
Abstract
Task shifting in healthcare has mainly been initiated and studied as a way to react to/or mitigate workforce shortages. Here, we define task shifting as the structural redistribution of tasks, usually including responsibilities and competencies between different professions. As such, task shifting is commonly focused on highly specialised and trained professionals who hand-over specific, standardised tasks to professionals with lower levels of education. It is expected that this type of task shifting will lead to efficiency and cost savings to healthcare organisations. Yet, there are more benefits to task shifting, in particular its contribution to integrated patient-centred quality of care and a tailored system that meets the changing care demands in society. Hence the importance to broaden the scope of task shifting, its goals, manifestations and how task shifting plays a role in addressing both the strengths and weaknesses in the healthcare system. In this focus piece, trends and conditions for task shifting and its (un)anticipated effects are discussed. We argue that, only when designed to face specific complexities at the workplace and taking into account the balance between specialists and generalists, task shifting may substantially contribute to enhanced quality of care that meets the changing needs of society.
Introduction
Globally, governments and healthcare organisations struggle to solve or prevent anticipated health workforce shortages and bottlenecks in the healthcare system and organization of care.1,2 The COVID-19 pandemic has further stressed the vulnerability of the complex landscape of health care organisations and their dependency on a skilled health workforce. 3 In order to provide high quality healthcare that is both accessible and affordable for all, organisations, teams, and professionals need to continuously adapt their processes to the changing demand for health care. A way to do this, is by redistributing tasks of those healthcare professionals that experience shortages to other existing or new types of professionals, or even technology. As recently defined by the European Commission and the World Health Organisation, “Task shifting per definition consists of delegation of tasks, and sharing roles within health professions, different groups of health professionals, also shifts to patients or to machines”.4,5
In practice, task shifting is initiated with various goals, comes in various forms, and plays a role in addressing both the strengths and weaknesses in the health care system. It is important to describe these variations, in order to better understand the trends and conditions under which task shifting may contribute to the health workforce problems for which it has been initiated in various health systems and countries.
Task shifting has been in place for quite some time. With the Netherlands operating at the frontline of this activity, reflection on conditions for task shifting and its (un)anticipated and (un)intended effects may offer relevant insights for other countries. Based on the conducted research as described in Box 1, this focus piece starts with an overview of the literature on task shifting, after which we describe how in the Netherlands task shifting has (un)intended consequences in various settings. We conclude this focus piece with a future perspective on task shifting, aimed for the health system in the Netherlands and other countries. Underlying research methodology.
Aims and types of task shifting
In 2020, we performed a scoping review of the international literature on trends and types of task shifting with a focus on systematic reviews. We included 33 systematic reviews on task shifting, that combine studies from many care domains and countries and highlight the topicality and level of expectation towards task shifting as part of a solution for problems occurring in the organisation of health care worldwide (see Appendix 1 for an overview of the identified systematic reviews). Scoping the 33 systematic reviews on task shifting reveals that many studies focussed on non-medical prescribing in relation to the acceptability, quality and organisation of care. For example, we identified reviews on nurses prescribing medication and the effect of this on patient satisfaction, as well as reviews on the facilitators and barriers towards non-medical prescribing. In terms of settings, most reviews related to task shifting within primary care, the setting where timely access to safe and appropriate medications is most critical for the wellbeing of any population. 7 The care providers to whom (non-medical prescribing) tasks are most often shifted are nurses, followed by pharmacists, paramedics and midwives. The profession from which (non-medical prescribing) tasks are most often redistributed (the professions providing ‘usual care’) were medical specialists.8,9 The most frequently reported reason for task shifting was the shortage of medical specialists and - related to this – the resulting capacity and efficiency problems in the workplace of care provision.
Anticipated and unanticipated effects of task shifting
Our scoping review highlights several effects of task shifting that are either anticipated or unanticipated and can either manifest as an advantage or a disadvantage to coordination of care in general. Beneficial effects of task shifting are reported across different settings and professions:
Studies described that trained nurses and pharmacists provide the same or better quality of care compared to doctors for certain physical complaints and care for chronic conditions.10,11 A number of studies showed that quality of care has increased through task shifting between general practitioners (GPs) and Nurse Practitioners (NPs), and also in care for the elderly where tasks were shifted between the specialist geriatric medicine and NPs.
12
Equal or better health outcomes for patients were demonstrated as nurses tend to achieve higher levels of patient satisfaction compared to doctors. Accessibility of care has been improved in for example primary care, where ‘new’ professionals such as Physician Assistants (PAs), NPs and Nurse Specialists (NSs) fulfil a bridging function between medical specialists working in hospitals and GPs. Other benefits of task shifting described in systematic reviews included: better use of the skills and knowledge of nurses and pharmacists, improved job satisfaction for nurses and pharmacists and reduced workload for doctors.
