
Abstract
Care pathway implementation is characterised by a dual complexity. A care pathway itself represents a complex intervention with multiple interacting and interdependent intervention components and outcomes. The organisations in which care pathways are being implemented represent complex systems that need to be directed at change through an in-depth understanding of their external and internal context in which they are functioning in. This study sets out a new evidence-based and pragmatic framework that unpacks how intervention mechanisms, intervention fidelity and care context are converge and represent interacting processes that determine success or failure of the care pathway. We recommend researchers looking to increase the effectiveness of care pathway implementation and accelerate improvement of desired outcomes to adopt this framework from inception to implementation of the intervention.
Introduction
Care pathways are a way to improve care coordination and make the patient-focused care concept operational. Care pathways are defined as ‘complex interventions for mutual decision making, organisation and standardization of predictable care for a well-defined group of patients during a well-defined period. The development and implementation of a care pathway is based on multidisciplinary teamwork, understanding the practical organisation of care and the integration of a set of evidence-based key interventions’. 1 The aim of care pathways is to improve outcomes by providing a mechanism to coordinate care and reduce fragmentation and ultimately costs. 2 The implementation of a care pathway leads to increased or clearer documentation of care,3,4 better interprofessional teamwork5,6 and higher level of organised care.5,6 Care pathways may lead to better clinical outcomes.7–9 However, this is organisation and pathology dependent, which lead to inconclusive evidence to support the effectiveness of care pathways on clinical outcomes. A possible explanation lies in the dual complexity. First, care pathways are seen as complex interventions as they comprise separate elements which seem to be essential to the proper functioning of the intervention. They target multiple outcomes, involve multiple interventions 10 and the ‘active component’ is difficult to specifiy. 11 Second, care pathways are developed and implemented in complex organisations taken into account the external and internal context. Taking into account this twofold complexity means that assumptions about the implementation of the intervention need to be considered carefully and reflect non-standardisation, multiplicity and interaction as well as recognise the importance of context. 12 In 2004, the European Pathway Association (E-P-A) was launched. The aim of E-P-A is to support organisations and individuals to develop, implement and evaluate care pathways with as primary goal to perform research on care pathways. 13 The other aims are (i) to set an international network and international training initiatives that go with it are set up to pool know-how, (ii) to foster an international cooperation between healthcare researchers, managers and healthcare providers from European countries and the wider international community and (iii) to advise policymaker within the area of healthcare management. 14 The objective of the E-P-A framework is to describe components that determine success or failure of care pathways. So that those who develop, evaluate and implement care pathways are assisted in how to increase the positive findings of care pathway implementation.
