
Abstract
Introduction
Pediatric complex chronic care patients present unique challenges regarding healthcare provision: complex medical regimes, complicated family/provider dynamics, and multiple healthcare teams that can result in inconsistent care. This study examined subspecialty providers’ perspectives regarding pediatric complex chronic care patients and compared them with acute care providers while exploring opportunities to better facilitate care provided to pediatric complex chronic care patients.
Methods
This survey study occurring within a Canadian tertiary care pediatric center, utilized REDCap to deploy surveys involving Likert Scale and short answer questions. The Kruskal–Wallis test compared subspecialty provider perspectives when providing care to pediatric complex chronic care patients versus non-pediatric complex chronic care patients; and perspectives between subspecialty and acute care providers.
Results
Survey response rate was 24/46 (52.2%). Eight overarching themes emerged from Likert scale questions. Short answer questions revealed factors that may facilitate care provided to pediatric complex chronic care patients: access to funding; discharge planning; communication methods between specialists; and healthcare provider continuity. Several differences were identified when working with pediatric complex chronic care patients, compared to non-pediatric complex chronic care patients: increased time/resource burden; managing expectations of patients/families; navigating discrepancies in goals of care; complexity of coordination between services; increased efforts in coordinating discharge from hospital and working with medicalized patients/families.
Discussion
Exploring pediatric subspecialty provider perspectives of pediatric complex chronic care patients revealed opportunities to enhance care provided: increased resources to ease the strain of care provision for parents, implementation of a discharge coordinator, complex care clinics with a pediatrician to “quarterback” care, and co-management between the complex care pediatrician and acute care physician when admitted to an acute care service. Implementation of these initiatives may improve the care provided to pediatric complex chronic care patients.
Keywords
Introduction
Formulating a definition of pediatric complex chronic patients (PCCPs) is inherently difficult. The definition needs to encompass the expansive variety of children and conditions that may need to fall under the term, without being overly broad. The seminal definition of PCCPs is “[children and adolescents] who have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition[s and/or those] who require health and related services of a type or amount beyond that required by children generally.” 1
While PCCPs only comprise 10–17% of pediatric hospital admissions in Canada and the United States,2–6 they represent 25–49% of hospital days,3,4,7 and 40–61% of hospital resources.3,4,6,7 In intensive care, this discrepancy is even greater as PCCPs are responsible for over 50% of pediatric intensive care unit (PICU) admissions, and more than 75% of PICU resources. 7 Furthermore, along with the increasing 3 and disproportionate resource allocation7,8 for PCCPs, previous literature reports PCCPs have higher rates of unplanned re-admissions, 9 longer hospitalizations,10,11 higher rates of in-hospital mortality,3,8,10,12 higher illness severity, require multiple healthcare teams with complex treatment plans 13 and receive inconsistent care. 11 While the above statistics primarily refer to Canada and the United States, literature from Spain recognizes increases in the number of hospital admissions, and the need for increased resources for PCCPs, but notes that little to no data exits regarding PCCPs in Spain.14,15 With global advancements in pediatric healthcare it is expected these considerations regarding PCCPs extend internationally, but limited data exists on the topic area.
Complicated healthcare team and family dynamics are common themes when working with PCCPs.13,16–20 Families of PCCPs often assume the role of healthcare provider for their child outside of the hospital setting. 16 As a result, during hospital admissions, family's roles may overlap with those of healthcare providers, 16 which has the potential to create tension or conflict between families and healthcare practitioners regarding methods of care provision and goals of care discussions. 17 Physician engagement may even diminish when working with medically complex “difficult” patients and families. 13 These psychosocial factors surrounding PCCPs have the potential to influence providers’ attitudes toward their patients and in turn impact the quality of care provided.13,18,19
Given the importance of provider attitudes regarding quality of care provision,13,18,19 there is a paucity of literature examining healthcare provider attitudes and perspectives when caring for PCCPs. Parents’ roles and perspectives have been explored out-of-hospital,16,20 in-patient16,20 and in a PICU setting. 21 Exploring PICU healthcare providers’ attitudes and perspectives revealed opportunities to both increase healthcare provider satisfaction when caring for PCCPs, and enhance care provided to PCCPs in the PICU. 22 However, there is a gap in extant literature exploring pediatric subspecialty healthcare provider attitudes and perspectives when caring for PCCPs. Pediatric subspecialist perspectives may inform the gaps between providers and families regarding provision of care and care related priorities.
The following study explored the attitudes and perspectives of pediatric subspecialty healthcare providers working in a Canadian pediatric hospital with PCCPs. Their attitudes and perspectives were then compared with those of PICU providers from previous literature. 22 Furthermore, enhancing the healthcare provided to PCCPs was explored through this inquiry.
Methods
Study design and setting
This prospective study distributed quantitative surveys to pediatric subspecialists and registered nurses (N = 46) working in outpatient pediatric subspecialty clinics at the Jim Pattison's Children's Hospital. The Jim Pattison's Children's Hospital is the only pediatric hospital in Saskatchewan, a geographically vast province with a population of 1.17 million.