13
Our review also showed disadvantages of task shifting:
First, there is evidence that professionals to whom tasks are shifted, like nurses and pharmacists, take or need more time for these tasks than physicians. Spending more time with the patient may well be related to achieving higher levels of patient satisfaction by these professions, as is also suggested by the European Commission Expert Panel on effective ways of investing in Health (EXPH).
4
Studies also show that physicians spend a significant amount of time on training and supervising due to task shifting.
14
This implies that there is also a loss of anticipated efficiency and cost savings of task shifting initiatives.
An important conclusion from our scoping review is that there is a lack of studies on the actual cost-effectiveness of task shifting. 15 While the outcome measurement of task shifting is rather complex itself (i.e. in defining and quantifying its potential benefits and costs), cost-effectiveness analyses are also hampered by the intertwined nature of its intended and unintended consequences as addressed above.
In addition to the insights in the advantages and disadvantages of task shifting, this review also showed a trend towards specialization of professions, on both sides of the task shifting dyad or care chain. Most prominent on the ‘doctors-side’, the result of task shifting is that they will gain more time for other tasks and to focus on more complex care and specific patient groups. On the one hand, this supports the need of medical doctors to become ‘super specialists’ in specific aspects of their field, care delivery or patient groups. On the other hand, the care professionals to whom tasks are shifted, a similar process of specialisation can take place. For example, ‘new’ professions such as PAs, NPs and NSs tend to specialise their role towards specific patient groups as a result of task shifting.
This review also shows the frequently made argument against specialisation. If medical doctors no longer see ‘standard cases’ in patients themselves and only coordinate or supervise such cases, they narrow their range of expertise. They float away from provision of generic care and become less flexible – both as a professional and as a team member within their healthcare organisation. In a similar way, new professions become less deployable for more generic tasks. At an organizational and macro level this will further increase the shortage of generic working professionals and the complexity of care coordination. As a result, the provision of integrated care becomes more challenging and task shifting will unintentionally put pressure on the flexibility of the care system that is increasingly needed.
Task shifting can have multiple consequences for patient experiences, the position of the professional groups involved, quality of services, efficiency of care processes and the level of collaboration and skill-mix distribution between organizations within or between healthcare sectors. Given these challenges, we believe that in particular research of complex interventions may benefit from making use of realist evaluation research. 16 Task shifting should be analysed at different levels, making such research challenging to define at the level of health delivery tasks, professionals, teams, healthcare organisations and health care systems. This implies that new research is needed to broaden the scope of task shifting, preferably by a multi-level, multi-actor and longitudinal approach, applying mixed-methods.
The diversity of task shifting in practice
To supplement and enrich the information we identified through this literature review, we interviewed several experts and analysed case studies in the Netherlands (Box 2). These sources have pointed out that the actual manifestation of task shifting is broader than non-medical prescribing, and that more (diverse) opportunities of task shifting should be recognised.17,18 Examples of opportunities that may increase the quality of care include a proactive role for pharmacists in drug management within general practices or the expanding role for technology in ophthalmology. In particular, task shifting as a way to achieve the right skill-mix of a team of professionals responsible for the care of a specific group of patients is vital.