New E-P-A framework for care pathways
The authors of this paper developed this new evidence-based pragmatic framework for care pathways based on the results of several international studies, assessing team and patient outcomes for various pathologies.6,15
This framework illustrates the interaction between intervention mechanisms, care context and intervention fidelity in achieving improved outcomes (four pillars) to understand how care pathways are working and are equally important. Context, mechanism and outcomes are the key concepts of realistic evaluation. 16 The framework is displayed in Figure 1 and discussed in detail below.
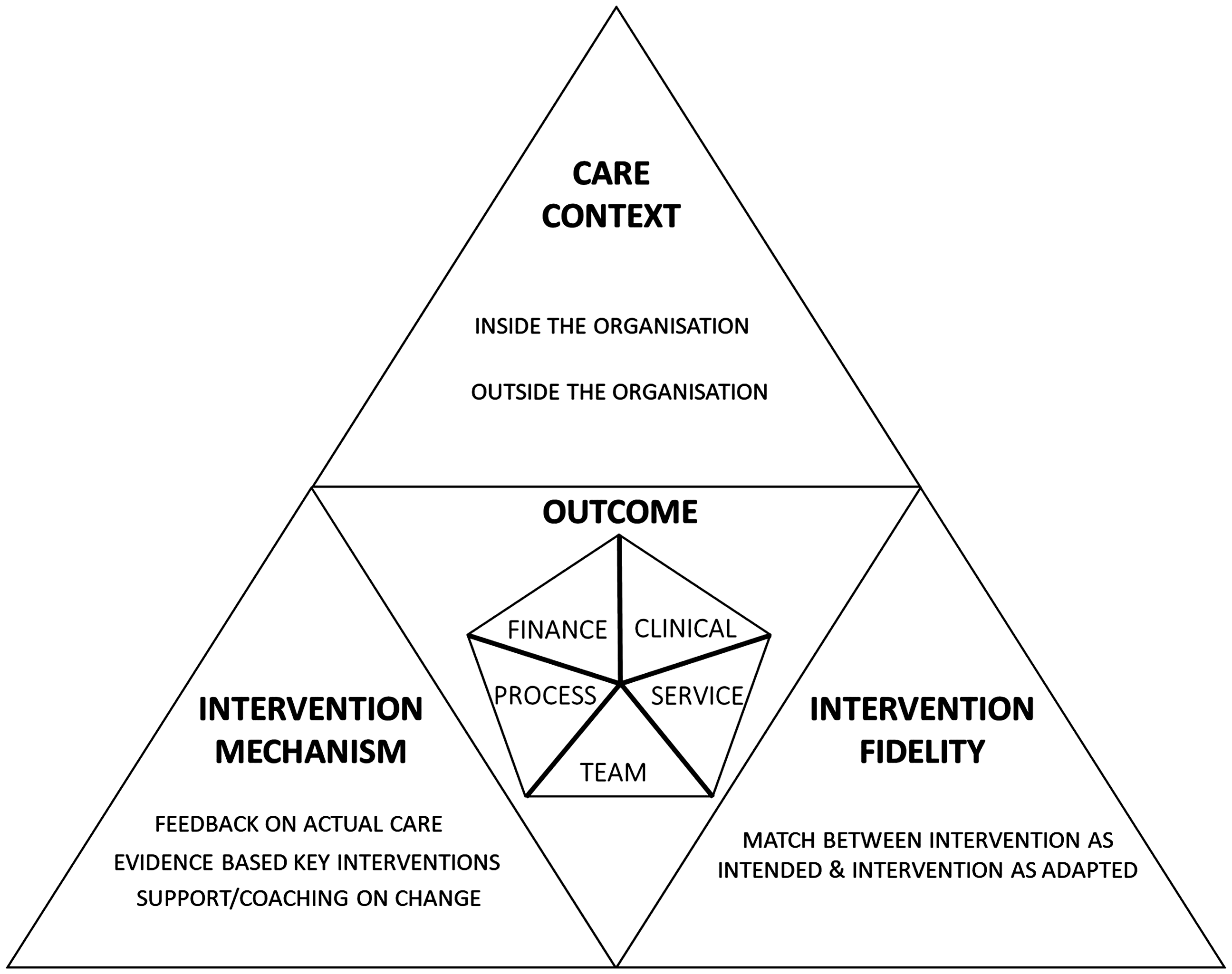
European Pathway Association framework for care pathways.
Outcome
Care pathways should start with a certain goal. To set this goal, the Leuven Clinical Pathway Compass can be used and includes patient centred care. In the future, patient centred care should be more explicitly visible. This tool includes finance, clinical, process, service and team aspects. 17 These five types of aspects, resemble the goals formulated in Institute for Healthcare Improvement (IHI’s) Quadruple Aim which are: (i) increase patient experience (process and service aspects), (ii) improve population health (clinical aspects) while (iii) reducing costs (finance aspects) and (iv) improving the well-being and work-life balance of healthcare professionals (team aspects). 18 Clinical, process and services indicators can give more information regarding the fourth pillar of our framework, intervention fidelity. Fidelity is ‘the degree to which … programs are implemented … as intended by the program developers’. 19 The focus of the service indicators should be patient’s perception regarding the received care. This indicator measures the services of the team or hospitals from patient perspective. 17 The finance and team indicators focus more on the second pillar, care context. The finance indicators should explore direct and indirect costs and the time horizon. On the other hand, they should also include different perspectives (i.e. patients, healthcare professionals, managers and insurers). 20 To increase outcomes, attention should be given to care context (important during the whole process of care pathway development and implementation), intervention mechanism and intervention fidelity, which are described in the next sections.
Care context
The care context may play an important role in the achieved results after care pathway implementation as it will influence the care which is delivered. 21 Changes in the context should be included to understand why and how care pathways are working. 10 It could be an underlying condition for the effectiveness of care pathways and can help to understand why and how care pathways are working. It is important that the openness of the care context is evaluated before, during and after implementation. Therefore, the Model for Understanding Success in Quality (MUSIQ) can be used. MUSIQ evaluates ‘Microsystem’, ‘Quality improvement team’ and ‘Quality improvement support and capacity’, ‘Organisation’, and ‘External’. 22 The latest can also give information regarding the third pillar intervention mechanism.
