaginal maturation value (VMV)
A vaginal smear was taken from the lateral, mid-vaginal walls using a Hologic Plastic Spatula, rather than a Cytobrush. The specimen was transferred to the laboratory in a ThinPrep® vial, where it was processed on the Hologic ThinPrep® 5000 multisample processor for preparation onto a slide. The resultant slide was stained using the Papanicolaou method and a coverslip applied for microscopic cell counting. In most women, a vaginal speculum was used to clearly visualise the lateral vaginal walls; however, in the most severely affected women, it was not possible to open the blades of the speculum, and the smear had to be taken blindly. VMV was calculated using the formula 0.2 x % parabasal cells +0.6% x % intermediate cells +1.0 × % superficial cells, to assess the ratio of superficial cells to intermediate and parabasal cells. 18 The lower the value, the lower the proportion of intermediate and superficial cells, reflecting a greater degree of atrophy.
There are three types or stages of vaginal epithelial cells; parabasal where the ratio of nucleus to cytoplasm is highest, intermediate and superficial with a smaller cell nucleus and more cytoplasm. VMV ranges from 0 to 100%, with different values reflecting the influence of estrogen. A value of 0%–49% suggests an absent or low estrogenic effect, 50%–64% indicates a moderate estrogenic effect, and 65%–100% is typical for a high estrogenic effect. 19