The University of Saskatchewan Research Ethics Board (approval number: BEH 18-145) and Saskatchewan Health Authority granted approval for the study.
Quantitative survey development
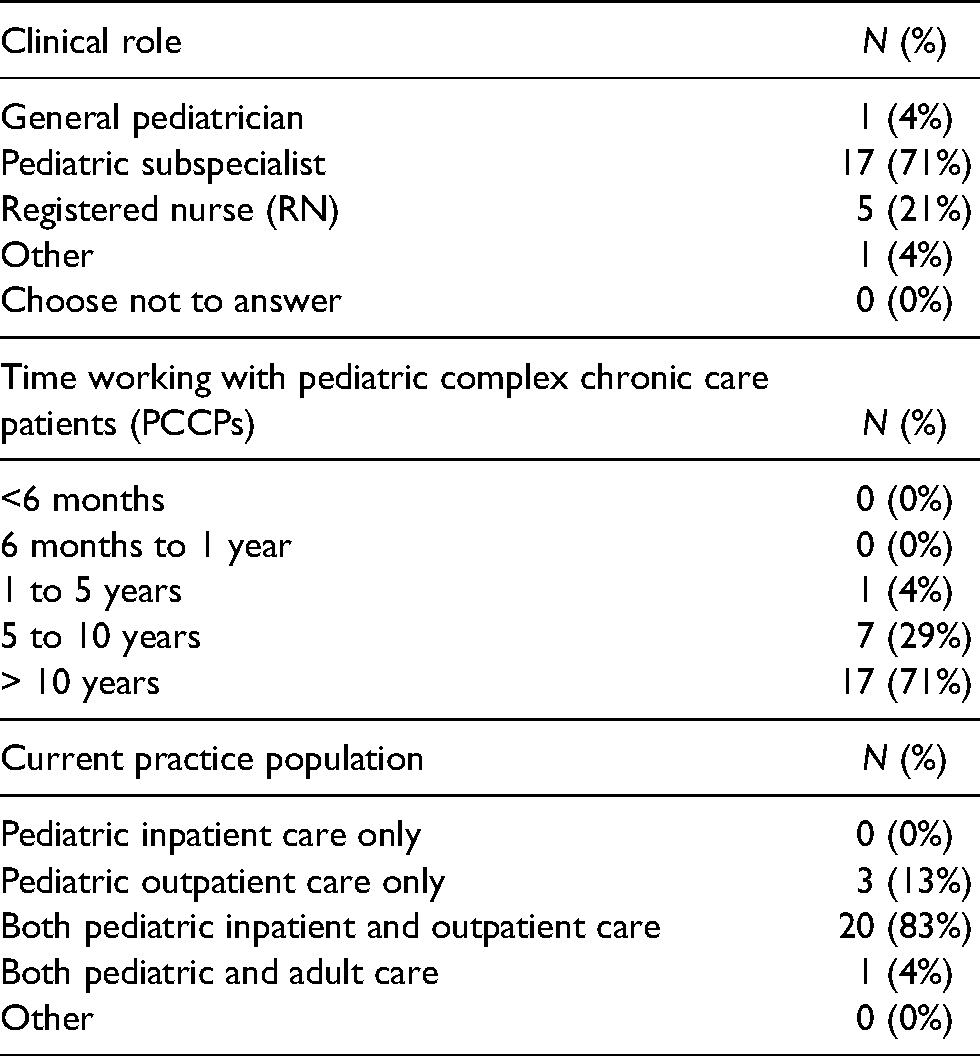
The survey used in this study was modeled after our previous work that studied perspectives and attitudes of healthcare providers working in the PICU. 22 The survey included multiple choice, Likert scale and short answer questions. The six multiple choice questions primarily surveyed employment demographics (i.e. current clinical practice, length of time in practice, relevant training regarding pediatric complex chronic care). The 14 sets of Likert scale questions explored healthcare provider's perspectives when caring for PCCPs compared to non-PCCPs (i.e. feelings of satisfaction/dissatisfaction, ease of care facilitation, perceived mistakes/errors when providing care, involvement of families in care, perception of families facilitating/hindering care). The 10 short answer questions provided an opportunity for participants to express themselves without the constraints of multiple choices/short answer questions and explored facilitators and barriers to providing care to PCCPs, stressors and satisfying factors when providing care to PCCPs, and differences in care between PCCPs and non-PCCPs. As the survey was closely modeled after previous work, prior to distribution, it was piloted by several healthcare providers and other professionals and modified accordingly to ensure completion ease, reliability, clarity, face validity, and to mitigate leading questions. Surveys were administered to all pediatric subspecialty physicians and registered nurses working in pediatric subspecialty clinics who have resided in their position for at least 6 months (Table 1). Resident physicians, pediatric emergency, and neonatal intensive care unit practitioners were excluded given the absence of long-term follow-up and continuity of care for PCCPs.