19
This goes beyond the traditional aim and process of task shifting, where (mostly standardised) tasks of highly specialised professionals with a high education (and salary) are shifted to professionals with lower education. This is of particular importance in the aftermath of the COVID-19 pandemic, which has increasingly overburdened both physicians and nurses. At the same time, the pandemic has accelerated new forms of task shifting, from and to physicians and nurses, in particular by health care and non-medical assistants to cope with boosted workload and burden in hospitals and many other health care sectors Learnings from case studies.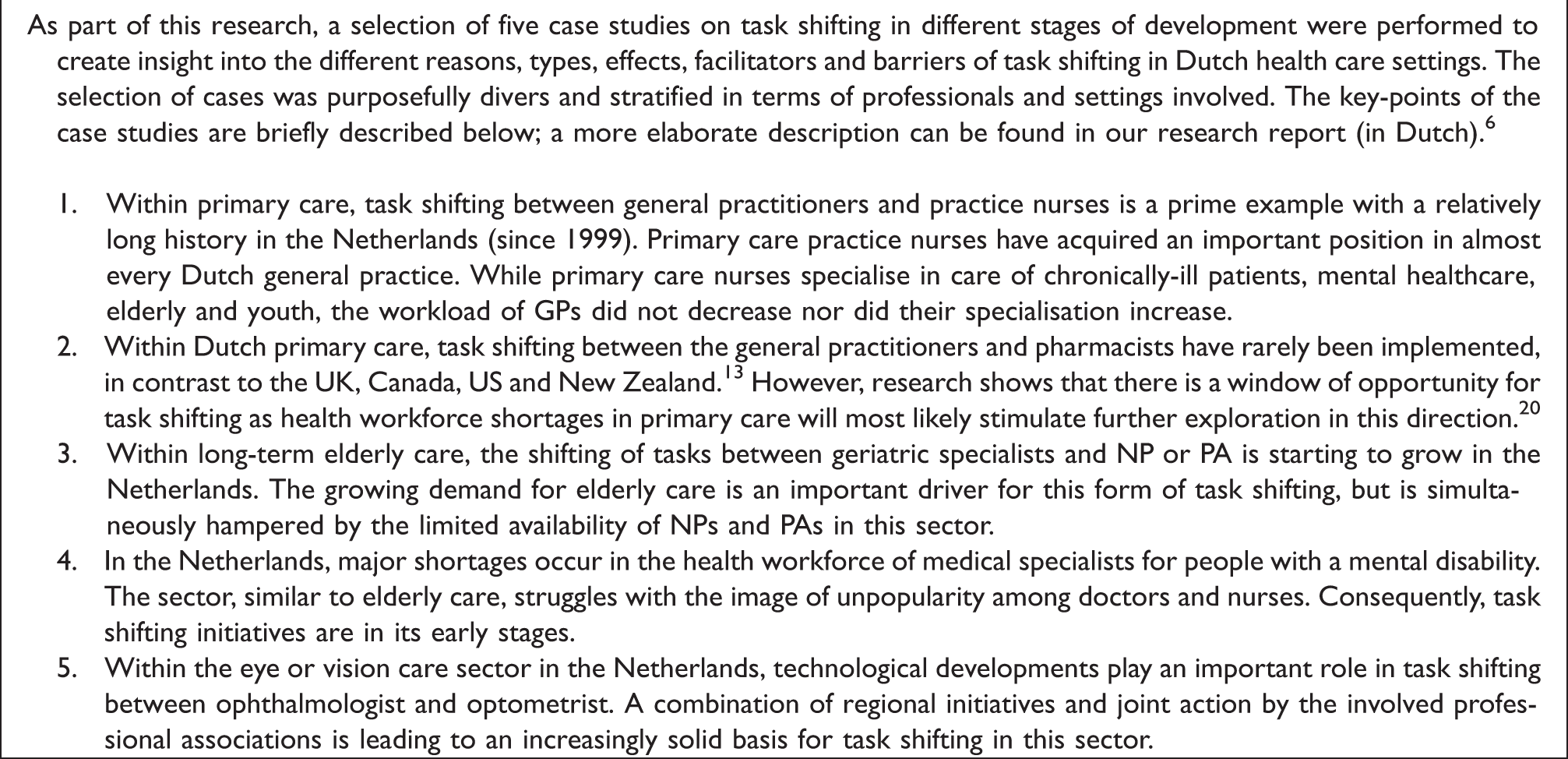
Towards a broader scope of task shifting
Our scoping review, expert consultation rounds, and analysis of case-studies, have shown the need to look beyond task shifting between professionals towards an adaptive and sustainable healthcare system. Broadening the scope of task shifting requires insight, monitoring and evaluation of a diversity of processes that occur at different levels within the organisation of healthcare.
While labour shortages are an important reason to explore task shifting opportunities, the same misbalances on the labour market can also be a barrier to realize the process of task shifting. This was shown by the cases in the long-term care and care for people with a mental disability, where the limited capacity of PAs and NSs block task shifting initiatives. This implies that task shifting initiatives should be aligned with other innovation and organizational change processes, and be accompanied with a human resources vision on how to achieve the right skill-mix for the right care in the right place, in consultation with the field. Thereby the balance between specialised and generic knowledge, skills and competences of professionals should be closely monitored – both at the professional, team, organisational and sector level. As task shifting has a persistent effect on further specialization, the retention of generic competences and professionals remains important in order to sustain flexible care organisations and thus a sustainable healthcare system.
Organisational factors -such as a vision on how an optimal skill-mix can be achieved to meet the changing needs of patients and policy on interprofessional work and teamwork -are of equal importance for task shifting as is adequate training, professional development and supervision of the profession to which tasks are reallocated. A clear vision requires organisational commitment to govern awareness, power shifts and inter-professional relationships. 21 As basic step for success, financial support should be in place as a condition for organisational change, including covering the issue of legal protections and liabilities that are known as important barriers. This calls for an extensive preparation of the care process to support task shifting initiatives. 22
The challenges healthcare systems face worldwide call for a broader vision on the various ways to initiate and implement task shifting. Given the vast diversity in task shifting initiatives, sharing of knowledge on what works and what does not, in different healthcare settings is key. This will help contribute to an effective innovation of care processes through task shifting in which the expertise of the varied health workforce comes into its own.
Supplemental Material
sj-pdf-1-icp-10.1177_20534345211039988 - Supplemental material for Broadening the scope of task shifting in the organisation of healthcare
Supplemental material, sj-pdf-1-icp-10.1177_20534345211039988 for Broadening the scope of task shifting in the organisation of healthcare by Lilian van Tuyl, Bert Vrijhoef, Miranda Laurant, Antoinette de Bont and Ronald Batenburg in International Journal of Care Coordination
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dutch Ministry of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.