Study outcome measures
The primary outcome
Comparison of the assessment scores using NGAT and VMV in asymptomatic healthy controls and symptomatic women with an assumed diagnosis of GSM, based on patient reported symptoms at the initial consultation.
The secondary outcomes
Correlation of NGAT and VMV scores with DIVA scores. The feasibility of using the same two methods to assess the influence of various routinely used treatments for GSM on NGAT score and VMV in symptomatic women assumed to have GSM. Treated women were assessed before and 16 weeks after initiation of the agreed treatment. Concordance between the NGAT scores and VMV, before and after treatment, was assessed along with their correlation with the DIVA scores.
Statistical analysis
In this feasibility study, we did not conduct any hypothesis testing as per the National Institute of Health Research (NIHR), UK recommendations for feasibility/pilot studies. Quantitative data is presented using standard summary statistics including mean, media and counts, along with a corresponding measure of variability and 95% confidence intervals. All statistical analysis was conducted using the IBM SPSS (Statistical Product and Service Solutions) software platform, version 27 for Windows.
Results
Participant demographics.
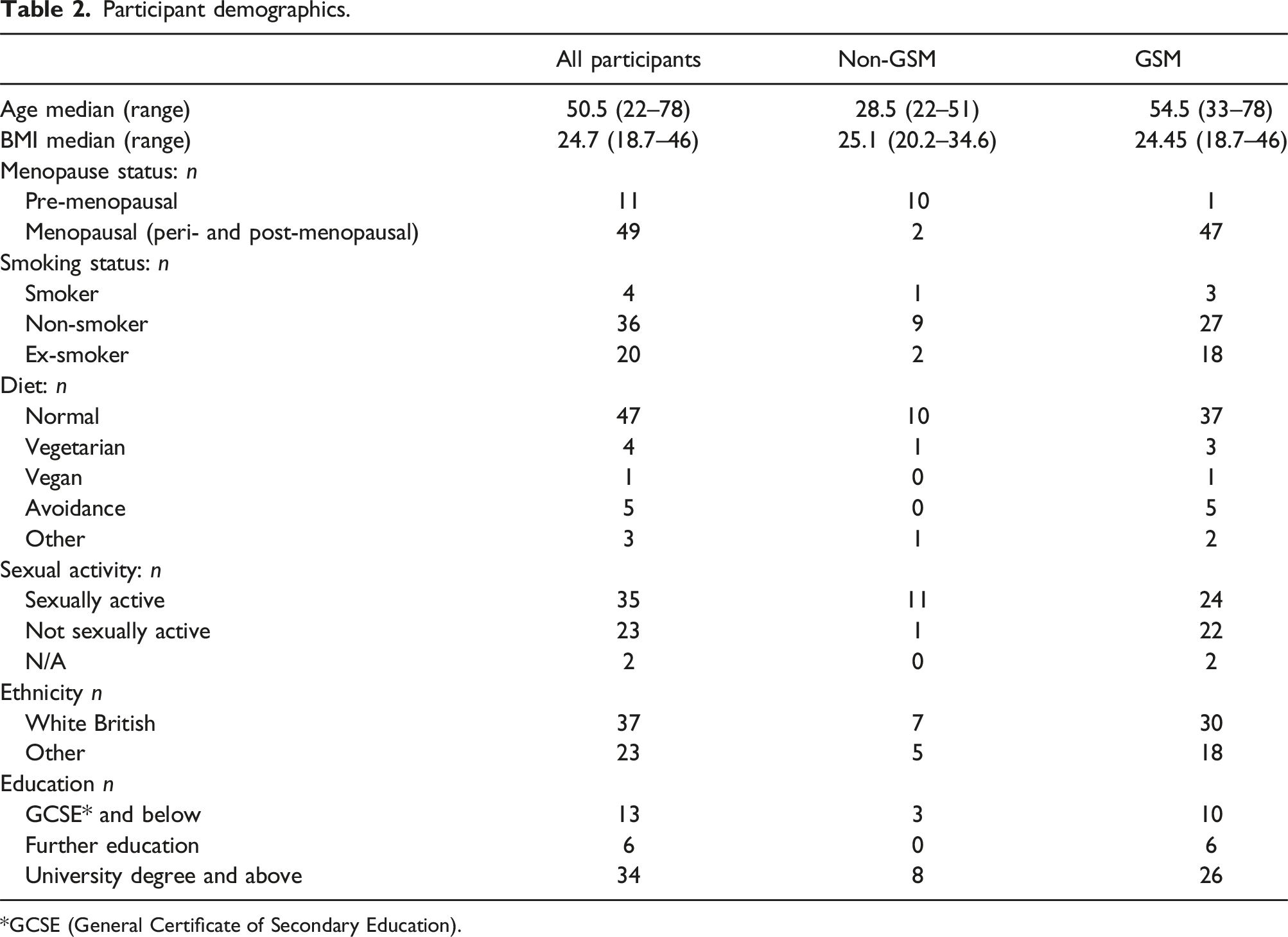
*GCSE (General Certificate of Secondary Education).
NGAT
