
Abstract
Clinical pathways were first developed at Sheikh Khalifa Medical Centre (SKMC), Abu Dhabi, in 2001 – one year after the facility first opened. Long lengths of stay and unjustified variances in clinical practice were the main reasons for the development. Laparoscopic cholcyctectomy was the first to be implemented six months after development began. Convincing the workgroup members to buy into clinical pathways was difficult in the initial stages of development, but after highlighting the benefits of clinical pathways, they became more receptive to change. Other problems that were faced during the development was the limited use of clinical pathways in the region, the rapidly changing workforce, the cultural/religious need of the patient and varied knowledge base among nursing staff. There were also many advantages to developing pathways in the Middle East; diverse workforce and an ever-changing work environment helped to make clinical pathways at SKMC effective in delivering high standards of care. There are currently nine clinical pathways: surgical, medical and paediatric, and two in development – paediatric acute gastroenteritis and coronary artery bypass grafting. Lengths of stay have been reduced since implementing clinical pathways, some more significant than others. In future months, clinical pathways will be in electronic format and will be known as power plans.
Introduction to the United Arab Emirates
Abu Dhabi is the capital of the United Arab Emirates (UAE), a federation of seven Emirates formed in 1971. The area was previously known as the Trucial states, referring to the nineteenth century truce between Britain and several Arab Sheikhs. The Emirates are situated in the eastern part of the Arabian Peninsula, extending along part of the Gulf of Oman and the southern coast of the Arabian Gulf.
The population of the UAE is around four million with only 11% being UAE nationals. Other Arabic nationals make up 21%, south Asians make up 57% and people from the western nations make up the remaining 11%.
Sheikh Khalifa Medical Centre (SKMC) in Abu Dhabi opened its doors in February 2000 to provide secondary and tertiary care to UAE nationals. Prior to its opening, citizens of the UAE often travelled to Europe and the USA for health care if it could not be provided in the UAE.
Guided privately under the management of Inter-health Canada Management Ltd, SKMC is an acute care hospital with 223 beds providing internationally accepted high standards of care.
In May 2003, restructuring combined the Abu Dhabi Ministry of Health facilities with the General Authority of Health Services (GAHS) for the emirate of Abu Dhabi and the expansion of what is now known as Sheikh Khalifa Medical City began. This process is ongoing and has led to enormous growth and change, putting pressure on both resources and personnel.
Sheikh Khalifa Medical City currently comprises acute care, behavioural sciences and primary health, employing approximately 6000 staff from over 50 different countries.
Development of Clinical Pathways at Sheikh Khalifa Medical Centre
Clinical pathways were developed in SKMC in 2001, one year after the facility first opened. Hospital management identified many factors influencing the need for pathways including high lengths of stay and unjustified variations in clinical practice. SKMC employed a multicultural and diverse workforce with different ideas and perceptions on how patients are best managed.
Physicians and nurses often continued to follow guidelines set by their respective countries of origin. With such variances in health-care management, it was decided to streamline and improve patient care by developing clinical pathways.
A clinical pathway coordinator was appointed and her role was defined. Then the hard work began. It was decided to begin with a surgical group of patients with a relatively low length of stay for ease of initial development. Laparoscopic cholcyctectomy was high on the list of the top 20 surgical admissions over the previous few months and was, therefore, chosen. The coordinator specified components crucial to the development of pathways to be:
Standard terminology;
Standard format;
Written standards for developing, implementing and evaluating clinical pathways;
A documented development process;
Specifically designed educational materials; and
Organizational support.
The coordinator scheduled the first meeting. She identified both the work group, chosen because of their surgical knowledge, and the steering committee comprising of senior staff. Key stakeholders were invited along to be involved from the early stages of development. It was felt that it would be beneficial to have a physician champion to support and give input, thus ensuring successful pathway development. The group discussed the purpose of clinical pathways, what they were, and why it was so important that they be implemented at SKMC. Some members of the group were familiar with pathways, and some even assisted in development of other pathways prior to their employment at SKMC. Following literature searches, process mapping and many workgroup meetings, the clinical pathway for laparoscopic cholecystectomy was ready for trial six months after the development began. The pathway was trialled for three months before finally being approved as an operational document.
Another area that needed to be addressed in the early stages of development was the link between clinical pathways and Meditech, the hospital health information system. After some in-house modifications, pathways were incorporated into the system and data captured on the pathway documentation tool by the attending nurse were extracted and entered into the system on a daily basis and then transmitted to a central database for analysis. The database also helped the coordinator develop a reporting system by generating a report containing average and actual amounts of variances, as well as average and actual lengths of stay. The coordinator then had an effective mechanism to monitor pathway volume and to analyse variances.
Problems Faced with the Development and Implementation of Clinical Pathways
In the initial stages of development, it became apparent that many of the workgroup members had either very little pathway experience or even negative experiences. Convincing them to buy the concept of clinical pathways was difficult, but crucial to success. Highlighting how clinical pathways can directly improve quality care, contain costs and increase appropriate bed utilization can lead to positive patient and health-care provider outcomes helped them become more receptive to change.