Participant demographics.
Surveys were administered through the research electronic data capture (REDCap), a secure web application affiliated with the University of Saskatchewan. 23 REDCap is a software designed to support clinical and translational research by ensuring secure web authentication, secure layer encryption, and anonymous participant responses. 23 Survey non-respondents were sent reminder emails at 1-week intervals. No incentives were provided to complete the survey.
Likert scale questions evaluated healthcare provider's attitudes related to caring for PCCPs and non-PCCPs. Proportions were calculated where appropriate. The Kruskal–Wallis test was used to compare pediatric subspecialty physicians and registered nurses’ attitudes concerning PCCPs to non-PCCPs, and to compare subspecialty providers’ attitudes to those of PICU providers. P values less than 0.05 were considered significant. All analyses were conducted using STATA 14 software (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP). Participant's written responses from the pediatric subspecialty provider survey (i.e. challenges when providing care, facilitators, and barriers to care), were analyzed and compared with previous literature to explore opportunities to enhance care provided to PCCPs.
Results
Quantitative results
The pediatric subspecialty providers response rate was 24/46 (52.2%). There were no statistically significant differences comparing pediatric subspecialty provider attitudes towards PCCPs to non-PCCPs. There were several statistically significant results found when comparing the Likert scale responses of the subspecialty provider survey to our previous PICU provider survey regarding PCCPs (Tables 2 and 3).
A comparison of PICU and subspeciality providers persprctives regarding non-PCCPs.
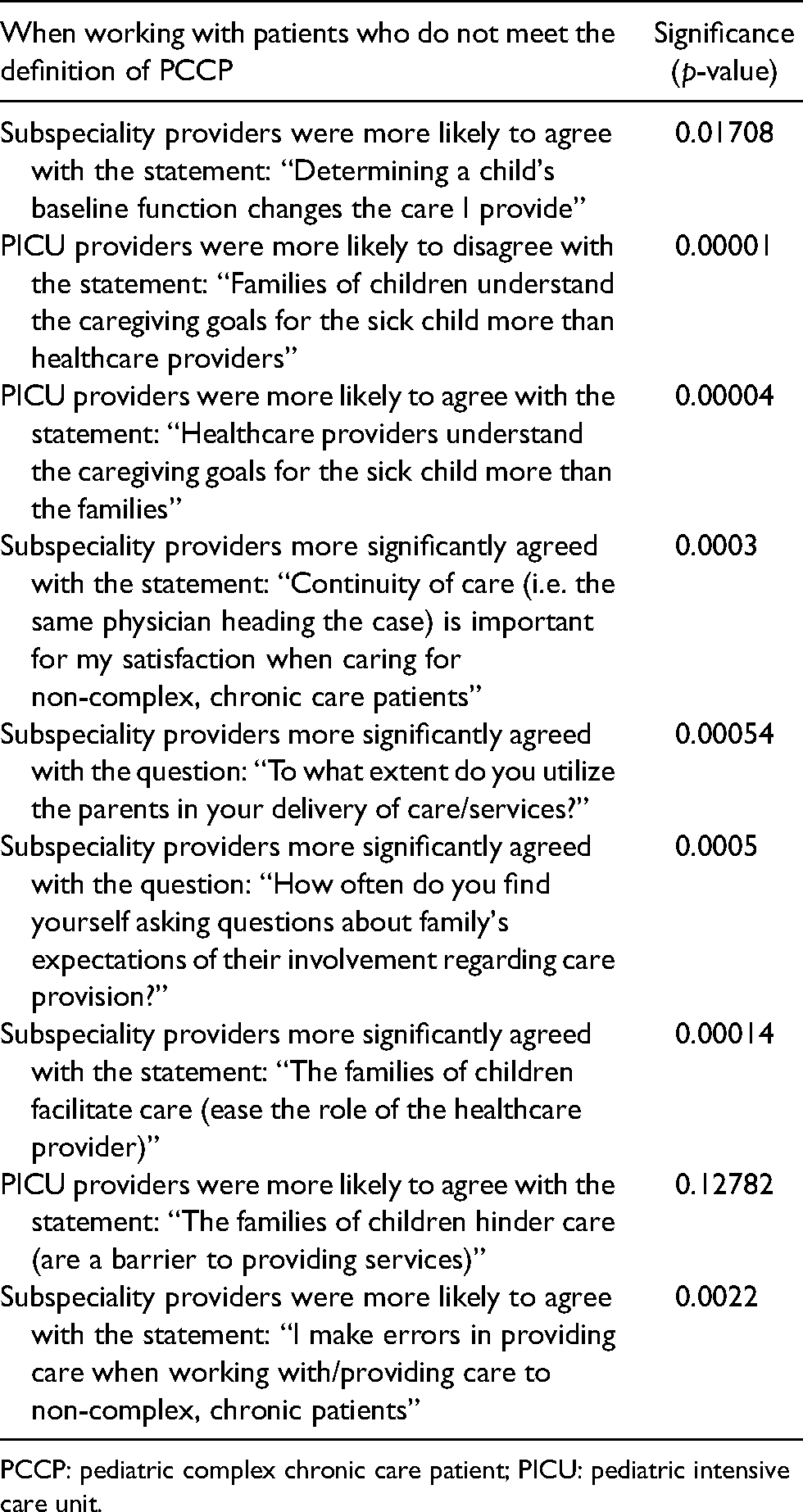
PCCP: pediatric complex chronic care patient; PICU: pediatric intensive care unit.