Scores were compared between the asymptomatic control group, n = 12 and the symptomatic group, n = 48, demonstrating a sizable difference in the median score between the asymptomatic and the symptomatic group, assumed to have GSM (1 (0–3) versus 7 (0–15)) (Figure 2(a)). When the scores were compared before and after treatment in the symptomatic group, the median NGAT scores reduced (7 (0–15) to 4 (0–13)) (Figure 2(b)). (A) Comparison of New Genitourinary Syndrome of Menopause Assessment Tool (NGAT) scores in the non-GSM population (control group) N = 12 and the GSM population (affected group) N = 48. (B) Comparison of NGAT scores before, and after treatment for GSM, N = 46.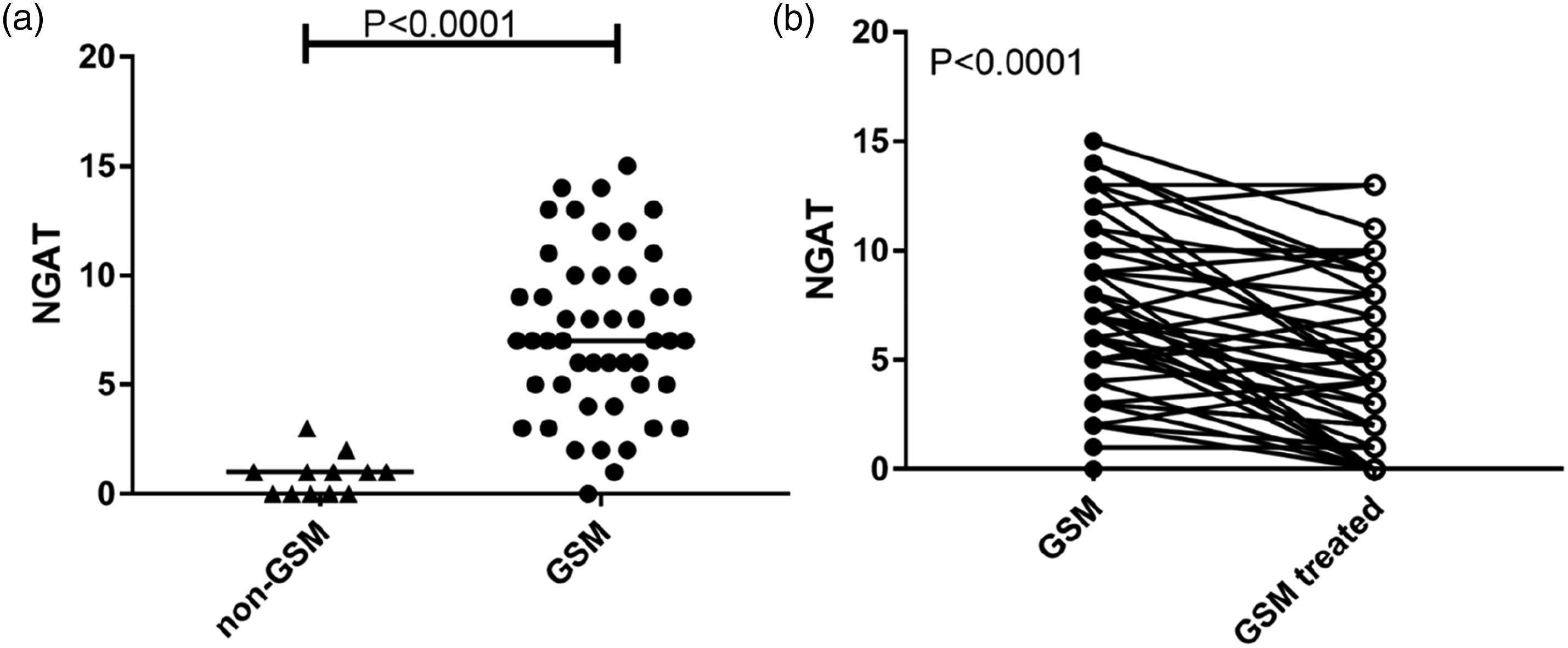
A moderate correlation between NGAT at baseline and the different DIVA categories was identified for symptoms relating to daily living (rho = 0.33) and for sexual function symptoms (rho = 0.44).
For symptomatic women, who received treatment and who had a further assessment at 16 weeks, there was no significant correlation observed between the NGAT score and any of the DIVA domains.
pH was assessed independently as part of the examination using NGAT.
A reduction in the number of women with a pH > 5 following various treatments was noted (87.5% reduced to 71.7% following treatment).
Although there was a higher proportion of women with pH < 5 following treatment (12.5% pre-treatment vs 28.3% after treatment), there was no positive correlation with any of the DIVA questionnaire domains.