Another problem the group faced was the limited use of pathways in the Middle East for comparison. It would have been beneficial to discuss the challenges faced with a facility that had actually encountered the same difficulties. Developing and implementing pathways in the UK is quite different from the Middle East. Sharing these experiences may have had positive outcomes. Most of the clinical staff only come to the Middle East for a short period of time on short-term contracts, one to two years on average. This means a rapidly changing workforce. Some members of the workgroup completed their contract during the development phase of the pathway, leading to change in group dynamics, often with a negative impact. The same problem was faced once the pathway was developed and operational. Clinical pathway education is vital both for new staff and current staff, especially when revisions have been made. To combat this problem, the pathway coordinator presents pathway information to all new clinical staff during their orientation period to the hospital.
The pathway had to also reflect the cultural and religious needs of the patient. During the holy month of Ramadan, every Muslim is expected to fast from dawn till dusk for the entire month. As the majority of patients who would be following the pathway would be Muslim, it was vital that pathway development took this into consideration. It was predicted that there would be many more variances throughout this month and, where applicable, some would be classified as unavoidable, respecting the patient as an individual.
There were also difficulties when implementing the pathways. The knowledge base was varied between nursing staff, in particular relating to clinical pathways. Some of the nurses were very familiar with them and adjusted to the change with ease, while others took longer to adapt to the changing style of patient management and documentation. Clinical pathways are well known in the UK, Australia and Canada, but they are limited in use in India and the Philippines, from where a vast majority of the nurses originate.
As English is not the first language of the majority of staff, difficulties with communication were sometimes apparent during the implementation phase. Teaching sessions were sometimes longer than anticipated to ensure complete understanding and compliance during the introduction of pathways. These difficulties were relatively minor and easily rectified. Translators were always readily available, so that communication between nurses, physicians and patients was never identified as a significant problem.
Advantages of Developing and Implementing Clinical Pathways in the Middle East
There are also advantages in implementing clinical pathways in the Middle East. As mentioned previously, SKMC employs a very diverse workforce from all parts of the world. The education each health-care provider received is unique to their country, providing the facility with a variety of styles of education. This ensures that the pathways developed are based upon a combination of evidence-based clinical practices from a variety of different sources.
SKMC is a new facility which has grown and developed extensively throughout the last two years and has seen many changes in a short period of time. Health-care providers are used to this ever-changing environment, which makes them more receptive to new ideas and strategies to deliver high standards of care.
In line with most Middle-Eastern hospitals, SKMC has a quick turnaround of staff, reflecting the nature of the region. When the pathways are revised, there are often only a few remaining members of the original workgroup, if any. This has both positive and negative impacts. The pathway is viewed in a different way. Therefore, the flaws in the original document can be highlighted and revised accordingly. On the other hand, as it was developed by a different group of health-care providers, the new group may not agree with the pathway contents, and the pathway, therefore, may need extensive revision. Fortunately, the latter example has never occurred.
Clinical Pathways at Sheikh Khalifa Medical Centre
There are nine clinical pathways that are operational at SKMC. They are acute coronary syndrome, cardiac catheterization, tonsil and adenoidectomy, adenoidectomy, myringotomy, paediatric diabetic management, laparoscopic cholecystectomy, total hip replacement and total knee replacement.
A pathway for paediatric acute gastroenteritis in the Emergency Room has been trialled and is awaiting medical records approval.
A pathway for coronary artery bypass grafting is in development stages.
A clinical pathway has four components:
Pre-printed orders (physicians’ orders);
Pathway (documentation tool);
Patient pathway (patient information); and
Variance tracking (outcome measurement).
The doctors’ pre-printed orders are designed and approved by the medical team and the pathway is developed accordingly.
The clinical pathway has three categories: care, interventions and outcomes.
Content of the pathway includes assessments, consultations, tests, treatments, activities, diet, medications, elimination, patient and family education, and discharge planning.
Some of the pathways commence when the patient arrives at the pre-admission clinic, some when the patient arrives at the Emergency Room and some when the patient arrives at the admitting ward.
For ease of identification, a yellow sticker is placed on the patients chart stating that the patient is following a clinical pathway.
Variances are charted if the outcome is not achieved based on the intervention and then documented accordingly. Variances are categorized into types: patient, family, hospital care-givers, physician and hospital system.
Patient pathways are educational materials comprising general hospital and clinical pathway information in simple language that the patient will understand. They are printed in both English and Arabic.
The acute coronary syndrome pathway is presently undergoing some major changes. It was felt that dividing the pathway into ST Elevation Myocardial Infarction/Primary Percutaneous Coronary Intervention (PPCI) and Non-ST Elevation Myocardial Infarction/Unstable Angina would enhance patient care due to the focus on door-to-balloon time for patients who require PPCI. This was not included in the current acute coronary syndrome pathway.
Lengths of stay have been reduced since pathway implementation, some more significant than others. (Table 1).
Reduction in lengths of stay since implementation of clinical pathways
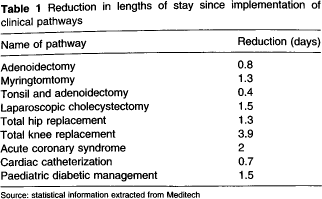
Source: statistical information extracted from Meditech
The Future of Clinical Pathways at Skmc
In coming months, the introduction of a more comprehensive health information system, Cerner, will facilitate documentation and information retrieval, leading to the provision of seamless care.
In Cerner, clinical pathways are in an electronic format and are known as power plans. There are presently five power plans programmed into the system and, once it ‘goes live’, the remainder will be entered.
High on the agenda in coming months are patient and staff satisfaction surveys to monitor clinical pathway effectiveness, thereby leading to continuous quality improvement.