A comparison of PICU and subspeciality providers persprctives regarding PCCPs.
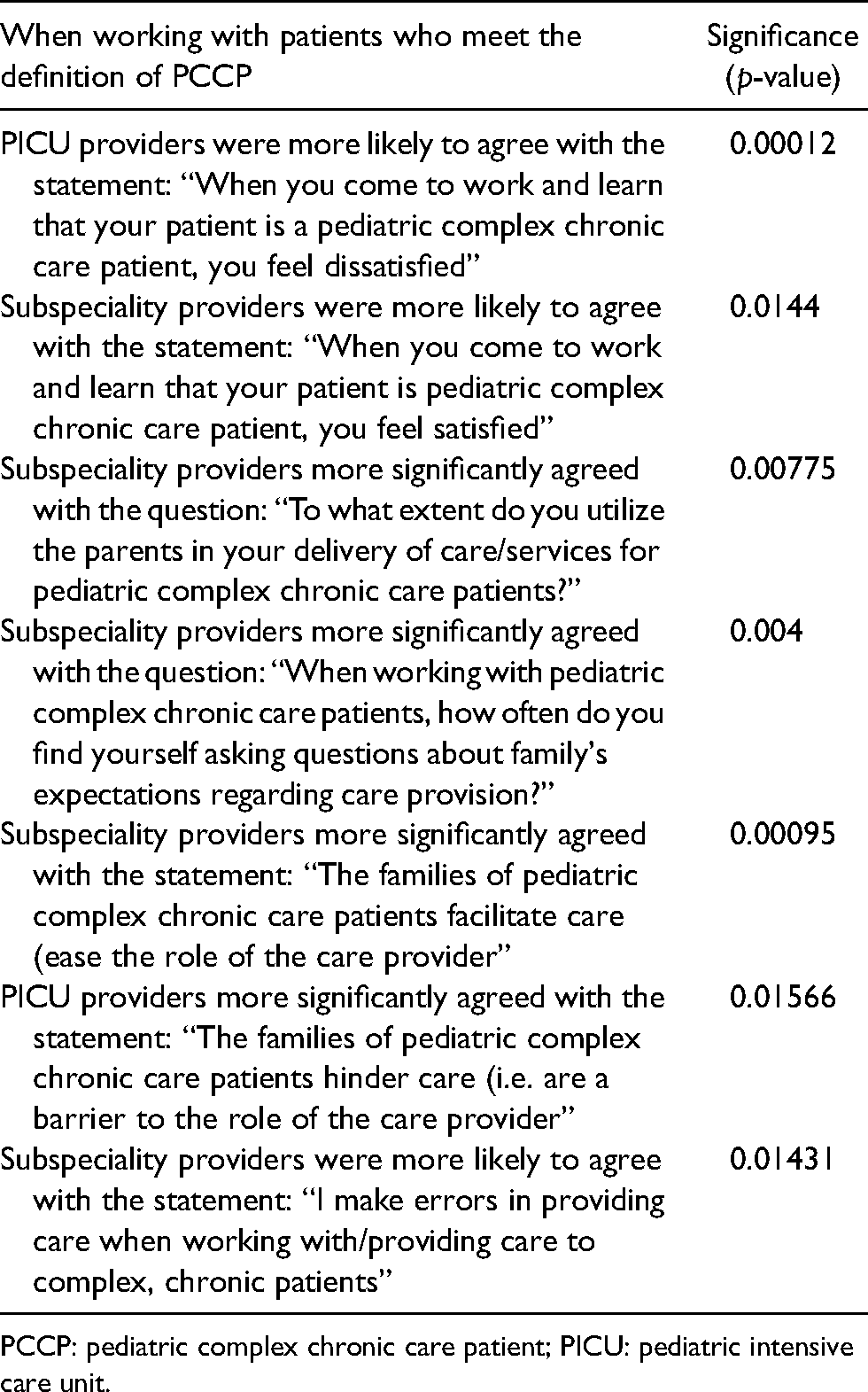
PCCP: pediatric complex chronic care patient; PICU: pediatric intensive care unit.
Summary of themes comparing perspectives between PICU and subspecialty providers.