VMV
Values were compared between the asymptomatic control group (n = 12) and the symptomatic group (n = 48) Figure 3(a). A small difference in median VMV between the asymptomatic group (64.4, range 56.8–80.4) and the symptomatic group (62.2, range 0–92.8) at baseline was observed. (A) Comparison of VMV scores in the non-GSM population (control group) N = 12 and the GSM population (affected group) N = 48. (B) Comparison of VMV scores before, and after treatment for GSM, N = 46.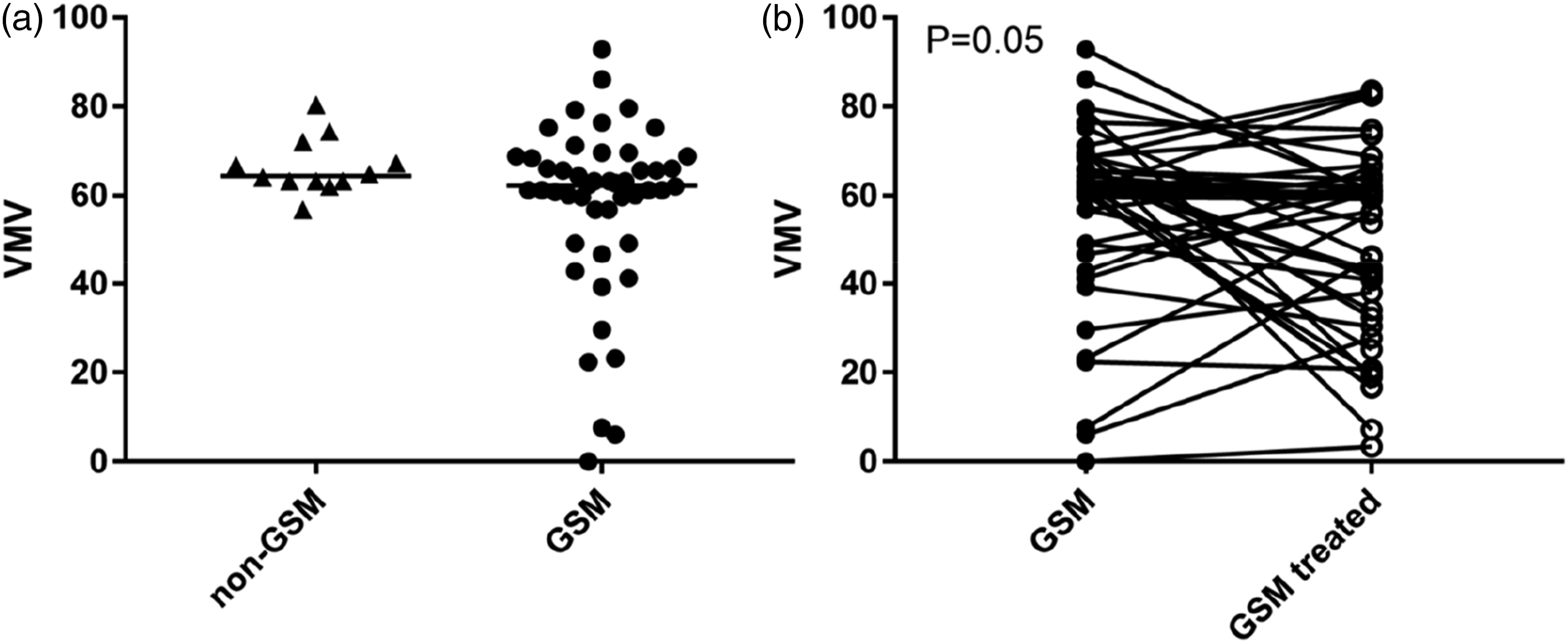
There was no significant correlation between VMV and DIVA scores at the initial assessment in any domain.
VMV was compared in the women assumed to have GSM before and after treatment.
A reduction in median VMV following treatment (62.2, range 0–92.8) versus (57.8, range 3.4–83.6) was observed as shown in Figure 3(b).
There was no correlation between VMV after treatment in all domains of the DIVA questionnaire.
Following treatment, the VMV would be predicted to increase, reflecting an increase in the number of superficial cells. In the VAN study, the number of superficial cells reduced following treatment.
The results were confirmed using bootstrap (Appendix 2).
Initial cell counts were undertaken by a single Consultant Biomedical Scientist.
Due to this unexpected result, 10% of the slides were quality assured by a second clinician, a histopathologist. On the initial scoring for the QA samples, there was agreement in 50% of the slides, with the counts changing in some slides when the biomedical scientist and histopathologist jointly reviewed the slides.