Another tool which can be used to evaluate the context inside the organisation is Team Climate for Innovation (TCI). TCI measures the extent to which organisations value and encourage teamwork and participation. 23 Through the implementation of a care pathway, it is expected that the teams develop a shared vision and task orientation due to clearly defined evidence-based key interventions which need to be performed for high quality of care. On the other hand, TCI can be a potential predictor of perceived organisation of care. 6
Another tool that can achieve more insight in the care context achieved by health care professionals is the Care Process Self-Evaluation Tool (CPSET). The CPSET evaluates the organisation of care by evaluating the perceived patient-focused organisation, coordination of the care process, collaboration with primary care, communication with patients and family and follow-up of the care process.24–26
The care context depends not only on the context inside the organisation but also on the context outside the organisation. Therefore, financial and legal constraints should also be taken into account and are thus system sensitive. 10
This framework will shed some light on the black box of care pathways and can give more information on why care pathways are not always working. The longitudinal follow-up of care pathways is important as the results on the first improvement priority will not be achieved immediately. For setting priorities, the context openness and the different characteristics of the context may play an important role. 27 Statistical process control can be used for the continuous follow-up of care pathways. This allows to evaluate the effect of the care pathway on predefined upper and lower limits by illustrating the effect of intervention fidelity and care context on the sustainability of care pathways. 28
Intervention mechanism
Multiple active ingredients may strengthen the effect of a care pathway but can also lead to a difference in dose of intervention. These active ingredients can be feedback on the actual care, evidence-based key interventions and support/coaching on change. For example, for patients admitted with a Chronic Obstructive Pulmonary Disease, the Global Initiative for Chronic Obstructive Lung Disease guidelines are used to define a set of evidence-based key interventions. An evidence-based key intervention should be performed in a standard way and is an example to assess the smoking status at admission. 29 The set of evidence-based key interventions and feedback should be based on one or two measurable goals, which allows for rapid feedback. Rapid feedback increases the success of improvement interventions.10,30,31 Implementation of the evidence-based key interventions should proceed according to the order of improvement priorities. These priorities can be based on a performance analysis or an importance-performance analysis.32,33 In an importance-performance analysis, the importance of the intervention, based on literature or Delphi study, is taken into account. Care activities with a high importance rate and low performance rate (underuse) should be high priorities for organisations. Over time and after completion of repeated Plan-Do-Study-Act cycles, the priorities evolve as the performance rate should increase. In the care pathway not each detail is mentioned but only the care activities which should be performed standard for all the patients. This means that the evidence-based key interventions are not based on patient preferences.
Intervention fidelity
The intervention fidelity represents a similarity between ‘intervention as intended’ and ‘intervention as adapted’, in other words is the intervention exactly implemented as intended?19,34 The effect of an intervention can be measured by adherence to guidelines (performance). These performances include interventions each patient should receive and should reduce unwarranted variation between patients. Intervention fidelity should thus include the rationale and logical assumptions of the key interventions, and clarity in planning and executing them. Clarity should be on planning of audit, feedback and follow-up of the implemented key interventions. Regular intern feedback on the performance of these key interventions to the team is likely to increase fidelity. 35 It is important that clinicians and management are involved in the project management. This has been positively associated with quality improvement systems. 36 On the other hand, an implementation approach should also be defined and should include study protocol, define strategies for change and audit and feedback. As theoretical base for the implementation of care pathways, the seven-phase methods can be used. 37 Sometimes, deviation from the evidence-based care is due to preferences of patients. When deviation is based on personalised care, this should be described in the patient report. Therefore, it is important that the used set of key-interventions are independent of patient preferences.
Conclusion
The development and implementation of a care pathway is labour-intensive, thus resources should be optimally used. As care pathways are continuous quality improvement initiatives, actions should be taken to achieve and increase their sustainability. The new E-P-A framework can help organisations and researchers to achieve this goal by keeping the focus on the three pillars (care context, intervention mechanism and intervention fidelity) that may determine success or failure of the intervention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: European Pathway Association obtained an unrestricted education grant form Pfizer SA, AstraZeneca and Baxter. The funders had no role in the design, data collection, analysis, interpretation of data, writing of the manuscript or decision to submit the manuscript for publication. The autonomy of European Pathway Association and all involved academic institutions with regard to scientific independence and intellectual property on the methodology was guaranteed.