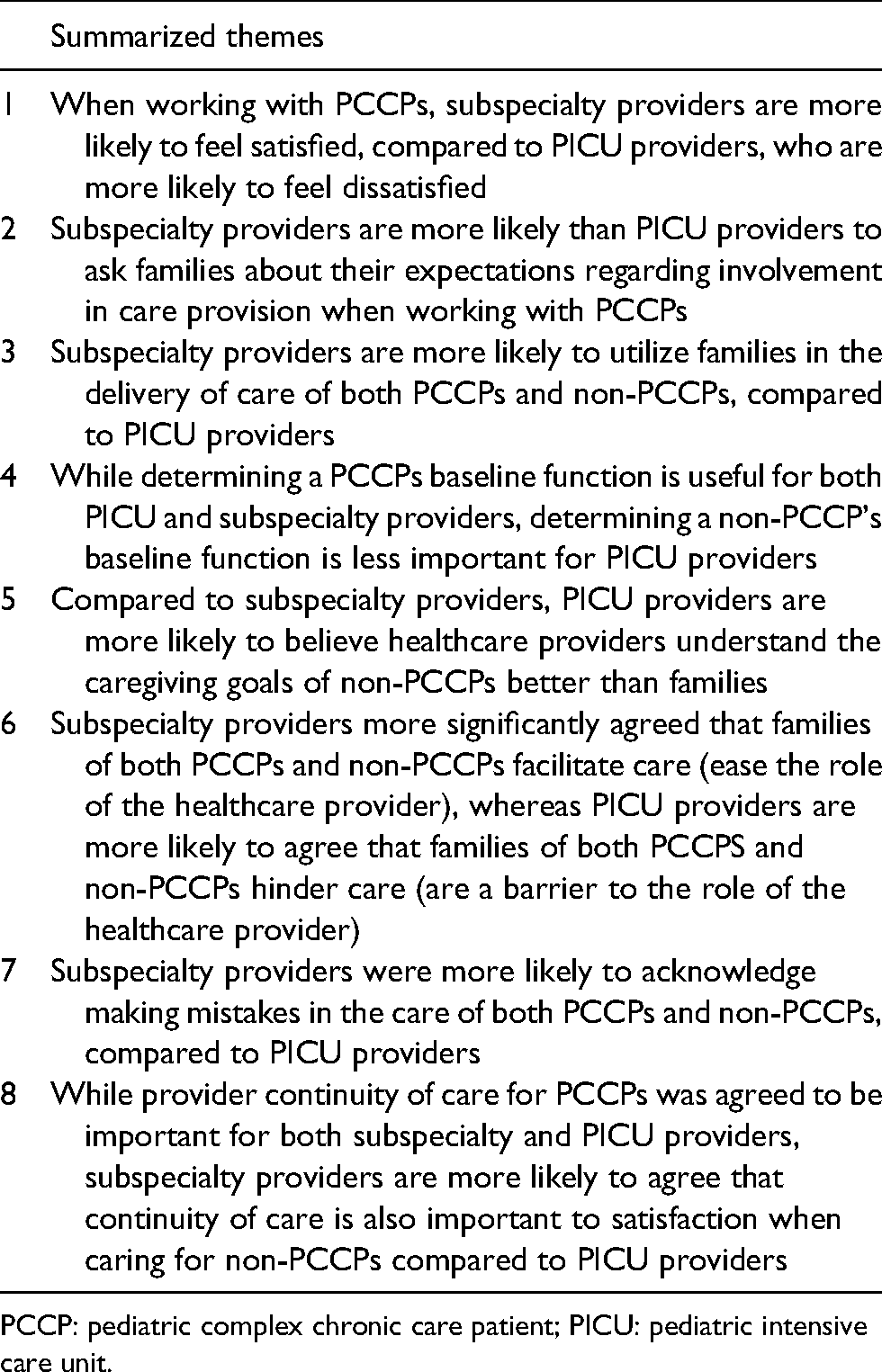
PCCP: pediatric complex chronic care patient; PICU: pediatric intensive care unit.
Themes from Likert scale questions comparing responses from subspecialty and PICU providers
When working with patients who do not meet the definition of PCCP: (1) Subspeciality providers were more likely to agree with the statement: “Determining a child's baseline function changes the care I provide”; (2) PICU providers were more likely to disagree with the statement: “Families of children understand the caregiving goals for the sick child more than healthcare providers”; (3) PICU providers were more likely to agree with the statement: “Healthcare providers understand the caregiving goals for the sick child more than the families”; (4) Subspeciality providers more significantly agreed with the statement: “Continuity of care (i.e. the same physician heading the case) is important for my satisfaction when caring for non-complex, chronic care patients”; (5) Subspeciality providers more significantly agreed with the question: “To what extent do you utilize the parents in your delivery of care/services?”; (6) Subspeciality providers more significantly agreed with the question: “How often do you find yourself asking questions about family's expectations of their involvement regarding care provision?”; (7) Subspeciality providers more significantly agreed with the statement: “The families of children facilitate care (ease the role of the healthcare provider)”; (8) PICU providers were more likely to agree with the statement: “The families of children hinder care (are a barrier to providing services)”; and (9) Subspeciality providers were more likely to agree with the statement: “I make errors in providing care when working with/providing care to non-complex, chronic patients” (Table 2).