The QA findings were analysed using a Bland-Altman plot (Figure 4(a)). This method of analysis is used to assess the measure of agreement between two quantitative measurements, based on the mean difference with constructed limits.
20
It helps to determine reliability and reproducibility by assessing the proximity of scoring, in this case, cell types in a vaginal smear (Figure 4(b)). Although the results fall between the limits of agreement (SD + or - 1.96), and the mean difference is close to 0, the pattern in the scatter suggests that there is a systematic difference in the scoring between the two observers. (A) Bland Altman Plot. (B) Intermediate squamous cells (blue) and superficial squamous cells (yellow).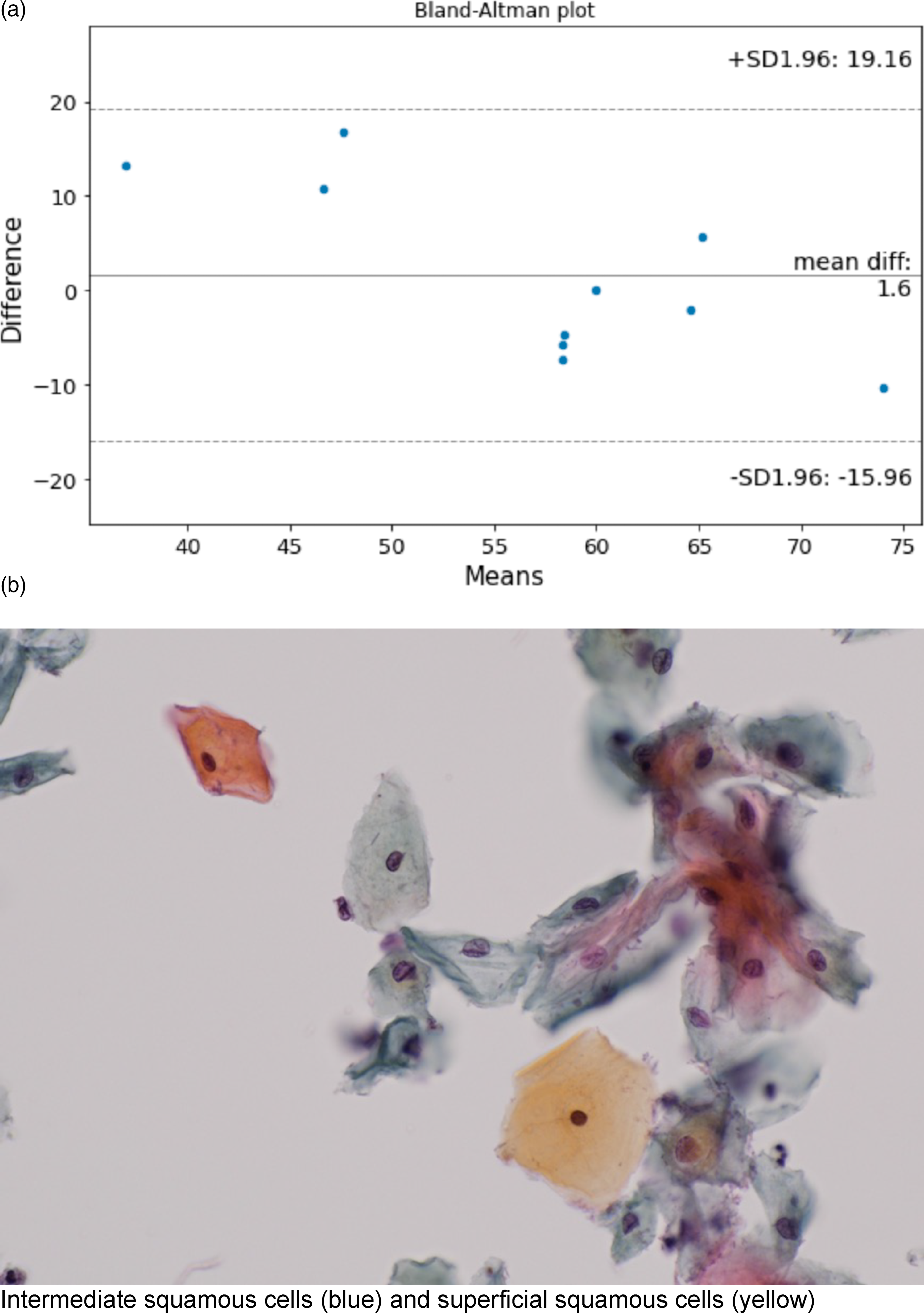
Discussion
The VAN study has demonstrated that asymptomatic women have lower DIVA scores and also lower scores with NGAT, than symptomatic women. Following treatment, symptomatic women also had a reduction in the scores for DIVA and NGAT. The correlation between NGAT and DIVA scores prior to treatment suggests an accurate clinical assessment with NGAT, although this correlation was not seen following treatment, perhaps linked to less extreme symptoms. VMV was higher in asymptomatic women as expected, reflecting a higher number of superficial cells. VMV would be predicted to increase following treatment. However, in this small feasibility study, the VMV following treatment was unexpectedly lower and did not correlate with the symptoms scores captured with DIVA questionnaire.
This demonstrates the complex nature of GSM symptoms, which may not be easily captured with objective clinical vaginal health assessment methods. pH was measured independently as part of NGAT and this was also lower after treatment. Measurement of pH is an FDA requirement along with assessment of most bothersome symptom and maturation index. In the literature review already published in PRH, 11 assessment of pH was undertaken in between 64%–91% of studies and the systematic review by Christmas et al. 21 found that it was assessed in more than 50% of studies. The COMMA group have recommended patient reported symptoms to diagnose GSM. Although it is suspected that many menopausal women have some degree of atrophy, diagnosis depends on the experience of the clinician to whom the patient presents. The VAN study was undertaken in an attempt to identify the best method to assess vaginal health and in so doing find an objective and reproducible diagnostic method for GSM. In the course of the study, we attempted to ascertain whether the diagnostic methods analysed provided concordant results. Although the numbers in this feasibility study are small, the results nevertheless provide outcomes, which following a larger definitive trial, could influence clinical practice in future.