When working with patients who meet the definition of PCCP: (1) PICU providers were more likely to agree with the statement: “When you come to work and learn that your patient is a pediatric complex chronic care patient, you feel dissatisfied”; (2) Subspeciality providers were more likely to agree with the statement: “When you come to work and learn that your patient is pediatric complex chronic care patient, you feel satisfied”; (3) Subspeciality providers more significantly agreed with the question: “To what extent do you utilize the parents in your delivery of care/services for pediatric complex chronic care patients?”; (4) Subspeciality providers more significantly agreed with the question: “When working with pediatric complex chronic care patients, how often do you find yourself asking questions about family's expectations regarding care provision?”; (5) Subspeciality providers more significantly agreed with the statement: “The families of pediatric complex chronic care patients facilitate care (ease the role of the care provider”; (6) PICU providers more significantly agreed with the statement: “The families of pediatric complex chronic care patients hinder care (i.e. are a barrier to the role of the care provider”; and (7) Subspeciality providers were more likely to agree with the statement: “I make errors in providing care when working with/providing care to complex, chronic patients” (Table 3).
Summary of themes from Likert scale questions
These statistically significant themes from the Likert Scale questions were then summarized into eight overarching themes (Table 4): (1) when working with PCCPs, subspecialty providers are more likely to feel satisfied, compared to PICU providers, who are more likely to feel dissatisfied; (2) subspecialty providers are more likely than PICU providers to ask families about their expectations regarding involvement in care provision when working with PCCPs; (3) subspecialty providers are more likely to utilize families in the delivery of care of both PCCPs and non-PCCPs, compared to PICU providers; (4) while determining a PCCPs baseline function is useful for both PICU and subspecialty providers, determining a non-PCCP's baseline function is less important for PICU providers; (5) compared to subspecialty providers, PICU providers are more likely to believe healthcare providers understand the caregiving goals of non-PCCPs better than families; (6) subspecialty providers more significantly agreed that families of both PCCPs and non-PCCPs facilitate care (ease the role of the healthcare provider), whereas PICU providers are more likely to agree that families of both PCCPS and non-PCCPs hinder care (are a barrier to the role of the healthcare provider); (7) subspecialty providers were more likely to acknowledge making mistakes in the care of both PCCPs and non-PCCPs, compared to PICU providers; and (8) while provider continuity of care for PCCPs was agreed to be important for both subspecialty and PICU providers, subspecialty providers are more likely to agree that continuity of care is also important to satisfaction when caring for non-PCCPs compared to PICU providers.
Themes from short answer questions comparing responses from subspecialty and PICU providers
Specific themes also emerged from the pediatric subspecialty provider survey's short answer questions. These themes were compared to those from the PICU provider study. There were several common themes between subspecialty and PICU providers. Both subspecialty and PICU providers identified several key differences when working with PCCPs, compared to working with non-PCCPs, including: (1) the increased time/resource burden; (2) managing expectations of patients/families; (3) navigating discrepancies regarding goals of care; (4) complexity of coordination between many services to ensure alignment between treatment plans and goals of care; (5) increased efforts in coordinating discharge from hospital and; (6) working with medicalized families and patients. Further, both PICU and subspecialty providers agree that the roles of families/parents of PCCPs varied from those of non-PCCPs in that families of PCCPs are primary decision makers, care providers outside of the hospital, historians, establish the child's baseline, advocate, provide support, and are deeply involved in the designing and delivery of healthcare plans. Additionally, both subspecialty and PICU providers agreed that families of PCCPs make significant sacrifices to care for their child including, but not limited to monetary expenses, time demands, and career sacrifices. Both PICU and subspecialty providers identified specific factors they believe would facilitate the care provided to PCCPs. These included: (1) improving access to funding; (2) improving discharge planning; (3) improving methods of communicating between specialists; and (4) continuity of healthcare providers who are involved in care delivery.
Several themes emerged from the subspecialty provider survey that did not transpire in the PICU provider survey. These themes included: (1) the challenge of coordinating outpatient subspecialist appointments to minimize the number of visits for families; (2) the challenge of information gathering regarding previous treatment plans and coordination between specialties; (3) the role of parents as “quarterback” in navigating care; (4) the lack of a primary healthcare provider (i.e. physician or nurse coordinator) to quarterback care; and (5) barriers to care such as excessive paperwork and time demands without corresponding compensation. Several factors that could enhance care for PCCPs were identified including: (1) reduced patient load without compromising overall provider compensation; (2) chronic care clinics to quarterback and provide continuity of care; (3) improved access to mental health services and therapies (i.e. speech-language pathology, physical therapy, occupational therapy, etc.); and (4) PCCPs co-managed when receiving tertiary care with acute inpatient physician and chronic care physician (i.e. the PCCP's primary provider in complex care clinics or the outpatient setting).
Discussion
The present survey evaluated pediatric subspecialists’ attitudes and perspectives regarding PCCPs, compared to non-PCCPs. Despite a number of challenges identified when caring for PCCPs, there was no significant difference in subspecialty provider attitudes when comparing care provision to PCCPs versus non-PCCPs. In contrast, our previous survey that explored PICU provider's attitudes and perspectives exposed several statistically significant differences. 22 However, several statistically significant themes were exposed when comparing pediatric subspecialist attitudes and perspectives with PICU providers attitudes regarding PCCPs (Tables 3 and 4). These statistically significant results were then summarized into eight overarching themes (Table 4).
The survey's short answer questions revealed a number of factors that may facilitate care provided to PCCPs including: access to funding; discharge planning; communication methods between specialists; and healthcare provider continuity. Furthermore, the short answer questions identified several differences when working with PCCPs, compared to non-PCCPs such as: increased time/resource burden; managing expectations of patients/families; navigating discrepancies in goals of care; complexity of coordination between services; increased efforts in coordinating discharge from hospital and working with medicalized patients/families.
To our knowledge, this study is the first to identify differences in attitudes between pediatric subspecialists and PICU providers regarding PCCPs. Traditionally, the focus of the PICU has been on provision of life saving measures for critically ill children.24,25 However, advancements in medical technology has resulted in the survival of many children who would have previously perished.24,26 In turn, these children often develop complex and chronic health conditions that require an increased level of care while hospitalized.17,24,26 As significant increases of PCCP admissions7,10,17,24,25 occurred, the culture of PICU evolved with a broader focus, encompassing values such as functional outcome and quality of life.17,24,27 To some, this paradigm shift may have conflicted with previous expectations and perceptions. Similarly, as PCCPs mortality is higher than non-PCCPs,8,12 PICU providers are continuously involved in challenging discussions around goals of care, palliation, and parental expectations, as unpredictable clinical trajectories may lead to uncertain outcomes. Although to our knowledge this is the first study to explore differences regarding PCCPs between pediatric subspecialists and PICU providers, given the increasing population of PCCPs in the PICU, this topic asserts increasing relevance and has the opportunity to provide meaningful clinical insight.
Several themes emerged from the survey's short answer questions which have been identified in prior research. First, previous literature reported parents of PCCPs self-identified roles which included the good parent, health care provider, student, advocate, detective, teacher, and case manager. 16 These align with the current study which reported pediatric subspecialists’ perception of PCCP's parents’ roles as primary decision makers, care providers outside of the hospital, historians, sources of the child's baseline, advocates, support providers, and recognition of parents’ involvement in formulating and executing care plans.
Second, previous literature acknowledges the unfavorable impact raising a PCCP has on a parents’ own physical and mental health.
16
The present study correspondingly identified a gap in services available to support parents, such as: resources to ease the strain of care provision for parents (i.e. speech language pathology, occupational therapy, physical therapy, etc.), and the value of access to mental health services for both the PCCP and their parents. In addition, the present study noted the various accommodations parents of PCCPs make, including economic expenses, time demands, and career sacrifices. A quote emerged from one of the survey respondents regarding the systemic pressure placed on parents: Sometimes I believe, the family system is unprepared to provide care for this child at home. Our system does not question whether the family believes they can take on this task, it just assumes they will.
Despite systemic awareness of the physical, emotional, and financial stressors on parents of PCCPs, there is an existing lack of systemic resources to adequately support these families, and an implicit assumption that they will have the capacity to adjust and cope at home. It is estimated that PCCPs make up <1% of the general pediatric population, 28 but in the foster care system approximately 10% are described as medically fragile or complex, and 50% are reported to have chronic problems (i.e. visual loss, hearing loss, neurological disorders, etc.). 29 Coordinated multidisciplinary teams and system advocacy are required for PCCPs and their families to successfully meet the challenges and complexities of their child's care needs. Preparing parents and coordinating the resources necessary to care for a PCCP may enhance outcomes for PCCPs and their caregivers.
Previous literature regarding PCCP's parents’ experiences with hospital readmissions, reported themes including: lack of care continuity; poor communication between specialties; and challenges surrounding discharge (i.e. difficulty filling prescriptions, not receiving all required elements to execute the management plan, a lack of long-term planning, and challenges with follow-up). 20 Interestingly, in our research, pediatric healthcare providers shared many of same systemic impediments/frustrations. For example, both the previous PICU provider survey and the present subspecialty provider survey identified several factors which healthcare providers believe would facilitate care provision for PCCPs including improving: (1) access to funding; (2) discharge planning; (3) methods of communicating between specialists; and (4) continuity of healthcare providers involved in care.