We have considered possible reasons for the unexpected results obtained with VMV in the VAN study. Of note, manual assessment of maturation index was previously recognised to be associated with inter- and intra-observer variation with the recommendation that outcomes may be improved by the use of automated image analysis systems. However, an automated and validated image analysis system is not yet used, even for cervical screening programs, and thus, it was not an option available for the VAN study. 22
There were challenges associated with obtaining a vaginal smear to assess VMV. To take a smear from the lateral vaginal walls, a lubricant was required to reduce patient discomfort and to make it possible to insert the speculum. Clumping of cells, despite use of a glacial acetic acid wash, to remove as much lubricant as possible, led to problems differentiating cell types and numbers. However, if the use of lubricants affected the result, it is a considerable weakness of the method since its use is needed for this particular patient group.
With only 50% agreement in the VMV scores described above, and the Bland-Altman scatter pattern, VMV in this small study appears to lack objectivity and is subject to human differences. A future adequately powered study is warranted to assess the inter- and intra-observer variance of VMV, in parallel with assessing the same for NGAT scores to conclude on the most objective method to assess GSM. Even in optimal circumstances, cell counting is subjective, and it is not part of routine practice and as a result, histopathologists and biomedical scientists with this skill are not readily available. Therefore, it does not appear practical or cost-effective to employ this method, requiring highly skilled manpower, for a very common condition such as GSM. Future studies should develop a computerised cytomorphometric method to assess the maturation index of vaginal epithelial cells to improve the reproducibility of the method. Using a different formulae to assess the karyopyknotic index, it made no difference to the results (Meisels index is calculated using the formula:
[parabasal cells x 0] + [intermediate cells x 0.5] + [superficial cells x 1]). 23
Strengths
The study employed a plastic spatula, proposed to be the best collection device for the assessment of VMV, and this was therefore expected to yield sufficient material in this particular patient group.