Implementing some of the above initiatives may have the potential to alleviate some of the previously identified tensions between PCCP's families and healthcare providers, increase rapport between providers and families, improve services and opportunities for PCCPs, shorten the length of hospital admissions by improving discharge coordination, improve communication between specialists and improve the overall care provided to PCCPs.
One potential approach to apply the previously identified initiatives would be the implementation of complex care clinics. When asked about the means of facilitating care provided to PCCPs, subspecialty providers noted that chronic/complex care clinics would be extremely beneficial to coordinate and reduce the number of appointments for families, cultivate healthcare provider continuity of care, promote alignment between various healthcare provider treatment plans and goals of care, and to reduce the parent's burden of having to “quarterback” care. Institutions that employ an integrated complex care model involving interdisciplinary complex care teams report a number of benefits including enhancing healthcare provider job satisfaction, increasing fluency of care, improving time efficiency, aligning goals, 30 enhancing organization, 31 improving discharge efficiency, 32 and generally contributing to better outcomes. 30 Survey respondents also noted that it would be beneficial for complex care clinics to have longer patient appointment times than traditional appointments to allow for the increased amount of paperwork and address the complexity of patient/family concerns, without compromising financial compensation.
Another factor identified that has the potential to contribute to the facilitation of care involves the implementation of a discharge coordinator. In recent years, discharge coordinators have become an increasingly common addition to the pediatric wards; yet are still not accessible in all centers. Discharge coordinators schedule follow-up appointments, 33 ensure patients and families receive the necessary information to optimize the chance for a successful discharge, provide a link between families and healthcare providers, 34 collaborate with multi-disciplinary services and community agencies, 33 facilitate continuity of care, increase patient/family satisfaction, shorten mean length of stay, 34 improve discharge time, and ease the discharge-admission bottleneck during periods of high patient volume. 35 Thus, complex care clinics and discharge coordinators both serve as a potential means to ease tensions between healthcare providers and families, and facilitate care for PCCPs.
Interestingly, a novel theme that arose in the subspecialty provider survey proposed the notion that PCCPs, could be co-managed by their primary complex care physician (i.e. from complex care clinic) when admitted to an acute care service. No one [is] taking primary ownership. Chronic patient [are] sitting in PICU being cared for by PICU MDs who are better suited to manage acute issues rather than chronic issues.
It was reported that this co-management would promote communication between specialties, alleviate some of the parents’ burden with regard to establishing the child's baseline and being an avid historian, may alleviate some of the inherent stress of hospitalization for families given the pre-established rapport with their primary provider, and ease the transition to lower acuity or outpatient care. A primary complex care physician may also augment the role of the acute care service by facilitating communication between specialties and promoting opportunities for a broad-based approach. However, our review of the literature did not reveal any previous research regarding co-management of PCCPs between an acute care service and a complex care pediatrician. Therefore, it would be worthwhile for further literature to explore this concept. An iterative process of discussion, development and assessment with all stakeholders would be imperative prior to any implementation of this novel style of care.
The present study is not without limitations. The surveys administered were limited to a single center which does not have organized complex care clinics, and thus may not be generalizable to all other centers. In addition, despite a rigorous process of survey development involving feedback and subsequent modification, the survey's psychometric properties were not formally examined. Further, while all pediatric subspecialty providers at the Jim Pattison Children's Hospital were surveyed, the relatively small sample size (N = 46) and survey response rate of 52.2% may not adequately encompass all pediatric subspecialty provider perspectives. Canada's publicly funded healthcare system may limit generalizability to healthcare systems using alternative models of funding and delivery. Given the somewhat broad definition of PCCPs, it is not possible to assure that all survey respondents interpreted the definition provided as intended by the researchers. The use of a seminal definition in the literature, a survey modeled after previous literature, and a pilot study aimed to mitigate these potential concerns. Despite promised anonymity through the use of the REDCap application, 23 it is possible that healthcare providers were not entirely candid in their responses, or chose to withhold information due to apprehension about portraying oneself in an unfavorable light or any perceived consequences of voicing controversial opinions.
The findings of this study address a significant gap in the literature, motivate future research, and contribute to potential opportunities to augment care provided to PCCPs. The increasing prevalence of PCCPs globally necessitates a need to better understand how PCCPs fit into the current culture of healthcare. It would be interesting for future research to explore healthcare providers perspectives of PCCPs in other countries that may have different healthcare systems/models. PCCPs and their family's experiences with healthcare includes a significant amount of care coordination and transcends many healthcare services including acute care, inpatient care, outpatient care, home care, and beyond. Evaluating healthcare provider perspectives when working with PCCPs promotes an enhanced understanding and provides potential opportunities to optimize care provided, including opportunities for care coordination. While improving the care provided to PCCPs is a valuable venture, it is essential to include all relevant parties in the evolution of care, and comprehensively examine the broad impacts for institutions, healthcare providers, families, and PCCPs themselves.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.