To our knowledge, this is the first study to question the validity of VMV, based on analysis of vaginal smear samples and collected using the plastic spatula.
This study presents feasibility data and potential benefits associated with use of a novel intervention, NGAT. This is a low-cost and easily accessible clinical assessment tool, readily available to primary care clinicians as well as researchers.
Limitations
This feasibility study does not have power to fully assess the diagnostic capability and correlation between different methods used to assess GSM. However, it provides the necessary variability data, in outcome measures, to estimate parameters, such as standard deviation, for use in sample size calculation for a future larger, definitive study.
Adherence to treatment was assessed using patient reporting, rather than by employing a specific objective method. However, the improvement of symptoms captured in the DIVA questionnaire implies good compliance.
We did not record time since menopause in women assumed to have GSM, eligible for treatment.
Conclusion
The results from the VAN study provide a timely opportunity to review diagnostic methods to complement the COS developed by the COMMA group, to improve diagnosis and management of GSM.
Use of defined clinical findings criteria (NGAT) supported by use of a modified vaginal speculum and including pH as an indicator of GSM, along with information from a questionnaire appears to be important, particularly for the initial diagnosis, to improve access to appropriate treatment. NGAT is likely to have most impact in primary care where the majority of affected women will present, particularly peri- and post-menopausal women presenting for a cervical smear.
The findings of this small study did not confirm the expected objectivity in relation to VMV and this should be further investigated in a larger, appropriately powered study. The findings highlight challenges associated with use of maturation value as a method of assessment for GSM and it is unlikely to be adopted into routine clinical practice.
If reliability of NGAT is confirmed in future studies, and the method is validated, it could be suitable for use in primary and secondary care, potentially supporting earlier diagnosis of GSM and reducing the number of women with severe symptoms and signs who are less likely to respond to treatment. 24
Supplemental Material
Supplemental Material - Feasibility of developing a new tool for assessing vaginal health in women with Genitourinary Syndrome of Menopause; The VAN study
Supplemental Material for Feasibility of developing a new tool for assessing vaginal health in women with Genitourinary Syndrome of Menopause; The VAN study by Paula Briggs, Christopher Evans, Steven Lane, Lora Kiosseva, Jo Drury, Tim Hillard, Nick Panay and Dharani K Hapangama in Post Reproductive Health.
Footnotes
Contributorship
PB and DH conceived the study and were involved in protocol development and gaining ethical approval. PB was responsible for patient recruitment. PB, SL and DH contributed to data analysis. PB wrote the first draft of the manuscript. All authors (PB, JD, SL,CE, LK, TH, NP and DH) reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PB has received honoraria from the following pharmaceutical companies: Bayer, MSD (Organon), GSK, Gedeon Richter, Consilient, Astellas, Actavis, Mylan, Theramex, Pfizer, Shionogi and Besins, unrestricted educational grants from Theramex and Actavis and has been supported to attend meetings by Bayer, MSD, GSK, Gedeon Richter, Mylan, Shionogi and Besins. NP has undertaken speaker’s bureau work for: Abbott, Astellas, Bayer, Besins, Gedeon Richter, Novo Nordisk, SeCur, Shionogi, Theramex, Viatris and participated in advisory committees for Abbott, Astellas, Bayer, Besins, Gedeon Richter, Mithra, Novo Nordisk, SeCur, Shionogi and Viatris. TM has received consultancy and speaker fees from Theramex, Besins and Astellas. LK, SL and DH have nothing to declare.
Funding
A small unrestricted educational grant was provided by Theramex. No financial support was provided in relation to authorship and/or publication of this article.
Guarantor
PB.
Ethical approval
LREC:21/WA/0026 (IRAS number: 288402).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.